Report: COVID-19 Tracking Survey and Focus Groups on Canadians' Views 2022-23
Submitted to
Department of Health Canada
Prepared by
Leger
Contract number: HT372-224613
POR 021-22
Contract Value: $282,441.24 (HST included)
Awarded 2022-08-05
Project 14224-016
Leger
507 Place d'Armes, Suite 700
Montréal, Québec
G1R 2K2
Phone: 514-982-2464
Fax: 514-987-1960
For more information on this report, please contact Health Canada at: hc.cpab.por-rop.dgcap.sc@canada.ca
Ce rapport est aussi disponible en français.
COVID-19 Tracking Survey and Focus Groups on Canadians' Views 2022-23
Prepared for Health Canada
Supplier Name: Leger
Executive Summary
March 2023
This public opinion research report presents the results of a tracking survey conducted by Leger Marketing Inc. on behalf of Health Canada. The research was conducted with the Canadian general population.
Cette publication est aussi disponible en français sous le titre : Sondage de suivi et groupes de discussion concernant le point de vue des Canadiens sur la COVID-19 2022-23.
This publication may be reproduced for non-commercial purposes only. Prior written permission must be obtained from Health Canada. For more information on this report, please contact Health Canada at hc.cpab.por-rop.dgcap.sc@canada.ca or at:
Health Canada, CPAB
200 Eglantine Driveway, Tunney's Pasture
Jeanne Mance Building, AL 1915C
Ottawa, Ontario K1A 0K9
Catalogue Number: H14-389/2023E-PDF
International Standard Book Number (ISBN): 978-0-660-47962-0
Related publications (registration number:): Catalogue Number: H14-389/2023F-PDF (Final Report, French)
ISBN: 978-0-660-47963-7
© His Majesty the King in Right of Canada, as represented by the Minister of Health, 2023.
Table of contents
- 1. Executive summary
- 1.1 Background and objectives
- 1.2 Quantitative methodology for Wave 16
- 1.3 Overview of findings of Wave 16
- 1.4 Qualitative methodology for Wave 17
- 1.5 Overview of findings of Wave 17
- 1.6 Quantitative methodology for Wave 18
- 1.7 Overview of findings of Wave 18
- 1.8 Qualitative methodology for Wave 19
- 1.9 Overview of findings of Wave 19
- 1.10 Quantitative methodology for Wave 20
- 1.11 Overview of findings of Wave 20
- 1.12 Intended use of the research results and benefits for canadians
- 1.13 Statement of limitations
- 1.14 Notes on interpretation of research findings
- 1.15 Political neutrality statement and contact information
- 2. Detailed results for Wave 16
- 3. Detailed results for Wave 17
- 4. Detailed results for Wave 18
- 5. Detailed results for Wave 19
- 6. Detailed results for Wave 20
- 7. Trends across the waves
- Appendix A: Detailed research methodology
- Appendix B: Survey questionnaire – WAVE 16
- Appendix C: Screening guide – WAVE 17
- Appendix D: Discussion guide – WAVE 17
- Appendix E: Survey questionnaire – WAVE 18
- Appendix F: Screening guide – WAVE 19
- Appendix G: Discussion guide – WAVE 19
- Appendix H: Survey questionnaire – WAVE 20
1. Executive summary
Leger is pleased to present Health Canada with this report on findings from wave sixteen (3.1) to wave twenty (3.5) of the tracking survey on respondents' views relating to COVID-19 issues. This report presents the results of three waves of quantitative surveys and two waves of qualitative research.
This report was prepared by Leger who was contracted by Health Canada (contract number HT372-224613 awarded August 5, 2022).
1.1 Background and objectives
The COVID-19 pandemic has been a significant challenge for the entire world. Since the beginning of the pandemic, the Government of Canada has acted — in collaboration with provincial and territorial governments and international partners—to minimize the health, economic, and social impacts of this evolving public health issue. Part of Health Canada (HC) and the Public Health Agency of Canada's (PHAC) response to COVID-19 is a tailored and ongoing public education and advertising campaign, to ensure that the response is effective and appropriate, HC and PHAC rely on several feedback mechanisms, including public opinion research (POR).
In addition to gathering information through POR on COVID-19 from various sources (e.g., PCO, external research firms, StatCan), since 2020, HC and PHAC have conducted a tracking survey using a multi-wave approach to seek Canadians' views, opinions and behavioural information on COVID-19 issues, as well as their mental health concerns and access to mental health services, allowing the timely development of effective communications and initiatives.
As Canada and the world gradually transition from a pandemic to an endemic state, Health Canada continued to track Canadians' awareness, opinions and behaviours through quantitative and qualitative research to ensure constant communications' effectiveness.
1.2 Quantitative methodology for Wave 16
The quantitative research was conducted through online surveys using Computer Aided Web Interviewing (CAWI) technology. The online survey was conducted from September 8 to 29, 2022. The participation rate for the survey was 12.41%. Calculation of the Web survey's participation rate is presented in Appendix A. A pre-test of the survey questions was carried out by conducting 43 interviews in both official languages (27 in English, 16 in French). The pre-test was completed on September 8, 2022. Survey interviews lasted 10 minutes on average.
A total sample of 3,004 Canadian adults were surveyed in all regions of the country, including an oversample of 400 Black-identifying individuals and 200 Indigenous-identifying individuals.
Special attention was given to ensure a distribution of respondents that provides a sufficient sample size to support analyses in the subgroups of the sample. The following table shows the effective sample collected by Leger in the different regions of the country:
| Region | Number of respondents |
|---|---|
| Ontario | 1,127 |
| Quebec | 761 |
| British Columbia and Territories | 360 |
| Alberta | 341 |
| Prairies | 219 |
| Atlantics | 196 |
| Total | 3,004 |
Based on the most recent data from Statistics Canada's national census, Leger weighted the results of this survey by age, gender, region, first language (mother tongue), education level, presence of children in the household, place of birth, and ethnicity. The most recent data regarding age, gender, region and first language was from the 2021 census. The data for education level, presence of children in the household, place of birth and ethnicity came from the 2016 census.
Details regarding the weighting procedures can be found in Appendix A.
As a member of the Canadian Research and Insights Council (CRIC), Leger adheres to the most stringent guidelines for quantitative research and acts in accordance with the Government of Canada requirements for quantitative research and Standards of the Conduct of Government of Canada Public Opinion Research. The details of the methodology and more information on Leger's quality control mechanisms are presented in Appendix A. The questionnaire is available in Appendix B.
1.3 Overview of findings of Wave 16
- A little less than half of the respondents (46%) had been (37%) or thought they had been (9%) infected with COVID-19, and a vast majority (86%) knew people in their immediate social network who had been infected.
- Overall, one person out of three considered themselves at risk. The proportion was higher among those over 55 years old (56%).
- Personal financial situation (22%) and the economy (17%) were the top two most pressing concerns, way ahead of physical health (9%) and the health of family/friends (9%).
- One person out of three rated their mental health as average (27%), bad (8%) or very bad (2%). Respondents under the age of 55, parents of children under 18, and those who had been infected with COVID-19 or believed they had been infected were more likely than other respondents to report their mental health as "average".
- One person out of ten (11%) had received mental health support in the month preceding the survey.
- Post-COVID concerns included crowded places (32%) and that the pandemic will never end (30%) for three people out of ten. One person out of five was not worried about COVID-19 (22%) or life after COVID-19 (19%), but the same proportion was worried about a new pandemic (20%).
- A vast majority of respondents were vaccinated at least once (92%): four in ten have received three doses (41%), and around one in four have either two (23%) or four doses (26%).
- Seven out of ten (71%) stated it was very (48%) or somewhat (23%) likely that they get a booster dose.
- The top three of reasons not to get a booster dose included: considering that current protection is enough (22%), belief that the vaccine does not protect much as infection remains possible (17%), and concern about the long-term effects of the vaccine (16%).
- Over eight children out of ten aged 12-17 were vaccinated with at least one dose: almost two-thirds were vaccinated with two doses (62%), and one in five had received three doses (21%).
- Around two-thirds of children aged 5-11 had received at least one dose of the COVID-19 vaccine (64%): 44% had received two doses, 13% had received one dose, and 7% had received three.
- Among parents of children under 18, the top reason for hesitation about vaccinating their children with a booster dose was the concern about long-term effects (26%).
- One out of five people (21%) stated that their children aged between 6 months and 5 years old were vaccinated (21%). One-third stated they would not get their child(ren) vaccinated (33%).
- Less than one person out of ten have stated that they missed or delayed their routine vaccinations because of the pandemic (8%).
- Confidence in vaccines was the same as before the pandemic for half the respondents (54%), while one in five stated being more confident (19%), and the same proportion stated being less confident now (21%).
- The top reasons for the decrease in general vaccine confidence included a negative impact of the COVID-19 vaccine on general views (44%) and increased concern about the safety of vaccines at large (44%).
- Half of the respondents planned on getting the flu shot in 2022 (48%). Those who did not mention never having gotten one as the main reason (47%).
- Washing hands (80%), staying home when sick (78%), and using hand sanitizer (66%) were the three individual public health measures that were practised by at least two-thirds of the population. Indoor (39%) and outdoor (21%) mask-wearing, along with improving ventilation (36%) were the three measures that were practised by less than half of the respondents.
- Over eight out of ten (84%) believed that individual public health measures help reduce the spread of other respiratory infectious diseases.
- Almost nine out of ten were confident in making their own decisions regarding the practice of public health measures (89%). Clear communications from the government and or public health officials on when and which individual public health measures should be used was considered the most useful element in helping decision-making (43%). Government of Canada websites (49%), local or regional health authorities (46%) were the main sources of information among respondents, along with conversations with their health care provider (47%).
- Three people out of ten (30%) stated feeling pressured by others to practise or not practice individual public health measures.
- Two people out of three (65%) stated being familiar with the potential long-term effects of COVID-19, and over half (54%) mentioned being very (17%) or somewhat (36%) worried about developing them. Worries about long-COVID were mainly due to uncertainty about future health prospects (67%) and limitations to leisure/personal life (64%).
1.4 Qualitative methodology for Wave 17
Leger conducted a series of eight virtual discussion group sessions with French-speaking and English-speaking Canadians recruited from all the regions in Canada. Participants were recruited, screened for vaccination status and assigned to virtual discussion groups by vaccination status and demographics of interest (e.g., young adults, parents, vaccinated/unvaccinated). Twelve participants were recruited by our professional recruiters for each discussion group session. A total of 64 recruits participated in the virtual discussion groups (see Table below for details). All participants received an honorarium of $135.
| Session detail | Date | Recruits | Participants | Language |
|---|---|---|---|---|
| #1 (Young adults, two doses (18-35), Ontario and ATL) | September 26th, 2022 | 12 | 8 | English |
| #2 (Young adults, two doses (18-35), BC, Prairies, Territories) | September 26th, 2022 | 12 | 9 | English |
| #3 (Young adults, two doses (18-35), QC, NB) | September 26th, 2022 | 12 | 9 | French |
| #4 (Gen pop 18+, three doses or more, BC, Prairies, Territories) | September 27th, 2022 | 12 | 8 | English |
| #5 (Gen pop 18+, three doses or more, Ontario and ATL) | September 27th, 2022 | 12 | 7 | English |
| #6 (Gen pop 18+, three doses or more, QC, NB) | September 26th, 2022 | 12 | 8 | French |
| #7 (Vaccinated parents (mix of unvaccinated and vaccinated child, BC, prairies, Ontario) | September 28th, 2022 | 12 | 5 | English |
| #8 (Vaccinated parents (mix of unvaccinated and vaccinated child), QC, NB) | September 27th, 2022 | 12 | 10 | French |
The virtual discussion group sessions lasted between 1h30 minutes and 2 hours and were conducted by a moderator using the CMNTY online platform. The choice of platform helped to facilitate the moderation, ensure an optimal interface between moderator and participants, and enable interaction as the discussion unfolded. The online platform also allowed for remote viewing of each session by Leger and Health Canada observers.
Further details regarding the qualitative methodology can be found in Appendix A. The screening and discussion guides are available in Appendix C and Appendix D.
1.5 Overview of findings of Wave 17
Concerns about COVID-19:
- Most participants mentioned that COVID-19 was not a top-of-mind concern anymore. They mentioned now living "normally" without thinking about it too much.
- Participants worried more about infecting other people with COVID-19, especially those who are vulnerable, rather than getting it themselves.
- Some participants mentioned getting anxious and worried when they felt any type of respiratory symptom and would wonder whether it was COVID-19 or just a common cold. Some parents mentioned they were worried about potential negative impacts on their children's schooling and their willingness to study.
- The fact that most participants had been infected with COVID-19 influenced their attitudes towards the pandemic: they felt like it was not "a big deal", and some of them considered that it was likely they would get it again, which did not bother them much.
- Regarding the end of fall and the arrival of winter, most considered that cases of COVID-19 were going to rise again, as well as infection with other illnesses (the flu and gastroenteritis).
- Although virtually all participants agreed that there will be a rise in cases of COVID-19 and possibly other diseases during the winter, they did not express much worry.
Public health measures:
- Most participants mentioned they continued to wash their hands and use hand sanitizer as frequently as possible. Hygiene measures seem to have become part of their daily habits.
- Most parents stated they kept their children at home if they had symptoms of any disease, not just COVID-19.
- In regard to masks, some participants mentioned not wearing them anymore unless it is mandatory (i.e., for travel), while others mentioned still wearing them in crowded or indoor places. Some participants mentioned they kept wearing masks by their own volition, out of consideration for more vulnerable people and those working in schools and hospitals.
- Aside from people working in schools or hospitals, participants were not really aware of ventilation measures other than opening windows. Most participants agreed that ventilation helps decrease the transmission of COVID-19 and other viruses but felt that it was a measure that may require more effort and time. They agreed that masks were a cheaper and efficient alternative for the time being.
Influence of COVID-19 infection:
- A majority of participants mentioned they had contracted COVID-19 at least once. Some had caught it before vaccine roll out, and others were infected after getting their primary doses. Most of them got tested, either by PCR or rapid tests.
- Different types of impacts of a COVID-19 infection were mentioned. Some of those who were infected and were already planning on getting their booster dose stated the infection did not have any impact on their intentions. Those who were already hesitant about getting the booster mentioned that since they were infected despite being vaccinated, and/or since their symptoms were mild, they did not see the need to get booster doses. Some participants mentioned they got sicker from the COVID-19 vaccine and booster than from the COVID-19 infection, which made them not want any other booster dose.
- On the other hand, others mentioned that because they did not get very sick from COVID-19, it meant that the vaccines were working, which motivated them to get the boosters.
Vaccines:
- Regarding the expression "staying up to date with COVID-19 vaccines," most participants agreed that it meant getting the latest booster dose available. Some participants mentioned feeling discouraged by this expression since they felt the booster vaccination was endless, as they were expected to get a booster dose on a regular basis for the foreseeable future.
- Some participants were very decided on getting all booster doses available to them in order to maximize their protection. They trust public health recommendations and follow them closely. On the other hand, a few participants considered that the booster doses were "overkill" and unnecessary. They felt like the initial doses were enough.
- The bivalent vaccine had a low awareness among participants. Most of them had not heard of it. Most participants mentioned that the existence of a bivalent vaccine did not change their intention to get a booster dose, because new variants were bound to appear, leading to the development of new doses.
Mental Health:
- The cost of living and inflation were seen as very impactful on mental health at large. These made participants feel anxious and helpless. Other elements that impacted their mental health were transitioning back to in-person activities and work, anxiety over small respiratory symptoms that immediately lead to suspecting being infected with COVID-19, personal health, and heavy workloads.
- A majority of participants mentioned the significant obstacles to accessing mental health care: lack of availability in the public system, prohibitive cost in the private system, etc.
- Some participants were dubious regarding online mental health services. They mentioned the importance of having in-person contact with the therapist or mental health professional to establish trust. For others, online resources were an option they would consider as they stated they would feel more comfortable talking about their personal issues in a virtual setting rather than in-person.
- Participants expected from the government to have a one-stop website referencing all types of help available. Since mental health is very personal and different from one person to another, some participants felt like the more information there is, the more chance people have to find the type of help that suits them.
- One participant indicated that they would have liked to see mental health resources available for children, especially during times of isolation, when the lack of social interactions weighted the most on children.
1.6 Quantitative methodology for Wave 18
The quantitative research was conducted through online surveys using Computer Aided Web Interviewing (CAWI) technology. The eighteenth wave of this online survey was conducted from November 18th to December 8th, 2022. The participation rate for the survey was 14.5%. Calculation of the Web survey's participation rate is presented in Appendix A. A pre-test of the survey questions was carried out by conducting 38 interviews in both official languages (25 in English, 13 in French). The pre-test was completed on November 18th, 2022. Survey interviews lasted 10 minutes on average.
A final sample of 3,000 Canadians was targeted, including 2,400 respondents from the general population and an oversample of Black (400) and Indigenous people (200). A total of 3,026 respondents completed wave 18 of the survey.
Special attention was given to ensure a distribution of respondents that provides a sufficient sample size to support analyses in the subgroups of the sample. The following table shows the effective sample collected by Leger in the different regions of the country:
| Region | Number of respondents |
|---|---|
| Ontario | 1,127 |
| Quebec | 813 |
| British Columbia and Territories | 382 |
| Alberta | 302 |
| Prairies | 212 |
| Atlantic | 190 |
| Total | 3,026 |
The following table details the distribution of the sample by ethnicity.
| Ethnicity | Number of respondents |
|---|---|
| White | 2,008 |
| Indigenous | 260 |
| Black | 432 |
| South Asian | 89 |
| East Asian | 132 |
| Other / None of the above | 210 |
| Total | 3,026 |
Based on the most recent data from Statistics Canada's national census, Leger weighted the results of this survey by age, gender, region, first language (mother tongue), education level, presence of children in the household, place of birth, and ethnicity. The most recent data regarding age, gender, region and first language was from the 2021 census. The data for education level, presence of children in the household, place of birth and ethnicity came from the 2016 census.
Details regarding the weighting procedures can be found in Appendix A.
As a member of the Canadian Research and Insights Council (CRIC), Leger adheres to the most stringent guidelines for quantitative research and acts in accordance with the Government of Canada requirements for quantitative research and Standards of the Conduct of Government of Canada Public Opinion Research. The details of the methodology and more information on Leger's quality control mechanisms are presented in Appendix A. The questionnaire is available in Appendix E.
1.7 Overview of findings of Wave 18
COVID-19 infection
- Around half of the respondents (50%) either had been (43%) or thought they had been (7%) infected with COVID-19, and a vast majority (89%) knew people in their immediate social network who had been infected.
- One person out of three considered themselves at risk (26%). The proportion was higher among those over 55 years old (58%).
- Around four people out of ten (42%) are either very (12%) or somewhat (30%) worried about becoming infected with COVID-19. On the other hand, a third of people state being a little worried (33%), and one out of four is not worried at all (24%). Those who were not worried mentioned they were vaccinated or that they previously caught COVID-19. While those who were worried were mostly anxious about getting others sick or themselves getting really sick.
Mental health
- Personal financial situation (21%) and the economy (17%) were the top two most pressing concerns, way ahead of physical health (10%) and the health of family/friends (8%).
- Over a third (38%) rated their mental health as average (28%), bad (8%) or very bad (2%). Respondents under the age of 55, parents of children under 18, and those who had been infected with COVID-19 or believed they had been infected were more likely than other respondents to report their mental health as "average".
- One person out of ten (13%) had received mental health support in the month preceding the survey.
COVID-19 vaccine
- A vast majority of respondents were vaccinated at least once (93%): three in ten have received three doses (29%), and around one out of four have either two (22%) or four doses (27%). Over one out of ten received five doses (14%).
- Four out of ten of those who have received at least one COVID-19 dose received it less than three months before data collection (42%), while around one out of four received either 3-6 months prior or six months to a year prior (25% and 27% respectively).
- Seven out of ten (69%) stated it was very (46%) or somewhat (23%) likely that they keep their COVID-19 doses up to date.
- The top three reasons not to get a booster dose included: the belief that the vaccine is not efficient as infection remains possible (16%), concern about the long-term effects of the vaccine (16%) and considering that current protection is enough (15%).
- Around one out of four respondents stated they have been reluctant to get a COVID-19 booster dose (23%), mainly because they were concerned about its safety and/or side effects (57%).
- Three out of four respondents mentioned it was likely they would get a COVID booster at the same time as a flu shot (74%) and if it were offered twice a year (78%).
- Around two out of three were likely to get vaccinated against COVID-19 routinely (64%). The main reason to hesitate about routine COVID-19 vaccines is concern about the long-term effects (20%).
- Over four out of ten respondents were aware of the bivalent vaccine (44%) while almost half (47%) were not. After being presented with brief information, four out of ten were more likely to get a bivalent booster dose (38%).
- Among parents of children aged 12-17, over eight out of ten stated their children were vaccinated with at least one dose: around half were vaccinated with two doses (51%), and one in four had received three doses (26%). A little less than one out of ten had four doses (8%).
- Among parents of children aged 5-11, around two-thirds stated their children were vaccinated with at least one dose (65%): a little less than half were vaccinated with two doses (45%), and around one out of ten had received either one (9%) or three (12%) doses.
- Among parents of children under 18, the top reason for hesitation about vaccinating their children with a booster dose was the concern about long-term effects (31%).
- One out of five people (21%) stated that their children between six months and five years old were vaccinated (21%). One-third stated they would not get their child(ren) vaccinated (35%).
- After reading about the bivalent vaccine, three out of ten parents of children under 18 (29%) stated it was more likely that they would have their child(ren) vaccinated with it.
Routine vaccinations
- Confidence in vaccines was the same as before the pandemic for half the respondents (51%), while one in five stated being more confident (20%), and the same proportion stated being less confident now (24%).
- The top reasons for the decrease in general vaccine confidence included a negative impact of the COVID-19 vaccine on general views (43%) and increased concern about the safety of vaccines at large (41%).
Flu vaccine
- One out of four respondents planned on getting the flu shot (24%), and around the same proportion (27%) has already received it. Regarding those who did not get the flu shot, they mentioned never having gotten one as the main reason (48%).
Public health measures
- Staying home when sick (81%), wearing a mask indoors with others when feeling sick (59%), and using individual public health measures when interacting with someone at-risk (56%) were the three individual public health measures that were practised by at least half of the population. Indoor mask-wearing (46%), ventilation improvement (37%) and outside mask-wearing (25%) were done by less than half of the respondents.
- Over eight out of ten (84%) believed that individual public health measures help reduce the spread of other respiratory infectious diseases. Around half would agree with reinstating mandatory public health measures (51%). The three main reasons to support individual public health measures reinstatement include a rising number of COVID-related hospitalizations (50%), healthcare system overload (46%), and a rising death toll (45%).
- Two people out of three (64%) stated being familiar with the potential long-term effects of COVID-19, and around three out of five (60%) mentioned being very (19%) or somewhat (40%) worried about developing them. Worries about long-COVID were mainly due to uncertainty about future health prospects (68%) and limitations to leisure/personal life (63%).
1.8 Qualitative methodology for Wave 19
Leger conducted a series of eight focus group sessions with French-speaking and English-speaking Canadians. Conducting the groups online offered the opportunity to regroup people from all the regions in Canada. Two focus groups were held with 2SLGBTQIA+ identifying individuals (18-55 years old), two groups were held with racialized populations (18-55 years old), three groups were held with parents and people who are pregnant, and one group was held with young adults (18-34 years old). All groups were interviewed using the same discussion guide, but questions were adapted for the parents' groups in order to gain insights on specific challenged they may face and perceptions they may hold regarding the topics under study. Overall, three focus groups were conducted in French (one of each demographic), and the remaining five were conducted in English.
For each online discussion session, ten participants were recruited by our professional recruiters. A total of 60 recruits participated in the online discussion sessions. All participants in each discussion session received an honorarium of $135. All groups were scheduled to be held on February 7th, 8th, and 9th, 2023. Because the study dealt with topics some participants may have found distressing, the following mental health resources were shared both at the beginning and the end of each focus group through the chat function:
- Mental health support: Get help
- Wellness Together Canada
- Talk Suicide Canada
- The Hope for Wellness Helpline
Groups were held in the following regions on the dates specified in Table below. Further details regarding the qualitative methodology can be found in Appendix A. The screening guide and discussion guide are available in Appendix F and Appendix G.
| GR | Region | Recruits | Participants | Target | Language | Date | Time |
|---|---|---|---|---|---|---|---|
| 1 | BC, Prairies, Ontario | 10 | 8 | 2SLGBTQI+ (18-55 years old) | English | February 7th, 2023 | 5pm |
| 2 | Québec, New-Brunswick | 10 | 6 | 2SLGBTQI+ (18-55 years old) | French | February 7th, 2023 | 5pm |
| 3 | Ontario | 10 | 9 | Racialized populations (18-55 years old) | English | February 7th, 2023 | 7pm |
| 4 | Québec, New-Brunswick | 10 | 7 | Racialized populations (18-55 years old) | French | February 7th, 2023 | 7pm |
| 5 | BC, Prairies | 10 | 8 | Young adults (18-34 years old) | English | February 9th, 2023 | 7pm |
| 6 | Ontario, Atlantic | 10 | 6 | Parents, people who are pregnant | English | February 8th, 2023 | 5pm |
| 7 | BC, Prairies, Territories | 10 | 8 | Parents, people who are pregnant | English | February 8th, 2023 | 7pm |
| 8 | Québec, New-Brunswick | 10 | 8 | Parents, people who are pregnant | French | February 8th, 2023 | 5pm |
| Total | 80 | 60 | |||||
1.9 Overview of findings of Wave 19
Mental health
- Participants noticed a certain decline in mental health state around them during the pandemic. They mentioned the examples of frontline and healthcare workers, the impacts of isolation and lockdowns on mental health, the closing of schools, and return to school's impact on their children, along with negative news coverage and an increase in violent attacks and domestic violence as examples illustrating this decline. However, they acknowledged the pandemic's role in raising awareness around mental health issues.
- Mental health has mostly a neutral connotation to Canadians. Those who view it positively do so because there is less and less stigma surrounding and more open conversations, while those who viewed it negatively did so because of said stigma.
- When participants were asked to define mental health, they defined it as psychological wellness at large, closely relating to day-to-day well-being and ability to perform daily tasks and challenges. Definitions of mental health were vaguer in parents' groups compared to others.
- Signs of poor mental health that have been mentioned include disruption in daily activities because of a lack of motivation, feeling sad, irritated, overwhelmed, having thoughts of self-harm or harming others, and not feeling like oneself.
- Workload, personal finances, negative news coverage, and personal family situations were the main aggravating factors to mental health.
- Lack of accessibility, unaffordability, excessively long waiting times, lack of education and accessible resources were the main barriers to taking care of one's mental health that were mentioned by participants. Social and cultural stigma surrounding mental health, feelings of inadequacy and failure were also elements that prevented some participants from seeking support. These barriers were mainly brought up by racialized participants, but a few men also mentioned social stigma surrounding mental health support.
- Close friends and family were the first lines of support for many participants, along with employee assistance programs offered by workplaces. However, among 2SLGBTQI+ groups, most participants mentioned not being comfortable addressing these issues with their family.
- In terms of signs of when to seek mental health support, the following elements were the most mentioned by participants: when there is a lack of enjoyment of usual activities, when they are having a hard time functioning daily, thoughts of suicide and self-harm.
- Participants mentioned wanting more accessible resources, online and in-person, and more timely support.
- Sleeping and eating well, taking time for oneself, making an effort to socialize, exercising and meditating were the main ways that participants take care of their mental health.
- Most participants admitted only thinking about their mental health when they were not doing well but acknowledged the need to care for it regularly just like physical health. The barriers they mentioned, like lack of time and accessibility, were some of the main reasons.
- Regarding message testing, participants wanted contact information to be included in the statements, and wished the statements were phrased more clearly and included more detailed information about the topics they dealt with.
Vaccines
- While some participants were in favour of the flu vaccine, most expressed serious doubts about its efficiency and had concerns about the potential side effects. Regardless of the opinion, they agreed that vaccination should be personal decision.
- Most participants mentioned the pandemic did not change their views on vaccines at large but confirmed their pre-existing opinions.
- Parents, even when they were vaccinated themselves, specifically had serious concerns about the COVID-19 vaccine's potential side effects on their children, and most of them preferred waiting for more studies before making a decision.
- Mistrust of the COVID-19 and flu vaccines did not bleed into other existing, established vaccines such as tetanus, polio, and measles, that benefit from high levels of confidence.
- Keeping up to date with routine vaccinations varied highly: while parents were up to date and aware of their and their children's vaccines, those who were not parents were much less knowledgeable on the topic and did not keep track.
- Only a few participants expressed concern about the COVID-19 vaccine's impact on their fertility, most had not heard of the link. A few parents were worried about their children's fertility after getting vaccinated.
Public health measures
- Only a couple of participants mentioned having seen the public health measure ads before the focus groups.
- Reactions towards the ads were mixed, both regarding their format and their content. A few participants found them too short and too fast, and some did not enjoy the holiday theme as they preferred for public health authorities to be straightforward with their messaging, rather than tying the topic of the COVID-19 pandemic into a cheerful period (holidays and Christmas).
- While a few participants mentioned these ads could be inefficient because of Canadians' pandemic fatigue, most acknowledged the ongoing need to broadcast such messages for caution.
- Most participants mentioned they kept practicing some public health measures like washing hands, disinfecting and wearing masks or staying home when feeling sick. A few participants mentioned they continued wearing masks in indoor or crowded spaces and wished others did so as well. Improving ventilation was not done by any of the participants.
1.10 Quantitative methodology for Wave 20
The quantitative research was conducted through online surveys using Computer Aided Web Interviewing (CAWI) technology. The online survey was conducted from January 12 to 23, 2023. The participation rate for the survey was 20.14%. Calculation of the Web survey's participation rate is presented in Appendix A. A pre-test of the survey questions was carried out by conducting 47 interviews in both official languages (24 in English, 23 in French). The pre-test was completed on January 12, 2023. Survey interviews lasted 14 minutes on average.
A total of 3,026 respondents participated in the survey, including a general population sample of 2,426 respondents as well as oversamples of 400 Black-identifying individuals and 200 Indigenous-identifying individuals.
Special attention was given to ensure a distribution of respondents that provides a sufficient sample size to support analyses in the subgroups of the sample. The following table shows the effective sample collected by Leger in the different regions of the country:
| Region | Number of respondents |
|---|---|
| Ontario | 1,114 |
| Quebec | 767 |
| British Columbia and Territories | 366 |
| Alberta | 351 |
| Prairies | 231 |
| Atlantic provinces | 197 |
| Total | 3,026 |
The following table details the distribution of the sample by ethnicity.
| Ethnicity | Number of respondents |
|---|---|
| White | 1961 |
| Indigenous | 262 |
| Black | 437 |
| South Asian | 110 |
| East Asian | 135 |
| Other / None of the above | 173 |
| Total | 3,026 |
Based on the most recent data from Statistics Canada's national census, Leger weighted the results of this survey by age, gender, region, first language (mother tongue), education level, presence of children in the household, place of birth, and ethnicity. The most recent data regarding age, gender, region and first language was from the 2021 census. The data for education level, presence of children in the household, place of birth and ethnicity came from the 2016 census.
Details regarding the weighting procedures can be found in Appendix A.
As a member of the Canadian Research and Insights Council (CRIC), Leger adheres to the most stringent guidelines for quantitative research and acts in accordance with the Government of Canada requirements for quantitative research and Standards of the Conduct of Government of Canada Public Opinion Research. The details of the methodology and more information on Leger's quality control mechanisms are presented in Appendix A. The questionnaire is available in Appendix H.
1.11 Overview of findings of Wave 20
COVID-19 infection
- More than half of respondents (54%) had been (47%) or thought they had been (8%) infected with COVID-19.
- Around a third of respondents considered themselves at risk (31%). The proportion was higher among respondents living with a disability (55%) or those over 55 years old (52%).
- Around four people out of ten (37%) are either very (9%) or somewhat (28%) worried about becoming infected with COVID-19. On the other hand, over a third of people state being a little worried (34%), and a quarter is not worried at all (27%).
- Those who were not worried mentioned as a top reason the fact that they are vaccinated so their symptoms would be mild. While those who were worried were mostly anxious about getting other sick or themselves getting really sick.
Mental health
- Personal financial situation (19%) and the economy (14%) were the top two most pressing concerns.
- More than half of respondents (57%) rated their mental health positively: either very good (20%) or good (36%). The remaining respondents rated their mental health status more negatively, ranging from average (30%) to bad (10%) or very bad (2%).
- Top actions taken to maintain a good mental health are to make sleep a priority (52%) or to engage in activities that they enjoy (51%).
- A third of respondents (33%) mentioned that is easy to manage their mental health, while around a quarter of respondents (23%) mentioned that it is difficult to do so. One respondent out of four (41%) think it is neither easy nor difficult to manage mental health challenges.
- When facing a mental health challenge, the top way of taking care of it is to reach out to friends and family, mentioned by one Canadian out of four (44%).
- The factors that influence the services and resources used to manage mental health challenges are mainly the availability (32%), the cost (32%) and the fact that it depends on how serious they feel about the challenge.
- The first step or the first person Canadians would contact to seek help are their primary health care provider (38%) and their family and friends (25%).
- More than half of Canadians know how to access resources and tips for taking care of yourself (61%), in-person support from support workers, social workers, psychologists or other professionals (55%). Less than half of respondents know how to access phone support (44%), online/virtual support from professionals (42%), digital apps or platforms (36%), resources and/or services through your provincial/territorial government (35%), support from a local or non-for-profit organization (34%), resources and/or services through your local government (32%) and resources and services through the Government of Canada (32%).
- Over half of Canadians (54%) are comfortable talking about their mental health needs, while around one out of five Canadians (22%) are uncomfortable doing so.
- More than one person out of ten (15%) had received mental health support in the month preceding the survey.
- The most popular types of support received are in person support from professionals (31%) and online/virtual support from professionals (28%).
- The main reasons for not seeking out mental health support are because they felt like they don't need it (54%), followed by the fact that they prefer to manage the challenge themselves (25%).
- When asked about their level of agreement on certain aspects of mental health, a majority of Canadians agreed that doing something enjoyable contributes to good mental health (90%), that mental health is interconnected with physical health, and central to overall health and well-being (84%), that factors such as resiliency and coping contribute to good mental health (81%), and that perceived control over life contributes to good mental health (71%). Around two thirds of Canadians agreed that they know when they need help with their mental health (66%) and that they have enough time to take care or their mental health (61%).
- More than half of Canadians agreed that they practice taking care of their mental health on a regular basis (59%), that they know how or where to get help for their mental health (57%), that they think they can manage their mental health struggle on their own (56%), that they are aware of free mental health and substance use resources online or by phone (52%), or that spirituality contributes to good mental health (52%). Less than half of Canadians agreed that they feel they have adequate access to mental health support services (47%), that they can afford to see a therapist (41%), that they can afford mental health support (40%) or that it's hard to ask for help if they are struggling with mental health (38%).
- Among Canadians who find it hard asking for mental health support (27%), the main reasons mentioned as a difficulty are that they cannot afford mental health support (25%) or that they are worried about what others would think of them (24%).
- A majority of Canadians (55%) would like to see links to free support services on the Government of Canada Website.
COVID-19 Vaccine
- A vast majority of respondents were vaccinated at least once (91%): either with one dose (1%), 2 doses (25%), 3 doses (26%), 4 doses (25%) or 5 doses (14%).
- Three out of four Canadians (72%) received at least one booster dose, while around a quarter (28%) have not received one.
- A quarter of those who have received at least one COVID-19 booster dose received it less than three months before data collection (27%), while around a third received either 3-6 months prior (34%), a quarter received it six months to a year prior (25%) and one out of ten (13%) received it over a year ago.
- Six out of ten (61%) stated it was very (39%) or somewhat (22%) likely that they keep their COVID-19 doses up to date.
- The top two reasons not to get a booster dose included: the belief that they are protected enough with the number of doses received (18%) or that they are concerned about the long-term effects of the vaccine (15%).
- The main source of motivation to get a booster dose among those who have not gotten one yet is to have more knowledge about the safety of booster doses (14%).
- Around one out of five respondents stated they have been reluctant to get a COVID-19 booster dose (22%), mainly because they were concerned about its safety and/or side effects (59%).
- Despite their initial reluctance, the main reasons mentioned getting the booster dose are because of the high number of COVID-19 cases (32%) and that the benefits are more important than risks (24%).
- Almost six out of ten respondents (58%) mentioned it was likely they would get a COVID-19 vaccine if it was offered as a routine vaccine.
- Among those who are not likely to get a COVID-19 vaccine as a routine vaccine, mentioned not wanting to do so mainly because they are concerned about the long-term effects of the vaccine (16%).
- If it was offered twice a year, three quarters (75%) of Canadians would be likely to get the COVID-19 vaccine.
- Almost half of respondents were aware of the bivalent vaccine (47%) while a similar proportion (44%) were not. After being presented with brief information, three out of ten were more likely to get a bivalent booster dose (28%).
Childhood vaccination
- Among parents of children aged 12-17, over eight out of ten (83%) stated their children were vaccinated with at least one dose: more than half were vaccinated with two doses (52%), and one in five had received three doses (21%). A little less than one out of ten had four doses (8%).
- Around four out of ten parents of children aged 12-17 (38%) are likely to have their children receive a booster dose of COVID-19 vaccine.
- Among parents of children aged 5-11, six out of ten (61%) stated their children were vaccinated with at least one dose: 12% received one dose, 35% received two doses and 14% received three doses.
- More than half of parents of children aged 5-11 (56%) stated being likely to have their children receive a booster dose of COVID-19 vaccine.
- Among parents of children aged 5-17, the top reason for hesitation about vaccinating their children with a booster dose was the concern about long-term effects (26%).
- One out of four parents (23%) stated that their children between six months and five years old were vaccinated. One-third stated they would not get their child(ren) vaccinated (34%).
- The main motivation to get parents of children aged between 6 months to 5 years to vaccinate their children is to have more information on children who have received the COVID-19 vaccine (19%). A quarter of parents (27%) stated that nothing would make them likely to vaccinate their children.
- After reading about the bivalent vaccine, a quarter of parents of children under 18 (25%) stated it was more likely that they would have their child(ren) vaccinated with it.
Confidence in vaccination
- Confidence in vaccines was the same as before the pandemic for half the respondents (51%), while one in five stated being more confident (19%), and the same proportion stated being less confident now (23%).
- The top reasons for the decrease in general vaccine confidence included a negative impact of the COVID-19 vaccine on general views (43%) and increased concern about the safety of vaccines at large (41%).
Public health measures
- Staying home when sick (79%), wearing a mask indoors with others when feeling sick (57%), and using individual public health measures when interacting with someone at-risk (56%) were the three individual public health measures that were practised by at least half of the population. Indoor mask-wearing (44%), ventilation improvement (37%) and outside mask-wearing (24%) were done by less than half of the respondents.
- Over two respondents out of five (44%) agree either strongly (19%) or somewhat (25%) with reinstating mandatory public health measures. One out of five people neither agreed nor disagreed (20%). On the other hand, a third of respondents disagreed either somewhat (11%) or strongly (22%).
- The main condition to reinstate mandatory public health measures would be if there is a rising number of hospitalizations related to COVID-19 (48%).
Long-COVID
- Around two-thirds of respondents mentioned being familiar with long-COVID (63%): around one out of ten stated being very familiar (12%), and around half were somewhat familiar (51%). On the other hand, one out of four was not very familiar (24%), and around 8% were not at all familiar.
- More than half (56%) mentioned being worried about developing long-term symptoms from a COVID-19 infection.
- The main reasons Canadians worry about post COVID-19 condition are the uncertainty about their future health prospects (66%) and limitations to their leisure/personal life (65%).
1.12 Intended use of the research results and benefits for canadians
As defined in the request for proposal documents, the results of this public opinion study will be put to various uses:
Manner in which research supports government or departmental priorities
As part of their mandate to promote and protect Canadians' health as well as respond to public health emergencies, HC and PHAC need to gain a solid understanding of Canadians' level of awareness, knowledge, concerns, behaviours and opinions on specific COVID-19 issues, as well as vaccines more broadly. The research will provide HC and PHAC essential health-specific information to support the ongoing public health response and communications.
Manner in which research findings will benefit Canadians
The research will allow the Government of Canada to develop and refine communications activities to meet the specific needs of Canadians with timely, up-to-date, easily understood information based on the current perceptions of Canadians in the requisite COVID-19 areas and vaccines more broadly.
1.13 Statement of limitations
The quantitative portion of the research is based on a web-survey methodology. Respondents for this survey were selected from among those who have volunteered to participate/registered to participate in online surveys. The results of such surveys cannot be described as statistically projectable to the target population. The data have been weighted to reflect the demographic composition of the target population. Because the sample is based on those who initially self-selected for participation, no estimates of sampling error can be calculated.
The qualitative portion of the research is based on a series of focus groups. Qualitative research is designed to reveal a rich range of participants' opinions, perceptions and interpretations. It does not and can not measure what percentage of the target population holds a given opinion or perception. Findings are qualitative in nature and cannot be used quantitatively to estimate the numeric proportion or number of individuals in the population who hold a particular opinion.
1.14 Notes on interpretation of research findings
The views and observations expressed in this document do not reflect those of Health Canada. This report was compiled by Leger based on the research conducted specifically for this project. This research is not probabilistic; the results cannot be inferred to the general population of Canada.
1.15 Political neutrality statement and contact information
I hereby certify as Senior Officer of Leger that the deliverables fully comply with the Government of Canada's political neutrality requirements outlined in the Policy on Communications and Federal Identity and the Directive on the Management of Communications- Appendix C (Appendix C: Mandatory Procedures for Public Opinion Research).
Specifically, the deliverables do not include information on electoral voting intentions, political party preferences, standings with the electorate, or ratings of the performance of a political party or its leaders.
Signed:
Christian Bourque
Executive Vice-President and Associate
Leger
507 Place d'Armes, bur 700
Montréal, Québec
H2Y 2W8
cbourque@leger360.com
Additional information
Supplier name: Leger
Contract Number: HT372-224613
Contract Award Date: 2022-08-05
The cost of this research was $282,441.24 (HST included).
To obtain more information on this study, please email: hc.cpab.por-rop.dgcap.sc@canada.ca
2. Detailed results for Wave 16
2.1 COVID-19 infection
Respondents were questioned about whether they had ever been infected with COVID-19. More than one out of three (37%) said they had been infected with the virus, while nearly one out of ten (9%) believed they had been infected but had not been properly tested. As a result, nearly half of the respondents (46%) have been or believe they have been infected with COVID-19. The other half of the respondents (50%) responded that they had never been infected.
Figure 16.1: Have you ever been infected with COVID-19?
Sample frame: All respondents (n=3,004)
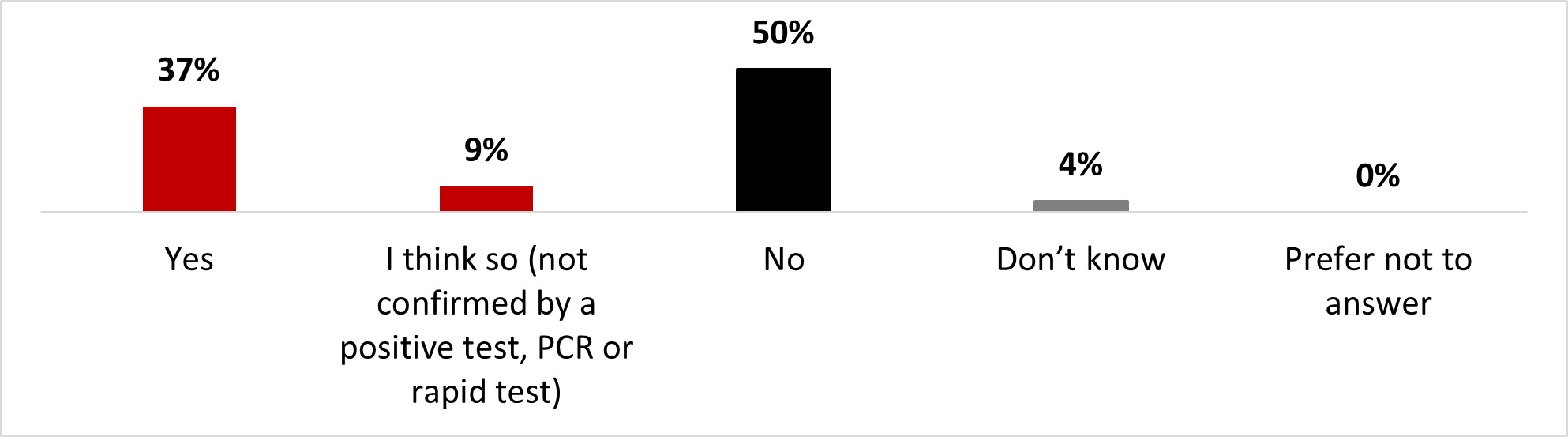
Figure 16.1 - Text description
- Yes
- 37%
- I think so (not confirmed by a positive test, PCR or rapid test)
- 9%
- No
- 50%
- Don't know
- 4%
- Prefer not to answer
- 0%
A significantly higher proportion of the following subgroups of respondents has indicated they had been infected with COVID-19:
- 18 to 34-year-old individuals (45%) and 35 to –54-year-old individuals (42%)
- Parents of children less than 18 (47%)
- Individuals who earn over $80,000 (43%)
Respondents were also questioned about COVID-19 infections in their immediate social network (i.e., family, friends, etc.). A strong majority of respondents (86%) indicated they knew someone in their immediate network who had been infected with COVID-19, and an additional 2% of respondents indicated they believed they knew someone who had been infected without being able to confirm this. One out of ten respondents (11%) were convinced they did not know anyone close to them who had been infected.
Figure 16.2: Do you know people in your immediate social network (i.e., friends or close family members) who have been infected with COVID-19?
Sample frame: All respondents (n=3,004)
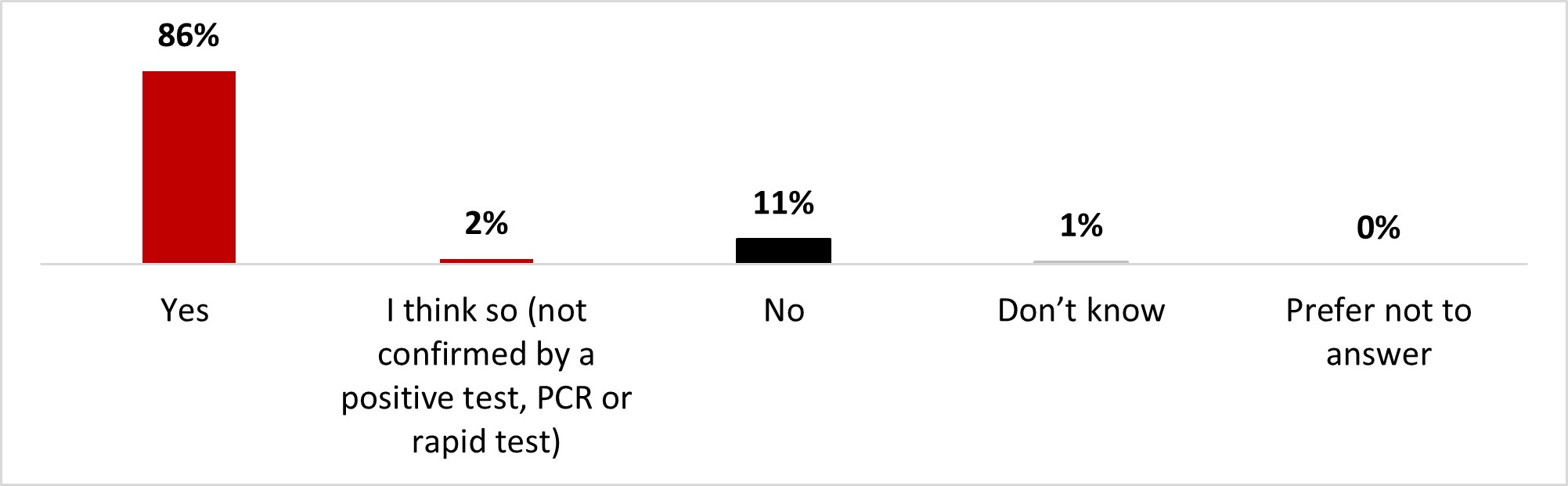
Figure 16.2: Text description
- Yes
- 86%
- I think so (not confirmed by a positive test, PCR or rapid test)
- 2%
- No
- 11%
- Don't know
- 1%
- Prefer not to answer
- 0%
Almost all of those who have been infected knew someone in their immediate network who has also been infected (97%). Other subgroups that were significantly more likely to know people who were infected include:
- Individuals who earn over $80,000 (91%)
- Individuals with a university degree (89%)
- Women (89%)
One-third of respondents (34%) identified themselves as being at risk of complications or severe consequences if they contracted COVID-19 because of their specific medical condition or because of having a chronic disease. More than half of the respondents (56%) reported that they were not at risk, while 10% were unsure.
Figure 16.3: Do you consider yourself to be at risk of more severe disease or outcomes from COVID-19 (e.g., are an older adult over the age of 60, are pregnant, have Down syndrome, have a chronic medical condition, are immunocompromised, or live with obesity, etc.)?
Sample frame: All respondents (n=3,004)
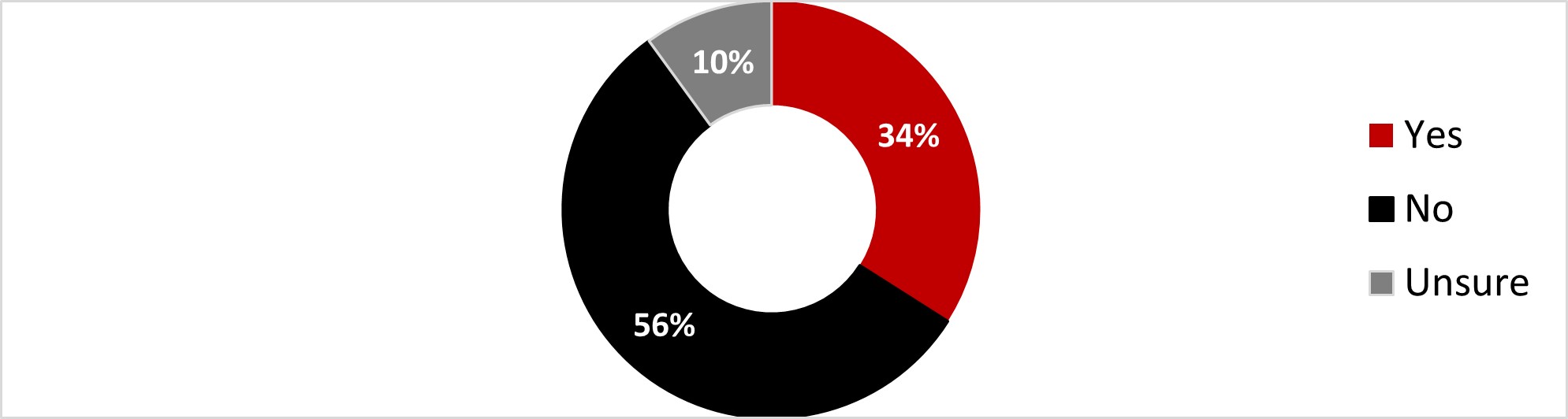
Figure 16.3: Text description
- Yes
- 34%
- No
- 56%
- Unsure
- 10%
The following subgroups were significantly more likely to consider themselves at risk:
- Respondents over 55 years old (56%)
- Respondents who earn less than $40,000 (39%)
- Individuals who are not parents (38%)
- Those who have never gotten COVID-19 (38%)
- Respondents who identify themselves as white (37%)
2.2 Mental health
When asked about their most pressing concerns, a large proportion of respondents mentioned their personal financial situation (22%) and the state of the economy (17%). These two concerns ranked highest, well ahead of the health of their family and friends (9%), their own physical health (9%) and mental health (7%). These were the five concerns that ranked highest, ahead of all other concerns that accounted for 6% or less of mentions among respondents. One respondent out of ten mentioned not having any pressing concerns (11%).
Figure 16.4: What is your most pressing concern at this time?
Sample frame: All respondents (n=3,004)
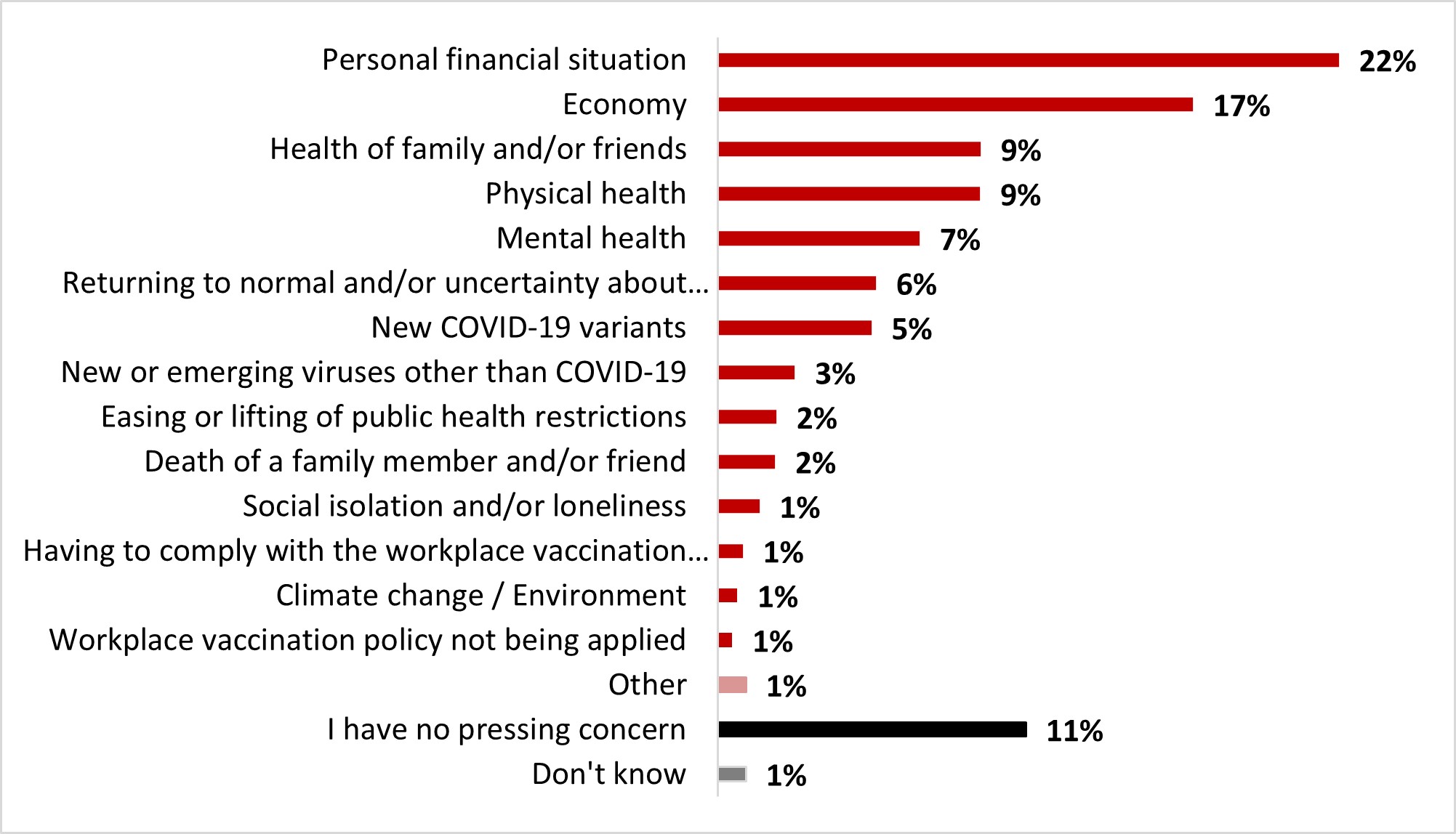
Figure 16.4: Text description
- Don't know
- 1%
- I have no pressing concern
- 11%
- Other
- 1%
- Workplace vaccination policy not being applied
- 1%
- Climate change / Environment
- 1%
- Having to comply with the workplace vaccination policy
- 1%
- Social isolation and/or loneliness
- 1%
- Death of a family member and/or friend
- 2%
- Easing or lifting of public health restrictions
- 2%
- New or emerging viruses other than COVID-19
- 3%
- New COVID-19 variants
- 5%
- Returning to normal and/or uncertainty about the future
- 6%
- Mental health
- 7%
- Physical health
- 9%
- Health of family and/or friends
- 9%
- Economy
- 17%
- Personal financial situation
- 22%
Some subgroups were significantly more likely to mention certain concerns, including:
- Women were significantly more likely to worry about their personal financial situation (24%), the health of family/friends (12%), and mental health (9%). Still they were also more likely to report not having any pressing concerns (12%). On the other hand, men were more likely to be worried about the economy (22%), the return to normal (7%) and new or emerging viruses (4%).
- Respondents between 18 and 34 years old were significantly more likely to worry about their personal situation (28%) and mental health (14%), while those over 55 years old were more likely to worry about health of family and or friends (12%), physical health (12%), the return to normal (7%), and new viruses (4%).
- Respondents from Alberta were significantly more likely to worry about the economy (23%). While those from the province of Quebec were more likely to worry about physical health (12%), they were also more likely to report not having any pressing concerns (14%).
- Respondents who earn less than $40,000 were more likely to worry about their personal financial situation (31%), while those who earn over $80,000 (22%), along with university degree holders (29%) were more likely to worry about the economy.
- Black-identifying individuals were significantly more likely to report being worried about their personal financial situation (33%), while those who identify as white were more likely to report being worried about their physical health (10%) and to report not having any pressing concerns (11%).
- Parents of children less than 18 were significantly more likely to be worried about their personal financial situation (28%), while those who are not parents of children less than 18 were more likely to be worried about their own physical health (10%) and to report not having any pressing concerns (12%).
Just under two-thirds of respondents (63%) rated their mental health positively: either really good (22%) or good (42%). The remaining respondents rated their mental health status more negatively, ranging from average (27%) to bad (8%) or really bad (2%).
Figure 16.5: How would you rate your overall mental health?
Sample frame: All respondents (n=3,004)
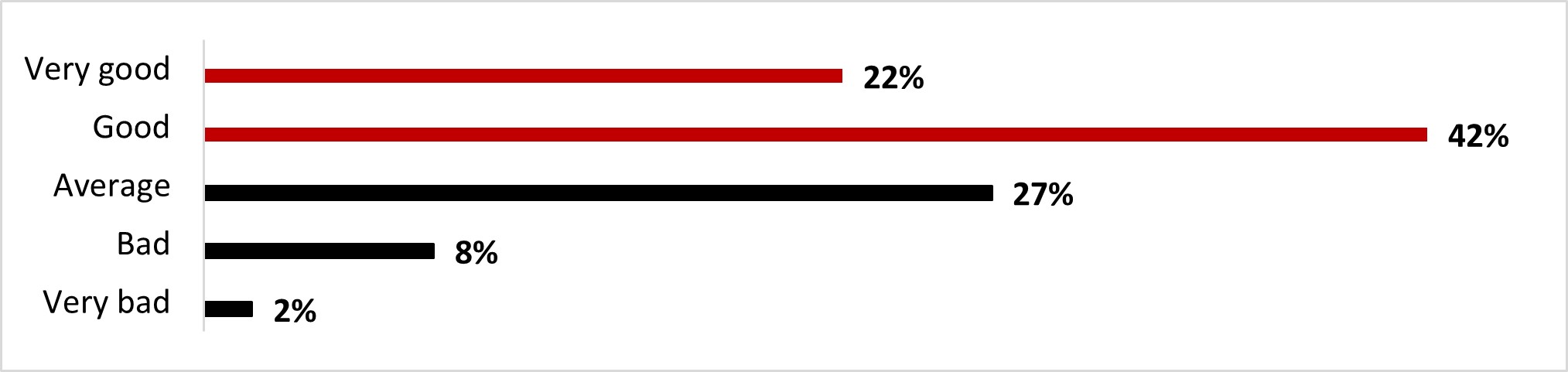
Figure 16.5: Text description
- Very bad
- 2%
- Bad
- 8%
- Average
- 27%
- Good
- 42%
- Very good
- 22%
Significant differences in terms of mental health include:
- Male respondents were significantly more likely to rate their mental health as very good (25%) compared to women (18%).
- Young respondents (18 to 34 year-olds) were significantly more likely to rate their mental health as average (36%) or bad (14%), while older respondents (over 55 years old) were more likely to rate it as very good (32%) or good (45%). Those aged between 35 and 54 were more likely to rate their mental health average (31%).
- Respondents in Ontario were more likely to rate their mental health as average (29%) and bad (10%), while those from Quebec were more likely to rate it as very good (30%) or good (49%).
- White-identifying individuals were more likely to rate their mental health as very good (23%), while Indigenous-identifying individuals were more likely to rate it as bad (15%).
- Parents of children less than 18 were more likely to rate it as average (33%), while non-parents were more likely to rate it as very good (24%).
Almost half of the respondents (47%) felt they have adequate access to mental health support services. One out of four (26%) respondents indicated that they neither agreed nor disagreed that access to mental health support services is adequate. Fewer than one out of five respondents (18%) disagreed with this statement.
Figure 16.6: Please indicate your level of agreement with the following statement: I feel I have adequate access to mental health support services.
Sample frame: All respondents (n=3,004)
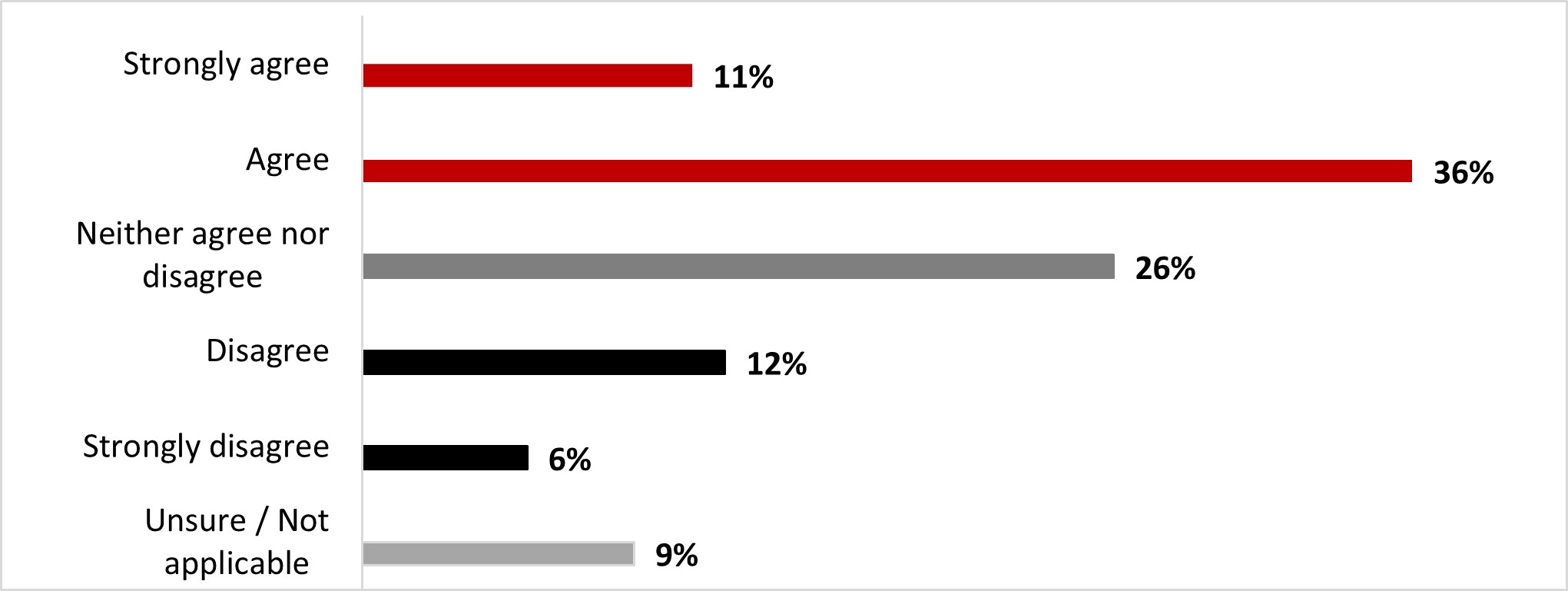
Figure 16.6: Text description
- Unsure / Not applicable
- 9%
- Strongly disagree
- 6%
- Disagree
- 12%
- Neither agree nor disagree
- 26%
- Agree
- 36%
- Strongly agree
- 11%
The following subgroups were significantly more likely to strongly agree or agree with the statement:
- Men (51%) compared to women (43%)
- Respondents from Alberta (62%)
- Respondents who earn over $80,000 (53%)
- Parents of children less than 18 (53%)
A strong majority of respondents (88%) indicated that they had not received mental health support in the month prior to the survey. In contrast, one out of ten respondents (11%) indicated that they had received some support in this regard.
Figure 16.7: In the past month, have you received any support for your mental health?
Sample frame: All respondents (n=3,004)
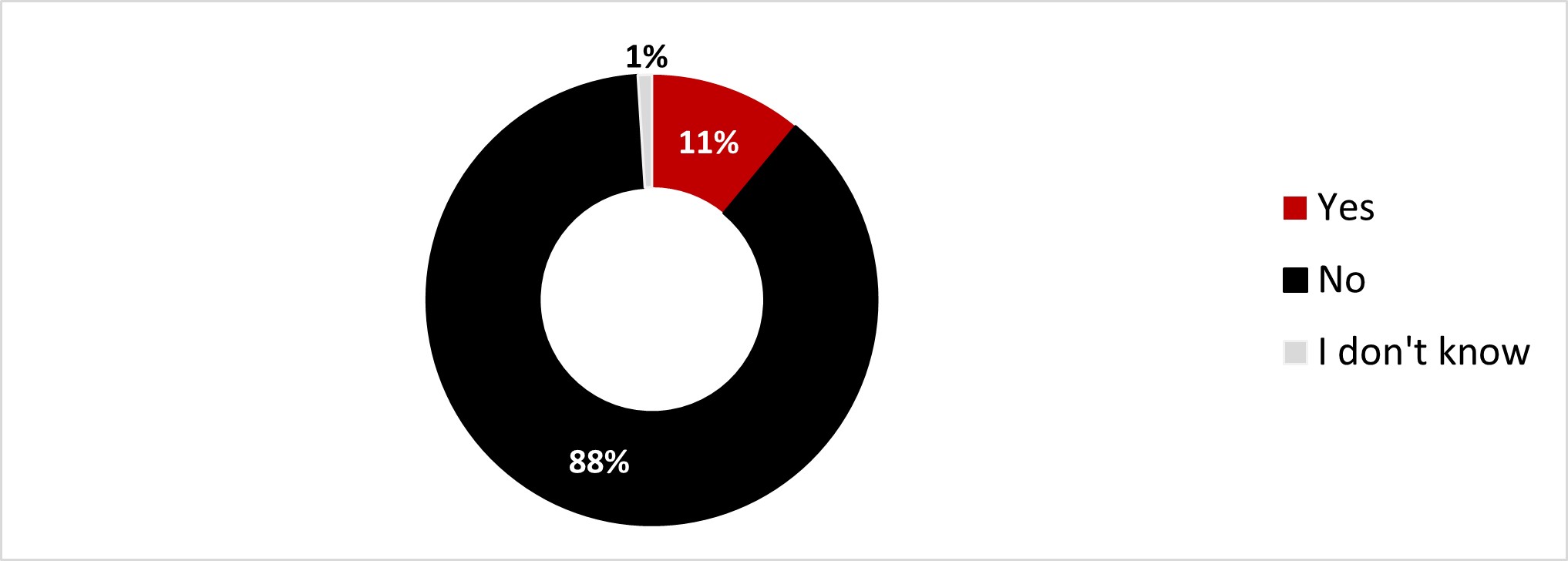
Figure 16.7: Text description
- Yes
- 11%
- No
- 88%
- I don't know
- 1%
The following subgroups were significantly more likely to have received support for coping with mental health:
- 18 to 34 year-olds (19%)
- Respondents who identify as Indigenous (18%)
- Parents of children less than 18 (15%)
Of those who had received support during the previous month, most reported having received in-person support from social workers, psychologists or other professionals (42%), virtual support from social workers, psychologists or other professionals (35%), or support from their primary health care provider (25%). Resources and tips for self-care (18%) and telephone (or SMS) support (17%) rounded out the top five types of support received.
Figure 16.8: What type of support have you received? Select all that apply.
Sample frame: Those who received support for their mental health in the past month (n=353)
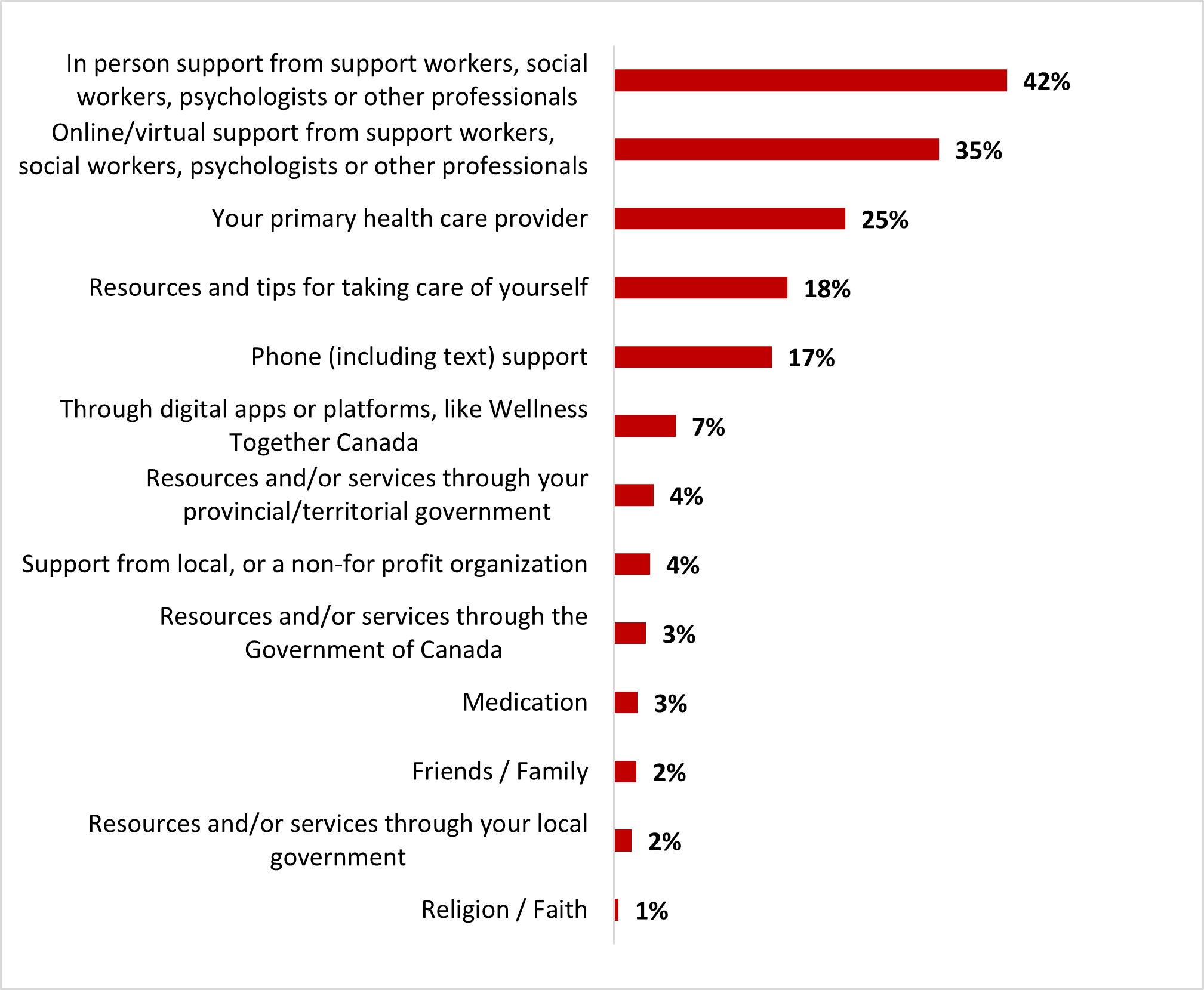
Figure 16.8: Text description
- Religion / Faith
- 1%
- Resources and/or services through your local government
- 2%
- Friends / Family
- 2%
- Medication
- 3%
- Resources and/or services through the Government of Canada
- 3%
- Support from local, or a non-for profit organization
- 4%
- Resources and/or services through your provincial/territorial government
- 4%
- Through digital apps or platforms, like Wellness Together Canada
- 7%
- Phone (including text) support
- 17%
- Resources and tips for taking care of yourself
- 18%
- Your primary health care provider
- 25%
- Online/virtual support from support workers, social workers, psychologists or other professionals
- 35%
- In person support from support workers, social workers, psychologists or other professionals
- 42%
Significant differences in terms of mental health support services include:
- 18-to -34-year-old individuals were significantly more likely to turn to resources and tips for taking care of themselves (29%) and resources through their provincial/territorial government (8%), while those between 35 and 54 years old were more likely to turn to phone support (26%).
- Parents of children less than 18 were significantly more likely to turn to digital apps or platforms (12%) and resources/services through the Government of Canada (8%).
Of those who had not received support for their mental health during the previous month, almost half (47%) reported that they did not need support and one out of five (18%) stated that they feel like their day-to-day physical and mindful activities are enough to support their mental health. Other reasons were mentioned to a lesser extent.
Figure 16.9: Why have you not received any support for your mental health?
Sample frame: Those who have not received support for their mental health in the past month (n=2,624)
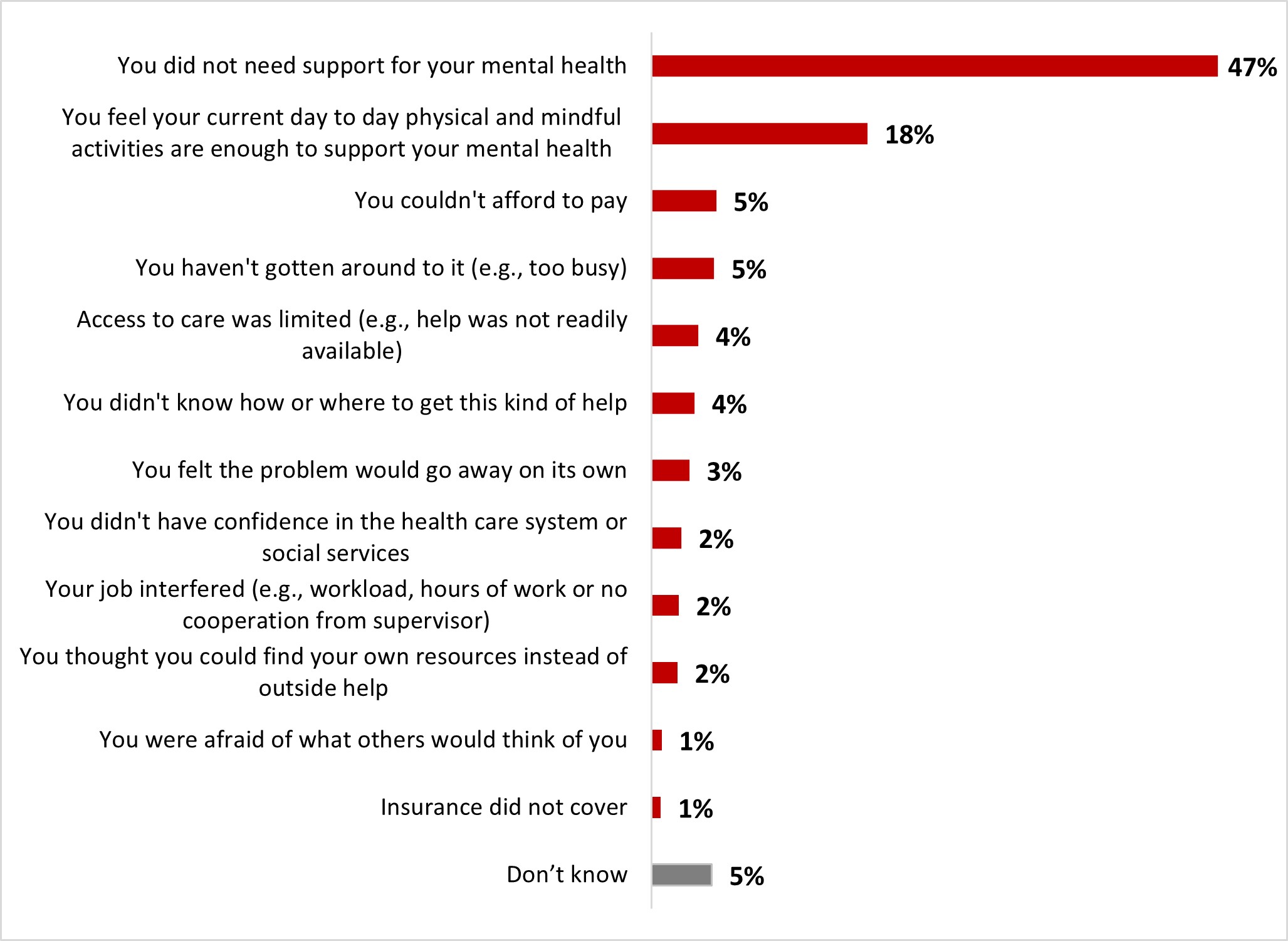
Figure 16.9: Text description
- Don't know
- 5%
- Insurance did not cover
- 1%
- You were afraid of what others would think of you
- 1%
- You thought you could find your own resources instead of outside help
- 2%
- Your job interfered (e.g., workload, hours of work or no cooperation from supervisor)
- 2%
- You didn't have confidence in the health care system or social services
- 2%
- You felt the problem would go away on its own
- 3%
- You didn't know how or where to get this kind of help
- 4%
- Access to care was limited (e.g., help was not readily available)
- 4%
- You haven't gotten around to it (e.g., too busy)
- 5%
- You couldn't afford to pay
- 5%
- You feel your current day to day physical and mindful activities are enough to support your mental health
- 18%
- You did not need support for your mental health
- 47%
Significant differences in terms of reasons not to seek mental health support services include:
- 18 to 34-year-old respondents were significantly more likely to mention not having gotten around to it (12%), not being able to afford it (10%), limited access to care (6%) and not knowing where to get help (6%).
- Those over 55 years old (61%), those living in British Columbia and the Territories (55%), in Quebec (52%) and the Atlantic regions (56%), those with a college degree (50%), those who identify as white (49%) and those who are not parents of children under 18 (50%) were significantly more likely to report not needing mental health support.
Being in a place that is crowded (32%) was mentioned by one out of three respondents as their main concern for returning to normal life after COVID-19. This was followed by concern that COVID-19 will never really end (30%), fear of a new pandemic (20%), being unsure if people around are vaccinated (15%) and having to interact and socialize with people (14%). These were the most common concerns of respondents. It is noteworthy that about one out of five respondents (22%) indicated that they were generally not afraid of COVID-19 and that some other respondents were not concerned about returning to normal life (19%).
Figure 16.10: When thinking about life after COVID-19, what makes you feel worried? Select all that apply.
Sample frame: All respondents (n=3,004)
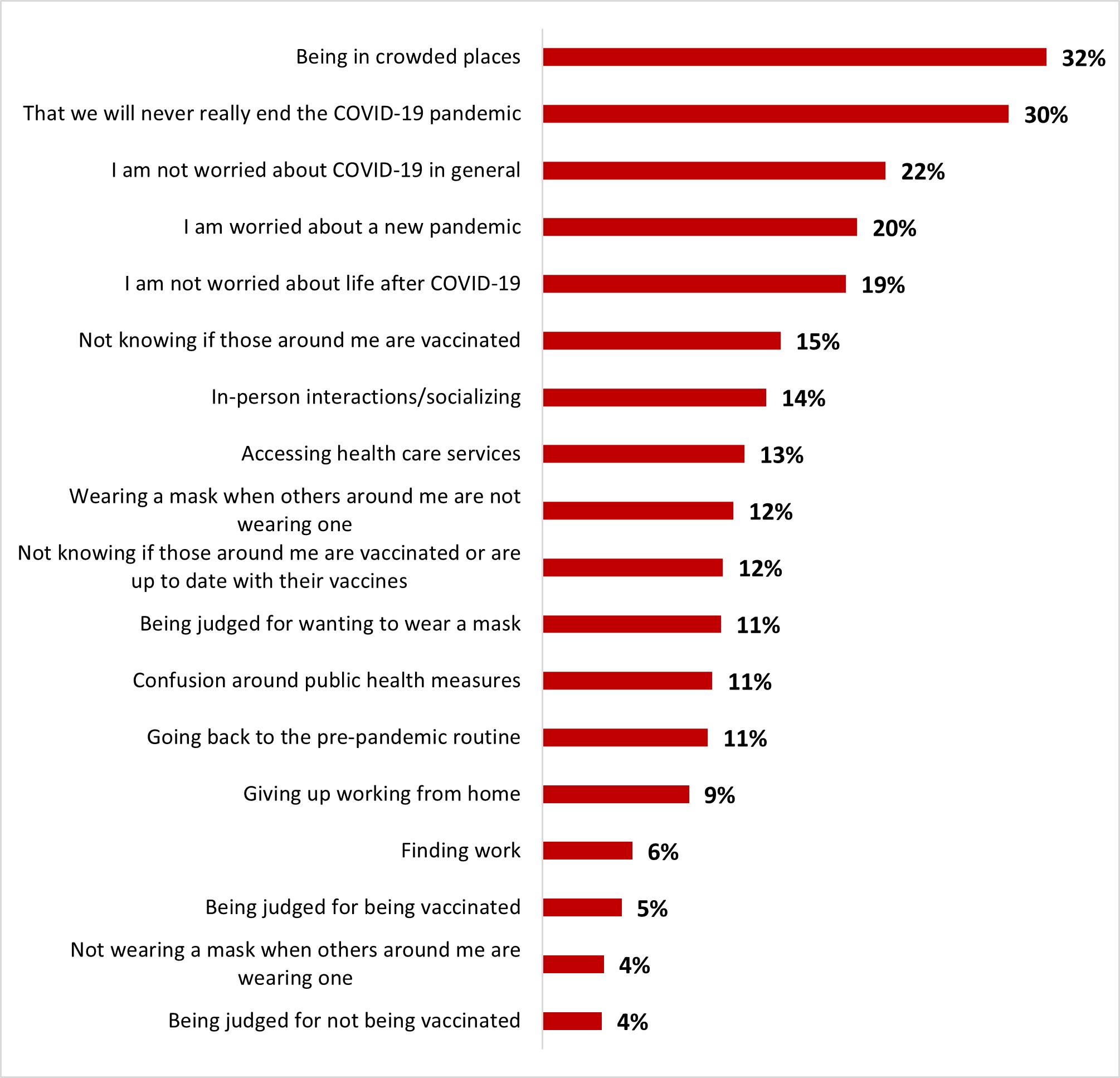
Figure 16.10: Text description
- Being judged for not being vaccinated
- 4%
- Not wearing a mask when others around me are wearing one
- 4%
- Being judged for being vaccinated
- 5%
- Finding work
- 6%
- Giving up working from home
- 9%
- Going back to the pre-pandemic routine
- 11%
- Confusion around public health measures
- 11%
- Being judged for wanting to wear a mask
- 11%
- Not knowing if those around me are vaccinated or are up to date with their vaccines
- 12%
- Wearing a mask when others around me are not wearing one
- 12%
- Accessing health care services
- 13%
- In-person interactions/socializing
- 14%
- Not knowing if those around me are vaccinated
- 15%
- I am not worried about life after COVID-19
- 19%
- I am worried about a new pandemic
- 20%
- I am not worried about COVID-19 in general
- 22%
- That we will never really end the COVID-19 pandemic
- 30%
- Being in crowded places
- 32%
Women and those over 55 years old were significantly more likely to be concerned about being in a crowded place (35% and 36%, respectively) and that the pandemic will never end (33% and 34%).
Those aged 18 to –34-years-old were significantly more likely to worry about giving up work from home (17%), being judged for wanting to wear a mask (14%), going back to pre-pandemic routine (13%) and finding work (11%).
Respondents from Ontario were more likely to be concerned about the social aspects of life after COVID-19: crowded places (39%), in-person interactions and not knowing if those around are vaccinated (18%). They were also more worried about wearing a mask when others aren't (15%), going back to the pre-pandemic routine (14%), confusion around public health measures (13%), and giving up work from home (11%).
2.3 Vaccine
With regard to knowledge about COVID-19, the strong majority of respondents indicated that they agreed (strongly agree and somewhat agree) with the following statements: it is possible to have COVID-19 even if vaccinated (96%), and it is possible to have COVID-19 on several occasions (92%). Eight out of ten respondents also agreed that a person would be less likely to become seriously ill if they are infected with COVID-19 after being vaccinated (80%). About three out of four respondents agreed that staying up to date with their vaccination includes booster doses (76%), while a smaller proportion of respondents (73%) said they consider it important to stay up to date with their vaccination. Slightly more than half of the respondents (58%) agreed that protection from vaccination was more durable and effective than immunity from infection. Less than half of respondents (49%) agreed that immunity from infection was short-lived and not as effective.
Figure 16.11: To what extent do you agree with the following statements?
Sample frame: All respondents (n=3,004)
| Strongly agree | Somewhat agree | Somewhat disagree | Strongly disagree | Don't know | |
|---|---|---|---|---|---|
| You can get COVID-19 even if vaccinated | 76% | 19% | 2% | 0% | 2% |
| You can catch COVID-19 multiple times | 64% | 28% | 2% | 1% | 5% |
| You are less likely to get seriously ill from COVID-19 if you are vaccinated (e.g. not be hospitalized) | 49% | 31% | 7% | 8% | 4% |
| Staying up to date with COVID-19 vaccinations includes boosters | 52% | 25% | 8% | 10% | 6% |
| It is important to stay up to date with COVID-19 vaccinations | 47% | 26% | 9% | 12% | 6% |
| Protection against COVID-19 is longer with vaccination and is more effective than immunity from infection | 30% | 29% | 10% | 10% | 21% |
| The immunity provided by a COVID-19 infection is short-lived and not as effective | 18% | 32% | 18% | 10% | 22% |
Reading note: Significantly lower differences are marked with a "-" sign, while significantly higher differences are marked with a "+".
| Age | Ethnicity | Parents of children under 18 | ||||||
|---|---|---|---|---|---|---|---|---|
| 18-34 | 35-54 | 55+ | White | Indigenous | Black | Yes | No | |
| You can get COVID-19 even if vaccinated | 93% - | 97% | 97% + | 97% + | 98% | 92% - | 96% | 96% |
| You can catch COVID-19 multiple times | 91% | 91% | 93% | 93% + | 90% | 87% - | 91% | 92% |
| You are less likely to get seriously ill from COVID-19 if you are vaccinated (e.g. not be hospitalized) | 79% | 74% - | 86% + | 80% | 74% | 71% - | 74% - | 83% + |
| Staying up to date with COVID-19 vaccinations includes boosters | 69% - | 71% - | 85% + | 76% | 76% | 65% - | 70% - | 79% + |
| It is important to stay up to date with COVID-19 vaccinations | 67% - | 66% | 83% + | 73% | 71% | 61% - | 64% - | 77% + |
| Protection against COVID-19 is longer with vaccination and is more effective than immunity from infection | 60% | 50% - | 63% + | 57% - | 60% | 51% - | 54% - | 60% + |
| The immunity provided by a COVID-19 infection is short-lived and not as effective | 49% | 48% | 51% | 49% | 48% | 46% | 49% | 50% |
| British Columbia + Territories | Alberta | Manitoba / Saskatchewan | Ontario | Quebec | Atlantic | |
|---|---|---|---|---|---|---|
| You can get COVID-19 even if vaccinated | 96% | 96% | 96% | 95% | 96% | 98% |
| You can catch COVID-19 multiple times | 97% + | 90% | 90% | 92% | 90% | 92% |
| You are less likely to get seriously ill from COVID-19 if you are vaccinated (e.g. not be hospitalized) | 85% + | 77% | 76% | 80% | 80% | 80% |
| Staying up to date with COVID-19 vaccinations includes boosters | 83% + | 75% | 72% | 73% - | 78% | 78% |
| It is important to stay up to date with COVID-19 vaccinations | 82% + | 70% | 67% | 73% | 71% | 77% |
| Protection against COVID-19 is longer with vaccination and is more effective than immunity from infection | 67% + | 59% | 62% | 59% | 52% - | 52% |
| The immunity provided by a COVID-19 infection is short-lived and not as effective | 53% | 47% | 50% | 51% | 47% | 42% |
A high proportion of respondents (92%) reported having received at least one dose of the COVID-19 vaccine. Very few respondents reported receiving only one dose (1%) or five doses (1%). Most indicated that they had received two doses (23%), three doses (41%), or four doses (26%). Fewer than one out of ten respondents (7%) mentioned not receiving any doses against COVID-19.
Figure 16.14: How many doses of the COVID-19 vaccine have you received?
Sample frame: All respondents (n=3,004)
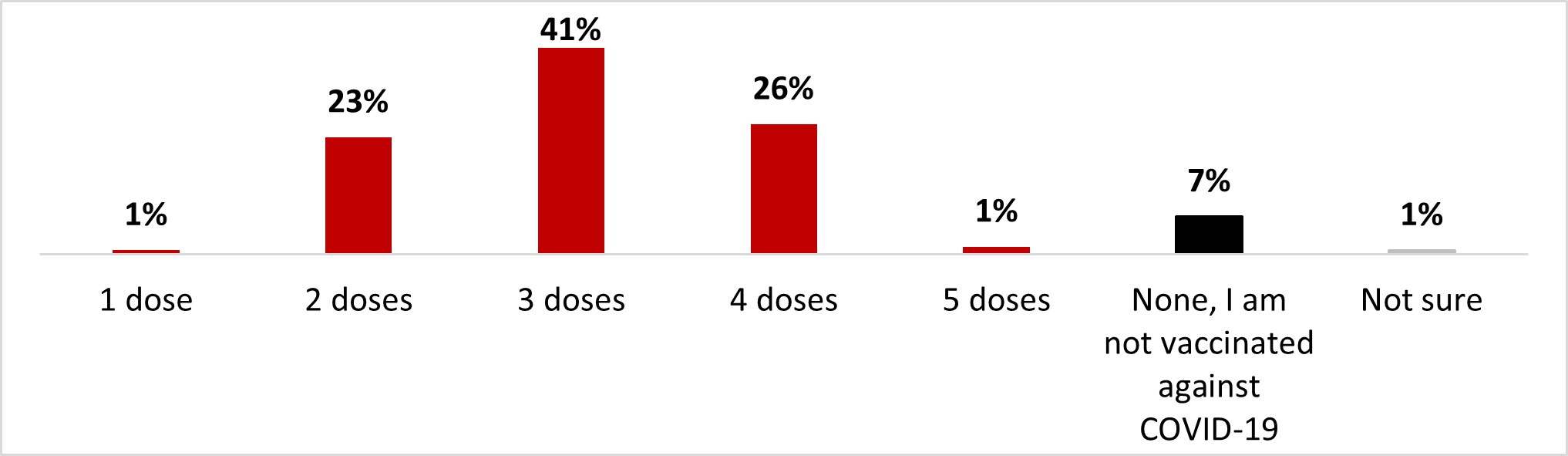
Figure 16.14: Text description
- 1 dose
- 1%
- 2 doses
- 23%
- 3 doses
- 41%
- 4 doses
- 26%
- 5 doses
- 1%
- None, I am not vaccinated against COVID-19
- 7%
- Not sure
- 1%
The following subgroups were significantly more vaccinated than their complement:
- Those over 55 years old (3.5 doses on average)
- Quebec respondents (3.2 doses)
- White-identifying individuals (3.1)
- Those who are not parents of children less than 18 (3.2)
The following subgroups were significantly less vaccinated than their complement:
- 18 to 34 year olds (2.7 doses on average)
- 35 to 54 year olds (2.8 doses)
- Albertans (2.9)
- Black-identifying individuals (2.7)
- Parents of children less than 18 (2.7)
Of those who said they had received at least one dose of COVID-19 vaccine (or were unsure), we asked if they had had any booster doses. Three out of four respondents (74%) reported receiving at least one booster dose of COVID-19. More than a third (37%) reported that they had received one booster dose, more than one out of four (27%) reported that they had had two booster doses, and one out of ten (10%) reported that they had received three booster doses. One out of four (26%) stated they did not receive a booster dose.
Figure 16.15: Have you received a COVID-19 booster dose?
Sample frame: Respondents who have received at least one dose or who are unsure about it (n=2,783)
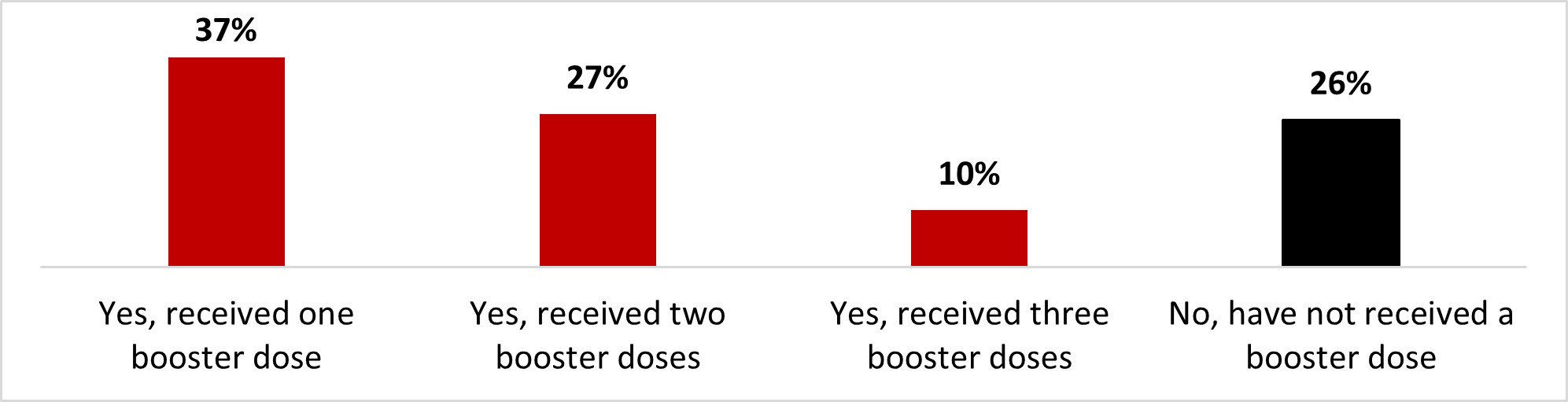
Figure 16.15: Text description
- Yes, received one booster dose
- 37%
- Yes, received two booster doses
- 27%
- Yes, received three booster doses
- 10%
- No, have not received a booster dose
- 26%
The following subgroups were significantly more likely to have received at least one booster dose:
- Those over 55 years old (85%)
- Those living in British Columbia and the Territories (81%)
- Those who earn over $80,000 (77%)
- Those with a university degree (79%)
- White-identifying individuals (76%)
- Those who are not parents of children under 18 (78%)
The following subgroups were significantly more likely not to have received a booster dose:
- 18 to 34 (34%) and 35 to -54-year-old (32%) individuals
- Albertans (36%)
- Those who earn less than $40,000 (32%)
- Black-identifying individuals (47%)
- Parents of children less than 18 (35%)
Among those who had received at least one dose of vaccine, more than seven out of ten respondents (71%) reported that they were likely to keep up with their booster doses: 48% very likely and 23% somewhat likely. In contrast, about one out of four respondents (23%) said they were unlikely to do so: 11% not very likely and 12% not at all likely.
Figure 16.16: How likely are you to get a booster dose of the COVID-19 vaccine?
Sample frame: Respondents who have received at least one dose (n=2,760)
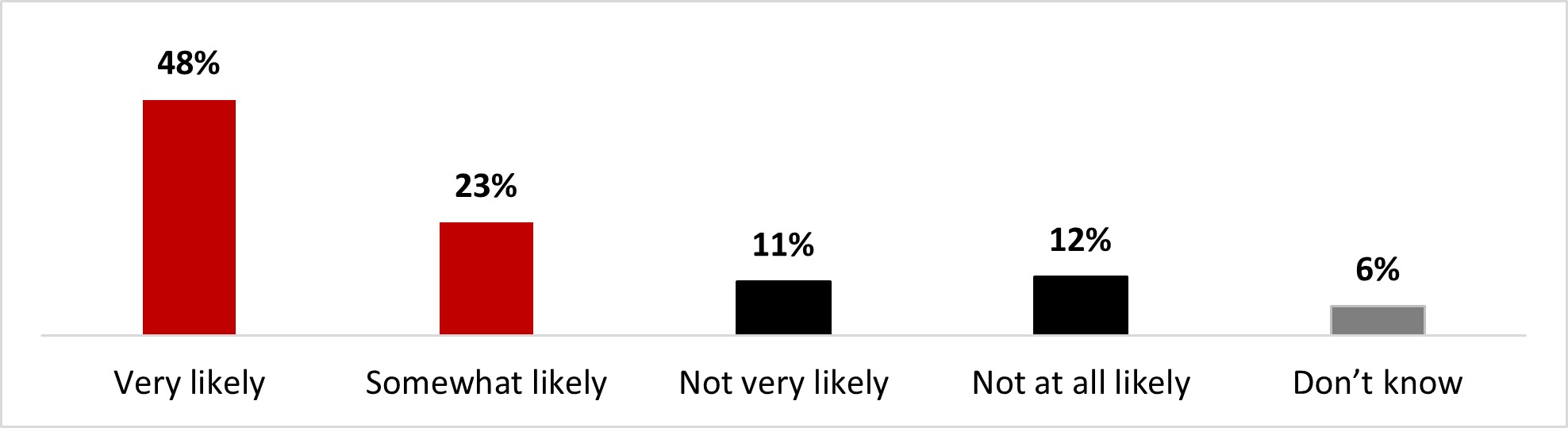
Figure 16.16: Text description
- Very likely
- 48%
- Somewhat likely
- 23%
- Not very likely
- 11%
- Not at all likely
- 12%
- Don't know
- 6%
The following subgroups were significantly more likely to state it's likely (very or somewhat) that they keep their COVID-19 doses up to date:
- Respondents over 55 years old (82%)
- Respondents from British Columbia and Territories (80%)
- University degree holders (76%)
- Individuals who are not parents of children less than 18 (73%)
Respondents who did not receive booster doses or were unsure about it indicated that they felt they were sufficiently protected with the number of vaccines they had received (22%), that the vaccines did not provide sufficient protection because it is possible to get infected with COVID-19 even if you are vaccinated (17%), that they were worried about the potential long-term effects of the vaccine (16%), and that they were fed up with being vaccinated (12%) as the main reasons for being hesitant to receive booster doses. Other reasons were mentioned by less than 10% of respondents.
Figure 16.17: What is the top reason you are unlikely or uncertain about getting a booster dose?
Sample frame: Those who have not received a booster dose or are unsure about it (n=860)
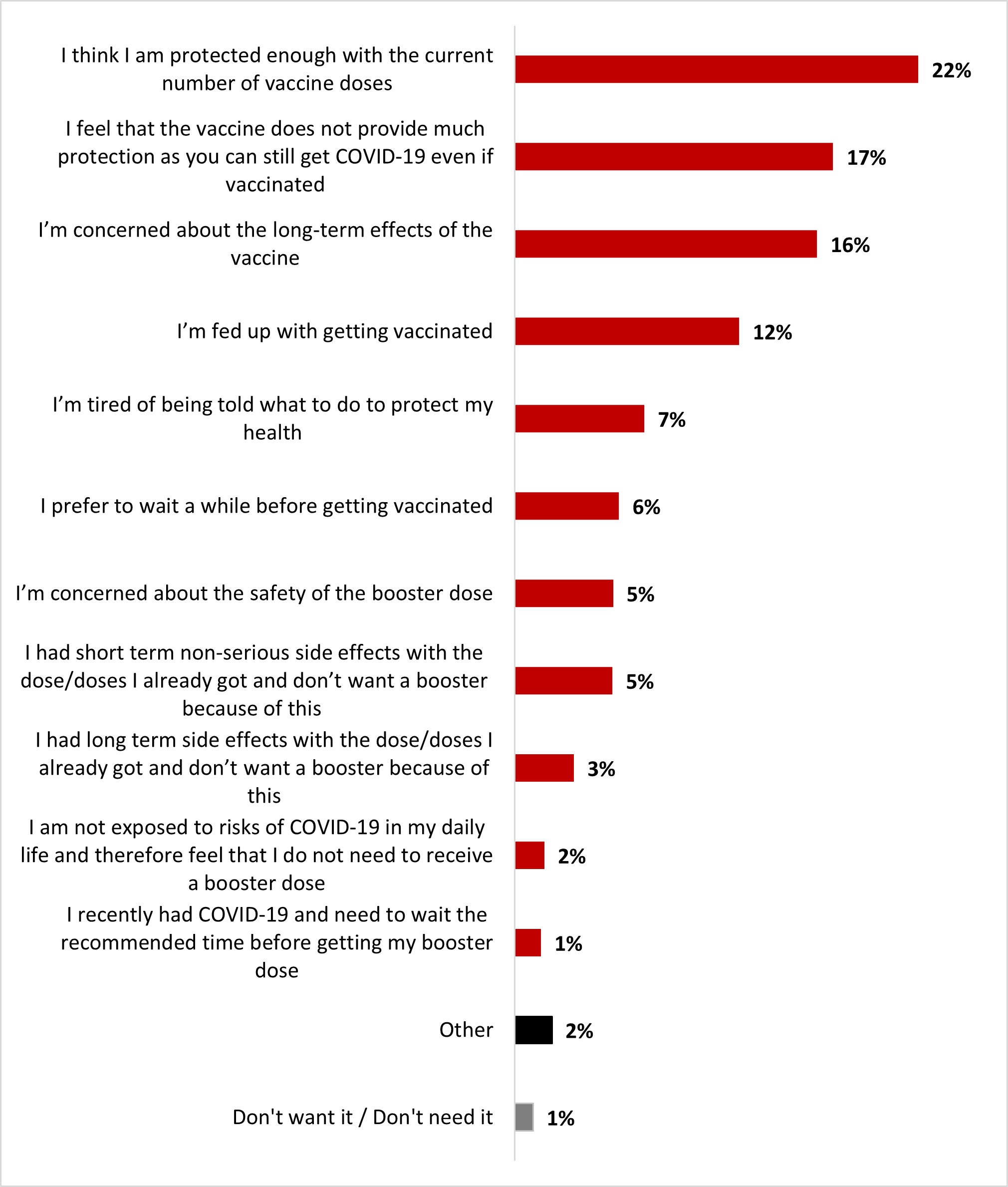
Figure 16.17: Text description
- Don't want it / Don't need it
- 1%
- Other
- 2%
- I recently had COVID-19 and need to wait the recommended time before getting my booster dose
- 1%
- I am not exposed to risks of COVID-19 in my daily life and therefore feel that I do not need to receive a booster dose
- 2%
- I had long term side effects with the dose/doses I already got and don't want a booster because of this
- 3%
- I had short term non-serious side effects with the dose/doses I already got and don't want a booster because of this
- 5%
- I'm concerned about the safety of the booster dose
- 5%
- I prefer to wait a while before getting vaccinated
- 6%
- I'm tired of being told what to do to protect my health
- 7%
- I'm fed up with getting vaccinated
- 12%
- I'm concerned about the long-term effects of the vaccine
- 16%
- I feel that the vaccine does not provide much protection as you can still get COVID-19 even if vaccinated
- 17%
- I think I am protected enough with the current number of vaccine doses
- 22%
Respondents of 18 to 34 years of age (27%) were more likely to feel like they are protected enough with the number of vaccine doses they had. Women (20%), those over 55 years old (23%), and those living in British Columbia and the Territories (33%) were significantly more likely to feel concerned about the long-term effects of the vaccine.
Respondents who had not had booster doses indicated that if it was required for travel outside the country (15%) if it was mandatory for Canadians (13%), and if the new vaccines covered the most recent variants (11%), these would be motivating factors for getting booster doses.
Figure 16.18: Amongst the following factors and thinking about the current COVID-19 context, what would motivate you to get your booster dose?
Sample frame: Respondents who have not gotten a booster dose (n=753)
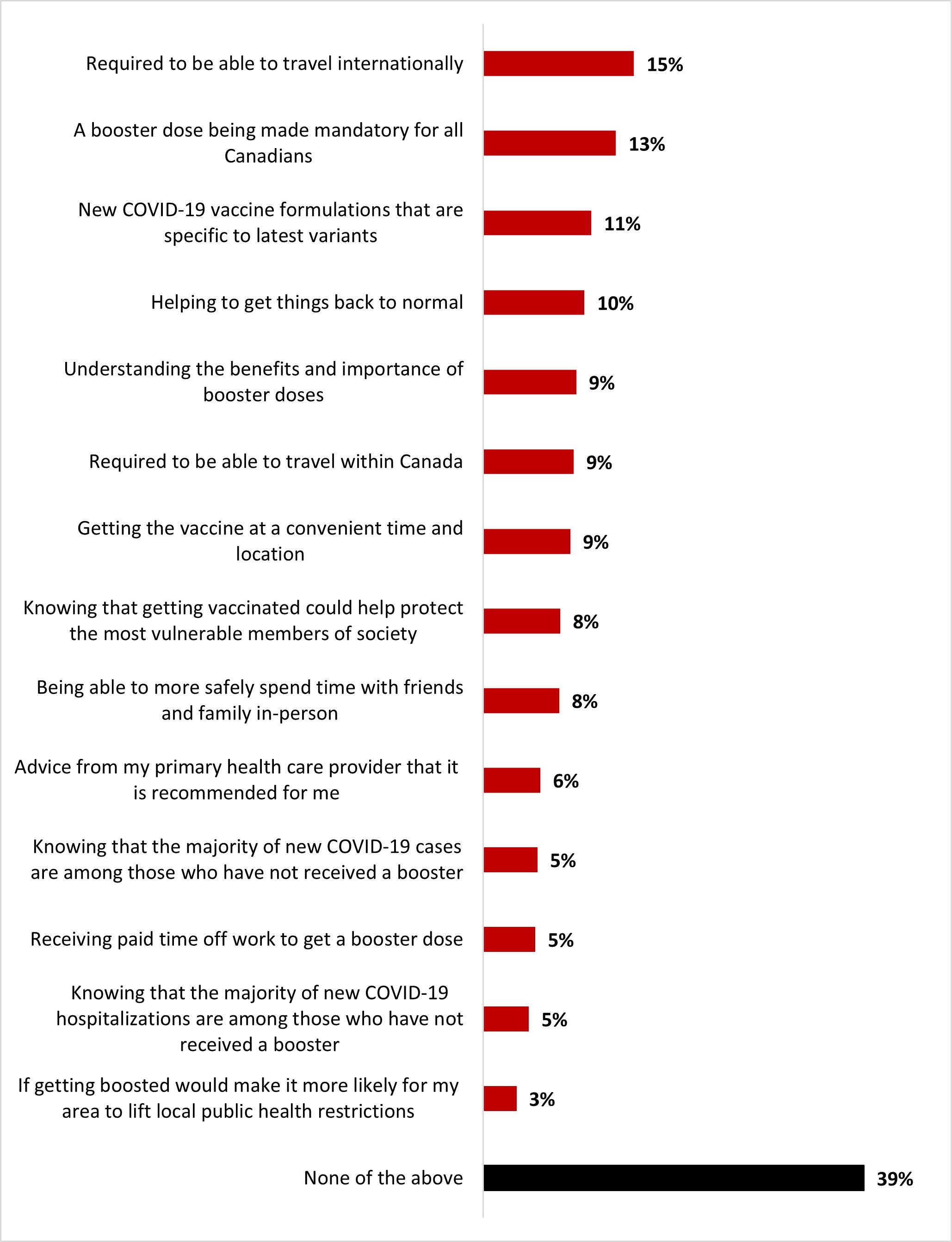
Figure 16.18: Text description
- None of the above
- 39%
- If getting boosted would make it more likely for my area to lift local public health restrictions
- 3%
- Knowing that the majority of new COVID-19 hospitalizations are among those who have not received a booster
- 5%
- Receiving paid time off work to get a booster dose
- 5%
- Knowing that the majority of new COVID-19 cases are among those who have not received a booster
- 5%
- Advice from my primary health care provider that it is recommended for me
- 6%
- Being able to more safely spend time with friends and family in-person
- 8%
- Knowing that getting vaccinated could help protect the most vulnerable members of society
- 8%
- Getting the vaccine at a convenient time and location
- 9%
- Required to be able to travel within Canada
- 9%
- Understanding the benefits and importance of booster doses
- 9%
- Helping to get things back to normal
- 10%
- New COVID-19 vaccine formulations that are specific to latest variants
- 11%
- A booster dose being made mandatory for all Canadians
- 13%
- Required to be able to travel internationally
- 15%
Residents of Manitoba and Saskatchewan (33%) were significantly more likely to mention new COVID-19 vaccine formulations specific to the latest variants as an incentive to get boosted.
Among respondents likely to pick up booster dose(s), nearly eight out of ten (79%) indicated that it was likely they would get their dose at the same time as the flu shot: 50% very likely and 29% somewhat likely. In contrast, just over one out of ten respondents (12%) said it was unlikely: 9% unlikely and 3% not at all likely. Less than one out of ten (7%) said they would not take a flu shot.
Figure 16.19: If recommended, how likely would you be to get a COVID vaccine at the same time as a flu shot?
Sample frame: Those who are likely to get a booster dose or another booster dose (n=1,893)
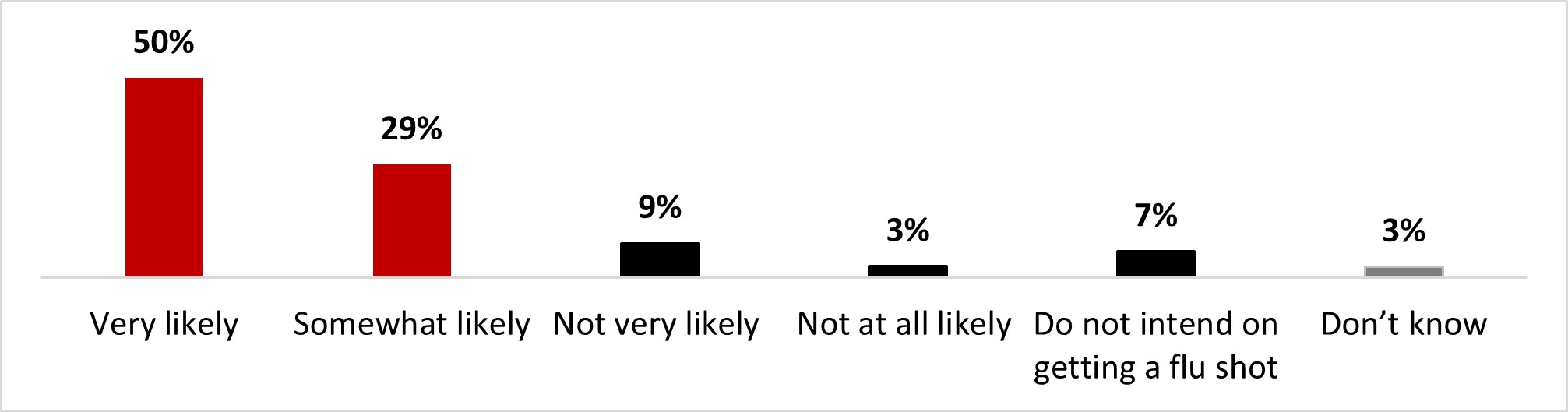
Figure 16.19: Text description
- Very likely
- 50%
- Somewhat likely
- 29%
- Not very likely
- 9%
- Not at all likely
- 3%
- Do not intend on getting a flu shot
- 7%
- Don't know
- 3%
The following subgroups were significantly more likely to state that it's likely (very or somewhat) that they get their booster dose at the same time as the flu shot:
- Male respondents (83%)
- Respondents over 55 years old (83%)
- Those who earn over $80,000 (82%)
All respondents were asked if they would consider taking the COVID-19 vaccine as a routine vaccine annually. About two-thirds of respondents (64%) indicated that they would be likely to take the COVID-19 vaccine as a routine vaccine: 41% very likely and 23% somewhat likely. In contrast, nearly one respondent out of four (23%) indicated it was unlikely: 11% not likely and 18%, not at all likely.
Figure 16.20: If COVID-19 vaccines were offered as a routine vaccine (e.g., annually), how likely would you be to get one?
Sample frame: All respondents (n=3,004)
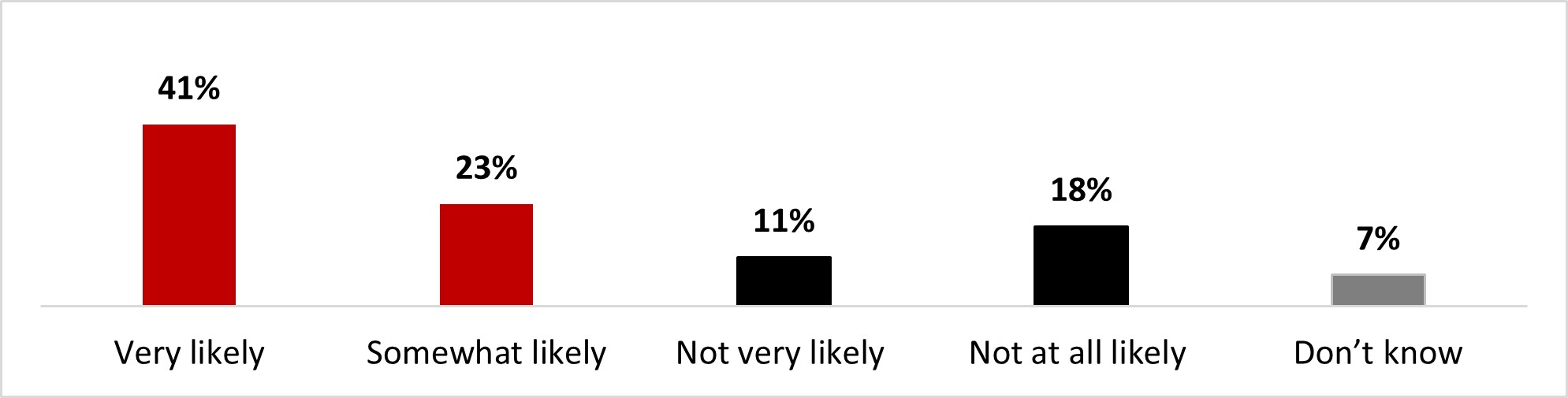
Figure 16.20: Text description
- Very likely
- 41%
- Somewhat likely
- 23%
- Not very likely
- 11%
- Not at all likely
- 18%
- Don't know
- 7%
Some subgroups were more likely to state it was very or somewhat likely that they get a COVID-19 vaccine as a routine vaccine, including:
- Male respondents (67%)
- Respondents over 55 years old (75%)
- Residents of British Columbia and the Territories (73%)
- Those who hold a university degree (71%)
- Respondents who are not parents of children less than 18 (67%)
Among respondents who were unsure or considered it unlikely that they would take the COVID-19 vaccine as a part of their annual vaccine routine, the main reasons given for their hesitation were concerns about long-term effects (19%), belief that COVID-19 is not a sufficiently serious infection to require booster shots (11%), being fed up with vaccination (9%), doubting the effectiveness of the vaccine in preventing the spread of the disease (9%), and the belief that they are sufficiently protected with the doses already had ( 9%).
Figure 16.21: What is the top reason you are unlikely or uncertain about getting a routine COVID-19 vaccine?
Sample frame: Those who are not likely or don't know if they would get a routine COVID-19 shot (n=1,138)
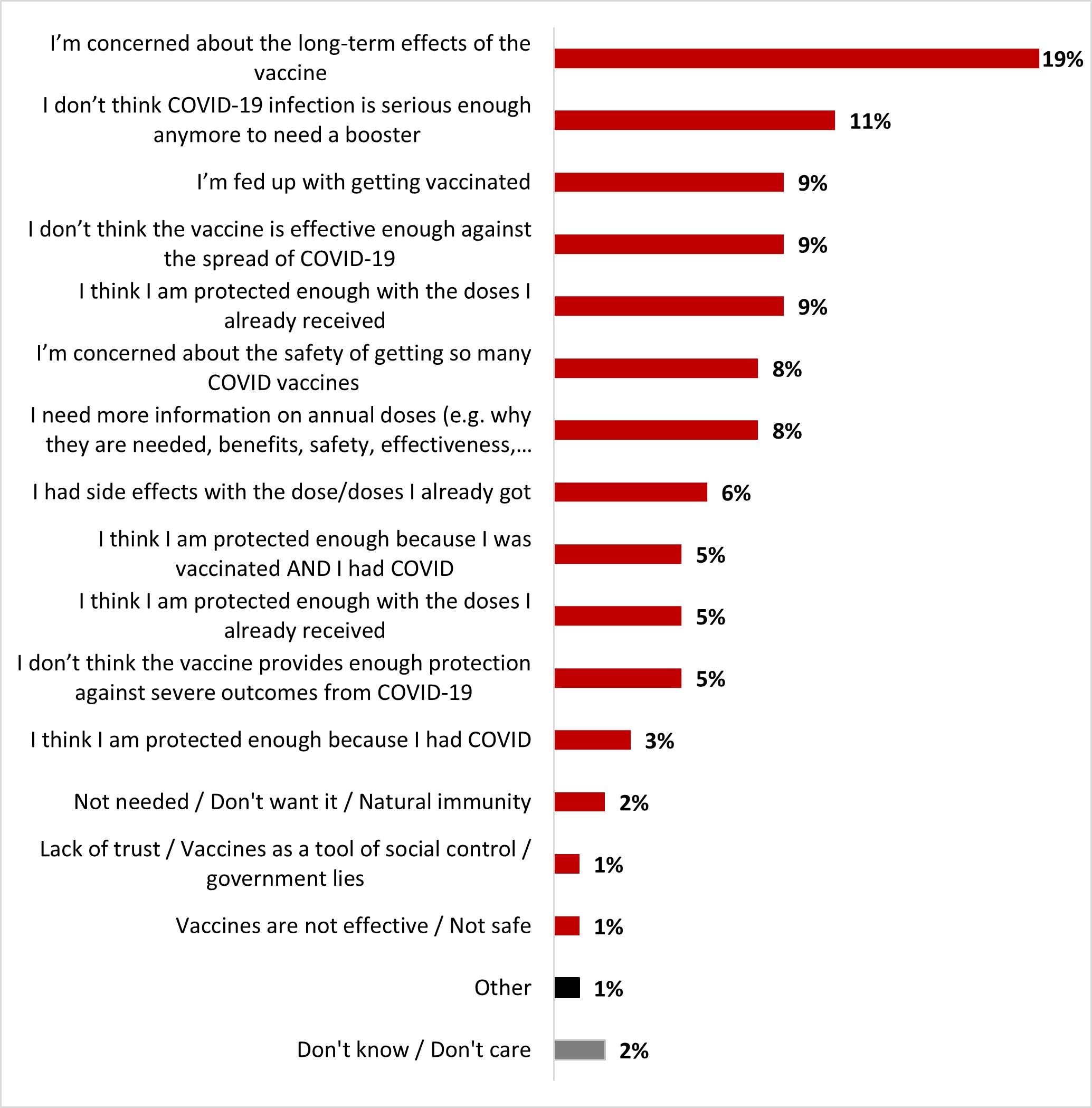
Figure 16.21: Text description
- Don't know / Don't care
- 2%
- Other
- 1%
- Vaccines are not effective / Not safe
- 1%
- Lack of trust / Vaccines as a tool of social control / government lies
- 1%
- Not needed / Don't want it / Natural immunity
- 2%
- I think I am protected enough because I had COVID
- 3%
- I don't think the vaccine provides enough protection against severe outcomes from COVID-19
- 5%
- I think I am protected enough with the doses I already received
- 5%
- I think I am protected enough because I was vaccinated AND I had COVID
- 5%
- I had side effects with the dose/doses I already got
- 6%
- I need more information on annual doses (e.g. why they are needed, benefits, safety, effectiveness, etc.)
- 8%
- I'm concerned about the safety of getting so many COVID vaccines
- 8%
- I think I am protected enough with the doses I already received
- 9%
- I don't think the vaccine is effective enough against the spread of COVID-19
- 9%
- I'm fed up with getting vaccinated
- 9%
- I don't think COVID-19 infection is serious enough anymore to need a booster
- 11%
- I'm concerned about the long-term effects of the vaccine
- 19%
Women (22%) were more likely to state that they are concerned about the long-term effects of the vaccine, while men were more likely to think that a COVID-19 infection is not serious enough anymore to need a routine vaccine (14%) or to think that they are protected enough with the doses they already have (11%).
2.4 Childhood vaccination
Among parents or legal guardians of children aged 12 The present study deals with topics that you might have found distressing. If you found participation distressing, we want to encourage you to conside% reported that their children (12-17) had been vaccinated with at least one dose. More specifically, 4% of these respondents indicated that their children had received only one dose, 62% reported two doses, 21% reported three doses, and 1% reported four doses. More than one out of ten respondents (13%) indicated that their children had not received any doses yet: 4% were waiting to decide whether the child(ren) would be vaccinated, and 10% were determined not to have their children aged 12 to 17 vaccinated.
Figure 16.22: Thinking about your child(ren) aged 12-17, how many doses of a COVID-19 vaccine have they received?
Sample frame: Parents or guardians of at least one child 12-17 (n=323)
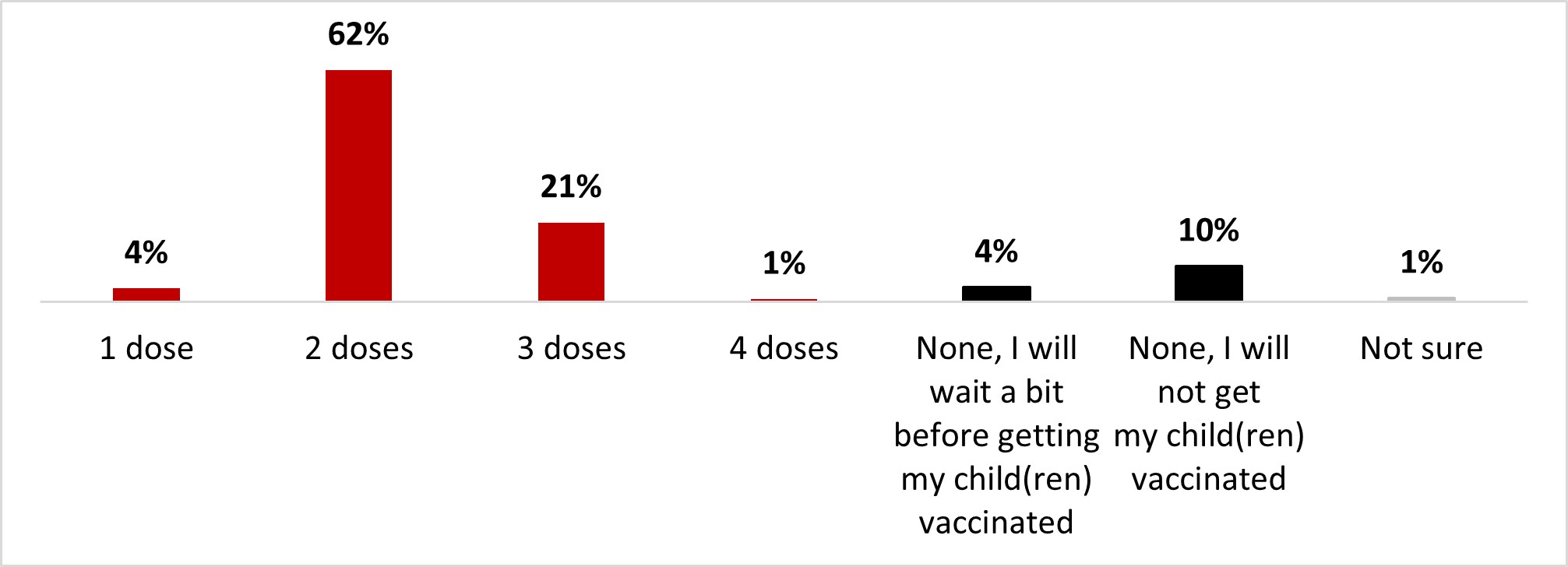
Figure 16.22: Text description
- 1 dose
- 4%
- 2 doses
- 62%
- 3 doses
- 21%
- 4 doses
- 1%
- None, I will wait a bit before getting my child(ren) vaccinated
- 4%
- None, I will not get my child(ren) vaccinated
- 10%
- Not sure
- 1%
Respondents from British Columbia were significantly more likely to have vaccinated their children with at least one dose (97%), while those in Quebec were more likely to have vaccinated them with two doses (74%). Parents who are vaccinated against COVID-19 (95%) were more likely to have vaccinated their children with at least one dose.
Among parents or legal guardians of children aged 12 to 17, the likelihood of getting booster doses for their child was 57%: 28% very likely and 29% somewhat likely. A third of these respondents (34%) reported that it was unlikely that they would seek out booster doses for their child(ren): 16% somewhat unlikely and 18% very unlikely.
Figure 16.23: Thinking about your child(ren) aged 12-17, how likely are you to have them receive a booster dose of the COVID-19 vaccine?
Sample frame: Parents or guardians of at least one child 12-17 who has received 1 or 2 doses (n=197)
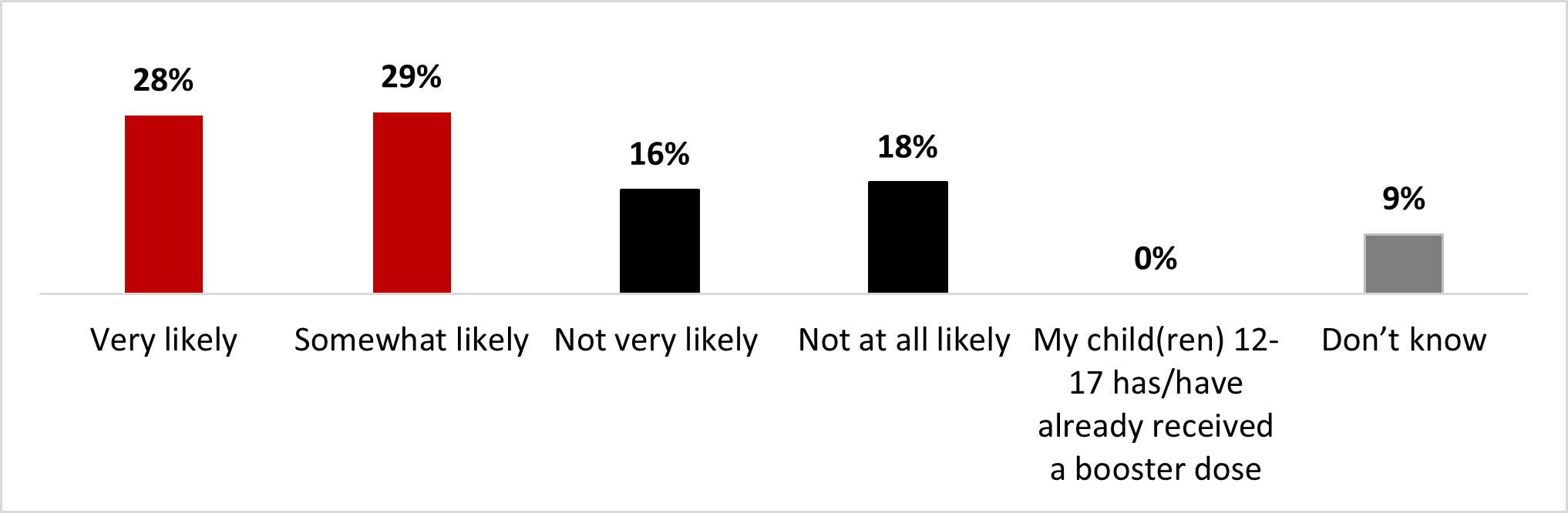
Figure 16.23: Text description
- Very likely
- 28%
- Somewhat likely
- 29%
- Not very likely
- 16%
- Not at all likely
- 18%
- My child(ren) 12-17 has/havealready received a booster dose
- 0%
- Don't know
- 9%
Parents who are vaccinated against COVID-19 (58%) were more likely to have their children receive a booster of the COVID-19 vaccine.
Among parents or legal guardians of children aged 5 to 11 years, 64% indicated that their child(ren) had had at least one dose of the COVID-19 vaccine. More specifically, 13% reported one dose, 44% reported two doses, and 7% reported three doses. A third of those respondents (33%) indicated that their child(ren) had not received any doses yet: 9% indicated that they were waiting to decide, and 24% stated that their child(ren) would not be vaccinated.
Figure 16.24: Thinking about your child(ren) aged 5-11, how many doses of a COVID-19 vaccine have they received?
Sample frame: Parents or guardians of at least one child 5-11 (n=365)
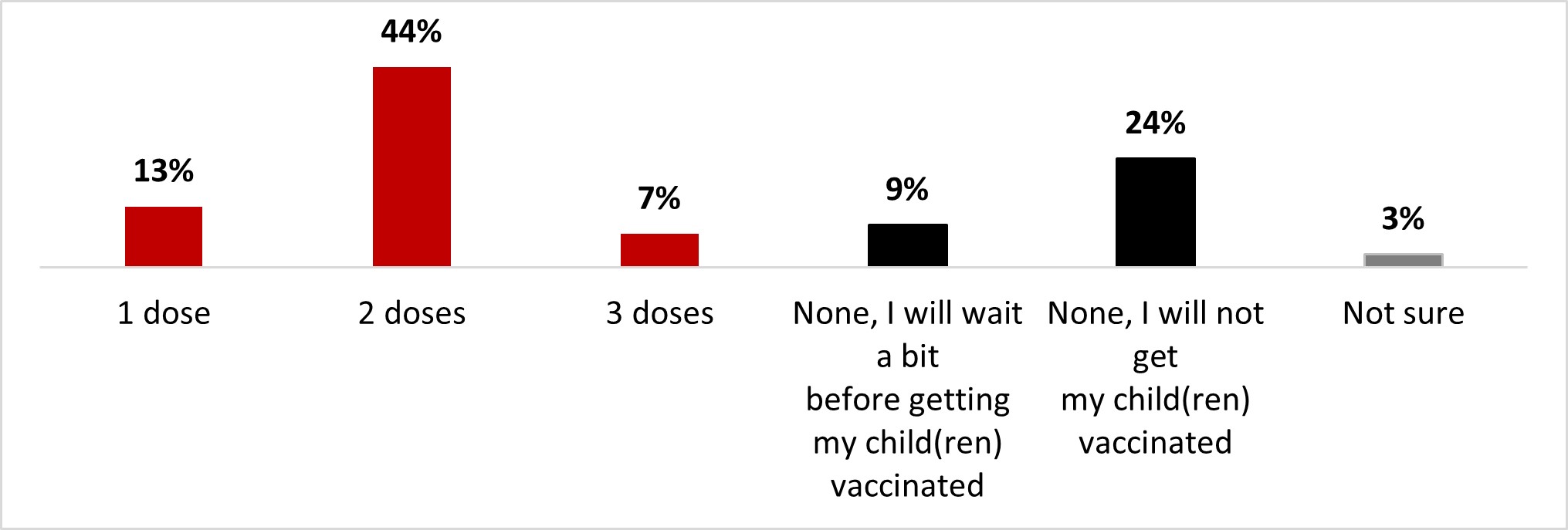
Figure 16.24: Text description
- 1 dose
- 13%
- 2 dose
- 44%
- 3 dose
- 7%
- None, I will wait a bitbefore getting my child(ren)vaccinated
- 9%
- None, I will not getmy child(ren)vaccinated
- 24%
- Not sure
- 3%
Parents who are vaccinated against COVID-19 (70%) were more likely to have vaccinated their children with at least one dose.
Among parents or legal guardians of children aged 5 to 11 who received at least one dose, seven out of ten respondents (70%) reported that it was likely that their child(ren) would receive a booster dose: 36% very likely and 35% somewhat likely. In contrast, one out of five respondents (21%) mentioned that it was unlikely that they would get booster doses for their child(ren): 13% unlikely and 8% not at all likely.
Figure 16.25: Thinking about your child(ren) aged 5-11, how likely are you to have them receive a booster dose of the COVID-19 vaccine?
Sample frame: Parents or guardians of at least one child 5-11 who has received 1 or 2 doses (n=207)
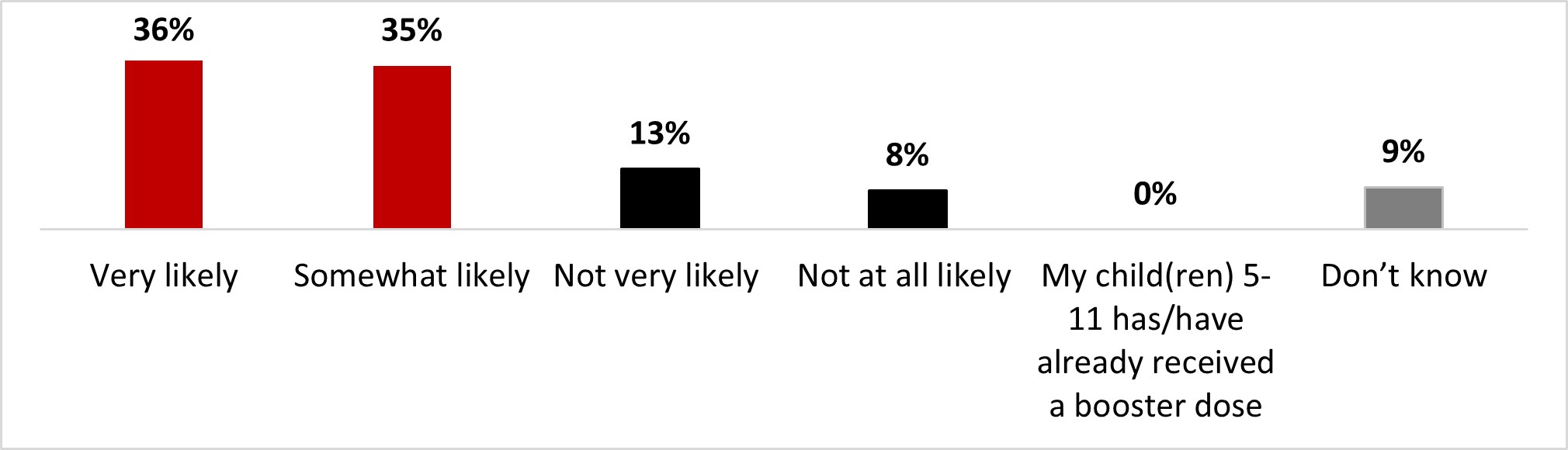
Figure 16.25: Text description
- Very likely
- 36%
- Somewhat likely
- 35%
- Not very likely
- 13%
- Not at all likely
- 8%
- My child(ren) 5-11 has/havealready received a booster dose
- 0%
- Don't know
- 9%
Parents who speak English (76%) were more likely to have their children receive a booster of the COVID-19 vaccine.
The main reasons that parents of children aged five to 17 were reluctant to pick up booster doses for their child(ren) were: concerns about long-term effects (26%), belief that their child(ren) was sufficiently protected with the doses they received (15%), concerns about the safety of the booster doses (14%), doubt about having to pick up booster doses after their child(ren) had been infected with COVID-19 and being fed up with the vaccination (10%).
Figure 16.26: Why are you not likely or not sure to have your child(ren) get a booster dose of a COVID-19 vaccine?
Sample frame: Those who are unlikely to or don't know if they will have their children 5-11 or 12-17 get a booster dose (n=142)
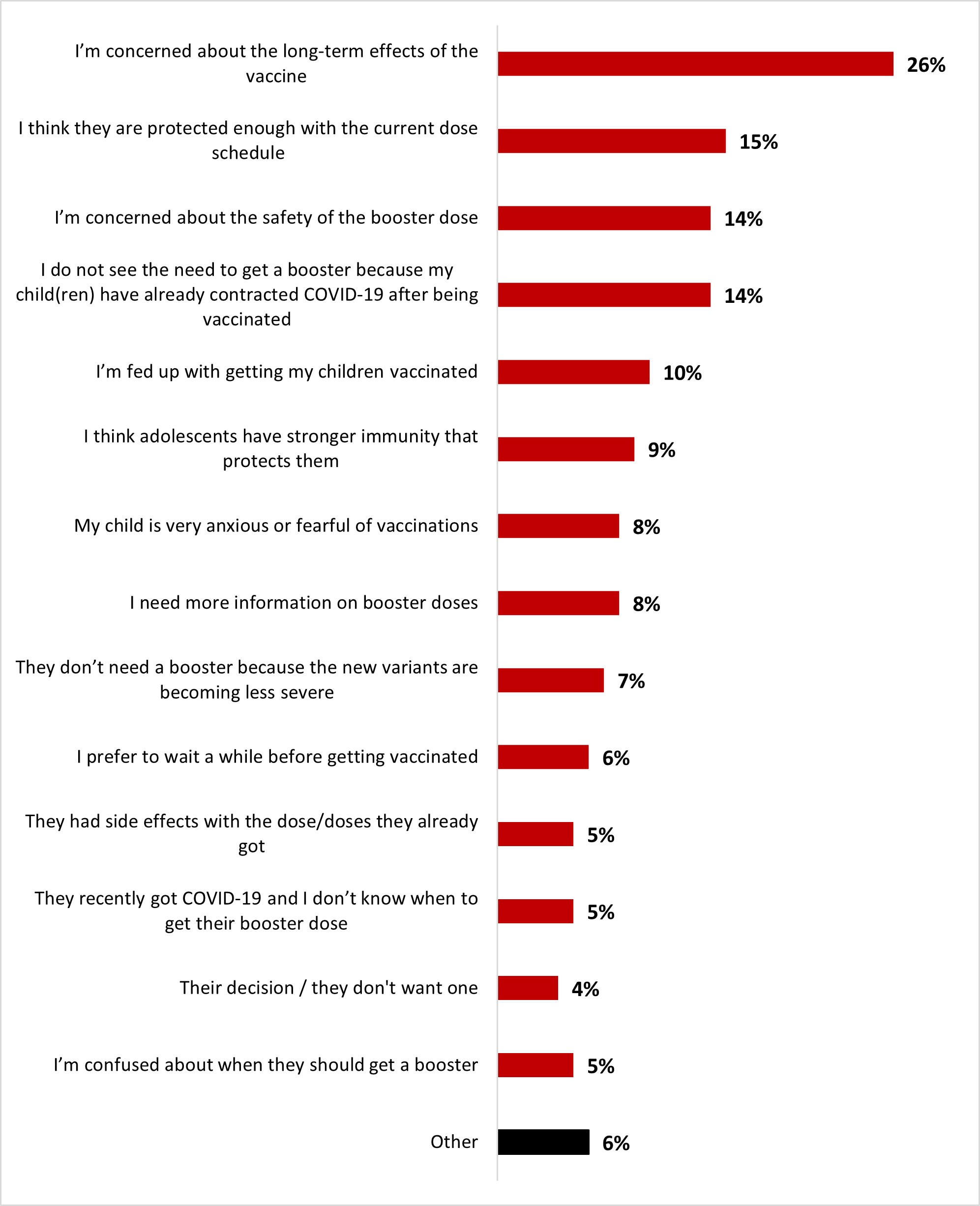
Figure 16.26: Text description
- Other
- 6%
- I'm confused about when they should get a booster
- 5%
- Their decision / they don't want one
- 4%
- They recently got COVID-19 and I don't know when to get their booster dose
- 5%
- They had side effects with the dose/doses they already got
- 5%
- I prefer to wait a while before getting vaccinated
- 6%
- They don't need a booster because the new variants are becoming less severe
- 7%
- I need more information on booster doses
- 8%
- My child is very anxious or fearful of vaccinations
- 8%
- I think adolescents have stronger immunity that protects them
- 9%
- I'm fed up with getting my children vaccinated
- 10%
- I do not see the need to get a booster because my child(ren) have already contracted COVID-19 after being vaccinated
- 14%
- I'm concerned about the safety of the booster dose
- 14%
- I think they are protected enough with the current dose schedule
- 15%
- I'm concerned about the long-term effects of the vaccine
- 26%
No relevant significant differences among subgroups are to be noted.
Among parents or guardians of children aged six months to five years, the rate of vaccination of their child(ren) in this age group was 21%. About four out of ten parents (44%) said they would wait to make a decision about vaccinating their child(ren), and one-third (33%) said they did not have any plans to have their child(ren) vaccinated.
Figure 16.27: Thinking about your child(ren) between the ages of 6 months and under 5, have they received at least one dose of a COVID-19 vaccine? Select all that apply.
Sample frame: Parents or guardians of at least one child between 6 months and under 5 years old (n=318)
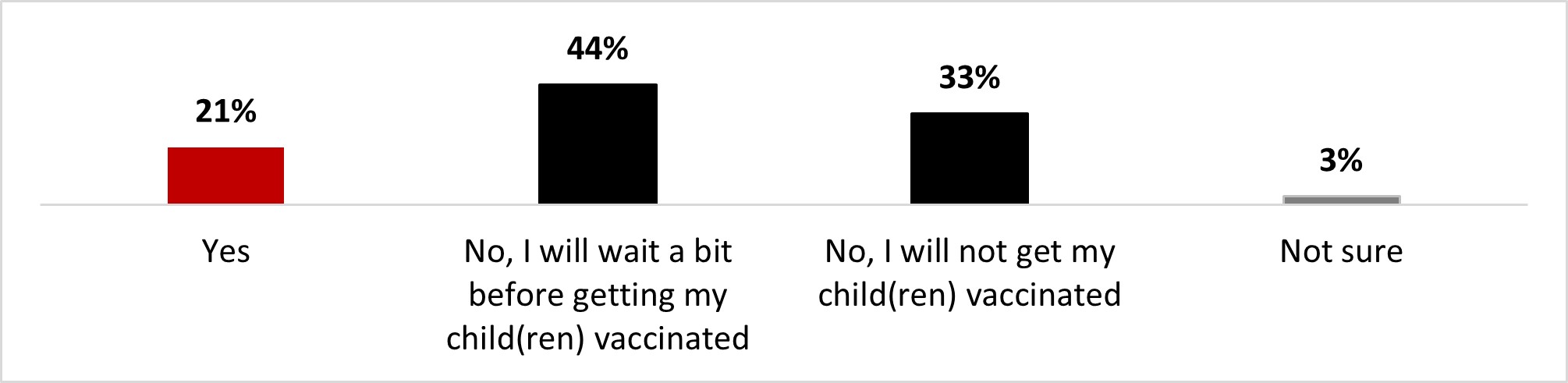
Figure 16.27: Text description
- Yes
- 21%
- No, I will wait a bit before getting my child(ren) vaccinated
- 44%
- No, I will not get my child(ren) vaccinated
- 33%
- Not sure
- 3%
Parents from Ontario (30%) and parents who have received at least one dose of the COVID-19 vaccine (24%) were more likely to have their children receive a dose of the COVID-19 vaccine.
Among parents or legal guardians of children aged six months to five years who do not intend to have their child(ren) vaccinated, the top three motivators to encourage vaccination were: having more information about children who have already received the vaccine (23%), having more information about the risks of COVID-19 for children (12%), and being reassured that the vaccine is safe for child(ren) (12%). It is important to note that one-quarter of respondents (25%) mentioned that nothing would make them more likely to have their child(ren) vaccinated.
Figure 16.28: Which of the following factors would make you more likely to vaccinate your child(ren) against COVID-19? Up to 3 answers.
Sample frame: Parents or guardians of children 6 months and under 5 who will not get their child vaccinated will wait a bit, or are not sure (n=266)
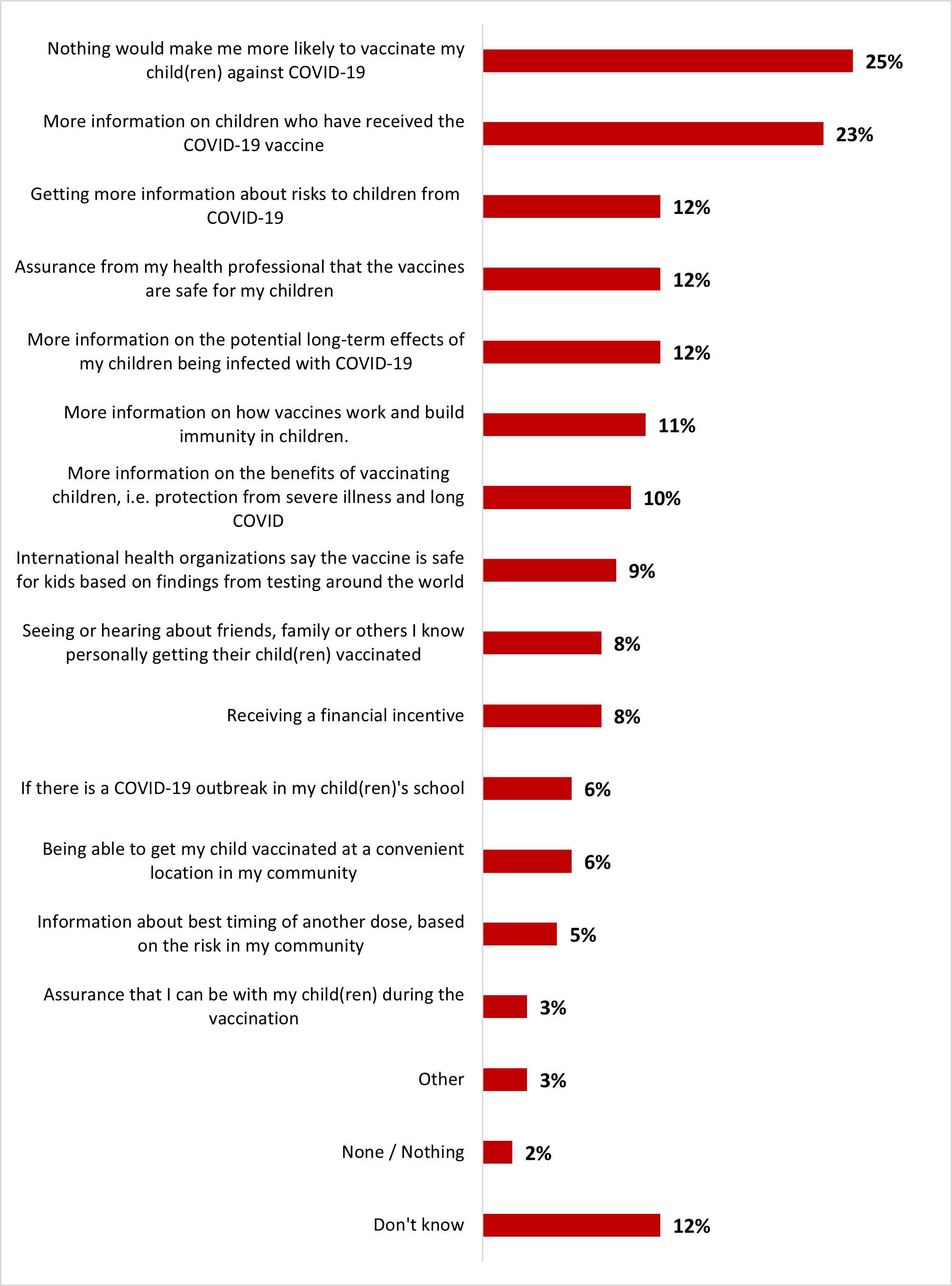
Figure 16.28: Text description
- Don't know
- 12%
- None / Nothing
- 2%
- Other
- 3%
- Assurance that I can be with my child(ren) during the vaccination
- 3%
- Information about best timing of another dose, based on the risk in my community
- 5%
- Being able to get my child vaccinated at a convenient location in my community
- 6%
- If there is a COVID-19 outbreak in my child(ren)'s school
- 6%
- Receiving a financial incentive
- 8%
- Seeing or hearing about friends, family or others I know personally getting their child(ren) vaccinated
- 8%
- International health organizations say the vaccine is safe for kids based on findings from testing around the world
- 9%
- More information on the benefits of vaccinating children, i.e. protection from severe illness and long COVID
- 10%
- More information on how vaccines work and build immunity in children.
- 11%
- More information on the potential long-term effects of my children being infected with COVID-19
- 12%
- Assurance from my health professional that the vaccines are safe for my children
- 12%
- Getting more information about risks to children from COVID-19
- 12%
- More information on children who have received the COVID-19 vaccine
- 23%
- Nothing would make me more likely to vaccinate my child(ren) against COVID-19
- 25%
Women were more likely (29%) to mention needing more information on children who have received the COVID-19 vaccine, e.g., from clinical trials involving children or from real-world use, including data on safety and effectiveness. Respondents of 18 to 34 years of age (13%) were more likely to mention wanting financial incentives. Parents who were not vaccinated (67%) with at least one dose of the COVID-19 vaccine were more likely to mention that nothing would make them more likely to vaccinate their children.
Parents of children under 18 years of age were asked if their child(ren)'s regular vaccination was missed or delayed due to the pandemic. Fewer than one out of five parents (16%) reported having missed a regular vaccination due to COVID-19. Eight out of ten parents (80%) reported that their child(ren) did not miss or delay any vaccinations during the pandemic.
Figure 16.29: Have any of your child's regular childhood vaccinations been missed/delayed as a result of the pandemic?
Sample frame: All respondents (n=3,004)
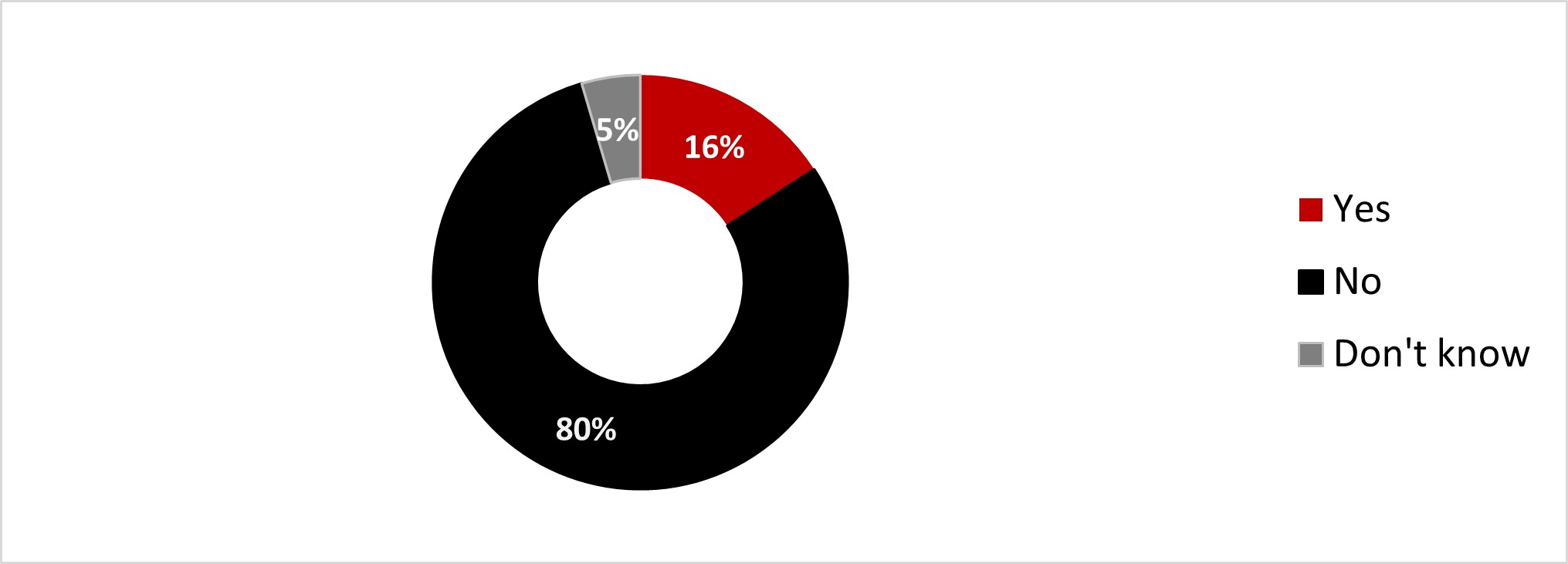
Figure 16.29: Text description
- Yes
- 16%
- No
- 80%
- Don't know
- 5%
Respondents from Ontario (20%) were significantly more likely to state that their child's regular childhood vaccinations have been delayed as a result of the pandemic.
Among the 16% of parents whose children missed or postponed vaccines during the pandemic, eight out of ten (79%) indicated that they intended to follow up on the missed vaccination. In contrast, 17% did not intend to follow up.
Figure 16.30: Do you intend to catch up on your child's missed/delayed regular childhood vaccinations?
Sample frame: Parents of children who have had missed/delayed vaccinations due to the pandemic (n=129)
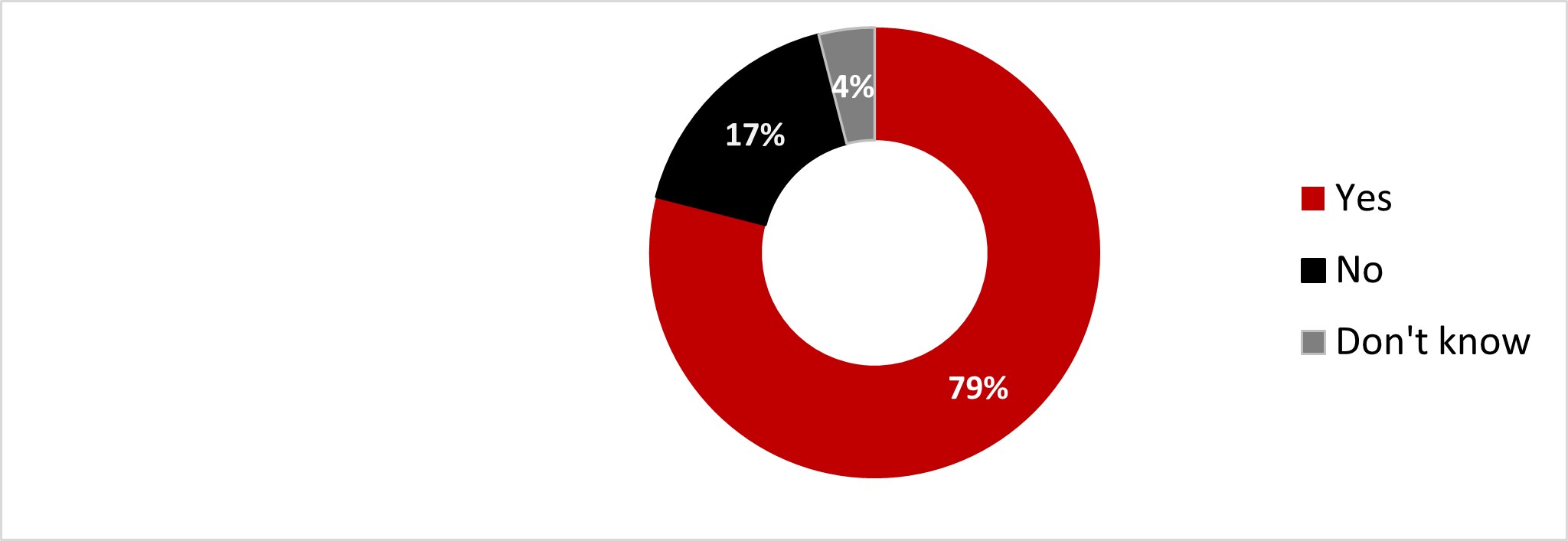
Figure 16.30: Text description
- Yes
- 79%
- No
- 17%
- Don't knowDon't know
- 4%
Women (88%) were more likely to state wanting to catch up on their child's missed or delayed vaccination.
2.5 Routine vaccination
Of all respondents, 8% indicated that they had missed a routine vaccination due to the COVID-19 pandemic. Seven out of ten respondents (70%) indicated that they had not missed any vaccinations for that reason. Just under one out of five respondents indicated that this did not apply to their personal situation (17%), while 5% did not know if they had missed a vaccination.
Figure 16.31: Adult routine vaccinations are defined as routine vaccines and/or boosters given in adulthood to protect against serious diseases such as shingles (recommended for 50+), tetanus, pertussis (whooping cough), influenza (flu) and pneumococcal (recommended for 18+ with chronic medical conditions and healthy adults aged 65+). Have you missed/delayed any routine vaccinations as a result of the pandemic?
Sample frame: All respondents (n=3,004)
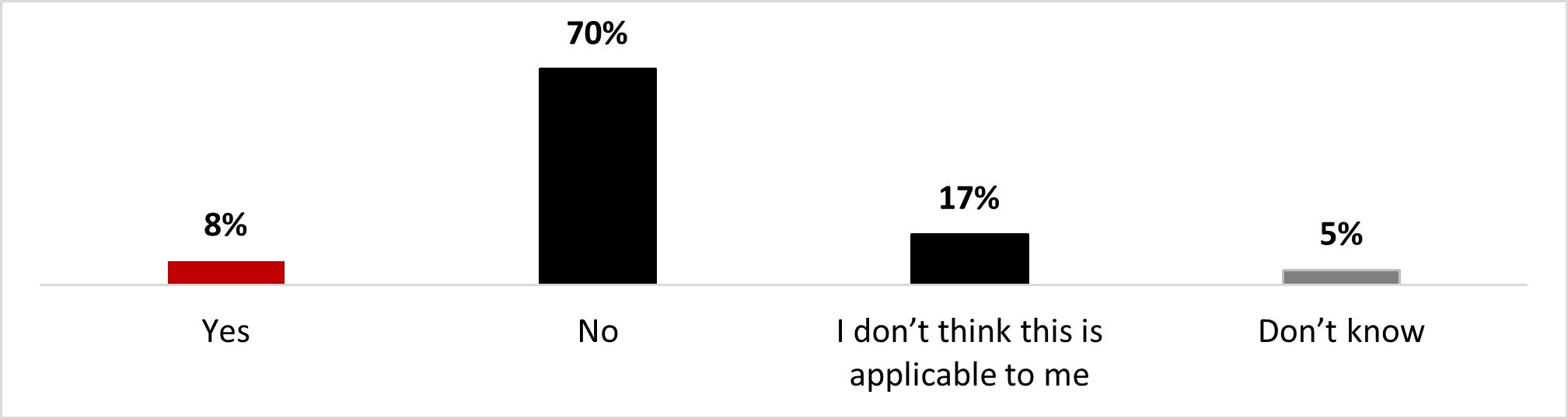
Figure 16.31: Text description
- Yes
- 8%
- No
- 70%
- I don't think this is applicable to me
- 17%
- Don't know
- 5%
18-to-34 year-olds (12%) were significantly more likely to state they have missed/delayed routine vaccinations as a result of the pandemic.
Sixty-three percent of respondents who have missed a vaccination intend to follow up to get the missed vaccinations done. In contrast, one out of four respondents in this situation indicated that they had no intention of getting those vaccines (24%), and 13% were undecided.
Figure 16.32: Do you intend to catch up on your missed or delayed routine vaccinations?
Sample frame: Those who have missed or delayed any routine vaccinations (n=233)
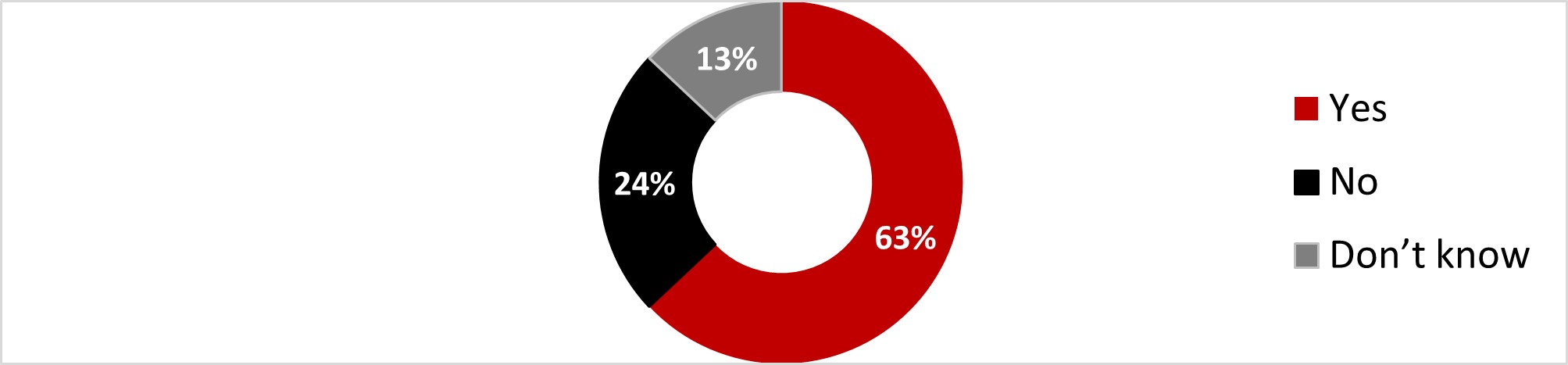
Figure 16.32: Text description
- Yes
- 63%
- No
- 24%
- Don't know
- 13%
Respondents from Alberta (87%) were significantly more likely to state they intend to catch up on their missed or delayed routine vaccination.
Respondents who do not intend to resume missed vaccines reported having concerns about vaccine side effects (22%), being worried about the long-term effects of vaccines (22%) and being convinced that the immune system is strong without vaccines (11%). These were the top three reasons for not wanting to follow up on missed vaccines.
Figure 16.33: Why do you not intend to catch up on your missed/delayed routine vaccinations?
Sample frame: Those who have missed or delayed any routine vaccinations (n=58)
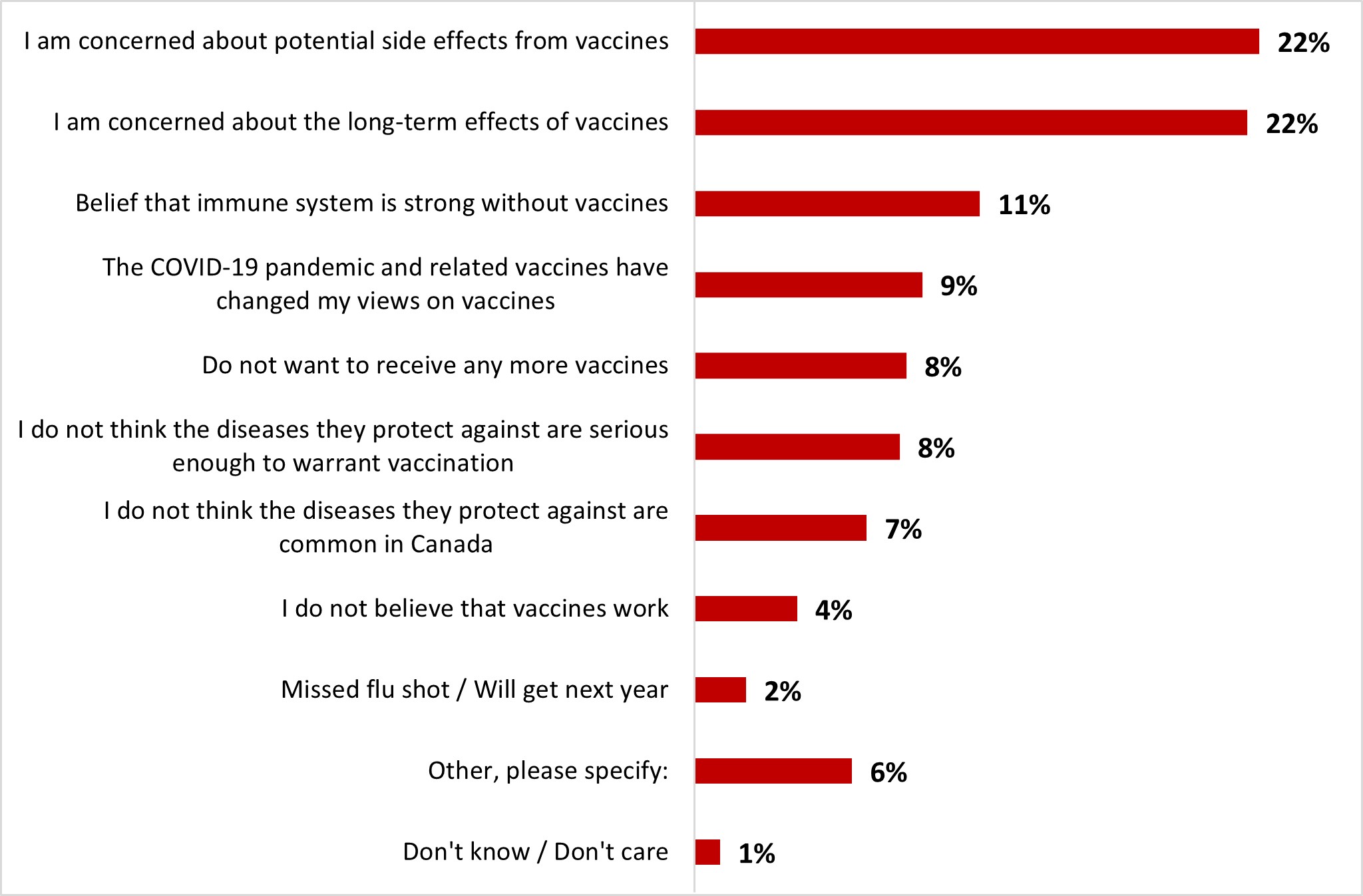
Figure 16.33: Text description
- Don't know / Don't care
- 1%
- Other, please specify:
- 6%
- Missed flu shot / Will get next year
- 2%
- I do not believe that vaccines work
- 4%
- I do not think the diseases they protect against are common in Canada
- 7%
- I do not think the diseases they protect against are serious enough to warrant vaccination
- 8%
- Do not want to receive any more vaccines
- 8%
- The COVID-19 pandemic and related vaccines have changed my views on vaccines
- 9%
- Belief that immune system is strong without vaccines
- 11%
- I am concerned about the long-term effects of vaccines
- 22%
- I am concerned about potential side effects from vaccines
- 22%
Due to the small sample size, no significant differences are to be noted.
The COVID-19 pandemic did not have a positive or negative impact on vaccine confidence for half of the respondents. Indeed, 54% of respondents stated that their confidence level was about the same as before the pandemic. Around one in five respondents (19%) indicated that they were now more confident (10% a lot more and 9% somewhat more confident), while 21% of respondents indicated that they were now less confident (9% a lot less and 12% somewhat less confident) about vaccination in general.
Figure 16.34: Has the recent COVID-19 pandemic had an impact on your confidence in vaccinations in general? Sample frame: All respondents (n=3,004)
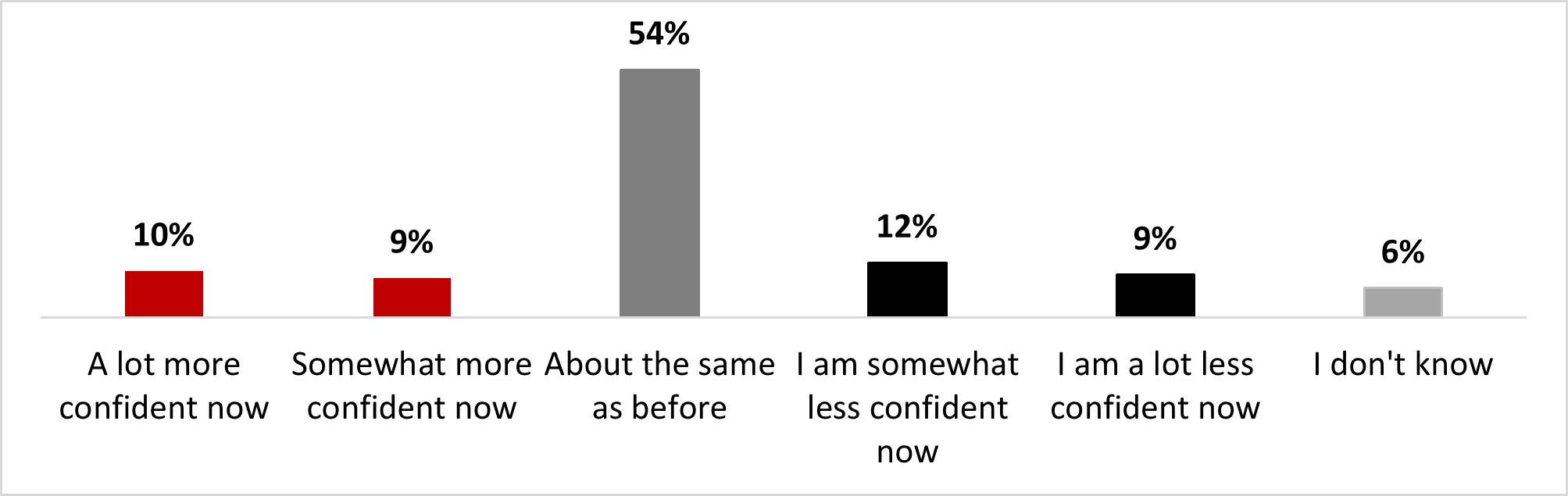
Figure 16.34: Text description
- A lot more confident now
- 10%
- Somewhat more confident now
- 9%
- About the same as before
- 54%
- I am somewhat less confident now
- 12%
- I am a lot less confident now
- 9%
- I don't know
- 6%
18-to-34 year-old individuals (17%), along with parents of children under 18 (16%) were significantly more likely to state being somewhat less confident about vaccines now.
The main reasons mentioned by respondents who experienced a decrease in their level of confidence in vaccines were that the COVID-19 vaccines have had a detrimental impact on their perception of vaccines in general (44%), that they are now more concerned about the safety of vaccines in general (44%), and the perception that the COVID-19 pandemic has shown that vaccines do not work well (32%). Each other reason was mentioned by less than a third of respondents.
Figure 16.35: Why are you less confident in vaccinations? Select all that apply.
Sample frame: Those who are less confident in vaccines now than before the pandemic (n=640)
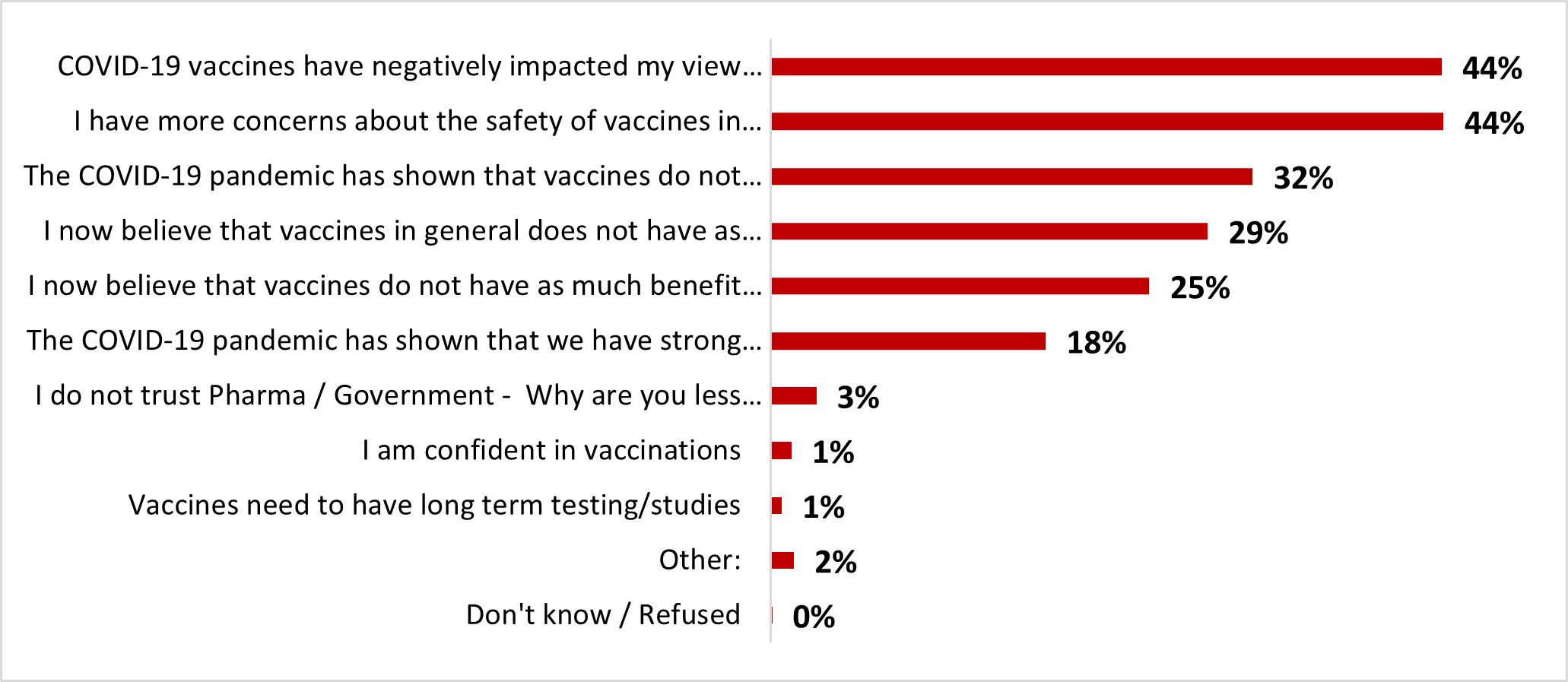
Figure 16.35: Text description
- Don't know / Refused
- 0%
- Other:
- 2%
- Vaccines need to have long term testing/studies
- 1%
- I am confident in vaccinations
- 1%
- I do not trust Pharma / Government - Why are you less confident in vaccinations
- 3%
- The COVID-19 pandemic has shown that we have strong immune systems without vaccines
- 18%
- I now believe that vaccines do not have as much benefit in preventing severe outcomes
- 25%
- I now believe that vaccines in general does not have as much benefit in stopping the spread of viruses
- 29%
- The COVID-19 pandemic has shown that vaccines do not work very well
- 32%
- I have more concerns about the safety of vaccines in general
- 44%
- COVID-19 vaccines have negatively impacted my view on vaccines in general
- 44%
Respondents 55 years of age or older were significantly more likely to state that:
- The pandemic has shown that vaccines do not work very well (43%),
- They believed that vaccines in general, do not have as much benefit in stopping the spread of viruses (39%)
White-identifying respondents were significantly more likely to state that:
- COVID-19 vaccines have negatively impacted their view on vaccines in general (49%)
- The pandemic has shown that we have strong immune systems without vaccines (20%)
Nearly half of the respondents (48%) indicated that they intend to take the flu vaccine this year. Slightly fewer (41%) indicated otherwise, while one out of ten (11%) were unsure.
Figure 16.36: Do you intend to get the flu vaccine this year?
Sample frame: All respondents (n=3,004)
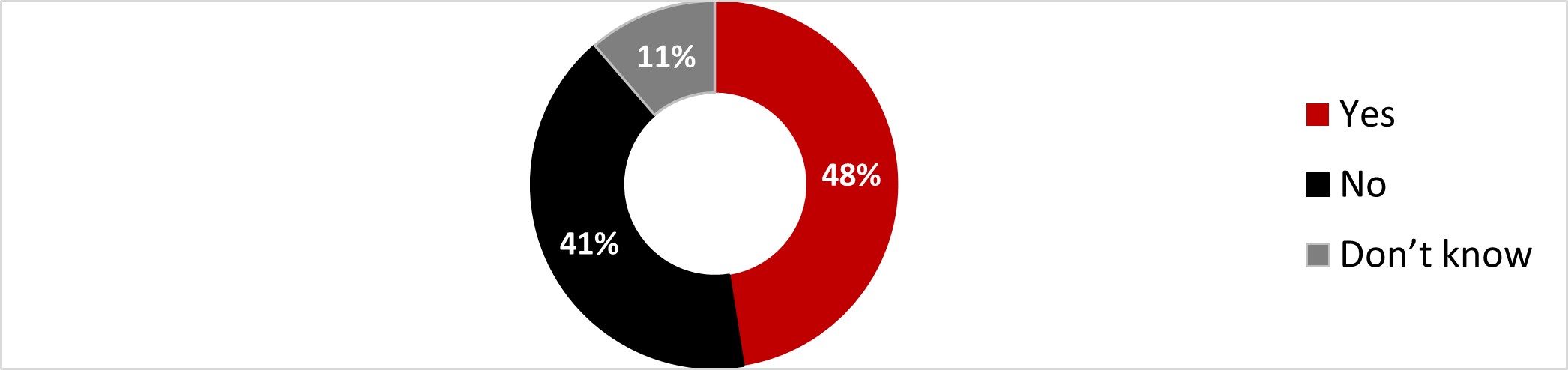
Figure 16.36: Text description
- Yes
- 48%
- No
- 41%
- Don't know
- 11%
The following subgroups were significantly more likely to intend on getting the flu vaccine this year:
- Those over 55 years old (63%)
- Respondents from British Columbia and the Territories (57%) and those from the Atlantic regions (57%)
- Those with a university degree (52%)
- Those who are not parents of children under 18 (51%)
The main reasons respondents gave for not intending to get the flu vaccine were that they had never had the flu shot before (47%), that they have the perception of being healthy and never catching the flu (21%), the perception that the flu shot doesn't work (12%) that the flu doesn't really make them sick (11%), and concerns about side effects of the flu shot (10%). The other reasons were all mentioned by less than 10% of respondents.
Figure 16.37: Why do you not intend to get your flu shot this year? Select all that apply.
Sample frame: Those who do not intend or do not know if they intend on getting the flu vaccine this year (n=1,651)
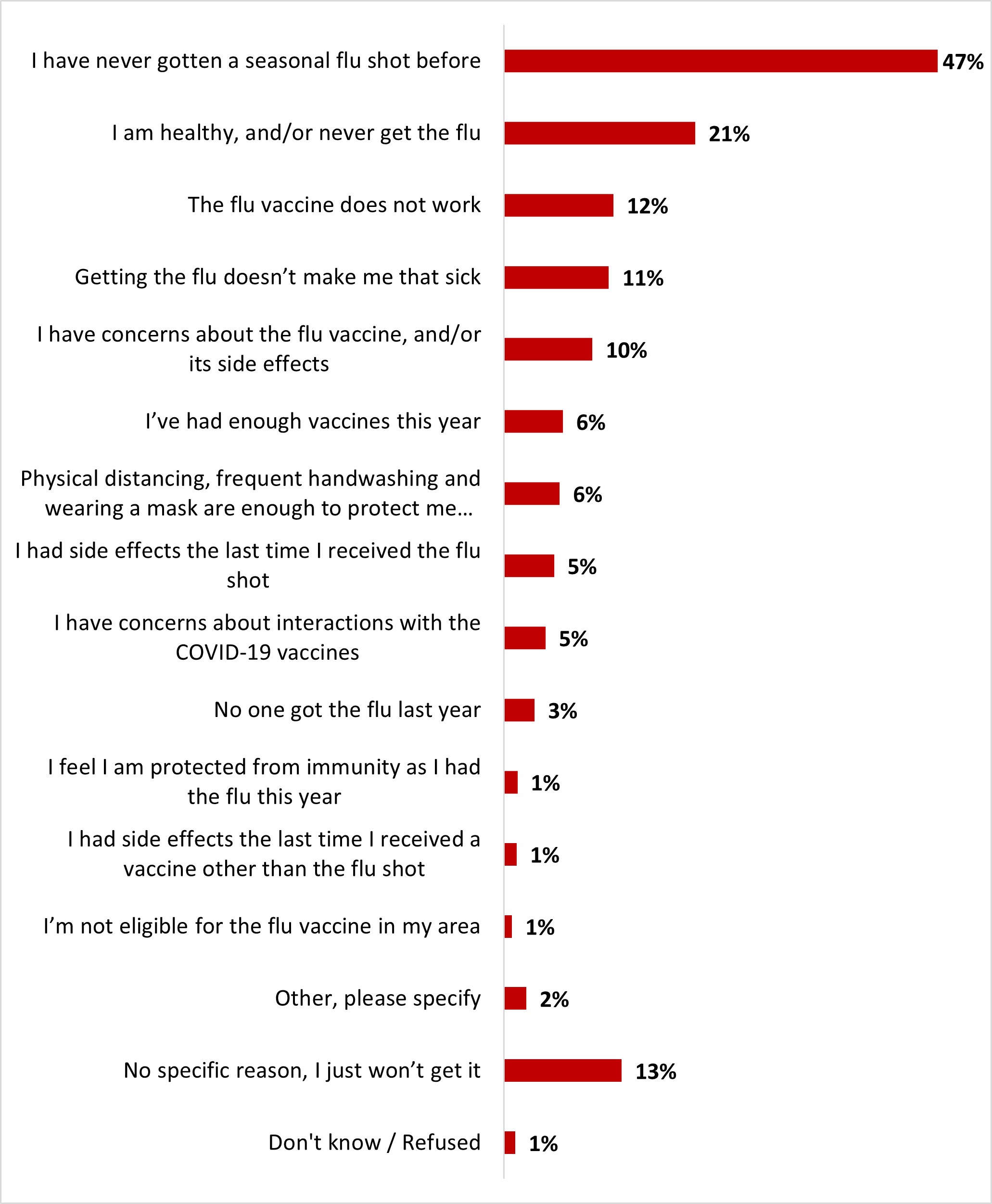
Figure 16.37: Text description
- Don't know / Refused
- 1%
- No specific reason, I just won't get it
- 13%
- Other, please specify
- 2%
- I'm not eligible for the flu vaccine in my area
- 1%
- I had side effects the last time I received a vaccine other than the flu shot
- 1%
- I feel I am protected from immunity as I had the flu this year
- 1%
- No one got the flu last year
- 3%
- I have concerns about interactions with the COVID-19 vaccines
- 5%
- I had side effects the last time I received the flu shot
- 5%
- Physical distancing, frequent handwashing and wearing a mask are enough to protect me from the flu
- 6%
- I've had enough vaccines this year
- 6%
- I have concerns about the flu vaccine, and/or its side effects
- 10%
- Getting the flu doesn't make me that sick
- 11%
- The flu vaccine does not work
- 12%
- I am healthy, and/or never get the flu
- 21%
- I have never gotten a seasonal flu shot before
- 47%
Respondents from Quebec were significantly more likely to state that:
- They had never gotten a flu shot before (54%)
- Getting the flu did not make them that sick (15%)
Parents of children less than 18 were significantly more likely to state that:
- They just won't get the flu vaccine (16%)
- It does not work (16%)
2.6 Public health measures
Washing hands for 20 seconds with soap and warm water (80%), staying home and away from others when sick (78%), and using a hand sanitizer with a 60% alcohol solution when soap is not available (66%) were the three most regularly adopted individual protection measures. Other individual protection measures, such as physical distancing (58%), avoiding closed and crowded spaces (53%), adopting individual protection measures when interacting with people at risk (52%), wearing a mask indoors when around others when feeling sick (52%), and limiting contact with people outside of one's household (50%) were followed by less than two-thirds of respondents but by at least half of the respondents. Other personal protection measures were less regularly adopted.
Figure 16.38: How often do you follow each of the following individual public health measures?
Sample frame: All respondents (n=3,004)
NET always + often
- Washing hands for at least 20 seconds with soap and warm water
- 80%
- Staying home and away from others if you feel sick
- 78%
- Using hand sanitizer containing at least 60% alcohol if soap and water aren't available
- 66%
- Practising physical distancing
- 58%
- Avoiding closed spaces and crowded places
- 53%
- Using individual public health measures when interacting with someone who is at risk of more severe disease or outcomes from COVID-19
- 52%
- Wearing a mask – inside with others when you're feeling sick
- 52%
- Limiting the number of people you have contact with outside of your household
- 50%
- Wearing a mask–when indoors in a public space or in an indoor space with people from outside your immediate household.
- 39%
- Improving ventilation / Improving ventilation when people from outside your immediate household are in your home
- 36%
- Wearing a mask– when outside in a public space
- 21%
Figure 16.39: How often do you follow each of the following individual public health measures?
Sample frame: All respondents (n=3,004)
Reading note: Significantly lower differences are marked with a "-" sign, while significantly higher differences are marked with a "+".
| Gender | Age | Parents of children under 18 | Ethnicity | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | 18-34 | 35-54 | 55+ | Yes | No | White | Indigenous | Black | |
| Washing hands for at least 20 seconds with soap and warm water | 74% - | 87% + | 79% | 81% | 81% | 81% | 82% | 85% + | 81% | 80% |
| Staying home and away from others if you feel sick | 72% - | 85% + | 73% - | 78% | 82% + | 78% | 82% | 78% | 76% | 79% |
| Using hand sanitizer containing at least 60% alcohol, if soap and water aren't available | 59% - | 72% + | 69% + | 67% | 62% - | 64% - | 68% | 78% + | 67% | 65% |
| Practising physical distancing | 53% - | 63% + | 49% - | 55% - | 67% + | 57% - | 62% | 68% + | 53% - | 60% + |
| Avoiding closed spaces and crowded places | 49% - | 57% + | 44% - | 49% - | 62% + | 52% - | 59% | 62% + | 47% - | 55% + |
| Using individual public health measures when interacting with someone who is at risk of more severe disease or outcomes from COVID-19 | 49% - | 55% + | 49% | 51% | 56% + | 50% - | 54% | 62% + | 49% | 53% |
| Wearing a mask – inside with others when you're feeling sick | 47% - | 56% + | 47% - | 47% - | 59% + | 51% - | 48% | 61% + | 49% | 53% |
| Limiting the number of people you have contact with outside of your household | 48% | 52% | 45% - | 46% - | 57% + | 49% - | 59% + | 61% + | 46% - | 51% |
| Wearing a mask–when indoors in a public space or in an indoor space with people from outside your immediate household. | 37% | 41% | 34% - | 33% - | 47% + | 36% - | 42% | 50% + | 32% - | 42% + |
| Improving ventilation / Improving ventilation when people from outside your immediate household are in your home | 32% - | 39% + | 37% | 35% | 36% | 33% - | 32% | 48% + | 36% | 36% |
| Wearing a mask– when outside in a public space | 21% | 22% | 24% | 20% | 20% | 17% - | 22% | 39% + | 23% | 21% |
Figure 16.40: How often do you follow each of the following individual public health measures?
Sample frame: All respondents (n=3,004)
Reading note: Significantly lower differences are marked with a "-" sign, while significantly higher differences are marked with a "+".
| British Columbia + Territories | Alberta | Manitoba / Saskatchewan | Ontario | Quebec | Atlantic | |
|---|---|---|---|---|---|---|
| Washing hands for at least 20 seconds with soap and warm water | 81% | 78% | 73% - | 82% | 80% | 84% |
| Staying home and away from others if you feel sick | 83% + | 79% | 70% - | 79% | 76% | 79% |
| Using hand sanitizer containing at least 60% alcohol if soap and water aren't available | 66% | 58% - | 58% | 67% | 70% + | 63% |
| Practising physical distancing | 61% | 52% - | 56% | 61% | 55% | 61% |
| Avoiding closed spaces and crowded places | 55% | 46% - | 44% - | 56% + | 52% | 56% |
| Using individual public health measures when interacting with someone who is at risk of more severe disease or outcomes from COVID-19 | 54% | 40% - | 41% - | 55% + | 56% | 52% |
| Wearing a mask – inside with others when you're feeling sick | 56% | 47% | 42% - | 55% | 48% - | 59% |
| Limiting the number of people you have contact with outside of your household. | 53% | 43% - | 48% | 54% + | 46% - | 52% |
| Wearing a mask–when indoors in a public space or in an indoor space with people from outside your immediate household. | 44% | 27% - | 36% | 44% + | 33% - | 43% |
| Improving ventilation / Improving ventilation when people from outside your immediate household are in your home. | 41% | 29% - | 27% - | 38% | 37% | 32% |
| Wearing a mask– when outside in a public space. | 19% | 16% - | 20% | 27% + | 16% - | 21% |
Among those who said they did not regularly follow at least one of the personal protective measures assessed in the questionnaire, slightly more than one out of five respondents (21%) said they did not believe it helped reduce the spread of respiratory diseases. This was the most frequently mentioned reason for rarely or never practising individual protection measures, well ahead of the desire to gain acquired immunity from respiratory illnesses (9%), or because enforcing these measures causes too much disruption in their lives (8%).
Figure 16.41: What is the top reason you rarely or never practice any individual public health measures to reduce the spread of other respiratory diseases?
Sample frame: Those who rarely or never follow at least one public health measure (n=2,069)
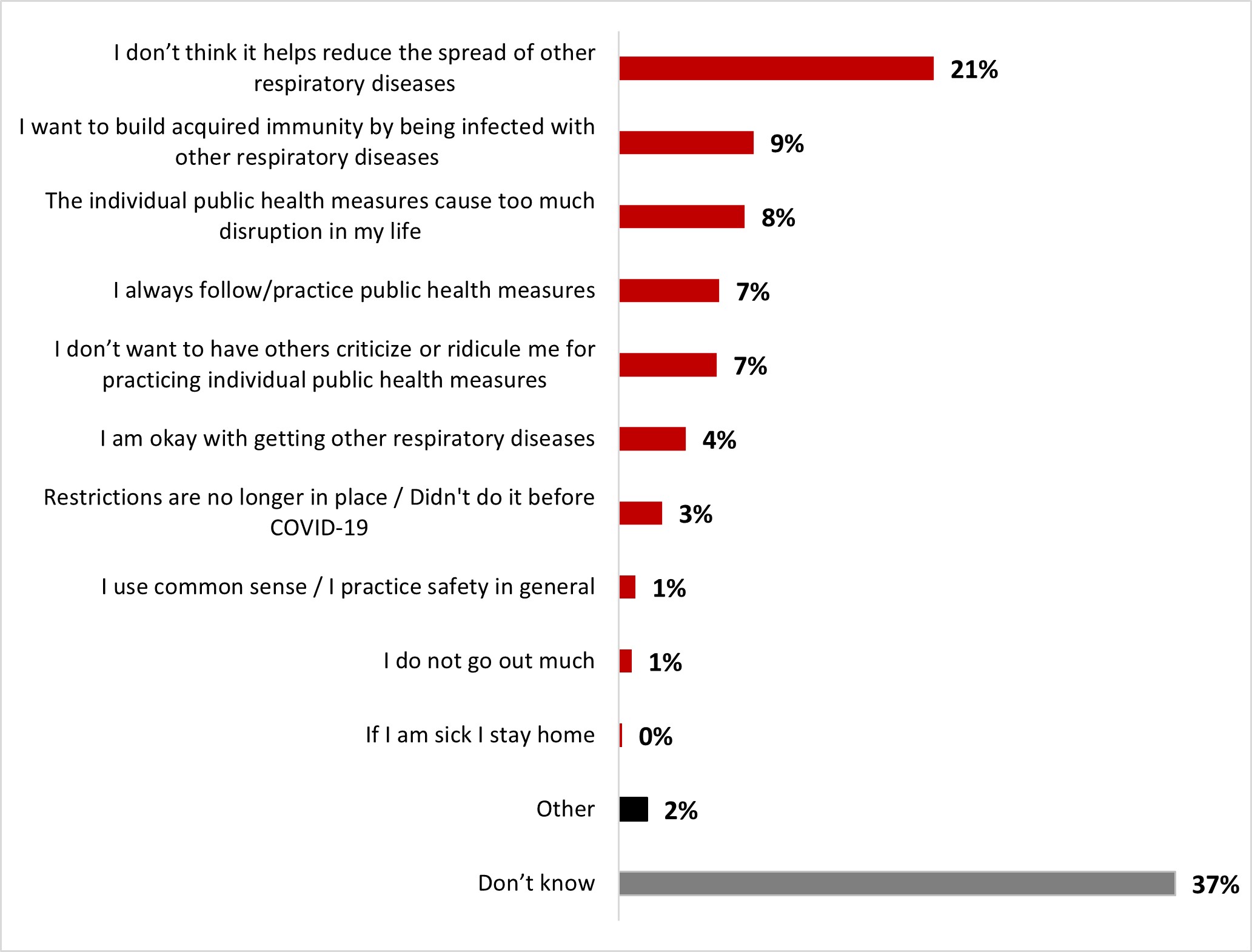
Figure 16.41: Text description
- Don't know
- 37%
- Other
- 2%
- If I am sick I stay home
- 0%
- I do not go out much
- 1%
- I use common sense / I practice safety in general
- 1%
- Restrictions are no longer in place / Didn't do it before COVID-19
- 3%
- I am okay with getting other respiratory diseases
- 4%
- I don't want to have others criticize or ridicule me for practicing individual public health measures
- 7%
- I always follow/practice public health measures
- 7%
- The individual public health measures cause too much disruption in my life
- 8%
- I want to build acquired immunity by being infected with other respiratory diseases
- 9%
- I don't think it helps reduce the spread of other respiratory diseases
- 21%
- White-identifying individuals were significantly more likely to state that they don't think individual public health measures help reduce the spread of other respiratory diseases (22%).
- Parents of children less than 18 were more likely to want to build acquired immunity (13%).
- 18 to 34 year-old respondents were more likely to state not wanting to be criticized or ridiculed for practising IPHM (11%), while those over 55 years old were more likely to state always practising public health measures (10%).
- Men were more likely than women to state that IPHM cause too much disruption in their life (11%).
A high proportion of respondents mentioned they thought that personal protective measures help reduce the transmission of respiratory diseases (84%): by a great deal (52%) or somewhat (32%). In contrast, about one out of ten respondents (11%) indicated that they did not believe this was the case: not very much (8%) and not at all (3%).
Figure 16.42: Many individual public health measures (e.g., staying home when sick, handwashing, mask-wearing) were recommended in 2020 to help control the spread of COVID-19. How much do you think these individual public health measures could help reduce the spread of other respiratory infectious diseases, such as seasonal influenza (the flu)?
Sample frame: All respondents (n=3,004)
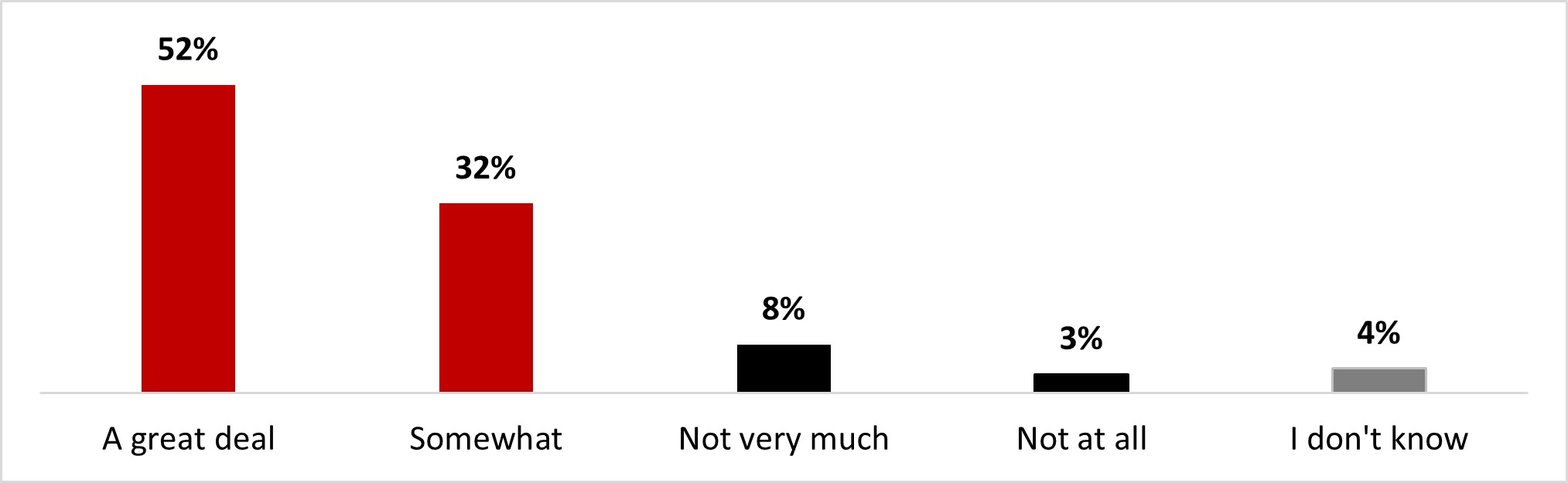
Figure 16.42: Text description
- A great deal
- 52%
- Somewhat
- 32%
- Not very much
- 8%
- Not at all
- 3%
- I don't know
- 4%
The following subgroups were significantly more likely to consider that individual public health measures help a great deal or somewhat reduce the spread of other respiratory infectious diseases:
- Respondents over 55 years old (90%)
- Residents of British Columbia and the Territories (90%), and the Atlantic regions (89%)
- Individuals who are not parents of children less than 18 (86%)
- Women (86%)
Overall, nine out of ten respondents (89%) indicated that they were confident when making decisions related to the choice of whether to use personal protective measures. Half of the respondents (50%) indicated that they were very confident, and more than a third (38%) indicated that they were somewhat confident about this. Only a minority of respondents indicated that they feel little (6%) or no (1%) confidence when making these choices.
Figure 16.43: How confident, if at all, do you feel about making your own decisions with respect to choosing to practice any or all of the individual public health measures mentioned in the previous questions (i.e. wearing a mask)?
Sample frame: All respondents (n=3,004)
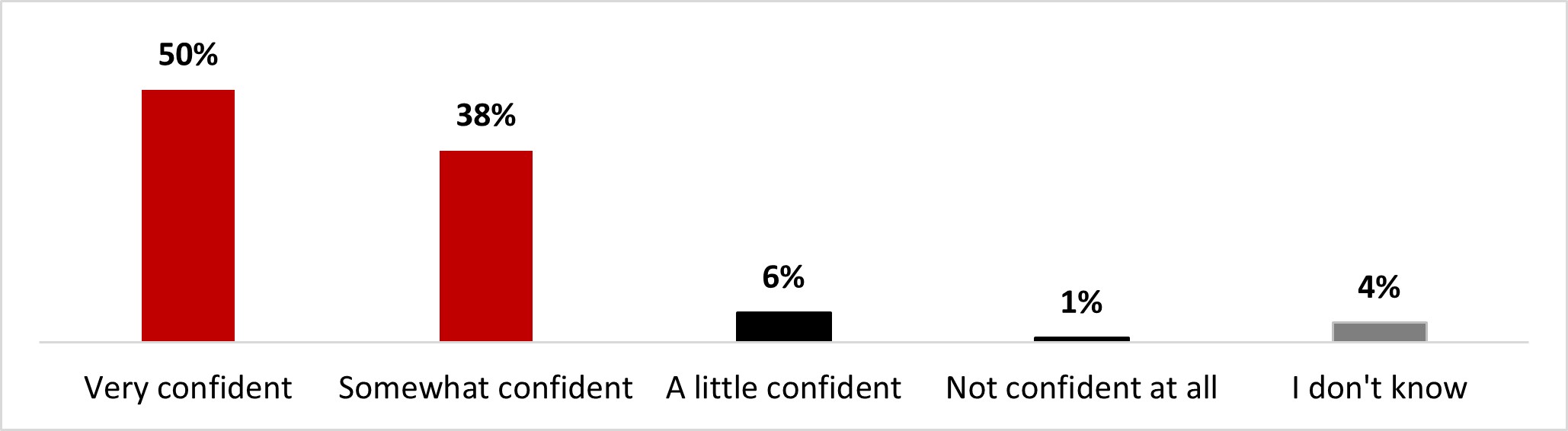
Figure 16.43: Text description
- Very confident
- 50%
- Somewhat confident
- 38%
- A little confident
- 6%
- Not confident at all
- 1%
- I don't know
- 4%
The following subgroups were significantly more likely to state being confident a great deal or somewhat about making their own decisions with respect to choosing to practise IPHM:
- Those over 55 years old (94%)
- Women (90%)
- Those who identify as white (89%)
Clear communication from government and health authorities about when measures should be used (43%), information about the spread of COVID-19 in their community (39%), and information about the spread of other respiratory diseases in their community (38%) were the top three factors that would help respondents in their decisions about using health measures.
Figure 16.44: Which of the following would be useful to help your decision-making about using any or all of the individual public health measures mentioned in the previous question (i.e. wearing a mask etc.)? Select all that apply.
Sample frame: All respondents (n=3,004)
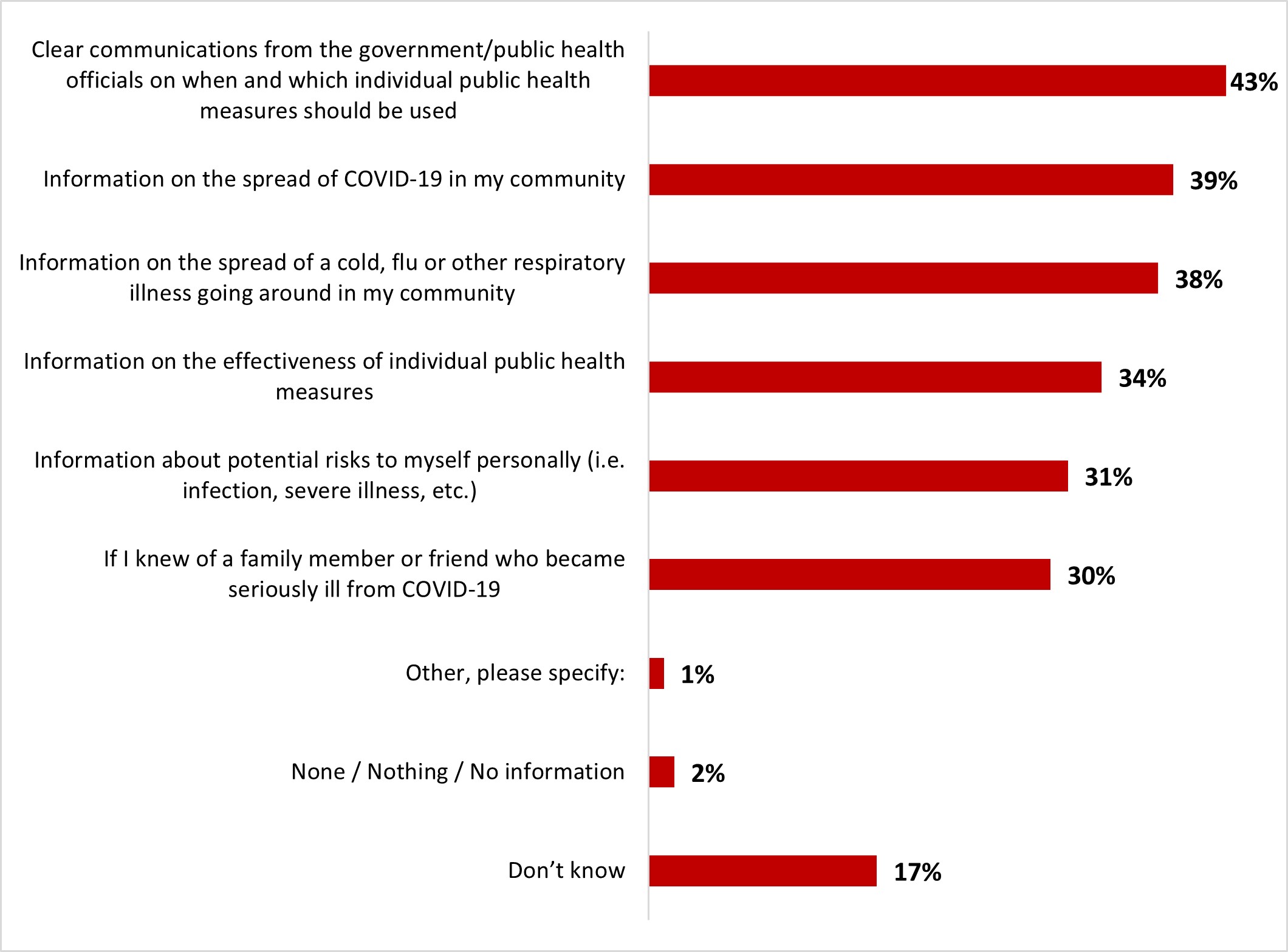
Figure 16.44: Text description
- Don't know
- 17%
- None / Nothing / No information
- 2%
- Other, please specify:
- 1%
- If I knew of a family member or friend who became seriously ill from COVID-19
- 30%
- Information about potential risks to myself personally (i.e. infection, severe illness, etc.)
- 31%
- Information on the effectiveness of individual public health measures
- 34%
- Information on the spread of a cold, flu or other respiratory illness going around in my community
- 38%
- Information on the spread of COVID-19 in my community
- 39%
- Clear communications from the government/public health officials on when and which individual public health measures should be used
- 43%
The following subgroups were significantly more likely to mention almost all the factors:
- Respondents who are over 55 years old
- Parents of children less than 18
- British Columbia and the Territories
Government of Canada websites (49%), conversations with a health care provider (47%) and local/regional health authorities (46%) were the three most preferred sources of information for survey respondents to learn about personal protective measures. Provincial/territorial public health authorities (41%) and provincial/territorial government websites (41%) were the fourth and fifth most preferred sources of information.
Figure 16.45: Where would you go for these types of information? Select all that apply.
Sample frame: Those who answered that some information would be useful to help their decision-making regarding public health measures (n=1,949)
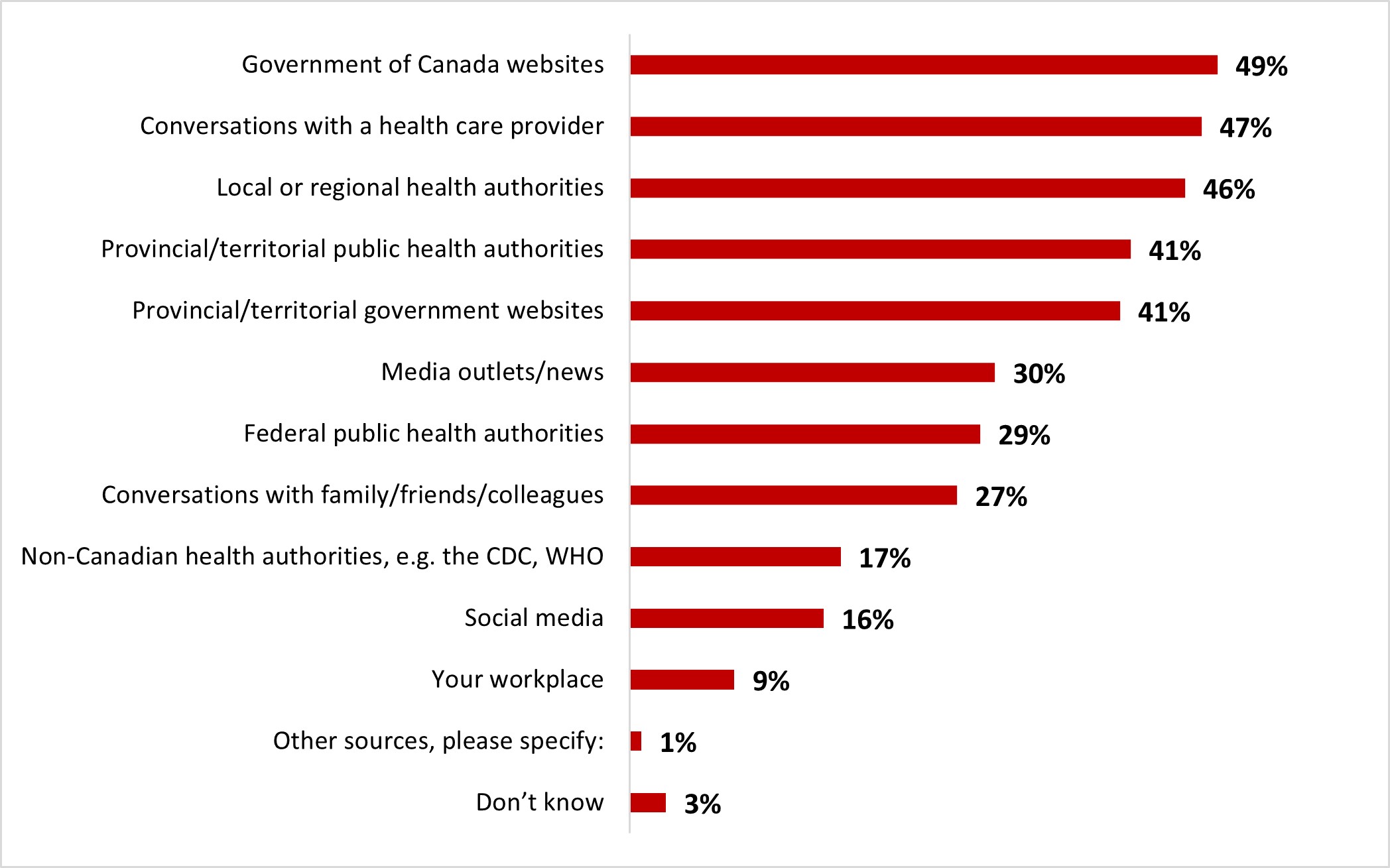
Figure 16.45: Text description
- Don't know
- 3%
- Other sources, please specify:
- 1%
- Your workplace
- 9%
- Social media
- 16%
- Non-Canadian health authorities, e.g. the CDC, WHO
- 17%
- Conversations with family/friends/colleagues
- 27%
- Federal public health authorities
- 29%
- Media outlets/news
- 30%
- Provincial/territorial government websites
- 41%
- Provincial/territorial public health authorities
- 41%
- Local or regional health authorities
- 46%
- Conversations with a health care provider
- 47%
- Government of Canada websites
- 49%
Respondents of 18 to 34 years of age were significantly more likely to mention conversations with:
- Family/friends/colleagues (34%)
- Social media (22%)
- The workplace (12%)
Respondents over 55 years old were significantly more likely to mention conversations with:
- Their health care provider (52%)
- Public health authorities (local/regional: 57%, provincial/territorial: 47%, federal: 33%)
- Media outlets/news (38%)
About three out of ten respondents (30%) indicated that they felt pressure to practise personal protective measures: a lot (6%) and somewhat (24%). One out of five respondents (20%) said they felt little pressure, while nearly half of the respondents (47%) said they felt no pressure at all.
Figure 16.46: To what extent do you feel pressured by others to practice or not practice individual public health measures?
Sample frame: All respondents (n=3,004)
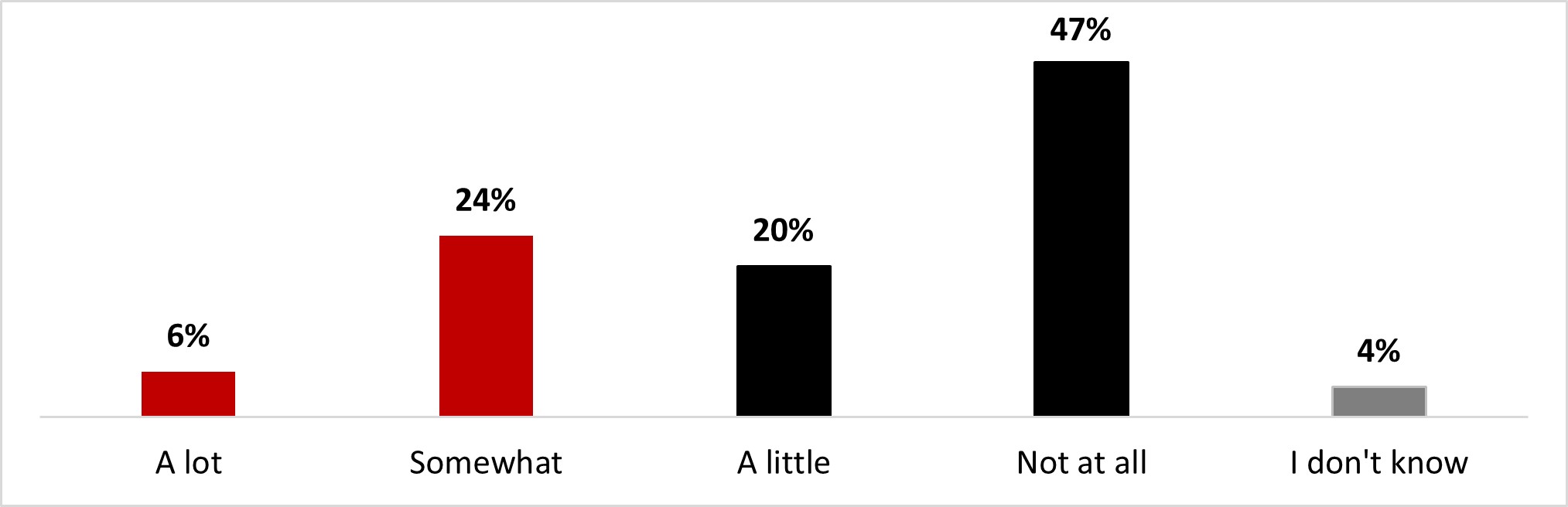
Figure 16.46: Text description
- A lot
- 6%
- Somewhat
- 24%
- A little
- 20%
- Not at all
- 47%
- I don't know
- 4%
The following subgroups were significantly more likely to feel pressured by others to practise or not practice individual public health measures:
- 18 to 34 year-old individuals (42%)
- Parents of children less than 18 (38%)
2.7 Long-COVID
Around two-thirds of respondents mentioned being familiar with long-COVID (65%): around one out of ten stated being very familiar (12%), and over half were somewhat familiar (53%). On the other hand, one out of four was not very familiar (23%), and around 9% were not at all familiar.
Figure 16.47: How familiar are you with the potential long-term effects of having COVID-19 (also known as "long-COVID" or "post COVID-19 condition")?
Sample frame: All respondents (n=3,004)
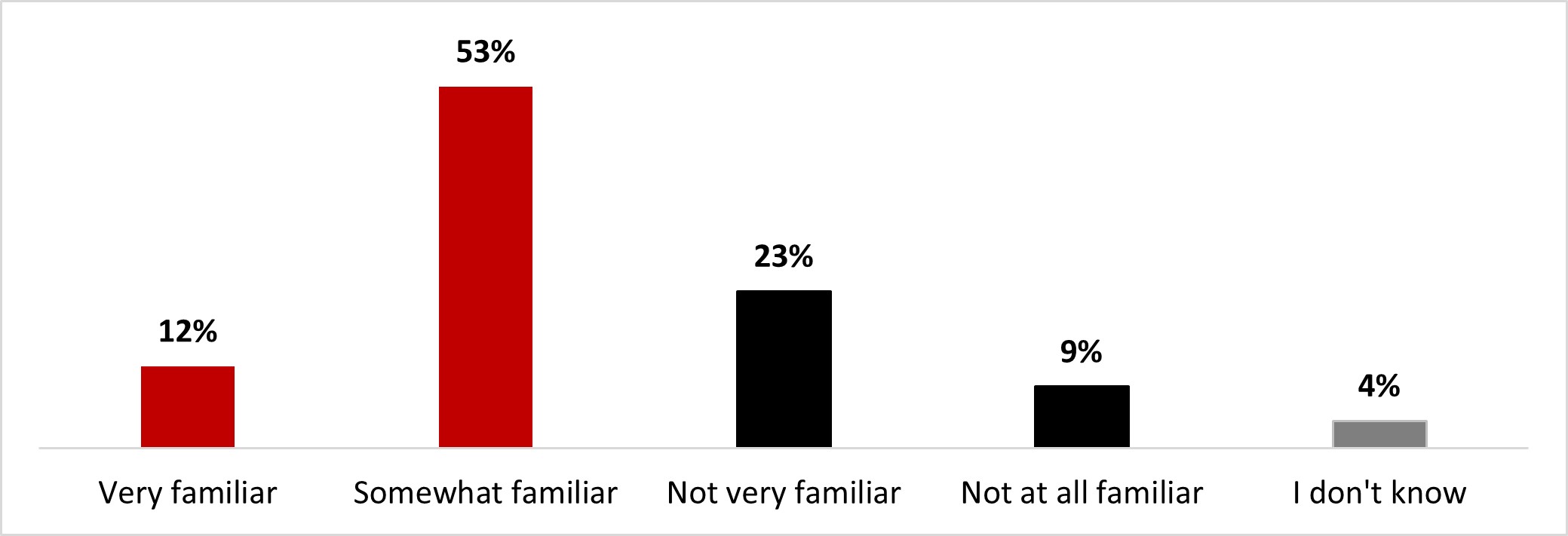
Figure 16.47: Text description
- Very familiar
- 12%
- Somewhat familiar
- 53%
- Not very familiar
- 23%
- Not at all familiar
- 9%
- I don't know
- 4%
The following subgroups were significantly more likely to state being very or somewhat familiar with long-COVID:
- Those with a university degree (70%)
- Ontario residents (69%)
- Those who earn over $80,000 (69%)
Overall, more than half (54%) mentioned being worried about developing long-term symptoms from a COVID-19 infection. More specifically, fewer than one out of five people stated being very worried (17%), while a third were somewhat worried (36%). Around three out of ten respondents were not very worried (28%), and 14% were not at all worried.
Figure 16.48: How worried are you/would you be about developing longer-term symptoms from a COVID-19 infection?
Sample frame: All respondents (n=3,004)
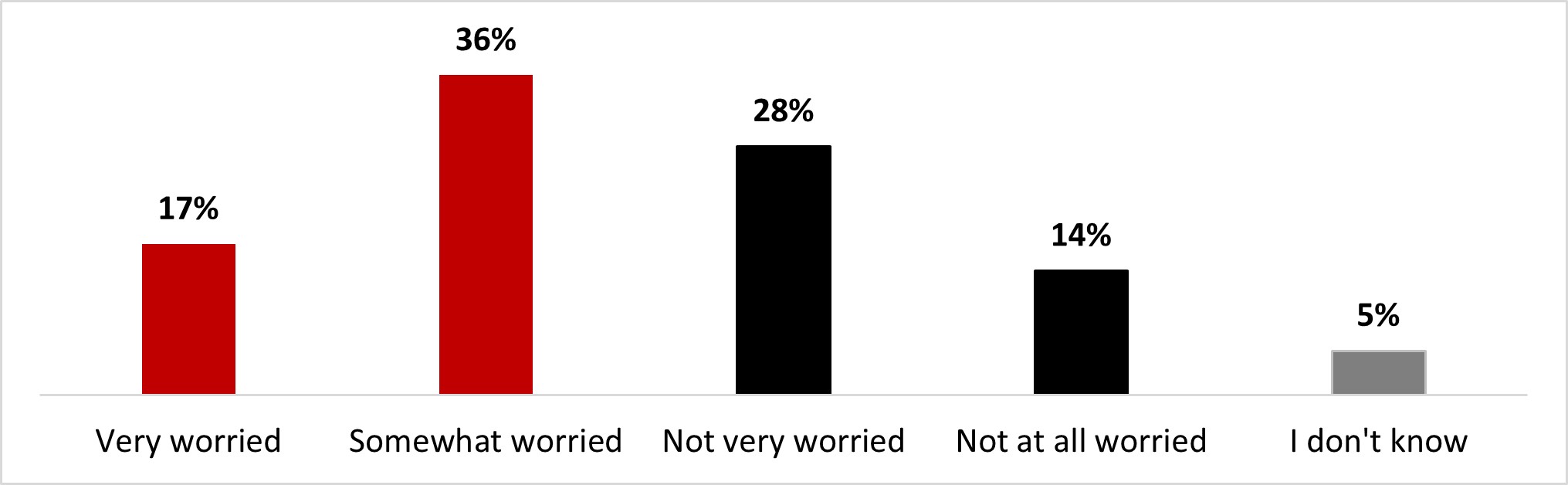
Figure 16.48: Text description
- Very worried
- 17%
- Somewhat worried
- 36%
- Not very worried
- 28%
- Not at all worried
- 14%
- I don't know
- 5%
The following subgroups were significantly more likely to state being worried about developing longer-term symptoms from a COVID-19 infection:
- Residents of British Columbia and the Territories (62%)
- Respondents with a university degree (60%)
- Women (58%)
- Respondents who earn less than $40,000 (58%)
- Respondents over 55 years old (57%)
Uncertainty about future health prospects and limitations to leisure/personal life were the two main reasons for worrying about long-COVID for around two-thirds of respondents (67% and 64%, respectively). A third of respondents were worried about limitations to their working life (34%) and lack of information/resources on the condition (32%). One person out of four was worried about lack of public acknowledgement from authority figures (25%), difficulty in accessing benefits related to the condition (23%), and not knowing if others would take their condition seriously (22%). One person out of five was worried because of difficulty in formally indicating their condition (18%), and around one person out of ten was worried about being judged (11%) or being terminated by their employer (9%).
Figure 16.49: What makes/would make you feel worried about long-term symptoms of COVID? Select all that apply.
Sample frame: Those who are worried about developing longer-term symptoms from COVID-19 (n=1,629)
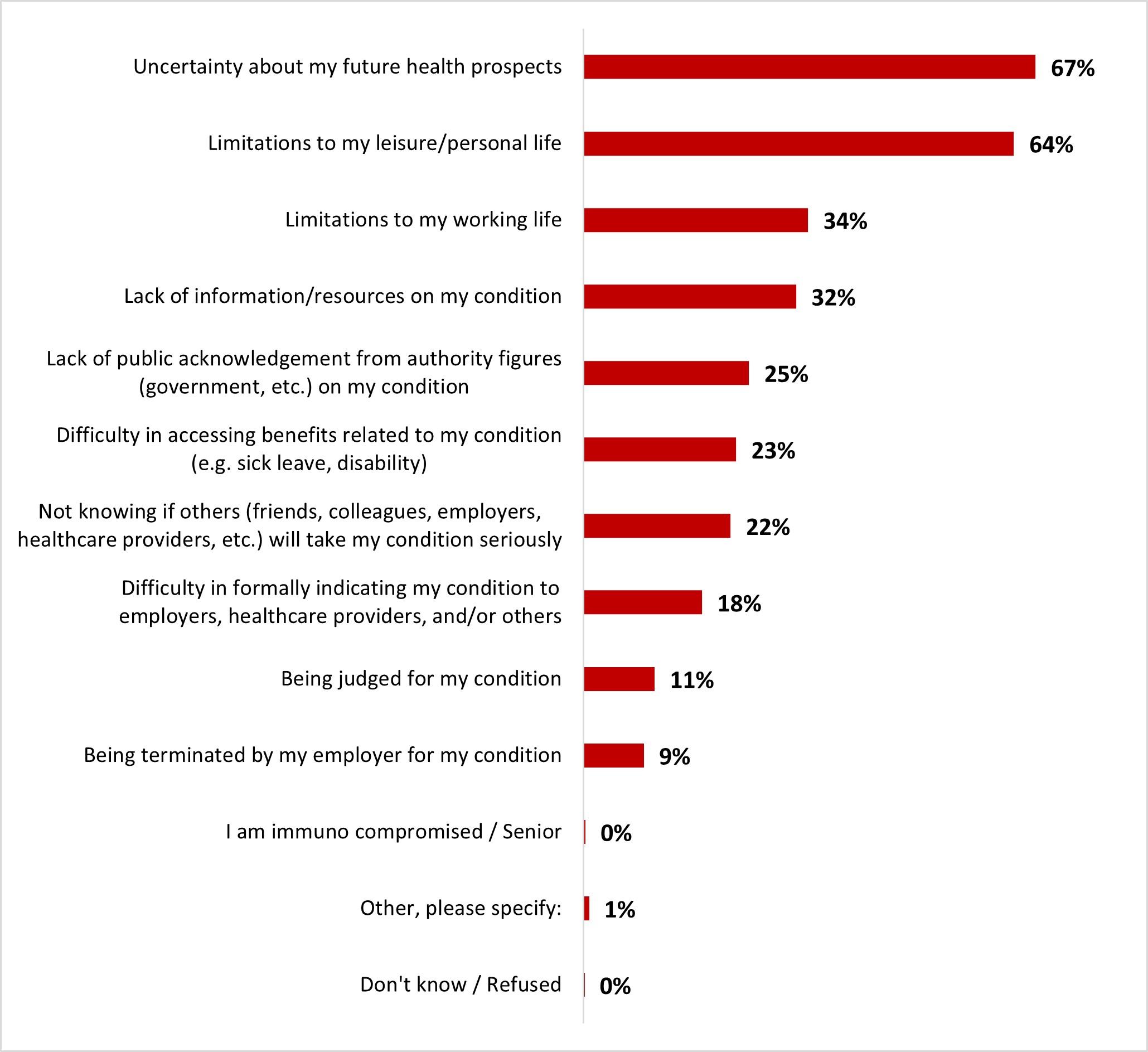
Figure 16.49: Text description
- Don't know / Refused
- 0%
- Other, please specify:
- 1%
- I am immuno compromised / Senior
- 0%
- Being terminated by my employer for my condition
- 9%
- Being judged for my condition
- 11%
- Difficulty in formally indicating my condition to employers, healthcare providers, and/or others
- 18%
- Not knowing if others (friends, colleagues, employers, healthcare providers, etc.) will take my condition seriously
- 22%
- Difficulty in accessing benefits related to my condition (e.g. sick leave, disability)
- 23%
- Lack of public acknowledgement from authority figures (government, etc.) on my condition
- 25%
- Lack of information/resources on my condition
- 32%
- Limitations to my working life
- 34%
- Limitations to my leisure/personal life
- 64%
- Uncertainty about my future health prospects
- 67%
The following subgroups were significantly more likely to feel uncertain about their future health prospects if they got long COVID:
- Residents of Manitoba and Saskatchewan (77%)
- Respondents over 55 years old (74%)
- Women (70%)
- White-identifying individuals (70%),
- Respondents who are not parents (69%)
The following subgroups were significantly more likely to worry about limitations to their working life:
- 35 to 54 year olds (46%)
- 18 to 34 year olds (44%)
- Parents of children less than 18 (44%)
- Black-identifying individuals (43%)
- Respondents who earn over $80,000 (42%)
- Respondents with a university degree (39%)
3. Detailed results for Wave 17
3.1 Concerns about COVID-19
Opinions towards the COVID-19 pandemic and levels of concern varied across the different groups. Some participants expressed ongoing concerns about COVID-19, while others declared having moved on and being less anxious about it. The latter were generally not concerned about the current state of the pandemic. They felt like COVID-19 does not pose much risk to them directly. A majority of participants have contracted COVID-19 once or more, which also informed their concern towards it. Since they felt like the illness was not that bad, they did not express a lot of worry about getting it again. In fact, some participants acknowledged that they are likely to get it again but were at peace with it, and comparisons with a "strong flu" have been drawn. Some also mentioned living their lives "normally", without giving the pandemic and the risk of catching COVID-19 much thought. Considering the advances that have been made during the pandemic in terms of public health measures, vaccines, and knowledge of the virus, participants agreed that things in Canada were in a better place than before, which relieved COVID-related anxiety. While parent and general population groups expressed various opinions, lack of concern with COVID-19 was especially present among young adults participants, who only got their primary vaccines (2 doses).
However, participants were still aware that COVID-19 still existed and mentioned being cautious about not contaminating other people if they were to get COVID-19 themselves, especially those who are immunocompromised or have weaker immune systems such as older individuals: "I'm not too worried because I'm young and healthy, but I am worried about my grandparents" (young adult, 2 doses). Concerns were also expressed by those who worked in a health care setting in contact with patients, as they worked in a setting that they made them at high-risk of catching COVID. Mild anxiety was also mentioned regarding showing mild respiratory symptoms like sneezing or congestion: "Is it COVID or is it just a cold?".
Participants at large considered that we were out of the COVID-19 pandemic but were still very much aware of the impacts of COVID-19 on day-to-day life and various institutions. They acknowledged that COVID did not disappear, and that some of its effects will be present for a long time: physical and cognitive symptoms of long COVID, delayed surgeries in hospitals, negative impacts on mental health, etc.
They also did not seem worried about the upcoming late fall/winter season, but still acknowledged that there would be an increase in all kinds of infectious diseases. Some participants working in hospital or school settings gave the example of the flu or the gastroenteritis as examples of illnesses that have seen an increase in case numbers since the beginning of the school year. Again, across all groups, those in more vulnerable situations expressed more concern.
Across all groups, concerns about COVID-19 came mainly from individuals who were either immunosuppressed themselves or had immunosuppressed individuals in their surroundings; others closely knew people who died from COVID-19. They also expressed their frustration with society at-large being less cautious and preventive towards COVID-19. "I am young and healthy so I will bounce back but 2 of my favorite persons in the world are in grave danger right now. I am angry and sad. People think we have moved on we haven't. I am angry with the fact that people have not been taking more precaution in recent times" (young adult, 2 doses). Others expressed concerns about daily life impacts, like having to share closed spaces with people who are potentially unvaccinated or being able to earn money (this point was brought up by a music performer). While some parents expressed some worry, their main concerns were about the impact of potential school closures on their children's willingness to learn and study as well as the potential long-term effects of a COVID infection.
3.2 Public Health Measures
Masks
Across all groups, a vast majority of participants have mentioned they did not systematically wear masks anymore. They only wore them in certain situations, like to protect a vulnerable person they are in close proximity with, or if they are sick and have to be in public, or to travel (when it was mandatory). Some participants have mentioned they kept wearing the mask on a regular basis if they are in crowded places such as shopping malls or grocery stores. Others mentioned they kept wearing them out of respect and consideration for vulnerable individuals. These opinions were shared across all demographics, with no notable differences. One participant indicated that when mask mandates were removed, their family upgraded to N95 masks in order to be better protected against the virus.
Participants generally agreed that masks are effective to protect against other diseases beside COVID-19. Parents indicated that their children fell sick significantly less often since masks were widely introduced, but none of them obligated their children to wear masks at school since the beginning of the 2022 school year.
Handwashing and sanitizer use
Handwashing and hand sanitizing have become a common habit among participants since the pandemic. A vast majority of them mentioned using them frequently or as often as they could (entering a store, getting home, etc.). These hygienic measures are now performed by force of habit and are seen as common sense. Some participants acknowledged that washing hands with soap and water is more effective than using hand sanitizer.
Ventilation
Participants almost unanimously agreed about the benefits of improved ventilation and its effectiveness at reducing the risk of disease transmission, including, but not limited to COVID-19. However, awareness of ventilation improvement measures was low among participants. While some participants mentioned opening windows in their home more often to improve air circulation, most did not do much to improve air quality in their homes. Regarding other facilities, those working in hospital settings or schools mentioned some measures that have been put in place: air quality testing, opening windows when air quality was bad. However, opening windows is one of the only improvements that have been brought up, and one participant who worked as a teacher complained that they had to keep them open even during winter. Some participants, both parents and teachers, denounced the lack of efforts put in place to improve in-school ventilation. One participant working as a musician mentioned the theater, they perform at made efforts to improve air circulation and had a strong communication campaign towards audiences in order to reassure them and draw them back to cultural venues after the pandemic. One other participant considered that improving ventilation in public buildings was unrealistic. They mentioned that masks were the most efficient alternative - cost and availability-wise.
Parents
Regarding measures to keep children safe, most parents mentioned keeping their children at home if they showed symptoms of illness, and not just COVID-19: fever, runny nose, congestion were mentioned as examples of symptoms to watch for. One participant mentioned keeping their children home a few days after the symptoms disappear to avoid contagion. Parents also brought up being more wary of sanitizing their kids' objects and toys and cleaning their house more often. And while they encouraged their children to be cautious when at school by trying to keep their distance from other children, they recognized it was hard to make sure they actually did.
3.3 Influence of a COVID-19 Infection
A majority of participants contracted COVID-19 at least once, and some had it twice. Some participants mentioned they contracted it during the first waves before vaccine rollout, and others after the initial vaccination campaign. Participants got tested in most cases, either by
PCR or rapid tests. One participant mentioned not getting tested themselves since they had symptoms and their son, who lives in the same household, tested positive, making it certain to them that they were positive as well.
Participants who had contracted COVID-19 mentioned three types of impacts of their infection on vaccination intentions: neutral, positive and negative. It is to be noted that there were no relevant demographic differences in opinions between groups. Those who were already planning on getting boosted reported not being influenced by their COVID-19 infection whatsoever. Three types of positive influence of COVID infection on booster vaccination intention were uncovered. First, a few participants stated that the severity of symptoms convinced them to get their first or second booster dose as to reduce the gravity of symptoms for a potential other infection. Others mentioned that they did not feel any strong symptoms when they were sick with COVID-19, which they took as a sign that the vaccine was effective, therefore confirming their willingness to get boosted. One participant mentioned realizing they were immunocompromised during their first COVID-19 infection, which strongly prompted them to get themselves and their family vaccinated with as many doses as available.
Neutral and negative influences of COVID-19 infection on the intention to get a booster shot were in the minority among participants. Among those who stated that their COVID-19 infection had a neutral or negative impact, some mentioned that it was unnecessary to get a booster since they got infected even though they were vaccinated, others felt that the symptoms they felt were not strong enough to actually incentivize them to get their booster shots, and others mentioned they felt stronger symptoms after getting vaccinated than with the actual COVID-19 infection, which also had a deterring effect. A few participants even mentioned that in hindsight, they might have chosen not to get vaccinated altogether if they were given the option.
3.4 Vaccines
Attitudes towards booster doses
The understanding of the expression "staying up to date" ("rester à jour" in French) with COVID-19 vaccines was different from one participant to other, but the most common definition was getting the latest booster dose available. Others thought it meant having received the number of vaccines and/or boosters that allows one to take part in activities such as going out and travelling, i.e., two doses. Personal beliefs and opinions had a strong influence on the definition of the expression. Those who had gotten booster doses were more likely to include the boosters in their understanding of the expression, and the opposite was true for those who only got their primary doses. Participants from Quebec and New Brunswick were more likely to make negative associations with the expression, as they felt it would be an "endless cycle" of vaccination. On the other hand, a few participants were very pro-vaccine and were set on getting vaccinated with all booster doses available to them. Some other participants considered that the booster doses every few months were not necessary and that having one booster dose is enough: "The first dose is enough. Like the flu shot every year, it's an added expense for the government and an annoyance to people. It's not like we're newborns" (general population group participant, 3 doses or more). Even though some participants across all groups showed some level of hesitancy or reluctancy and mentioned that booster doses may not be necessary, this opinion was particularly strong among young adult groups: "[I got COVID] and it wasn't bad enough to make me want to take another shot" (young adult, 2 doses).
Confidence in COVID-19 vaccines and boosters and perception of their effectiveness is informed by anecdotal stories and hearsay about the experiences of peers with COVID-19: a few participants mentioned that some of the vaccinated people they knew had to be hospitalized after getting infected with COVID-19, and other unvaccinated individuals did not get any severe symptoms after infection.
Parent confidence in child vaccination
A majority of parents agreed that "staying up to date" with their children's COVID-19 vaccination means getting them all the doses available to them as recommended by public health guidelines. While some parents trusted public health authorities in recommending what is best for their children and acknowledged the importance of being vaccinated and staying up to date, others were more dubious about vaccine effectiveness on children and deplored the lack of studies done on children. Potential pervasive long-term impacts of vaccination on their children were a source of worry, that led some parents to adopt a "wait and see" approach, until they get new reliable information on the subject. Some elements were mentioned as examples of motivators to get their children vaccinated: having clear and updated information from trusted government or public health authorities, having recommendations from their health care professionals, and knowing how the vaccine works and how much protection it precisely gives.
Attitudes towards the bivalent vaccine
A majority of participants had not heard of the bivalent vaccine before the focus group sessions. Some individuals were able to understand what the expression meant intuitively. Intentions to get a booster dose remained unchanged, as participants agreed that new variants of the COVID-19 virus might appear, which would render the bivalent vaccine less appealing as new adapted boosters would be developed: "Since there are constantly new variants, it doesn't reassure me much that there is a bivalent vaccine now. I'm not looking to get COVID-19 another time but at this point, I'm not scared of getting it again" (young adult, 2 doses). While some participants were convinced of the importance of getting boosted, others mentioned they would only get the booster if it were mandatory for travel or other types of activities and the fact that a bivalent booster is now available had no influence on their decision. A few participants raised concerns about the potential side effects of a bivalent vaccine. While they were considered a significant constraint by some, others accepted them: "I'm in favor of vaccination, but I'm aware of the risk. It's a risk we're willing to take, versus the potential downside of having bad symptoms from covid infection" (general population, 3 doses or more).
3.5 Mental Health
Factors impacting mental health
When prompted about what was negatively impacting their mental health, participants mentioned financial issues first: rising cost of living, inflation, and anxiety about making a livelihood were mentioned by several people. Participants stated being anxious about their current and future financial situation. Some elements related to the COVID-19 pandemic were also mentioned as stress factors for some participants notably the transition back to in-person activities and work. Some participants also mentioned feeling anxiety whenever they showed symptoms that are similar to those of COVID-19: congestion, cough, fever; leading them to wonder whether or not they had COVID-19.
The social isolation that was imposed as a public health measure during the first few waves of the pandemic was also mentioned by a majority of participants as a strongly impactful factor that deteriorated their mental health. A few participants also mentioned the negative impacts of living alone. Now that the restrictions have been lifted, all participants agree that their mental health has improved.
Some participants touched on other mental health impacts that public health measures have had on themselves: anxiety over surveillance by public authorities and over not being able to leave the house. Some participants mentioned feeling a deep sense of guilt when they contracted COVID-19, as the infection was seen as a failure on their part to comply with public health or to keep themselves and their surroundings safe. News coverage of the COVID-19 pandemic, more specifically death tolls and infection numbers, was also perceived as anxiogenic by a few participants.
A participant mentioned that the negative impacts of the pandemic on their mental health led them to get their prescription readjusted accordingly. They acknowledged how expensive and how inaccessible it can be to have access to therapy or mental health services in general.
Parent specific concerns
While parents mentioned some general elements like inflation as stress factors, they also had specific concerns relating to their children and their schooling. They sometimes felt overwhelmed having to handle their children's at-home schooling and their own workload. Some parents criticized online schooling as it could reduce their children's motivation to study and stay on top of their homework and lessons, but others on the other hand worried about sending their children back to in-person schooling. This anxiety mainly stemmed from the fact that it was difficult for them to ensure their children adopted preventive measures to avoid infection such as keeping their distance. One parent said the divisiveness that ensued from the pandemic and public health measures had a negative impact on themselves and their children.
Access to mental health support and obstacles
No participant mentioned getting mental health support specifically because of COVID-19 impacts. Some participants were already getting help with their mental health (through therapy mainly), and they mentioned addressing COVID-19 issues and how it impacted them with their therapist or mental health specialist.
All participants reached a consensus on the difficulty of accessing mental health support. Availability, cost, and stigma were the three main obstacles that have been uncovered by the discussion. Participants deplored the lack of resources and availability in the public system, as wait times were prohibitively long and did not allow to address current worries and get immediate care, and some felt left to their own devices: "I asked my doctor, but they said it would take years to see a psychologist, and that for a councillor, I'd have to look for myself". Some participants also mentioned they would feel guilty to seek help and put more strain on the public health system when other people might be needing it more.
They also mentioned the high cost of therapy sessions as an obstacle to get access to mental health support. Those who could afford therapy or had insurances to cover their cost felt lucky and acknowledged their privilege over the majority of individuals that could not afford it.
Stigma was the third obstacle to getting appropriate mental health support in several cases. While it was seen as a cultural phenomenon by some, others perceived it as a generational issue, and others as a generalized issue. "In Jamaica, it is frowned upon to get mental health care: the biggest obstacle was my family. […] It is viewed as something only critically insane people need, not those who suffer from anxiety or depression. I had to step out of my comfort zone."
In addition to that, participants also recognized that it was not as easy finding a mental health professional as a physical health professional, as approaches vary and finding the right fit with a mental health professional is key to the efficiency of the therapy and the smooth running of the care the patient receives.
Online resources
Awareness of online mental health services among participants was quite low, as most were not able to name one. However, some were aware of a wider online service offering since the pandemic, for both mental and physical health support. Those who knew specific services mentioned Headspace and Betterhelp, and Tel-Aide in the province of Quebec. Overall, participants agreed that the availability of such services as a complement to other in-person services, especially during the pandemic, was beneficial. However, they also highlighted the difficulty of establishing a relationship with a therapist online, compared to in-person. Trust is a key component of a therapist-patient relationship, and participants considered it would be harder to build trust online. Some participants wondered about the efficacy of such alternative mental health resources and would have liked to see more research done on the matter to assess their quality.
Some participants stated that even if said services were recommended to them, they still would not use them. Difficulty building trust and finding the right kind of help for oneself were the main obstacles. Participants also seemed dubious about the recommendation of such services and questioned its legitimacy: "Is it recommended because it is the only service available or is it recommended because it has been evaluated and is in fact a good service?". However, most participants agreed that they would feel comfortable turning to these types of resources if they were recommended to them by a trusted source. The definitions of a trusted source varied, with some mentioning the government and public health institutions, and others mentioning their medical practitioner, or their peers (friends, family, colleagues).
Desired resources
Participants all agreed about the fact that government-backed online mental health services would greatly increase their perceived legitimacy and would increase the chances of considering turning to online resources. They expected to have exhaustive information on the online mental health services available. Participants agreed that the more information available the better, as mental health is seen as highly personal. Having several types of resources listed increases the chances of each and everyone finding the right resource for them and their issue. Specific situations and types of mental health resources that participants would like to have information about include:
- Sector-specific mental health issues: for instance, anxiety and depression among healthcare or education workers.
- Resources for children and how to accompany them, especially in isolation times.
- Methods on how to manage anxiety and depression
- How to handle suicidal thoughts
- How to access counselling with short waitlists
- Reliable online mental health website that offers live chatting with mental health professionals
3.6 Message Testing
General population message testing
Message 1
-
Restez à jour avec vos vaccins contre la COVID-19 afin de vous protéger contre les conséquences graves liés à la maladie. Obtenez toutes les doses de rappel qui sont recommandées pour vous.
Restez à jour avec vos vaccins contre la COVID-19 afin de vous protéger contre les conséquences graves liés à la maladie. Obtenez toutes les doses de rappel qui sont recommandées pour vous.
- Stay up to date with your COVID-19 vaccines to help protect against severe outcomes. Get all vaccine doses recommended for you.
Restez à jour avec vos vaccins contre la COVID-19 afin de vous protéger contre les conséquences graves liés à la maladie. Obtenez toutes les doses de vaccins qui sont recommandées pour vous.
The second version of this message using "vaccine doses" (doses de vaccins in French) rather than "booster doses" (doses de rappel in French) was preferred by a majority of participants. The term "booster doses" had negative connotations among participants. Some mentioned the use of "booster doses" seemed to imply that the first two doses were not effective, and others mentioned that the term "booster" evokes an "endless cycle" of getting booster vaccines. Other reasons for preferring this statement revolved around inclusivity of unvaccinated individuals: some participants considered that they should be the main focus of the message, rather than people who have received their first two doses and maybe a booster. One participant mentioned that the term "protect" should be replaced with "reduce", as total protection against severe outcomes is impossible. On the other hand, those who preferred the first version of the statement ("booster doses") felt did so because the message felt clearer and more precise.
In order to improve the message and make it more appealing, suggestions included a combination of both statements that mentioned explicitly booster and vaccine doses; and mentioning the community and human aspects of vaccination in order to motivate people more (e.g., "Vaccines protect families"). Some other participants however, declared they stopped paying attention to this type of messaging altogether after being overexposed to similar statements throughout the past two pandemic years.
Message 2
-
When talking about COVID-19 vaccination, do you know what the term "Primary Series" means?
En pensant à la vaccination contre la COVID-19 que pensez-vous que le terme, "série primaire" signifie?
A vast majority of participants had not heard of the term "primary series" (série primaire in French) before. While some were able to understand it contextually, comprehension was left to assumption. While some assumed it referred to the first two doses, others included the first booster as well. One participant who knew the meaning of the term stated that it made them feel more knowledgeable about vaccines in general.
Participants felt the use of the term "primary series" was unnecessarily complicated – some described it as "too academic", and that it would not be understood by a majority. Suggestions to replace the term included "first and second doses" or "primary doses".
Message 3
-
Consult your local health care resources, or provincial or territorial public health authority to find out when you're due for your next COVID-19 vaccine dose.
Consultez votre service de santé publique local ou votre bureau de santé publique provinciale ou territoriale pour savoir quand vous devriez recevoir votre prochaine dose de vaccin contre la COVID-19.
-
Check with your province or territory to find out when you're due for your next COVID-19 vaccine dose.
Vérifiez auprès de votre province ou territoire pour savoir quand vous devriez recevoir votre prochaine dose de vaccin contre la COVID-19.
Preferences between the two versions of this message were divided but leaned towards the message D. It was seen as more reassuring because of the mention of public health. Participants also liked the term "consult" better than "check", as it evoked more of an interaction and advice from a healthcare professional. The term "check" was seen as somewhat more dismissive and was interpreted as "verify". Those who preferred statement D considered statement E to be confusing and unclear because of the lack of a precise reference to turn to ("province or territory" was too vague), hence considering it dismissive or "snarky". On the other hand, those who preferred statement E considered it to be "short and more direct".
Suggestions to improve the message was to combine both the statements in order to include both health care authorities and government, and many others suggested adding a specific website to refer to.
Parent-specific message testing
Message 1
Vaccinating children against COVID-19 is beneficial for their health and well-being. Research shows that vaccinating children with a COVID-19 vaccine provides very good protection against serious illness, hospitalization and death from COVID-19.
La vaccination des enfants contre la COVID-19 est bénéfique pour leur santé et leur bien-être. Les recherches indiquent que la vaccination des enfants avec un vaccin contre la COVID-19 offre une très bonne protection contre les maladies graves, les hospitalisations et les décès attribuables à la COVID-19.
Opinions about this statement were torn. Francophone parents were not convinced by the message, while Anglophone parents appreciated it.
Francophone participants did not feel the message was convincing nor reassuring. Their perception was that severe illness, hospitalization, and death, as mentioned in the statement, are very rare among children to begin with. Similar to comments made in previous waves of the qualitative study (edition 2), Francophone participants did not understand the phrase "contre les maladies graves" (against serious illness in English) as it seemed to include other illnesses unrelated to COVID-19, causing confusion. To make the message more appreciated, they suggested adding a source for credibility.
Conversely, Anglophone participants appreciated this first statement. They considered it to be clear, straight to the point, and credible. One participant stated that being a parent, they felt drawn to the words "serious illness", "hospitalization" and "death", as they caught their attention. To further improve the message, participants suggested adding more details or data to the message: efficacy levels, an age range, or a graph.
Message 2
While most children who get COVID-19 experience mild or no symptoms, some, including previously healthy children, can experience severe disease and require hospitalization. Fortunately, severe COVID-19 outcomes, including hospitalization, are lower in children who are vaccinated against COVID-19.
Bien que la plupart des enfants qui contractent la COVID-19 présentent des symptômes légers ou ne présentent aucun symptôme, certains, dont des enfants auparavant en bonne santé, peuvent développer une maladie grave et devoir être hospitalisés. Heureusement, les complications sévères de la COVID-19, y compris les hospitalisations, sont plus faibles chez les enfants qui sont vaccinés contre la COVID-19.
This message was more appreciated than the first one by Francophone respondents, although they had improvement suggestions and were still not very receptive. Parents accused this message of fearmongering, which made them less receptive. They would have liked numbers or mention of a study. Parents felt they should be given concrete reasons to get their child or children vaccinated.
Anglophone participants did not dislike the message, but also had suggestions. Adding statistics or numbers was mentioned again. One participant would have liked the message to mention the proportion of vaccinated and unvaccinated children with COVID-19 related hospitalizations, and another suggested to add information about the age range to have a precise idea about who is included in the message.
Message 3
Even if a child has already had COVID-19, vaccination is still important. While infection alone provides some protection, vaccination combined with infection helps improve the immune response. Studies in adults show that vaccination following infection provides stronger and longer-lasting protection.
Même si un enfant a déjà contracté la COVID-19, la vaccination demeure importante. Bien que l'infection procure à elle seule une certaine protection, la vaccination combinée à l'infection aide à améliorer la réponse immunitaire. Des études effectuées chez les adultes montrent que la vaccination après une infection offre une protection plus solide et plus durable.
This message was much more appreciated by Francophone parents, who considered it to be more positive, and less harsh towards parents. Participants however considered that mentioning studies in adults rather than children gave the impression that no studies were done on children, making the message less credible.
Anglophones liked the message for its clarity and straightforwardness. Again, adding more concrete details was suggested. Participants mentioned dosage or the type of vaccine needed for children specifically. One participant suggested changing the word "important" for "vital", in order to make it more impactful.
4. Detailed results for Wave 18
4.1 COVID-19 infection
Respondents were questioned about whether they had ever been infected with COVID-19. More than four out of ten (43%) said they had been infected with the virus, while around 7% believed they had been infected but had not been properly tested. As a result, half of the respondents (50%) have been or believe they have been infected with COVID-19. Less than half of the respondents (46%) responded that they had never been infected.
Figure 18.1: Have you ever been infected with COVID-19?
Sample frame: All respondents (n=3,026)
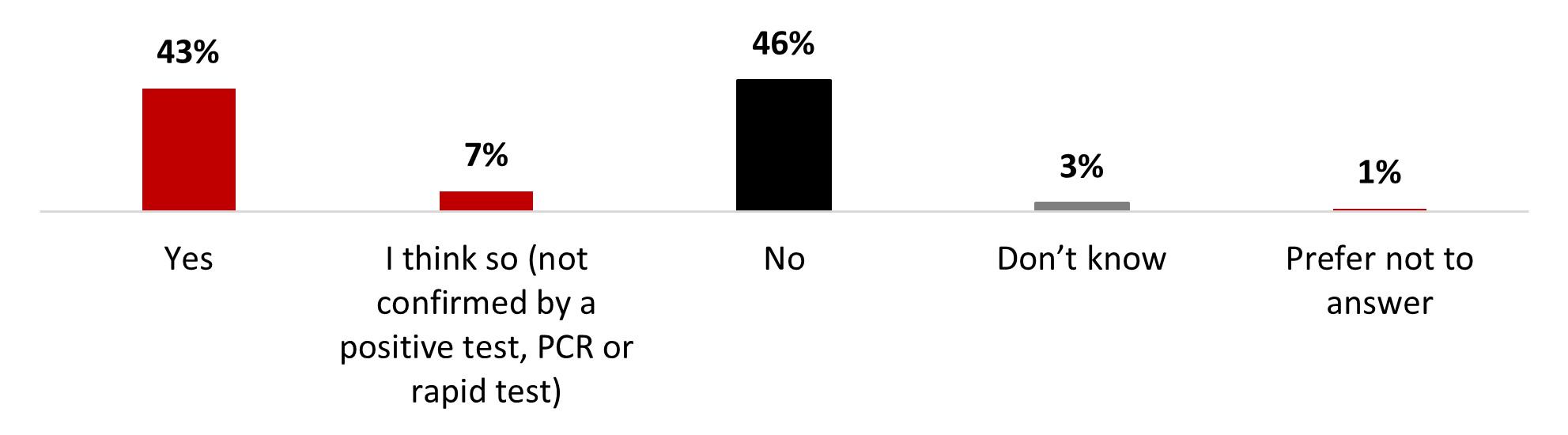
Figure 18.1: Text description
- Yes
- 43%
- I think so (not confirmed by a positive test, PCR or rapid test)
- 7%
- No
- 46%
- Don't know
- 3%
- Prefer not to answer
- 1%
A significantly higher proportion of the following subgroups of respondents indicated they had been infected with COVID-19:
- 18-34 year-olds (51%) and 35-54 year-olds (47%)
- Parents of children younger than 18 years old (55%)
- Individuals who earn between $40,000-$80,000 (47%) and those who earn over $80,000 (49%)
Respondents were also questioned about COVID-19 infections in their immediate social network (i.e., family, friends, etc.). A strong majority of respondents (87%) indicated they knew someone in their immediate network who had been infected with COVID-19, and an additional 1% of respondents indicated they believed they knew someone who had been infected without being able to confirm this. One out of ten respondents (10%) were convinced they did not know anyone close to them who had been infected.
Figure 18.2: Do you know people in your immediate social network (i.e., friends or close family members) who have been infected with COVID-19?
Sample frame: All respondents (n=3,026)
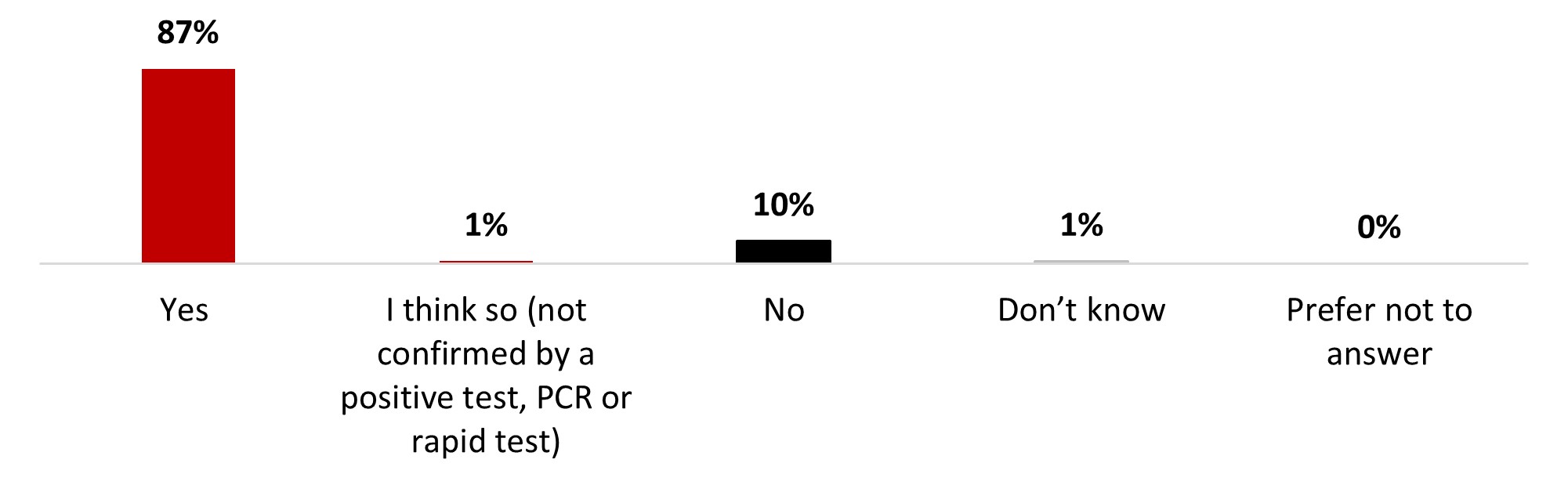
Figure 18.2: Text description
- Yes
- 87%
- I think so (not confirmed by a positive test, PCR or rapid test)
- 1%
- No
- 10%
- Don't know
- 1%
- Prefer not to answer
- 0%
Almost all those infected knew someone in their immediate network who has also been infected (97%). Other subgroups that were significantly more likely to know people who were infected include:
- Individuals who earn over $80,000 (92%)
- Women (90%)
- Respondents from the province of Quebec (90%)
- Those who have been infected with COVID-19 (96%)
- White-identifying individuals (89%)
Over one-third of respondents (36%) identified themselves as being at risk of complications or severe consequences if they contracted COVID-19 because of their specific medical condition or because of having a chronic disease. More than half of the respondents (53%) reported that they were not at risk, while 11% were unsure.
Figure 18.3: Do you consider yourself to be at risk of more severe disease or outcomes from COVID-19 (e.g., are an older adult over the age of 60, are pregnant, have Down syndrome, have a chronic medical condition, are immunocompromised, or live with obesity, etc.)?
Sample frame: All respondents (n=3,026)
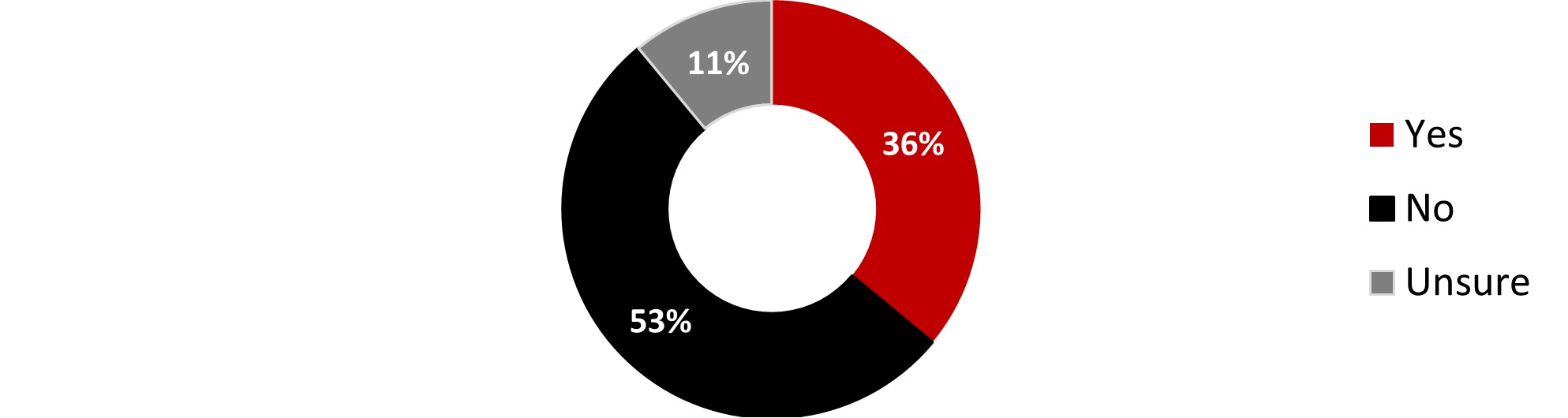
Figure 18.3: Text description
- Yes
- 36%
- No
- 53%
- Unsure
- 11%
The following subgroups were significantly more likely to consider themselves at risk:
- Respondents over 55 years old (58%)
- Respondents who earn less than $40,000 (43%)
- Individuals who are not parents of children younger than 18 years old (40%)
- Those who have never gotten COVID-19 (39%)
- Respondents who identify themselves as white (39%)
Respondents were asked about their level of worry about getting infected with COVID-19. Overall, three people out of four were worried: either very (12%), somewhat (30%), or a little (33%). On the other hand, one person out of four states not being worried at all (24%).
Figure 18.4: How worried are you of becoming infected with COVID-19?
Sample frame: All respondents (n=3,026)
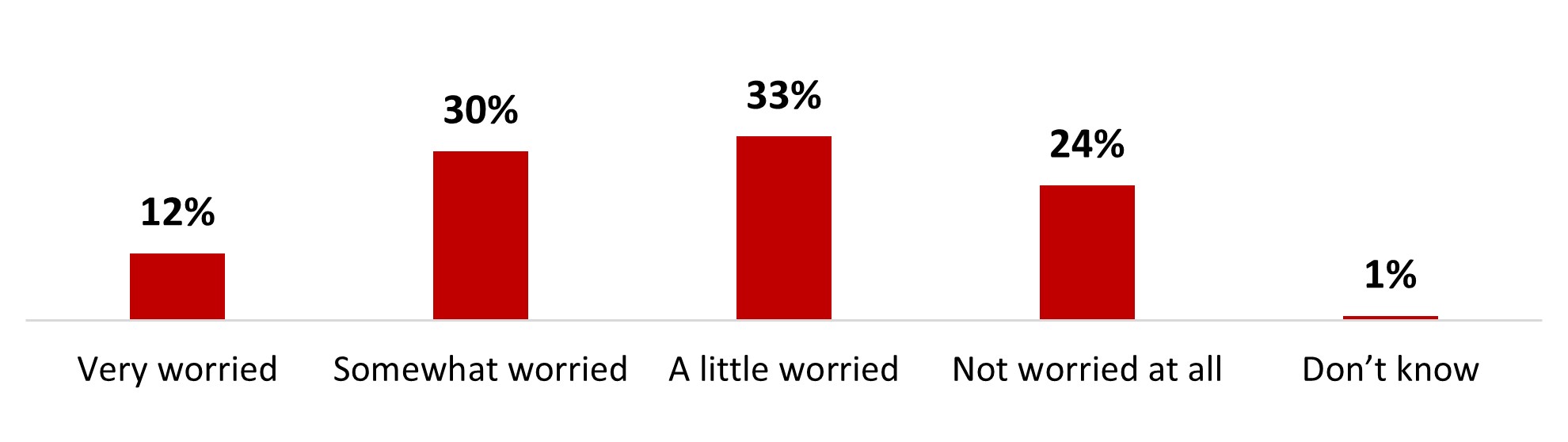
Figure 18.4: Text description
- Very worried
- 12%
- Somewhat worried
- 30%
- A little worried
- 33%
- Not worried at all
- 24%
- Don't know
- 1%
While those over 55 years old were significantly more likely to state being somewhat worried (34%), those aged between 35 and 54 years old were more likely to not be worried at all (29%). Ontario has a significantly higher proportion of respondents at the two ends of the scale: a higher proportion of Ontarians were very (14%) or not at all (27%) worried.
Those who were not worried about becoming infected with COVID-19 mentioned a variety of reasons to justify their position: believing that symptoms would be mild because of the vaccine (32%), that COVID-19 is here to stay (28%) and having contracted COVID-19 previously and not been really sick (28%) were the top three reasons. Around one person out of four mentioned having other more important concerns (26%) and that COVID-19 is just another flu (24%). One out of five mentioned they are not worried because they now know what to expect following a previous infection (20%). Lack of concern with new variants (16%), believing one is immune because of vaccination (11%), that COVID-19 is not very dangerous (11%), and the fact there are low levels of COVID-19 in the community (10%) were all mentioned by around one person out of ten. Other reasons were mentioned by a minority of respondents.
Figure 18.5: Why are you not worried about becoming infected with COVID-19? Select all that apply.
Sample frame: Respondents who are not worried at all about becoming infected with COVID-19 or are unsure (n=750)
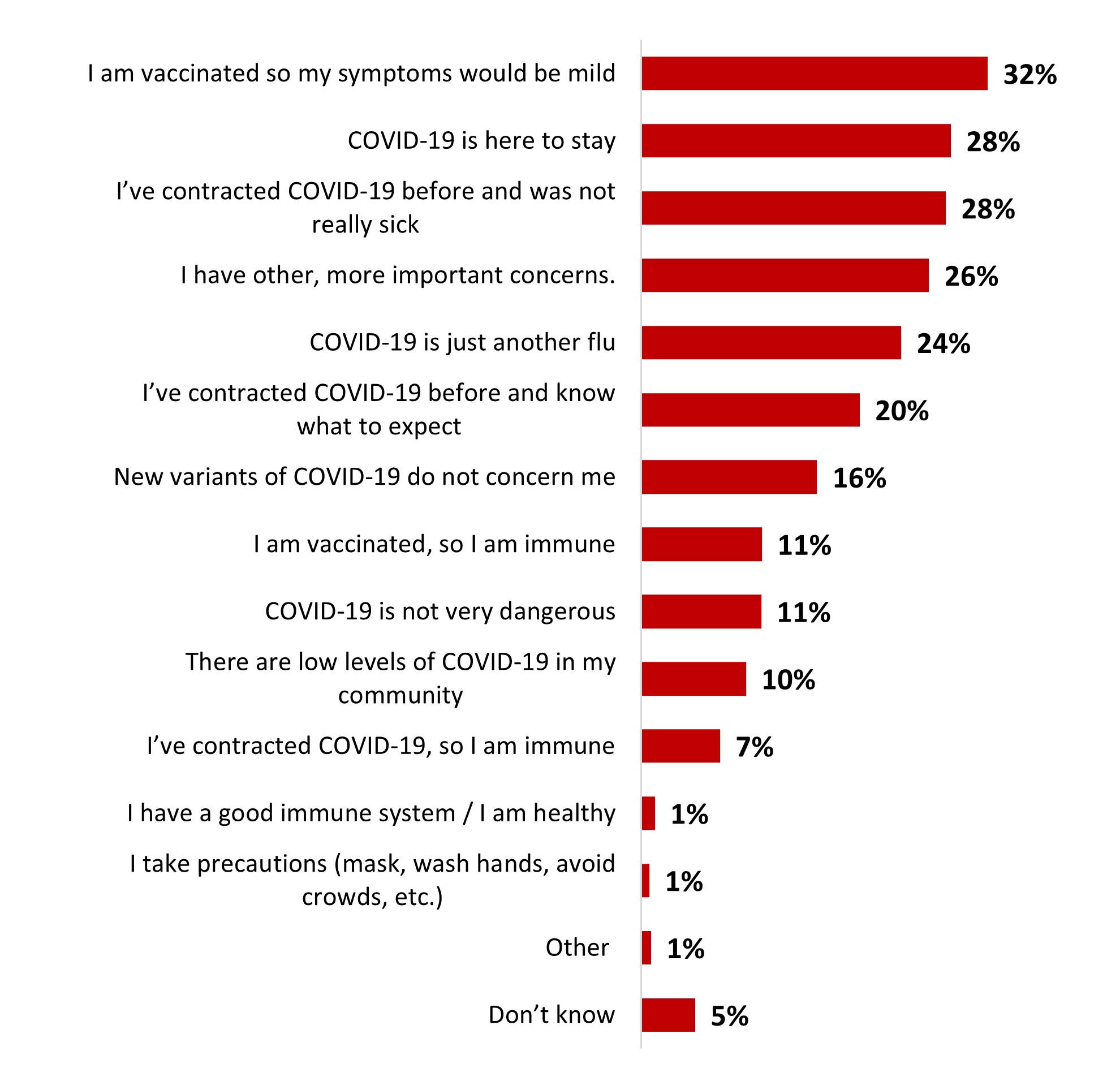
Figure 18.5: Text description
- I am vaccinated so my symptoms would be mild
- 32%
- COVID-19 is here to stay
- 28%
- I've contracted COVID-19 before and was not really sick
- 28%
- I have other, more important concerns.
- 26%
- COVID-19 is just another flu
- 24%
- I've contracted COVID-19 before and know what to expect
- 20%
- New variants of COVID-19 do not concern me
- 16%
- I am vaccinated, so I am immune
- 11%
- COVID-19 is not very dangerous
- 11%
- There are low levels of COVID-19 in my community
- 10%
- I've contracted COVID-19, so I am immune
- 7%
- I have a good immune system / I am healthy
- 1%
- I take precautions (mask, wash hands, avoid crowds, etc.)
- 1%
- Other
- 1%
- Don't know
- 5%
Significant differences regarding reasons to not worry about catching COVID-19 include the following:
- While 18-34 year-olds were significantly more likely to mention having contracted the disease before and not having been sick (35%), those over 55 years old were more likely to justify their lack of worry by their vaccination: either because they believe the symptoms would be mild (42%), or because they believe they are immune (21%).
- Parents of children younger than 18 years old were more likely to mention they were not very sick after having contracted COVID-19 before (34%), while those who were not parents of children younger than 18 years old were more likely to believe they were immune because of vaccination (13%), that the symptoms would be mild because of vaccination (36%), and to mention there are low levels of COVID-19 in their community (12%).
Around half of those who were worried about catching COVID-19 said they were worried about getting others sick (50%), getting significant complications (49%), or getting really sick (48%). One-third mentioned being worried about new variants (36%), and one out of five mentioned being worried an infection would impact their plans (22%) or their work (21%). One person out of ten mentioned having been really sick after a previous COVID-19 infection (11%).
Figure 18.6: Why are you worried about becoming infected with COVID-19? Select all that apply.
Sample frame: Respondents who are worried about becoming infected with COVID-19 (n=2,276)
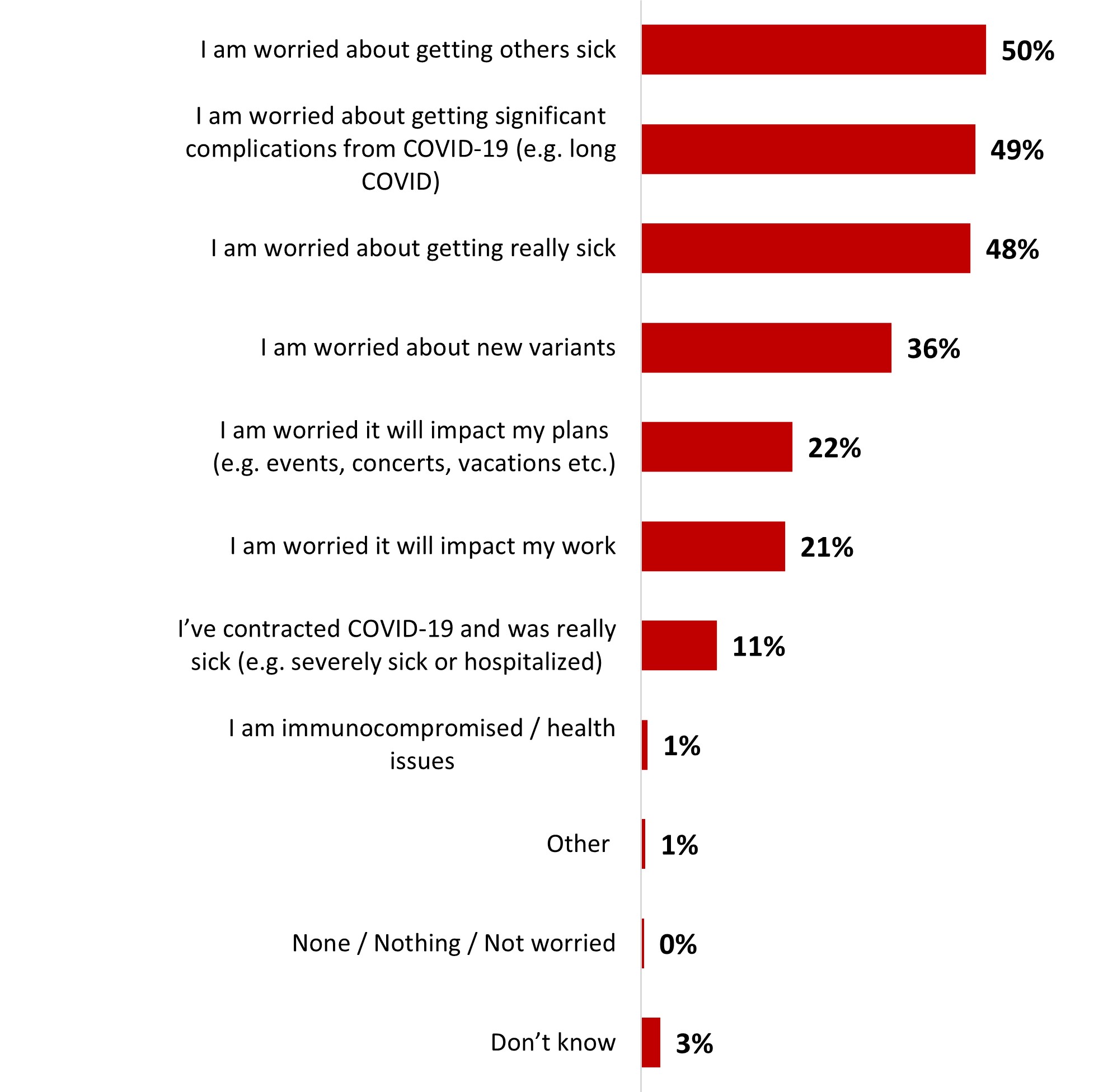
Figure 18.6: Text description
- I am worried about getting others sick
- 50%
- I am worried about getting significant complications from COVID-19 (e.g. long COVID)
- 49%
- I am worried about getting really sick
- 48%
- I am worried about new variants
- 36%
- I am worried it will impact my plans (e.g. events, concerts, vacations etc.)
- 22%
- I am worried it will impact my work
- 21%
- I've contracted COVID-19 and was really sick (e.g. severely sick or hospitalized)
- 11%
- I am immunocompromised / health issues
- 1%
- Other
- 1%
- None / Nothing / Not worried
- 0%
- Don't know
- 3%
Significant differences regarding reasons to be worried include:
- 18-34 year-olds were more likely to worry about an infection's impact on their plans (26%) and work (34%) or because they have gotten really sick after a previous infection (18%), while those over 55 years old were more likely to worry about significant complications (53%) or new variants (49%).
- Parents of children younger than 18 years old were more likely to worry because they got really sick after a previous infection (17%) and because of its impact on their work (31%). On the other hand, those who were not parents of children younger than 18 years old were more likely to mention worries about significant complications (50%) and new variants (39%).
4.2 Mental health
When asked about their most pressing concerns, a large proportion of respondents mentioned their personal financial situation (21%) and the state of the economy (17%). These two concerns ranked highest, well ahead of their physical health (10%), the health of their family and friends (8%), and mental health (7%). These were the five concerns that ranked highest, ahead of all other concerns that accounted for 6% or less of mentions among respondents. Around 6% of respondents mentioned not having any pressing concerns.
Figure 18.7: What is your most pressing concern at this time?
Sample frame: All respondents (n=3,026)
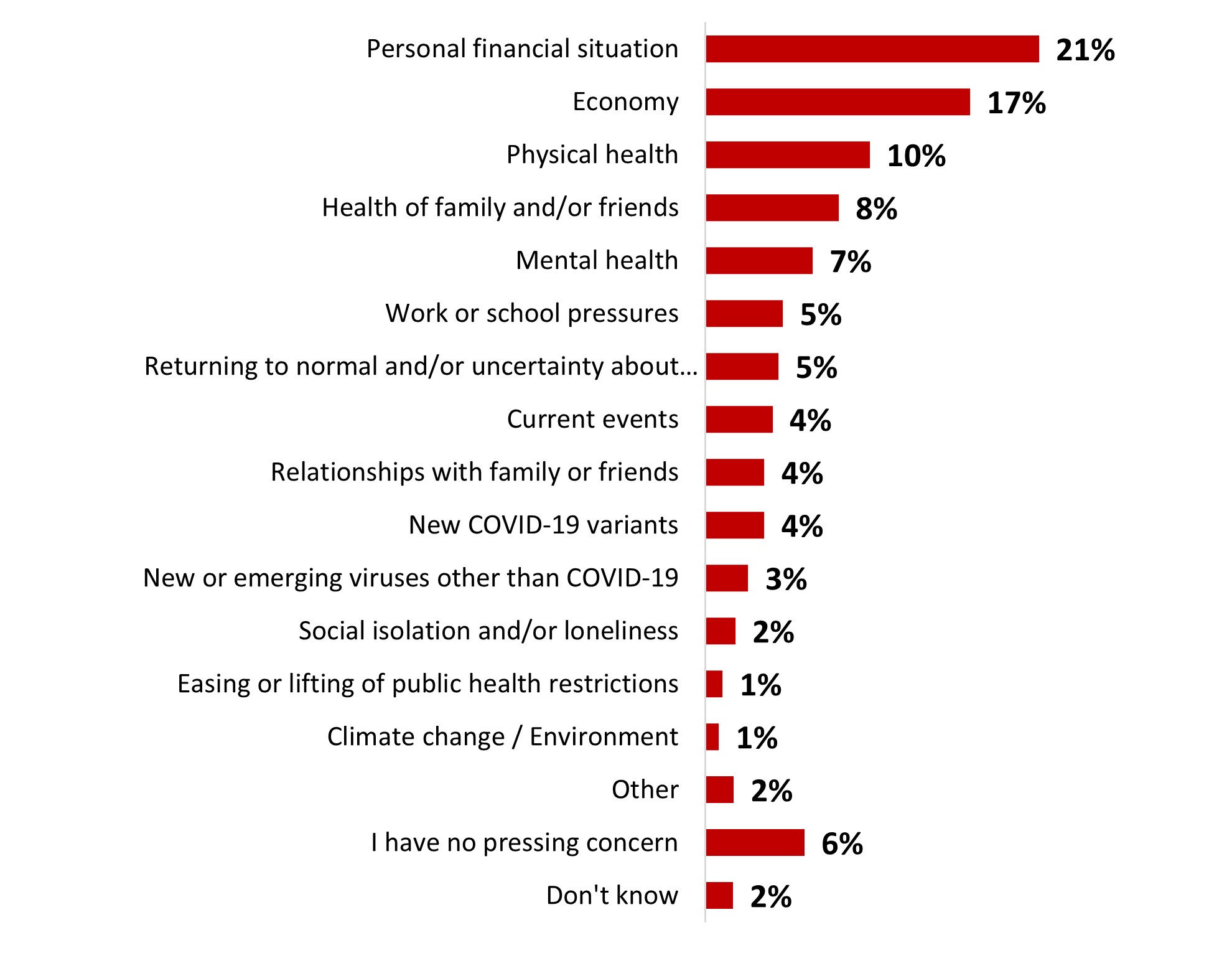
Figure 18.7: Text description
- Personal financial situation
- 21%
- Economy
- 17%
- Physical health
- 10%
- Health of family and/or friends
- 8%
- Mental health
- 7%
- Work or school pressures
- 5%
- Returning to normal and/or uncertainty about the future
- 5%
- Current events
- 4%
- Relationships with family or friends
- 4%
- New COVID-19 variants
- 4%
- New or emerging viruses other than COVID-19
- 3%
- Social isolation and/or loneliness
- 2%
- Easing or lifting of public health restrictions
- 1%
- Climate change / Environment
- 1%
- Other
- 2%
- I have no pressing concern
- 6%
- Don't know
- 2%
Some subgroups were significantly more likely to mention certain concerns, including:
- Women were significantly more likely to worry about their personal financial situation (23%), the health of family/friends (11%), and mental health (8%). On the other hand, men were more likely to be worried about the economy (20%).
- 18-34 year-olds were significantly more likely to worry about work or school pressures (13%) and their mental health (11%), while those over 55 years old were more likely to worry about the health of family and or friends (11%) and their own physical health (15%).
- Respondents who earn less than $40,000 were more likely to worry about their personal financial situation (27%), while those who earn over $80,000 were more likely to worry about the economy (20%).
- Black-identifying individuals were significantly more likely to report being worried about their personal financial situation (29%), while those who identify as white were more likely to report being worried about their physical health (11%) and to report not having any pressing concerns (7%).
- Parents of children younger than 18 years old were significantly more likely to be worried about their personal financial situation (24%).
Around three out of five respondents (60%) rated their mental health positively: either very good (21%) or good (40%). The remaining respondents their mental health status more negatively, ranging from average (28%) to bad (8%) or very bad (2%).
Figure 18.8: How would you rate your overall mental health?
Sample frame: All respondents (n=3,026)
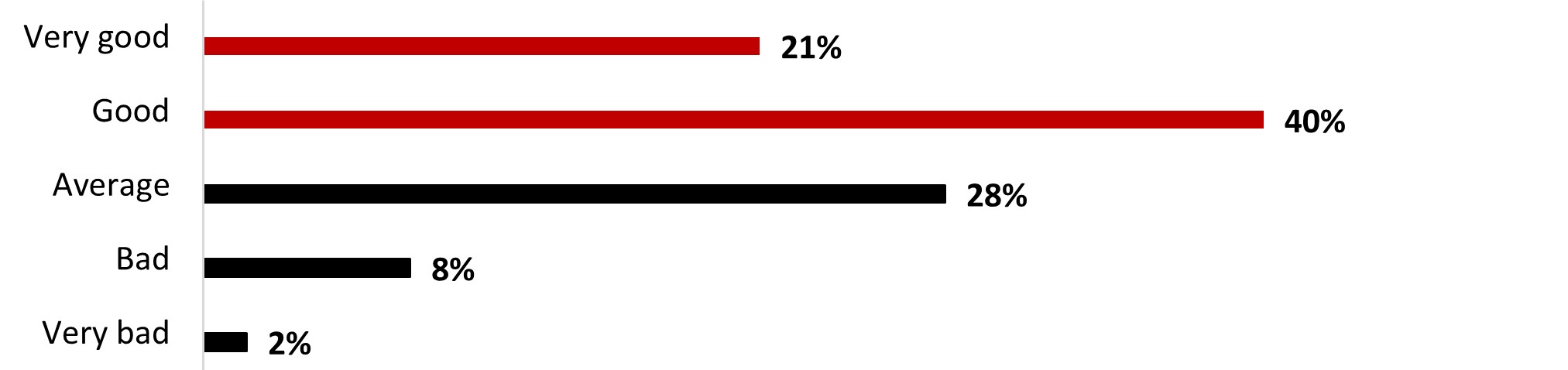
Figure 18.8: Text description
- Very bad
- 2%
- Bad
- 8%
- Average
- 28%
- Good
- 40%
- Very good
- 21%
Significant differences in terms of mental health include:
- Male respondents were significantly more likely to rate their mental health as very good (24%) compared to women (18%).
- Young respondents (18-34 year-olds) were significantly more likely to rate their mental health as average (32%) or bad (15%), while older respondents (over 55 years old) were more likely to rate it as very good (28%) or good (43%). Those aged between 35 and 54 were more likely to rate their mental health average (34%).
- Respondents in Ontario were more likely to rate their mental health bad (11%), while those from Quebec were more likely to rate it as very good (29%) or good (48%).
- Parents of children younger than 18 years old were more likely to rate it as average (34%), while non-parents were more likely to rate it as very good (22%).
A strong majority of respondents (86%) indicated that they had not received mental health support in the month before the survey. In contrast, one out of ten respondents (13%) indicated that they had received some support in this regard.
Figure 18.9: In the past month, have you received any support for your mental health?
Sample frame: All respondents (n=3,026)
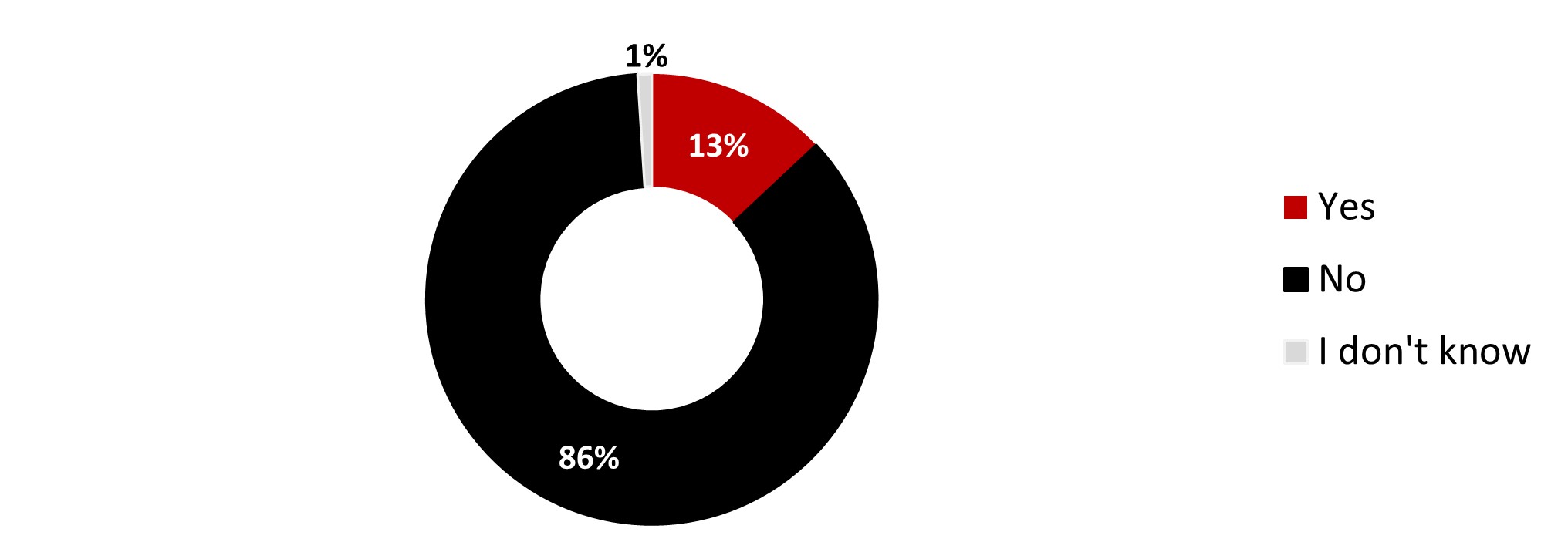
Figure 18.9: Text description
- Yes
- 13%
- No
- 86%
- I don't know
- 1%
The following subgroups were significantly more likely to have received support for coping with mental health:
- 18-34 year-olds (20%) and 35-54 year-olds (16%)
- Respondents who identify as Indigenous (20%)
- Parents of children younger than 18 years old (17%)
Of those who had received support during the previous month, most reported having received in-person support from social workers, psychologists or other professionals (40%), virtual support from social workers, psychologists or other professionals (35%), or support from their primary health care provider (28%). Telephone (or SMS) support (23%) and resources and tips for self-care (21%) rounded out the top five types of support received.
Figure 18.10: What type of support have you received? Select all that apply.
Sample frame: Those who received support for their mental health in the past month (n=430)
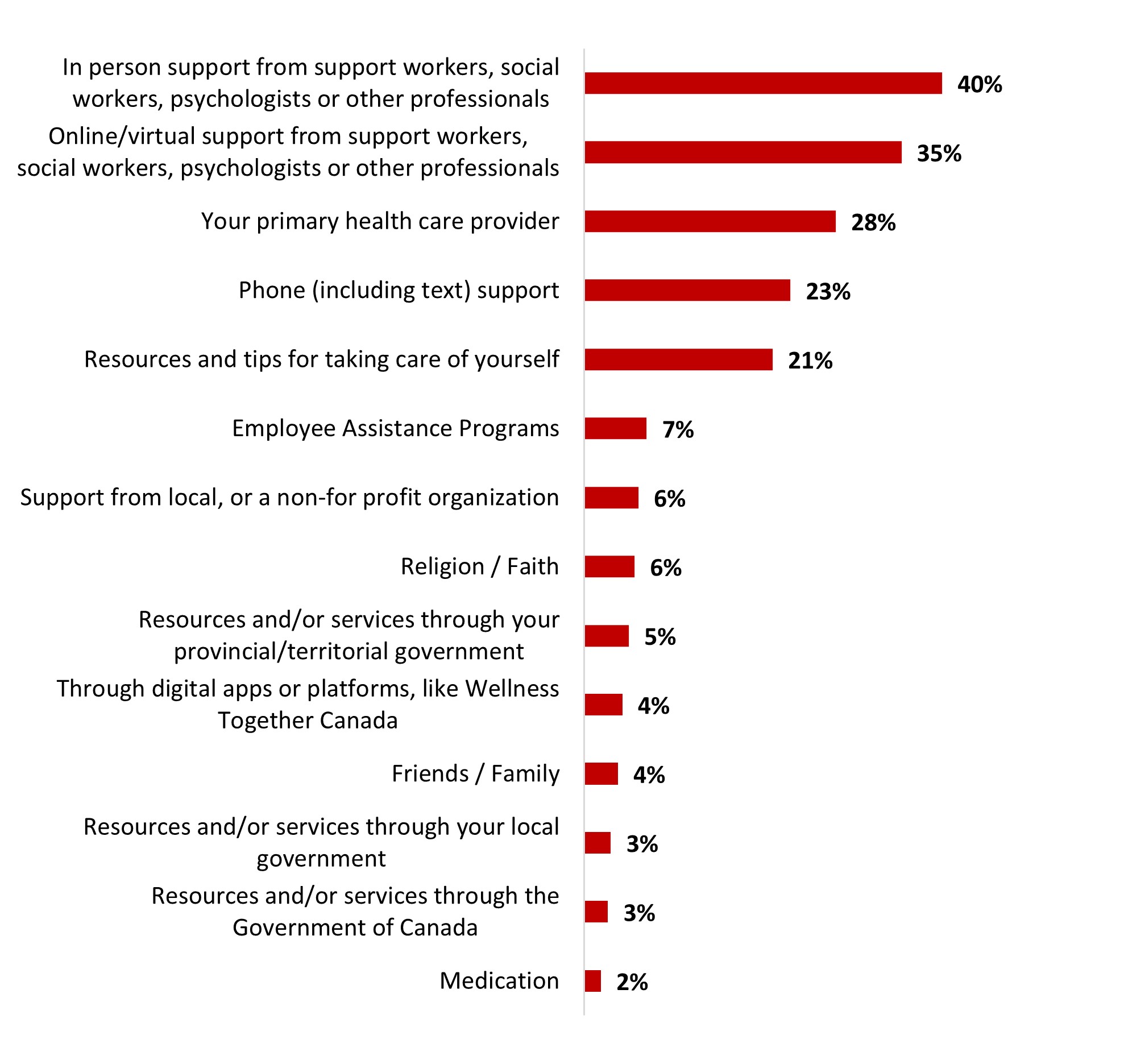
Figure 18.10: Text description
- Medication
- 2%
- Resources and/or services through the Government of Canada
- 3%
- Resources and/or services through your local government
- 3%
- Friends / Family
- 4%
- Through digital apps or platforms, like Wellness Together Canada
- 4%
- Resources and/or services through your provincial/territorial government
- 5%
- Religion / Faith
- 6%
- Support from local, or a non-for profit organization
- 6%
- Employee Assistance Programs
- 7%
- Resources and tips for taking care of yourself
- 21%
- Phone (including text) support
- 23%
- Your primary health care provider
- 28%
- Online/virtual support from support workers, social workers, psychologists or other professionals
- 35%
- In person support from support workers, social workers, psychologists or other professionals
- 40%
Significant differences in terms of mental health support services include:
- 18-34 year-olds were significantly more likely to turn to online/virtual support from support workers, social workers, psychologists or other professionals (48%). While those over 55 years old were more likely to turn to their primary healthcare provider (51%).
- Indigenous-identifying individuals were more likely to turn to in-person support (56%), while Black-identifying individuals were more likely to turn to online/virtual support (52%).
Respondents were asked to rate each statement according to their level of agreement with it. Almost nine out of ten (87%) agreed either strongly (52%) or somewhat (34%) that mental health is interconnected with physical health and central to overall health and well-being. Around two-thirds of respondents agreed with the statement "I know when I need help with my mental health" (65%), "I practice taking care of my mental health on a regular basis" (63%), and "I have enough time to take care of my mental health" (62%). Six out of ten were aware of free mental health and substance use resources online or by phone (60%), and knew how or where to get help for their mental health (59%). Around half feel they have adequate access to mental health support services (52%) and think they can manage their mental health struggles on their own (52%). Around two out of five could afford to see a mental health therapist (44%), considered it hard to ask for help (41%), and could afford mental health support (41%).
Table 18.11: To what extent do you agree or disagree with the following statements?
Sample frame: All respondents (n=3,026)
| Mental health is interconnected with physical health, and central to overall health and well-being | Strongly agree | Somewhat agree | Neither agree nor disagree | Somewhat disagree | Strongly disagree | Unsure / Not applicable |
|---|---|---|---|---|---|---|
| Mental health is interconnected with physical health, and central to overall health and well-being | 52% | 34% | 8% | 2% | 1% | 2% |
| I know when I need help with my mental health. | 24% | 41% | 21% | 6% | 2% | 6% |
| I practice taking care of my mental health on a regular basis. | 20% | 43% | 24% | 8% | 2% | 3% |
| I have enough time to take care of my mental health. | 24% | 38% | 20% | 11% | 4% | 3% |
| I am aware of free mental health and substance use resources online or by phone. | 24% | 36% | 15% | 11% | 6% | 7% |
| I know how or where to get help for my mental health. | 21% | 39% | 19% | 11% | 5% | 7% |
| I feel I have adequate access to mental health support services. | 19% | 33% | 22% | 11% | 6% | 9% |
| I think I can manage my mental health struggles on my own. | 16% | 36% | 24% | 13% | 5% | 6% |
| I can afford to see a mental health therapist such as a social worker, psychologist, or counsellor. | 16% | 28% | 17% | 14% | 17% | 8% |
| It's hard to ask for help if I'm struggling with my mental health. | 14% | 28% | 23% | 16% | 10% | 9% |
| I can afford mental health support. | 15% | 26% | 20% | 15% | 16% | 8% |
The following tables detail the significant differences between subgroups according to age, ethnicity, parental status, and region.
Reading note: In the following tables, significantly lower differences are marked with a "-" sign, while significantly higher differences are marked with a "+".
| Age | Ethnicity | Parents of children under 18 | ||||||
|---|---|---|---|---|---|---|---|---|
| 18-34 | 35-54 | 55+ | White | Indigenous | Black | Yes | No | |
| I know when I need help with my mental health. | 83% - | 88% | 88% | 87% | 86% | 87% | 88% | 86% |
| I practice taking care of my mental health on a regular basis. | 62% | 64% | 67% | 65% | 73% + | 62% | 68% | 64% |
| I have enough time to take care of my mental health. | 59% - | 64% | 64% | 64% | 61% | 69% + | 67% + | 61% - |
| I am aware of free mental health and substance use resources online or by phone. | 45% - | 58% - | 76% + | 63% + | 60% | 60% | 53% - | 65% + |
| I know how or where to get help for my mental health. | 60% | 59% | 61% | 61% | 70% + | 64% | 63% | 59% |
| I feel I have adequate access to mental health support services. | 57% | 59% | 61% | 60% | 66% | 59% | 63% + | 58% |
| I think I can manage my mental health struggles on my own. | 50% | 54% | 53% | 52% | 61% + | 55% | 58% + | 50% - |
| I can afford to see a mental health therapist such as a social worker, psychologist, or counsellor. | 52% | 50% | 54% | 51% - | 54% | 53% | 55% | 51% |
| It's hard to ask for help if I'm struggling with my mental health. | 42% | 43% | 46% | 44% | 33% - | 40% | 48% + | 43% |
| I can afford mental health support. | 51% + | 44% | 33% - | 39% - | 44% | 40% | 46% + | 40% - |
| I know when I need help with my mental health. | 40% | 40% | 41% | 40% | 30% - | 37% | 45% + | 39% - |
| British Columbia + Territories | Alberta | Manitoba / Saskatchewan | Ontario | Quebec | Atlantic | |
|---|---|---|---|---|---|---|
| I know when I need help with my mental health. | 91% + | 88% | 85% | 85% | 86% | 90% |
| I practice taking care of my mental health on a regular basis. | 65% | 59% - | 63% | 66% | 68% | 63% |
| I have enough time to take care of my mental health. | 61% | 62% | 64% | 60% - | 70% + | 60% |
| I am aware of free mental health and substance use resources online or by phone. | 59% | 61% | 61% | 61% | 65% | 63% |
| I know how or where to get help for my mental health. | 58% | 62% | 53% | 54% - | 72% + | 63% |
| I feel I have adequate access to mental health support services. | 62% | 59% | 53% | 57% - | 62% | 66% |
| I think I can manage my mental health struggles on my own. | 52% | 55% | 51% | 52% | 51% | 52% |
| I can afford to see a mental health therapist such as a social worker, psychologist, or counsellor. | 52% | 50% | 56% | 55% | 48% - | 51% |
| It's hard to ask for help if I'm struggling with my mental health. | 45% | 45% | 45% | 44% | 42% | 44% |
| I can afford mental health support. | 43% | 43% | 52% + | 42% | 32% - | 51% + |
| I know when I need help with my mental health. | 42% | 42% | 40% | 41% | 39% | 43% |
4.3 COVID-19 Vaccine
- With regard to knowledge about COVID-19, a strong majority of respondents indicated that they agreed (strongly agree and somewhat agree) with the following statements:
- it is possible to have COVID-19 even if vaccinated (96%),
- it is possible to have COVID-19 on several occasions (92%).
- Eight out of ten respondents also agreed that a person would be less likely to become seriously ill if infected with COVID-19 after being vaccinated (80%).
- About three out of four respondents agreed that staying up to date with their vaccination includes booster doses (78%).
- A smaller proportion of respondents (74%) said they consider it important to stay up to date with their vaccination.
- Slightly more than half of the respondents (57%) agreed that protection from vaccination was more durable and effective than immunity from infection.
- Less than half of respondents (50%) agreed that immunity from infection was short-lived and not as effective.
Table 18.14: To what extent do you agree with the following statements?
Sample frame: All respondents (n=3,026)
| Strongly agree | Somewhat agree | Somewhat disagree | Strongly disagree | Don't know | |
|---|---|---|---|---|---|
| You can get COVID-19 even if vaccinated | 78% | 18% | 2% | 0% | 2% |
| You can catch COVID-19 multiple times | 69% | 23% | 2% | 1% | 4% |
| You are less likely to get seriously ill from COVID-19 if you are vaccinated (e.g. not be hospitalized) | 51% | 29% | 7% | 7% | 6% |
| Staying up to date with COVID-19 vaccinations includes boosters | 54% | 24% | 7% | 8% | 7% |
| It is important to stay up to date with COVID-19 vaccinations | 49% | 25% | 9% | 10% | 6% |
| Protection against COVID-19 is longer with vaccination and is more effective than immunity from infection | 30% | 27% | 11% | 9% | 23% |
| The immunity provided by a COVID-19 infection is short-lived and not as effective | 20% | 30% | 18% | 8% | 24% |
The following tables detail the significant differences between subgroups according to age, ethnicity, parental status, and region.
Reading note: In the following tables, significantly lower differences are marked with a "-" sign, while significantly higher differences are marked with a "+".
| Age | Ethnicity | Parents of children under 18 | ||||||
|---|---|---|---|---|---|---|---|---|
| 18-34 | 35-54 | 55+ | White | Indigenous | Black | Yes | No | |
| You can get COVID-19 even if vaccinated | 91% - | 96% | 98% + | 97% + | 94% | 91% - | 93% | 92% |
| You can catch COVID-19 multiple times | 88% - | 92% | 95% + | 93% + | 89% | 87% - | 95% | 96% |
| You are less likely to get seriously ill from COVID-19 if you are vaccinated (e.g. not be hospitalized) | 73% - | 75% - | 87% + | 81% + | 75% | 70% - | 73% - | 82% + |
| Staying up to date with COVID-19 vaccinations includes boosters | 66% - | 74% - | 88% + | 79% + | 68% - | 66% - | 66% - | 78% + |
| It is important to stay up to date with COVID-19 vaccinations | 63% - | 69% - | 86% + | 75% | 66% - | 66% - | 71% - | 81% + |
| Protection against COVID-19 is longer with vaccination and is more effective than immunity from infection | 56% | 52% - | 62% + | 56% | 57% | 45% - | 52% | 49% |
| The immunity provided by a COVID-19 infection is short-lived and not as effective | 52% | 50% | 48% | 47% - | 50% | 44% | 55% | 58% |
| British Columbia + Territories | Alberta | Manitoba / Saskatchewan | Ontario | Quebec | Atlantic | |
|---|---|---|---|---|---|---|
| You can get COVID-19 even if vaccinated | 97% | 96% | 95% | 94% - | 96% | 97% |
| You can catch COVID-19 multiple times | 94% | 93% | 93% | 91% | 92% | 95% |
| You are less likely to get seriously ill from COVID-19 if you are vaccinated (e.g. not be hospitalized) | 83% | 79% | 82% | 78% | 78% | 87% + |
| Staying up to date with COVID-19 vaccinations includes boosters | 79% | 76% | 81% | 76% | 78% | 85% + |
| It is important to stay up to date with COVID-19 vaccinations | 79% + | 72% | 75% | 73% | 73% | 79% |
| Protection against COVID-19 is longer with vaccination and is more effective than immunity from infection | 65% + | 59% | 59% | 56% | 49% - | 63% |
| The immunity provided by a COVID-19 infection is short-lived and not as effective | 53% | 51% | 52% | 50% | 45% - | 47% |
A high proportion of respondents (93%) reported having received at least one dose of the COVID-19 vaccine. Very few respondents reported receiving only one dose (1%). Most indicated that they had received two doses (22%), three doses (29%), or four doses (27%). Over one out of ten indicated they had five doses (14%). Fewer than one out of ten respondents (6%) mentioned not receiving any doses against COVID-19.
Figure 18.17: How many doses of the COVID-19 vaccine have you received?
Sample frame: All respondents (n=3,026)
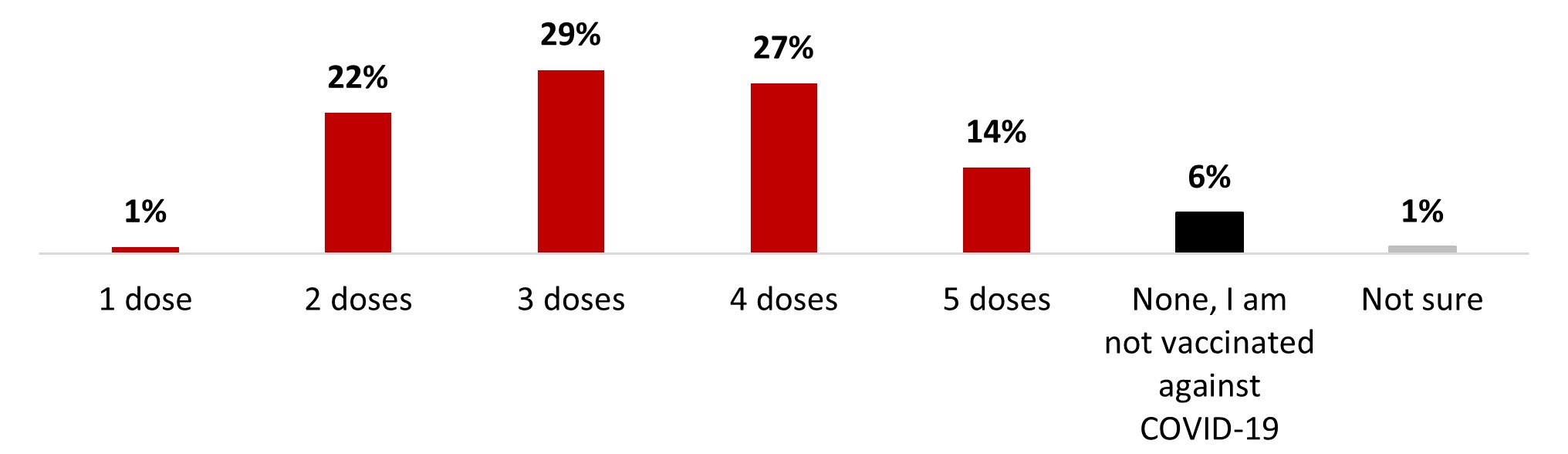
Figure 18.17: Text description
- 1 dose
- 1%
- 2 dose
- 22%
- 3 dose
- 29%
- 4 dose
- 27%
- 5 dose
- 14%
- None, I am not vaccinatedagainst COVID-19
- 6%
- Not sure
- 1%
The following subgroups were significantly more vaccinated than their complement:
- Those over 55 years old (3.9 doses on average)
- Quebec respondents (3.5 doses)
- White-identifying individuals (3.4)
- Those who are not parents of children younger than 18 years old (3.5)
The following subgroups were significantly less vaccinated than their complement:
- 18-34 year-olds (2.7 doses on average)
- 35-54 year-olds (3.1 doses)
- Black-identifying individuals (2.7)
- Parents of children younger than 18 years old (2.9)
Of those who said they had received at least one dose of the COVID-19 vaccine or were unsure (94% of the total sample), we asked if they had had any booster doses. Three out of four respondents (75%) reported receiving at least one booster dose of the COVID-19 vaccine. Almost three out of ten respondents (28%) reported that they had received one booster dose, one out of four (25%) reported that they had had two booster doses, and one out of five (22%) reported that they had received three booster doses. One out of four (25%) stated they did not receive a booster dose.
Figure 18.18: Have you received a COVID-19 booster dose?
Sample frame: Respondents who have received at least one dose or who are unsure about it (n=2,823)
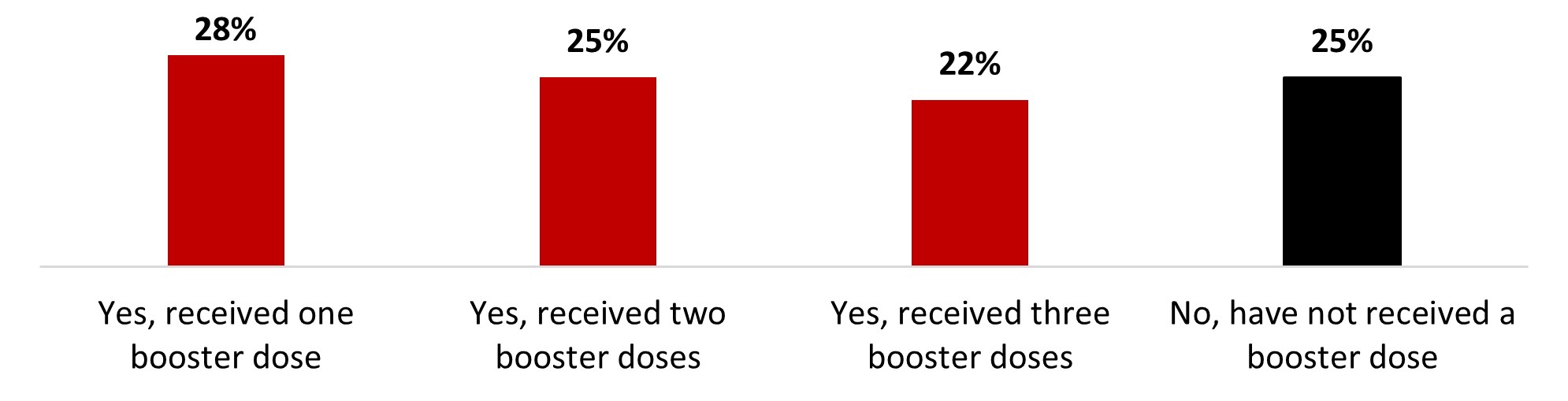
Figure 18.18: Text description
- Yes, received one booster dose
- 28%
- Yes, received two booster doses
- 25%
- Yes, received three booster doses
- 22%
- No, have not received a booster dose
- 25%
The following subgroups were significantly more likely to have received at least one booster dose:
- Those over 55 years old (87%)
- Those who earn over $80,000 (79%)
- Those with a university degree (83%)
- White-identifying individuals (77%)
- Those who are not parents of children under 18 (80%)
The following subgroups were significantly more likely not to have received a booster dose:
- 18-34 (36%) and 35-54 year-old (31%) individuals
- Those who earn less than $40,000 (30%)
- Black-identifying individuals (48%)
- Parents of children younger than 18 years old (37%)
Over two out of five respondents who have received at least one dose got their latest one less than three months ago (42%), and around one out of four got it between 3-6 months prior (25%) or six months to a year prior (27%) to the survey. A very small proportion stated their latest dose was over a year prior (5%).
Figure 18.19: When did you receive your most recent COVID-19 booster dose?
Sample frame: Respondents who have received at least one dose (n=2,086)
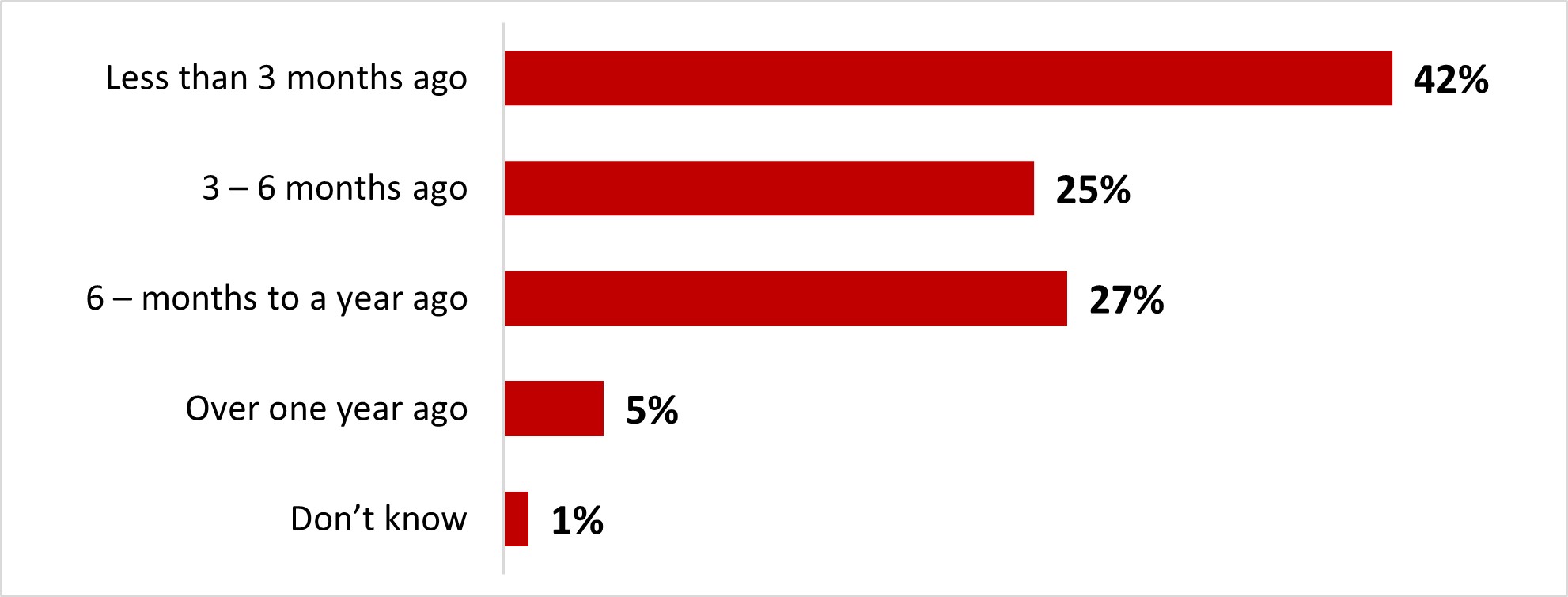
Figure 18.19: Text description
- Less than 3 months ago
- 42%
- 3 – 6 months ago
- 25%
- 6 – months to a year ago
- 27%
- Over one year ago
- 5%
- Don't know
- 1%
The following subgroups were significantly more likely to have gotten their latest dose less than three months before the survey:
- Those over 55 years old (54%)
- Residents of British Columbia and the Territories (58%)
The following subgroups were significantly more likely to have gotten their latest dose over one year before the survey:
- 18-34 year-olds (8%)
- Black-identifying individuals (14%)
- Parents of children younger than 18 years old (8%)
Among those who had received at least one dose of vaccine, more than seven out of ten respondents (69%) reported that they were likely to keep their booster doses up to date: 46% very likely and 23% somewhat likely. In contrast, about one out of four respondents (26%) said they were unlikely to do so: 14% not very likely and 12% not at all likely.
Figure 18.20: How likely are you to keep your COVID-19 doses up to date (i.e. continue to receive them as you become eligible for additional doses)?
Sample frame: Respondents who have received at least one dose (n=2,795)
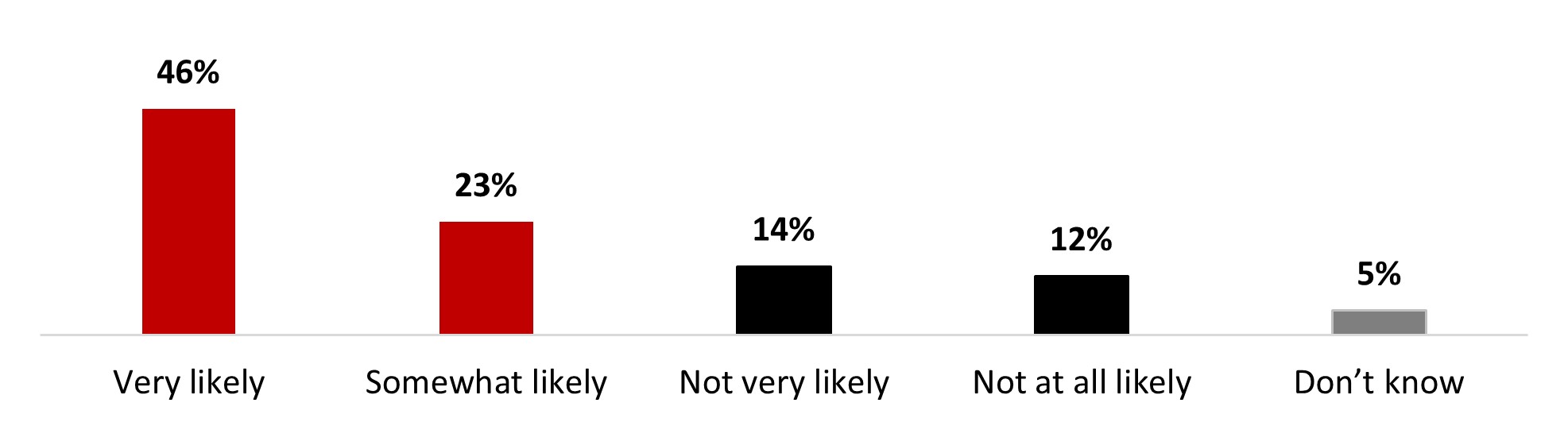
Figure 18.20: Text description
- Very likely
- 46%
- Somewhat likely
- 23%
- Not very likely
- 14%
- Not at all likely
- 12%
- Don't know
- 5%
The following subgroups were significantly more likely to state it's likely (very or somewhat) that they keep their COVID-19 doses up to date:
- Men (72%)
- Respondents over 55 years old (83%)
- Respondents from British Columbia and Territories (74%)
- University degree holders (75%)
- Individuals who are not parents of children younger than 18 years old (73%)
Respondents who did not receive booster doses or were unsure about it indicated that the vaccines did not provide sufficient protection because it is possible to get infected with COVID-19 even if you are vaccinated (16%), that they were worried about the potential long-term effects of the vaccine (16%), that they felt they were sufficiently protected with the number of vaccines they had received (15%), and that they were fed up with being vaccinated (14%) as the main reasons for being hesitant to receive booster doses. Other reasons were mentioned by less than 10% of respondents.
Figure 18.21: What is the top reason you are unlikely or uncertain about getting a booster dose?
Sample frame: Those who have not received a booster dose or are unsure about it (n=931)
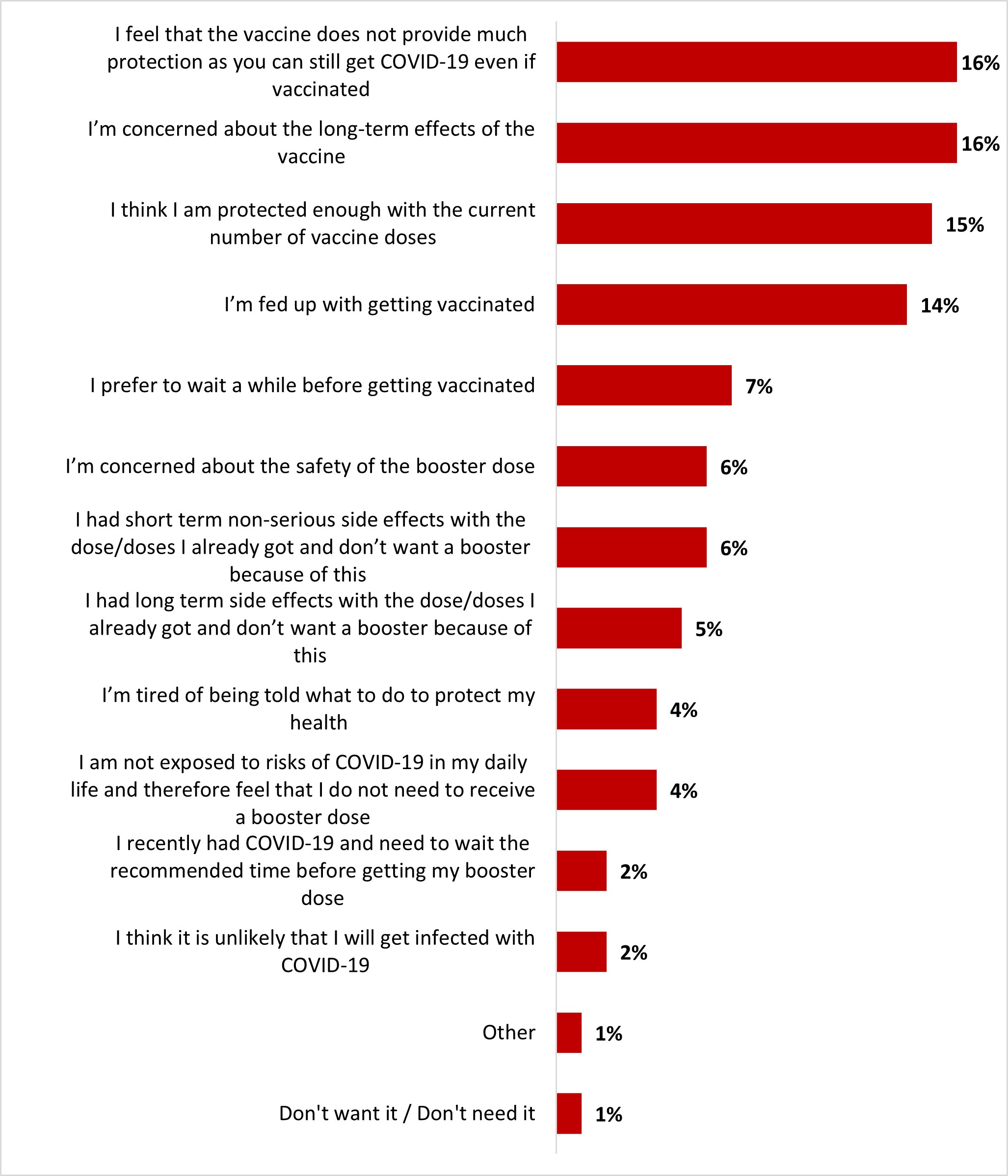
Figure 18.21: Text description
- I feel that the vaccine does not provide much protection as you can still get COVID-19 even if vaccinated
- 16%
- I'm concerned about the long-term effects of the vaccine
- 16%
- I think I am protected enough with the current number of vaccine doses
- 15%
- I'm fed up with getting vaccinated
- 14%
- I prefer to wait a while before getting vaccinated
- 7%
- I'm concerned about the safety of the booster dose
- 6%
- I had short term non-serious side effects with the dose/doses I already got and don't want a booster because of this
- 6%
- I had long term side effects with the dose/doses I already got and don't want a booster because of this
- 5%
- I'm tired of being told what to do to protect my health
- 4%
- I am not exposed to risks of COVID-19 in my daily life and therefore feel that I do not need to receive a booster dose
- 4%
- I recently had COVID-19 and need to wait the recommended time before getting my booster dose
- 2%
- I think it is unlikely that I will get infected with COVID-19I think it is unlikely that I will get infected with COVID-19
- 2%
- Other
- 1%
- Don't want it / Don't need it
- 1%
Those over 55 years old were significantly more likely to feel concerned about the long-term effects of the vaccine (22%). On the other hand, parents of children under 18 were more likely to feel that the vaccine does not provide much protection as you can still get infected (21%).
Respondents who had not had booster doses indicated that the following reasons would be motivating factors for getting booster doses: if it was required for travel outside the country (15%), if the new vaccines covered the most recent variants (12%), and/or if it were required to be able to travel within Canada (11%). Two out of five respondents who did not get a booster dose said that none of the factors would motivate them to get their booster dose (40%).
Figure 18.22: Amongst the following factors and thinking about the current COVID-19 context, what would motivate you to get your booster dose?
Sample frame: Respondents who have not gotten a booster dose (n=737)
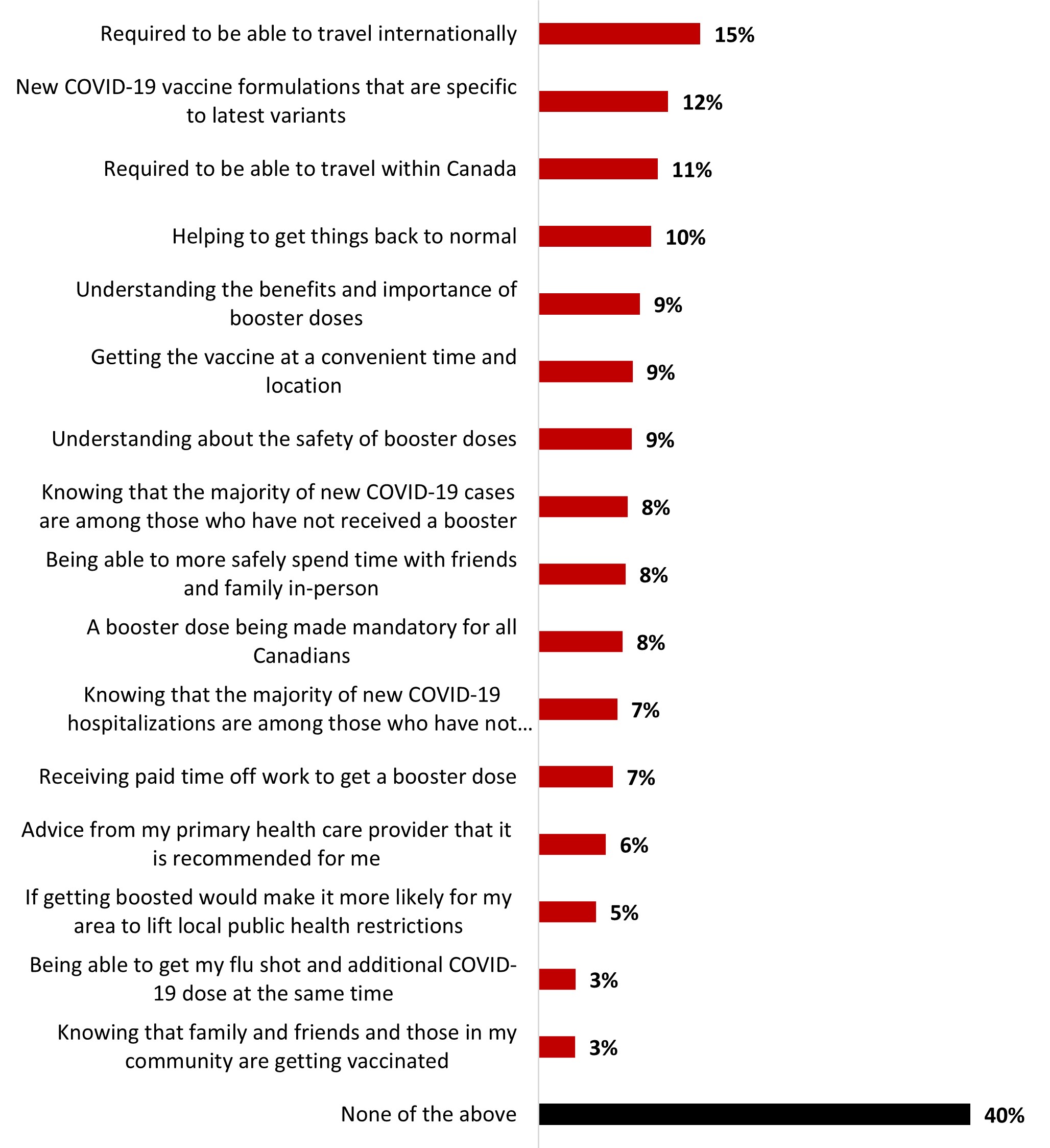
Figure 18.22: Text description
- Required to be able to travel internationally
- 15%
- New COVID-19 vaccine formulations that are specific to latest variants
- 12%
- Required to be able to travel within Canada
- 11%
- Helping to get things back to normal
- 10%
- Understanding the benefits and importance of booster doses
- 9%
- Getting the vaccine at a convenient time and location
- 9%
- Understanding about the safety of booster doses
- 9%
- Knowing that the majority of new COVID-19 cases are among those who have not received a booster
- 8%
- Being able to more safely spend time with friends and family in-person
- 8%
- A booster dose being made mandatory for all Canadians
- 8%
- Knowing that the majority of new COVID-19 hospitalizations are among those who have not received a booster
- 7%
- Receiving paid time off work to get a booster dose
- 7%
- Advice from my primary health care provider that it is recommended for me
- 6%
- If getting boosted would make it more likely for my area to lift local public health restrictions
- 5%
- Being able to get my flu shot and additional COVID-19 dose at the same time
- 3%
- Knowing that family and friends and those in my community are getting vaccinated
- 3%
- None of the above
- 40%
Respondents from the Atlantic region were significantly more likely to mention that helping things get back to normal would motivate them to get boosted (25%). Indigenous-identifying respondents were more likely to mention that understanding the benefits and importance of booster doses would motivate them (21%).
Respondents were asked if they ever hesitated to get a COVID-19 booster dose, and almost one person out of four has been reluctant or hesitated to get boosted (23%), while three out of four never did (75%).
Figure 18.23: Have you ever been reluctant or hesitated to get a COVID-19 booster dose?
Sample frame: Respondents who have received at least one booster dose (n=2,086)
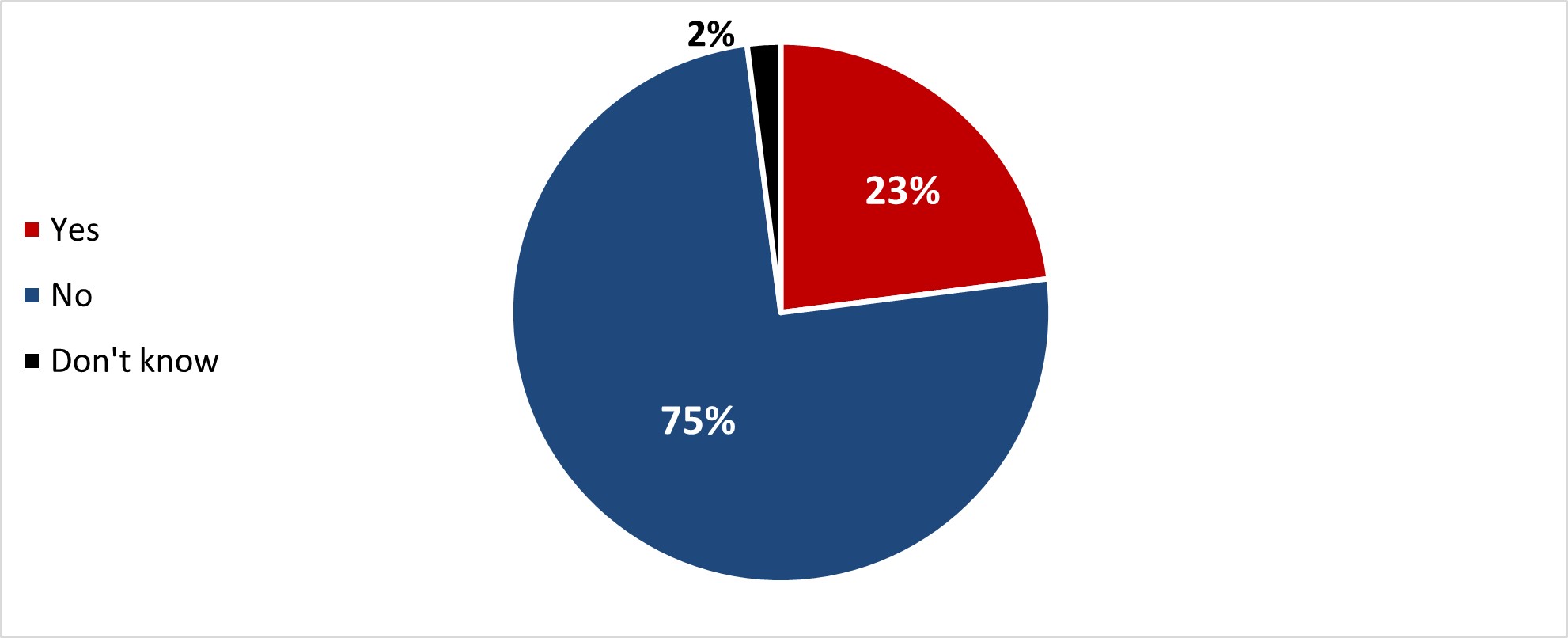
Figure 18.23: Text description
- Yes
- 23%
- No
- 75%
- Don't know
- 2%
18-34 year-olds (32%) and 35-54 year-olds (28%), women (28%), parents of children under 18 (28%), as well as Black-identifying (35%) and Indigenous-identifying (31%) respondents were all more likely to have been reluctant.
Over half of those who have been reluctant mentioned concerns about the safety and/or side effects of getting boosted as a justification (57%), way ahead of the other reasons. One person out of five (19%) mentioned thinking that COVID-19 vaccines are not effective in protecting them or that they had bad reactions to the previous doses. Other reasons were mentioned by a lower proportion of respondents.
Figure 18.24: For which reasons were you reluctant to get a COVID-19 booster dose?
Sample frame: Respondents who have received at least one booster dose (n=506)
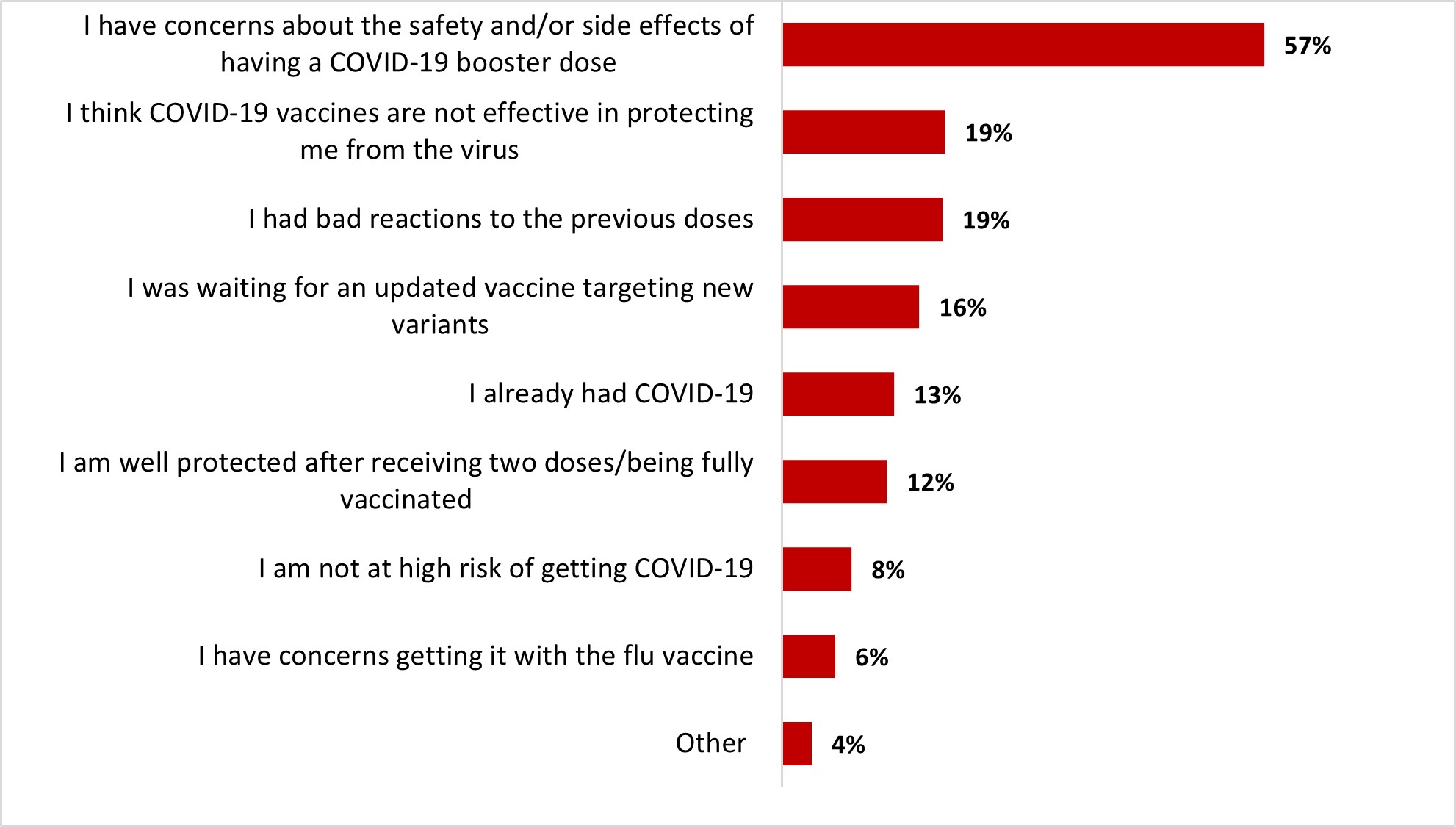
Figure 18.24: Text description
- Other
- 4%
- I have concerns getting it with the flu vaccine
- 6%
- I am not at high risk of getting COVID-19
- 8%
- I am well protected after receiving two doses/being fully vaccinated
- 12%
- I already had COVID-19
- 13%
- I was waiting for an updated vaccine targeting new variants
- 16%
- I had bad reactions to the previous doses
- 19%
- I think COVID-19 vaccines are not effective in protecting me from the virus
- 19%
- I have concerns about the safety and/or side effects of having a COVID-19 booster dose
- 57%
Respondents aged 18-34 were more likely to state being well protected after their two initial doses (22%) and that they had bad reactions to the previous doses (29%). Albertan respondents were more likely to express concerns about the safety and/or side effects of the boosters (76%), while respondents from Manitoba and Saskatchewan (29%) and those from Quebec (21%) were more likely to state having already had COVID-19 as a reason for reluctance.
Those who were reluctant and ended up getting their booster dose mentioned the high number of cases as the main reason (34%), followed by a fear of regret (28%) and benefits outweighing the risks (26%). Other reasons were mentioned by less than one out of five respondents.
Figure 18.25: What made you decide to get a COVID-19 booster dose despite your initial reluctance?
Sample frame: Those who were reluctant to get a COVID-19 booster dose (n=506)
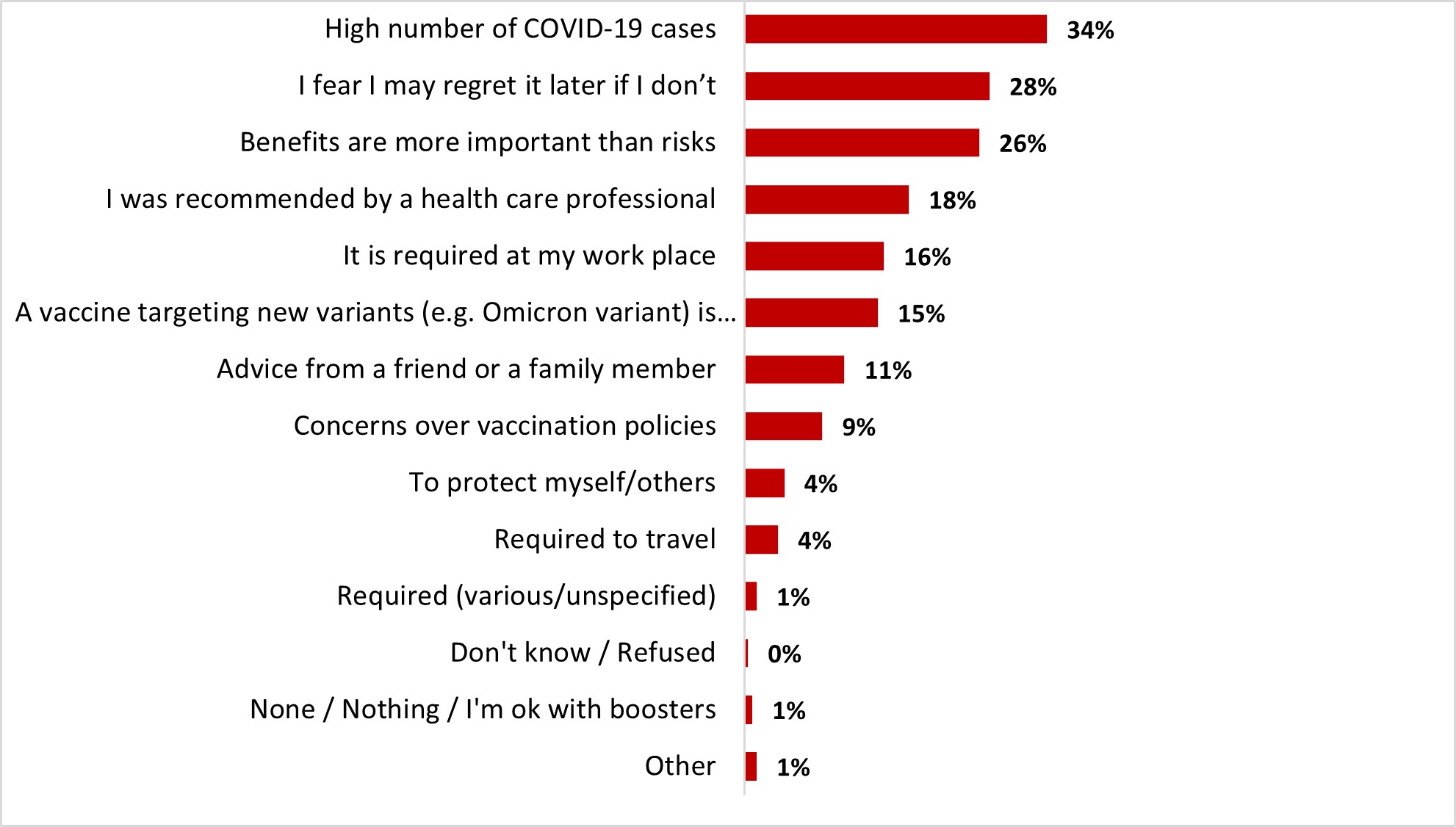
Figure 18.25: Text description
- Other
- 1%
- None / Nothing / I'm ok with boosters
- 1%
- Don't know / Refused
- Required (various/unspecified)
- 1%
- Required to travel
- 4%
- To protect myself/others
- 4%
- Concerns over vaccination policies
- 9%
- Advice from a friend or a family member
- 11%
- A vaccine targeting new variants (e.g. Omicron variant) is available
- 15%
- It is required at my work place
- 16%
- I was recommended by a health care professional
- 18%
- Benefits are more important than risks
- 26%
- I fear I may regret it later if I don't
- 28%
- High number of COVID-19 cases
- 34%
18-34 year-olds were more likely to mention that concern over vaccination policies (16%) and the booster being required at their workplace (24%) made them get their booster dose. Non-parents of children younger than 18 were more likely to have gotten their booster after reluctance because of the vaccine targeting new variants (18%).
Among respondents likely to pick up booster dose(s), nearly three out of four (74%) indicated that it was likely they would get their dose at the same time as the flu shot: 51% very likely and 23% somewhat likely. In contrast, almost one out of five respondents (18%) said it was unlikely: 13% unlikely and 5% not at all likely. Less than one out of ten (6%) said they would not take a flu shot.
Figure 18.26: If recommended, how likely would you be to get a COVID vaccine at the same time as a flu shot?
Sample frame: Those who are likely to get a booster dose or another booster dose (n=1,857)
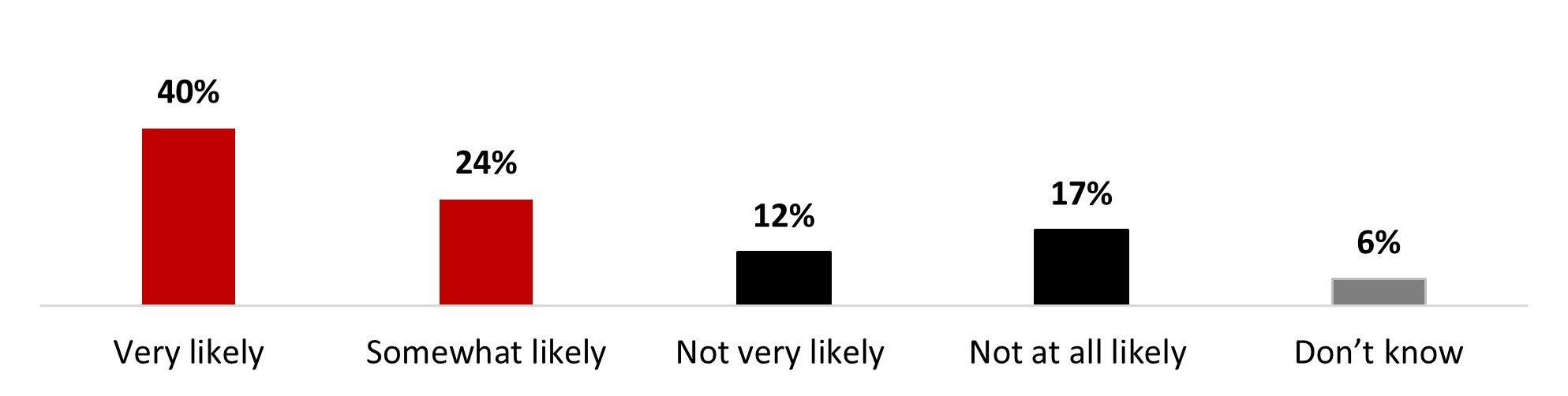
Figure 18.27: Text description
- Very likely
- 51%
- Somewhat likely
- 23%
- Not very likely
- 13%
- Not at all likely
- 5%
- Do not intend on getting a flu shot
- 6%
- Don't know
- 2%
Male respondents (80%) were significantly more likely to state that it's likely (very or somewhat) that they get their booster dose at the same time as the flu shot.
All respondents were asked if they would consider taking the COVID-19 vaccine as a routine vaccine annually. About two-thirds of respondents (64%) indicated that they would be likely to take the COVID-19 vaccine as a routine vaccine: 40% very likely and 24% somewhat likely. In contrast, nearly one respondent out of four (29%) indicated it was unlikely: 12% not likely and 17% not at all likely.
Figure 18.27: If COVID-19 vaccines were offered as a routine vaccine (e.g., annually), how likely would you be to get one?
Sample frame: All respondents (n=3,026)
Figure 18.27: Text description
- Very likely
- 40%
- Somewhat likely
- 24%
- Not very likely
- 12%
- Not at all likely
- 17%
- Don't know
- 6%
Some subgroups were more likely to state it was very or somewhat likely that they get a COVID-19 vaccine as a routine vaccine, including:
- Male respondents (68%)
- Respondents over 55 years old (78%)
- Those who hold a university degree (71%)
- Respondents who are not parents of children younger than 18 years old (68%)
- Those who had not been infected with COVID-19 (68%)
Among respondents who were unsure or considered it unlikely that they would take the COVID-19 vaccine as a part of their annual vaccine routine, the main reasons given for their hesitation were concerns about long-term effects (20%), far ahead of being fed up with vaccination (11%), or feeling that the vaccine does not provide much protection as you can still get infected (9%). Other reasons were also mentioned to a lesser extent.
Figure 18.28: What is the top reason you are unlikely or uncertain about getting a routine COVID-19 vaccine?
Sample frame: Those who are not likely or don't know if they would get a routine COVID-19 shot (n=1,166)
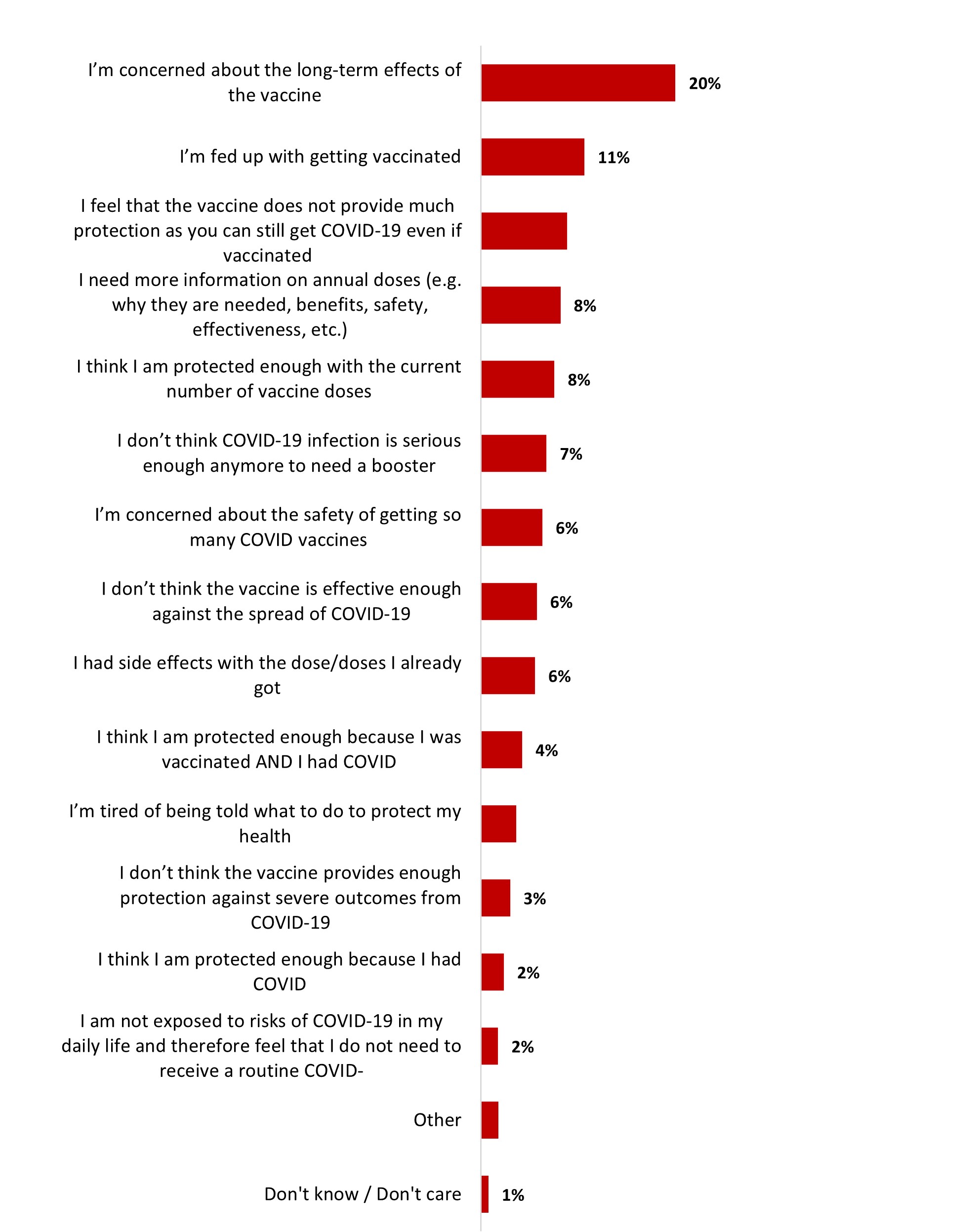
Figure 18.28: Text description
- Don't know / Don't care
- 1%
- Other
- 2%
- I am not exposed to risks of COVID-19 in my daily life and therefore feel that I do not need to receive a routine COVID-
- 2%
- I think I am protected enough because I had COVID
- 2%
- I don't think the vaccine provides enough protection against severe outcomes from COVID-19
- 3%
- I'm tired of being told what to do to protect my health
- 4%
- I think I am protected enough because I was vaccinated AND I had COVID
- 4%
- I had side effects with the dose/doses I already got
- 6%
- I don't think the vaccine is effective enough against the spread of COVID-19
- 6%
- I'm concerned about the safety of getting so many COVID vaccines
- 6%
- I don't think COVID-19 infection is serious enough anymore to need a booster
- 7%
- I think I am protected enough with the current number of vaccine doses
- 8%
- I need more information on annual doses (e.g. why they are needed, benefits, safety, effectiveness, etc.)
- 8%
- I feel that the vaccine does not provide much protection as you can still get COVID-19 even if vaccinated
- 9%
- I'm fed up with getting vaccinated
- 11%
- I'm concerned about the long-term effects of the vaccine
- 20%
Those over 55 years old were more likely to state needing more information on annual doses (13%). Respondents from British Columbia and the Territories were more likely to mention being concerned about the long-term effects of the vaccine (29%).
Respondents were also asked about the likelihood they would get COVID-19 vaccines if they were offered twice a year: almost eight out of ten said it was likely (78%: very: 48%; somewhat: 30%), while a little over one out of ten considered it unlikely (14%: not very likely: 12%; not at all likely: 2%).
Figure 18.29: And what about if the COVID vaccines were offered twice a year, how likely would you be to get them?
Sample frame: Respondents who are likely or unsure about getting routinely vaccinated against COVID-19 (n=2,051)
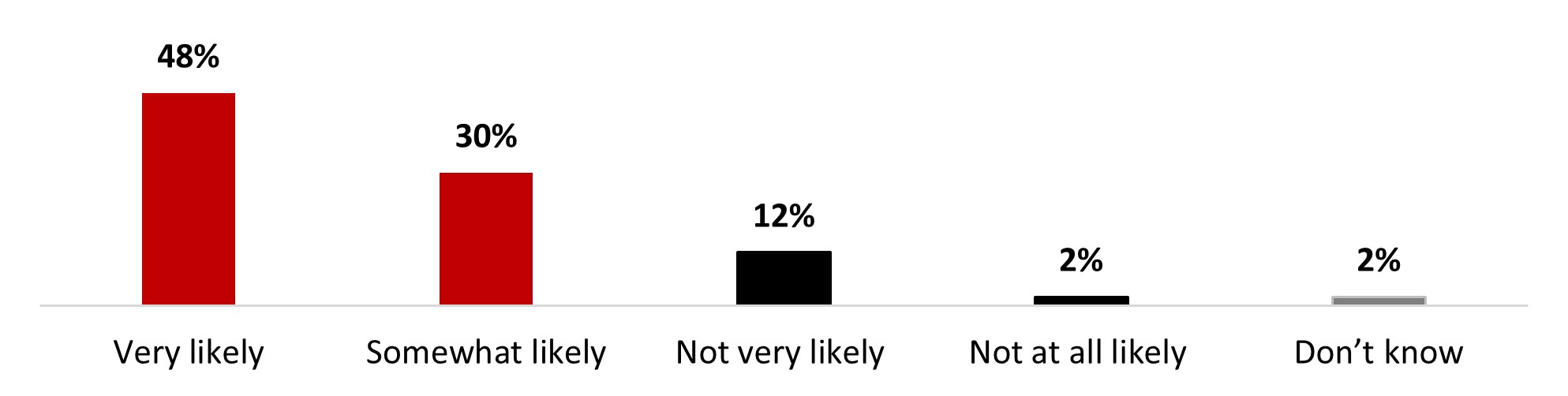
Figure 18.29: Text description
- Very likely
- 48%
- Somewhat likely
- 30%
- Not very likely
- 12%
- Not at all likely
- 2%
- Don't know
- 2%
Men (82%), those over 55 years old (85%), those who are not parents of any children under 18 at home (80%), and residents of British Columbia (83%) were the most likely to get vaccinated against COVID-19 twice a year.
Awareness of the bivalent vaccine was average: similar proportions of respondents were aware (44%) or unaware (47%) of the bivalent vaccine. Around one out of ten (9%) did not provide an answer.
Figure 18.30: Have you seen, read or heard anything about the bivalent COVID-19 vaccine?
Sample frame: All respondents (n=3,026)
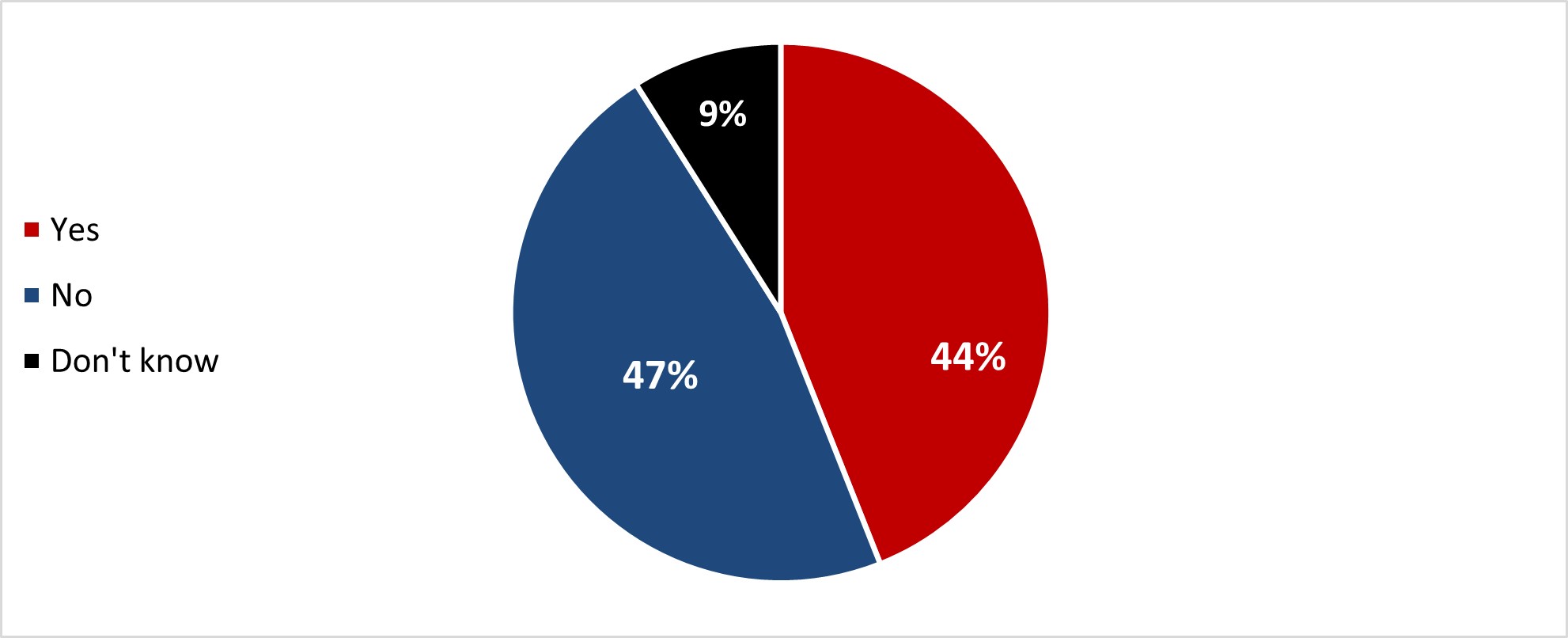
Figure 18.30: Text description
- Yes
- 44%
- No
- 47%
- Don't know
- 9%
Men (47%), those over 55 years old (57%), those who are not parents of children younger than 18 years old (47%), white-identifying individuals (47%), and those who have been previously infected with COVID-19 were all more likely to be aware of it (47%).
After reading an explanation about the bivalent COVID-19 vaccine, almost two out of five respondents (38%) said they were now more likely to get a bivalent booster dose. On the other hand, almost half of the respondents (46%) said their opinion didn't change, either because they were planning on it regardless (24%) or because they did not intend to get it (22%).
Figure 18.31: The bivalent COVID-19 vaccine targets the original COVID-19 and the omicron variant, which helps provide further protection against omicron strains. Based on this explanation, are you more or less likely to get a COVID-19 bivalent booster dose?
Sample frame: All respondents (n=3,026)
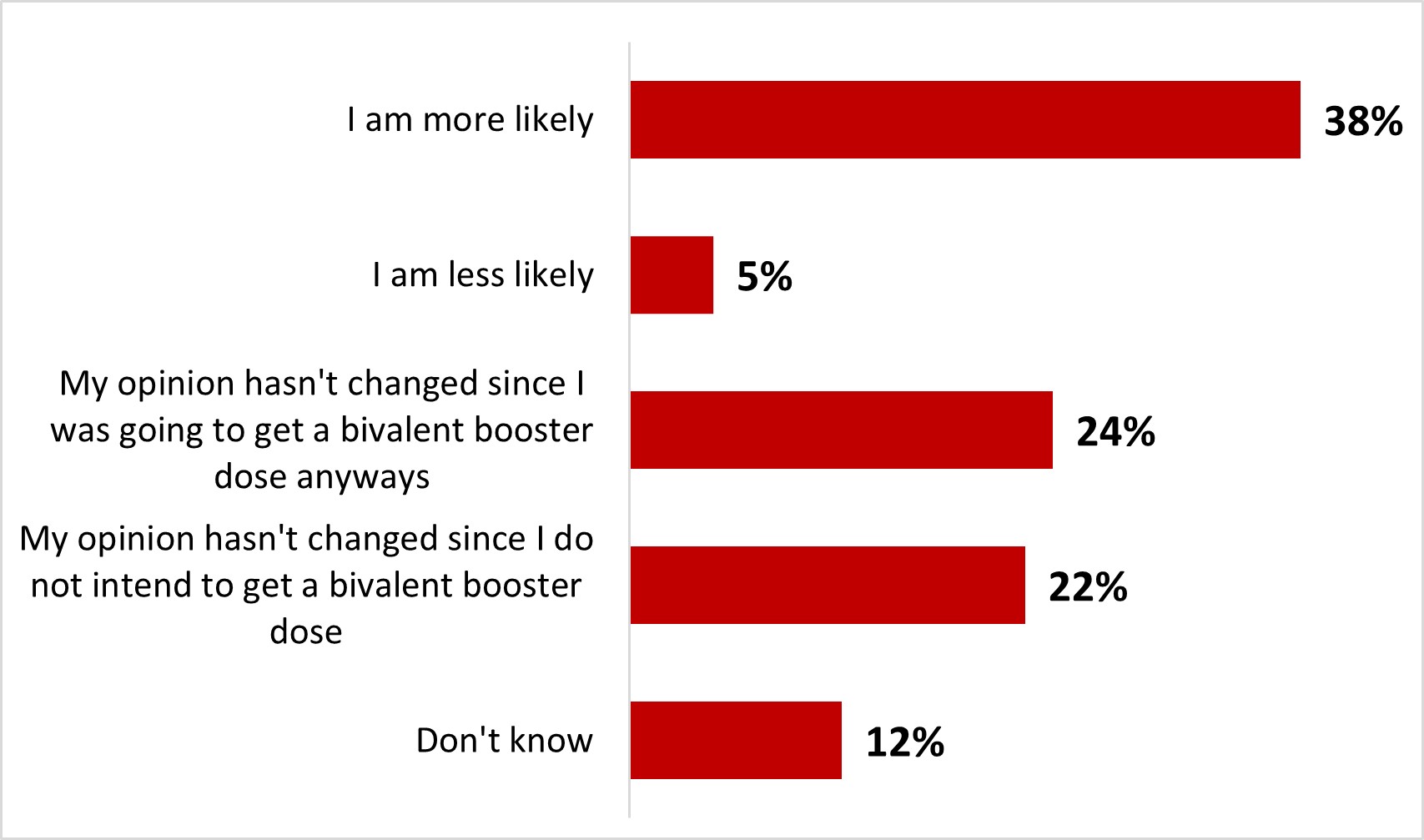
Figure 18.31: Text description
- I am more likely
- 38%
- I am less likely
- 5%
- My opinion hasn't changed since I was going to get a bivalent booster dose anyways
- 24%
- My opinion hasn't changed since I do not intend to get a bivalent booster dose
- 22%
- Don't know
- 12%
The following subgroups were significantly more likely to state they were more likely to get a bivalent booster:
- Men (40%)
- Those over 55 years old (48%)
- Those who are not parents of children younger than 18 (40%)
- Those who have already been infected with COVID-19 (41%)
2.3.1 COVID-19 childhood vaccination
Among parents or legal guardians of children aged 12 to 17, 90% reported that their children (12-17) had been vaccinated with at least one dose. More specifically, 6% of these respondents indicated that their children had received only one dose, 51% reported two doses, 26% reported three doses, and 8% reported four doses. Less than one out of ten respondents (9%) indicated that their children had not received any doses yet: 2% were waiting to decide whether the child(ren) would be vaccinated, and 7% were determined not to have their children aged 12 to 17 vaccinated.
Figure 18.32: Thinking about your child(ren) aged 12-17, how many doses of a COVID-19 vaccine have they received?
Sample frame: Parents or guardians of at least one child 12-17 (n=320)
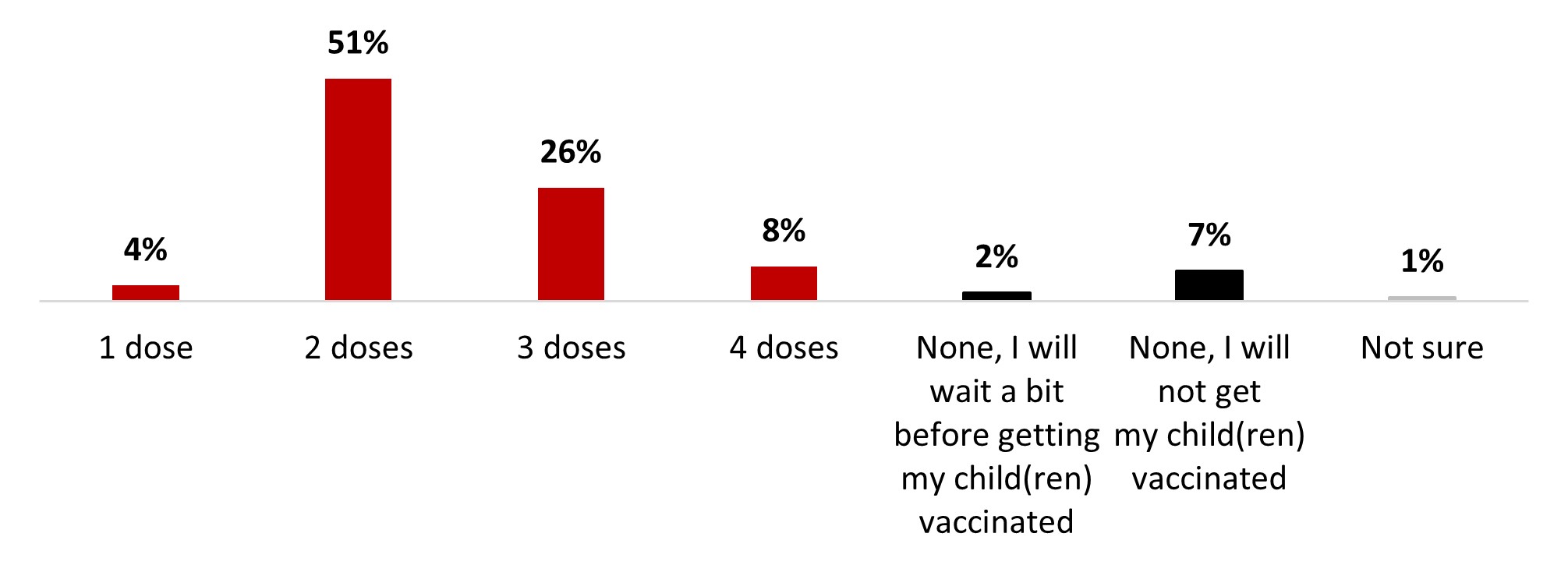
Figure 18.32: Text description
- 1 dose
- 4%
- 2 dose
- 51%
- 3 dose
- 26%
- 4 dose
- 8%
- None, I will wait a bit before getting my child(ren) vaccinated
- 2%
- None, I will not get my child(ren) vaccinated
- 7%
- Not Sure
- 1%
Respondents from British Columbia were significantly more likely to have vaccinated their children with four doses (26%).
Among parents or legal guardians of children aged 12 to 17, the likelihood of getting booster doses for their child was 49%: 21% very likely and 28% somewhat likely. Four out of ten respondents (42%) reported that it was unlikely they would seek out booster doses for their child(ren): 23% not very likely, and 19% not at all likely.
Figure 18.33: Thinking about your child(ren) aged 12-17, how likely are you to have them receive a booster dose of the COVID-19 vaccine?
Sample frame: Parents or guardians of at least one child 12-17 who has received one or two doses (n=175)
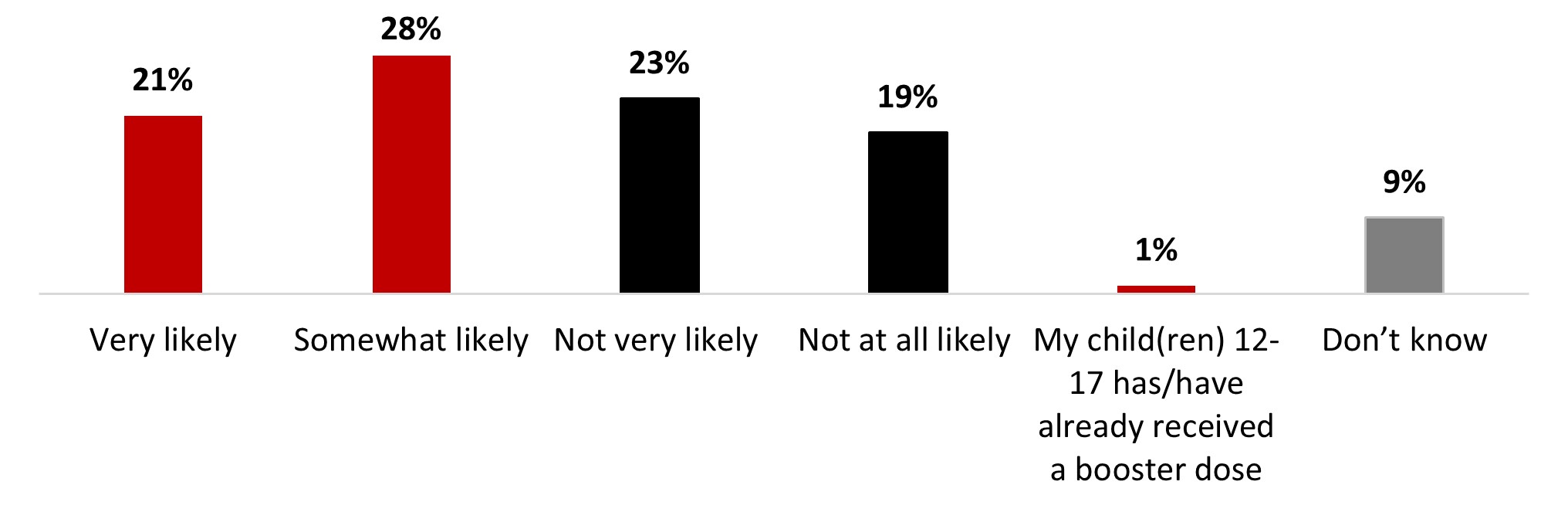
Figure 18.33: Text description
- Very likely
- 21%
- Somewhat likely
- 28%
- Not very likely
- 23%
- Not at all likely
- 19%
- My child(ren) 12-17 has/have already received a booster dose
- 1%
- Don't know
- 9%
Among parents or legal guardians of children aged five to 11, 65% indicated that their child(ren) had had at least one dose of the COVID-19 vaccine. More specifically, 9% reported one dose, 45% reported two doses, and 12% reported three doses. A third of those respondents (32%) indicated that their child(ren) had not received any doses yet: 11% indicated that they were waiting to decide, and 21% stated that their child(ren) would not be vaccinated.
Figure 18.34: Thinking about your child(ren) aged 5-11, how many doses of a COVID-19 vaccine have they received?
Sample frame: Parents or guardians of at least one child 5-11 (n=364)
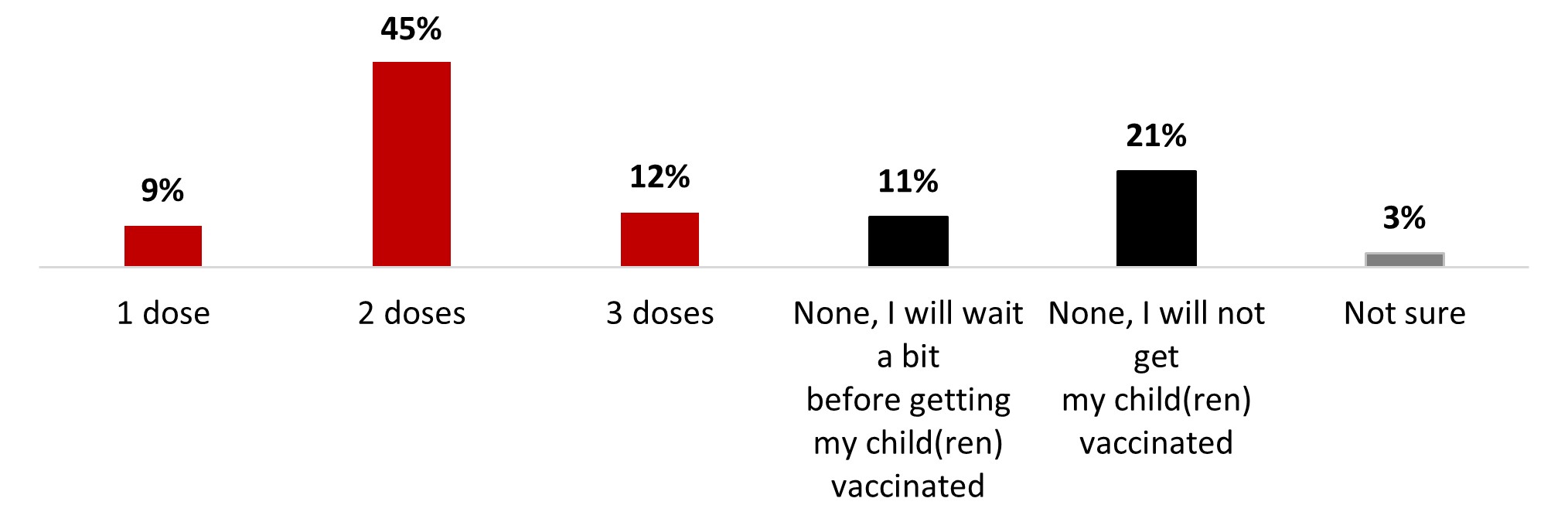
Figure 18.34: Text description
- 1 dose
- 9%
- 2 dose
- 45%
- 3 dose
- 12%
- None, I will wait a bit before getting my child(ren) vaccinated
- 11%
- None, I will not get my child(ren) vaccinated
- 21%
- Not sure
- 3%
Parents who are vaccinated against COVID-19 (72%) were more likely to have vaccinated their children with at least one dose.
Among parents or legal guardians of children aged five to 11 who received at least one dose, around six out of ten respondents (58%) reported that it was likely that their child(ren) would receive a booster dose: 26% very likely and 32% somewhat likely. In contrast, three out of ten respondents (29%) mentioned that it was unlikely they would get booster doses for their child(ren): 15% not very likely and 14% not at all likely.
Figure 18.35: Thinking about your child(ren) aged 5-11, how likely are you to have them receive a booster dose of the COVID-19 vaccine?
Sample frame: Parents or guardians of at least one child 5-11 who has received one or two doses (n=198)
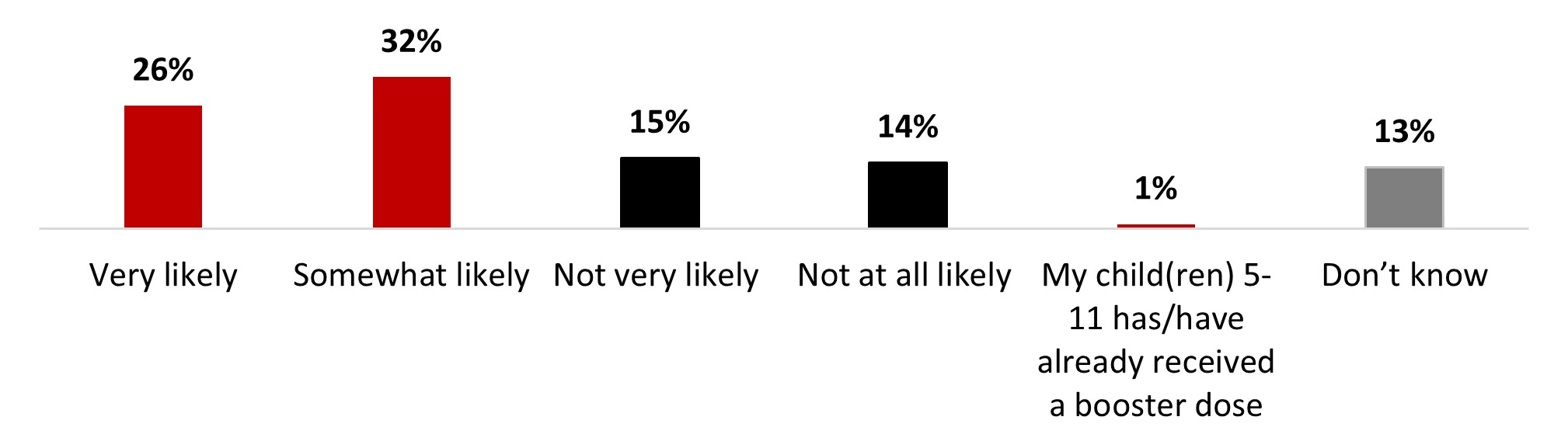
Figure 18.35: Text description
- Very likely
- 26%
- Somewhat likely
- 32%
- Not very likely
- 15%
- Not at all likely
- 14%
- My child(ren) 5-11 has/have already received a booster dose
- 1%
- Don't know
- 13%
Parents who speak English (66%) were more likely to have their children receive a booster of the COVID-19 vaccine.
The main reasons that parents of children aged five to 17 were reluctant to pick up booster doses for their child(ren) were: concerns about long-term effects (31%), concerns about the safety of the booster dose (17%), doubt about having to pick up booster doses after their child(ren) had been infected with COVID-19 (17%), the belief that their child(ren) was sufficiently protected with the doses they received (16%), preferring to wait a while before getting vaccinated (13%), and needing more information on booster doses (12%). Other reasons were mentioned by less than one person out of ten.
Figure 18.36: Why are you not likely or not sure to have your child(ren) get a booster dose of a COVID-19 vaccine?
Sample frame: Those who are unlikely to or don't know if they will have their children 5-11 or 12-17 get a booster dose (n=159)
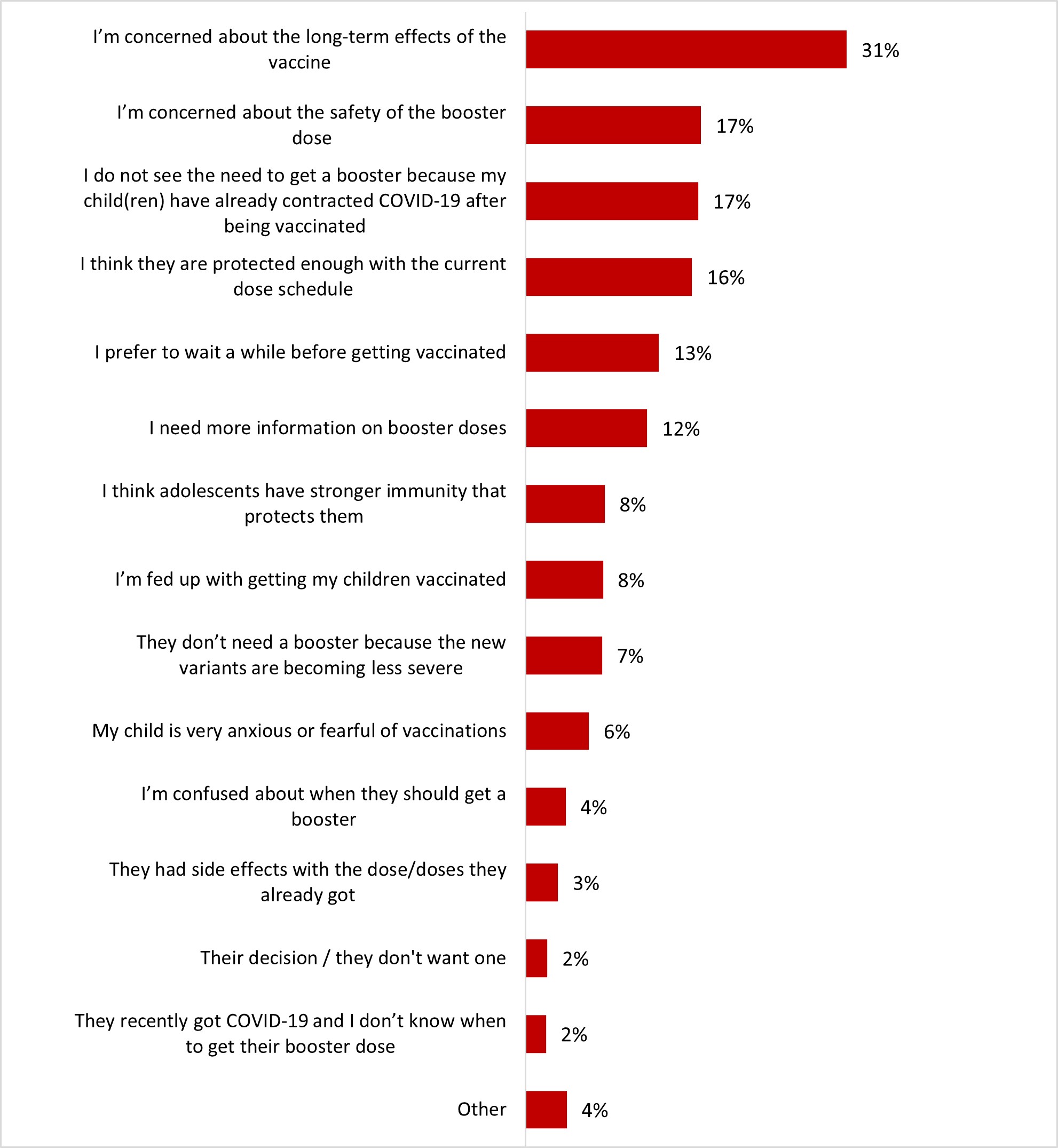
Figure 18.36: Text description
- I'm concerned about the long-term effects of the vaccine
- 31%
- I'm concerned about the safety of the booster dose
- 17%
- I do not see the need to get a booster because my child(ren) have already contracted COVID-19 after being vaccinated
- 17%
- I think they are protected enough with the current dose schedule
- 16%
- I prefer to wait a while before getting vaccinated
- 13%
- I need more information on booster doses
- 12%
- I think adolescents have stronger immunity that protects them
- 8%
- I'm fed up with getting my children vaccinated
- 8%
- They don't need a booster because the new variants are becoming less severe
- 7%
- My child is very anxious or fearful of vaccinations
- 6%
- I'm confused about when they should get a booster
- 4%
- They had side effects with the dose/doses they already got
- 3%
- Their decision / they don't want one
- 2%
- They recently got COVID-19 and I don't know when to get their booster dose
- 2%
- Other
- 4%
No relevant significant differences among subgroups are to be noted.
Among parents or guardians of children aged six months and under five years, the rate of vaccination of child(ren) in this age group was 21%. About four out of ten parents (41%) said they would wait to make a decision about vaccinating their child(ren), and one-third (35%) said they did not have any plans to have their child(ren) vaccinated.
Figure 18.37: Thinking about your child(ren) between the ages of 6 months and under 5, have they received at least one dose of a COVID-19 vaccine? Select all that apply.
Sample frame: Parents or guardians of at least one child between 6 months and under 5 years old (n=262)
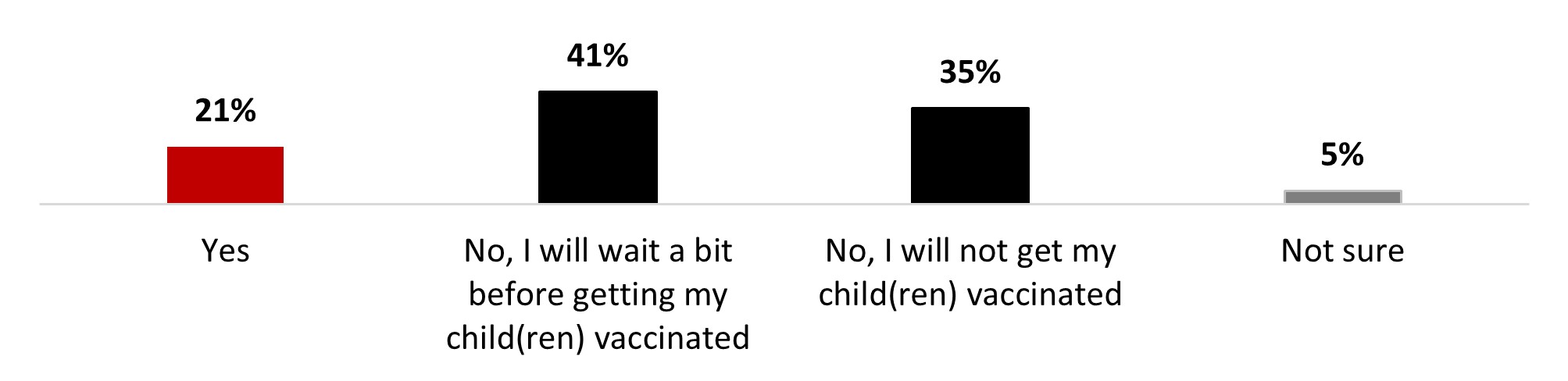
Figure 18.37: Text description
- Yes
- 21%
- No, I will wait a bit before getting my child(ren) vaccinated
- 41%
- No, I will not get my child(ren) vaccinated
- 35%
- Not sure
- 5%
No relevant significant differences are to be noted.
Among parents or legal guardians of children aged 6 months and under 5 years who do not intend to have their child(ren) vaccinated, the top three motivators to encourage vaccination were: having more information about children who have already received the vaccine (18%), having more information about the risks of COVID-19 for children (16%), and more information on how vaccines work and build immunity in children (12%). It is important to note that one-quarter of respondents (25%) mentioned that nothing would make them more likely to have their child(ren) vaccinated.
Figure 18.38: Which of the following factors would make you more likely to vaccinate your child(ren) against COVID-19? Up to 3 answers.
Sample frame: Parents or guardians of children 6 months and under 5 years who will not get their child vaccinated will wait a bit, or are not sure (n=217)
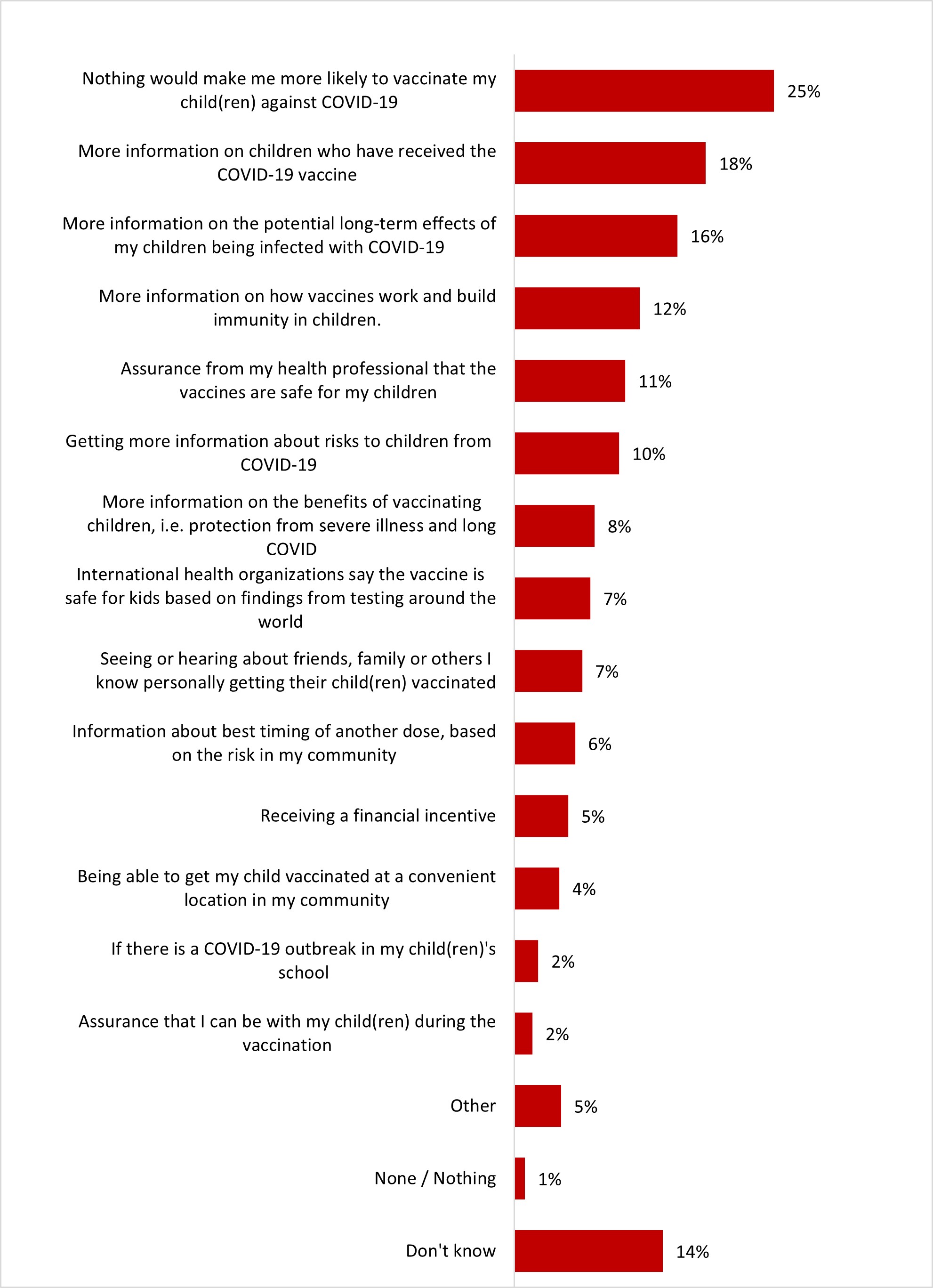
Figure 18.38: Text description
- Don't know
- 14%
- None / Nothing
- 1%
- Other
- 5%
- Assurance that I can be with my child(ren) during the vaccination
- 2%
- If there is a COVID-19 outbreak in my child(ren)'s school
- 2%
- Being able to get my child vaccinated at a convenient location in my community
- 4%
- Receiving a financial incentive
- 5%
- Information about best timing of another dose, based on the risk in my community
- 6%
- Seeing or hearing about friends, family or others I know personally getting their child(ren) vaccinated
- 7%
- International health organizations say the vaccine is safe for kids based on findings from testing around the world
- 7%
- More information on the benefits of vaccinating children, i.e. protection from severe illness and long COVID
- 8%
- Getting more information about risks to children from COVID-19
- 10%
- Assurance from my health professional that the vaccines are safe for my children
- 11%
- More information on how vaccines work and build immunity in children.
- 12%
- More information on the potential long-term effects of my children being infected with COVID-19
- 16%
- More information on children who have received the COVID-19 vaccine
- 18%
- Nothing would make me more likely to vaccinate my child(ren) against COVID-19
- 25%
Women and white-identifying individuals were more likely (25%) to mention needing more information on children who have received the COVID-19 vaccine.
After being presented with information about the bivalent COVID-19 vaccine, three out of ten parents of children younger than 18 years old (29%) stated they were more likely to have their child(ren) get a COVID-19 bivalent booster dose. While less than one out of ten said they were less likely (8%). Half of parents of children younger than 18 years old stated they did not change their opinion, either because they were planning on it regardless (19%) or because they still do not intend to get their children a bivalent booster dose (29%).
Figure 18.39: The bivalent COVID-19 vaccine targets the original COVID-19 virus strain and the omicron variant, which helps provide further protection against omicron strains. Based on this explanation, are you more or less likely to have your child(ren) get a COVID-19 bivalent booster dose?
Sample frame: Respondents who have children under 18 (n=789)
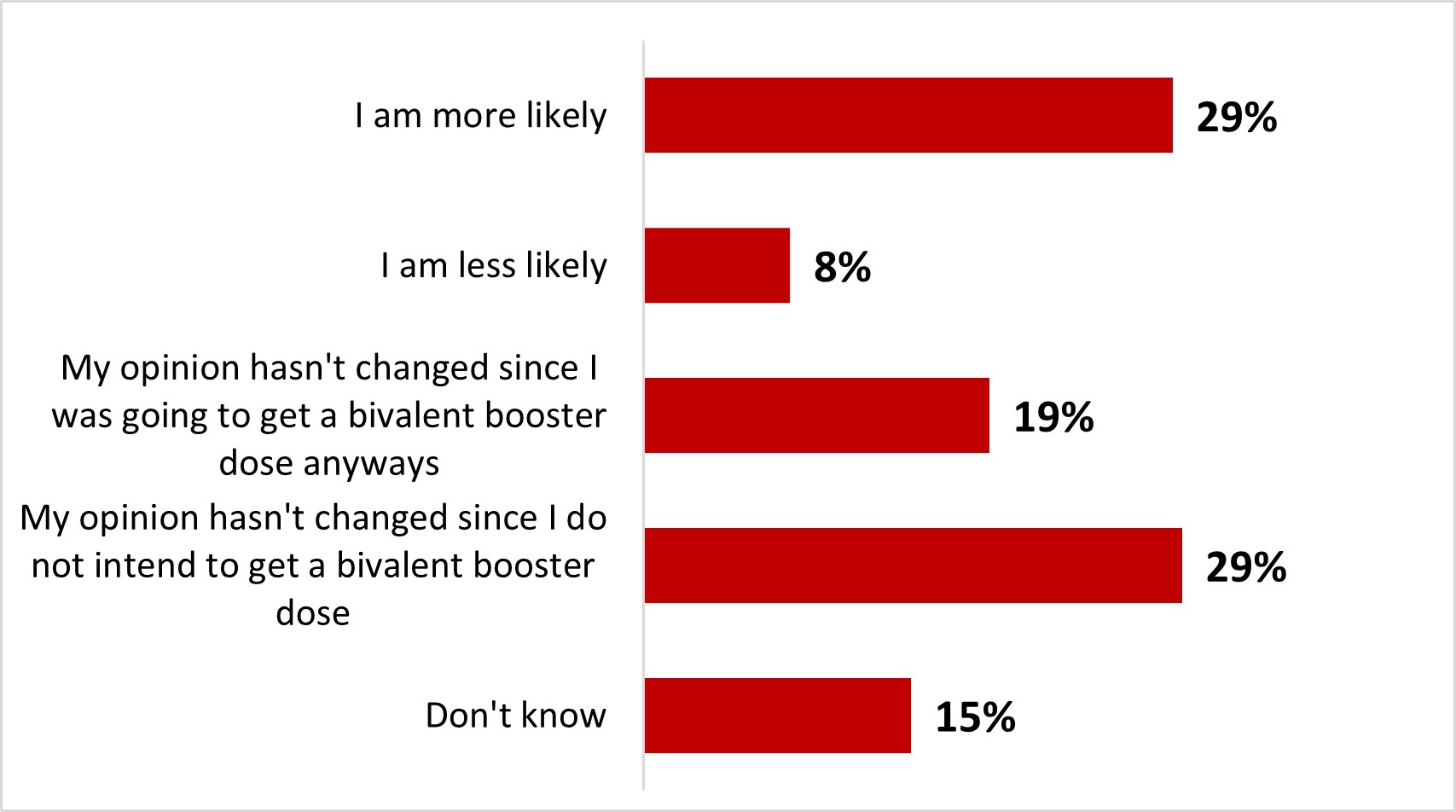
Figure 18.39: Text description
- I am more likely
- 29%
- I am less likely
- 8%
- My opinion hasn't changed since I was going to get a bivalent booster dose anyways
- 19%
- My opinion hasn't changed since I do not intend to get a bivalent booster dose
- 29%
- Don't know
- 15%
18-34 year-old parents of children younger than 18 years old were more likely to state it was less likely that they get their child(ren) a bivalent booster dose (14%), while vaccinated parents of children under 18 years old were more likely to consider it more likely (32%).
4.4 Confidence in vaccination
The COVID-19 pandemic did not have a positive or negative impact on vaccine confidence for half of the respondents. Indeed, 51% of respondents stated that their confidence level was about the same as before the pandemic. Around one in five respondents (20%) indicated that they were now more confident (10% a lot more and 9% somewhat more confident). In contrast, 24% of respondents indicated that they were now less confident (13% a lot less and 11% somewhat less confident) about vaccination in general.
Figure 18.40: Has the recent COVID-19 pandemic had an impact on your confidence in vaccinations in general?
Sample frame: All respondents (n=3,026)
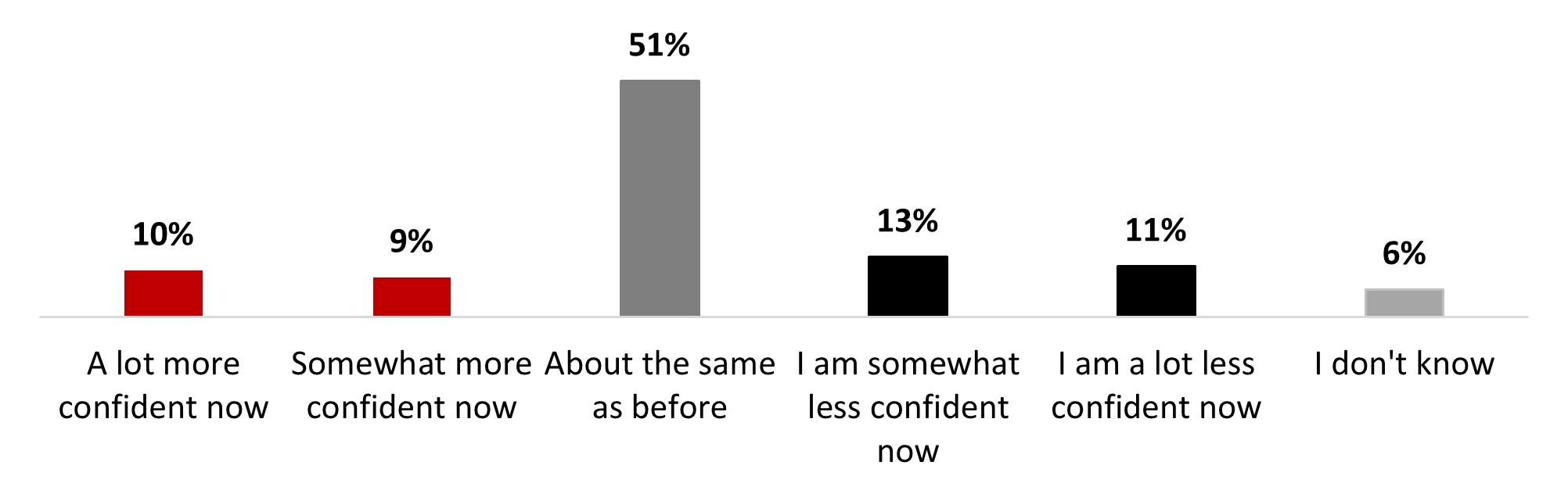
Figure 18.40: Text description
- A lot more confident now
- 10%
- Somewhat more confident now
- 9%
- About the same as before
- 51%
- I am somewhat less confident now
- 13%
- I am a lot less confident now
- 11%
- I don't know
- 6%
18-34 (31%) and 35-54 (27%) year-old individuals, Black-identifying individuals (33%), along with parents of children under 18 (32%), and those who were previously infected with COVID-19 (27%) were significantly more likely to state being somewhat less confident about vaccines now.
The main reasons mentioned by respondents who experienced a decrease in their level of confidence in vaccines were that the COVID-19 vaccines have had a detrimental impact on their perception of vaccines in general (43%), that they are now more concerned about the safety of vaccines in general (41%), the perception that the COVID-19 pandemic has shown that vaccines do not work well (28%), and belief that vaccines in general, do not have as much benefit in stopping the spread of viruses (28%). Around one out of four (26%) mentioned they now believed that vaccines do not have as much benefit in preventing severe outcomes (26%). Around one person out of ten (13%) mentioned that the COVID-19 pandemic has shown that we have strong immune systems without vaccines.
Figure 18.41: Why are you less confident in vaccinations? Select all that apply.
Sample frame: Those who are less confident in vaccines now than before the pandemic (n=741)
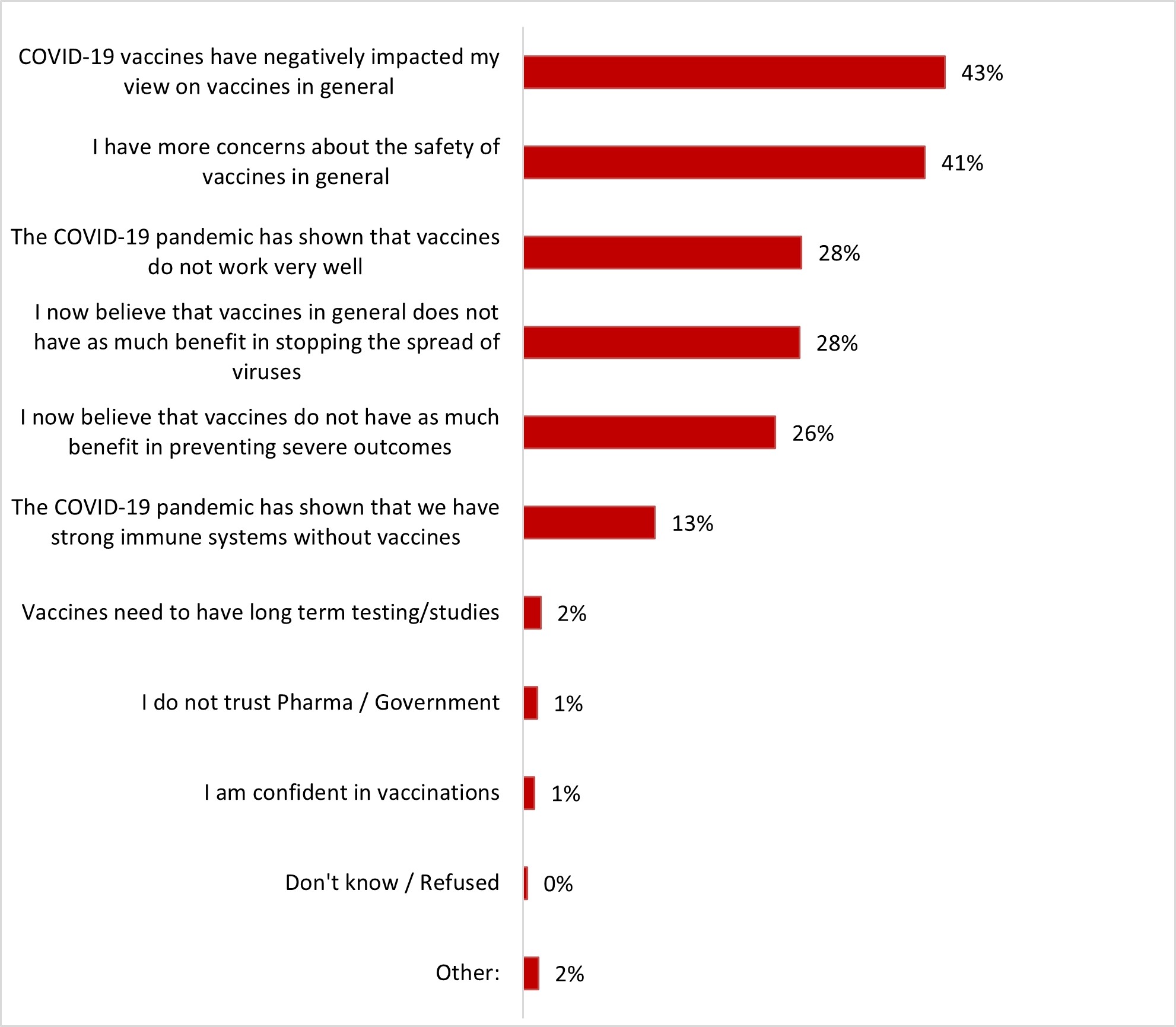
Figure 18.41: Text description
- COVID-19 vaccines have negatively impacted my view on vaccines in general
- 43%
- I have more concerns about the safety of vaccines in general
- 41%
- The COVID-19 pandemic has shown that vaccines do not work very well
- 28%
- I now believe that vaccines in general does not have as much benefit in stopping the spread of viruses
- 28%
- I now believe that vaccines do not have as much benefit in preventing severe outcomes
- 26%
- The COVID-19 pandemic has shown that we have strong immune systems without vaccines
- 13%
- Vaccines need to have long term testing/studies
- 2%
- I do not trust Pharma / Government
- 1%
- I am confident in vaccinations
- 1%
- Don't know / Refused
- 0%
- Other:
- 2%
Respondents 55 years of age or older (35%) and those from Quebec (37%) were significantly more likely to state that the pandemic has shown that vaccines do not work very well.
4.5 Flu vaccine
A quarter of respondents (24%) indicated that they intend to take the flu vaccine this year, and almost the same proportion indicated having already received it. More than four respondents out of ten indicated not having the intention to get the flu vaccine this year.
Figure 18.42: Do you intend to get the flu vaccine this year?
Sample frame: All respondents (n=3,026)
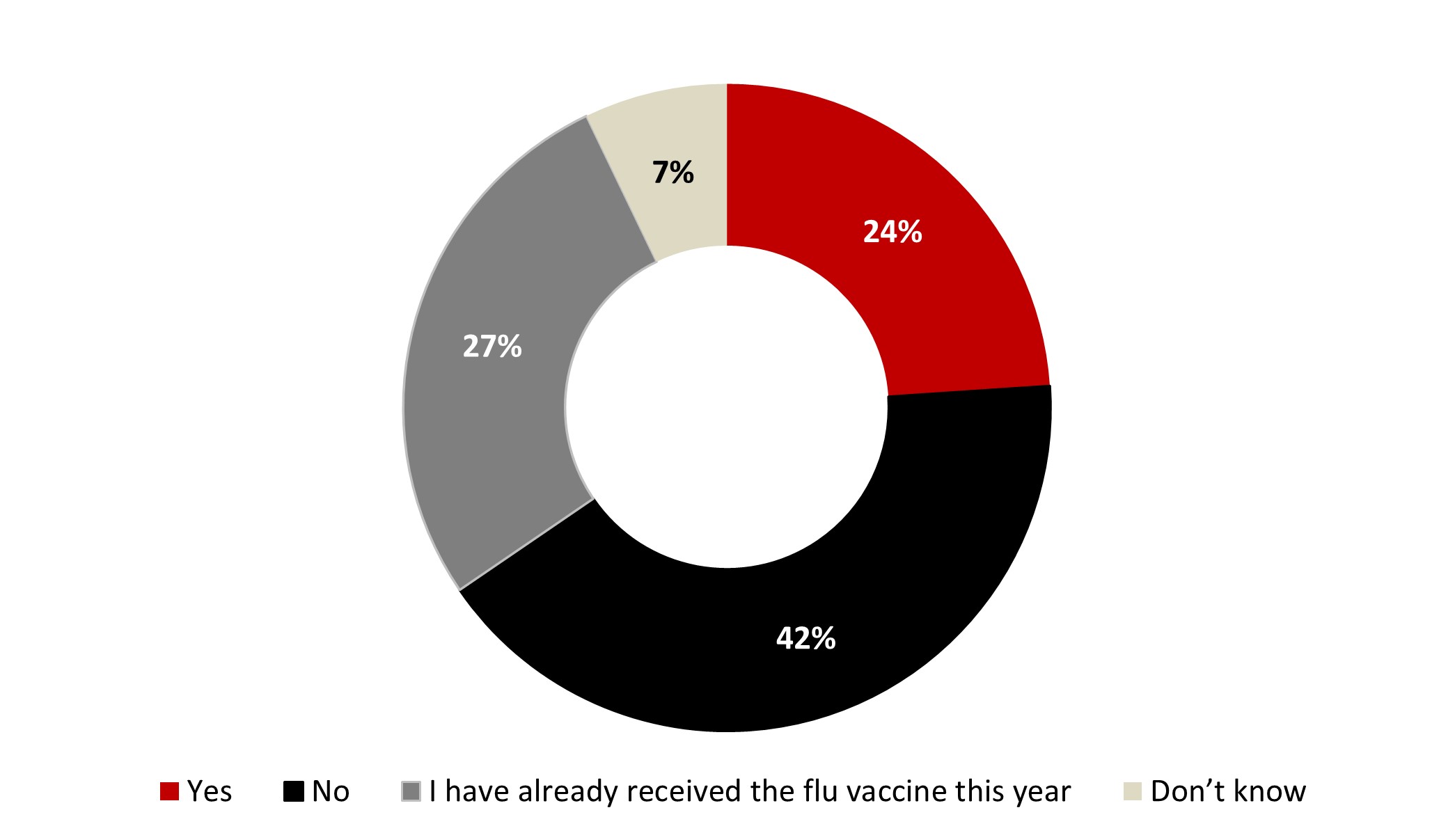
Figure 18.42: Text description
- Yes
- 24%
- No
- 42%
- I have already received the flu vaccine this year
- 27%
- Don't know
- 7%
The following subgroups were significantly more likely to intend on getting the flu vaccine this year:
- Respondents who have the intention to get the COVID-19 vaccine and the flu vaccine at the same time (38%)
- Respondents who received three doses (27%), four doses (29%) or five doses (31%) of the COVID-19 vaccine
- Those over 55 years old (27%)
The main reason respondents gave for not intending to get the flu vaccine was that they had never had the flu shot before (48%). Other reasons mentioned are that they have the perception of being healthy and never catching the flu (18%), concerns about side effects of the flu shot (13%), the perception that the flu doesn't really make them sick (10%) or that the flu shot doesn't work (10%). The other reasons were all mentioned by less than 10% of respondents.
Figure 18.43: Why do you not intend to get your flu shot this year? Select all that apply.
Sample frame: Those who do not intend or do not know if they intend on getting the flu shot this year (n=1,544)
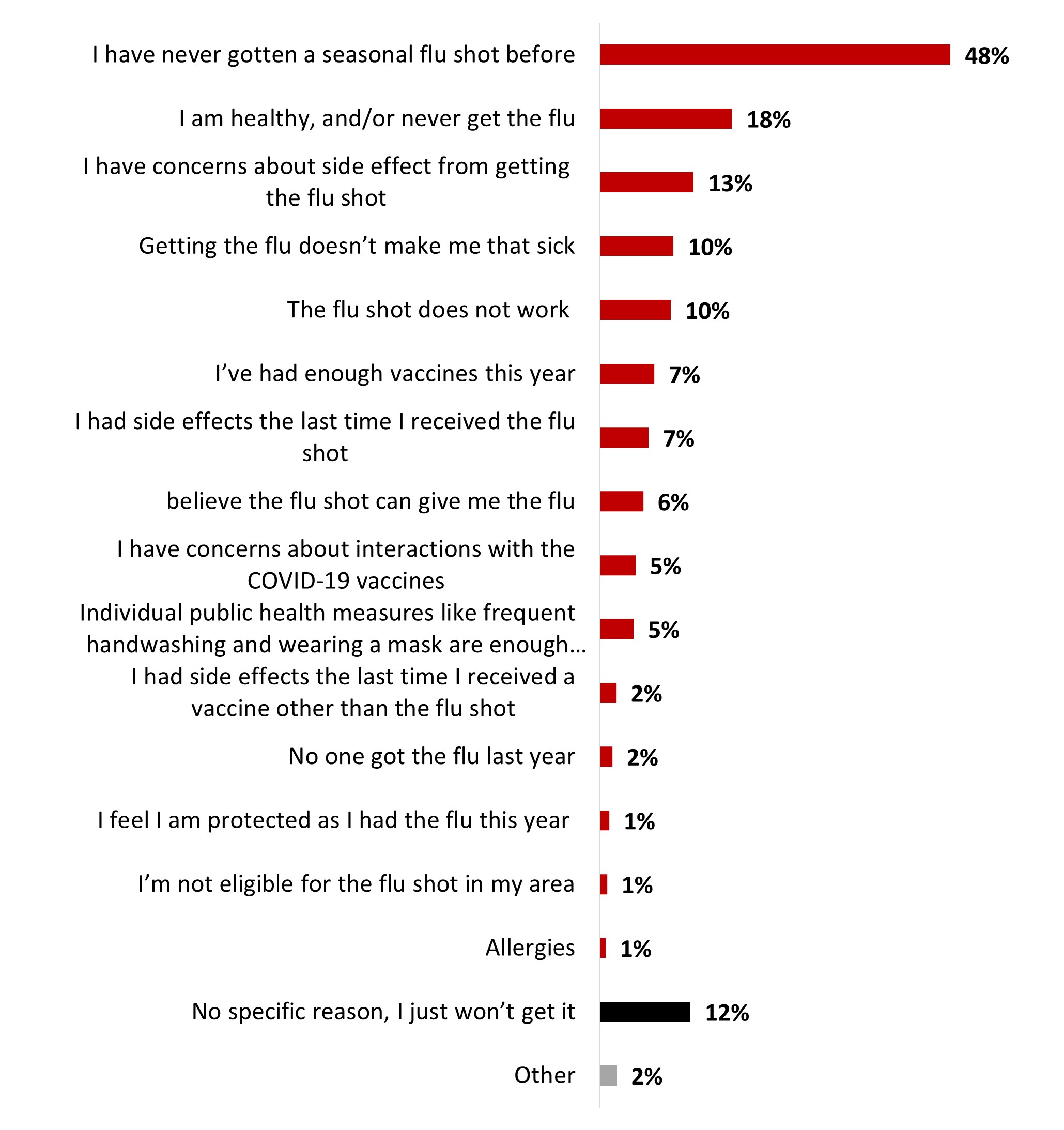
Figure 18.43: Text description
- I have never gotten a seasonal flu shot before
- 48%
- I am healthy, and/or never get the flu
- 18%
- I have concerns about side effect from getting the flu shot
- 13%
- Getting the flu doesn't make me that sick
- 10%
- The flu shot does not work
- 10%
- I've had enough vaccines this year
- 7%
- I had side effects the last time I received the flu shot
- 7%
- believe the flu shot can give me the flu
- 6%
- I have concerns about interactions with the COVID-19 vaccines
- 5%
- Individual public health measures like frequent handwashing and wearing a mask are enough to protect me from the flu
- 5%
- I had side effects the last time I received a vaccine other than the flu shot
- 2%
- No one got the flu last year
- 2%
- I feel I am protected as I had the flu this year
- 1%
- I'm not eligible for the flu shot in my area
- 1%
- Allergies
- 1%
- No specific reason, I just won't get it
- 12%
- Other
- 2%
Respondents from Quebec were significantly more likely to state that:
- They had never gotten a flu shot before (53%)
Women are more likely to state that:
- They have concerns about side effects (16%)
- It does not work (12%)
Men are more likely to state that:
- They are healthy and/or they never get the flu (22%)
More than half of respondents (54%) indicated that no factors can motivate them to get the flu shot. Less than one out of ten respondents mentioned some factors, including a shot being made mandatory (9%), knowing that getting the shot can protect them from severe outcomes (8%), receiving advice from their primary health care provider (8%) or getting the flu shot at a convenient time and location (8%).
Figure 18.44: Among the following factors, what would motivate you to get a flu shot this year?
Sample frame: Those who do not intend or do not know if they intend on getting the flu shot this year (n=1,544)
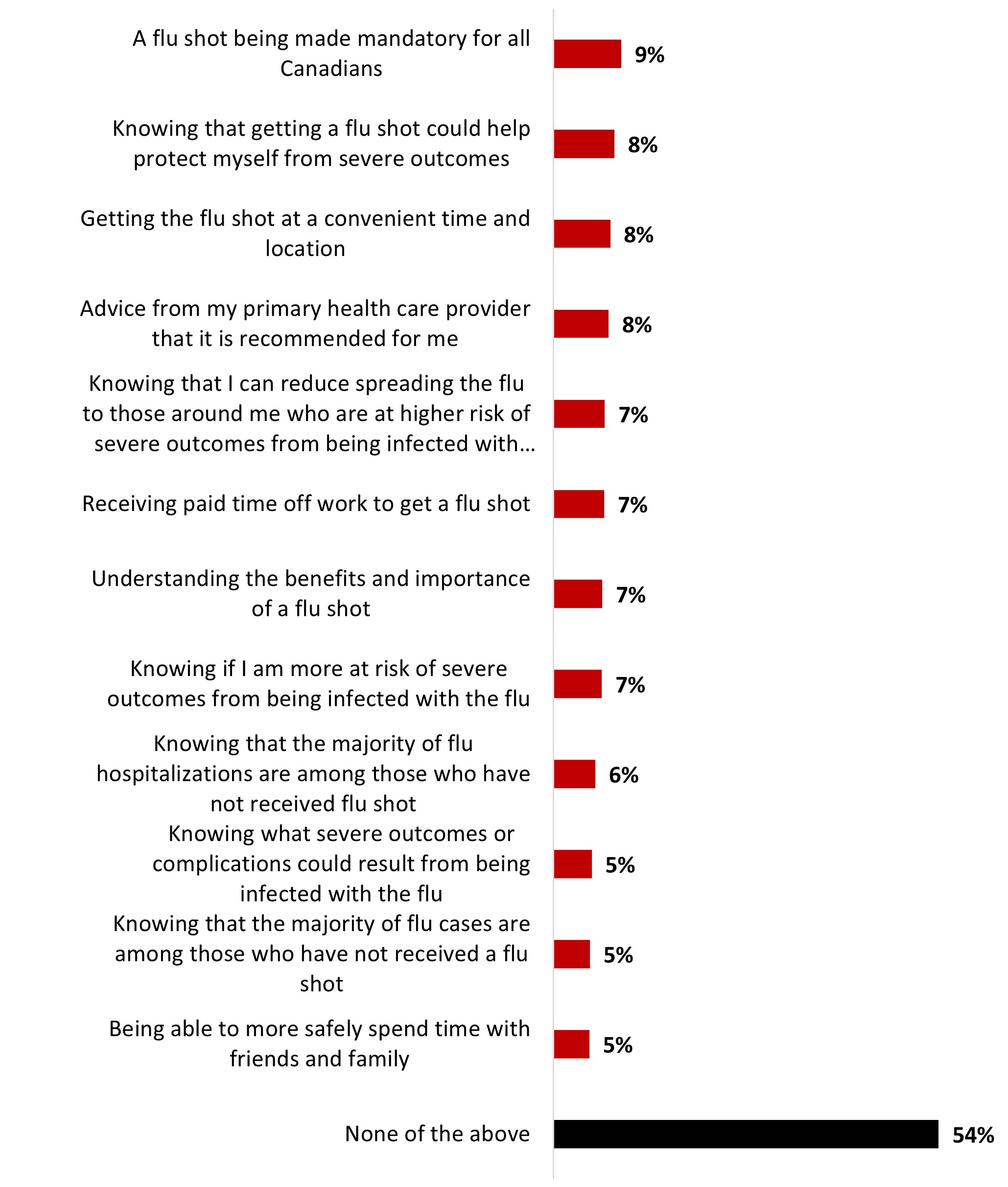
Figure 18.44: Text description
- A flu shot being made mandatory for all Canadians
- 9%
- Knowing that getting a flu shot could help protect myself from severe outcomes
- 8%
- Getting the flu shot at a convenient time and location
- 8%
- Advice from my primary health care provider that it is recommended for me
- 8%
- Knowing that I can reduce spreading the flu to those around me who are at higher risk of severe outcomes from being infected with the flu
- 7%
- Receiving paid time off work to get a flu shot
- 7%
- Understanding the benefits and importance of a flu shot
- 7%
- Knowing if I am more at risk of severe outcomes from being infected with the flu
- 7%
- Knowing that the majority of flu hospitalizations are among those who have not received flu shot
- 6%
- Knowing what severe outcomes or complications could result from being infected with the flu
- 5%
- Knowing that the majority of flu cases are among those who have not received a flu shot
- 5%
- Being able to more safely spend time with friends and family
- 5%
- None of the above
- 54%
The following subgroups were significantly more likely to indicate that no factor would motivate them to get the flu shot this year:
- Respondents who are not vaccinated against COVID-19 (86%)
- 35-54 year-olds (59%)
- White-identifying respondents (58%)
4.6 Public health measures
Staying home and away from others if you feel sick (81%) is the most regularly adopted individual protection measure. Two measures are adopted regularly by over half of respondents: wearing a mask inside with others when feeling sick (59%) and using individual public health measures when interacting with someone who is at risk of more severe disease or outcomes from COVID-19 (56%). Other personal protection measures were less regularly adopted.
Table 18.45: How often do you follow each of the following individual public health measures?
Sample frame: All respondents (n=3,026)
NET always + often
- Staying home and away from others if you feel sick
- 81%
- earing a mask – inside with others when you're feeling sick
- 59%
- Using individual public health measures when interacting with someone who is at risk of more severe disease or outcomes from COVID-19
- 56%
- Wearing a mask–when indoors in a public space or in an indoor space with people from outside your immediate household.
- 46%
- Improving ventilation / Improving ventilation when people from outside your immediate household are in your home
- 37%
- Wearing a mask– when outside in a public space
- 25%
The following tables detail the significant differences between subgroups according to age, ethnicity, parental status, and region.
Reading note: In the following tables, significantly lower differences are marked with a "-" sign, while significantly higher differences are marked with a "+".
Table 18.46: How often do you follow each of the following individual public health measures?
Sample frame: All respondents (n=3,026)
Reading note: Significantly lower differences are marked with a "-" sign, while significantly higher differences are marked with a "+".
| Gender | Age | Parents of children under 18 | Ethnicity | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | 18-34 | 35-54 | 55+ | Yes | No | White | Indigenous | Black | |
| Staying home and away from others if you feel sick | 77% - | 85% + | 67% - | 80% | 91% + | 75% - | 83% + | 81% | 79% | 81% |
| Wearing a mask – inside with others when you're feeling sick | 57% | 61% | 49% - | 56% - | 68% + | 54% - | 61% + | 56% - | 58% | 68% + |
| Using individual public health measures when interacting with someone who is at risk of more severe disease or outcomes from COVID-19 | 52% - | 60% + | 46% - | 55% | 63% + | 55% | 56% | 54% - | 59% | 67% + |
| Wearing a mask–when indoors in a public space or in an indoor space with people from outside your immediate household. | 47% | 46% | 37% - | 42% - | 56% + | 43% - | 48% + | 43% - | 41% | 52% |
| Improving ventilation / Improving ventilation when people from outside your immediate household are in your home | 37% | 37% | 36% | 40% | 36% | 43% + | 35% - | 33% - | 41% | 54% + |
| Wearing a mask– when outside in a public space | 23% | 26% | 24% | 24% | 25% | 28% + | 23% - | 20% - | 20% | 38% + |
Table 18.47: How often do you follow each of the following individual public health measures?
Sample frame: All respondents (n=3,026)
Reading note: Significantly lower differences are marked with a "-" sign, while significantly higher differences are marked with a "+".
| British Columbia + Territories | Alberta | Manitoba / Saskatchewan | Ontario | Quebec | Atlantic | |
|---|---|---|---|---|---|---|
| Staying home and away from others if you feel sick | 83% | 78% | 78% | 82% | 81% | 78% |
| Wearing a mask – inside with others when you're feeling sick | 59% | 51% - | 52% | 61% | 63% | 56% |
| Using individual public health measures when interacting with someone who is at risk of more severe disease or outcomes from COVID-19 | 56% | 52% | 50% | 58% | 56% | 57% |
| Wearing a mask–when indoors in a public space or in an indoor space with people from outside your immediate household. | 50% | 36% - | 39% - | 51% + | 43% | 47% |
| Improving ventilation / Improving ventilation when people from outside your immediate household are in your home | 33% | 30% - | 27% - | 39% | 43% + | 35% |
| Wearing a mask– when outside in a public space | 23% | 19% - | 22% | 27% + | 25% | 25% |
A high proportion of respondents mentioned they thought that personal protective measures help reduce the transmission of respiratory diseases (84%): by a great deal (55%) or somewhat (29%). In contrast, about one out of ten respondents (11%) indicated that they did not believe this was the case: not very much (7%) and not at all (4%).
Figure 18.48: Many individual public health measures (e.g., staying home when sick, handwashing, mask-wearing) were recommended in 2020 to help control the spread of COVID-19. How much do you think these individual public health measures could help reduce the spread of other respiratory infectious diseases, such as seasonal influenza (the flu)?
Sample frame: All respondents (n=3,026)
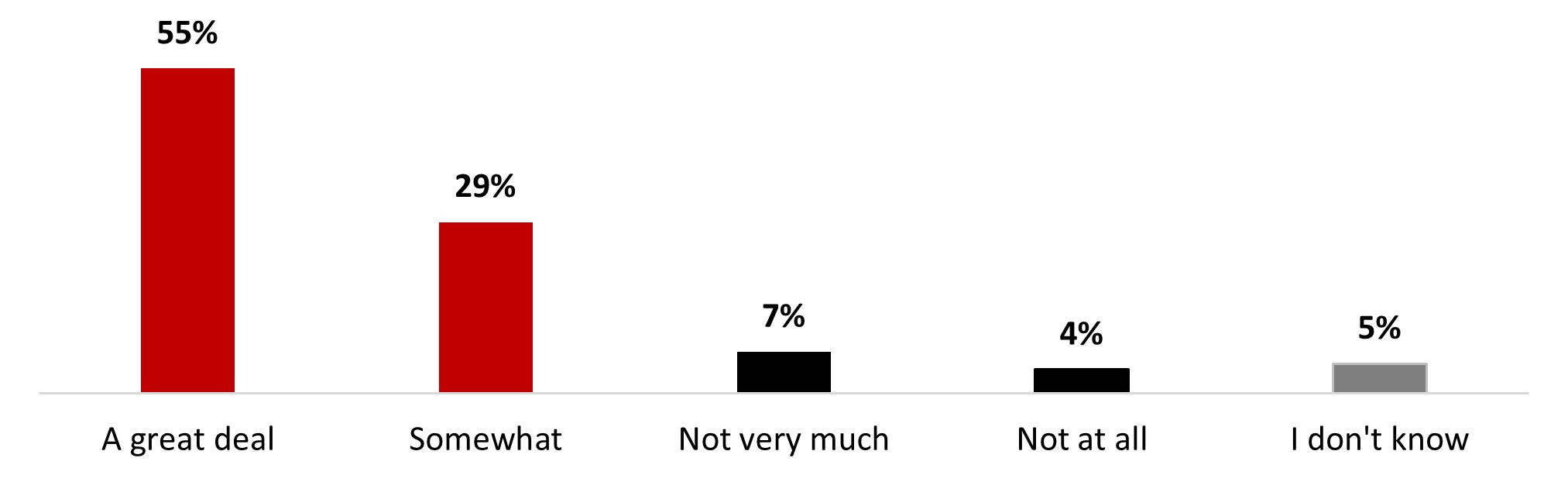
Figure 18.48: Text description
- A great deal
- 55%
- Somewhat
- 29%
- Not very much
- 7%
- Not at all
- 4%
- I don't know
- 5%
The following subgroups were significantly more likely to consider that individual public health measures help a great deal or somewhat reduce the spread of other respiratory infectious diseases:
- Those who have received four doses (95%) or five doses (97%) of the COVID-19 vaccine
- Respondents over 55 years old (92%)
- Those with a university degree (87%)
- Women (86%)
Half of the respondents (51%) indicated that they would agree with reinstating mandatory public health measures: a quarter (25%) would strongly agree, and about the same proportion would somewhat agree (26%). About a third of respondents (29%) would disagree either strongly (19%) or somewhat (10%). A little less than one respondent out of five (16%) would neither agree nor disagree.
Figure 18.49: To what extent would you agree or disagree with reinstating mandatory public health measures (e.g. policies on masking, or capacity limits)?
Sample frame: All respondents (n=3,026)
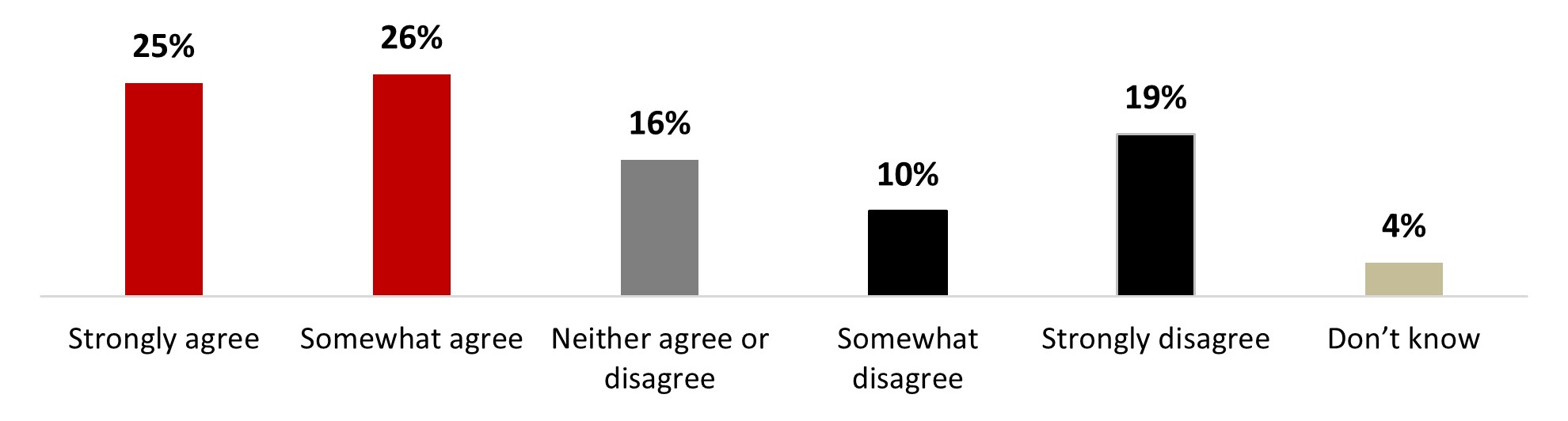
Figure 18.49: Text description
- Strongly agree
- 25%
- Somewhat agree
- 26%
- Neither agree or disagree
- 16%
- Somewhat disagree
- 10%
- Strongly disagree
- 19%
- Don't know
- 4%
The following subgroups were significantly more likely to agree with the reinstating of mandatory public measures:
- Respondents over 55 years old (62%)
- Ontario residents (56%)
- Respondents with a university degree (56%)
- Those who are not parents of children younger than 18 years old (52%)
The following subgroups were significantly more likely to disagree with the reinstating of mandatory public measures:
- Those who are not vaccinated (69%)
- Quebec residents (37%)
- 35-54 year-olds (34%)
- Women (31%)
Half of the respondents (50%) would agree with reinstating mandatory public measures if there was a rising number of hospitalizations related to COVID-19. About the same proportion would agree if the health care or public health capacities are becoming overloaded (46%) or if there was a rising number of deaths related to COVID-19 (45%). Around four out of ten respondents would agree to reinstate the public measures if there was a local outbreak of COVID-19 cases (43%), if the spread of COVID-19 is increasing (41%) or if there are new variants (38%). A quarter of respondents would agree if there were other viruses in circulation (26%), and the same proportion (24%) would not agree with reinstating the measure under any conditions.
Figure 18.50: Under what conditions would you support reinstating mandatory public health measures (e.g. policies on masking, or capacity limits) Select all that apply
Sample frame: All respondents (n=3,026)
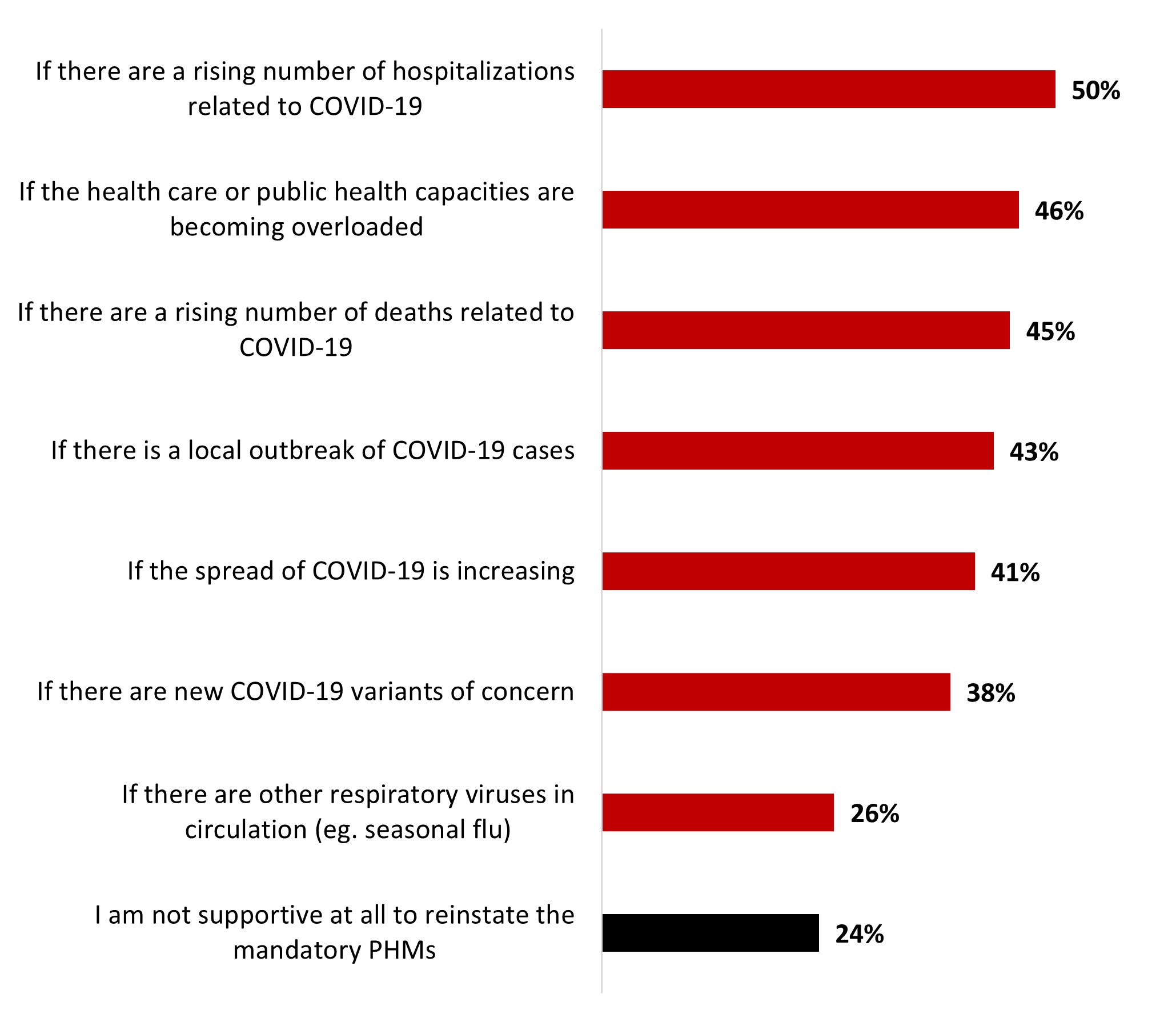
Figure 18.50: Text description
- If there are a rising number of hospitalizations related to COVID-19
- 50%
- If the health care or public health capacities are becoming overloaded
- 46%
- If there are a rising number of deaths related to COVID-19
- 45%
- If there is a local outbreak of COVID-19 cases
- 43%
- If the spread of COVID-19 is increasing
- 41%
- If there are new COVID-19 variants of concern
- 38%
- If there are other respiratory viruses in circulation (eg. seasonal flu)
- 26%
- I am not supportive at all to reinstate the mandatory PHMs
- 24%
The following subgroups were significantly more likely not to be supportive at all to reinstate the mandatory public health measures:
- Respondents who are not vaccinated (79%)
- Ontario residents (30%)
- 35-54 year-olds (29%)
- Parents of children younger than 18 years old (29%)
Table 18.51: Under what conditions would you support reinstating mandatory public health measures (e.g. policies on masking, or capacity limits) Select all that apply
Sample frame: All respondents (n=3,026)
The following table details the significant differences between subgroups according to age, ethnicity, and parental status.
Reading note: In the following table, significantly lower differences are marked with a "-" sign, while significantly higher differences are marked with a "+".
| Gender | Age | Parents of children under 18 | Ethnicity | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | 18-34 | 35-54 | 55+ | Yes | No | White | Indigenous | Black | ||
| If there are a rising number of hospitalizations related to COVID-19 | 49% | 50% | 43% - | 44% - | 59% + | 42% - | 53% + | 49% | 42% - | 46% | |
| If the health care or public health capacities are becoming overloaded | 44% | 47% | 35% - | 41% - | 57% + | 37% - | 49% + | 48% + | 35% - | 35% - | |
| If there are a rising number of deaths related to COVID-19 | 43% | 46% | 37% - | 41% - | 53% + | 39% - | 47% + | 46% | 40% | 39% | |
| If there is a local outbreak of COVID-19 cases | 43% | 43% | 36% - | 37% - | 52% + | 37% - | 46% + | 42% | 37% | 39% | |
| If the spread of COVID-19 is increasing | 38% - | 44% + | 30% - | 34% - | 53% + | 34% - | 44% + | 42% | 37% | 35% - | |
| If there are new COVID-19 variants of concern | 37% | 40% | 26% - | 33% - | 51% + | 29% - | 42% + | 40% + | 34% | 30% - | |
| If there are other respiratory viruses in circulation (eg. seasonal flu) | 23% - | 28% + | 15% - | 22% - | 35% + | 21% - | 28% + | 27% + | 20% | 22% | |
2.6.1 Long COVID
Around two-thirds of respondents mentioned being familiar with long-COVID (64%): around one out of ten stated being very familiar (13%), and half were somewhat familiar (51%). On the other hand, one out of four was not very familiar (22%), and 9% were not at all familiar.
Figure 18.52: How familiar are you with the potential long-term effects of having COVID-19 (also known as "long-COVID" or "post COVID-19 condition")?
Sample frame: All respondents (n=3,026)
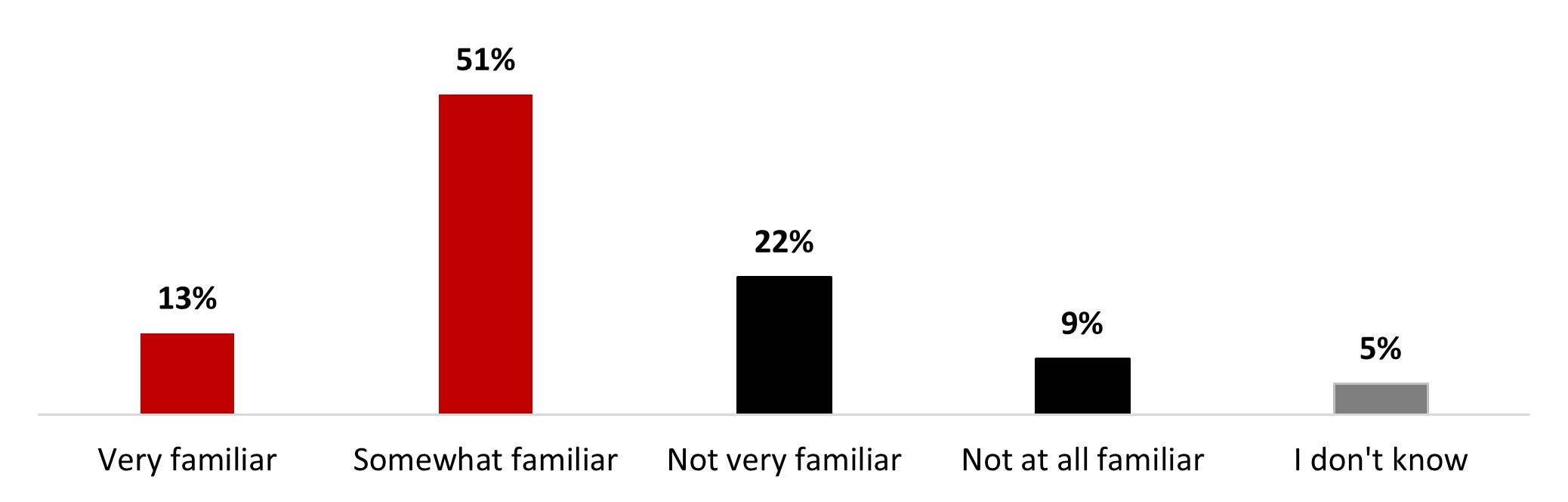
Figure 18.52: Text description
- Very familiar
- 13%
- Somewhat familiar
- 51%
- Not very familiar
- 22%
- Not at all familiar
- 9%
- I don't know
- 5%
The following subgroups were significantly more likely to state being very or somewhat familiar with long-COVID:
- Alberta residents (72%)
- Respondents who received four doses (71%) or five doses (74%) of the COVID-19 vaccine
- Those with a university degree (71%)
- Women (67%)
- Those who have been infected with COVID-19 (66%)
Six out of ten respondents (60%) mentioned being worried about developing long-term symptoms from a COVID-19 infection. More specifically, about one out of five people stated being very worried (19%), while more than a third were somewhat worried (40%). Around one out of five respondents were not very worried (22%), and 12% were not at all worried.
Figure 18.53: How worried are you/would you be about developing longer-term symptoms from a COVID-19 infection?
Sample frame: All respondents (n=3,026)
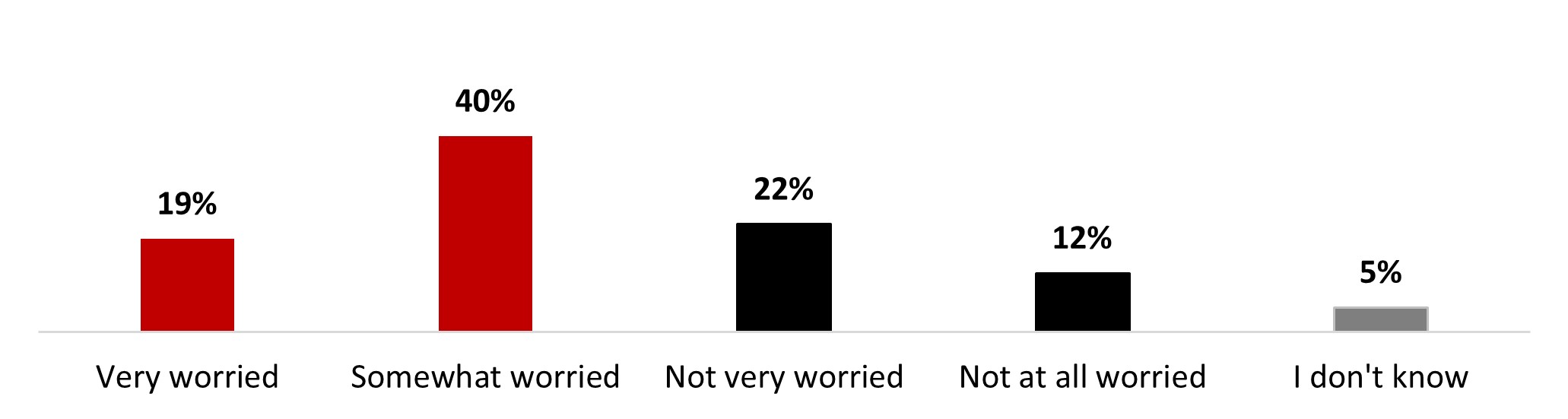
Figure 18.53: Text description
- Very worried
- 19%
- Somewhat worried
- 40%
- Not very worried
- 22%
- Not at all worried
- 12%
- I don't know
- 5%
The following subgroups were significantly more likely to state being worried about developing longer-term symptoms from a COVID-19 infection:
- Respondents who are worried about catching COVID-19 (88%)
- Respondents who received four doses (73%) or five doses (76%) of the COVID-19 vaccine
- Respondents with a disability (67%)
- Respondents over 55 years old (66%)
- Respondents with a university degree (66%)
- Women (64%)
Uncertainty about future health prospects and limitations to leisure/personal life were the two main reasons for worrying about long-COVID for around two-thirds of respondents (68% and 63%, respectively). A third of respondents were worried about limitations to their working life (35%) and lack of information/resources on the condition (32%). Around one person out of four mentioned the following:
- Being worried about the lack of public acknowledgement from authority figures (27%),
- not knowing if others would take their condition seriously (22%),
- difficulty in accessing benefits related to the condition (22%).
Less than one person out of five was worried because of difficulty in formally indicating their condition (16%), and around one person out of ten was worried about being terminated by their employer (10%) and being judged (9%).
Figure 18.54: What makes/would make you feel worried about long-term symptoms of COVID? Select all that apply.
Sample frame: Those who are worried about developing longer-term symptoms from COVID-19 (n=1,796)
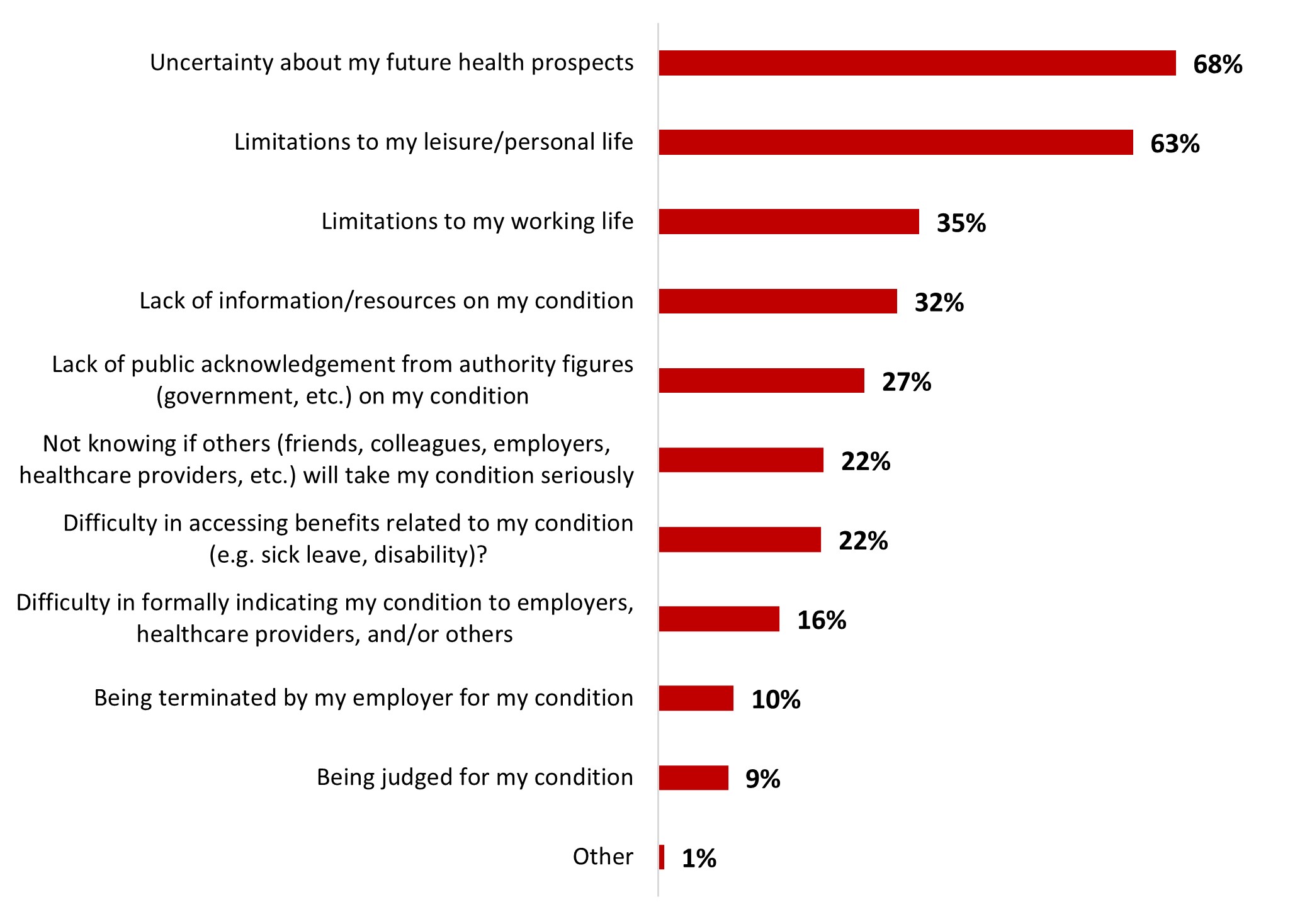
Figure 18.54: Text description
- Uncertainty about my future health prospects
- 68%
- Limitations to my leisure/personal life
- 63%
- Limitations to my working life
- 35%
- Lack of information/resources on my condition
- 32%
- Lack of public acknowledgement from authority figures (government, etc.) on my condition
- 27%
- Not knowing if others (friends, colleagues, employers, healthcare providers, etc.) will take my condition seriously
- 22%
- Difficulty in accessing benefits related to my condition (e.g. sick leave, disability)?
- 22%
- Difficulty in formally indicating my condition to employers, healthcare providers, and/or others
- 16%
- Being terminated by my employer for my condition
- 10%
- Being judged for my condition
- 9%
- Other
- 1%
The following subgroups were significantly more likely to feel uncertain about their future health prospects if they got long COVID:
- Respondents who received five doses of the COVID-19 vaccine (78%)
- Respondents over 55 years old (77%)
- Women (72%)
- Respondents who are not parents of children younger than 18 years old (72%)
The following subgroups were significantly more likely to worry about limitations to their leisure or personal life:
- Respondents who received five doses of the COVID-19 vaccine (69%)
- Respondents who are not parents of children younger than 18 years old (65%)
5. Detailed results for Wave 19
5.1. Mental Health
Understanding and perceptions of mental health
Overall, the participants seemed to notice an increase in the general presence of mental health as a matter of public interest and discussed topic over the past years, particularly since the beginning of the COVID-19 pandemic. Many of them mentioned noticing what seems to be a general decline in mental health among the Canadian population and more people seemingly struggling with mental health issues such as anger, stress and anxiety. Many participants talked about the COVID-19 pandemic and related lockdowns and isolation as an important disruption in the habits of Canadians, which had, and continues to have, a significant negative impact on the mental health of many. Some participants highlighted the toll that the pandemic had on the healthcare system and frontline workers in particular, and an increase in domestic violence. However, participants also highlighted that openness about mental health had come a long way over the past decades and that the COVID-19 pandemic played a role in accelerating this. Many participants, including younger ones, mentioned that when they were younger, mental health was closely associated with severe mental illness and was seen as a weakness or as something shameful, which was better not to be discussed. One participant added that mental health seemed especially important and talked about openly in her generation (generation Z), giving the example of coworkers who take mental health days at work and are open about this subject with their colleagues and superiors.
Most participants indicated having recently noticed more ads and social media posts increasing awareness about mental health. These included ads from provincial and federal governments, along with ads or personal posts on social media and the "Bell Let's Talk/Bell Cause pour la Cause" initiative. A few participants mentioned seeing more mentions of mental health over the past few years but indicated that they did not hear about it as much now compared to the first years of the pandemic. Members of 2SLGBTQIA+ groups have pointed out that they frequently come across relatable personal posts or content related to mental health on social media, which helps to raise awareness about specific challenges or issues that are more commonly experienced in their community.
The majority of the participants considered the term "mental health" to be neutral. Those who stated seeing it in a positive light said that they did so because they found it was positive that there are fewer taboos and stigmas associated with it and that it was talked about more openly than before. Those who stated seeing it in a negative light mentioned that they did so because they felt there still is some degree of stigma associated with it today, or that they generally hear negative things related to mental health issues in the news. Some of them gave examples of mental health-related crimes and incidents or of worsening levels of mental health being covered in the media as contributing to their negative perspective of the term "mental health".
A majority of participants described mental health as psychological wellness in general. Many of them mentioned that mental health closely relates to day-to-day well-being, the ability to cope with daily tasks and challenges, having a positive and optimistic outlook on life, emotional stability and the presence of close ones to rely on for support. A few participants also highlighted that the well-being of individuals impacts the collective well-being of society as a whole and that they should not be regarded as mutually exclusive. They generally equated mental health to an aspect of a person's overall health that should be considered similarly to physical health. Parents' groups seemed to have a somewhat poorer understanding of what mental health means, putting forward vague definitions of it.
The participants' definitions of "bad mental health" included the following: not being able to complete daily tasks or to function normally in society, feeling sad, having thoughts of self-harm or harming others, and generally not being in the right state of mind. A few participants also mentioned that mental health felt to them like an "umbrella term" used to fit too many different issues.
When asked about personal indicators of worsening mental health, many participants mentioned the following:
- Disruptions to their eating, sleeping and/or cleaning habits
- Difficulty completing daily tasks due to lack of motivation
- A lack of interest in one's usually enjoyable hobbies or activities
- Self-harm or suicidal thoughts
- Unusual tiredness, irritability or sadness
- Anxiety, panic attacks, and not feeling like oneself
- Peers being worried and actively inquiring about one's mental health
- Appearance of symptoms of mental illnesses (specific to those who have a personal or familial history of mental illness).
When asked about aggravating factors to their mental health, many participants mentioned their workload or work-related stress. Many of them, particularly among anglophone, racialized and parents' groups, also mentioned inflation or stress relating to their personal finances. Some participants highlighted that continuously seeing bad news in the media could significantly contribute to their negative mental state, while others mentioned the same thing for their exposure to negative content on social media. Some parents highlighted the fact that parenthood-related factors could become a strain on their mental health, one of them giving the example of their baby crying increasing their anxiety.
In terms of barriers preventing them from being able to improve their mental health, many participants mentioned the lack of accessible resources, specifying that support and resources are expensive, that information can be hard to find, and that there are very long wait lists to access more affordable resources, and they had to wait up months to get support, which was more than enough time for their condition to worsen. A few participants mentioned getting stuck at the referrals stage without getting any continuous support for their mental health. They acknowledged that it was less difficult to get help for an isolated mental health problem than finding longer term resources like therapy or counseling. Some others stated that they sometimes feel bad for trying to get support, thinking that they might be preventing others with more urgent needs from having access to the resources they need. Some parents indicated that their family responsibilities and related lack of time due to tending to their children are significant barriers to accessing mental health support and resources. A participant shared that taking walks in the city centre is beneficial for their mental health, but the presence of mentally unstable and potentially threatening individuals in the area makes them feel unsafe and prevents them from doing so.
A sizeable number of male participants raised the fact that they often found it difficult to ask for help and to open up about their mental health with their close ones. One of them mentioned feelings of inadequacy and "feeling like a failure" for not being able to handle their problems on their own. Similarly, some participants, especially among the 2SLGBTQIA+ group, were less likely to talk to their families about their mental health. Internalized stigma regarding mental health issues therefore proves to be a barrier as well. Some other respondents also mentioned the taboo surrounding mental health in some cultural or rural communities and the related fear of judgment as barriers to action.
Some participants mentioned turning to professionals such as therapists or family doctors to improve their mental health, although recognizing that they were lucky to be able to have access to such resources that are not accessible to everyone. Others mentioned that they would rather try to find solutions on the internet and try to deal with their issues on their own, unless they became too severe, in which case they would also turn to professional help. While some participants had mentioned stigma and difficulty addressing mental health issues with their family, some others mentioned their friends and families as their "first line" of support, which they would turn to, while others who are in the workforce indicated having access to employee assistance programs provided by their employers. Parents' groups tended to identify suicidal thoughts or thoughts of self-harm as the most prominent sign to seek help for mental health, often waiting until a later stage to seek help compared to other groups. On the other hand, racialized and 2SLGBTQI+ groups tended to recognize earlier signs of poor mental health, such as experiencing difficulties in performing daily tasks, lack of enjoyment of usual hobbies or activities, or feeling a loss of oneself, as indicators to seek help.
In terms of expected mental health resources from the Government of Canada, most participants mentioned efficient, accessible and timely resources. Others proposed that tailored resources should be collaboratively developed in close partnership with diverse cultural groups and organizations in order to effectively meet their unique needs and cultural nuances with sensitivity, highlighting the specific needs of Indigenous peoples. A participant also noted the importance of integrating the current network of community-specific support into efforts to deliver mental health assistance to groups facing unique challenges, such as farmers or veterans. This integration would better enable mental health services to address the specific issues and realities that these groups face.
Most participants seemed to agree on the fact that mental health should be actively taken care of in the same way as physical health. Participants mentioned taking care of themselves through relaxing, baths, eating, sleeping well, exercising, taking time for themselves, and making an effort to socialize with friends and family (especially in the current post-COVID context). A few participants also noted that their involvement in their community or religious group played a significant role in maintaining positive mental health. One Indigenous participant also put forward that reconnecting with their roots, history, and traditional practices and beliefs significantly contributed to their well-being. Some participants suggested that taking a break from the news could be a method for shielding oneself from negativity and reducing the potential negative impact on mental health. One parent specifically mentioned shielding their autistic child from the news to protect their mental health, as they were particularly sensitive to such negative.
Most participants mentioned that they only think of their mental health when they are not feeling well. Some others stated that they think about it daily, particularly when doing things that are beneficial to their mental health, such as exercising. A few participants indicated thinking of their mental health in its extreme states (either when they are doing very good or very bad), and a few stated that they mostly think about it when doing well since they try not to think about it when doing bad.
Polling exercise 1 – Statement agreement
Participants were asked to either agree or disagree with three statements regarding mental health. For all three, opinions were quasi-unanimous.
Statement 1: Inequality of any kind (such as social, economic, health, etc.) can have an impact on one's mental health.
- In all groups, a vast majority of participants agreed with this statement. Participants acknowledged that a lack of fair access to opportunities has an impact on individuals. Cultural stigma and lack of financial resources to access mental health support services were mentioned as examples.
- Those who did not agree explained that regarding economic inequality specifically, anyone regardless of their economic status or income level could experience mental health issues.
- Participants also acknowledged that challenges can be faced at any stage of life and that the stress they can cause can be just as impactful regardless of one's age.
Statement 2:Only adults have mental health challenges.
- All participants disagreed unanimously with this statement. They mentioned their own personal experiences with mental health when they were growing up, as well as their children's (for those who had any).
- Parents acknowledged that school can be a stressful environment for children, and preoccupations about things such as reputation, popularity, in addition to bullying and harassment that can have a significant negative impact on their mental health. They also acknowledged that the pandemic, coupled with isolation and school closures, definitely had an impact on children's mental health. Other factors, like parents divorcing, were also seen as having an impact on a child's mental health.
- Participants also acknowledged that challenges can be faced at any stage of life and that the stress they can cause can be just as impactful regardless of one's age.
Statement 3: The sooner mental challenges are identified and treated, the better.
- Again, agreement with the statement was quasi-unanimous. Participants mentioned experiences they or their close ones have faced, and how early treatment can help avoid severe complications that require heavier support. One participant mentioned the situation of their mother: "My mother had major mental health issues and because of a lack of education, she couldn't address it early. Now she suffers from early onset dementia." One participant mentioned it was beneficial on all levels that mental health challenges be identified early on, as it means less complications for the individual, and less expenses for the government.
- Those who disagreed with the statement considered that it was never too late to identify and treat mental health challenges. One participant mentioned that some may only realize having a problem after a long period of struggling with poor mental health, but that they should definitely still seek help.
Message testing
Participants were presented with three public health messages relating to mental health. For each statement, participants were asked to rate it on how clear it was and were then asked about their opinions towards the statement. The following table details the average clarity score (out of four) for each message, in both English and French.
| Message 1 | Message 2 | Message 3 | |
|---|---|---|---|
| French average | 3.17 | 2.97 | 3.30 |
| English average | 3.44 | 3.17 | 3.26 |
| Overall average | 3.34 | 3.09 | 3.27 |
The following section will detail the perceived clarity of each statement, as well as their most and least appreciated elements, along with how to improve them.
Message 1
English: If you are struggling with mental health challenges and addiction, please know that you are not alone. There are programs and services that can help, including Wellness Together Canada which is free and confidential, and available 24/7.
French: Si vous avez des problèmes de santé mentale ou de dépendance, sachez que vous n'êtes pas seul. Il existe des programmes et des services qui peuvent vous aider, notamment le portail Espace mieux-être Canada, qui est gratuit, confidentiel et accessible en tout temps.
Overall, this message was perceived as somewhat clear by participants. They appreciated the use of the phrase "you are not alone", as it was seen as reassuring and comforting. There were no differences in terms of perception of this phrase, as no participant found issues with it. However, some participants in the francophone groups mentioned it could be understood in two different ways: not being alone in facing mental health issues, or not being alone because support is available. While anglophone groups did not explicitly raise the same issue, it still came up naturally in their answers, as they mentioned it made them feel less alone to know that support was available, but also that other people are struggling with their mental health. In both cases, participants mentioned it felt nice to be reminded that other people struggle with mental health issues, and/or that they can seek support or help.
Nevertheless, several elements made the message harder to understand. Grouping mental health challenges and addiction was often not understood nor appreciated by some participants. They felt that these two issues were different and should be addressed separately. One participant mentioned that it made them feel like they had to struggle with both mental health and addiction in order to be eligible to receive help through Wellness Together Canada.
Participants found the message to be missing some important information. Most participants mentioned the message should include contact information (either a link to a website or a 1-800 number), in order to easily and directly be able to access relevant information about the services offered. Their argument was that individuals who are experiencing a mental health crisis may not possess the ability to conduct adequate research on the organization's contact details, thus proposing that the contact information be directly included in the message.
Some participants mentioned that they were not sure what to expect when visiting the website/platform, and that additional information about the types of support available was needed.
Some participants mentioned that the message should be directed to a broader audience, as the first sentence may only resonate with those who are already familiar with the topic of mental health challenges. According to them, those who might be suffering from anxiety or depression but are not familiar with mental health might not feel concerned by this message. These participants often indicated that the message's first sentence leads to believe that one needs a formal diagnostic to be the target of the message.
According to one participant, the message should also speak to people who may not be facing mental health or addiction challenges themselves but may know someone who does. This way, the message can also prompt people to research and offer help to their close ones who may need it.
Message 2
English: We all know that the past few years have been challenging. The pandemic has disproportionately affected already marginalized populations, such as women, youth, racialized communities, 2SLGBTQIA+, First Nations, Inuit and Métis. There have been, and continues to be, significant impacts on peoples' mental well-being.
French: Nous savons tous que les dernières années ont été éprouvantes. La pandémie a eu des répercussions disproportionnées sur certaines populations déjà marginalisées, comme les femmes, les jeunes, les personnes racisées, les personnes 2ELGBTQIA+ et les membres des Premières Nations, des Inuits et des Métis. Il y a eu, et il continue d'y avoir, des retombées importantes sur le bien-être mental des personnes.
This message was, without a doubt, the one that sparked the most debate in the focus groups. First of all, the message was perceived as wordy and too long by many participants, but most still found it somewhat clear. Some acknowledged and appreciated the detailing of marginalized communities and the specific impacts of the pandemic on their mental health, especially among the racialized and the 2SLGBTQIA+ groups. However, they also felt the message could be more explicit and provide a better explanation as to how or why these marginalized communities were disproportionately affected by the pandemic in terms of mental health. Some participants mentioned other groups that were left out of the statement: people with disabilities, people living below the poverty line, senior individuals and individuals facing homelessness. A few participants, mostly men, felt that the statement was false as the pandemic exacerbated everybody's mental health challenges.
On the other hand, some participants felt like this message, by trying to be inclusive, could create a feeling of exclusion in some individuals who may not identify as part of any of the mentioned groups. Specifically, in addition to the opinion of the few men mentioned previously, some mentioned that men could feel left out from the message, when their mental health has been affected as well. The exclusion of men from the statement was the most brought up, and some felt like the statement invalidated their experiences and their struggles with mental health: "J'ai un peu de la misère avec le fait qu'on parle de certaines communautés seulement. Comme si on enlève le fait que certains aient pu passer un mauvais moment durant la pandémie aussi." ("I have an issue with the fact that the message only mentions some communities, it feels like it's taking away the fact that some people might have had a hard time during the pandemic as well.") Some participants stated that the message should just include everyone, as all Canadians are prone to facing mental health issues.
Participants also struggled to understand the objective behind the statement: while it was seen as factual and true by a vast majority of participants, they did not understand what was intended with this message. They mentioned wanting to know more, and that there should be a call to action.
The statement "we all know that the past few years have been challenging" was also divisive. While some felt like it was a neutral acknowledgement of the challenges that the pandemic brought up, a few mentioned it felt like "putting words in people's mouths", and some mentioned they were tired of hearing similar phrases as they just wish to move on from the pandemic and its negative impacts on their mental health. This phrase was often perceived as unnecessary as, to them, it was only stating the obvious, but a few felt it was a good reminder for those who may have not struggled as much during the thick of the pandemic.
One participant in the Francophone 2SLGBTQIA+ group mentioned the message should be in inclusive writing considering the topic.
Message 3
English: If you need help, please reach out. If you are struggling, know that you can access the Wellness Together Canada (WTC) portal and its companion app PocketWell for free 24/7 educational content, and self-guided and moderated peer-to-peer support, as well as one-to-one counselling with qualified health professionals.
French: N'hésitez pas à demander de l'aide, si vous en avez besoin. Si vous éprouvez des difficultés, sachez que vous pouvez accéder au portail Espace Mieux-être Canada (EMC) et à son application complémentaire, Mieux-être, pour obtenir en tout temps et gratuitement du contenu informatif, du soutien autoguidé ou par les pairs et du counseling individuel offert par des professionnels qualifiés.
The third message was compared to the first one in that they have similar objectives, and a vast majority of participants found it clearer and more helpful than the first. One of the few aspects that participants sought clarification on was whether the message specifically targeted mental health issues. Participants understood it contextually, but figured that without context, it could be understood differently (e.g., physical health issues or financial problems). Some participants also found it too wordy, and opening with the two "if" statements was seen as redundant. One participant mentioned they appreciated the mention of peer-to-peer support as well as self-guided support as they could handle their problems "on their own" but could also look for support from people facing the same issues. The comment about including those who are not facing mental health challenges but may know someone who does was brought up again, suggesting the message should add a mention including those looking for resources for helping their close ones. Participants also reiterated wanting a link or a phone number, as well as more emphasis on the resources available on the portal that are usually hard to get, such as counselling.
One francophone participant mentioned they would trust provincial resources more than federal ones, and one anglophone participant mentioned they dismissed federal/provincial resources as they were distrustful of their governments.
5.2. Vaccines
Flu vaccine
Across all groups, most participants were doubtful towards the flu vaccine, regardless of their profile. Hesitance and/or reticence to get the flu shot were expressed in all groups. The general consensus was that getting the flu shot should be an individual decision that each person can make for themselves, depending on their health and situation. Most participants have never gotten the flu shot and do not intend to. Participants mentioned two main reasons for not getting vaccinated against the flu: not seeing the need considering they never got the vaccine, and wanting to build natural immunity against the flu. Participants considered that their immune systems were strong enough to fight off the virus without needing a vaccine, and that fighting off the disease naturally contributes to strengthening their immune defenses. Furthermore, some participants mentioned they were unsure about the vaccine efficiency considering that the flu virus mutates and changes every year. Participants also expressed distrust as they felt its efficacy lacked widespread evidence supporting it. Some participants mentioned that not everyone should get vaccinated against the flu as complications can happen, and interactions with other medicine can occur (one participant mentioned multiple sclerosis medication as an example).
A few participants expressed their distrust towards public health authorities, who, according to them, lacked transparency and did not share all the relevant information with the public. One participant mentioned having researched and read peer-reviewed medical articles to get information on the flu vaccine and that people should not have to get to that point to be informed about the vaccine and its potential risks: "If you don't want to share the information freely, then it's not something I would personally trust."
However, most participants agreed that immunocompromised individuals, elders, and anyone with a weaker immune system or who is in regular contact with people with weaker immune systems should get the flu vaccine. These were the most frequent cases that prompted participants to recommend getting vaccinated. The overcrowding of children's hospitals because of respiratory diseases has not influenced any of the participants into getting the flu shot for themselves or their children. While some participants had not heard of it, those who did stated it did not influence their decision towards the vaccine, whether they were parents or not. One participant living in a small rural area mentioned their community was highly distrustful of vaccines, leading them to stock up on over-the-counter medicine when the overcrowding occurred, instead of getting vaccinated.
A minority of participants were in favour of the flu vaccine and considered that anyone who can get it should get it in order to protect the community. A few of them also indicated they had gotten it. For instance, one participant living in a small rural community mentioned they had gotten vaccinated to protect others rather than themselves, considering that the vast majority of the community did not believe in vaccines and would not get vaccinated. Another participant mentioned their children as the only reason they have gotten the flu shot.
Vaccine confidence
The pandemic did not influence participants' views towards vaccines at large aside from confirming or reinforcing their pre-existing opinions: those who were trustful saw the pandemic as a confirmation that the COVID-19 works, and those who were distrustful saw it as a sign that it did not work. A few participants mentioned they had COVID-19 before and after vaccination, and that the symptoms were noticeably weaker after vaccination, which proves its efficacy. While participants stated they were worried about potential side effects of the COVID-19 vaccine (mainly because of a perceived lack of testing and fast rollout), these concerns did not translate to other vaccines that have already proven themselves (such as the polio or mumps vaccines). Concerns about the flu vaccine and the COVID-19 vaccine were expressed by all demographics, even those who self-identified as "pro-vaccine." Some participants touched on the subject of societal pressure regarding getting the COVID-19 vaccine, mentioning restrictions to their work as well.
Furthermore, a few participants mentioned the pandemic helped them better understand how vaccines work. One participant explained that they were somewhat less confident in the COVID-19 vaccine's efficiency but only because of all the misinformation going around about vaccines, resulting in the fact that not enough people might get vaccinated for some vaccines to attain the adequate coverage level needed to successfully eradicate certain illnesses, such as measles.
Regarding the COVID-19 vaccine specifically, parents especially weighed the pros and cons of getting their children vaccinated or not and based their decision on that, regardless of the child's age. Conclusions differed: while some considered getting them vaccinated was the riskiest alternative, others preferred avoiding the potential complications that could ensue from a COVID-19 infection through vaccination. Some mothers also mentioned having gotten vaccinated when they were pregnant specifically to pass on the antibodies to their child.
Regarding the link between the COVID-19 vaccine and fertility, a majority of participants did not have any concerns. Some participants were unaware of the link between vaccines and fertility and asking the question during the focus group caused them to worry a little. Some participants did, however express concern, most of them women. One participant mentioned the vaccine's impact on her menstrual cycle as a reason to worry. Some parents mentioned the vaccine's effect on their children's fertility. One participant mentioned they did worry about the link but were reassured by close ones who did not face any fertility issues after getting vaccinated. Another participant stated they noticed it was harder for their wife to get pregnant after the vaccine than before getting it, which to this day made them question whether or not it had an impact on their fertility.
Routine vaccinations
In terms of keeping up to date with the recommended adult routine vaccinations, parents were the most knowledgeable on the topic. A majority of participants who were not parents were not even aware of what vaccines they had gotten and which ones they missed or weren't even aware that they had to keep them up to date. Some participants mentioned that they were able to keep their vaccinations up to date because they traveled frequently, either for work or leisure, which required them to stay on top of their immunization status.
Parents, on the other hand, were conscientious with their own and their children's vaccinations. They trusted their family doctor or general practitioner to recommend the most relevant, useful, and trustworthy vaccines. Parents were strongly in favour of established vaccines that have been tested for years and have been on the market for decades and mentioned they helped eradicate some diseases that were previously prevalent (e.g., polio). However, they did express some distrust towards more recent vaccines, naming COVID-19, the flu, and gastroenteritis vaccines as examples. According to them, these vaccines are too novel to have been tested properly, and they preferred to wait a few years before using them on their children. Some also expressed concern over the lack of information about potential long-term side effects of certain vaccines, especially the ones against COVID-19.
Regarding travel, most participants mentioned checking the Government of Canada's website to ensure they are protected adequately before the trip. However, researching public health information before travelling varied depending on the level of disease-related risk associated with their destination. One participant mentioned they would not research such information if travelling to London, United Kingdom for instance.
Participants were then asked to indicate to what extent they agreed or disagreed with the following statement, that was adapted for the parents' groups as well:
- General groups statement: Recommended vaccinations provide adequate protection against vaccine preventable diseases.
- Parents groups statement: Recommended vaccinations provide my child with adequate protection against vaccine preventable diseases.
A vast majority of participants, regardless of whether they were parents or not, agreed with the statement. Those who disagreed explained their position with different elements: one person mentioned that the pandemic had shown that the vaccine did not help curb COVID-19 cases as everyone they know caught the disease at least once or even twice; another person disagreed because they felt like vaccines gave some people a false sense of protection, leading them to be careless and stop using public health measures. On the other hand, those who agreed justified their opinion by their knowledge and understanding of how vaccines work and by their trust in public health authorities and governments in recommending the safest course of action in terms of vaccination. Some parents also gave the example of some diseases that have been almost eradicated thanks to vaccination campaigns (e.g., polio) to justify their trust in vaccines. The term "adequate" was, however divisive: while some felt it was the right term to use, others felt like it was too weak of a term and made them distrustful.
5.3 Public health measures
Participants were presented with two holiday-themed video ads broadcasted during the holiday season in December 2022. Aside from a few participants, nobody had seen the videos before the focus group sessions. Neither awareness nor reactions varied between groups. The ads received very mixed reactions from the participants. While participants agreed that broadcasting public health measures that should be adopted to reduce virus transmission was still relevant, they were unsure about the reach of the ads and their effectiveness in changing behaviors. Some participants had the feeling that the ads would not be effective, as those who were already cautious would keep being so, and those who weren't would not be convinced by the ads to be more prudent. A few participants considered that broadcasting these messages would further amplify the feelings of pandemic fatigue that some Canadians might feel, especially if they were to be displayed throughout the year or around other holiday periods. One participant specifically considered the ads anachronical as COVID-19 is not as present in our daily lives anymore. However, others compared them to campaigns against impaired driving to highlight the importance of continuing to broadcast them. Some participants mentioned the campaigns should contain more information about how adopting public health measures can curb transmission to increase their effectiveness at raising awareness around virus transmission and the part that we play.
Despite mixed reactions, participants agreed that having the ads broadcasted could serve as a reminder throughout the holiday season. Some participants also stated being in favour of broadcasting them more often, but rather than having them play throughout the entire year, they should be strategically broadcast before holiday periods, and before peaks in COVID-19 or flu transmission as a preventive measure.
The holiday theme of the ads was also divisive. While some found them to be playful and fun, others thought it was unnecessary to tie COVID-19 issues into the holidays: "The holidays are to focus on the holidays and remember what the holidays are about." A few participants considered that public health authorities should be direct with their messaging. Furthermore, some participants found the ads too fast and did not allow them to take in the information that was shared, which led to having to display the ads a second time for them to be able to provide their feedback.
While awareness of the ads was low, most participants mentioned they still followed the advice that was provided in them: they regularly wash their hands and/or disinfect them and isolate or wear a mask when they feel sick. Only a few participants mentioned still wearing a mask in indoor or crowded spaces and wishing that others kept doing so as well. Not much effort was made regarding improving ventilation, however, and a few participants living in the Prairies found the recommendation to be absurd considering the outside temperatures during winter. Overall, practicing of individual public health measures did not vary across groups, but those who were immunocompromised, or were in close contact with immunocompromised individuals were more likely to wear masks in public spaces and were more cautious in general.
Some participants mentioned that the government should focus more of its resources on improving the situation in the health care system which is under a lot of pressure because of COVID-19 and other respiratory diseases that were circulating rather than investing in ad campaigns whose effectiveness remains to be proven. Some others stated that more effort should be put into ensuring that businesses do their part in preventing virus transmission, rather than putting all of the burden of caution on individuals - they felt that most businesses stopped disinfecting surfaces and refilling the hand sanitizing bottles that customers can use.
6. Detailed results for Wave 20
Note on testing for statistical differences
According to the normal distribution, a two-tailed test is always done between two proportions and based on the unweighted total columns. The test is performed by comparing a percentage with the percentage formed by the complement of the relevant category (e.g., of the male subgroup is the female subgroup; the complement of the 18–24 age subgroup is the 25+ age subgroup, and the complement of the college-educated subgroup is the sub-group consisting of respondents with elementary, high school or university education). The test results (if they are significant at a confidence level of at least 95%) are mentioned in the table analysis.
In the report, when we indicate that a sub-group of the sample is "more likely" or "less likely", it means that the statistical testing returned a valid statistically significant difference between this subgroup and its complement, even if the percentage is low.
6.1 COVID-19 infection
Respondents were questioned about whether they had ever been infected with COVID-19. Almost half (47%) said they had been infected with the virus, while nearly one out of ten (8%) believed they had been infected but had not been properly tested. As a result, more than half of Canadians (54%) have been or believe they have been infected with COVID-19. Four respondents out of ten (41%) responded that they had never been infected.
Figure 20.1: Have you ever been infected with COVID-19?
Sample frame: All respondents (n=3,026)
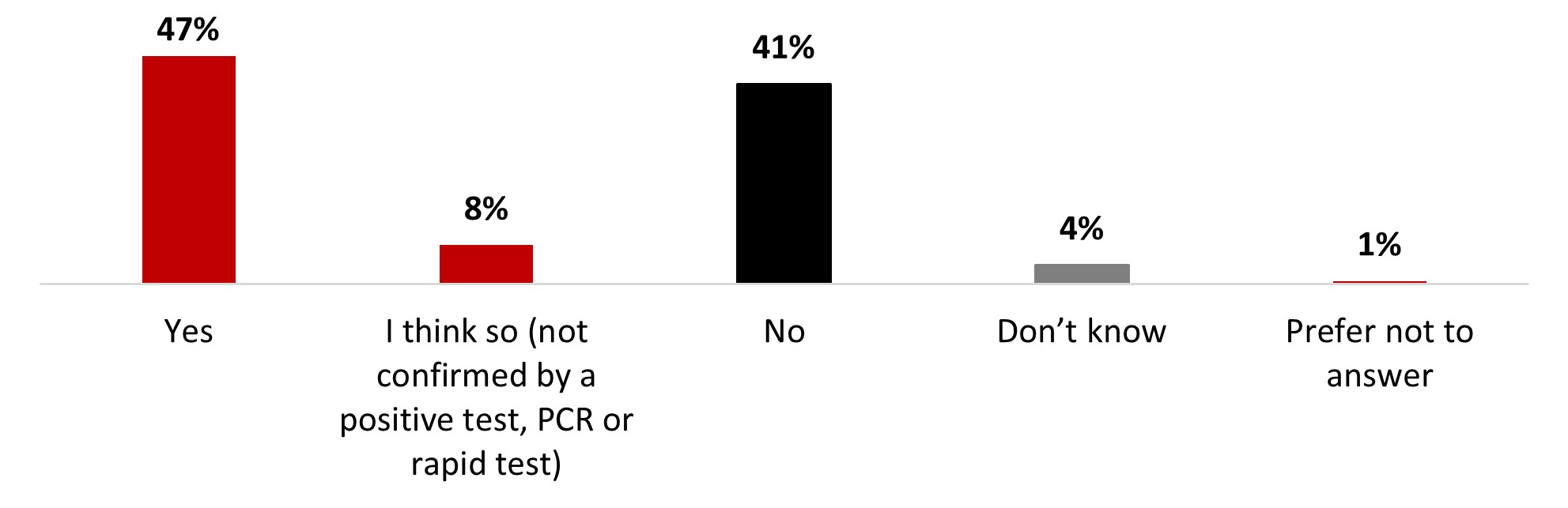
Figure 20.1: Text description
- Yes
- 47%
- I think so (not confirmed by a positive test, PCR or rapid test)
- 8%
- No
- 41%
- Don't know
- 4%
- Prefer not to answer
- 1%
A significantly higher proportion of the following subgroups of respondents has indicated they had been infected with COVID-19:
- 18 to 34-year-olds (54%) and 35 to 54-year-olds (52%)
- Quebec residents (59%)
- Women (49%)
- Parents of children younger than 18 years old (58%)
One-third of respondents (31%) identified themselves as being at risk of complications or severe consequences if they contracted COVID-19 because of their specific medical condition or because of having a chronic disease. More than half of the respondents (57%) reported that they were not at risk, while 12% were unsure.
Figure 20.2: Do you consider yourself to be at risk of more severe disease or outcomes from COVID-19 (e.g., are an older adult over the age of 60, are pregnant, have Down syndrome, have a chronic medical condition, are immunocompromised, or live with obesity, etc.)?
Sample frame: All respondents (n=3,026)
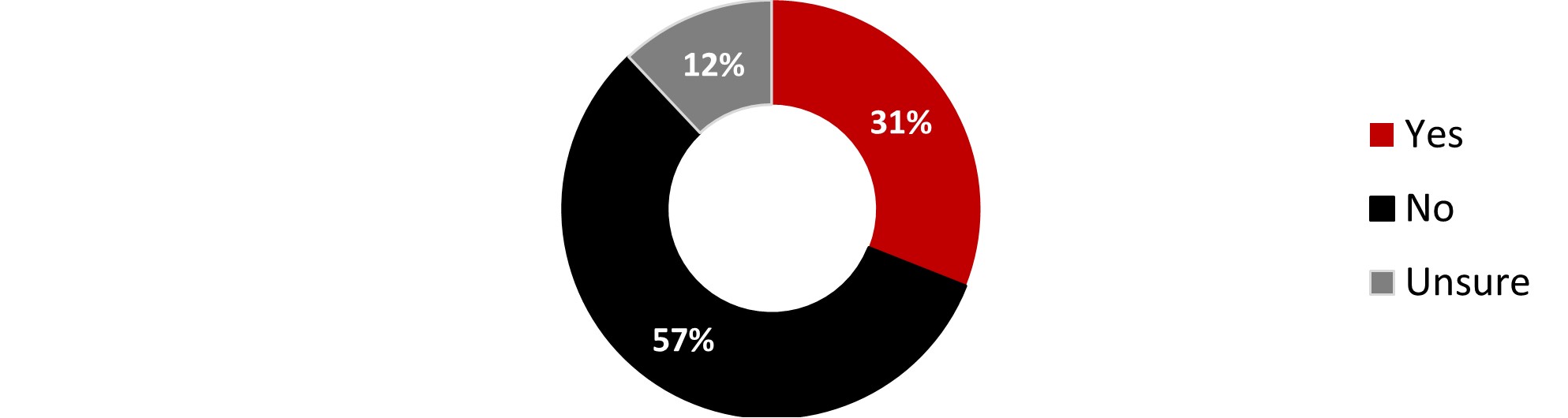
Figure 20.2: Text description
- Yes
- 31%
- No
- 57%
- Unsure
- 12%
The following subgroups were significantly more likely to consider themselves at risk:
- Respondents living with a disability (55%)
- Respondents over 55 years old (52%)
- Respondents who identify as Indigenous (38%)
Respondents were asked about how worried they are about getting infected with COVID-19. More than a third (37%) mentioned being very worried (9%) or somewhat worried (28%) while about a third (34%) are only a little worried. On the other hand, a quarter of Canadians (27%) are not at all worried about becoming infected with COVID-19.
Figure 20.3: How worried are you of becoming infected with COVID-19?
Sample frame: All respondents (n=3,026)
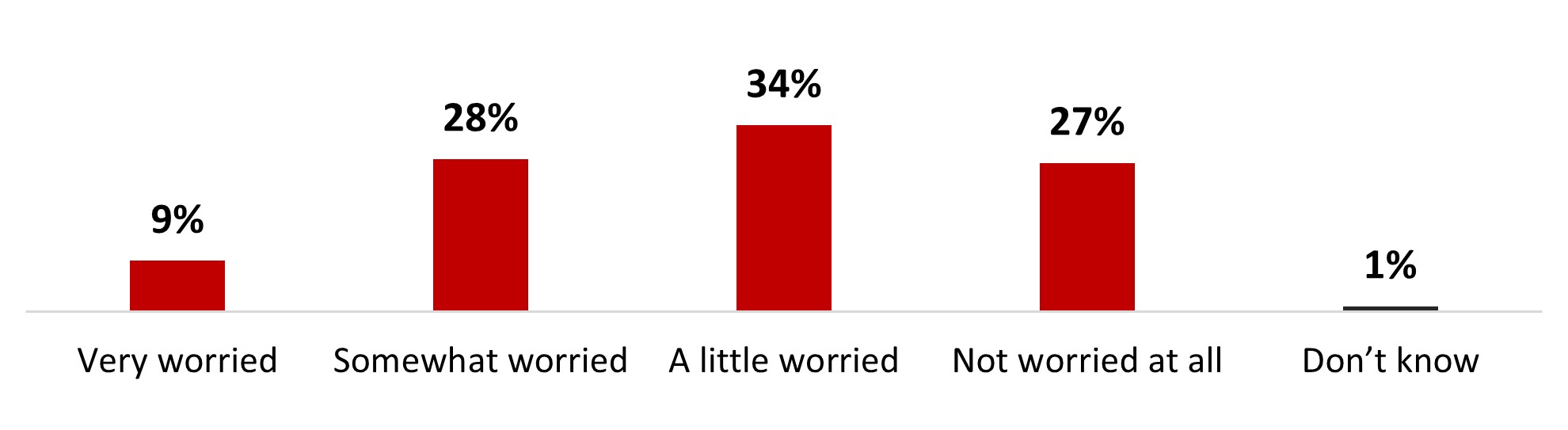
Figure 20.3: Text description
- Very worried
- 9%
- Somewhat worried
- 28%
- A little worried
- 34%
- Not worried at all
- 27%
- Don't know
- 1%
The following subgroups were significantly more likely to be very or somewhat worried about catching COVID-19:
- Respondents living with a disability (48%)
- Respondents who identify as 2SLGBTQIA+ (47%)
- Respondents from British Columbia and the Territories (44%)
- Respondents over 55 years old (42%)
- Those who had not been infected with COVID-19 (41%)
- Respondents who received three (41%), four (47%) or five (49%) doses of the COVID-19 vaccine.
Those who were not worried about becoming infected with COVID-19 mentioned a variety of reasons to justify their position. Believing that symptoms would be mild because of the vaccine (32%), that COVID-19 is here to stay (27%), having contracted COVID-19 previously and not been really sick (26%), having contracted COVID-19 before so they know what to expect (25%), having more important concerns (23%) or that COVID-19 is just another flu (23%) were mentioned by a quarter of respondents. Other reasons were mentioned by fewer respondents.
Figure 20.4: Why are you not worried about becoming infected with COVID-19? Select all that apply.
Sample frame: Respondents who are not worried at all about becoming infected with COVID-19 or are unsure (n=844)
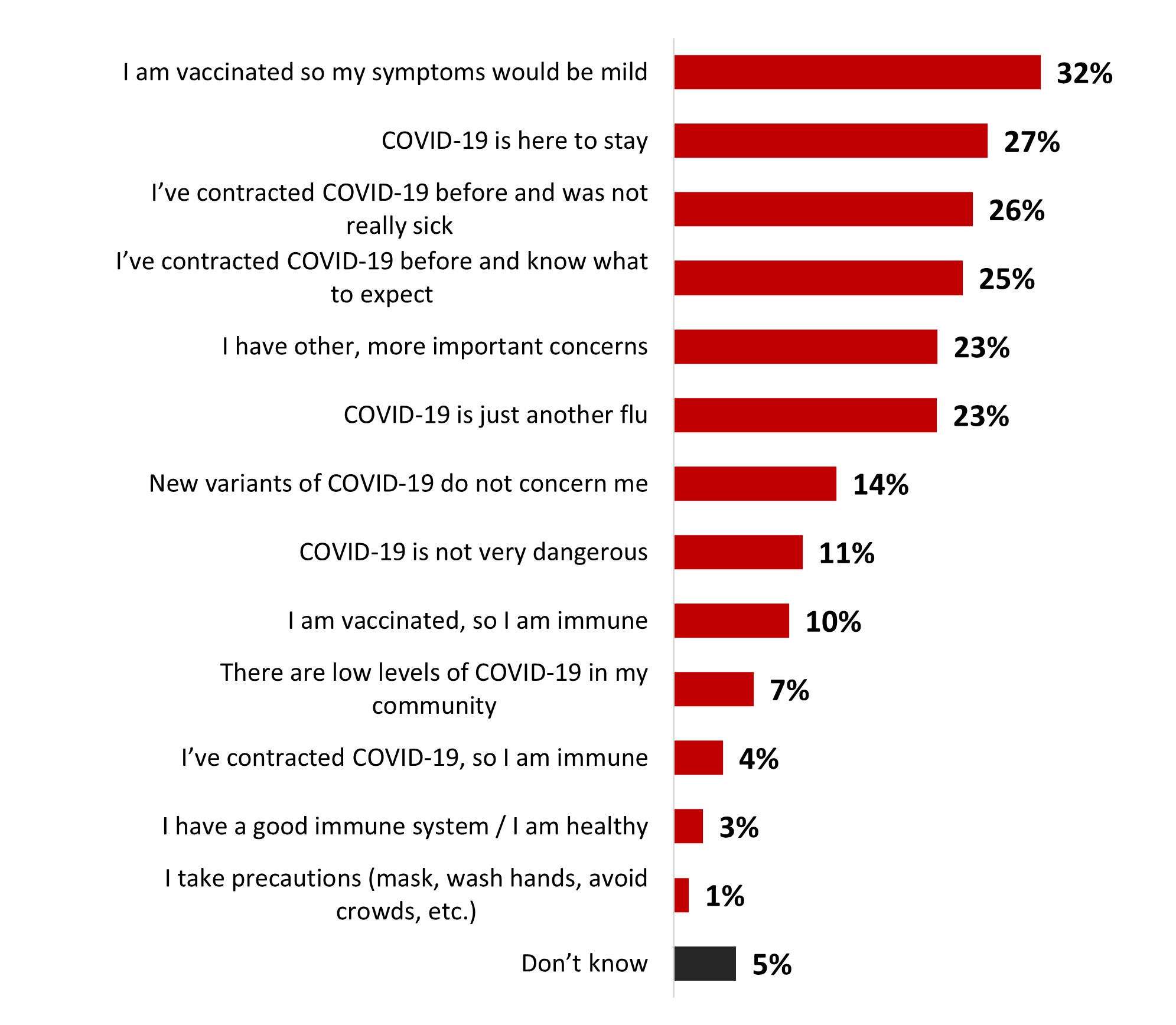
Figure 20.4: Text description
- I am vaccinated so my symptoms would be mild
- 32%
- COVID-19 is here to stay
- 27%
- I've contracted COVID-19 before and was not really sick
- 26%
- I've contracted COVID-19 before and know what to expect
- 25%
- I have other, more important concerns
- 23%
- COVID-19 is just another flu
- 23%
- New variants of COVID-19 do not concern me
- 14%
- COVID-19 is not very dangerous
- 11%
- I am vaccinated, so I am immune
- 10%
- There are low levels of COVID-19 in my community
- 7%
- I've contracted COVID-19, so I am immune
- 4%
- I have a good immune system / I am healthy
- 3%
- I take precautions (mask, wash hands, avoid crowds, etc.)
- 1%
- Don't know
- 5%
Significant differences regarding reasons to not worry about catching COVID-19 include the following:
- 18–34-year-olds were more likely to mention having contracted COVID-19 so they know what to expect (35%), while those aged 55 years or older were more likely to mention being vaccinated so their symptoms would be mild (49%).
- Women were more likely to mention having contracted COVID-19 so they know what to expect (29% vs 21% for men).
- Respondents from Ontario were more likely to mention being vaccinated so the symptoms would be mild (37%).
- Parents of children younger than 18 years old were more likely to mention that COVID-19 is here to stay (35%), that it is just another flu (32%), that they have more important concerns (29%) or that new variants do not concern them (22%).
- Black-identifying individuals were more likely to think that they are immune because they have received the vaccine (24%).
- Respondents who identify as Indigenous were more likely to think that COVID-19 is just another flu (34%).
More than half of those who were worried about catching COVID-19 said they were worried about getting others sick (52%), getting really sick themselves (47%) or getting significant complications (46%).
Figure 20.5: Why are you worried about becoming infected with COVID-19? Select all that apply.
Sample frame: Respondents who are worried about becoming infected with COVID-19 (n=2,182)
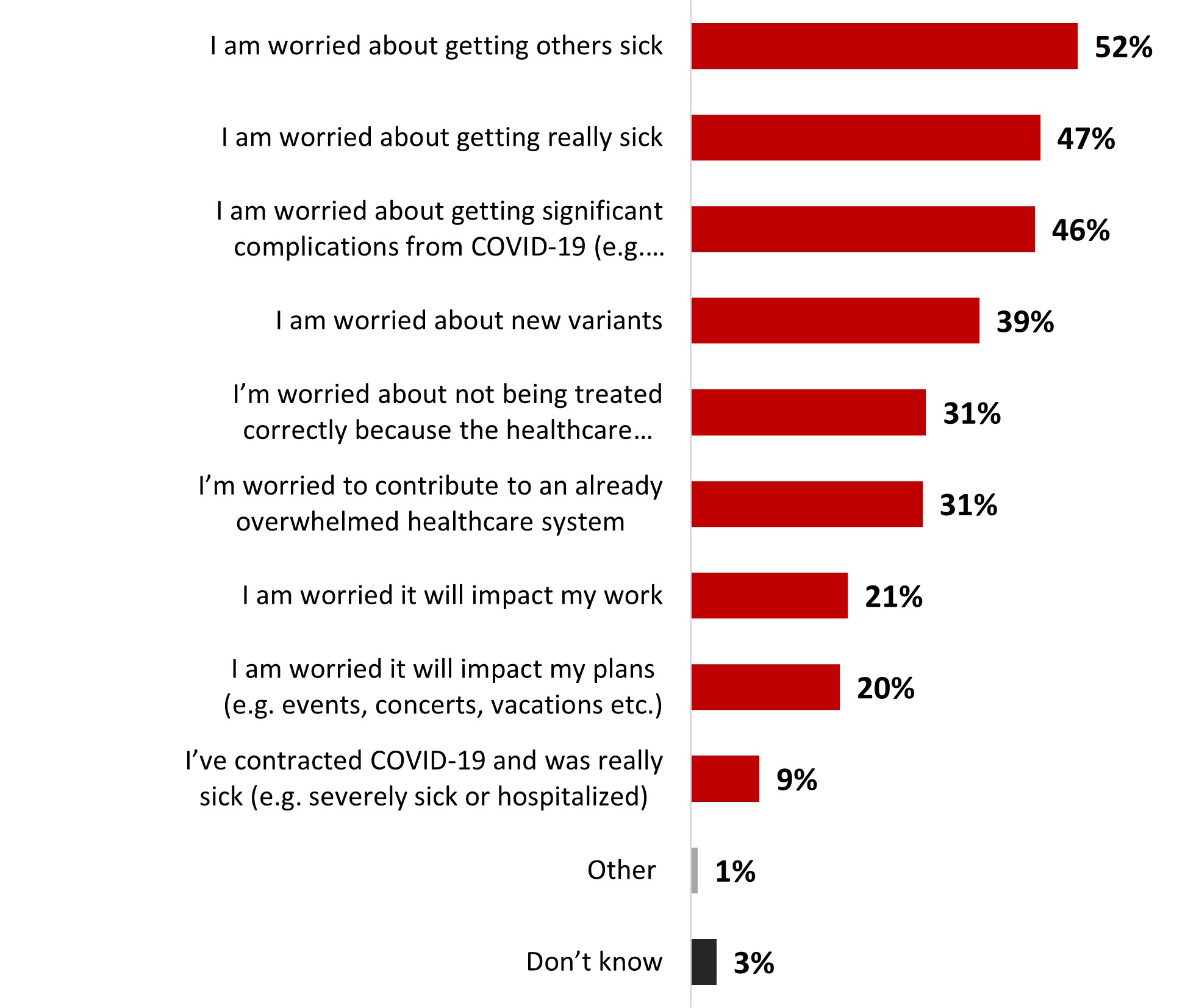
Figure 20.5: Text description
- I am worried about getting others sick
- 52%
- I am worried about getting really sick
- 47%
- I am worried about getting significant complications from COVID-19 (e.g. long COVID)
- 46%
- I am worried about new variants
- 39%
- I'm worried about not being treated correctly because the healthcare system is overwhelmed
- 31%
- I'm worried to contribute to an already overwhelmed healthcare system
- 31%
- I am worried it will impact my work
- 21%
- I am worried it will impact my plans (e.g. events, concerts, vacations etc.)
- 20%
- I've contracted COVID-19 and was really sick (e.g. severely sick or hospitalized)
- 9%
- Other
- 1%
- Don't know
- 3%
Significant differences regarding reasons to be worried include:
- Women were more likely to mention being worried about getting other sick (55% vs 48% for men).
- Respondents over 55 years old were more likely to be worried about getting complications from COVID-19 (52% vs 39% among 18–34-year-olds).
- Respondents from Alberta (56%) and British Columbia (54%) were more likely to be worried about getting really sick, while respondents from Ontario (56%) are more likely be worried about getting others sick and other variants (45%).
- Respondents living with a disability were more likely to be worried about getting really sick themselves (57%) or not being treated correctly because of the healthcare system being overwhelmed (40%).
- Parents of children younger than 18 years old were more likely to be worried about the impact an infection may have on their work (27%).
6.2 Mental health
When asked about their most pressing concerns, the top concerns mentioned were the personal financial situation (19%), the state of the economy (14%) and the overwhelmed healthcare system (10%). Other concerns were mentioned by less than one respondents out of ten.
Figure 20.6: What is your most pressing concern at this time?
Sample frame: All respondents (n=3,026)
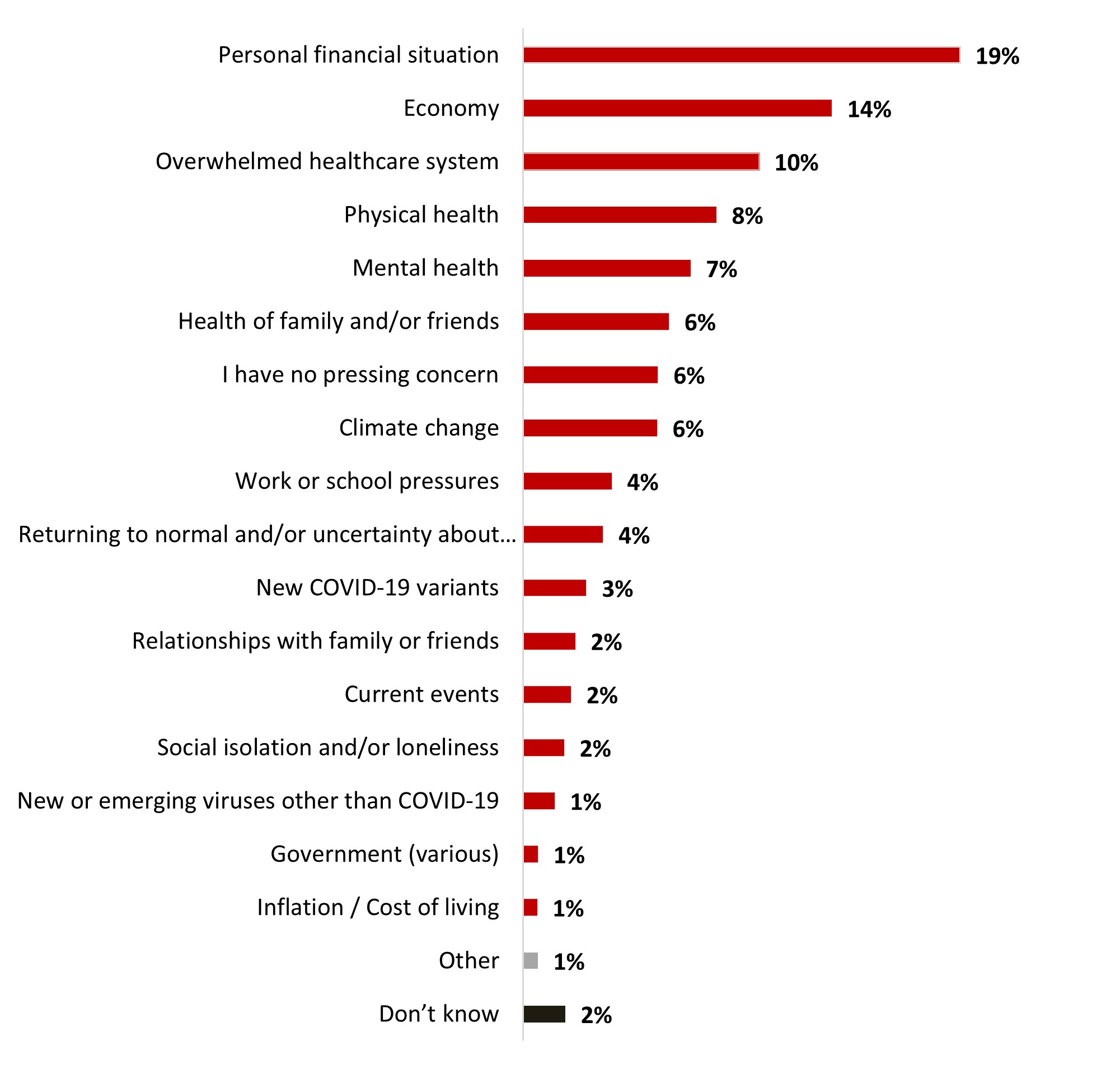
Figure 20.6: Text description
- Personal financial situation
- 19%
- Economy
- 14%
- Overwhelmed healthcare system
- 10%
- Physical health
- 8%
- Mental health
- 7%
- Health of family and/or friends
- 6%
- I have no pressing concern
- 6%
- Climate change
- 6%
- Work or school pressures
- 4%
- Returning to normal and/or uncertainty about the future
- 4%
- New COVID-19 variants
- 3%
- Relationships with family or friends
- 2%
- Current events
- 2%
- Social isolation and/or loneliness
- 2%
- New or emerging viruses other than COVID-19
- 1%
- Government (various)
- 1%
- Inflation / Cost of living
- 1%
- Other
- 1%
- Don't know
- 2%
Some subgroups were significantly more likely to mention certain concerns, including:
- Respondents from Alberta (28%), those who make less than 40K annually (28%), parents of children younger than 18 years old (24%), 18-34-year-olds (22%) and 35–54-year-olds (23%) were more likely to be concerned about their personal financial situation.
- Respondents over 55 years old (15%) were more likely to be concerned about the healthcare system being overwhelmed.
- Respondents living with a disability were more likely to be concerned by their physical (16%) and their mental (14%) health.
More than half of respondents (57%) rated their mental health positively: either very good (20%) or good (36%). The remaining respondents rated their mental health status more negatively, ranging from average (30%) to bad (10%) or very bad (2%).
Figure 20.7: How would you rate your overall mental health?
Sample frame: All respondents (n=3,026)
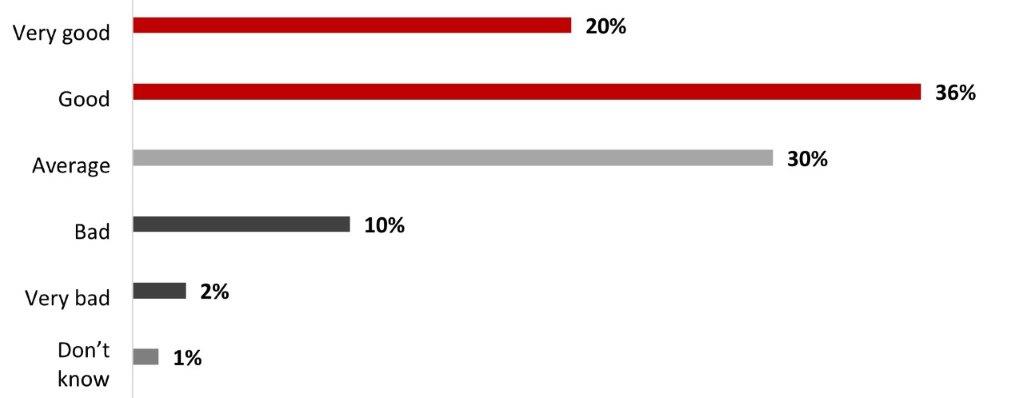
Figure 20.7: Text description
- Very good
- 20%
- Good
- 36%
- Average
- 30%
- Bad
- 10%
- Very bad
- 2%
- Don't know
- 1%
The following subgroups were significantly more likely to state having a good mental health:
- Quebec respondents (71%)
- Respondents over 55 years old (70%)
- Black-identifying individuals (67%)
- Respondents who have received four (61%) or five (68%) doses of the COVID-19 vaccine
- Men (61%)
The following subgroups were significantly more likely to state having a bad mental health:
- Respondents who identify as 2SLGBTQIA+ (35%)
- Respondents living with a disability (27%)
- 18 to 34-years-olds (20%)
The top actions mentioned by respondents to maintain a good mental health on a regular basis are making sleep a priority (52%) and engaging in activities that they enjoy (51%). Other actions mentioned by a third of Canadians or more are eating a healthy diet (44%), exercising regularly (41%), creating healthy and trusting relationships (38%), or setting realistic goals for themselves (34%). Other actions were mentioned by a smaller number of respondents.
Figure 20.8: Which of the following actions, if any, do you take to maintain good mental health on a regular basis?
Sample frame: All respondents (n=3,026)
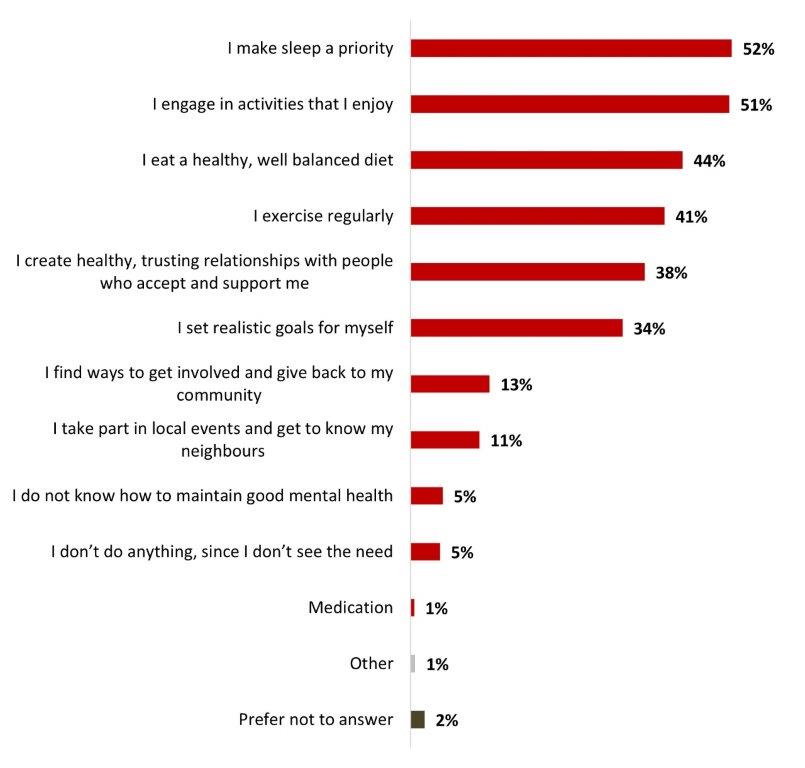
Figure 20.8: Text description
- I make sleep a priority
- 52%
- I engage in activities that I enjoy
- 51%
- I eat a healthy, well balanced diet
- 44%
- I exercise regularly
- 41%
- I create healthy, trusting relationships with people who accept and support me
- 38%
- I set realistic goals for myself
- 34%
- I find ways to get involved and give back to my community
- 13%
- I take part in local events and get to know my neighbours
- 11%
- I do not know how to maintain good mental health
- 5%
- I don't do anything, since I don't see the need
- 5%
- Medication
- 1%
- Other
- 1%
- Prefer not to answer
- 2%
Significant differences regarding reasons to be worried include:
- Women were more likely to state making sleep a priority (54% vs 49% for men) or to create healthy and trusting relationships with people (43% vs 31% for men).
- Respondents over 55 years old were more likely to make sleep a priority (57%), to exercise regularly (45%), to engage in activities that they enjoy (59%), to eat a healthy, well balanced diet (59%), take part in local events and get to know their neighbours (17%), to find ways to get involved and give back to their community (18%), to set realistic goals for themselves (38%) or to create healthy, trusting relationships with people who accept and support them (41%).
- Respondents who are not parents of any children younger than 18 years old were more likely to make sleep a priority (54%), to exercise regularly (42%), to engage in activities that they enjoy (55%), to eat a healthy, well-balanced diet (47%) or to take part in local events and get to know their neighbours (12%).
- Respondents with a university degree were more likely to make sleep a priority (56%), to exercise regularly (49%), to engage in activities that they enjoy (57%), to eat a healthy, well balanced diet (51%), to take part in local events and get to know their neighbours (15%), to find ways to get involved and give back to their community (16%), or to create healthy, trusting relationships with people who accept and support them (44%).
A third of respondents (33%) mentioned that it is very easy (9%) or easy (24%) for them to manage a mental health challenge when they experience it. On the other hand, around a quarter of respondents (23%) mentioned that it is either difficult (18%) or very difficult (5%) to manage a mental health challenge and four respondents out of ten mentioned that it was neither easy nor difficult.
Figure 20.9: When you experience a challenge or something in your life that affects your mental health, how easy or difficult is it for you to manage a mental health challenge?
Sample frame: All respondents (n=3,026)
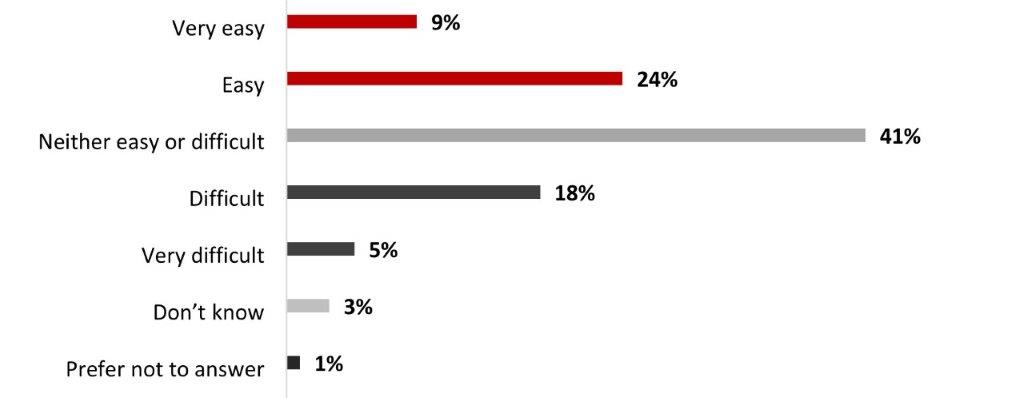
Figure 20.9: Text description
- Very easy
- 9%
- Easy
- 24%
- Neither easy or difficult
- 41%
- Difficult
- 18%
- Very difficult
- 5%
- Don't know
- 3%
- Prefer not to answer
- 1%
The following subgroups were significantly more likely to state that it is easy to manage a mental health challenge:
- Men (41%)
- Respondents over 55 years old (41%)
- Quebec residents (39%)
- Black-identifying individuals (39%)
- Respondents who have a university degree (38%)
The following subgroups were significantly more likely to state that it is difficult to manage a mental health challenge:
- Respondents who identify as 2SLGBTQIA+ (37%)
- Respondents living with a disability (32%)
- 18 to 34-years-olds (31%)
- Women (27%)
Reaching out to friends and family (44%) is the main way Canadians take care of their mental health when they experience a challenge. It is followed by making sleep a priority (31%), participating in relaxing activities (30%) and exercising (28%). Other ways to take care of their mental health were mentioned by a smaller number of respondents. One Canadian out of ten (10%) does not do anything or does not seek help for their mental health. The same proportion mentioned not having been affected by a mental health challenge before (9%) and a smaller proportion (4%) don't know how to take care of their mental health.
Figure 20.10: How do you take care of your mental health when you experience a challenge or something in your life that affects your mental health?
Sample frame: All respondents (n=3,026)
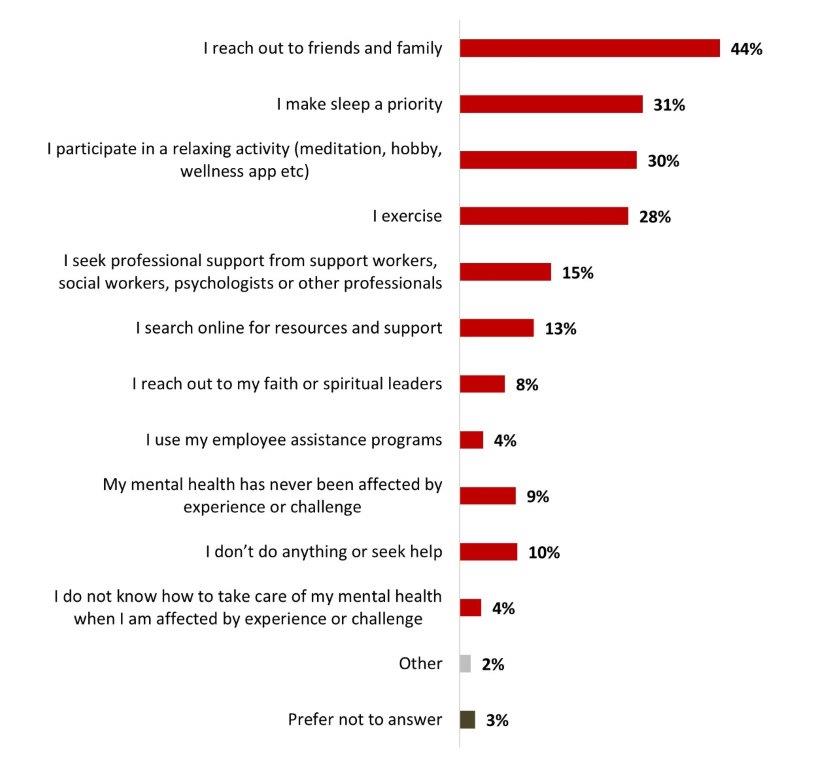
Figure 20.10: Text description
- I reach out to friends and family
- 44%
- I make sleep a priority
- 31%
- I participate in a relaxing activity (meditation, hobby, wellness app etc)
- 30%
- I exercise
- 28%
- I seek professional support from support workers, social workers, psychologists or other professionals
- 15%
- I search online for resources and support
- 13%
- I reach out to my faith or spiritual leaders
- 8%
- I use my employee assistance programs
- 4%
- My mental health has never been affected by experience or challenge
- 9%
- I don't do anything or seek help
- 10%
- I do not know how to take care of my mental health when I am affected by experience or challenge
- 4%
- Other
- 2%
- Prefer not to answer
- 3%
Significant differences regarding reasons to be worried include:
- Women were more likely to reach out to friends and family (52%)
- 18 to 34-years-olds (19%) were more likely to seek professional support
- Men were more likely to mention never having been affected by mental health challenges (12%) or of not doing anything to take care of their mental health (11%)
- Respondents with a university degree were more likely to exercise (37%), to make sleep a priority (36%), to participate in a relaxing activity (meditation, hobby, wellness app, etc.) (36%), to search online for resources and support (17%), or to reach out to their faith or spiritual leaders (7%).
- Black-identifying individuals (23%) and respondents who identify as Indigenous (12%) were more likely to reach out to their faith or spiritual leaders.
- Respondents who identify as 2SLGBTQIA+ (31%) and respondents living with a disability (27%) were more likely to seek professional support from support workers, social workers, psychologists or other professionals.
Availability of the services or resources (32%) and monetary cost (32%) are the main reasons that influence Canadians when it comes to services or resources used to manage a mental challenge, followed closely by the fact that it depends on how serious the challenge is (29%). A quarter on Canadians (26%) mentioned having never been in a situation where they would need to use mental health services or resources.
Figure 20.11: What factors, if any, influence the services or resources you use to manage a mental health challenge?
Sample frame: All respondents (n=3,026)
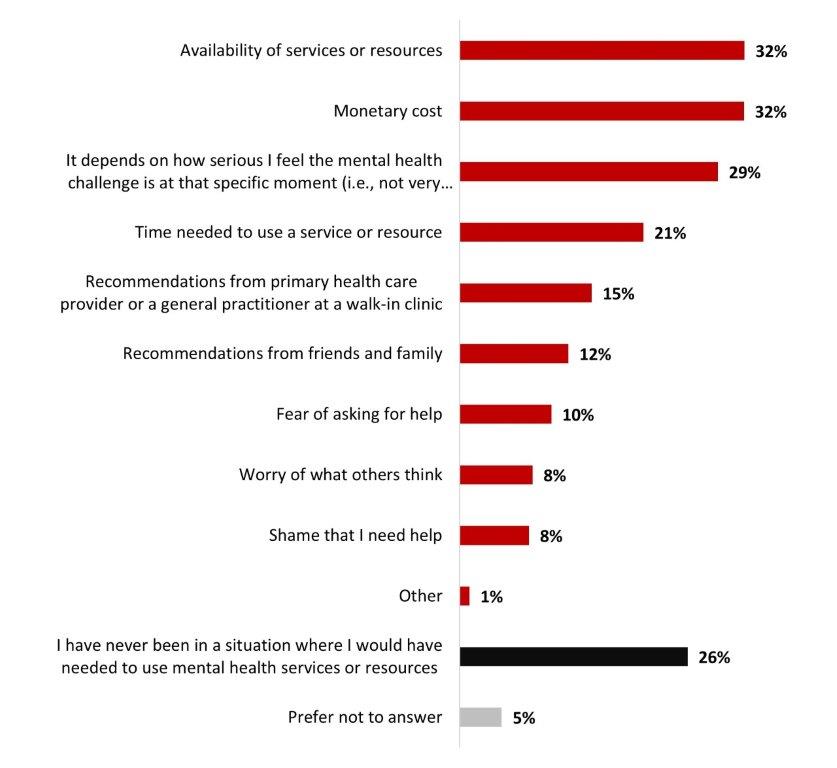
Figure 20.11: Text description
- Availability of services or resources
- 32%
- Monetary cost
- 32%
- It depends on how serious I feel the mental health challenge is at that specific moment (i.e., not very serious, somewhat serious, or very serious)
- 29%
- Time needed to use a service or resource
- 21%
- Recommendations from primary health care provider or a general practitioner at a walk-in clinic
- 15%
- Recommendations from friends and family
- 12%
- Fear of asking for help
- 10%
- Worry of what others think
- 8%
- Shame that I need help
- 8%
- Other
- 1%
- I have never been in a situation where I would have needed to use mental health services or resources
- 26%
- Prefer not to answer
- 5%
The following tables detail the significant differences between subgroups according to gender, age, and self-identifying status.
Table 20.12: What factors, if any, influence the services or resources you use to manage a mental health challenge?
Sample frame: All respondents (n=3,026)
Reading note: Significantly lower differences are marked with a "-" sign, while significantly higher differences are marked with a "+".
| Gender | Age | Self identifying | |||||
|---|---|---|---|---|---|---|---|
| Male | Female | 18-34 |
35-54 | 55+ | Respondents who identify as 2SLGBTQIA+ | Respondents living with a disability | |
| Availability of services or resources | 28% - | 36% + | 37% + | 35% | 26% - | 47% + | 41% + |
| Monetary cost | 27% - | 36% + | 41% + | 35% + | 23% - | 47% + | 41% + |
| It depends on how serious I feel the mental health challenge is at that specific moment (i.e., not very serious, somewhat serious, or very serious) | 25% - | 32% + | 33% + | 29% | 27% | 34% | 32% |
| Time needed to use a service or resource | 19% | 22% | 32% + | 25% + | 10% - | 28% + | 20% |
| Recommendations from primary health care provider or a general practitioner at a walk-in clinic | 15% | 15% | 16% | 14% | 14% | 15% | 17% |
| Recommendations from friends and family | 12% | 13% | 13% | 13% | 11% | 13% | 13% |
| Fear of asking for help | 9% - | 12% | 16% + | 10% | 7% - | 20% + | 17% + |
| Worry of what others think | 7% | 9% | 14% + | 8% | 5% - | 12% | 14% + |
| Shame that I need help | 6% - | 9% + | 12% + | 8% | 5% - | 13% + | 14% + |
| Other | 1% | 1% | 1% | 1% | 2% | 2% | 2% |
| I have never been in a situation where I would have needed to use mental health services or resources | 30% + | 22% - | 11% - | 18% - | 42% + | 11% - | 16% - |
| Prefer not to answer | 5% | 4% | 7% + | 6% | 2% - | 3% | 4% |
When thinking about the first step they would take to seek help for their mental health, a majority of Canadians mentioned going to their primary health care provider or a general practitioner at a walk-in clinic (38%). This is followed by reaching out to family or friends (25%). Other steps were mentioned by less than one respondents out of ten.
Figure 20.13: Who or what would be your first step when seeking help for mental health support, if needed?
Sample frame: All respondents (n=3,026)
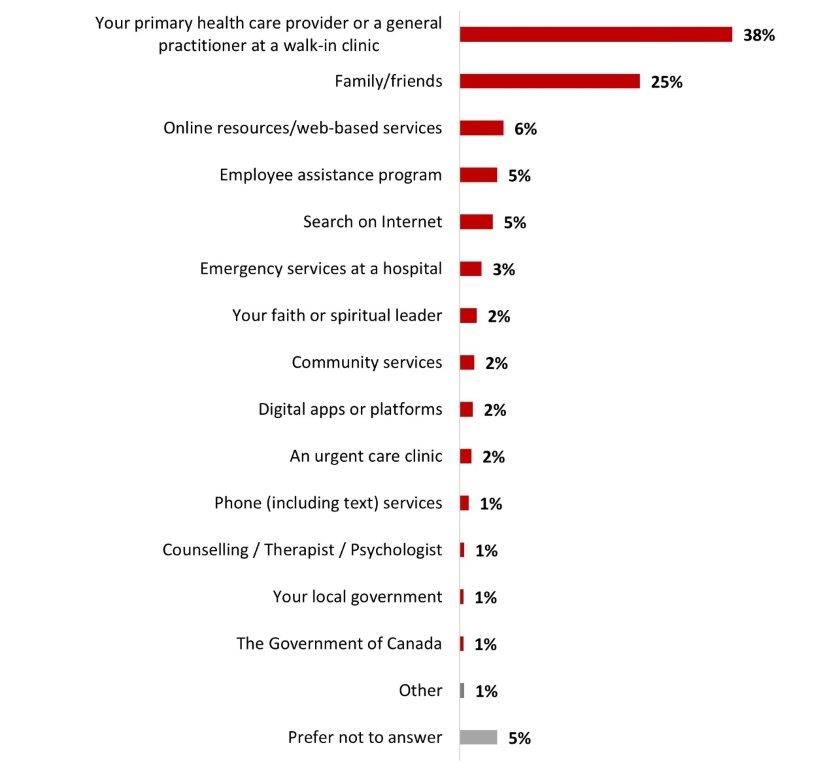
Figure 20.13: Text description
- Your primary health care provider or a general practitioner at a walk-in clinic
- 38%
- Family/friends
- 25%
- Online resources/web-based services
- 6%
- Employee assistance program
- 5%
- Search on Internet
- 5%
- Emergency services at a hospital
- 3%
- Your faith or spiritual leader
- 2%
- Community services
- 2%
- Digital apps or platforms
- 2%
- An urgent care clinic
- 2%
- Phone (including text) services
- 1%
- Counselling / Therapist / Psychologist
- 1%
- Your local government
- 1%
- The Government of Canada
- 1%
- Other
- 1%
- Prefer not to answer
- 5%
Significant differences regarding steps taken to seek help include:
- Respondents over 55 years old (49%) and women (40%) were more likely to go to their primary healthcare provider.
- 18 to 34-years-olds were more likely to reach out to family and friends (30%), to go for online resources/Web-based services (9%) or to use digital apps or platforms (4%).
- Respondents who identify as Indigenous (6%) were more likely to seek help through community services.
Six out of ten Canadians (61%) mentioned knowing how to access resources and tips for taking care of themselves. More than half (55%) mentioned knowing how to access in-person support from professionals. For the other resources surveyed, less than half of Canadians knew how to access them, more precisely, 44% knew how to access phone support, 42% knew how to access online/virtual support from support workers, 36% knew how to access digital apps or platforms, 35% knew how to access resources and services through their provincial government, 34% knew how to access from a local organization, 32% knew how to access resources and services through their local government as well as resources through the Government of Canada.
Figure 20.14: For each of the following mental health supports, please tell us if you would know how to access them if you needed to
Sample frame: All respondents (n=3,026)
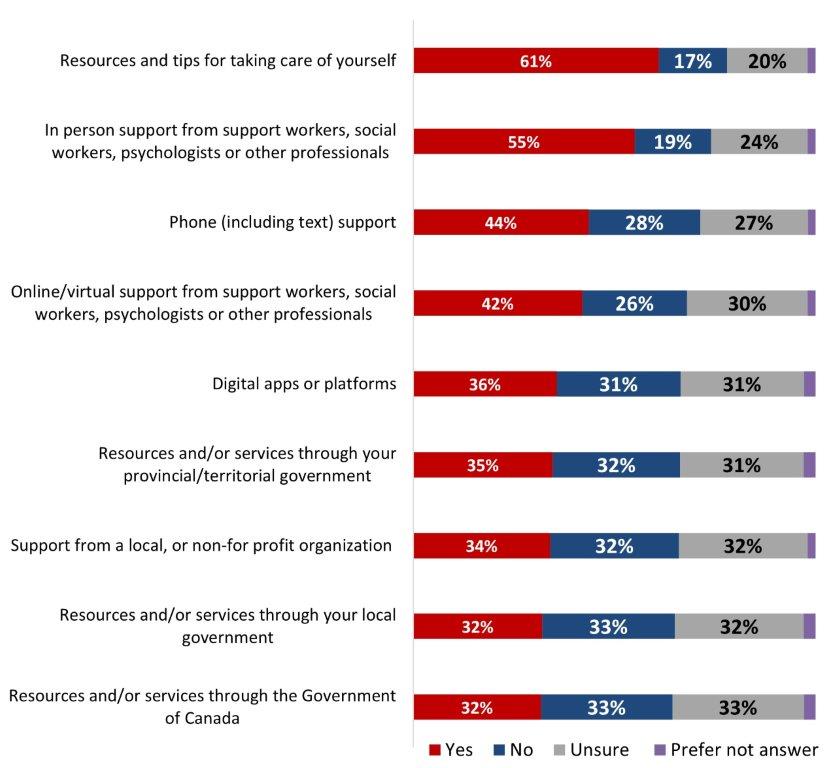
Figure 20.14: Text description
| Yes | No | Unsure | Prefer not answer | |
|---|---|---|---|---|
| Resources and tips for taking care of yourself | 61% | 17% | 20% | 2% |
| In person support from support workers, social workers, psychologists or other professionals | 55% | 19% | 24% | 2% |
| Phone (including text) support | 44% | 28% | 27% | 2% |
| Online/virtual support from support workers, social workers, psychologists or other professionals | 42% | 26% | 30% | 2% |
| Digital apps or platforms | 36% | 31% | 31% | 3% |
| Resources and/or services through your provincial/territorial government | 35% | 32% | 31% | 3% |
| Support from a local, or non-for profit organization | 34% | 32% | 32% | 2% |
| Resources and/or services through your local government | 32% | 33% | 32% | 3% |
| Resources and/or services through the Government of Canada | 32% | 33% | 33% | 3% |
The following tables detail the significant differences between subgroups according to gender, age, and self-identification status.
Table 20.15: For each of the following mental health supports, please tell us if you would know how to access them if you needed to
Sample frame: All respondents (n=3,026)
Reading note: Significantly lower differences are marked with a "-" sign, while significantly higher differences are marked with a "+".
| Gender | Age | Ethnicity | ||||||
|---|---|---|---|---|---|---|---|---|
| Male | Female | 18-34 |
35-54 | 55+ | White | Indigenous | Black | |
| Resources and tips for taking care of yourself | 55% - | 65% + | 61% |
62% | 59% | 61% | 64% | 59% |
| In person support from support workers, social workers, psychologists or other professionals | 51% - | 58% + | 48% - |
60% + | 55% | 55% | 63% + | 57% |
| Phone (including text) support | 41% - | 46% | 46% |
46% | 40% - | 43% | 51% + | 45% |
| Online/virtual support from support workers, social workers, psychologists or other professionals | 43% | 41% | 48% + |
45% + | 35% - | 40% - | 52% + | 45% |
| Digital apps or platforms | 35% | 37% | 51% + |
40% + | 22% - | 34% - | 44% + | 46% + |
| Resources and/or services through your provincial/territorial government | 38% + | 32% - | 31% - |
39% + | 34% | 33% - | 43% + | 38% |
| Support from a local, or non-for-profit organization | 33% | 35% | 31% |
37% + | 33% | 32% - | 44% + | 40% + |
| Resources and/or services through your local government | 35% + | 30% - | 29% |
35%+ | 31% | 30% - | 39% + | 34% |
| Resources and/or services through the Government of Canada | 35% + | 29% - | 30% |
37% + | 28% - | 29% - | 39% + | 36% |
Over half of Canadians (54%) feel either very (22%) or somewhat (32%) comfortable talking about their mental health needs with their relatives, while around one out of five Canadians (22%) are uncomfortable doing so (somewhat uncomfortable: 14%; very uncomfortable: 8%). One out of ten respondents (8%) mentioned feeling like they don't have any mental health needs.
Figure 20.16: How comfortable do you feel talking about your mental health needs with those closest to you?
Sample frame: All respondents (n=3,026)
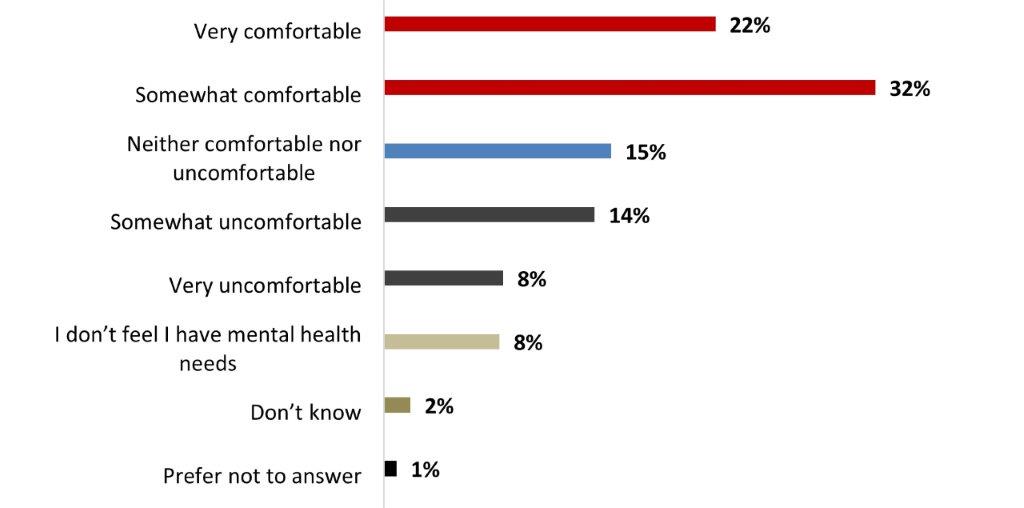
Figure 20.16: Text description
- Very comfortable
- 22%
- Somewhat comfortable
- 32%
- Neither comfortable nor uncomfortable
- 15%
- Somewhat uncomfortable
- 14%
- Very uncomfortable
- 8%
- I don't feel I have mental health needs
- 8%
- Don't know
- 2%
- Prefer not to answer
- 1%
The following subgroups were significantly more likely to state they were comfortable talking about their mental health needs to their relatives:
- Respondents living in the Atlantic provinces (64%)
- Respondents with a university degree (58%)
- Women (56% vs 51% of men)
The following subgroups were significantly more likely to state they were uncomfortable talking about their mental health needs to their relatives:
- Alberta residents (27%)
- Respondents living with a disability (27%)
- 18 to 34-years-olds (26%)
A strong majority of respondents (83%) indicated that they had not received mental health support in the month prior to the survey. In contrast, more than one out of ten respondents (15%) indicated that they had received some support in this regard.
Figure 20.17: In the past month, have you received any support for your mental health?
Sample frame: All respondents (n=3,026)
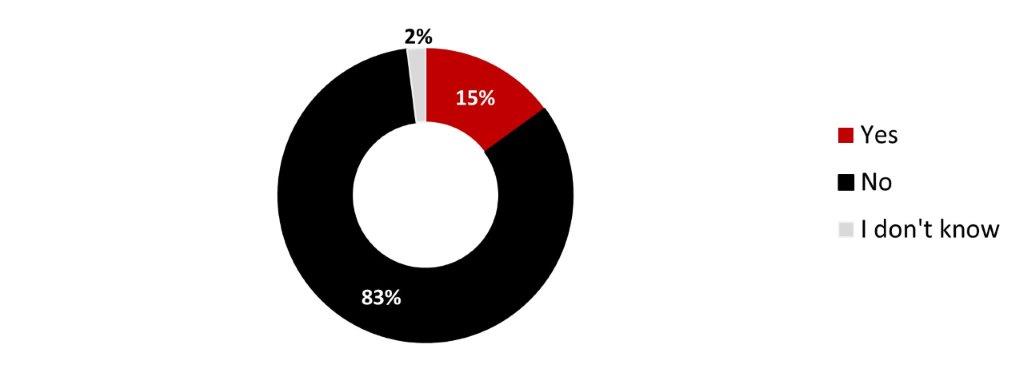
Figure 20.17: Text description
- Yes
- 15%
- No
- 83%
- I don't know
- 2%
The following subgroups were significantly more likely to have received support for coping with mental health:
- Respondents who identify as Indigenous (28%)
- Respondents who identify as 2SLGBTQIA+ (28%)
- Respondents living with a disability (26%)
- 18 to 34-years-olds (24%)
- Parents of children younger than 18 years old (19%)
- Women (17%)
- 35 to 54-years-olds (17%)
Of those who had received support during the previous month, most reported having received in-person support from social workers, psychologists or other professionals (31%), online and virtual support from social workers, psychologists or other professionals (28%). Primary health care provider (18%), resources and tips for taking care of yourself (18%), phone support (17%), and friends and family (12%) were also mentioned by more than one respondent out of ten. Other types of support were mentioned to a lesser extent.
Figure 20.18: What type of support have you received? Select all that apply.
Sample frame: Those who received support for their mental health in the past month (n=513)
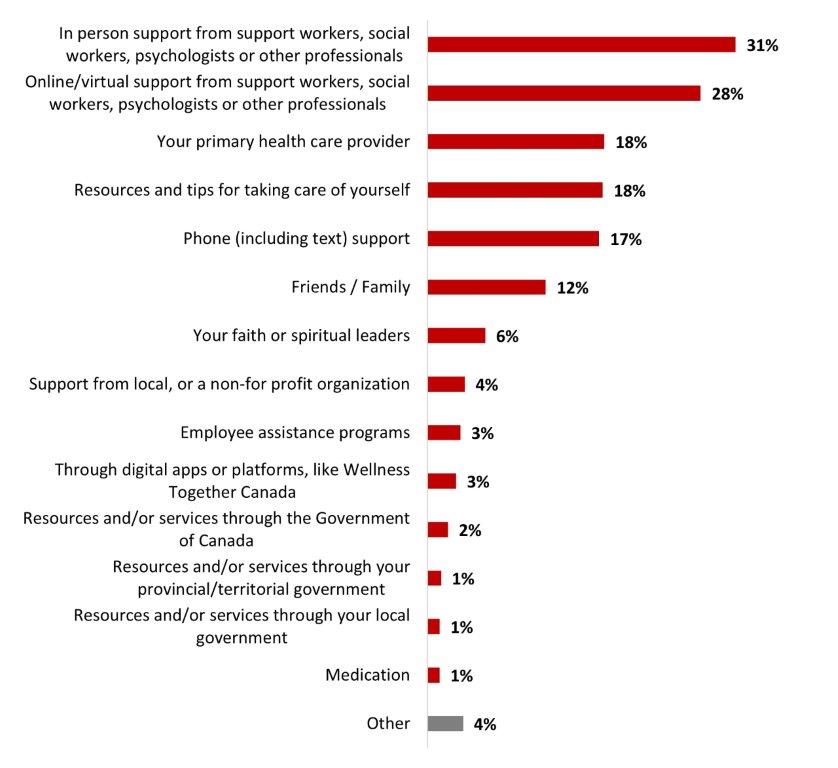
Figure 20.18: Text description
- In person support from support workers, social workers, psychologists or other professionals
- 31%
- Online/virtual support from support workers, social workers, psychologists or other professionals
- 28%
- Your primary health care provider
- 18%
- Resources and tips for taking care of yourself
- 18%
- Phone (including text) support
- 17%
- Friends / Family
- 12%
- Your faith or spiritual leaders
- 6%
- Support from local, or a non-for profit organization
- 4%
- Employee assistance programs
- 3%
- Through digital apps or platforms, like Wellness Together Canada
- 3%
- Resources and/or services through the Government of Canada
- 2%
- Resources and/or services through your provincial/territorial government
- 1%
- Resources and/or services through your local government
- 1%
- Medication
- 1%
- Other
- 4%
Significant differences in terms of mental health support include:
- Men were more likely to turn to online/virtual support (35% vs 22% for women).
- 18 to 34-years-olds were more likely to turn to online/virtual support (38% vs 9% for respondents over 55 years old) and to use resources and tips for taking care of themselves (25% vs 10% for respondents over 55 years old).
- Respondents with an annual income of more than $80 000 (38%), Ontarians (35%) and parents of children younger than 18 years old (35%) were more likely to turn to online or virtual support.
- Respondents living with a disability were more likely to turn to in-person support (43%) and phone support (28%).
- Respondents who identify as Indigenous (31%) were more likely to turn to phone support.
Of those who had not received support for their mental health during the previous month, more than half (54%) reported that they did not need support and one out of four (25%) stated that they prefer to manage their mental health themselves. Other reasons were mentioned to a lesser extent.
Figure 20.19: Why have you not received any support for your mental health?
Sample frame: Those who have not received support for their mental health in the past month (n=2,456)
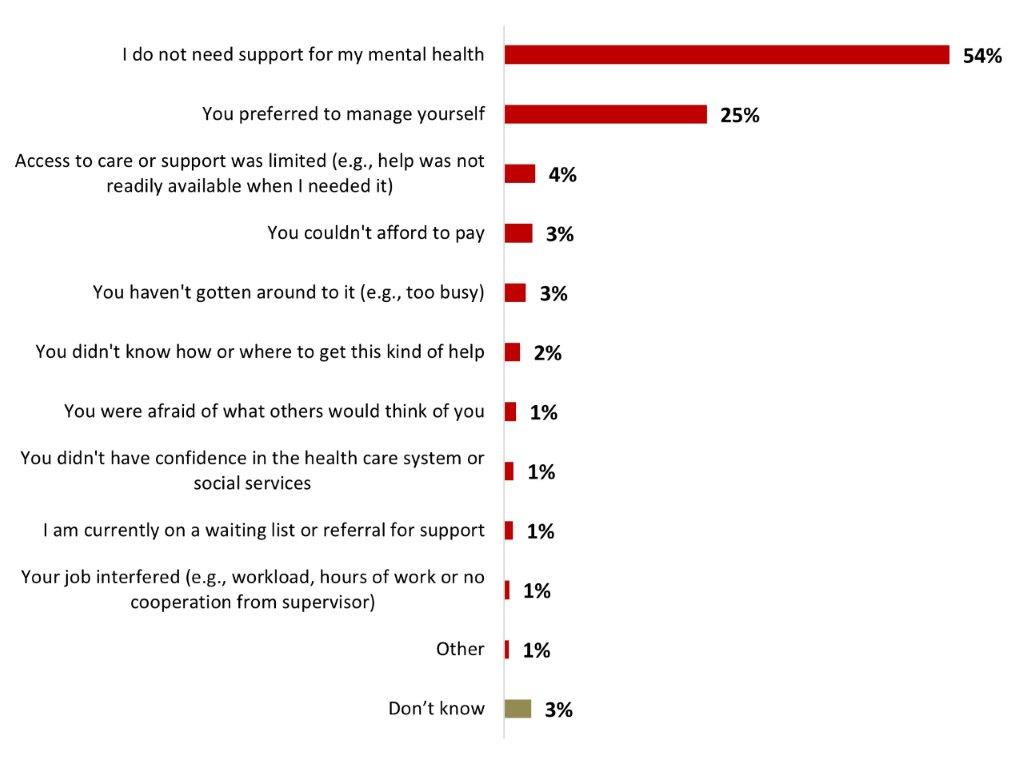
Figure 20.19: Text description
- I do not need support for my mental health
- 54%
- You preferred to manage yourself
- 25%
- Access to care or support was limited (e.g., help was not readily available when I needed it)
- 4%
- You couldn't afford to pay
- 3%
- You haven't gotten around to it (e.g., too busy)
- 3%
- You didn't know how or where to get this kind of help
- 2%
- You were afraid of what others would think of you
- 1%
- You didn't have confidence in the health care system or social services
- 1%
- I am currently on a waiting list or referral for support
- 1%
- Your job interfered (e.g., workload, hours of work or no cooperation from supervisor)
- 1%
- Other
- 1%
- Don't know
- 3%
Significant differences in terms of reasons not to seek mental health support services include:
- Respondents over 55 years old (71%) were more likely to mention not needing any support for their mental health, while 18 to 34-years-olds (34%) and the 35 to 54-years-olds (29%) were more likely to prefer to manage their issues themselves.
- Quebec residents were more likely to mention not needing any support for their mental health (59%).
- Parents of children younger than 18 years old (31%) were more likely to prefer to manage their issues themselves, while those who were not parents of any children younger than 18 years old were more likely to state not needing mental health support (58%).
Respondents were asked to rate each statement according to their level of agreement with it. Nine out of ten (90%) agreed that doing something enjoyable contributes to good mental health. Fewer respondents (84%) agreed that mental health is interconnected with physical health, and central to overall health and well-being and more than eight out of ten (81%) agreed that factors such as resiliency and coping contribute to good mental health. Seven respondents out of ten (71%) agreed that perceived control over life contributes to good mental health. Two-thirds (66%) agreed that they know when they need help with my mental health. A smaller number of respondents agreed that they have enough time to take care of their mental health (61%) and that they practice taking care of their mental health on a regular basis (59%). More than half of respondents agreed that they know how or where to get help for their mental health (57%), that they think they can manage their mental health struggles on their own (56%), that they are aware of free mental health and substance use resources online or by phone (52%), and that spirituality contributes to good mental health (52%). Less than half of respondents agreed on the following statements: I feel I have adequate access to mental health support services (47%), I can afford to see a mental health therapist such as a social worker, psychologist, or counsellor (41%), I can afford mental health support (40%), it's hard to ask for help if I'm struggling with my mental health (38%).
Table 20.20: To what extent do you agree or disagree with the following statements?
Sample frame: All respondents (n=3,026)
| %Total Agree | Strongly agree | Somewhat agree | Neither agree nor disagree | Somewhat disagree | Strongly disagree | Unsure / Not applicable | |
|---|---|---|---|---|---|---|---|
| Doing something enjoyable contributes to good mental health. | 90% | 53% | 37% | 7% | 1% | 0% | 2% |
| Mental health is interconnected with physical health, and central to overall health and well-being. | 84% | 47% | 37% | 10% | 2% | 0% | 3% |
| Factors such as resiliency and coping contribute to good mental health. | 81% | 36% | 45% | 12% | 2% | 0% | 4% |
| Perceived control over life contributes to good mental health. | 71% | 25% | 46% | 18% | 4% | 1% | 6% |
| I know when I need help with my mental health. | 66% | 25% | 41% | 20% | 6% | 2% | 7% |
| I have enough time to take care of my mental health. | 61% | 22% | 39% | 21% | 10% | 4% | 4% |
| I practice taking care of my mental health on a regular basis. | 59% | 19% | 40% | 26% | 8% | 3% | 4% |
| I know how or where to get help for my mental health | 57% | 20% | 37% | 19% | 11% | 5% | 9% |
| I think I can manage my mental health struggles on my own | 56% | 16% | 41% | 23% | 10% | 5% | 5% |
| I am aware of free mental health and substance use resources online or by phone | 52% | 18% | 34% | 17% | 12% | 8% | 11% |
| Spirituality contributes to good mental health. | 52% | 23% | 30% | 25% | 7% | 7% | 9% |
| I feel I have adequate access to mental health support services | 47% | 14% | 33% | 23% | 10% | 7% | 12% |
| I can afford to see a mental health therapist such as a social worker, psychologist, or counsellor | 41% | 15% | 26% | 18% | 14% | 18% | 9% |
| I can afford mental health support | 40% | 14% | 25% | 20% | 13% | 17% | 10% |
| It's hard to ask for help if I'm struggling with my mental health | 38% | 11% | 27% | 24% | 17% | 11% | 11% |
The following table details the significant differences between subgroups according to age, ethnicity, and gender.
Reading note: In the following tables, significantly lower differences are marked with a "-" sign, while significantly higher differences are marked with a "+".
Table 20.21: To what extent do you agree or disagree with the following statements?
| Gender | Age | Ethnicity | ||||||
|---|---|---|---|---|---|---|---|---|
| Male | Female | 18-34 | 35-54 | 55+ | White | Indigenous | Black | |
| Doing something enjoyable contributes to good mental health. | 88% - | 92% + | 82% - | 90% | 95% + | 91% + | 94% + | 88% |
| Mental health is interconnected with physical health, and central to overall health and well-being. | 82% - | 86% + | 82% | 83% | 87% + | 85% | 83% | 81% |
| Factors such as resiliency and coping contribute to good mental health. | 79% - | 83% + | 73% - | 80% | 87% + | 83% + | 78% | 77% |
| Perceived control over life contributes to good mental health. | 70% | 71% | 69% | 67% - | 76% + | 71% | 77% + | 68% |
| I know when I need help with my mental health. | 62% - | 70% + | 60% - | 66% | 69% + | 66% | 74% + | 67% |
| I have enough time to take care of my mental health. | 61% | 61% | 46% - | 54% - | 76% + | 62% + | 64% | 57% |
| I practice taking care of my mental health on a regular basis. | 55% - | 62% + | 54% - | 60% | 62% + | 59% | 63% | 65% + |
| I know how or where to get help for my mental health | 55% | 58% | 54% | 58% | 57% | 57% | 66% + | 58% |
| I think I can manage my mental health struggles on my own | 61% + | 53% - | 53% | 54% | 60% + | 56% | 61% | 54% |
| I am aware of free mental health and substance use resources online or by phone | 54% | 51% | 51% | 56% + | 50% - | 52% | 63% + | 55% |
| Spirituality contributes to good mental health. | 47% - | 57% + | 47% - | 54% | 54% | 48% - | 61% + | 74% + |
| I feel I have adequate access to mental health support services | 49% | 46% | 47% | 49% | 46% | 47% | 57% + | 50% |
| I can afford to see a mental health therapist such as a social worker, psychologist, or counsellor | 46% + | 36% - | 35% - | 41% | 46% + | 41% | 42% | 38% |
| I can afford mental health support | 44% + | 35% - | 34% - | 41% | 43% + | 41% | 42% | 35% |
| It's hard to ask for help if I'm struggling with my mental health | 35% | 39% | 47% + | 43% + | 27% - | 36% - | 40% | 37% |
Of those who think it can be hard to ask for help when they are struggling, a quarter (25%) mentioned it being because they think they cannot afford mental health support or because they are worried about what others would think of them (24%). A fifth of respondents who admit that it can be hard to ask for help mentioned it being because they don't think that their concerns warrant outside help (20%), that they are not sure their concern would be understood (19%), that they are not sure where to look for help (18%), that they are worried no one would understand (17%), or that they do not have the time for that (16%). Other reasons were mentioned by fewer respondents.
Figure 20.22: Why do you think it is hard to ask for help if you are struggling with your mental health?
Sample frame: Respondents who find it hard asking for mental health or are unsure (n=2,213)
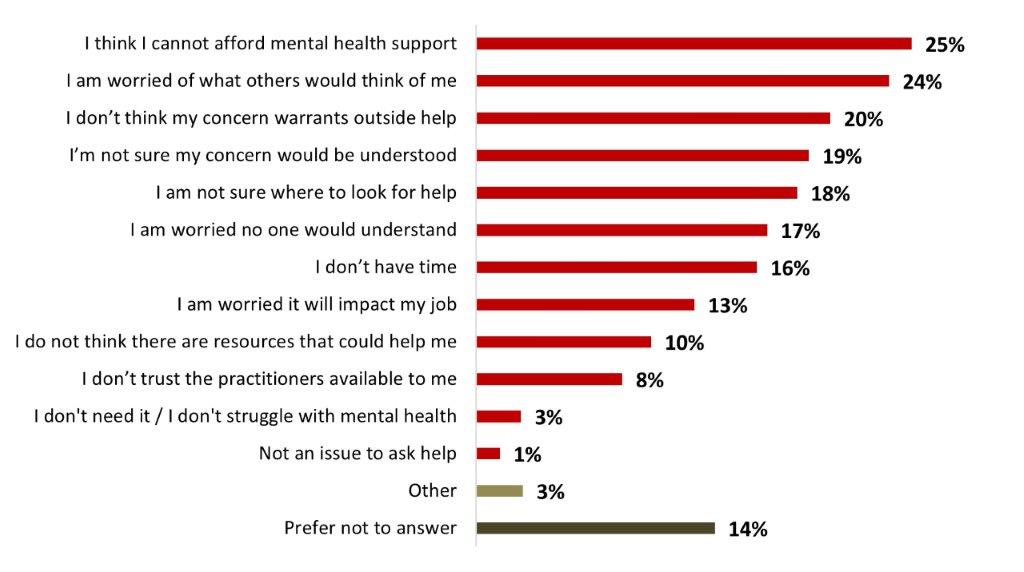
Figure 20.22: Text description
- I think I cannot afford mental health support
- 25%
- I am worried of what others would think of me
- 24%
- I don't think my concern warrants outside help
- 20%
- I'm not sure my concern would be understood
- 19%
- I am not sure where to look for help
- 18%
- I am worried no one would understand
- 17%
- I don't have time
- 16%
- I am worried it will impact my job
- 13%
- I do not think there are resources that could help me
- 10%
- I don't trust the practitioners available to me
- 8%
- I don't need it / I don't struggle with mental health
- 3%
- Not an issue to ask help
- 1%
- Other
- 3%
- Prefer not to answer
- 14%
Significant differences in terms of reasons not to seek mental health support services include:
- 18 to 34-year-olds were more likely to mention finding it hard to ask for help because they can not afford it (34%), because they don't have time (29%), because they are worried about what others would think of them (28%) or because they are not sure their problem would be understood (23%).
- Respondents over 55 years old (28%) were more likely to think their concerns do not warrant outside help.
- Respondents from Alberta (34%), respondents with an annual income of less than 40K (31%) and women (29%) were more likely to think they can not afford help.
- Black-identifying individuals were more likely to be worried about what others would think of them (32%) or to worry that it would impact their job (18%).
- Parents of children younger than 18 years old were more likely to mention not having the time (24%) and concerns about it impacting their job (21%).
More than half of Canadians (55%) would like to find links to free support services on the Government Website. Around a third would like to find links to crisis lines or distress centres (35%) or links to organizations providing online counselling (32%) and around a quarter would like to find tips for improving their mental health (26%) or tips on how to cope with stress and life's challenges (24%). Other types of information were mentioned to a lesser extent.
Figure 20.23: What kind of information would you like to find on a Government of Canada mental health website?
Sample frame: All respondents (n=3,026)
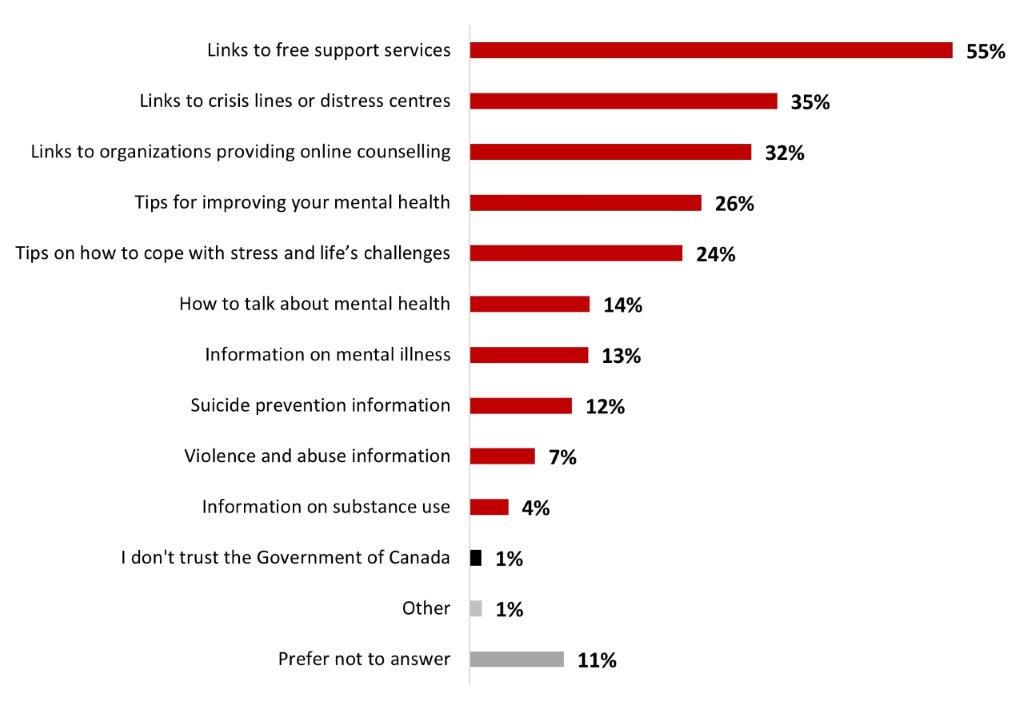
Figure 20.23: Text description
- Links to free support services
- 55%
- Links to crisis lines or distress centres
- 35%
- Links to organizations providing online counselling
- 32%
- Tips for improving your mental health
- 26%
- Tips on how to cope with stress and life's challenges
- 24%
- How to talk about mental health
- 14%
- Information on mental illness
- 13%
- Suicide prevention information
- 12%
- Violence and abuse information
- 7%
- Information on substance use
- 4%
- I don't trust the Government of Canada
- 1%
- Other
- 1%
- Prefer not to answer
- 11%
Significant differences in terms of information wanted on the Government Website include:
- Women were more likely to want to see links to free support services (60% vs 50% for men) and tips on how to cope with stress and life's challenges (28% vs 20% for men).
- 18 to 34-year-olds were more likely to want to see information on violence and abuse (12%) and information about how to talk about mental health (17%).
- Respondents over 55 years old were more likely to want to see links to free support services (59%), links to crisis lines or distress centres (38%), or links to organizations providing online counselling (35%).
- Respondents who identify as 2SLGBTQIA+ were more likely to want to see information on suicide prevention information (19%).
6.3 COVID-19 vaccine
A high proportion of respondents (91%) reported having received at least one dose of the COVID-19 vaccine. On average, Canadians have received 3.3 doses of the COVID-19 vaccine. Very few respondents reported receiving only one dose (1%). Most respondents indicated that they had received two doses (25%), three doses (26%), four doses (25%) or five doses (14%). Less than one out of ten respondents (7%) mentioned not receiving any doses against COVID-19.
Figure 20.24: How many doses of the COVID-19 vaccine have you received?
Sample frame: All respondents (n=3,026)
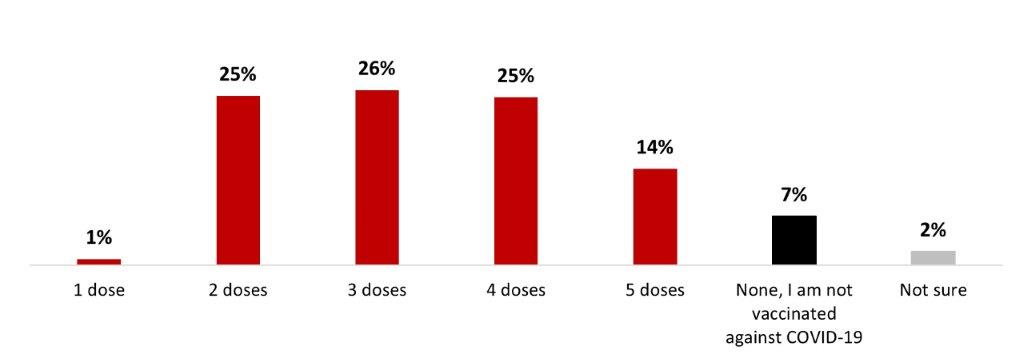
Figure 20.24: Text description
- 1 dose
- 1%
- 2 doses
- 25%
- 3 doses
- 26%
- 4 doses
- 25%
- 5 doses
- 14%
- None, I am not vaccinated against COVID-19
- 7%
- Not sure
- 2%
The following subgroups were more likely to have received at least one dose of the COVID-19 vaccine:
- Respondents over 55 years old (3.9 doses)
- Those who are at-risk of severe COVID-19 disease (3.8 doses)
- Those who are more confident in vaccines since the pandemic (3.8 doses)
- Those who are not parents of children younger than 18 years old (3.5 doses)
- British Columbia and Territories respondents (3.4 doses)
- Respondents with a university degree (3.4 doses)
- White respondents (3.4 doses)
- Those who had not been infected with COVID-19 (3.5)
The following subgroups were significantly less vaccinated than their complement:
- 18 to-34-year-olds (2.7 doses)
- Black-identifying individuals (2.7 doses)
- Parents of children younger than 18 years old (2.9 doses)
- 35 to 54-year-olds (3.0 doses)
- Those who are not at-risk of severe COVID-19 disease (3.0 doses)
- Residents of Alberta (3.0 doses)
- Respondents with a high school degree or less (3.1 doses)
- Respondents who identify as Indigenous (3.1 doses)
- Those who have been infected with COVID-19 (3.1)
Of those who said they had received at least one dose of COVID-19 vaccine (or were unsure), we asked if they had had any booster doses. Three out of four respondents (72%) reported receiving at least one booster dose of COVID-19. One-fourth (25%) reported that they had received one booster dose, more than one out of five (22%) reported that they had had two booster doses, and almost one-fourth (24%) reported that they had received three booster doses. Almost three out of ten (28%) stated they did not receive a booster dose.
Figure 20.25: Have you received a COVID-19 booster dose?
Sample frame: Respondents who have received at least one dose or who are unsure about it (n=2,809)
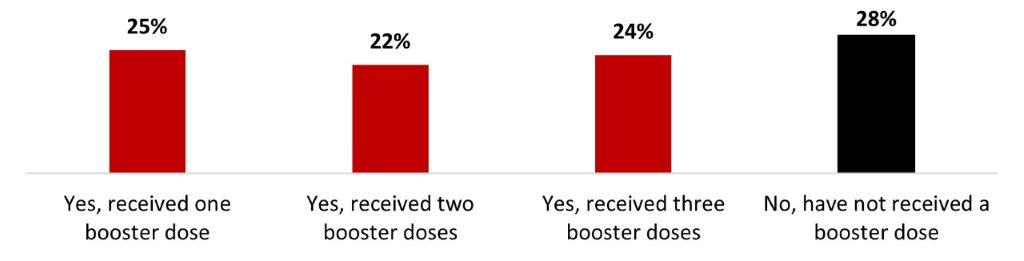
Figure 20.25: Text description
- Yes, received one booster dose
- 5%
- Yes, received two booster doses
- 22%
- Yes, received three booster doses
- 24%
- No, have not received a booster dose
- 28%
The following subgroups were significantly more likely to have received at least one booster dose:
- 55-year-olds or older (84%)
- Those living in British Columbia and the Territories (80%)
- Those with a university degree (80%)
- Respondents who identify as 2SLGBTQIA+ (78%)
- Those living with a disability (77%)
- Those who are not parents of children younger than 18 years old (76%)
- White-identifying individuals (74%)
The following subgroups were significantly more likely not to have received a booster dose:
- 18 to 34-year-olds (36%) and 35 to 54-year-olds (36%) respondents
- Albertans (36%)
- Those who earn less than $40,000 (33%)
- Those with a high school degree or less (33%)
- Black-identifying individuals (51%)
- Parents of children younger than 18 years old (40%)
Over a quarter of respondents who have received at least one dose got their latest one less than three months ago (27%), around a third (34%) had gotten it between 3-6 months prior (34%), and one-fourth had gotten it six months to a year prior (25%) to the survey. One respondent out of ten (13%) stated their latest dose was over a year prior (5%).
Figure 20.26: When did you receive your most recent COVID-19 booster dose?
Sample frame: Respondents who have received at least one dose (n=2,011)
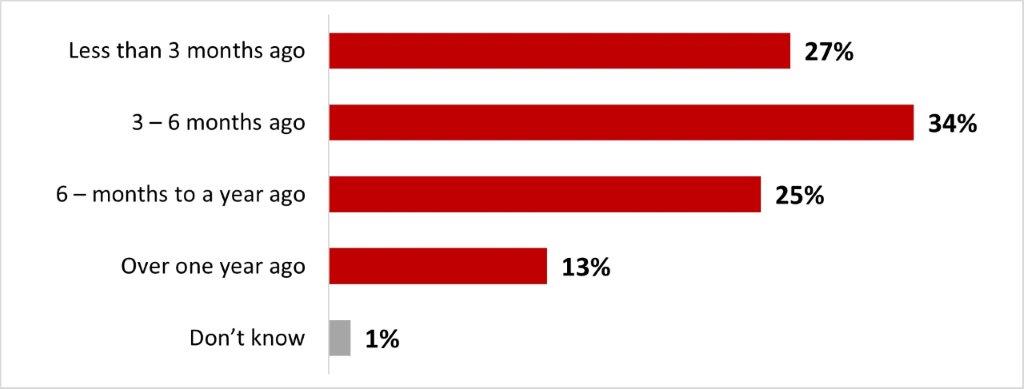
Figure 20.26: Text description
- Less than 3 months ago
- 27%
- 3 – 6 months ago
- 34%
- 6 – months to a year ago
- 25%
- Over one year ago
- 13%
- Don't know
- 1%
The following subgroups were significantly more likely to have gotten their latest dose less than three months before the survey:
- Residents of the Atlantic provinces (39%)
- Respondents over 55 years old (34%)
- Respondents who considered themselves at risk of having a severe disease (32%)
- Those who had not been infected with COVID-19 (30%)
The following subgroups were significantly more likely to have gotten their latest dose over one year before the survey:
- 18 to 34-year-olds (18%) and 35 to 54-year-olds (17%)
- Women (15%)
Among those who had received at least one dose of vaccine, six out of ten respondents (61%) reported that they were likely to keep their booster doses up to date: 39% very likely and 22% somewhat likely. In contrast, about a third of respondents (33%) said they were unlikely to do so: 16% not very likely and 16% not at all likely.
Figure 20.27: How likely are you to keep your COVID-19 doses up to date (i.e. continue to receive them as you become eligible for additional doses)?
Sample frame: Respondents who have received at least one dose (n=2,766)
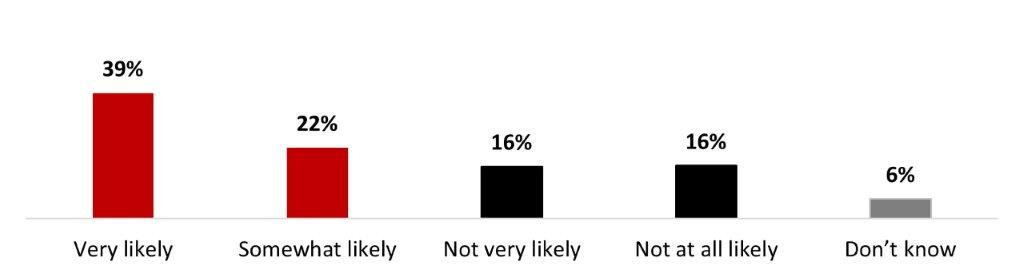
Figure 20.27: Text description
- Very likely
- 39%
- Somewhat likely
- 22%
- Not very likely
- 16%
- Not at all likely
- 16%
- Don't know
- 6%
The following subgroups were significantly more likely to state it's likely (very or somewhat) that they keep their COVID-19 doses up to date:
- Respondents over 55 years old (76%)
- Respondents from British Columbia and Territories (72%)
- Men (65%)
- Respondents who identify as 2SLGBTQIA+ (69%)
- Those with a university degree (69%)
- Individuals who are not parents of children younger than 18 years old (64%)
Top reasons for being unlikely or uncertain about getting a booster dose among those who did not receive booster doses or were unsure about it are that think they are protected enough with the number of vaccines they had received (18%), that they are concerned about the long-term effects of the vaccine (15%), that they feel the vaccine does not provide much protection as you can still get COVID-19 even if they are vaccinated (13%) and that they are fed up with getting vaccinated (12%). Other reasons were mentioned by less than one respondent out of ten.
Figure 20.28: What is the top reason you are unlikely or uncertain about getting a booster dose?
Sample frame: Those who have not received a booster dose or are unsure about it (n=1,076)
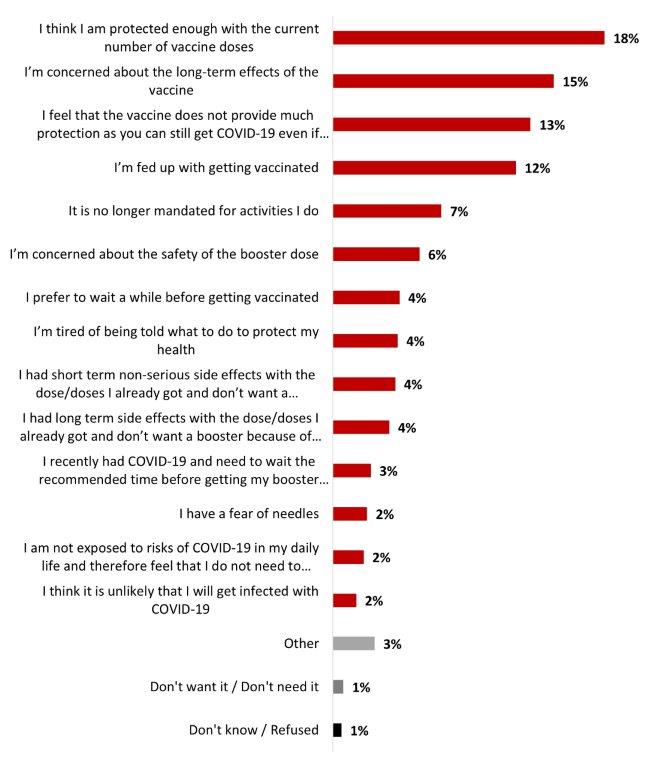
Figure 20.28: Text description
- I think I am protected enough with the current number of vaccine doses
- 18%
- I'm concerned about the long-term effects of the vaccine
- 15%
- I feel that the vaccine does not provide much protection as you can still get COVID-19 even if vaccinated
- 13%
- I'm fed up with getting vaccinated
- 12%
- It is no longer mandated for activities I do
- 7%
- I'm concerned about the safety of the booster dose
- 6%
- I prefer to wait a while before getting vaccinated
- 4%
- I'm tired of being told what to do to protect my health
- 4%
- I had short term non-serious side effects with the dose/doses I already got and don't want a booster because of this
- 4%
- I had long term side effects with the dose/doses I already got and don't want a booster because of this
- 4%
- I recently had COVID-19 and need to wait the recommended time before getting my booster dose
- 3%
- I have a fear of needles
- 2%
- I am not exposed to risks of COVID-19 in my daily life and therefore feel that I do not need to receive a booster dose
- 2%
- I think it is unlikely that I will get infected with COVID-19
- 2%
- Other
- 3%
- Don't want it / Don't need it
- 1%
- Don't know / Refused
- 1%
Significant differences include:
- Women were more likely to mention that they feel the vaccine does not provide much protection as you can still get COVID-19 even if vaccinated (17%) or that they are concerned about the long-term effects of the vaccine (17%).
- Men were more likely to mention being fed up with getting vaccinated (15%) or that it is not mandatory anymore for the activities they practice (10%).
- Respondents aged 55 years old or older were more likely to mention that they feel like the vaccine does not provide much protection as you can still get COVID-19 even if vaccinated (19%)
- 18 to 34 year-olds were more likely to mention that it is not mandatory anymore for the activities they practiced (10%).
- Respondents living in Quebec were more likely to mention feeling like they are protected enough with their current number of vaccine doses (25%).
- Respondents living in Alberta were more likely to mention being concerned about the safety of the booster dose (14%).
The top motivation to get a booster dose among the respondents who have not gotten a booster dose yet is to have more knowledge about the safety of booster doses (14%). Other reasons were mentioned by less than one respondents out of ten and almost half of respondents (46%) would not be motivated by any factors.
Figure 20.29: Among the following factors and thinking about the current COVID-19 situation, what would motivate you to get your booster dose?
Sample frame: Respondents who have not gotten a booster dose (n=798)
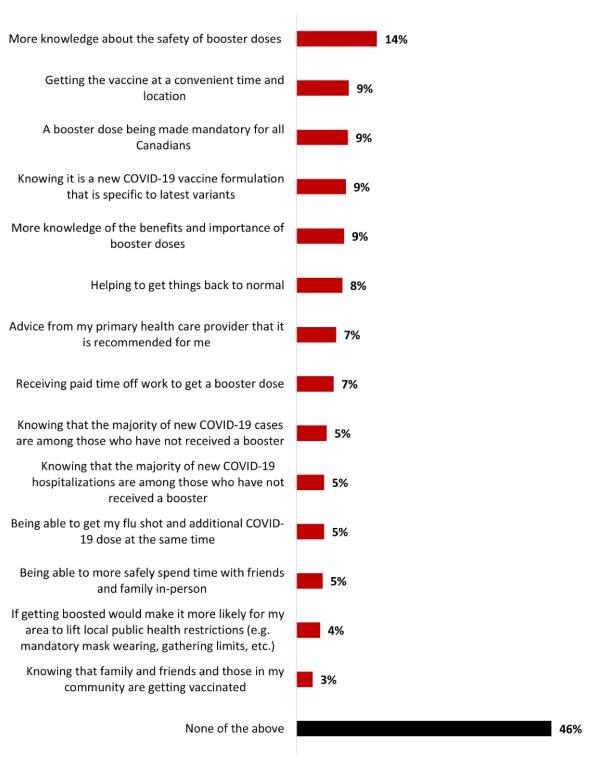
Figure 20.29: Text description
- More knowledge about the safety of booster doses
- 14%
- Getting the vaccine at a convenient time and location
- 9%
- A booster dose being made mandatory for all Canadians
- 9%
- Knowing it is a new COVID-19 vaccine formulation that is specific to latest variants
- 9%
- More knowledge of the benefits and importance of booster doses
- 9%
- Helping to get things back to normal
- 8%
- Advice from my primary health care provider that it is recommended for me
- 7%
- Receiving paid time off work to get a booster dose
- 7%
- Knowing that the majority of new COVID-19 cases are among those who have not received a booster
- 5%
- Knowing that the majority of new COVID-19 hospitalizations are among those who have not received a booster
- 5%
- Being able to get my flu shot and additional COVID-19 dose at the same time
- 5%
- Being able to more safely spend time with friends and family in-person
- 5%
- If getting boosted would make it more likely for my area to lift local public health restrictions (e.g. mandatory mask wearing, gathering limits, etc.)
- 4%
- Knowing that family and friends and those in my community are getting vaccinated
- 3%
- None of the above
- 46%
Significant differences include:
- Respondents from the Atlantic provinces were more likely to mention wanting to have more knowledge about the safety of booster doses (30%).
- Respondents living with a disability (14%) were more likely to mention knowing that the majority of new COVID-19 hospitalizations are among those who have not received a booster as a motivation.
- 18 to 34-year-olds were more likely to mention being motivated by receiving paid time off work to get a booster doses (11%) and if getting boosted would make it more likely for their area to lift local public health restrictions (8%).
Respondents who received at least one booster dose were asked if they have ever been reluctant to get a COVID-19 booster dose, and a little over one out of five said yes (22%), while three out of four have never been reluctant.
Figure 20.30: Have you ever been reluctant or hesitated to get a COVID-19 booster dose?
Sample frame: Respondents who have received at least one booster dose (n=2,011)
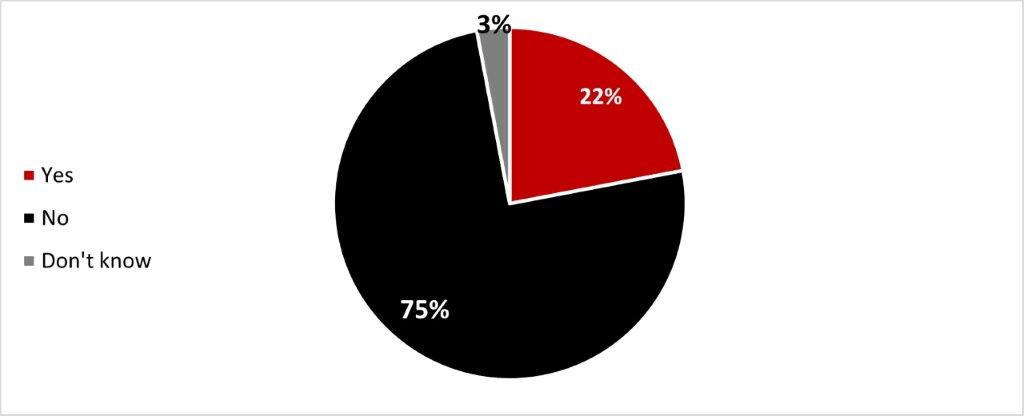
Figure 20.30: Text description
- Yes
- 22%
- No
- 75%
- Don't know
- 3%
The following subgroups were significantly more likely to express they were reluctant to get a COVID-19 booster dose:
- Women (27%)
- 18 to 34-year-olds (30%) and 35 to 54-year-olds (29%)
- Black-identifying individuals (31%)
- Parents of children younger than 18 years old (31%)
- Those who have been infected with COVID-19 (27%).
Respondents who were reluctant to get a COVID-19 booster dose mentioned concerns about the safety and/or side effects of having a booster dose as their main reason for reluctance (59%), way ahead of other reasons that were mentioned by less than one-fifth of respondents.
Figure 20.31: For which reasons were you reluctant to get a COVID-19 booster dose?
Sample frame: Respondents who were reluctant to get a COVID-19 booster dose (n=451)
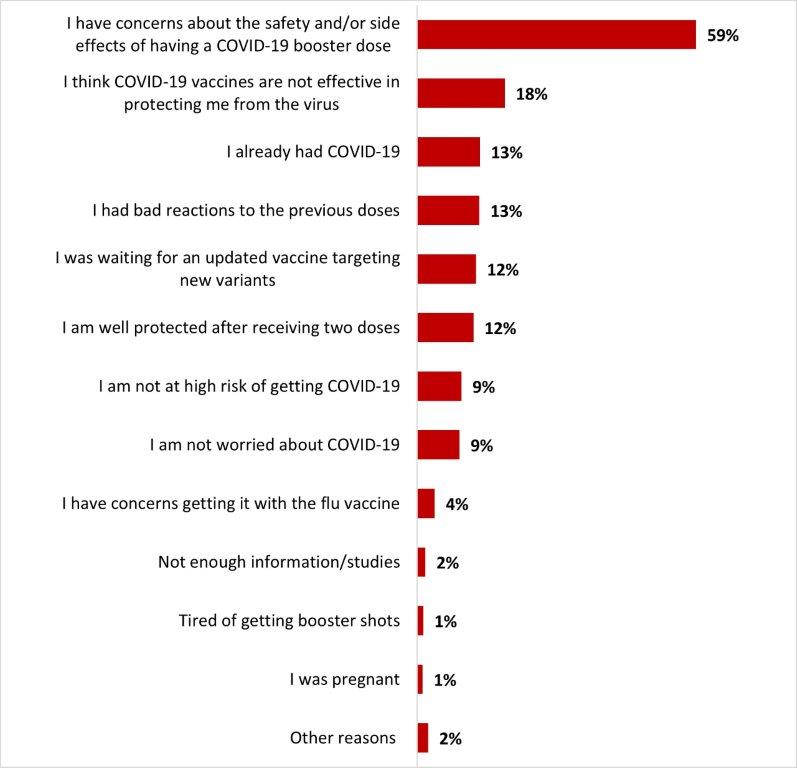
Figure 20.31: Text description
- I have concerns about the safety and/or side effects of having a COVID-19 booster dose
- 59%
- I think COVID-19 vaccines are not effective in protecting me from the virus
- 18%
- I already had COVID-19
- 13%
- I had bad reactions to the previous doses
- 13%
- I was waiting for an updated vaccine targeting new variants
- 12%
- I am well protected after receiving two doses
- 12%
- I am not at high risk of getting COVID-19
- 9%
- I am not worried about COVID-19
- 9%
- I have concerns getting it with the flu vaccine
- 4%
- Not enough information/studies
- 2%
- Tired of getting booster shots
- 1%
- I was pregnant
- 1%
- Other reasons
- 2%
Significant differences in terms of reasons for reluctance include:
- Women were more likely to mention they had bad reactions to the previous doses (16%), while men were more likely to state not being worried about COVID-19 (14%).
- Alberta residents were more likely to express their concerns over the safety and/or side effects of the booster (77%).
- Black-identifying individuals were more likely to think COVID-19 vaccines are not effective in protecting against the virus (34%).
- Those who have been infected with COVID-19 were more likely to think COVID-19 vaccines are not effective in protecting against the virus (22%).
Respondents who were reluctant to get a COVID-19 booster dose were then asked what made them decide to get the booster despite their initial reluctance. Almost a third mentioned the high number of COVID-19 cases (32%), and one-fourth mentioned that benefits were more important than the risks (24%). One person out of five mentioned it was recommended to them by a healthcare professional (21%) and that they feared regretting if they didn't (20%). Other reasons were mentioned by 16% or less of respondents.
Figure 20.32: What made you decide to get a COVID-19 booster dose despite your initial reluctance?
Sample frame: Respondents who were reluctant to get a COVID-19 booster dose (n=451)
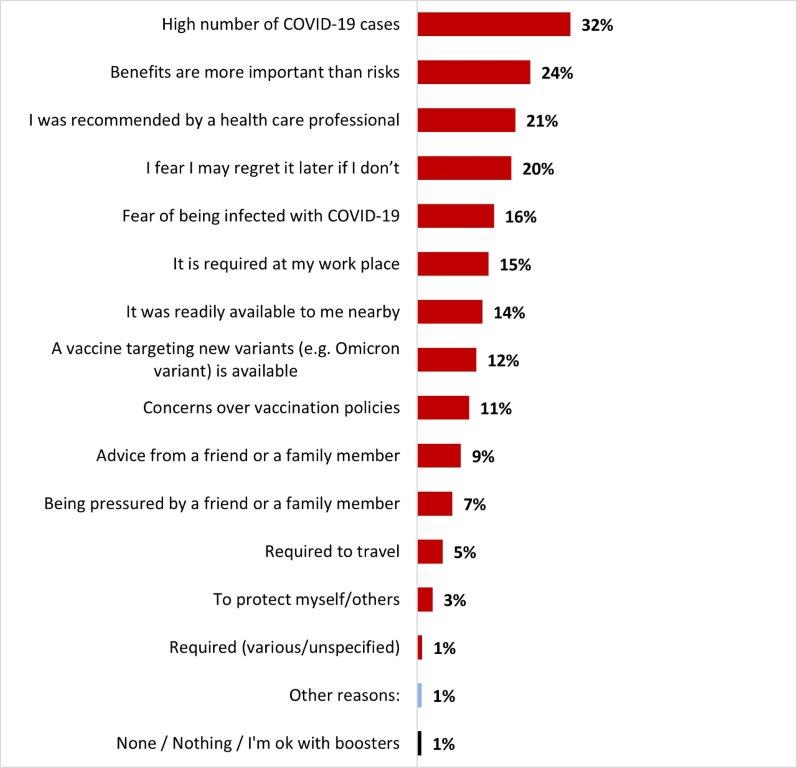
Figure 20.32: Text description
- High number of COVID-19 cases
- 32%
- Benefits are more important than risks
- 24%
- I was recommended by a health care professional
- 21%
- I fear I may regret it later if I don't
- 20%
- Fear of being infected with COVID-19
- 16%
- It is required at my work place
- 15%
- It was readily available to me nearby
- 14%
- A vaccine targeting new variants (e.g. Omicron variant) is available
- 12%
- Concerns over vaccination policies
- 11%
- Advice from a friend or a family member
- 9%
- Being pressured by a friend or a family member
- 7%
- Required to travel
- 5%
- To protect myself/others
- 3%
- Required (various/unspecified)
- 1%
- Other reasons:
- 1%
- None / Nothing / I'm ok with boosters
- 1%
Significant differences in terms of getting the booster dose despite an initial reluctance include:
- Women were more likely to say they feared they may regret it later if they did not get it (24%). Respondents from British Columbia and the Territories (36%) shared the same concern.
- 18–34-year-olds were more likely to state the booster was required at their workplace (24%).
- Those who were not parents of children younger than 18 years old were more likely to state the booster was readily available to them nearby (17%).
All respondents were asked if they would consider taking the COVID-19 vaccine as a routine vaccine annually. Almost six respondents out of ten (58%) indicated that they would be likely to take the COVID-19 vaccine as a routine vaccine: 36% very likely and 22% somewhat likely. In contrast, over one-third of respondents (35%) indicated it was unlikely: 14% not likely and 20%, not at all likely.
Figure 20.33: If COVID-19 vaccines were offered as a routine vaccine (e.g., annually), how likely would you be to get one?
Sample frame: All respondents (n=3,026)
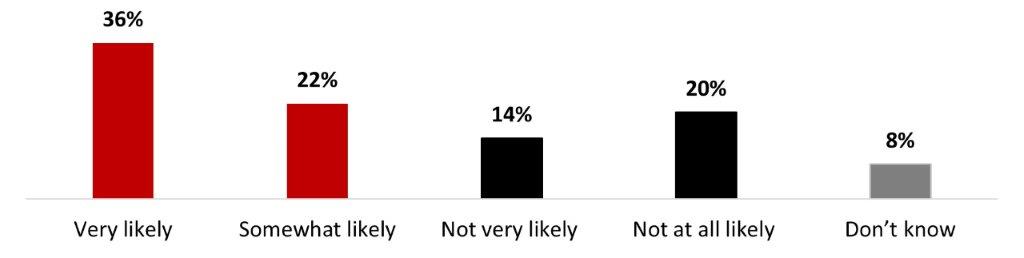
Figure 20.33: Text description
- Very likely
- 36%
- Somewhat likely
- 22%
- Not very likely
- 14%
- Not at all likely
- 20%
- Don't know
- 8%
Some subgroups were more likely to state it was very or somewhat likely that they get a COVID-19 vaccine as a routine vaccine, including:
- Male respondents (62%)
- Respondents over 55 years old (74%)
- Residents of British Columbia and the Territories (65%)
- Those who hold a university degree (68%)
- Respondents who are not parents of children younger than 18 years old (61%)
- Those who had not been infected with COVID-19 (60%)
Among respondents who were unsure or considered it unlikely that they would take the COVID-19 vaccine as a part of their annual vaccine routine, the main reasons given for their hesitation were concerns about long-term effects (16%), feeling that the vaccine does not provide much protection as you can still get infected (10%), belief that COVID-19 is not a sufficiently serious infection to require booster shots (8%), and being fed up with vaccination (8%). Around 7% of respondents mentioned thinking they are protected enough with their current number of vaccine doses, and that they were concerned about the safety of the vaccine. Other reasons were mentioned to a lesser extent.
Figure 20.34: What is the top reason you are unlikely or uncertain about getting a routine COVID-19 vaccine?
Sample frame: Those who are not likely or don't know if they would get a routine COVID-19 shot (n=1,288)
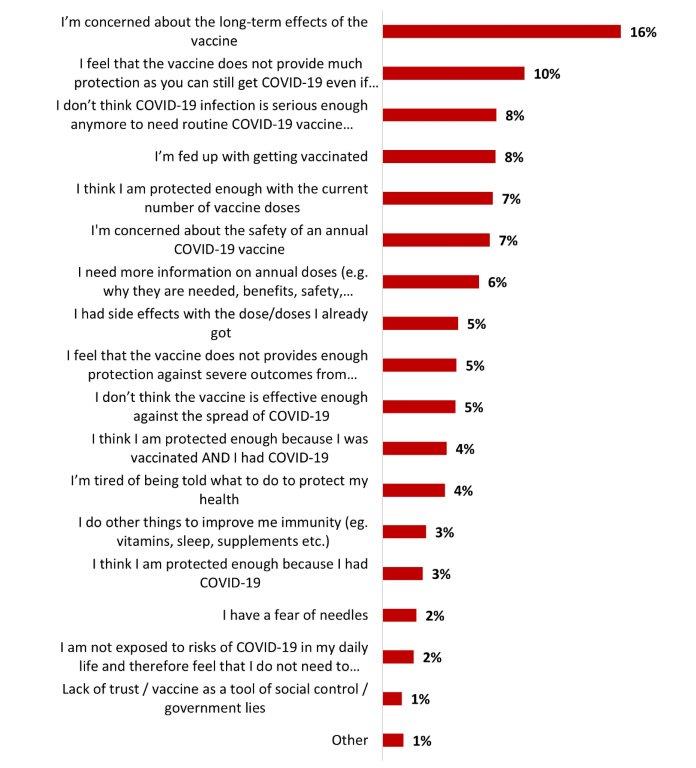
Figure 20.34: Text description
- I'm concerned about the long-term effects of the vaccine
- 16%
- I feel that the vaccine does not provide much protection as you can still get COVID-19 even if vaccinated
- 10%
- I don't think COVID-19 infection is serious enough anymore to need routine COVID-19 vaccine (e.g. annually)
- 8%
- I'm fed up with getting vaccinated
- 8%
- I think I am protected enough with the current number of vaccine doses
- 7%
- I'm concerned about the safety of an annual COVID-19 vaccine
- 7%
- I need more information on annual doses (e.g. why they are needed, benefits, safety, effectiveness, etc.)
- 6%
- I had side effects with the dose/doses I already got
- 5%
- I feel that the vaccine does not provides enough protection against severe outcomes from COVID-19
- 5%
- I don't think the vaccine is effective enough against the spread of COVID-19
- 5%
- I think I am protected enough because I was vaccinated AND I had COVID-19
- 4%
- I'm tired of being told what to do to protect my health
- 4%
- I do other things to improve me immunity (eg. vitamins, sleep, supplements etc.)
- 3%
- I think I am protected enough because I had COVID-19
- 3%
- I have a fear of needles
- 2%
- I am not exposed to risks of COVID-19 in my daily life and therefore feel that I do not need to receive a routine COVID-
- 2%
- Lack of trust / vaccine as a tool of social control / government lies
- 1%
- Other
- 1%
Significant differences include:
- Women (19%) were more likely to state that they are concerned about the long-term effects of the vaccine.
- Respondents from Quebec were more likely to think that the vaccine does not provide much protection as you can still catch COVID-19 (15%).
Around three respondents out of four stated it was either very (45%) or somewhat (29%) likely that they would get biyearly COVID-19 vaccines. A little over one person out of ten (12%) mentioned it was not very likely and 3% said it was not at all likely. One person out of ten did not provide an answer (10%).
Figure 20.35: And what about if the COVID vaccines were offered twice a year, how likely would you be to get them?
Sample frame: Respondents who are likely or unsure about getting routinely vaccinated against COVID-19 (n=1,948)
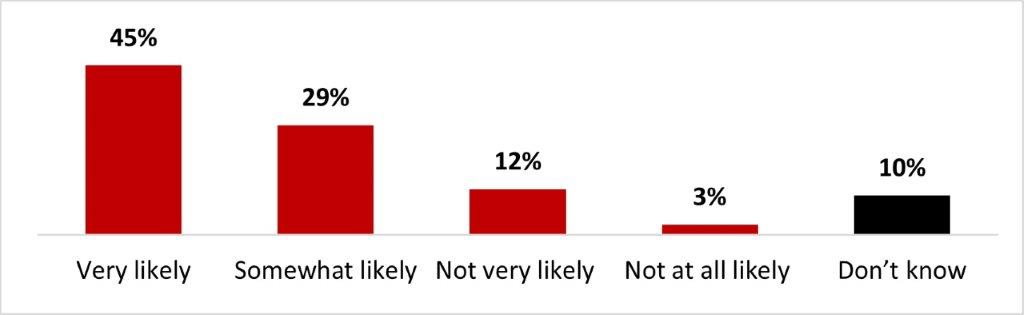
Figure 20.35: Text description
- Very likely
- 45%
- Somewhat likely
- 29%
- Not very likely
- 12%
- Not at all likely
- 3%
- Don't know
- 10%
The following subgroups were significantly more likely to get the COVID-19 vaccine if it were offered twice a year:
- Male respondents (78%)
- Respondents over 55 years old (84%)
- Respondents from the Atlantic region (84%)
- Respondents who have a university degree (79%)
- Those who are not parents of any children younger than 18 years old (77%)
The following subgroups were significantly less likely to get the COVID-19 vaccine if it were offered twice a year:
- Women (18%)
- 18 to 34-year-olds (22%)
- Parents of children younger than 18 years old (19%)
- Those who have been infected with COVID-19 (17%)
About half of the respondents were aware of the bivalent vaccine (47%), while over four out of ten were not (44%) and less than one out of ten (9%) were unsure.
Figure 20.36: Have you seen, read or heard anything about the bivalent COVID-19 vaccine?
Sample frame: All respondents (n=3,026)
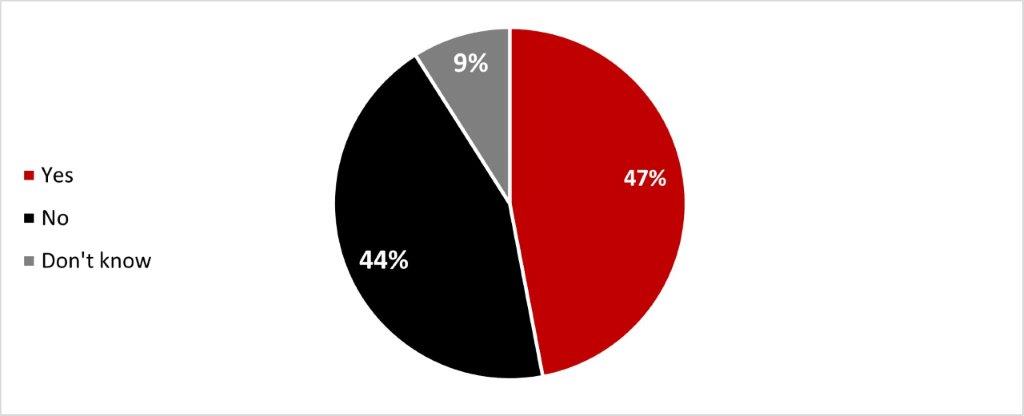
Figure 20.36: Text description
- Yes
- 47%
- No
- 44%
- Don't know
- 9%
The following subgroups were significantly more likely to be aware of the bivalent vaccine:
- Respondents over 55 years old (62%)
- Ontario residents (52%)
- Men (49%)
- White respondents (49%)
- Those who are not parents of any children younger than 18 years old (50%)
After being presented with explanation about the bivalent COVID-19 vaccine, almost three people out of ten were more likely to get it (28%), and over half (56%) have not changed their opinion: the same proportion of respondents have indicated they did or did not plan on getting it anyways (28%). Around 5% of respondents stated they were less likely to get a bivalent booster dose after reading about it.
Figure 20.37: The bivalent COVID-19 vaccine targets the original COVID-19 and the omicron variant, which helps provide further protection against omicron strains. Based on this explanation, are you more or less likely to get a COVID-19 bivalent booster dose?
Sample frame: All respondents (n=3,026)
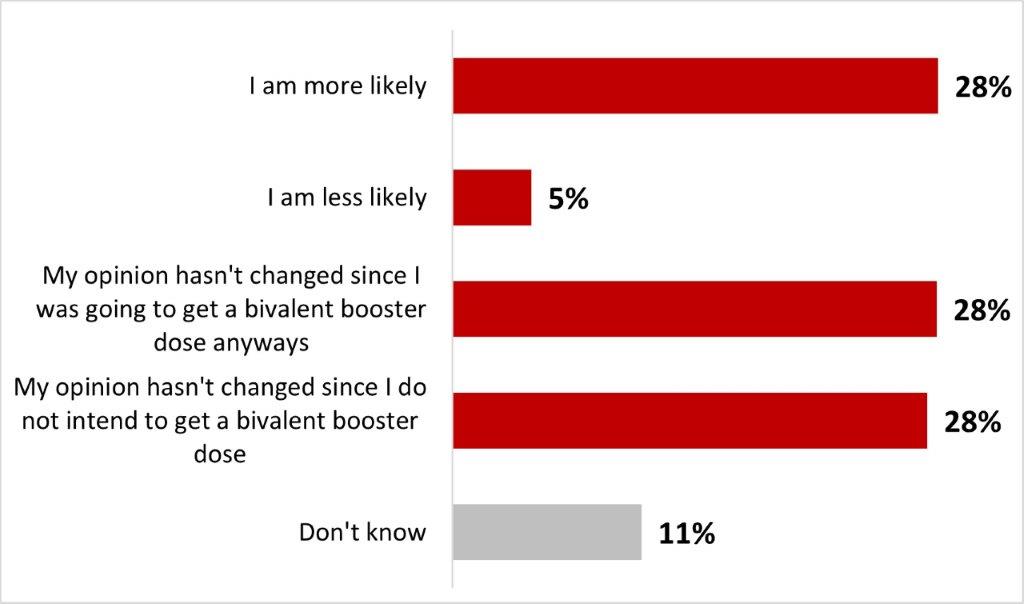
Figure 20.37: Text description
- I am more likely
- 28%
- I am less likely
- 5%
- My opinion hasn't changed since I was going to get a bivalent booster dose anyways
- 28%
- My opinion hasn't changed since I do not intend to get a bivalent booster dose
- 28%
- Don't know
- 11%
Significant differences among subgroups include:
- Respondents over 55 years old (36%) and men (32%) were significantly more likely to state they were more likely to get a COVID-19 bivalent booster dose after reading about it.
- Respondents from British Columbia and the Territories (34%), along with those over 55 years old (36%) were more likely to state their opinion hasn't changed since they were going to get a bivalent booster dose anyways.
- Black-identifying individuals (40%), parents of children younger than 18 years old (34%), and those who have been infected with COVID-19 (31%) were significantly more likely to state their opinion did not change since they did not intend to get a bivalent booster dose.
6.4 COVID-19 childhood vaccination
Among parents or legal guardians of children aged 12 to 17, 83% reported that their children (12-17) had been vaccinated with at least one dose. More specifically, 3% of these respondents indicated that their children had received one dose, 52% reported two doses, 21% reported three doses, and 8% reported four doses. More than one out of ten respondents (14%) indicated that their children had not received any doses yet: 2% were waiting to decide whether the child(ren) would be vaccinated, and 12% were determined not to have their children aged 12 to 17 vaccinated.
Figure 20.38: Thinking about your child(ren) aged 12-17, how many doses of a COVID-19 vaccine have they received?
Sample frame: Parents or guardians of at least one child 12-17 (n=355)
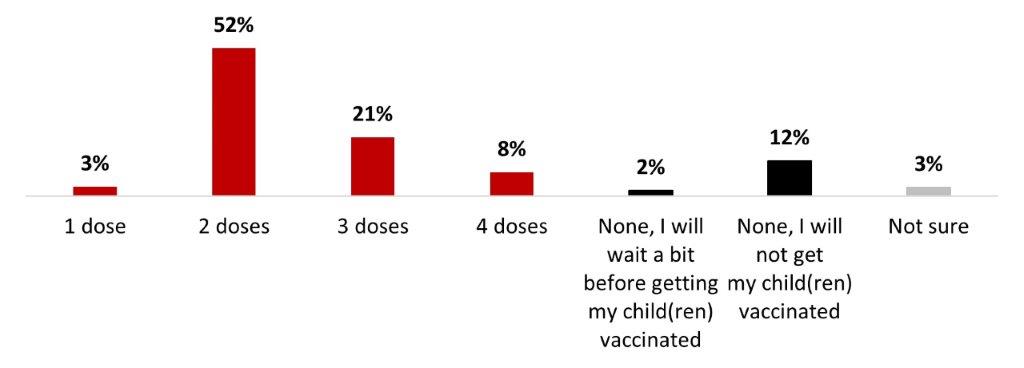
Figure 20.38: Text description
- 1 dose
- 3%
- 2 doses
- 52%
- 3 doses
- 21%
- 4 doses
- 8%
- None, I will wait a bit before getting my child(ren) vaccinated
- 2%
- None, I will not get my child(ren) vaccinated
- 12%
- Not sure
- 3%
Significant differences among subgroups include:
- Respondents from British Columbia were significantly more likely to say they will not vaccinate their child(ren) against COVID-19 (25%)
- Respondents from Quebec were more likely to have vaccinated them with two doses (64%)
- Parents who are vaccinated against COVID-19 (92%) were more likely to have vaccinated their children with at least one dose.
Among parents or legal guardians of children aged 12 to 17, the likelihood of getting booster doses for their child was 38%: 19% very likely and 19% somewhat likely. Half of these respondents (52%) reported that it was unlikely that they would seek out booster doses for their child(ren): 28% not very likely and 24% not at all likely.
Figure 20.39: Thinking about your child(ren) aged 12-17, how likely are you to have them receive a booster dose of the COVID-19 vaccine?
Sample frame: Parents or guardians of at least one child 12-17 who has received 1 or 2 doses (n=180)
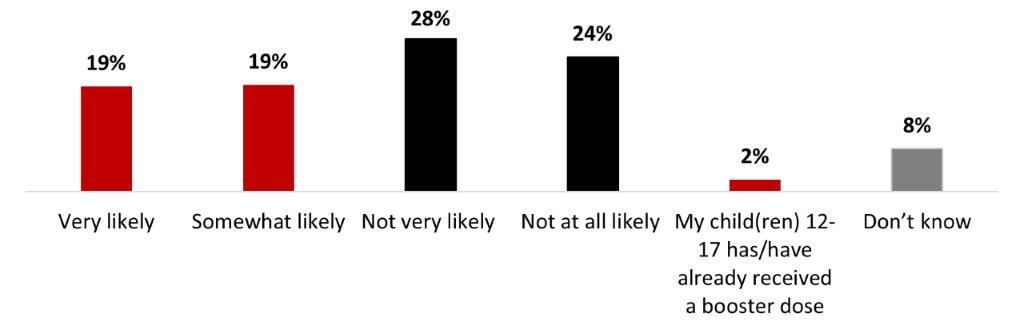
Figure20.39: Text description
- Very likely
- 19%
- Somewhat likely
- 19%
- Not very likely
- 28%
- Not at all likely
- 24%
- My child(ren) 12-17 has/have already received a booster dose
- 2%
- Don't know
- 8%
No relevant significant differences are to be noted.
Among parents or legal guardians of children aged 5 to 11 years, 61% indicated that their child(ren) had had at least one dose of the COVID-19 vaccine. More specifically, 12% reported one dose, 35% reported two doses, and 14% reported three doses. Over a third of those respondents (37%) indicated that their child(ren) had not received any doses yet: 10% indicated that they were waiting to decide, and 27% stated that their child(ren) would not be vaccinated.
Figure 20.40: Thinking about your child(ren) aged 5-11, how many doses of a COVID-19 vaccine have they received?
Sample frame: Parents or guardians of at least one child 5-11 (n=356)
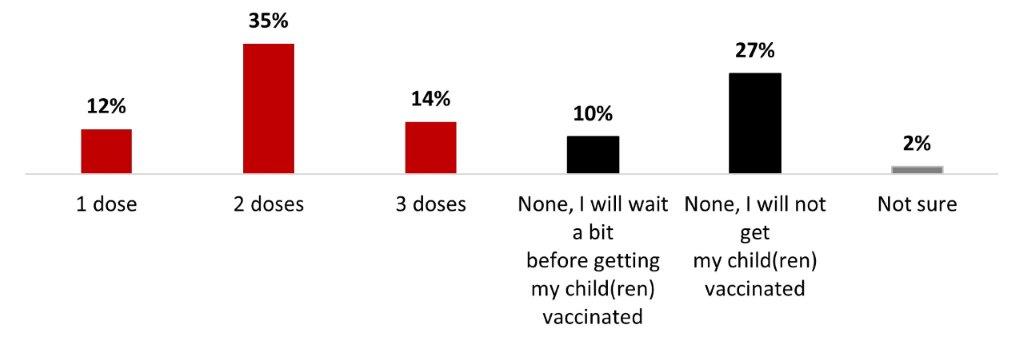
Figure 20.40: Text description
- 1 dose
- 12%
- 2 doses
- 35%
- 3 doses
- 14%
- None, I will wait a bit before getting my child(ren) vaccinated
- 10%
- None, I will not get my child(ren) vaccinated
- 27%
- Not sure
- 2%
18 to 34-year-old parents were significantly more likely to not get their children vaccinated (39%).
Among parents or legal guardians of children aged 5 to 11 who received at least one dose, over half of respondents (56%) reported that it was likely that their child(ren) would receive a booster dose: 27% very likely and 29% somewhat likely. In contrast, three out of ten respondents (31%) mentioned that it was unlikely that they would get booster doses for their child(ren): 14% unlikely and 17% not at all likely.
Figure 20.41: Thinking about your child(ren) aged 5-11, how likely are you to have them receive a booster dose of the COVID-19 vaccine?
Sample frame: Parents or guardians of at least one child 5-11 who has received 1 or 2 doses (n=161)
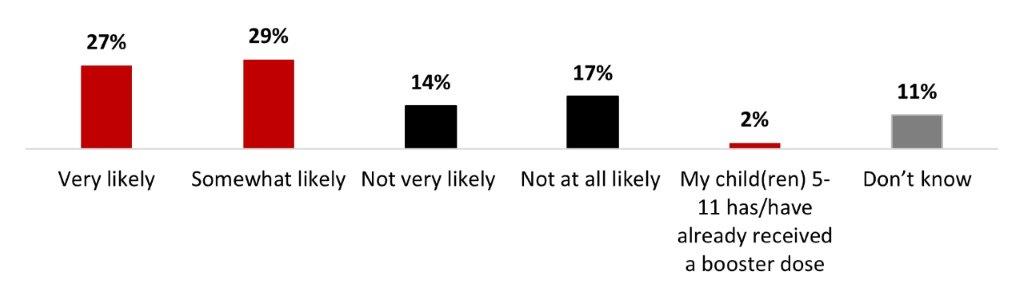
Figure 20.41: Text description
- Very likely
- 27%
- Somewhat likely
- 29%
- Not very likely
- 14%
- Not at all likely
- 17%
- My child(ren) 5-11 has/have already received a booster dose
- 2%
- Don't know
- 11%
No relevant significant differences are to be noted.
The main reasons that parents of children aged five to 17 were reluctant to pick up booster doses for their child(ren) were: concerns about long-term effects (26%), the child(ren) being anxious or fearful of vaccinations (16%), being concerned about the safety of the booster dose (13%), being fed up with getting their child(ren) vaccinated (12%) and not seeing the need to get a booster since their child(ren) has already been infected (12%). Other reasons were mentioned by less than one person out of ten.
Figure 20.42: Why are you not likely or not sure to have your child(ren) get a booster dose of a COVID-19 vaccine?
Sample frame: Those who are unlikely to or don't know if they will have their children 5-11 or 12-17 get a booster dose (n=155)
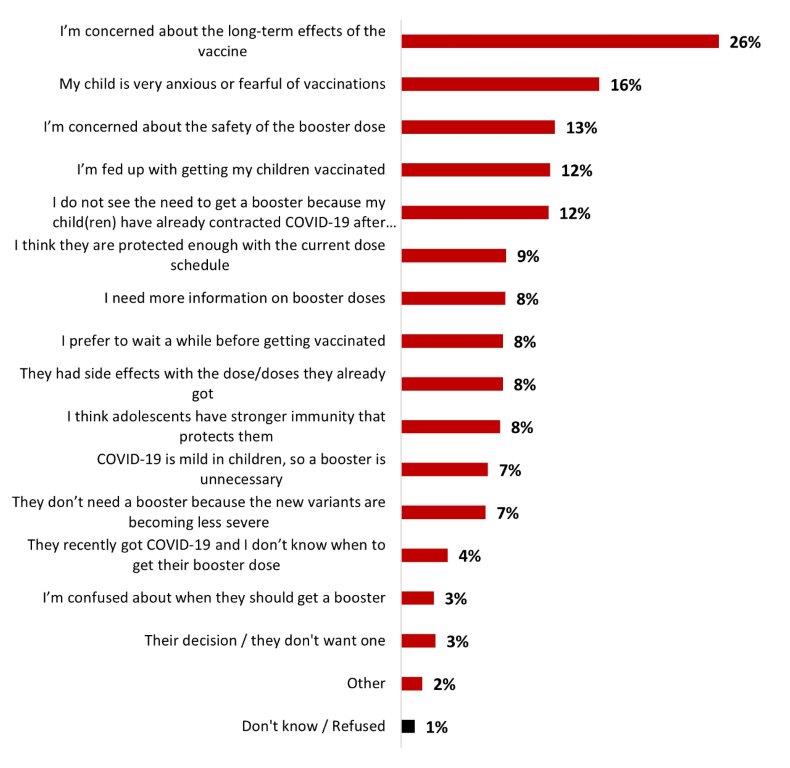
Figure 20.42: Text description
- I'm concerned about the long-term effects of the vaccine
- 26%
- My child is very anxious or fearful of vaccinations
- 16%
- I'm concerned about the safety of the booster dose
- 13%
- I'm fed up with getting my children vaccinated
- 12%
- I do not see the need to get a booster because my child(ren) have already contracted COVID-19 after being vaccinated
- 12%
- I think they are protected enough with the current dose schedule
- 9%
- I need more information on booster doses
- 8%
- I prefer to wait a while before getting vaccinated
- 8%
- They had side effects with the dose/doses they already got
- 8%
- I think adolescents have stronger immunity that protects them
- 8%
- COVID-19 is mild in children, so a booster is unnecessary
- 7%
- They don't need a booster because the new variants are becoming less severe
- 7%
- They recently got COVID-19 and I don't know when to get their booster dose
- 4%
- I'm confused about when they should get a booster
- 3%
- Their decision / they don't want one
- 3%
- Other
- 2%
- Don't know / Refused
- 1%
No relevant significant differences among subgroups are to be noted.
Among parents or guardians of children aged six months to five years, the rate of vaccination of their child(ren) in this age group was 23%. About four out of ten parents (40%) said they would wait to make a decision about vaccinating their child(ren), and one-third (34%) said they did not have any plans to have their child(ren) vaccinated.
Figure 20.43: Thinking about your child(ren) between the ages of 6 months and under 5, have they received at least one dose of a COVID-19 vaccine?
Sample frame: Parents or guardians of at least one child between 6 months and under 5 years old (n=302)
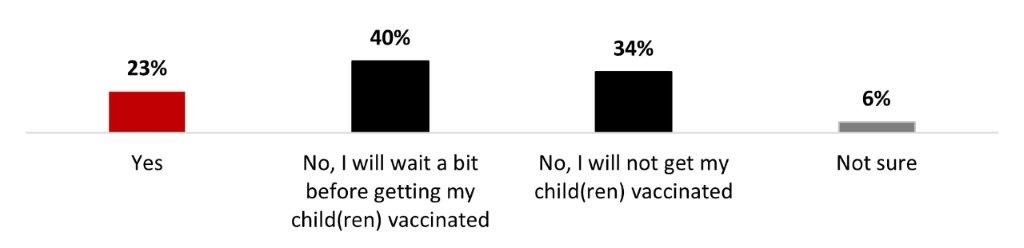
Figure 20.43: Text description
- Yes
- 23%
- No, I will wait a bit before getting my child(ren) vaccinated
- 40%
- No, I will not get my child(ren) vaccinated
- 34%
- Not sure
- 6%
Parents who have received at least one dose of the COVID-19 vaccine (26%) were more likely to have their children receive a dose of the COVID-19 vaccine.
Among parents or legal guardians of children aged six months to five years who do not intend to have their child(ren) vaccinated, the top three motivators to encourage vaccination were: having more information about children who have already received the vaccine (19%), having more information about the potential long-term effects of COVID-19 for children (17%), and if the vaccine was required for child(ren) to attend school (17%). It is important to note that over one-quarter of respondents (27%) mentioned that nothing would make them more likely to have their child(ren) vaccinated.
Figure 20.44: Which of the following factors would make you more likely to vaccinate your child(ren) against COVID-19? Up to 3 answers.
Sample frame: Parents or guardians of children 6 months and under 5 who will not get their child vaccinated will wait a bit, or are not sure (n=245)
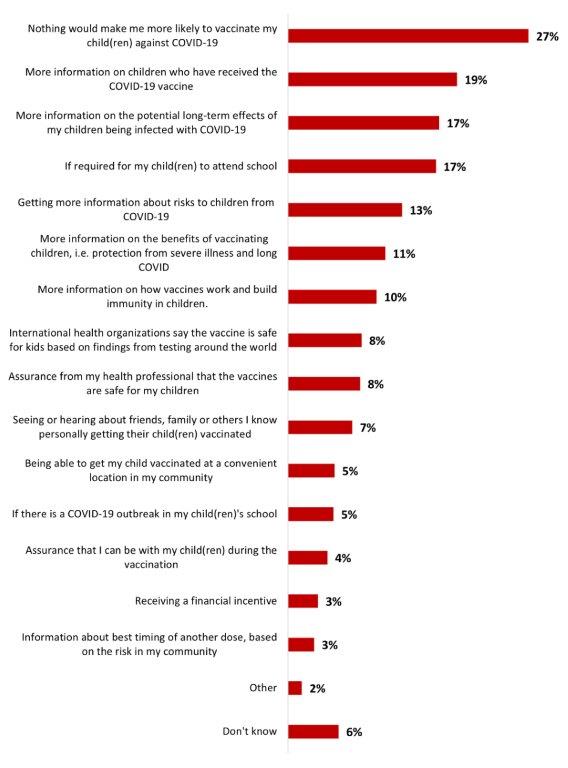
Figure 20.44: Text description
- Nothing would make me more likely to vaccinate my child(ren) against COVID-19
- 27%
- More information on children who have received the COVID-19 vaccine
- 19%
- More information on the potential long-term effects of my children being infected with COVID-19
- 17%
- If required for my child(ren) to attend school
- 17%
- Getting more information about risks to children from COVID-19
- 13%
- More information on the benefits of vaccinating children, i.e. protection from severe illness and long COVID
- 11%
- More information on how vaccines work and build immunity in children.
- 10%
- International health organizations say the vaccine is safe for kids based on findings from testing around the world
- 8%
- Assurance from my health professional that the vaccines are safe for my children
- 8%
- Seeing or hearing about friends, family or others I know personally getting their child(ren) vaccinated
- 7%
- Being able to get my child vaccinated at a convenient location in my community
- 5%
- If there is a COVID-19 outbreak in my child(ren)'s school
- 5%
- Assurance that I can be with my child(ren) during the vaccination
- 4%
- Receiving a financial incentive
- 3%
- Information about best timing of another dose, based on the risk in my community
- 3%
- Other
- 2%
- Don't know
- 6%
Significant differences among subgroups include:
- Women were more likely to mention needing more information on the potential long-term effects of COVID-19 infection on children (22%).
- Parents who were not vaccinated (79%) with at least one dose of the COVID-19 vaccine were more likely to mention that nothing would make them more likely to vaccinate their children.
Parents were presented on information about the bivalent COVID-19 vaccine and were asked whether this information had an impact on their likelihood to get their child(ren) vaccinated. Around one parent out of four (25%) stated they were more likely to have their child(ren) get a COVID-19 bivalent booster dose after reading the explanation about it, while over half (55%) stated their opinion has not changed: one out of five were planning to get a bivalent booster dose anyways (21%) and one-third were not intending to anyways (34%). Less than one out of ten (7%) were less likely to vaccinate their children after reading about the bivalent vaccines.
Figure 20.45: The bivalent COVID-19 vaccine targets the original COVID-19 virus strain and the omicron variant, which helps provide further protection against omicron strains. Based on this explanation, are you more or less likely to have your child(ren) get a COVID-19 bivalent booster dose?
Sample frame: Respondents who have children under 18 (n=845)
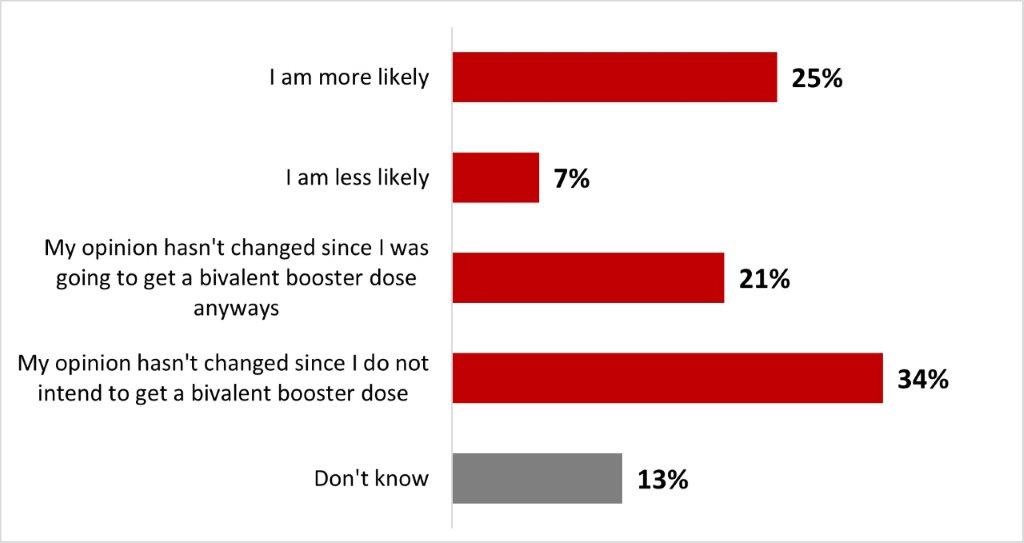
Figure 20.45: Text description
- I am more likely
- 25%
- I am less likely
- 7%
- My opinion hasn't changed since I was going to get a bivalent booster dose anyways
- 21%
- My opinion hasn't changed since I do not intend to get a bivalent booster dose
- 34%
- Don't know
- 13%
Significant differences among subgroups include:
- Parents over 55 years old (56%) and vaccinated parents of children under 18 (28%) were more likely to state they were more likely to have their child(ren) get a COVID-19 bivalent booster dose.
- Unvaccinated parents of children under 18 were more likely to state their opinion hasn't changed since they do not intend to get a bivalent booster dose (83%).
6.5 Confidence in vaccination
The COVID-19 pandemic did not have a positive or negative impact on vaccine confidence for half of the respondents. Indeed, 51% of respondents stated that their confidence level was about the same as before the pandemic. Around one in five respondents (19%) indicated that they were now more confident (10% a lot more and 10% somewhat more confident), while almost one-fourth (23%) of respondents indicated that they were now less confident (12% a lot less and 11% somewhat less confident) about vaccination in general.
Figure 20.46: Has the recent COVID-19 pandemic had an impact on your confidence in vaccinations in general?
Sample frame: All respondents (n=3,026)
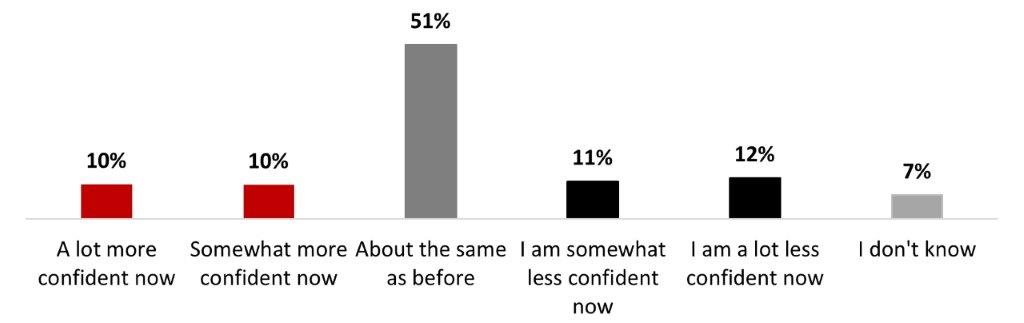
Figure 20.46: Text description
- A lot more confident now
- 10%
- Somewhat more confident now
- 10%
- About the same as before
- 51%
- I am somewhat less confident now
- 11%
- I am a lot less confident now
- 12%
- I don't know
- 7%
The following subgroups were significantly more likely to state they were somewhat or a lot less confident in vaccinations now:
- Parents of children younger than 18 years old (29%)
- Black-identifying individuals (28%)
- 18 to 34-year-olds (27%) and 35 to 54-year-olds (27%),
- Those who have never been infected with COVID-19 (26%)
The main reasons mentioned by respondents who experienced a decrease in their level of confidence in vaccines were that the COVID-19 vaccines have had a detrimental impact on their perception of vaccines in general (43%), that they were now more concerned about the safety of vaccines in general (41%), and the perception that the COVID-19 pandemic has shown that vaccines do not work well (30%). Around one-fourth of respondents mentioned they now believe that vaccines in general do not have as much benefit in stopping the spread of viruses (26%) and that they do not have as much benefit in preventing severe outcomes (25%). One person out of five mentioned that the changing recommendations in vaccine schedules impacted their views on vaccines (21%). Every other reason was mentioned by less than a fifth of respondents.
Figure 20.47: Why are you less confident in vaccinations? Select all that apply.
Sample frame: Those who are less confident in vaccines now than before the pandemic (n=692)
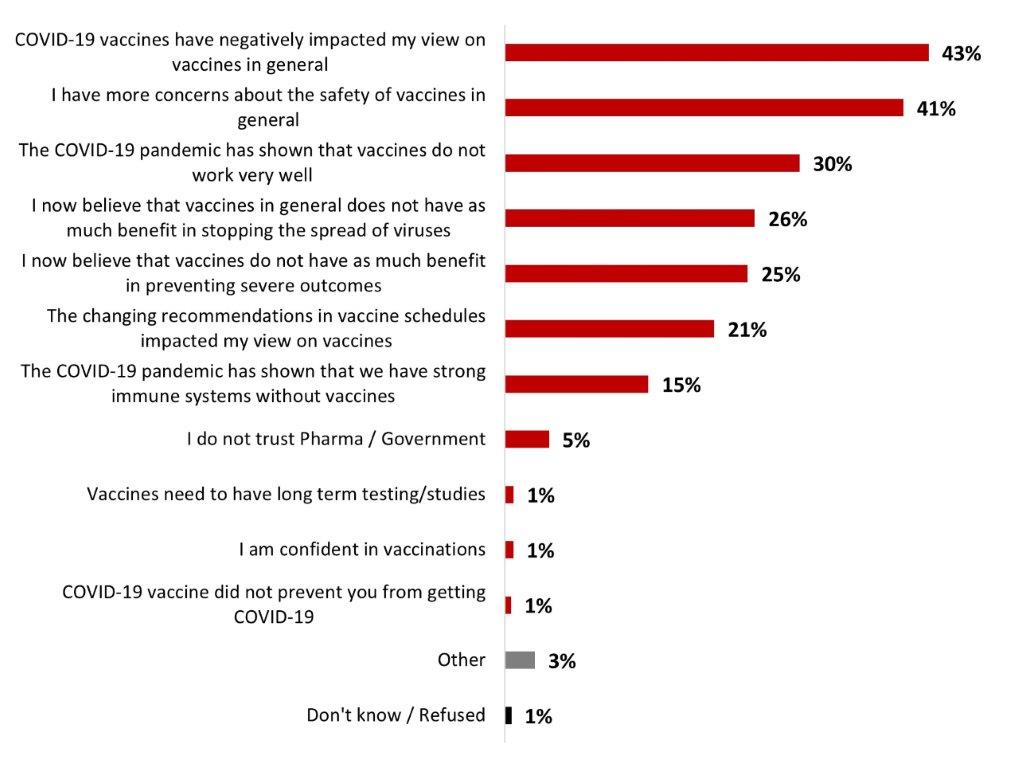
Figure 20.47: Text description
- COVID-19 vaccines have negatively impacted my view on vaccines in general
- 43%
- I have more concerns about the safety of vaccines in general
- 41%
- The COVID-19 pandemic has shown that vaccines do not work very well
- 30%
- I now believe that vaccines in general does not have as much benefit in stopping the spread of viruses
- 26%
- I now believe that vaccines do not have as much benefit in preventing severe outcomes
- 25%
- The changing recommendations in vaccine schedules impacted my view on vaccines
- 21%
- The COVID-19 pandemic has shown that we have strong immune systems without vaccines
- 15%
- I do not trust Pharma / Government
- 5%
- Vaccines need to have long term testing/studies
- 1%
- I am confident in vaccinations
- 1%
- COVID-19 vaccine did not prevent you from getting COVID-19
- 1%
- Other
- 3%
- Don't know / Refused
- 1%
Significant differences include:
- Respondents from Ontario were more likely to have concerns about the safety of vaccines in general (48%).
- Respondents from Manitoba and Saskatchewan were significantly more likely to now believe that vaccines in general do not have as much benefit in stopping the spread of viruses (44%).
- Those who have never been infected with COVID-19 were more likely to state they now believes that vaccines in general do not have as much benefit in stopping the spread of viruses (31%).
6.6 Public health measures
Staying home and away from others when sick (79%), wearing a mask inside with others when feeling sick (57%), and using individual public health measures when interacting with someone at risk (56%) were the three most regularly adopted individual protection measures. Other measures like wearing a mask indoors in a public space (44%), improving ventilation when people from outside the immediate household are in the home (37%), and wearing a mask outside (24%) were practiced always or often by less than half of respondents.
Table 20.48: How often do you follow each of the following individual public health measures?
Sample frame: All respondents (n=3,026)
NET always + often
- Staying home and away from others if you feel sick
- 79%
- Wearing a mask – inside with others when you're feeling sick
- 57%
- Using individual public health measures when interacting with someone who is at risk of more severe disease or outcomes from COVID-19
- 56%
- Wearing a mask–when indoors in a public space or in an indoor space with people from outside your immediate household
- 44%
- Improving ventilation when people from outside your immediate household are in your home
- 37%
- Wearing a mask– when outside in a public space
- 24%
Significant differences in terms of following individual public health measures include:
- Respondents over 55 years old were significantly more likely to follow all but one of the individual public health measures (improving ventilation when people from outside the immediate household are in the house)
- Black-identifying individuals were significantly more likely to follow all but two of the individual public health measures (staying home and away from others when feeling sick and using IPHM when interacting with someone more at-risk), while white individuals were significantly less likely to follow all but one of the IPHM (staying home and away from others when feeling sick).
Over two respondents out of five (44%) agree either strongly (19%) or somewhat (25%) with reinstating mandatory public health measures. One out of five people neither agreed nor disagreed (20%). On the other hand, a third of respondents disagreed either somewhat (11%) or strongly (22%).
Figure 20.49: To what extent would you agree or disagree with reinstating mandatory public health measures (e.g., policies on masking, or capacity limits)?
Sample frame: All respondents (n=3,026)
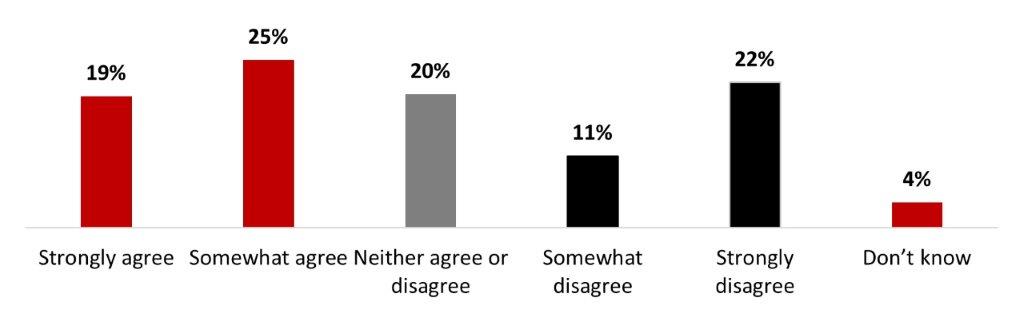
Figure 20.49: Text description
- Strongly agree
- 19%
- Somewhat agree
- 25%
- Neither agree or disagree
- 20%
- Somewhat disagree
- 11%
- Strongly disagree
- 22%
- Don't know
- 4%
A rising number of COVID-19 related hospitalizations (48%), a local outbreak of COVID-19 cases (43%), and a rising number of deaths related to COVID-19 (42%) were the three main conditions respondents mentioned in order for them to support reinstating mandatory public health measures. They were followed by if the healthcare capacities become overloaded (40%), if the spread of COVID-19 is increasing (39%), and if there are new COVID-19 variants of concern (34%). One out of five respondents mentioned they would support reinstating public health measures if there are other respiratory viruses in circulation (20%), and one-fourth are not supportive at all to reinstate the mandatory PHMs (25%).
Figure 20.50: Under what conditions would you support reinstating mandatory public health measures (e.g. policies on masking, or capacity limits)?
Sample frame: All respondents (n=3,026)
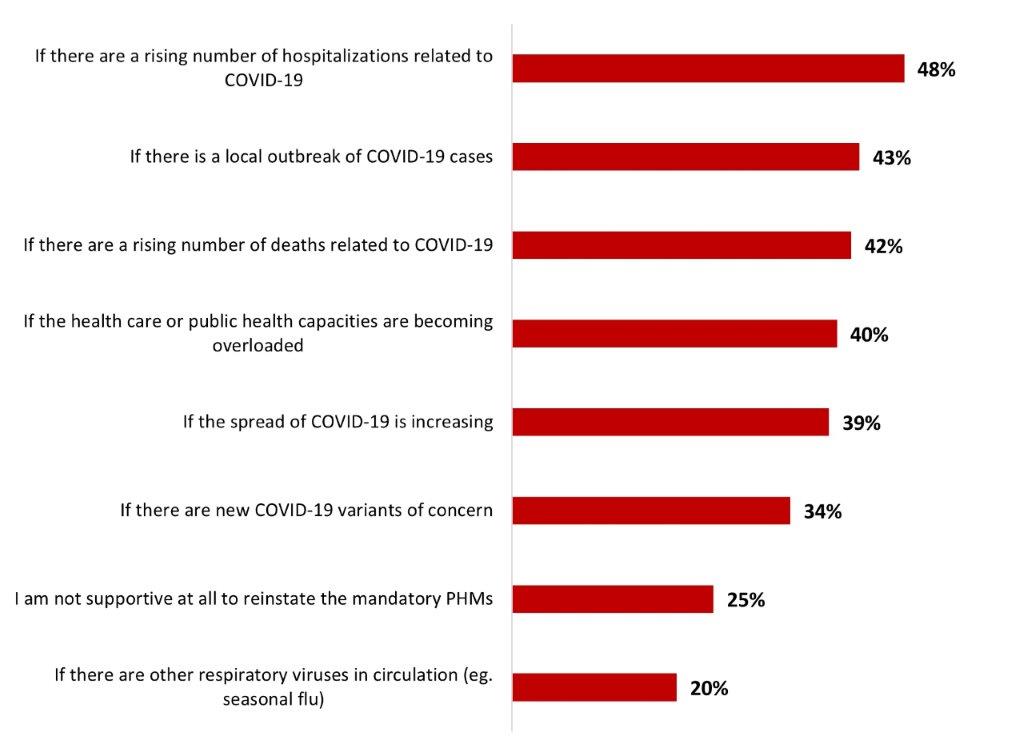
Figure 20.50: Text description
- If there are a rising number of hospitalizations related to COVID-19
- 48%
- If there is a local outbreak of COVID-19 cases
- 43%
- If there are a rising number of deaths related to COVID-19
- 42%
- If the health care or public health capacities are becoming overloaded
- 40%
- If the spread of COVID-19 is increasing
- 39%
- If there are new COVID-19 variants of concern
- 34%
- I am not supportive at all to reinstate the mandatory PHMs
- 25%
- If there are other respiratory viruses in circulation (eg. seasonal flu)
- 20%
The following subgroups were significantly more likely to mention almost all conditions:
- Respondents over 55 years old
- At-risk respondents
- Those who are not parents of any children younger than 18 years old
- Those who had not been infected with COVID-19
6.7 Long-COVID
Around two-thirds of respondents mentioned being familiar with long-COVID (63%): around one out of ten stated being very familiar (12%), and around half were somewhat familiar (51%). On the other hand, one out of four was not very familiar (24%), and around 8% were not at all familiar.
Figure 20.51: How familiar are you with the potential long-term effects of having COVID-19 (also known as "long-COVID" or "post COVID-19 condition")?
Sample frame: All respondents (n=3,026)
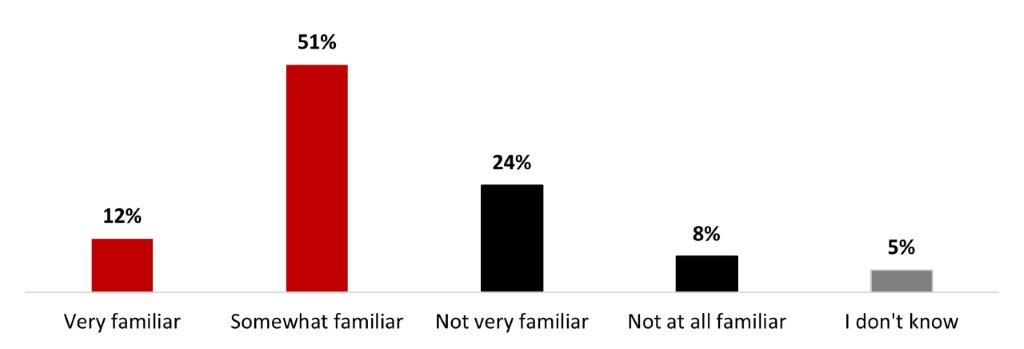
Figure 20.51: Text description
- Very familiar
- 12%
- Somewhat familiar
- 51%
- Not very familiar
- 24%
- Not at all familiar
- 8%
- I don't know
- 5%
The following subgroups were significantly more likely to state being very or somewhat familiar with long-COVID:
- Those with a university degree (70%)
- British Columbia and Territories residents (69%)
- Those who earn over $80,000 (68%)
- Parents of children younger than 18 years old (68%)
- Those who have been infected with COVID-19 (66%)
- White individuals (64%)
Overall, more than half (56%) mentioned being worried about developing long-term symptoms from a COVID-19 infection. More specifically, fewer than one out of five people stated being very worried (17%), while over a third were somewhat worried (38%). Around three out of ten respondents were not very worried (25%), and 14% were not at all worried.
Figure 20.52: How worried are you/would you be about developing longer-term symptoms from a COVID-19 infection?
Sample frame: All respondents (n=3,026)
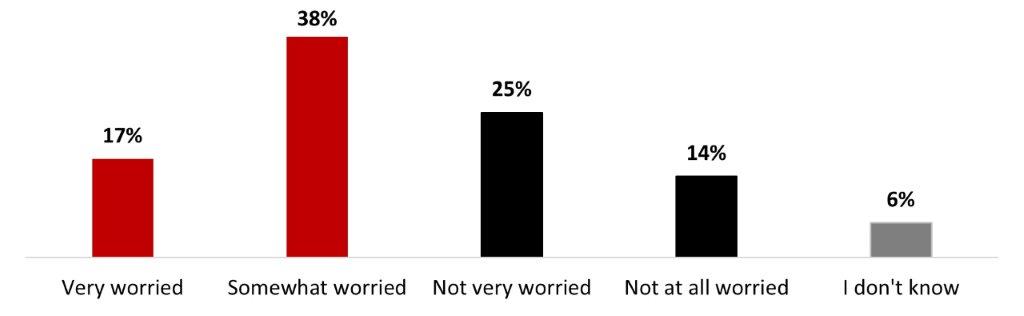
Figure 20.52: Text description
- Very worried
- 17%
- Somewhat worried
- 38%
- Not very worried
- 25%
- Not at all worried
- 14%
- I don't know
- 6%
Uncertainty about future health prospects and limitations to leisure/personal life were the two main reasons for worrying about long-COVID for around two-thirds of respondents (66% and 65%, respectively), way ahead of other reasons. Over one-third of respondents were worried about limitations to their working life (39%) and three out of ten worried because of a lack of information/resources on the condition (29%). Over one person out of four was worried about difficulty in accessing benefits related to the condition (23%) lack of public acknowledgement from authority figures (22%), and not knowing if others would take their condition seriously (21%). Around one person out of ten or more were worried about difficulty in formally indicating their condition to employers, healthcare providers and others (15%), about being terminated or judged because of their condition (10%).
Figure 20.53: What makes/would make you feel worried about long-term symptoms of COVID? Select all that apply.
Sample frame: Those who are worried about developing longer-term symptoms from COVID-19 (n=1,670)
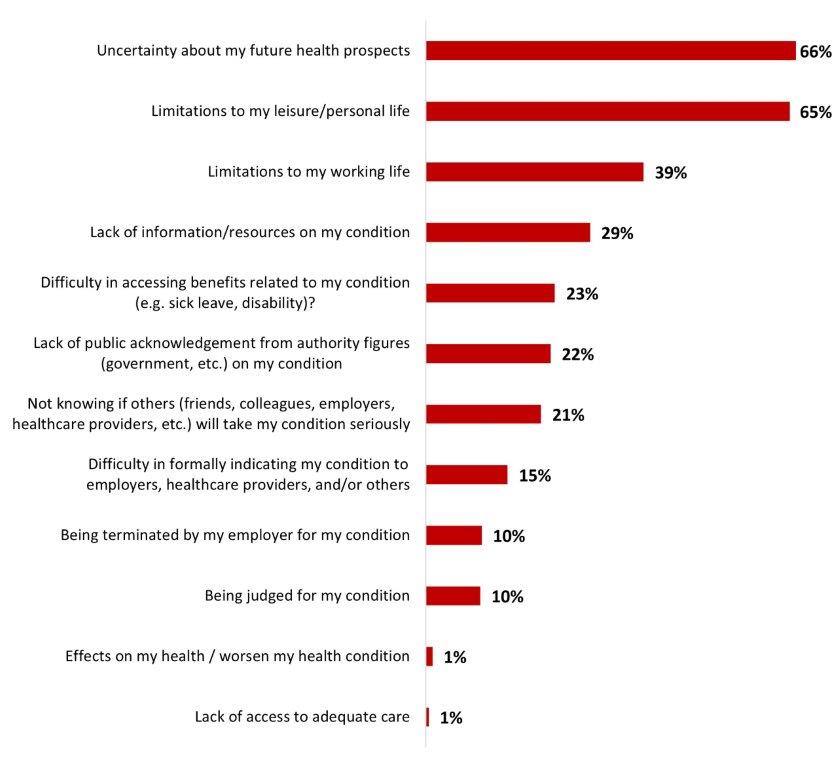
Figure 20.53: Text description
- Uncertainty about my future health prospects
- 66%
- Limitations to my leisure/personal life
- 65%
- Limitations to my working life
- 39%
- Lack of information/resources on my condition
- 29%
- Difficulty in accessing benefits related to my condition (e.g. sick leave, disability)?
- 23%
- Lack of public acknowledgement from authority figures (government, etc.) on my condition
- 22%
- Not knowing if others (friends, colleagues, employers, healthcare providers, etc.) will take my condition seriously
- 21%
- Difficulty in formally indicating my condition to employers, healthcare providers, and/or others
- 15%
- Being terminated by my employer for my condition
- 10%
- Being judged for my condition
- 10%
- Effects on my health / worsen my health condition
- 1%
- Lack of access to adequate care
- 1%
The following subgroups were significantly more likely to feel uncertain about their future health prospects if they got long COVID:
- Residents of the Atlantic region (75%)
- Respondents over 55 years old (73%)
- Women (71%)
- Respondents who are not parents of any children younger than 18 years old (69%)
The following subgroups were significantly more likely to worry about limitations to their leisure/personal life:
- Respondents who identify as 2SLGBTQIA+ (82%)
- Respondents from Quebec (70%)
- Respondents who earn over $80,000 (70%)
- White individuals (69%)
7. Trends across the waves
Over the course of the different waves, certain trends became apparent and certain changes that were observable in the quantitative phases were also confirmed in the focus groups.
In the last wave, for the first time, the number of Canadians who said they have been infected with COVID-19 has surpassed the number of Canadians who have never been infected. Almost half of respondents have now been infected with COVID-19 (47%), while around four out of ten were not (41%).
In terms of keeping up to date with their COVID-19 vaccination, there was a decrease in the interest of Canadians to receive all the booster doses available to them. In fact, there has been a decrease in the number of Canadians who say they are likely to stay up to date (71% in wave 16 to 61% in wave 20) and a decrease in the number of respondents who say they have received a booster dose in the last three months (42% to 27% from wave 18 to 20).
In addition, there has been a decreased of Canadians saying they are likely to take the COVID-19 vaccine as a routine shot (64% to 58% from wave 16 to 20) or to take the shot twice a year (78% to 75% from wave 18 to 20). This reflects some of what was heard in the focus groups. Some participants mentioned being fed up with being vaccinated and feeling that they are adequately protected with the doses they have already received. Some did not see the need to be vaccinated several times a year, since they could still get COVID-19.
This same trend can also be observed for the vaccination of children aged 12 to 17 years. There is a strong decrease in the number of parents who say their children are likely to receive a booster dose (57% to 38% from wave 16 to 20).
When it comes to mental health, there has been a decrease in the number of Canadians who report feeling like they have adequate access to mental health support services (52% to 47% from wave 18 to 20) and a decrease of Canadians who report being able to afford to see a mental health therapist (55% to 41% from wave 18 to 20), as well as a decrease in the number of Canadians who stated they were aware of free mental health and substance use resources online or by phone (60% to 52% between from wave 18 to 20). These tracked changes were corroborated by the qualitative findings of the focus groups, as cost and availability of mental health care services were the main barriers mentioned by participants.
Appendix A: Detailed Research Methodology.
A.16.1 Methods for Wave 16
Quantitative research was conducted through online surveys using Computer Aided Web Interviewing (CAWI) technology. As a CRIC Member, Leger adheres to the most stringent guidelines for quantitative research. The survey was conducted in accordance with the Government of Canada requirements for quantitative research, including the Standards of the Conduct of Government of Canada Public Opinion Research—Series D—Quantitative Research. Respondents were assured of the voluntary, confidential and anonymous nature of this research. As with all research conducted by Leger, all information that could allow for the identification of participants was removed from the data in accordance with the Privacy Act.
A.16.2 Sampling Procedures for Wave 16
Computer Aided Web Interviewing (CAWI)
Leger conducted a panel-based Internet survey with a sample of adult Canadians. A total of 3,004 respondents participated in the survey, including oversamples of 400 Black-identifying individuals and 200 Indigenous-identifying individuals. The exact distribution is presented in the following section. Participant selection was done randomly from Leo's online panel.
Leger owns and operates an Internet panel of more than 400,000 Canadians from coast to coast. An Internet panel is made up of Web users profiled on different sociodemographic variables. The majority of Leger's panel members (61%) have been recruited randomly over the phone over the past decade, making it highly similar to the actual Canadian population on many demographic characteristics.
Since an Internet sample is non-probabilistic in nature, the margin of error does not apply.
A.16.3 Data Collection for Wave 16
Fieldwork for the survey was conducted from September 8 to 29, 2022. The participation rate for the survey was 12.41%. A pre-test of 43 interviews was completed on September 8, 2022. More specifically, 27 interviews were conducted in English and 16 were conducted in French. Survey interviews lasted 10 minutes on average.
To achieve data reliability in all subgroups, a total sample of 3,004 Canadians were surveyed in all regions of the country. The overall sample also included oversamples of 400 Black-identifying and 200 Indigenous-identifying individuals.
| Region | Number of respondents |
|---|---|
| Ontario | 1,127 |
| Quebec | 761 |
| British Columbia and Territories | 360 |
| Alberta | 341 |
| Prairies | 219 |
| Atlantic Region | 196 |
| Total | 3,004 |
Since a sample drawn from an Internet panel is not probabilistic in nature, the margin of error cannot be calculated for this survey. Respondents for this survey were selected from those who volunteered to participate/registered to participate in online surveys. The results of such surveys cannot be described as statistically projectable to the target population. The data have been weighted to reflect the demographic composition of the target population. Because the sample is based on those who initially self-selected for participation, no estimates of sampling error can be calculated.
Based on the most recent data from Statistics Canada's national census, Leger weighted the results of this survey by age, gender, region, first language (mother tongue), education level, presence of children in the household, place of birth, and ethnicity. The most recent data regarding age, gender, region and first language was from the 2021 census. The data for education level, presence of children in the household, place of birth and ethnicity came from the 2016 census.
A.16.4 Participation Rate for the Web Survey for Wave 16
The overall participation rate for this study is 12.4%.
Below is the calculation of the Web survey's participation rate. The participation rate is calculated by dividing the number of completed questionnaires by the number of invitations sent. The typical participation rates for Web-surveys are between 20% and 30%. A response rate of 12.4% may seem a bit low but given the limited amount of time for fieldwork and the specific oversamples of Black-identifying and Indigenous-identifying individuals, invitations had to be spread more widely in the panel to achieve the objectives, which has an impact on the participation rate.
| Total email addresses used | |
|---|---|
| Invalid cases | 263 |
| -invitations mistakenly sent to people who did not qualify for the study | 120 |
| -incomplete or missing email addresses | 143 |
| Unresolved (U) | 20,924 |
| -email invitations bounce back | 29 |
| -email invitations unanswered | 20,895 |
| In-scope non-responding units (IS) | 272 |
| -respondent refusals | 272 |
| -language problem | NA |
| -early breakoffs | NA |
| Responding units (R) | 3,004 |
| -completed surveys disqualified—quota filled | 295 |
| -completed surveys disqualified for other reasons | 120 |
| -completed surveys | 3,004 |
| Participation rate/response rate = R ÷ (U + IS + R) | 12.41% |
A.16.5 Additional Socio-Demographic Analysis
A basic comparison of the unweighted and weighted sample sizes was conducted to identify any potential non-response bias that could be introduced by lower response rates among specific demographic subgroups (see tables below).
A.16.6 Unweighted and Weighted Samples for Wave 16
The table below presents the geographic distribution of respondents before and after weighting. There were almost no imbalances in geographical distribution in the unweighted sample. The weighting process has mainly adjusted some minor discrepancies.
| Province/Territory | Unweighted | Weighted |
|---|---|---|
| Ontario | 1,127 | 1,166 |
| Quebec | 761 | 687 |
| British Columbia and Territories | 360 | 419 |
| Alberta | 341 | 335 |
| Prairies | 219 | 194 |
| Atlantics | 196 | 203 |
The following tables present the demographic distribution of respondents according to gender, age group, first language and education. First, regarding gender, we can see that weighting has adjusted slightly the proportion of males and females. Female respondents were a little bit overrepresented in this survey. The weight of the men was therefore boosted so as not to underestimate their actual weight in the results.
| Gender | Unweighted | Weighted |
|---|---|---|
| Male | 1,377 | 1,461 |
| Female | 1,617 | 1,535 |
Regarding age distribution, the weighting process has corrected some minor discrepancies.
| Age | Unweighted | Weighted |
|---|---|---|
| Between 18 and 34 | 865 | 803 |
| Between 35 and 55 | 1,073 | 969 |
| 55 years old and over | 1,066 | 1,231 |
Minor imbalances with language distribution were corrected with weighting, as presented below.
| Language (Mother tongue) | Unweighted | Weighted |
|---|---|---|
| English | 1,987 | 2,060 |
| French | 743 | 594 |
| Other | 262 | 333 |
The table below presents the distribution based on education. The weighting corrected every gap between the actual distribution in the population and the final sample.
| Education | Unweighted | Weighted |
|---|---|---|
| Elementary/High school | 668 | 903 |
| College | 908 | 1,234 |
| University | 1,407 | 834 |
The following two tables present the distribution based on the presence of children in the household and place of birth. Again, imbalances were minor and corrected by weighting.
| Presence of children in the household | Unweighted | Weighted |
|---|---|---|
| Yes | 830 | 820 |
| No | 2,163 | 2,171 |
| Place of birth | Unweighted | Weighted |
|---|---|---|
| Canada | 2,372 | 2,353 |
| Other | 617 | 630 |
The last table presents the distribution based on ethnicity. Weighting boosted the weight of white individuals and reduced that of Indigenous-identifying and Black-identifying respondents to closely follow the actual distribution in the population.
| Ethnicity | Unweighted | Weighted |
|---|---|---|
| White | 2,067 | 2,364 |
| Indigenous | 248 | 145 |
| Black | 435 | 108 |
| South Asian | 78 | 100 |
| Chinese | 144 | 167 |
| Other | 177 | 219 |
There is no evidence from the data that having achieved a different age or gender distribution prior to weighting would have significantly changed the results of this study. The relatively small weight factors (see the section below) and differences in responses between various subgroups suggest that data quality was not affected. The weight that was applied corrected the initial imbalance for data analysis purposes, and no further manipulations were necessary.
As with all research conducted by Leger, the contact information was kept entirely confidential and all information that could allow for the identification of participants was removed from the data in accordance with Canada's Privacy Act.
Note on testing for statistical differences
According to the normal distribution, a two-tailed test is always done between two proportions and based on the unweighted total columns. The test is performed by comparing a percentage with the percentage formed by the complement of the relevant category (e.g., of the male subgroup is the female subgroup; the complement of the 18–24 age subgroup is the 25+ age subgroup, and the complement of the college-educated subgroup is the sub-group consisting of respondents with elementary, high school or university education). The test results (if they are significant at a confidence level of at least 95%) are mentioned in the table analysis.
In the report, when we indicate that a sub-group of the sample is "more likely" or "less likely", it means that the statistical testing returned a valid statistically significant difference between this subgroup and its complement, even if the percentage is low.
A.16.7 Weighting Factors for Wave 16
Some subgroups are sometimes under or overrepresented in a sample compared to their actual distribution in the population. The weighting of a sample makes it possible to correct the differences that exist in the representation of the various subgroups of this sample compared to what is usually observed in the population under study. Therefore, the weighting factors are the weight given to each respondent corresponding to a subgroup of the sample.
The following tables present the weight accorded to each target of the sample.
| Gender by age by province | Weight |
|---|---|
| British Columbia Male 18-24 | 0.69 |
| British Columbia Male 25-34 | 1.18 |
| British Columbia Male 35-44 | 1.12 |
| British Columbia Male 45-54 | 1.04 |
| British Columbia Male 55-64 | 1.16 |
| British Columbia Male 65+ | 1.60 |
| British Columbia Female 18-24 | 0.65 |
| British Columbia Female 25-34 | 1.17 |
| British Columbia Female 35-44 | 1.15 |
| British Columbia Female 45-54 | 1.12 |
| British Columbia Female 55-64 | 1.25 |
| British Columbia Female 65+ | 1.83 |
| Alberta Male 18-24 | 0.61 |
| Alberta Male 25-34 | 1.01 |
| Alberta Male 35-44 | 1.09 |
| Alberta Male 45-54 | 0.92 |
| Alberta Male 55-64 | 0.90 |
| Alberta Male 65+ | 1.00 |
| Alberta Female 18-24 | 0.57 |
| Alberta Female 25-34 | 1.01 |
| Alberta Female 35-44 | 1.10 |
| Alberta Female 45-54 | 0.91 |
| Alberta Female 55-64 | 0.92 |
| Alberta Female 65+ | 1.13 |
| Manitoba / Saskatchewan Male 18-24 | 0.38 |
| Manitoba / Saskatchewan Male 25-34 | 0.56 |
| Manitoba / Saskatchewan Male 35-44 | 0.55 |
| Manitoba / Saskatchewan Male 45-54 | 0.48 |
| Manitoba / Saskatchewan Male 55-64 | 0.53 |
| Manitoba / Saskatchewan Male 65+ | 0.66 |
| Manitoba / Saskatchewan Female 18-24 | 0.35 |
| Manitoba / Saskatchewan Female 25-34 | 0.55 |
| Manitoba / Saskatchewan Female 35-44 | 0.56 |
| Manitoba / Saskatchewan Female 45-54 | 0.49 |
| Manitoba / Saskatchewan Female 55-64 | 0.55 |
| Manitoba / Saskatchewan Female 65+ | 0.78 |
| Ontario Male 18-24 | 2.13 |
| Ontario Male 25-34 | 3.33 |
| Ontario Male 35-44 | 3.01 |
| Ontario Male 45-54 | 2.99 |
| Ontario Male 55-64 | 3.30 |
| Ontario Male 65+ | 4.05 |
| Ontario Female 18-24 | 1.98 |
| Ontario Female 25-34 | 3.28 |
| Ontario Female 35-44 | 3.20 |
| Ontario Female 45-54 | 3.21 |
| Ontario Female 55-64 | 3.48 |
| Ontario Female 65+ | 4.86 |
| Quebec Male 18-24 | 1.09 |
| Quebec Male 25-34 | 1.80 |
| Quebec Male 35-44 | 1.89 |
| Quebec Male 45-54 | 1.76 |
| Quebec Male 55-64 | 2.08 |
| Quebec Male 65+ | 2.71 |
| Quebec Female 18-24 | 1.04 |
| Quebec Female 25-34 | 1.79 |
| Quebec Female 35-44 | 1.90 |
| Quebec Female 45-54 | 1.75 |
| Quebec Female 55-64 | 2.12 |
| Quebec Female 65+ | 2.95 |
| Atlantic Male 18-24 | 0.32 |
| Atlantic Male 25-34 | 0.47 |
| Atlantic Male 35-44 | 0.47 |
| Atlantic Male 45-54 | 0.52 |
| Atlantic Male 55-64 | 0.63 |
| Atlantic Male 65+ | 0.85 |
| Atlantic Female 18-24 | 0.30 |
| Atlantic Female 25-34 | 0.47 |
| Atlantic Female 35-44 | 0.50 |
| Atlantic Female 45-54 | 0.55 |
| Atlantic Female 55-64 | 0.67 |
| Atlantic Female 65+ | 0.99 |
| CMAs | Weight |
|---|---|
| British Columbia (Vancouver CMA) | 7.39 |
| British Columbia (Other) | 6.57 |
| Alberta (Calgary CMA) | 3.91 |
| Alberta (Edmonton CMA) | 3.74 |
| Alberta (Other) | 3.51 |
| Saskatchewan | 2.93 |
| Manitoba | 3.51 |
| Ontario (Toronto CMA) | 16.97 |
| Ontario (Other) | 21.85 |
| Quebec (Montreal CMA) | 11.33 |
| Quebec (Quebec City CMA) | 2.30 |
| Quebec (Other) | 9.25 |
| New-Brunswick | 2.16 |
| Nova Scotia | 2.72 |
| Prince Edward Island | 0.42 |
| Newfoundland | 1.44 |
| Education | Weight |
|---|---|
| Primary/Collegial | 72.25 |
| University – Rest of Canada | 21.87 |
| University - Quebec | 5.88 |
| Language by region | Weight |
|---|---|
| French - Rest of Canada | 2.45 |
| French - QC | 17.32 |
| Non-French - Rest of Canada | 74.67 |
| Non-French - QC | 5.56 |
| Presence of children in the household | Weight |
|---|---|
| Yes | 27.75 |
| No | 72.25 |
| Place of birth | Weight |
|---|---|
| Born in Canada | 78.31 |
| Born outside Canada | 21.69 |
| Ethnicity | Weight |
|---|---|
| Indigenous | 4.82 |
| Black | 3.46 |
| Other | 91.72 |
A.17.1 Qualitative Methodology for Wave 17
Leger conducted a series of eight virtual discussion group sessions with French-speaking and English-speaking Canadians recruited from all the regions in Canada. Participants were recruited, screened for vaccination status and assigned to virtual discussion groups by vaccination status and demographics of interest (e.g., young adults, vaccinated parents, vaccinated/unvaccinated individuals). Twelve participants were recruited by our professional recruiters for each discussion group session. Some sessions were conducted with young adults, others with vaccinated parents, and others were held with individuals from the general population at large.
A total of 64 recruits participated in the online focus groups (see Table 2 for details). All participants in the focus group received an honorarium of $135.
Online discussion sessions were conducted using the CMNTY software to facilitate moderation and to ensure an optimal interface between moderator and participants. Participants could interact with one another and the moderator as the discussion unfolded. Each session had a duration of 1h30 to 2h.
All sessions allowed for remote viewing by Leger and Health Canada observers.
| Session Detail | Date | Recruits | Participants | Language |
|---|---|---|---|---|
| #1 (Young adults, two doses (18-35), Ontario and ATL) | September 26th, 2022 | 12 | 8 | English |
| #2 (Young adults, two doses (18-35), BC, Prairies, Territories) | September 26th, 2022 | 12 | 9 | English |
| #3 (Young adults, two doses (18-35), QC, NB) | September 26th, 2022 | 12 | 9 | French |
| #4 (Gen pop 18+, three doses or more, BC, Prairies, Territories) | September 27th, 2022 | 12 | 8 | English |
| #5 (Gen pop 18+, three doses or more, Ontario and ATL) | September 27th, 2022 | 12 | 7 | English |
| #6 (Gen pop 18+, three doses or more, QC, NB) | September 26th, 2022 | 12 | 8 | French |
| #7 (Vaccinated parents (mix of unvaccinated and vaccinated child, BC, prairies, Ontario) | September 28th, 2022 | 12 | 5 | English |
| #8 (Vaccinated parents (mix of unvaccinated and vaccinated child), QC, NB) | September 27th, 2022 | 12 | 10 | French |
Recruitment was carried out by professional recruiters. The recruitment guide (available in appendix 2) ensured that the participants met the profiles sought for each session and that they were equipped to participate in an online discussion session. To do so, they had to confirm that they had a high-speed Internet connection, a computer or a laptop.
Moderation
All focus group sessions were moderated and supervised by a senior Leger researcher, assisted by a research analyst. Health Canada employees were able to observe the discussion forum. The discussion guide (available in appendix 3) consisted of a semi-structured discussion guide. It allowed the moderator to follow the thread of the discussion and ensured that an array of themes was covered while leaving sufficient room for the participants to express themselves and develop in detail their experiences, ideas, opinions and perceptions.
The qualitative portion of the research provides insight into the opinions of a population, rather than providing a measure in percent of the opinions held, as would be measured in a quantitative study. The results of this type of research should be viewed as directional only. No inference to the general population can be done with the results of this research.
Limitation
Qualitative research is designed to reveal a rich range of opinions and interpretations rather than to measure what percentage of the target population holds a given opinion. These results must not be used to estimate the numeric proportion or number of individuals in the population who hold a particular opinion because they are not statistically projectable.
A.18.1 Quantitative Methodology for Wave 18
Quantitative research was conducted through online surveys using Computer Aided Web Interviewing (CAWI) technology.
As a CRIC Member, Leger adheres to the most stringent guidelines for quantitative research. The survey was conducted in accordance with the Government of Canada requirements for quantitative research, including the Standards of the Conduct of Government of Canada Public Opinion Research—Series D—Quantitative Research.
Respondents were assured of the voluntary, confidential and anonymous nature of this research. As with all research conducted by Leger, all information that could allow for the identification of participants was removed from the data in accordance with the Privacy Act.
The questionnaire is available in Appendix E.
A.18.2 Sampling Procedures for Wave 18
Computer Aided Web Interviewing (CAWI)
Leger conducted a panel-based Internet survey with a sample of adult Canadians. A total of 3,026 respondents participated in the Wave 18 of the Custom survey. Leger targeted 3,000 Canadians, including 2,400 panelists form the general population and oversamples of 400 Black-identifying individuals and 200 Indigenous-identifying individuals. The exact distribution is presented in the following section. Participant selection was done randomly from Leo's online panel.
Leger owns and operates an Internet panel of more than 400,000 Canadians from coast to coast. An Internet panel is made up of Web users profiled on different sociodemographic variables. The majority of Leger's panel members (61%) have been recruited randomly over the phone over the past decade, making it highly similar to the actual Canadian population on many demographic characteristics.
Since an Internet sample is non-probabilistic in nature, the margin of error does not apply.
A.18.3 Data Collection for Wave 18
Fieldwork for the survey was conducted from November 18th to December 8th, 2022. The participation rate for the survey was 14.5%. A pre-test of 38 interviews was completed on November 18th, 2022. More specifically, 25 interviews were conducted in English and 13 were conducted in French. Survey interviews lasted 10 minutes on average.
To achieve data reliability in all subgroups Canadian adults were surveyed in all regions of the country. The following tables detail sample distribution by region and ethnicity.
| Region | Number of respondents |
|---|---|
| Ontario | 1,127 |
| Quebec | 813 |
| British Columbia and Territories | 382 |
| Alberta | 302 |
| Prairies | 212 |
| Atlantic Region | 190 |
| Total | 3,026 |
| Ethnicity | Number of respondents |
|---|---|
| White | 2,008 |
| Indigenous | 260 |
| Black | 432 |
| South Asian | 89 |
| East Asian | 132 |
| Other / None of the above | 210 |
| Total | 3,026 |
Since a sample drawn from an Internet panel is not probabilistic in nature, the margin of error cannot be calculated for this survey. Respondents for this survey were selected from those who volunteered to participate/registered to participate in online surveys. The results of such surveys cannot be described as statistically projectable to the target population. The data have been weighted to reflect the demographic composition of the target population. Because the sample is based on those who initially self-selected for participation, no estimates of sampling error can be calculated.
Based on the most recent data from Statistics Canada's national census, Leger weighted the results of this survey by age, gender, region, first language (mother tongue), education level, presence of children in the household, place of birth, and ethnicity. The most recent data regarding age, gender, region and first language was from the 2021 census. The data for education level, presence of children in the household, place of birth and ethnicity came from the 2016 census.
A.18.4 Participation rate for the Web Survey for Wave 18
The overall participation rate for this study is 14.5%.
Below is the calculation of the Web survey's participation rate. The participation rate is calculated by dividing the number of completed questionnaires by the number of invitations sent. The typical participation rates for Web-surveys are between 20% and 30%. A response rate of 14.5% may seem a bit low but given the limited amount of time for fieldwork and the specific oversamples of Black-identifying and Indigenous-identifying individuals, invitations had to be spread more widely in the panel to achieve the objectives, which has an impact on the participation rate.
| Total email addresses used | |
|---|---|
| Invalid Cases | - |
| -invitations mistakenly sent to people who did not qualify for the study | 39 |
| -incomplete or missing email addresses | - |
| Unresolved (U) | 19,707 |
| -email invitations bounce back | 16 |
| -email invitations unanswered | 19,691 |
| In-scope non-responding units (IS) | 383 |
| -respondent refusals | 250 |
| -language problem | - |
| -early breakoffs | 133 |
| Responding units (R) | 3,404 |
| -completed surveys disqualified—quota filled | 339 |
| -completed surveys disqualified for other reasons | 39 |
| -completed surveys | 3,026 |
| Participation rate/response rate = R ÷ (U + IS + R) | 14.5% |
A.18.5 Additional Socio-Demographic Analysis
A basic comparison of the unweighted and weighted sample sizes was conducted to identify any potential non-response bias that could be introduced by lower response rates among specific demographic subgroups (see tables below).
A.18.6 Unweighted and Weighted Samples for Wave 18
The table below presents the geographic distribution of respondents before and after weighting. There were almost no imbalances in geographical distribution in the unweighted sample. The weighting process has mainly adjusted some minor discrepancies.
| Province/Territory | Unweighted | Weighted |
|---|---|---|
| Ontario | 1,127 | 1,171 |
| Quebec | 813 | 699 |
| British Columbia and Territories | 382 | 421 |
| Alberta | 302 | 337 |
| Prairies | 212 | 195 |
| Atlantic | 190 | 204 |
The following tables present the demographic distribution of respondents according to gender, age group, first language and education. First, regarding gender, we can see that weighting has adjusted slightly the proportion of males and females. Female respondents were a little bit overrepresented in this survey. The weight of the men was therefore boosted so as not to underestimate their actual weight in the results.
| Gender | Unweighted | Weighted |
|---|---|---|
| Male | 1,261 | 1,460 |
| Female | 1,748 | 1,550 |
Regarding age distribution, the weighting process has corrected some minor discrepancies.
| Age | Unweighted | Weighted |
|---|---|---|
| Between 18 and 34 | 879 | 807 |
| Between 35 and 55 | 1,068 | 974 |
| 55 years old and over | 1,079 | 1,245 |
Minor imbalances with language distribution were corrected with weighting, as presented below.
| Language (Mother tongue) | Unweighted | Weighted |
|---|---|---|
| English | 1,975 | 2,102 |
| French | 777 | 597 |
| Other | 260 | 308 |
The table below presents the distribution based on education. The weighting corrected every gap between the actual distribution in the population and the final sample.
| Education | Unweighted | Weighted |
|---|---|---|
| Elementary/High school | 685 | 893 |
| College | 992 | 1,253 |
| University | 1,317 | 837 |
The following two tables present the distribution based on the presence of children in the household and place of birth. Again, imbalances were minor and corrected by weighting.
| Presence of children in the household | Unweighted | Weighted |
|---|---|---|
| Yes | 789 | 822 |
| No | 2,223 | 2,189 |
| Place of birth | Unweighted | Weighted |
|---|---|---|
| Canada | 2,378 | 2,363 |
| Other | 634 | 642 |
The last table presents the distribution based on ethnicity. Weighting boosted the weight of white individuals and reduced that of Indigenous-identifying and Black-identifying respondents to closely follow the actual distribution in the population.
| Ethnicity | Unweighted | Weighted |
|---|---|---|
| White | 2,008 | 2,283 |
| Indigenous | 260 | 146 |
| Black | 432 | 111 |
| South Asian | 89 | 121 |
| East Asian | 132 | 152 |
| Other | 192 | 242 |
There is no evidence from the data that having achieved a different age or gender distribution prior to weighting would have significantly changed the results of this study. The relatively small weight factors (see the section below) and differences in responses between various subgroups suggest that data quality was not affected. The weight that was applied corrected the initial imbalance for data analysis purposes, and no further manipulations were necessary.
As with all research conducted by Leger, the contact information was kept entirely confidential and all information that could allow for the identification of participants was removed from the data in accordance with Canada's Privacy Act.
Note on testing for statistical differences
According to the normal distribution, a two-tailed test is always done between two proportions and based on the unweighted total columns. The test is performed by comparing a percentage with the percentage formed by the complement of the relevant category (e.g., of the male subgroup is the female subgroup; the complement of the 18–24 age subgroup is the 25+ age subgroup, and the complement of the college-educated subgroup is the sub-group consisting of respondents with elementary, high school or university education). The test results (if they are significant at a confidence level of at least 95%) are mentioned in the table analysis.
In the report, when we indicate that a sub-group of the sample is "more likely" or "less likely", it means that the statistical testing returned a valid statistically significant difference between this subgroup and its complement, even if the percentage is low.
A.18.7 Weighting Factors for Wave 18
Some subgroups are sometimes under or overrepresented in a sample compared to their actual distribution in the population. The weighting of a sample makes it possible to correct the differences that exist in the representation of the various subgroups of this sample compared to what is usually observed in the population under study. Therefore, the weighting factors are the weight given to each respondent corresponding to a subgroup of the sample.
The following tables present the weight accorded to each target of the sample.
| Gender by age by province | Weight |
|---|---|
| British Columbia Male 18-24 | 0.69 |
| British Columbia Male 25-34 | 1.18 |
| British Columbia Male 35-44 | 1.12 |
| British Columbia Male 45-54 | 1.04 |
| British Columbia Male 55-64 | 1.16 |
| British Columbia Male 65+ | 1.60 |
| British Columbia Female 18-24 | 0.65 |
| British Columbia Female 25-34 | 1.17 |
| British Columbia Female 35-44 | 1.15 |
| British Columbia Female 45-54 | 1.12 |
| British Columbia Female 55-64 | 1.24 |
| British Columbia Female 65+ | 1.83 |
| Alberta Male 18-24 | 0.61 |
| Alberta Male 25-34 | 1.01 |
| Alberta Male 35-44 | 1.09 |
| Alberta Male 45-54 | 0.91 |
| Alberta Male 55-64 | 0.90 |
| Alberta Male 65+ | 0.99 |
| Alberta Female 18-24 | 0.57 |
| Alberta Female 25-34 | 1.01 |
| Alberta Female 35-44 | 1.09 |
| Alberta Female 45-54 | 0.91 |
| Alberta Female 55-64 | 0.92 |
| Alberta Female 65+ | 1.13 |
| Manitoba / Saskatchewan Male 18-24 | 0.38 |
| Manitoba / Saskatchewan Male 25-34 | 0.56 |
| Manitoba / Saskatchewan Male 35-44 | 0.55 |
| Manitoba / Saskatchewan Male 45-54 | 0.48 |
| Manitoba / Saskatchewan Male 55-64 | 0.53 |
| Manitoba / Saskatchewan Male 65+ | 0.66 |
| Manitoba / Saskatchewan Female 18-24 | 0.35 |
| Manitoba / Saskatchewan Female 25-34 | 0.55 |
| Manitoba / Saskatchewan Female 35-44 | 0.56 |
| Manitoba / Saskatchewan Female 45-54 | 0.49 |
| Manitoba / Saskatchewan Female 55-64 | 0.55 |
| Manitoba / Saskatchewan Female 65+ | 0.78 |
| Ontario Male 18-24 | 2.12 |
| Ontario Male 25-34 | 3.32 |
| Ontario Male 35-44 | 3.00 |
| Ontario Male 45-54 | 2.98 |
| Ontario Male 55-64 | 3.29 |
| Ontario Male 65+ | 4.04 |
| Ontario Female 18-24 | 1.97 |
| Ontario Female 25-34 | 3.27 |
| Ontario Female 35-44 | 3.19 |
| Ontario Female 45-54 | 3.20 |
| Ontario Female 55-64 | 3.47 |
| Ontario Female 65+ | 4.85 |
| Quebec Male 18-24 | 1.09 |
| Quebec Male 25-34 | 1.80 |
| Quebec Male 35-44 | 1.89 |
| Quebec Male 45-54 | 1.76 |
| Quebec Male 55-64 | 2.07 |
| Quebec Male 65+ | 2.70 |
| Quebec Female 18-24 | 1.04 |
| Quebec Female 25-34 | 1.78 |
| Quebec Female 35-44 | 1.89 |
| Quebec Female 45-54 | 1.74 |
| Quebec Female 55-64 | 2.11 |
| Quebec Female 65+ | 3.21 |
| Atlantic Male 18-24 | 0.32 |
| Atlantic Male 25-34 | 0.47 |
| Atlantic Male 35-44 | 0.47 |
| Atlantic Male 45-54 | 0.52 |
| Atlantic Male 55-64 | 0.63 |
| Atlantic Male 65+ | 0.85 |
| Atlantic Female 18-24 | 0.30 |
| Atlantic Female 25-34 | 0.47 |
| Atlantic Female 35-44 | 0.50 |
| Atlantic Female 45-54 | 0.55 |
| Atlantic Female 55-64 | 0.67 |
| Atlantic Female 65+ | 0.99 |
| CMAs | Weight |
|---|---|
| British Columbia (Vancouver CMA) | 7.37 |
| British Columbia (Other) | 6.55 |
| Alberta (Calgary CMA) | 3.90 |
| Alberta (Edmonton CMA) | 3.73 |
| Alberta (Other) | 3.50 |
| Saskatchewan | 2.93 |
| Manitoba | 3.51 |
| Ontario (Toronto CMA) | 16.92 |
| Ontario (Other) | 21.79 |
| Quebec (Montreal CMA) | 11.57 |
| Quebec (Quebec City CMA) | 2.30 |
| Quebec (Other) | 9.22 |
| New-Brunswick | 2.16 |
| Nova Scotia | 2.71 |
| Prince Edward Island | 0.42 |
| Newfoundland | 1.44 |
| Education | Weight |
|---|---|
| Primary/Collegial | 72.33 |
| University – Rest of Canada | 21.81 |
| University - Quebec | 5.86 |
| Language by region | Weight |
|---|---|
| French - Rest of Canada | 2.45 |
| French - QC | 17.28 |
| Non-French - Rest of Canada | 74.47 |
| Non-French - QC | 5.81 |
| Presence of children in the household | Weight |
|---|---|
| Yes | 27.67 |
| No | 72.33 |
| Place of birth | Weight |
|---|---|
| Born in Canada | 78.10 |
| Born outside Canada | 21.90 |
| Ethnicity | Weight |
|---|---|
| Indigenous | 4.81 |
| Black | 3.45 |
| Other | 91.74 |
A.19.1 Qualitative methodology for Wave 19
Leger conducted a series of eight focus group sessions with French-speaking and English-speaking Canadians. Conducting the groups online offered the opportunity to regroup people from all the regions in Canada. Two focus groups were held with 2SLGBTQIA+ identifying individuals (18-55 years old), two groups were held with racialized populations (18-55 years old), three groups were held with parents and people who are pregnant, and one group was held with young adults (18-34 years old). All groups were interviewed using the same discussion guide, but questions were adapted for the parents' groups in order to gain insights on specific challenged they may face and perceptions they may hold regarding the topics under study. Overall, three focus groups were conducted in French (one of each demographic), and the remaining five were conducted in English.
For each online focus group, ten participants were recruited by our professional recruiters. In the end, a total of 60 participants took part in the online focus groups (see table 2 for details). All participants in the focus groups received an honorarium of $135. Because the study dealt with topics some participants may have found distressing, the following mental health resources were shared both at the beginning and the end of each focus group through the chat function:
- Get Help Here: https://www.canada.ca/mental-health
- Wellness Together Canada: https://www.wellnesstogether.ca/en-CA
- Talk Suicide Canada: https://talksuicide.ca/
- The Hope for Wellness Helpline: https://www.hopeforwellness.ca/
The focus groups were conducted online using Focus Vision's CMNTY platform. This platform allowed for video conferencing groups, observers in a separate virtual room, chat between participants and the moderator, and chat between the observation room and the moderator. Each group was 120 minutes long, to ensure the participation of each participant. All sessions allowed for remote viewing by Leger and Government of Canada observers. All groups were scheduled to be held on February 7th, 8th, or 9th, 2023.
| GR | Region | Recruits | Participants | Target | Language | Date | Time |
|---|---|---|---|---|---|---|---|
| 1 | BC, Prairies, Ontario | 10 | 8 | 2SLGBTQI+ (18-55 years old) | English | February 7th, 2023 | 5pm |
| 2 | Québec, New-Brunswick | 10 | 6 | 2SLGBTQI+ (18-55 years old) | French | February 7th, 2023 | 5pm |
| 3 | Ontario | 10 | 9 | Racialized populations (18-55 years old) | English | February 7th, 2023 | 7pm |
| 4 | Québec, New-Brunswick | 10 | 7 | Racialized populations (18-55 years old) | French | February 7th, 2023 | 7pm |
| 5 | BC, Prairies | 10 | 8 | Young adults (18-34 years old) | English | February 9th, 2023 | 7pm |
| 6 | Ontario, Atlantic | 10 | 6 | Parents, people who are pregnant | English | February 8th, 2023 | 5pm |
| 7 | BC, Prairies, Territories | 10 | 8 | Parents, people who are pregnant | English | February 8th, 2023 | 7pm |
| 8 | Québec, New-Brunswick | 10 | 8 | Parents, people who are pregnant | French | February 8th, 2023 | 5pm |
Total |
80 | 60 | |||||
Recruitment was carried out by professional recruiters. The recruitment guide (available in the appendix C) ensured that the participants met the profiles sought for each session and that they were equipped to participate in an online discussion session. To do so, they had to confirm that they had a high-speed Internet connexion, a computer or laptop.
Moderation
All focus group sessions were moderated and supervised by a Leger researcher assisted by a research analyst. One researcher moderated the groups in French and one other moderated the groups in English. The discussion guide (available in appendix B) consisted of a semi-structured discussion guide. It allowed moderators to follow the thread of the discussion and ensured that an array of themes was covered while leaving sufficient room for the participants to express themselves and develop in detail their experiences, ideas, opinions and perceptions.
This qualitative portion of the research provides insight into the opinions of a population, rather than providing a measure in percent of the opinions held, as would be measured in a quantitative study. The results of this type of research should be viewed as directional only. No inference to the general population can be done with the results of this research.
Quality Control
Leger recruited participants with the help of CRC Research, our qualitative recruitment partner, using a hybrid method. First, an online screening was used followed by a final recruitment screening over the phone. The online recruitment enabled us to find many potential candidates that fit the recruitment criteria across all regions of Canada. Then, these potential candidates were contacted by phone by CRC's professional recruiters to confirm their eligibility and that they have access to a computer, a high-speed online connection as well as a webcam to participate in the online discussion session. After being adequately screened and recruited, participants (as well as observers) received detailed instructions from CRC Research on how to log in to the live session and other key information regarding the procedure itself.
The recruitment screener informed participants of all their rights under Canada's Privacy legislation and the Standards for the Conduct of Government of Canada Public Opinion Research. Specifically, their confidentiality was guaranteed, and that participation is voluntary.
After each group, a meeting was organized with the researchers in order to get the general outlines and trends.
Limitation
Qualitative research is designed to reveal a rich range of opinions and interpretations rather than to measure what percentage of the target population holds a given opinion. These results must not be used to estimate the numeric proportion or number of individuals in the population who hold a particular opinion because they are not statistically projectable.
A.20.1 Quantitative Methodology for Wave 20
Quantitative research was conducted through online surveys using Computer Aided Web Interviewing (CAWI) technology.
As a CRIC Member, Leger adheres to the most stringent guidelines for quantitative research. The survey was conducted in accordance with the Government of Canada requirements for quantitative research, including the Standards of the Conduct of Government of Canada Public Opinion Research—Series D—Quantitative Research.
Respondents were assured of the voluntary, confidential and anonymous nature of this research. As with all research conducted by Leger, all information that could allow for the identification of participants was removed from the data in accordance with the Privacy Act.
The questionnaire is available in Appendix B.
A.20.2 Sampling Procedures
Computer Aided Web Interviewing (CAWI)
Leger conducted a panel-based Internet survey with a sample of adult Canadians. A total of 3,026 respondents participated in the survey, including a general population sample of 2,426 respondents as well as oversamples of 400 Black-identifying individuals and 200 Indigenous-identifying individuals. The exact distribution is presented in the following section. Participant selection was done randomly from Leo's online panel.
Leger owns and operates an Internet panel of more than 400,000 Canadians from coast to coast. An Internet panel is made up of Web users profiled on different sociodemographic variables. The majority of Leger's panel members (61%) have been recruited randomly over the phone over the past decade, making it highly similar to the actual Canadian population on many demographic characteristics.
Since an Internet sample is non-probabilistic in nature, the margin of error does not apply.
A.20.3 Data Collection for Wave 20
Fieldwork for the survey was conducted from January 12 to 30, 2023. The participation rate for the survey was 20.14%. A pre-test of 47 interviews was completed on January 12, 2023. More specifically, 24 interviews were conducted in English and 23were conducted in French. Survey interviews lasted 10 minutes on average.
To achieve data reliability in all subgroups, a total sample of 3,026 Canadians were surveyed in all regions of the country. The overall sample also included oversamples of 400 Black-identifying and 200 Indigenous-identifying individuals.
| Region | Number of respondents |
|---|---|
| Ontario | 1,114 |
| Quebec | 767 |
| British Columbia and Territories | 366 |
| Alberta | 351 |
| Prairies | 231 |
| Atlantic Region | 197 |
| Total | 3,026 |
Since a sample drawn from an Internet panel is not probabilistic in nature, the margin of error cannot be calculated for this survey. Respondents for this survey were selected from those who volunteered to participate/registered to participate in online surveys. The results of such surveys cannot be described as statistically projectable to the target population. The data have been weighted to reflect the demographic composition of the target population. Because the sample is based on those who initially self-selected for participation, no estimates of sampling error can be calculated.
Based on the most recent data from Statistics Canada's national census, Leger weighted the results of this survey by age, gender, region, first language (mother tongue), education level, presence of children in the household, place of birth, and ethnicity. The most recent data regarding age, gender, region and first language was from the 2021 census. The data for education level, presence of children in the household, place of birth and ethnicity came from the 2016 census.
A.20.4 Participation Rate for the Web Survey for Wave 20
The overall participation rate for this study is 20.14%.
Below is the calculation of the Web survey's participation rate. The participation rate is calculated by dividing the number of completed questionnaires by the number of invitations sent. The typical participation rates for Web-surveys are between 20% and 30%. A response rate of 20.14% may seem a bit low but given the limited amount of time for fieldwork and the specific oversamples of Black-identifying and Indigenous-identifying individuals, invitations had to be spread more widely in the panel to achieve the objectives, this had a slight impact on the response rate, which explains why it is a little lower but still in the average range.
| Total email addresses used | |
|---|---|
| Invalid Cases | 76 |
| -invitations mistakenly sent to people who did not qualify for the study | 76 |
| -incomplete or missing email addresses | - |
| Unresolved (U) | 12,955 |
| -email invitations bounce back | 15 |
| -email invitations unanswered | 12,940 |
| In-scope non-responding units (IS) | 245 |
| -respondent refusals | 245 |
| -language problem | - |
| -early breakoffs | - |
| Responding units (R) | 3,329 |
| -completed surveys disqualified—quota filled | 293 |
| -completed surveys disqualified for other reasons | 10 |
| -completed surveys | 3,026 |
| Participation rate/response rate = R ÷ (U + IS + R) | 20.14% |
A.20.5 Additional socio-demographic analysis
A basic comparison of the unweighted and weighted sample sizes was conducted to identify any potential non-response bias that could be introduced by lower response rates among specific demographic subgroups (see tables below).
A.20.6 Unweighted and Weighted Samples for Wave 20
The table below presents the geographic distribution of respondents before and after weighting. There were almost no imbalances in geographical distribution in the unweighted sample. The weighting process has mainly adjusted some minor discrepancies in Quebec and British Columbia and the territories.
| Province/Territory | Unweighted | Weighted |
|---|---|---|
| Ontario | 1,114 | 1,171 |
| Quebec | 767 | 699 |
| British Columbia and Territories | 366 | 421 |
| Alberta | 351 | 337 |
| Prairies | 231 | 195 |
| Atlantic | 197 | 204 |
The following tables present the demographic distribution of respondents according to gender, age group, first language and education. First, regarding gender, we can see that weighting has adjusted slightly the proportion of males and females. Female respondents were a little bit overrepresented in this survey. The weight of the men was therefore boosted so as not to underestimate their actual weight in the results.
| Gender | Unweighted | Weighted |
|---|---|---|
| Male | 1,327 | 1,459 |
| Female | 1,686 | 1,550 |
Regarding age distribution, the weighting process has corrected some minor discrepancies.
| Age | Unweighted | Weighted |
|---|---|---|
| Between 18 and 34 | 876 | 792 |
| Between 35 and 54 | 1,120 | 1,054 |
| 55 years old and over | 1,030 | 1,180 |
Minor imbalances with language distribution were corrected with weighting, especially French respondents who were slightly over-represented.
| Language (Mother tongue) | Unweighted | Weighted |
|---|---|---|
| English | 1,982 | 2,074 |
| French | 747 | 597 |
| Other | 280 | 329 |
The table below presents the distribution based on education. The weighting corrected mainly the respondents with a university degree which were over-represented in the sample.
| Education | Unweighted | Weighted |
|---|---|---|
| Elementary/High school | 685 | 918 |
| College | 925 | 1,241 |
| University | 1,396 | 837 |
The following two tables present the distribution based on the presence of children in the household and place of birth. Again, imbalances were minor and corrected by weighting.
| Presence of children in the household | Unweighted | Weighted |
|---|---|---|
| Yes | 845 | 819 |
| No | 2,162 | 2,189 |
| Place of birth | Unweighted | Weighted |
|---|---|---|
| Canada | 2,294 | 2,363 |
| Other | 708 | 641 |
The last table presents the distribution based on ethnicity. Weighting boosted the weight of white individuals and reduced that of Indigenous-identifying and Black-identifying respondents to closely follow the actual distribution in the population.
| Ethnicity | Unweighted | Weighted |
|---|---|---|
| White | 1,961 | 2,276 |
| Indigenous | 262 | 146 |
| Black | 437 | 106 |
| South Asian | 110 | 126 |
| Chinese | 135 | 140 |
| Other | 173 | 220 |
There is no evidence from the data that having achieved a different age or gender distribution prior to weighting would have significantly changed the results of this study. The relatively small weight factors (see the section below) suggest that data quality was not affected. The weight that was applied corrected the initial imbalance for data analysis purposes, and no further manipulations were necessary.
As with all research conducted by Leger, the contact information was kept entirely confidential and all information that could allow for the identification of participants was removed from the data in accordance with Canada's Privacy Act.
A.20.7 Weighting Factors
Some subgroups are sometimes under or overrepresented in a sample compared to their actual distribution in the population. The weighting of a sample makes it possible to correct the differences that exist in the representation of the various subgroups of this sample compared to what is usually observed in the population under study. Therefore, the weighting factors are the weight given to each respondent corresponding to a subgroup of the sample.
The following tables present the weight accorded to each target of the sample.
| Gender by age by province | Weight |
|---|---|
| British Columbia Male 18-24 | 0.69 |
| British Columbia Male 25-34 | 1.18 |
| British Columbia Male 35-44 | 1.12 |
| British Columbia Male 45-54 | 1.04 |
| British Columbia Male 55-64 | 1.16 |
| British Columbia Male 65+ | 1.60 |
| British Columbia Female 18-24 | 0.65 |
| British Columbia Female 25-34 | 1.17 |
| British Columbia Female 35-44 | 1.15 |
| British Columbia Female 45-54 | 1.12 |
| British Columbia Female 55-64 | 1.24 |
| British Columbia Female 65+ | 1.83 |
| Alberta Male 18-24 | 0.61 |
| Alberta Male 25-34 | 1.01 |
| Alberta Male 35-44 | 1.09 |
| Alberta Male 45-54 | 0.91 |
| Alberta Male 55-64 | 0.90 |
| Alberta Male 65+ | 0.99 |
| Alberta Female 18-24 | 0.57 |
| Alberta Female 25-34 | 1.01 |
| Alberta Female 35-44 | 1.09 |
| Alberta Female 45-54 | 0.91 |
| Alberta Female 55-64 | 0.92 |
| Alberta Female 65+ | 1.13 |
| Manitoba / Saskatchewan Male 18-24 | 0.38 |
| Manitoba / Saskatchewan Male 25-34 | 0.56 |
| Manitoba / Saskatchewan Male 35-44 | 0.55 |
| Manitoba / Saskatchewan Male 45-54 | 0.48 |
| Manitoba / Saskatchewan Male 55-64 | 0.53 |
| Manitoba / Saskatchewan Male 65+ | 0.66 |
| Manitoba / Saskatchewan Female 18-24 | 0.35 |
| Manitoba / Saskatchewan Female 25-34 | 0.55 |
| Manitoba / Saskatchewan Female 35-44 | 0.56 |
| Manitoba / Saskatchewan Female 45-54 | 0.49 |
| Manitoba / Saskatchewan Female 55-64 | 0.55 |
| Manitoba / Saskatchewan Female 65+ | 0.78 |
| Ontario Male 18-24 | 2.12 |
| Ontario Male 25-34 | 3.32 |
| Ontario Male 35-44 | 3.00 |
| Ontario Male 45-54 | 2.98 |
| Ontario Male 55-64 | 3.29 |
| Ontario Male 65+ | 4.04 |
| Ontario Female 18-24 | 1.97 |
| Ontario Female 25-34 | 3.27 |
| Ontario Female 35-44 | 3.19 |
| Ontario Female 45-54 | 3.20 |
| Ontario Female 55-64 | 3.47 |
| Ontario Female 65+ | 4.85 |
| Quebec Male 18-24 | 1.09 |
| Quebec Male 25-34 | 1.80 |
| Quebec Male 35-44 | 1.89 |
| Quebec Male 45-54 | 1.76 |
| Quebec Male 55-64 | 2.07 |
| Quebec Male 65+ | 2.70 |
| Quebec Female 18-24 | 1.04 |
| Quebec Female 25-34 | 1.78 |
| Quebec Female 35-44 | 1.89 |
| Quebec Female 45-54 | 1.74 |
| Quebec Female 55-64 | 2.11 |
| Quebec Female 65+ | 3.21 |
| Atlantic Male 18-24 | 0.32 |
| Atlantic Male 25-34 | 0.47 |
| Atlantic Male 35-44 | 0.47 |
| Atlantic Male 45-54 | 0.52 |
| Atlantic Male 55-64 | 0.63 |
| Atlantic Male 65+ | 0.85 |
| Atlantic Female 18-24 | 0.30 |
| Atlantic Female 25-34 | 0.47 |
| Atlantic Female 35-44 | 0.50 |
| Atlantic Female 45-54 | 0.55 |
| Atlantic Female 55-64 | 0.67 |
| Atlantic Female 65+ | 0.99 |
| CMAs | Weight |
|---|---|
| British Columbia (Vancouver CMA) | 7.37 |
| British Columbia (Other) | 6.55 |
| Alberta (Calgary CMA) | 3.90 |
| Alberta (Edmonton CMA) | 3.73 |
| Alberta (Other) | 3.50 |
| Saskatchewan | 2.93 |
| Manitoba | 3.51 |
| Ontario (Toronto CMA) | 16.92 |
| Ontario (Other) | 21.79 |
| Quebec (Montreal CMA) | 11.57 |
| Quebec (Quebec City CMA) | 2.30 |
| Quebec (Other) | 9.22 |
| New-Brunswick | 2.16 |
| Nova Scotia | 2.71 |
| Prince Edward Island | 0.42 |
| Newfoundland | 1.44 |
| Education | Weight |
|---|---|
| Primary/Collegial | 72.33 |
| University – Rest of Canada | 21.81 |
| University - Quebec | 5.86 |
| Language by region | Weight |
|---|---|
| French - Rest of Canada | 2.45 |
| French - QC | 17.28 |
| Non-French - Rest of Canada | 74.47 |
| Non-French - QC | 5.81 |
| Presence of children in the household | Weight |
|---|---|
| Yes | 27.67 |
| No | 72.33 |
| Place of birth | Weight |
|---|---|
| Born in Canada | 78.10 |
| Born outside Canada | 21.90 |
| Ethnicity | Weight |
|---|---|
| Indigenous | 4.81 |
| Black | 3.45 |
| Other | 91.74 |
Appendix B: Survey questionnaire – WAVE 16.
[QLANG] Would you prefer to complete the survey in English or French?
Préféreriez-vous répondre à ce questionnaire en anglais ou en français?
Condition: not(QLANG.selected)
Row:
[english] English / Anglais
[french] Français / French
Thank you for agreeing to take part in this survey. We anticipate that the survey will take approximately 12 minutes to complete.
Background information
This research is being conducted by Léger Marketing, a Canadian public opinion research firm on behalf of Health Canada.
The purpose of this online survey is to collect opinions and feedback from Canadians that will be used by the Government of Canada to help inform government actions and decisions.
How does the online survey work? You are being asked to offer your opinions and experiences through an online survey. You have to be 18 or over in order to participate in this survey. We anticipate that the survey will take 12 minutes to complete. Your participation in the survey is completely voluntary, and you are able to withdraw at any time during the survey if you no longer wish to participate. Your responses are confidential and will only ever be reported in aggregate – never in any way that can identify any individual respondent or their responses. Your decision on whether or not to participate will not affect any dealings you may have with the Government of Canada. How is your personal information protected? The personal information you provide to Health Canada is governed in accordance with the Privacy Act and is being collected under the authority of section 4 of the Department of Health Act in accordance with the Treasury Board Directive on Privacy Practices. We only collect the information we need to conduct the research project. Why is your personal information collected?We require your personal information such as demographic information to better understand the topic of the research. However, your responses are always combined with the responses of others for analysis and reporting; you will never be identified. Your rights under the Privacy Act: In addition to protecting your personal information, the Privacy Act gives you the right to request access to and correction of your personal information. For more information about these rights, or about our privacy practices, please contact Health Canada's Privacy Coordinator at 613-948-1219 or privacy-vie.privee@hc-sc.gc.ca. You also have the right to file a complaint with the Privacy Commissioner of Canada if you think your personal information has been handled improperly.
If you are experiencing technical issues while responding to the survey, please contact Leger's technical support team at support@legeropinion.com.
Your help is greatly appreciated, and we look forward to receiving your feedback.
[GDR] What is your gender identity?
Gender refers to current gender which may be different from sex assigned at birth and may be different from what is indicated on legal documents.
Row:
[r1] Male
[r2] Female
[r96] Other
[r99] I prefer not to answer
[PROV] In which province or territory do you currently live?
Row:
[BC] British Columbia
[AB] Alberta
[SK] Saskatchewan
[MB] Manitoba
[ON] Ontario
[QC] Quebec
[NB] New Brunswick
[NS] Nova Scotia
[PE] Prince Edward Island
[NF] Newfoundland
[NT] Northwest Territories
[YK] Yukon
[NU] Nunavut
[YEAR] In what year and month were you born?
[MONTH] MONTH
Choice:
[ch1] January
[ch2] February
[ch3] March
[ch4] April
[ch5] May
[ch6] June
[ch7] July
[ch8] August
[ch9] September
[ch10] October
[ch11] November
[ch12] December
[AGE2] Would you be willing to indicate in which of the following age categories you belong?
Condition: (AGERef.r1)
Row:
[r0] Under 18
[r1] Between 18 and 24
[r2] Between 25 and 34
[r3] Between 35 and 44
[r4] Between 45 and 54
[r5] Between 55 and 64
[r6] 65 or older
[r9] I prefer not to answer
[ETHNIC] Do you identify as any of the following?
Select all that apply
Row:
[r1] White
[r2] Indigenous person (First Nations, Inuit or Métis)
[r3] South Asian
[r4] Chinese
[r5] Filipino
[r6] Southeast Asian
[r7] West Asian
[r8] Korean
[r9] Japanese
[r10] Black
[r11] Latin American
[r12] Arab
[r96] Other, please specify:
[r97] None of the above
[r99] Prefer not to answer
[CHILD] Are you the parent or guardian of a child or children under 18 years of age living in your household?
Row:
[r1] Yes
[r2] No
[r99] Prefer not to answer
[CHILD_AGE] How old is/are the child/children?
Condition: (CHILD.r1)
Select all that apply
Row:
[r1] Under 6 months of age
[r2] Between 6 months and LESS than 5 years of age
[r3] 5 to 11 years of age
[r4] 12 to 17 years of age
[r99] Prefer not to answer
[Q89] Have you ever been infected with COVID-19?
Row:
[r1] Yes
[r2] No
[r3] I think so (not confirmed by a positive test, PCR or rapid test)
[r98] Don't know
[r99] Prefer not to answer
[Q90] Do you know people in your immediate social network (i.e., friends or close family members) who have been infected with COVID-19?
Row:
[r1] Yes
[r2] No
[r3] I think so (not confirmed by a positive test, PCR or rapid test)
[r98] Don't know
[r99] Prefer not to answer
[Q130] Do you consider yourself to be at risk of more severe disease or outcomes from COVID-19 (e.g., are an older adult over age 60, are pregnant, have Down syndrome, have a chronic medical condition, are immunocompromised, or live with obesity, etc.)?
Row:
[r1] Yes
[r2] No
[r98] Unsure
[r99] Prefer not to answer
[Q1] What is your most pressing concern at this time?
Select only one.
Row:
[r1] Physical health
[r2] Mental health
[r3] Health of family and/or friends
[r5] Economy
[r7] Personal financial situation
[r8] Returning to normal and/or uncertainty about the future
[r9] New COVID-19 variants
[r10] Death of a family member and/or friend
[r11] Social isolation and/or loneliness
[r12] Workplace vaccination policy not being applied
[r13] Having to comply with the workplace vaccination policy
[r15] Easing or lifting of public health restrictions
[r16] New or emerging viruses other than COVID-19
[r96] Other, please specify:
[r97] I have no pressing concern
[r98] Don't know
[Q3C] How would you rate your overall mental health?
Row:
[r1] Very good
[r2] Good
[r3] Average
[r4] Bad
[r5] Very bad
[r98] Don't know
[Q108] Please indicate your level of agreement with the following statement: I feel I have adequate access to mental health support services.
Row:
[r1] Strongly agree
[r2] Agree
[r3] Neither agree nor disagree
[r4] Disagree
[r5] Strongly disagree
[r97] Unsure/ Not applicable
[Q4] In the past month, have you received any support for your mental health?
Row:
[r1] Yes
[r2] No
[r98] Don't know
[Q4B] What type of support have your received?
Condition: (Q4.r1)
Select all that apply.
Row:
[r1] Online/virtual support from support workers, social workers, psychologists or other professionals
[r2] In person support from support workers, social workers, psychologists or other professionals
[r3] Phone (including text) support
[r4] Resources and tips for taking care of yourself
[r5] Your primary health care provider
[r6] Resources and/or services through your local government
[r7] Resources and/or services through your provincial/territorial government
[r8] Resources and/or services through the Government of Canada
[r9] Through digital apps or platforms, like Wellness Together Canada
[r10] Support from local, or a non-for profit organization
[r96] Other, please specify:
[Q4C] What is the main reason why have you not received any support for your mental health?
Condition: (Q4.r2)
Row:
[r1] You preferred to manage yourself
[r2] You didn't know how or where to get this kind of help
[r3] You haven't gotten around to it (e.g., too busy)
[r4] Your job interfered (e.g., workload, hours of work or no cooperation from supervisor)
[r5] Access to care was limited (e.g., help was not readily available)
[r6] You didn't have confidence in the health care system or social services
[r7] You couldn't afford to pay
[r8] Insurance did not cover
[r9] You were afraid of what others would think of you
[r10] Language problems
[r11] You did not need support for your mental health
[r12] You felt the problem would go away on its own
[r13] You thought you could find your own resources instead of outside help
[r14] You feel your current day to day physical and mindful activities are enough to support your mental health (e.g., working out, walking, yoga, meditation, etc.)
[r96] Other, please specify:
[r98] Don't know
[Q10] When thinking about life after COVID-19, what makes you feel worried, if any?
Select all that apply
Row:
[r1] In-person interactions/socializing
[r2] Being in crowded places
[r3] Going back to the pre-pandemic routine
[r4] Giving up working from home
[r5] Not knowing if those around me are vaccinated
[r6] That we will never really end the COVID-19 pandemic
[r7] Confusion around public health measures
[r8] Being judged for wanting to wear a mask
[r9] Finding work
[r10] Being judged for being vaccinated
[r11] Accessing health care services
[r12] Being judged for not being vaccinated
[r13] Wearing a mask when others around me are not wearing one
[r14] Not wearing a mask when others around me are wearing one
[r15] Not knowing if those around me are vaccinated or are up to date with their vaccines
[r16] I am worried about a new pandemic
[r17] I am not worried about life after COVID-19
[r18] I am not worried about COVID-19 in general
[r96] Other, please specify
[Q131] To what extent do you agree with the following statements?
Column:
[c1] Strongly agree
[c2] Somewhat agree
[c3] Somewhat disagree
[c4] Strongly disagree
[c98] Don't know
Row:
[r1] You can catch COVID-19 multiple times
[r2] You can get COVID-19 even if vaccinated
[r3] You are less likely to get seriously ill from COVID-19 if you are vaccinated (e.g. not be hospitalized)
[r4] It is important to stay up to date with COVID-19 vaccinations
[r5] Staying up to date with COVID-19 vaccinations includes boosters
[r6] The immunity provided by a COVID-19 infection is short-lived and not as effective
[r7] Protection against COVID-19 is longer with vaccination and is more effective than immunity from infection
[Q132] How many doses of a COVID-19 vaccine have you received?
Row:
[r1] 1 dose
[r2] 2 doses
[r3] 3 doses
[r4] 4 doses
[r5] 5 doses
[r97] None, I am not vaccinated against COVID-19
[r98] Not sure
[Q132B] Have you received a COVID-19 booster dose?
Condition: not(Q132.r97)
Row:
[r1] Yes, received one booster dose
[r2] Yes, received two booster doses
[r3] Yes, received three booster doses
[r4] No, have not received a booster dose
[Q154] How likely are you to keep your COVID-19 doses up to date (i.e. continue to receive them as you become eligible for additional doses)?
Condition: (Q132.r1 or Q132.r2 or Q132.r3 or Q132.r4 or Q132.r5)
Row:
[r1] Very likely
[r2] Somewhat likely
[r3] Not very likely
[r4] Not at all likely
[r98] Don't know
[Q93] What is the top reason you are unlikely or uncertain about keeping your COVID-19 doses up to date?
Condition: (Q154.r3 or Q154.r4 or Q154.r98)
Row:
[r1] I think I am protected enough with the current number of vaccine doses
[r2] I had side effects with the dose/doses I already got
[r3] I'm concerned about how long it will take to get it
[r4] I'm concerned about the safety of the booster dose
[r5] I'm concerned about getting a different vaccine type than my previous doses
[r6] I'm concerned about the long-term effects of the vaccine
[r7] I need more information on booster doses
[r8] I prefer to wait a while before getting vaccinated
[r9] I'm fed up with getting vaccinated
[r10] I don't need a booster because the new variant is less severe, even if it is more contagious
[r11] I think those who are most vulnerable should get their booster dose first
[r12] I think we should help developing countries get fully vaccinated first
[r13] I do not see the need to get a booster because I've contracted COVID-19 after being vaccinated
[r14] I recently got COVID-19 and I don't know when to get the booster dose
[r15] I don't need a booster because I have natural immunity from having had COVID
[r16] I had short term non-serious side effects with the dose/doses I already got and don't want a booster because of this
[r17] I'm tired of being told what to do to protect my health
[r18] I recently had COVID-19 and need to wait the recommended time before getting my booster dose
[r19] I feel that the vaccine does not provide much protection as you can still get COVID-19 even if vaccinated
[r20] I am not exposed to risks of COVID-19 in my daily life and therefore feel that I do not need to receive a booster dose
[r21] I had long term side effects with the dose/doses I already got and don't want a booster because of this
[r22] Booster doses are not available in my area
[r96] Other, please specify:
[Q76] Amongst the following factors and thinking about the current COVID-19 context, what would motivate you to get your booster dose?
Condition: (Q132B.r4)
Please select up to your top 3
Row:
[r1] Advice from my primary health care provider that it is recommended for me
[r2] Required to be able to travel within Canada
[r3] Required to be able to travel internationally
[r4] Helping to get things back to normal
[r5] Being able to more safely spend time with friends and family in-person
[r6] Knowing that the majority of new COVID-19 cases are among those who have not received a booster
[r7] Knowing that the majority of new COVID-19 hospitalizations are among those who have not received a booster
[r8] Knowing that getting vaccinated could help protect the most vulnerable members of society
[r9] If getting boosted would make it more likely for my area to lift local public health restrictions (e.g. mandatory mask wearing, gathering limits, etc.)
[r10] Getting the vaccine at a convenient time and location
[r11] Receiving paid time off work to get a booster dose
[r12] A booster dose being made mandatory for all Canadians
[r13] Understanding the benefits and importance of booster doses
[r14] New COVID-19 vaccine formulations that are specific to latest variants
[r97] None of the above
[Q133] If recommended, how likely would you be to get a COVID-19 vaccine at the same time as a flu shot?
Condition: (Q154.r1 or Q154.r2)
Row:
[r1] Very likely
[r2] Somewhat likely
[r3] Not very likely
[r4] Not at all likely
[r5] I do not intend to get a flu shot
[r98] Don't know
[Q134] If COVID-19 vaccines were offered as a routine vaccine (e.g. annually), how likely would you be to get one?
Row:
[r1] Very likely
[r2] Somewhat likely
[r3] Not very likely
[r4] Not at all likely
[r98] Don't know
[Q134B] What is the top reason you are unlikely or uncertain about getting a routine COVID-19 vaccine?
Condition: (Q134.r3 or Q134.r4 or Q134.r98)
Row:
[r1] I think I am protected enough with the doses I already received
[r2] I had side effects with the dose/doses I already got
[r3] I think I am protected enough because I had COVID-19
[r4] I'm concerned about the safety of getting so many COVID-19 vaccines
[r5] I think I am protected enough because I was vaccinated AND I had COVID-19
[r6] I'm concerned about the long-term effects of the vaccine
[r7] I need more information on annual doses (e.g. why they are needed, benefits, safety, effectiveness, etc.)
[r8] I'm fed up with getting vaccinated
[r9] I don't think the vaccine is effective enough against the spread of COVID-19
[r10] I don't think the vaccine provides enough protection against severe outcomes from COVID-19
[r11] I don't think COVID-19 infection is serious enough anymore to need a routine COVID-19 vaccine (e.g. annually)
[r96] Other, please specify:
[Q135] Thinking about your child(ren) aged 12-17, how many doses of a COVID-19 vaccine have they received?
Condition: (CHILD_AGE.r4)
Select all that apply
Row:
[r1] 1 dose
[r2] 2 doses
[r3] 3 doses
[r7] 4 doses
[r4] None. I will wait a bit before getting my child(ren) vaccinated
[r5] None. I will not get my child(ren) vaccinated
[r6] Not sure
[Q95] Thinking about your child(ren) aged 12-17, how likely are you to have them receive a booster dose of the COVID-19 vaccine?
Condition: (Q135.r1 or Q135.r2)
Row:
[r1] Very likely
[r2] Somewhat likely
[r3] Not very likely
[r4] Not at all likely
[r5] My child(ren) 12-17 has/have already received a booster dose
[r98] Don't know
[Q136] Thinking about your child(ren) aged 5-11, how many doses of a COVID-19 vaccine have they received?
Condition: (CHILD_AGE.r3)
Select all that apply
Row:
[r1] 1 dose
[r2] 2 doses
[r3] 3 doses
[r4] None. I will wait a bit before getting my child(ren) vaccinated
[r5] None. I will not get my child(ren) vaccinated
[r6] Not sure
[Q136B] Thinking about your child(ren) aged 5-11, now that a booster has been authorized for them how likely are you to have them receive one?
Condition: (Q136.r1 or Q136.r2 or Q136.r6)
Row:
[r1] Very likely
[r2] Somewhat likely
[r3] Not very likely
[r4] Not at all likely
[r5] My child(ren) 5-11 has/have already received a booster dose
[r98] Don't know
[Q110] Why are you not likely or not sure to have your child(ren) get a booster dose of a COVID-19 vaccine?
Condition: (Q95.r3 or Q95.r4 or Q95.r98) or (Q136B.r3 or Q136B.r4 or Q136B.r98)
Select up to 3 reasons.
Row:
[r1] I think they are protected enough with the current dose schedule
[r2] They had side effects with the dose/doses they already got
[r3] I'm concerned about how long it will take to get it
[r4] I'm concerned about the safety of the booster dose
[r5] I'm concerned about the long-term effects of the vaccine
[r6] I need more information on booster doses
[r7] I prefer to wait a while before getting vaccinated
[r15] I'm confused about when they should get a booster
[r8] I'm fed up with getting my children vaccinated
[r9] They don't need a booster because the new variants are becoming less severe
[r10] I think those who are most vulnerable should get their booster dose first
[r11] I think we should help developing countries get fully vaccinated first
[r12] I do not see the need to get a booster because my child(ren) have already contracted COVID-19 after being vaccinated
[r13] They recently got COVID-19 and I don't know when to get their booster dose
[r16] I think adolescents have stronger immunity that protects them
[r14] My child is very anxious or fearful of vaccinations
[r96] Other, please specify:
[Q98B] Thinking about your child(ren) between the ages of 6 months and under 5, have they received at least one dose of a COVID-19 vaccine?
Condition: (CHILD_AGE.r2)
Select all that apply.
Row:
[r1] Yes
[r2] No, I will wait a bit before getting my child(ren) vaccinated
[r3] No, I will not get my child(ren) vaccinated
[r98] Not sure
[Q28] Which of the following factors would make you more likely to vaccinate your child(ren) against COVID-19?
Condition: (Q98B.r2 or Q98B.r3 or Q98B.r98)
Please choose your top three.
Row:
[r1] Assurance from my health professional that the vaccines are safe for my children
[r2] More information on the COVID-19 vaccine clinical trials involving children, including data on safety and effectiveness
[r3] Vaccinating my child(ren) would contribute to the collective benefit of ending the pandemic
[r4] Health Canada announces the vaccine is safe for kids and shares details of their findings from reviewing clinical trials
[r5] International health organizations say the vaccine is safe for kids based on findings from testing around the world
[r6] Being able to get my child vaccinated at a convenient location in my community
[r7] Assurance that I can be with my child(ren) during the vaccination
[r8] Encouragement from my child's school or school board that parents vaccinate their children
[r9] Seeing or hearing about friends, family or others I know personally getting their child(ren) vaccinated
[r10] Understanding the benefits of vaccinating children
[r11] Seeing or hearing about people that are "like" my child(ren) (i.e., similar age, health status, ethnicity, etc.) getting safely vaccinated
[r12] Getting more information about COVID cases and hospitalizations among children
[r13] My child(ren) can return to activities and socialization that they miss and need
[r14] My child(ren)'s mental health has suffered during the pandemic and I want them to get their regular lives back
[r15] Nothing would make me more likely to vaccinate my child(ren) against COVID-19
[r16] Receiving a financial incentive
[r17] If there was a financial penalty for not being vaccinated
[r18] More information on the potential long-term effects of my children being infected with COVID-19
[r19] More information on children who have received the COVID-19 vaccine, e.g. from clinical trials involving children or from real world use, including data on safety and effectiveness
[r20] International health organizations say the vaccine is safe for kids based on findings from testing around the world
[r21] More information on the benefits of vaccinating children, i.e. protection from severe illness and long COVID
[r22] More information on how vaccines work and build immunity in children
[r23] Getting more information about risks to children from COVID-19 (e.g. "Long COVID") and hospitalizations
[r24] Information about best timing of another dose, based on the risk in my community
[r25] If there is a COVID-19 outbreak in my child (children)'s school
[r96] Other, please specify:
[r98] Don't know
[Q111] Have any of your child's regular childhood vaccinations been missed/delayed as a result of the pandemic?
Condition: (CHILD.r1)
Childhood vaccinations are defined as routine vaccines given in childhood to protect against serious diseases such as diphtheria, tetanus, pertussis (whooping cough), polio, Haemophilus influenzae type B (Hib), rotavirus, hepatitis B, measles, mumps, rubella, chickenpox, pneumococcal and meningococcal diseases, and human papillomavirus virus (HPV).
Row:
[r1] Yes
[r2] No
[r98] Don't know
[Q112] Do you intend to catch up on your child's missed/delayed regular childhood vaccinations?
Condition: (Q111.r1)
Row:
[r1] Yes
[r2] No
[r98] Don't know
[Q137] Why do you not plan for your children to get the recommended childhood vaccines?
Condition: (Q112.r2)
Row:
[r1] I am concerned about potential side effects from the vaccine
[r2] I am concerned about the long-term effects of the vaccine
[r3] I believe that children have strong immune systems and do not need vaccines
[r4] I do not think the diseases they protect against are common in Canada
[r5] I do not think the diseases they protect against are serious enough to warrant vaccination
[r6] I do not want my child(ren) to receive any more vaccines
[r7] I had not planned for my child(ren) to get the recommended childhood vaccines
[r8] I do not believe that vaccines work
[r9] The COVID-19 pandemic and related vaccines have changed my views on vaccines
[r96] Other, please specify:
[Q138] Adult routine vaccinations are defined as routine vaccines and/or boosters given in adulthood to protect against serious diseases such as shingles (recommended for 50+), tetanus, pertussis (whooping cough), influenza (flu) and pneumococcal (recommended for 18+ with chronic medical conditions and healthy adults aged 65+).
Have you missed/delayed any routine vaccinations as a result of the pandemic?
Row:
[r1] Yes
[r2] No
[r3] I don't think this is applicable to me
[r98] Don't know
[Q139] Do you intend to catch up on your missed/delayed routine vaccinations?
Condition: (Q138.r1)
Row:
[r1] Yes
[r2] No
[r98] Don't know
[Q140] Why do you not intend to catch up on your missed/delayed routine vaccinations?
Condition: (Q139.r2)
Row:
[r1] I am concerned about potential side effects from vaccines
[r2] I am concerned about the long-term effects of vaccines
[r3] I do not think the diseases they protect against are common in Canada
[r4] I do not think the diseases they protect against are serious enough to warrant vaccination
[r5] Do not want to receive any more vaccines
[r6] Belief that immune system is strong without vaccines
[r7] I do not believe that vaccines work
[r8] The COVID-19 pandemic and related vaccines have changed my views on vaccines
[r96] Other, please specify:
[Q142] Has the recent COVID-19 pandemic had an impact on your confidence in vaccinations in general?
Row:
[r1] I am a lot less confident now
[r2] I am somewhat less confident now
[r3] About the same as before
[r4] Somewhat more confident now
[r5] A lot more confident now
[r98] I don't know
[Q143] Why are you less confident in vaccinations?
Condition: (Q142.r1 or Q142.r2)
Select all that apply
Row:
[r1] COVID-19 vaccines have negatively impacted my view on vaccines in general
[r2] I have more concerns about the safety of vaccines in general
[r3] I now believe that vaccines do not have as much benefit in preventing severe outcomes
[r4] I now believe that vaccines in general does not have as much benefit in stopping the spread of viruses
[r5] The COVID-19 pandemic has shown that we have strong immune systems without vaccines
[r6] The COVID-19 pandemic has shown that vaccines do not work very well
[r96] Other:
[Q144] Do you intend to get the flu vaccine this year?
Row:
[r1] Yes
[r2] No
[r98] Don't know
[Q145] Why do you not intend to get your flu shot this year?
Condition: (Q144.r2 or Q144.r98)
Select all that apply
Row:
[r1] I have never gotten a seasonal flu shot before
[r2] I am healthy, and/or never get the flu
[r3] Getting the flu doesn't make me that sick
[r4] I have concerns about the flu shot, and/or its side effects
[r5] The flu vaccine does not work
[r6] I have concerns about interactions with the COVID-19 vaccines
[r7] No one got the flu last year
[r8] I've had enough vaccines this year
[r9] I'm not eligible for the flu shot in my area
[r10] I feel I am protected from immunity as I had the flu this year
[r11] I had side effects the last time I received the flu shot
[r12] I had side effects the last time I received a vaccine other than the flu shot
[r13] Physical distancing, frequent handwashing and wearing a mask are enough to protect me from the flu
[r96] Other, please specify:
[r14] No specific reason, I just won't get it
[Q1B] How often do you follow each of the following public health measures?
Individual public health measures are actions you can use every day to help reduce the spread of COVID-19 and other respiratory infectious diseases. These measures are also sometimes referred to as personal preventive practices. Examples include: wearing a well-fitting respirator or mask, staying home when sick, improving indoor ventilation, practising respiratory etiquette and hand hygiene and cleaning and disinfecting high-touch surfaces and objects.
NOTE: In any questions below that refer to masks, the word mask refers to a non-medical mask, medical mask or respirator (eg: N95 or KN95).
Column:
[c1] Always
[c2] Often
[c3] Sometimes
[c4] Rarely
[c97] Never
[c98] Don't know/Not applicable
Row:
[r1] Washing hands for at least 20 seconds with soap and warm water
[r2] Using hand sanitizer containing at least 60% alcohol, if soap and water aren't available
[r3] Staying home and away from others if you feel sick
[r4] Practising physical distancing
[r5] Limiting the number of people you have contact with outside of your household
[r6] Avoiding closed spaces and crowded places
[r7] Wearing a mask–when indoors in a public space or in an indoor space with people from outside your immediate household
[r8] Wearing a mask– when outside in a public space
[r9] Improving ventilation when people from outside your immediate household are in your home (as examples: open windows and doors regularly, use a heating, ventilation and air conditioning (HVAC) system or run kitchen or bathroom exhaust fans)
[r10] Using individual public health measures when interacting with someone who is at risk of more severe disease or outcomes from COVID-19 (e.g., are an older adult over age 60, are pregnant, have Down syndrome, have a chronic medical condition, are immunocompromised, or live with obesity etc.)
[r11] Wearing a mask – inside with others when you're feeling sick
[Q115] Many individual public health measures (e.g., staying home when sick, handwashing, wearing a mask) were recommended in 2020 to help control the spread of COVID-19. How much do you think these individual public health measures could help reduce the spread of other respiratory infectious diseases, such as seasonal influenza (the flu)?
Row:
[r1] A great deal
[r2] Somewhat
[r3] Not very much
[r4] Not at all
[r98] Don't know
[Q146] What is the top reason you rarely or never practise any individual public health measures to reduce the spread of other respiratory diseases?
Condition: (Q1B.r1.c4 or Q1B.r1.c97) or (Q1B.r2.c4 or Q1B.r2.c97) or (Q1B.r3.c4 or Q1B.r3.c97) or (Q1B.r4.c4 or Q1B.r4.c97) or (Q1B.r5.c4 or Q1B.r5.c97) or (Q1B.r6.c4 or Q1B.r6.c97) or (Q1B.r7.c4 or Q1B.r7.c97) or (Q1B.r8.c4 or Q1B.r8.c97) or (Q1B.r9.c4 or Q1B.r9.c97) or (Q1B.r10.c4 or Q1B.r10.c97) or (Q1B.r11.c4 or Q1B.r11.c97)
Row:
[r1] I don't think it helps reduce the spread of other respiratory diseases
[r2] I am okay with getting other respiratory diseases
[r3] I want to build acquired immunity by being infected with other respiratory diseases
[r4] The individual public health measures cause too much disruption in my life
[r5] I don't want to have others criticize or ridicule me for practising individual public health measures
[r98] Don't know
[r96] Other, please specify:
[Q147] How confident, if at all, do you feel about making your own decisions with respect to choosing to practise any or all of the individual public health measures mentioned in the previous questions (i.e. wearing a mask, staying home when sick, hand hygiene, etc)?
Row:
[r1] Very confident
[r2] Somewhat confident
[r3] A little confident
[r4] Not confident at all
[r98] I don't know
[Q148] Which of the following would be useful to help your decision-making about using any or all of the individual public health measures mentioned in the previous question (i.e. wearing a mask, staying home when sick, hand hygiene, etc)?
Select all that apply.
Row:
[r1] Information about potential risks to myself personally (i.e. infection, severe illness, etc.)
[r2] Information on the effectiveness of individual public health measures
[r3] Information on the spread of COVID-19 in my community
[r4] Information on the spread of a cold, flu or other respiratory illness going around in my community
[r5] If I knew of a family member or friend who became seriously ill from COVID-19
[r6] Clear communications from the government/public health officials on when and which individual public health measures should be used
[r96] Other, please specify:
[r98] Don't know
[Q149] Where would you go for these types of information?
Condition: (Q148.r1 or Q148.r2 or Q148.r3 or Q148.r4)
Select all that apply.
Row:
[r1] Conversations with family/friends/colleagues
[r2] Conversations with a health care provider
[r3] Government of Canada websites
[r4] Provincial/territorial government websites
[r5] Provincial/territorial public health authorities
[r6] Local or regional health authorities
[r7] Federal public health authorities
[r8] Non-Canadian health authorities, e.g. the CDC, WHO
[r9] Social media
[r10] Your workplace
[r11] Media outlets/news
[r96] Other sources, please specify:
[r98] Don't know
[Q150] To what extent do you feel pressured by others to practise or not practice individual public health measures?
Row:
[r1] A lot
[r2] Somewhat
[r3] A little
[r4] Not at all
[r98] Don't know
[Q151] How familiar are you with the potential long-term effects of having COVID-19 (also known as "long-COVID" or "post COVID-19 condition")?
Row:
[r1] Very familiar
[r2] Somewhat familiar
[r3] Not very familiar
[r4] Not at all familiar
[r98] Don't know
[Q152] How worried are you/would you be about developing longer-term symptoms from a COVID-19 infection?
Row:
[r1] Very worried
[r2] Somewhat worried
[r3] Not very worried
[r4] Not at all worried
[r98] Don't know
[Q153] What makes/would make you feel worried about long-term symptoms of COVID?
Condition: (Q152.r1 or Q152.r2)
Select all that apply.
Row:
[r1] Limitations to my working life
[r2] Limitations to my leisure/personal life
[r3] Uncertainty about my future health prospects
[r4] Being judged for my condition
[r5] Not knowing if others (friends, colleagues, employers, healthcare providers, etc.) will take my condition seriously
[r6] Difficulty in formally indicating my condition to employers, healthcare providers, and/or others
[r7] Difficulty in accessing benefits related to my condition (e.g. sick leave, disability)
[r8] Being terminated by my employer for my condition
[r9] Lack of information/resources on my condition
[r10] Lack of public acknowledgement from authority figures (government, etc.) on my condition
[r96] Other, please specify:
The last few questions are strictly for statistical purposes. All of your answers are completely confidential.
[LANGU] What is the language you first learned at home as a child and still understand?
Row:
[r1] English
[r2] French
[r96] Other
[r99] I prefer not to answer
[MINO] Do you identify as any of the following?
SELECT ALL THAT APPLY
Row:
[r3] A member of the LGBTQ2 community
[r4] A person with a disability
[r97] None of the above
[r99] I prefer not to answer
[IMM] Where were you born?
Row:
[r1] Born in Canada
[r2] Born outside Canada
[r99] I prefer not to answer
[YIMM] In what year did you move to Canada?
Condition: (IMM.r2)
[MainAutoCountry] What is your country of origin?
Condition: (IMM.r2)
[PAYS] What is your country of origin?
Condition: IMM.r2 and not(MainAutoCountry.r99)
[SCOL] What is the highest level of formal education that you have completed?
Select one only
Row:
[r1] Some high school or less
[r2] High school diploma or equivalent
[r3] Registered Apprenticeship or other trades certificate or diploma
[r4] College, CEGEP or other non-university certificate or diploma
[r5] University certificate or diploma below bachelor's level
[r6] Bachelor's degree
[r7] Postgraduate degree above bachelor's level
[r99] I prefer not to answer
[OCCUP] Which of the following categories best describes your current employment status? Are you...
Select one only
Row:
[r1] Working full-time (35 or more hours per week)
[r2] Working part-time (less than 35 hours per week)
[r3] Self-employed
[r4] Unemployed, but looking for work
[r5] A student attending school full-time
[r6] Retired
[r7] Not in the workforce (full-time homemaker, full-time parent, or unemployed and not looking for work)
[r96] Other employment status. Please specify.
[r99] I prefer not to answer
[REVEN] Which of the following categories best describes your total household income? That is, the total income of all persons in your household combined, before taxes?
Select one only
Row:
[r1] Under $20,000
[r2] Between $20,000 and under $40,000
[r3] Between $40,000 and under $60,000
[r4] Between $60,000 and under $80,000
[r5] Between $80,000 and under $100,000
[r6] Between $100,000 and under $150,000
[r7] $150,000 and above
[r99] I prefer not to answer
[HH_SIZE] How many people, including yourself, are supported by your total household income?
[FSA] Please indicate the first 3 characters of your postal code.
If you would rather not provide it, please select I don't know/I prefer not to answer
Appendix C: Screening guide – WAVE 17.
Project description
The groups will be held online via CMNTY.
8 groups in total: three groups in French (3): Quebec and New-Brunswick and five (5) group in English: Ontario, BC, Prairies, Atlantic and territories.
The objective is to have 8-10 participants per focus group (recruits 12 per group).
| Date / Time | Participants | |
|---|---|---|
| GROUP 1 8-10 participants |
September 26, 2022, 5pm | Group with Young adults (18-35) who received two doses of a COVID-19 vaccine (English, Ontario and Atlantic provinces)
|
| GROUP 2 8-10 participants |
September 26, 2022, 7pm | Group with Young adults (18-35) who received two doses of a COVID-19 vaccine (English, BC, Prairies, Territories)
|
| GROUP 3 8-10 participants |
September 26, 2022, 5pm | Group with Young adults (18-35) who received two doses of a COVID-19 vaccine (French, Qc, NB)
|
| GROUP 4 8-10 participants |
September 27, 2022, 5pm | General population, who received three doses of a COVID-19 vaccine or more (English, BC, Prairies, Territories)
|
| GROUP 5 8-10 participants |
September 27, 2022, 7pm | General population, who received three doses of a COVID-19 vaccine or more (English, Ontario and Atlantic provinces)
|
| GROUP 6 8-10 participants |
September 26, 2022, 7pm | General population, who received three doses of a COVID-19 vaccine or more (French, Qc, NB)
|
| GROUP 7 8-10 participants |
September 28, 2022, 5pm | Vaccinated parents (with a mix of unvaccinated and vaccinated children) (English, BC, Prairies, Ontario)
|
| GROUP 8 8-10 participants |
September 27, 2022, 5pm | Vaccinated parents (with a mix of unvaccinated and vaccinated children) (French, Qc, NB)
|
Indigenous participants, participants from different ethnic communities and participants from the LGBTQ2 community will be recruited. There will be at least one participant from a different ethnic community in each group.
For each participant, collect the following information:
Participant name:
Phone number at home:
Cell phone:
Email address:
Recruitment date: Recruiter :
Group #:
Confirmation (date):
Introduction
Hello/Bonjour, I'm ___________ of Leger, a marketing research company. We are organizing a research project on behalf of Health Canada. The research's objective is to collect opinions and feedback from Canadians that will be used by Health Canada to understand Canadians' behaviours and attitudes with respect to COVID-19.
We are preparing to hold a few research sessions with people like yourself. Participation is completely voluntary. We are interested in your opinions. The format is an "online" discussion led by a research professional with up to ten participants. All opinions will remain anonymous and will be used for research purposes only in accordance with laws designed to protect your privacy. You don't need to be an expert to participate. We don't have anything to sell and we don't advertise and it's not an opinion poll on current events or politics. We are organizing several of these discussions. We would be interested in possibly having you participate.
Your participation is voluntary. All information collected, used and/or disclosed will be used for research purposes only and the research is entirely confidential. We are also committed to protecting the privacy of all participants. The names of the participants will not be provided to any third party. May I continue?
[INTERVIEWER NOTE: IF ASKED ABOUT PRIVACY LAWS, SAY: "The information collected through the research is subject to the provisions of the Privacy Act, the legislation of the Government of Canada, and to the provisions of relevant provincial privacy legislation.]
The focus group would take place online on the (INSERT DATE/TIME) and will be a maximum of 2 hours. You will be compensated $135 for your time.
I repeat that participation is entirely voluntary, and all information you provide is completely confidential. The full names of participants will not be provided to any third party.
A1. Are you interested in participating?
| Yes | 1 | Continue |
|---|---|---|
| No | 2 | Thank and conclude |
I would now like to ask you a few questions to see if you meet our eligibility criteria to participate.
When you conclude, say: Thank you for your cooperation. We have already reached the number of participants with a profile similar to yours. Therefore, we cannot invite you to participate.
A2. The group discussions we are organizing are going to be held over the Internet. They are going to be "online focus groups". Participants will need to have a computer, a high-speed Internet connection, and a WebCam in order to participate in the group. Would you be able to participate under these conditions?
| Yes | 1 | Continue |
|---|---|---|
| No | 2 | Thank and conclude |
Profiling
INTRO1.
Do you or anyone in your immediate family work or have you ever worked in...?
| Marketing Research | 1 Thank and conclude |
|---|---|
| Marketing and Advertising | 2 Thank and conclude |
| Public relations, communications | 3 Thank and conclude |
| Media (newspapers, television, radio, etc.) | 4 Thank and conclude |
| Telecommunications | 5 Thank and conclude |
| The federal or provincial government department or agency | 6 Thank and conclude |
| None of the above | 9 |
Gender
Please indicate the gender of the person.
| Male | 1 |
|---|---|
| Female | 2 |
| Other | 3 |
Gender: Ensure a good mix during the recruitment, Other is not a screening criteria
Province
In which province or territory do you live?
| British Columbia | 1 |
|---|---|
| Alberta | 2 |
| Saskatchewan | 3 |
| Manitoba | 4 |
| Ontario | 5 |
| Quebec | 6 |
| New Brunswick | 7 |
| Nova Scotia | 8 |
| Prince Edward Island | 9 |
| Newfoundland | 10 |
| Northwest Territories | 11 |
| Yukon | 12 |
| Nunavut | 13 |
Area
Which of the following best describes the area in which you live?
| Urban area | 1 |
|---|---|
| Rural area | 2 |
Ensure a good mix during the recruitment
Language
What is your first official language spoken?
Note for recruiter if respondent asks: In Canada, 'first official language spoken' is specified within the framework of the Official Languages Act. It refers to the first official language (i.e., English or French) that is spoken by an individual.
| French | 1 |
|---|---|
| English | 2 |
LANGU2
Do you speak any other languages?
| Yes (please specify) | 1 |
|---|---|
| No | 2 |
AGE.
What age category do you fall into?
| 18 to 25 | 1 |
|---|---|
| 26 to 35 | 2 |
| 36 to 45 | 3 |
| 46 to 55 | 4 |
| 56 to 65 | 5 |
| Over 65 years old | 6 |
| Groupe 1,2 and 3 should be 18-35 only. | |
MINO
Do you identify as any of the following?
| Yes | No | Prefer not to answer | |
|---|---|---|---|
| A member of the LGBTQ2 community | - | - | - |
| A person with a disability | - | - | - |
| A visible minority | - | - | - |
ETHN.
What is your ethnic origin?
| Caucasian (white) | 1 |
|---|---|
| Indigenous / First Nations | 2 |
| Latin American (Mexican, Chilean, Costa Rican, etc.) | 3 |
| Arabic (Middle East, North Africa) | 4 |
| Black (African, African-American, etc.) | 5 |
| South Asian (Indian, Bangladeshi, Pakistani, Sri Lankan, etc.) | 6 |
| Southeast Asian (Vietnamese, Cambodian, Malaysian, etc.) | 7 |
| West Asian (Iranian, Afghan, etc.) | 8 |
| Chinese | 9 |
| Filipino | 10 |
| Korean | 11 |
| Japanese | 12 |
| ETHN: There should be at least one participant from another ethnic community in each group. | |
VACC.
What is your vaccination status with respect to COVID-19?
| Three doses or more | 1 |
|---|---|
| Two doses | 2 |
| One dose | 3 Thank and conclude |
| I am not vaccinated | 4 Thank and conclude |
CHILD.
How many children under the age of 18 do you have?
| None | 1 Go to EDUCATION |
|---|---|
| [ ] enter number of child/children | Go to CHILDb |
CHILDB.
How many children do you have in the following age categories?
| Under 5 years old [ ] enter number of child/children | 1 Go to VACCB |
|---|---|
| 5 to 11 years old [ ] enter number of child/children | 2 Go to VACCB |
| 12 to 17 years old [ ] enter number of child/children | 3 Go to VACCB |
VACCB.
Thinking about your [child(ren) aged 12-17/child(ren) aged 5-11/Under 5 years old], have they received a COVID-19 vaccine?
| Yes, two doses or more | 1 |
|---|---|
| Yes, one dose | 2 |
| No, my child is not vaccinated | 3 |
If the participant has more than one child at childb, ask vaccb for each child
VACCB: For groups 7 and 8, ensure a good mix of parents who have had their children vaccinated and who have not had their children vaccinated
Ask to parents
VACC2.
Are your children/is your children up to date with their routine vaccinations?
If respondents asked about routine vaccination: Childhood vaccinations are defined as routine vaccines given in childhood to protect against serious diseases such as diphtheria, tetanus, pertussis (whooping cough), polio, Haemophilus influenza type B (Hib), rotavirus, hepatitis B, measles, mumps, rubella, chickenpox, pneumococcal and meningococcal diseases, and human papillomavirus virus (HPV).
| Yes | 1 |
|---|---|
| No | 2 |
| Not sure | 3 |
EDUCATION.
What is the highest level of education you completed?
| Some high school or less | 1 |
|---|---|
| High school diploma or equivalent | 2 |
| Registered Apprenticeship or other trades certificate or diploma | 3 |
| College, CEGEP or other non-university certificate or diploma | 4 |
| University certificate or diploma below bachelor's level | 5 |
| Bachelor's degree | 6 |
| Postgraduate degree above bachelor's level | 7 |
| Ensure a good mix for all groups if possible during the recruitment | |
OCCUP.
Which of the following categories best describes your current employment status? Are you…
| Working full-time (35 or more hours per week) | 1 |
|---|---|
| Working part-time (less than 35 hours per week) | 2 |
| Self-employed | 3 |
| Unemployed, but looking for work | 4 |
| A student attending school full-time | 5 |
| Retired | 6 |
| Not in the workforce (full-time homemaker, full-time parent, or unemployed and not looking for work) | - |
| Other employment status. Please specify. | - |
GROUP ATTRIBUTION
| If Province = 5-8-9-10-11 AND Language = 2 AND Age = 1-2 AND VACC=2 | Group #1 |
|---|---|
| If Province = 1-3-4-11-12-13 AND Language = 2 AND Age = 1-2 AND VACC=2 | Group #2 |
| If Province = 6 or 7 AND Language = 1 AND Age = 1-2 AND VACC=2 | Group #3 |
| If Province = 1-3-4-11-12-13 AND Language = 2 AND VACC=1 | Group #4 |
| If Province = 5-8-9-10-11 AND Language = 2 AND VACC=1 | Group #5 |
| If Province = 6 or 7 AND Language = 1 AND VACC=1 | Group #6 |
| If Province = 1, 3, 4 or 5 AND Language = 2 AND VACC=1-2 AND CHILD = yes Make sure there is a good mix of vaccinated and unvaccinated children (VACCB) | Group #7 |
| If Province = 6-7 AND Language = 1 AND VACC=1-2 AND CHILD = yes Make sure there is a good mix of vaccinated and unvaccinated children (VACCB) | Group #8 |
Also, make sure to have at least one participant from a different ethnic community in each group:
| IF ETHN=3,4,5,6,7,8,9,10,11,12 or 13= AND Language =2 | Group #1,2,4,5 or 7 |
|---|---|
| IF ETHN=3,4,5,6,7,8,9,10,11,12 or 13= AND Language =1 | Group #3, 6 or 8 |
AND try to have 3 indigenous participants distributed among the eight groups:
| IF ETHN=2 | Group #1-8 |
|---|
PSPC POR1
Have you ever attended a discussion group or taken part in an interview on any topic that was arranged in advance and for which you received money for participating?
| Yes | 1 |
|---|---|
| No | 2 Go to PSPC POR |
PSPC POR2
When did you last attend one of these discussion groups or interviews?
| Within the last 6 months | 1 Thank and conclude |
|---|---|
| Over 6 months ago | 2 |
PSPC POR 3
Thinking about the groups or interviews that you have taken part in, what were the main topics discussed?
RECORD: _______________ THANK/TERMINATE IF RELATED TO HEALTH, VACCINE OR COVID-19
PSPC POR4
| How many discussion groups or interviews have you attended in the past 5 years? Fewer than 5 | 1 |
|---|---|
| Five or more | 2 Thank and conclude |
Conclusion
Q1.
By participating in this focus group, you will be asked to discuss with other participants and share your opinion on various topics related to the COVID-19 pandemic, public health measure, and vaccines. Please note that you do not need to be an expert to participate. You may also be asked to read during the meeting.
How comfortable do you feel in such an environment?
Read the answer choices.
| Very comfortable | 1 |
|---|---|
| Somewhat comfortable | 2 |
| Not very comfortable | 3 Thank and conclude |
| Not at all comfortable | 4 Thank and conclude |
Invitation
Thank you. We'd like to invite you to participate in this focus group.
We are thrilled to have you as one of our participants in this study; your profile perfectly fits the target respondent we are looking for. We would like to invite you to participate in an online focus group that will be facilitated by an experienced professional moderator and will last approximately 120 minutes. The session will take place at [XX], on____XX____ (date/time) __XX__.
For your participation, you will receive a financial incentive of $135.
Please note that the session will be recorded. Your interview may also be observed by people who are directly working on the research study.
Just a quick reminder that the groups of discussion are going to be held over the Internet. They are going to be "online focus groups". You will need a computer, a high-speed Internet connection, and a WebCam in order to participate in the group.
INV1.
Are you still interested in participating in this research study?
| Yes | 1 |
|---|---|
| No | 2 Thank and conclude |
The information provided by you will be kept confidential and will only be disclosed to those who are directly working on the research that is relevant to the topic of discussion.
INV2.
Representatives from Health Canada may observe the discussion, but will not have access to any of your private information. You will be asked to sign a consent form in order to participate in this research. Would you be willing to do this?
| Yes | 1 |
|---|---|
| No | 2 Thank and conclude |
Privacy section
Now I have a few questions that relate to privacy, your personal information and the research process. We will need your consent on a few issues that enable us to conduct our research. As I run through these questions, please feel free to ask me any questions you would like clarified.
P1) First, we will provide the online platform and session moderator with a list of respondents' names and profiles (screener responses) so that they can sign you into the group. Do we have your permission to do this? I assure you it will be kept strictly confidential.
| Yes | 1 Go to P2 |
|---|---|
| No | 2 Read information below and P1A |
We need to provide the online platform and session moderator with the names and background of the people attending the focus group because only the individuals invited are allowed in the session and the facility and moderator must have this information for verification purposes. Please be assured that this information will be kept strictly confidential. GO TO P1A
P1a) Now that I've explained this, do I have your permission to provide your name and profiles to the online platform and moderator?
| Yes | 1 Go to P2 |
|---|---|
| No | 2 Thank and conclude |
P2) A recording of the group session will be produced for research purposes. The recording will only be used by the team of researchers at Léger to assist in preparing a report on the research findings.
Do you agree to be recorded for research purposes only?
| Yes | 1 Go to invitation |
|---|---|
| No | 2 Read information below and P2A |
It is necessary for the research process for us to record the session as the researcher needs this material to complete the report.
P2a) Now that I've explained this, do I have your permission for recording?
| Yes | 1 Go to INVITATION |
|---|---|
| No | 2 Thank and conclude |
As we are only inviting a small number of people to take part, your participation is very important to us. If for some reason you are unable to participate, please call so that we can get someone to replace you. You can reach us at ____ at our office. Please ask for ____.
To ensure that the focus groups run smoothly, we remind you:
- To make sure you are connected to the Internet and logged on 15 minutes in advance of the group
- To turn off your cellular phones – to avoid disruptions during the group.
- Make sure your WebCam is ON and functional
- To bring reading glasses, if necessary, to be able to go over the material.
- To make sure you will be located in a clear room (luminous)
- That the session will be recorded for analysis purposes only.
Email address:
Thank you very much for your assistance!
Contact information
Someone from our company will contact you to confirm the group. Could you leave me a phone number where we can reach you in the evening as well as during the day?
Name :
Phone number:
Cell phone:
Recruited by:
Confirmed by:
Appendix D: Discussion guide – WAVE 17.
A.3.1. General population groups
| BLOC 1 | Introduction and explanation |
|---|---|
| Length | 10 minutes |
Welcome and presentation
- Reception of participants
- Introduction of the moderator
- Presentation of Leger
Primary aim
- The research is being conducted by Léger Marketing on behalf of Health Canada. The objective of the meeting is to learn about your opinion and perception on different elements related to the COVID-19 pandemic to help inform government actions and decisions.
Rules of discussion
- Dynamics of the discussion (duration, discussion, round table)
- No wrong answers
- Importance of giving personal, spontaneous and honest opinions
- Importance of reacting respectfully to the opinions of others
- Importance of speaking one person at a time
Presentation of the group room
- Audio and video recording for subsequent analysis
- Presence of observers from the Government of Canada
- Presence of analyst to take notes
Results confidentiality
- The discussions we will have this evening will remain confidential at all times.
- Your name will never be mentioned in the report
- Information collected for study purposes only
Do you have any questions before we get started?
Introduction of participants
- What's your first name?
- Your place of residence (province and city)?
- What is your main occupation?
| BLOC 2 | Concerns about COVID-19 |
|---|---|
| Length | 10 minutes |
After more than two years of the pandemic, I would like to know…
What risks does COVID-19 represent for you today?
Do you think we are now out of the COVID-19 pandemic?
PROBE: why (or why not) do you think so?
Is the upcoming late Fall or winter season make you more worried about COVID-19?
PROBE: why or why not?
| BLOC 3 | PUBLIC health measures |
|---|---|
| Length | 25 minutes |
We will now discuss the public health measures.
Will you continue to use individual public health measures now that they are no longer mandatory in most places? Which one(s)?
(If needed, examples of individual PHM include mask wearing, staying home when you are sick, respiratory etiquette, cleaning and disinfecting, ventilation, etc.)
PROBE: If so why? Or why not?
Are there specific situations when you would use them?
(If needed, examples of situation include work, school, indoor or outdoor gathering, shopping, etc.)
Which ones do you feel offer the most protection against COVID-19?
Now thinking about wearing masks in particular…
When you think about masks and public health measures, do you think they are still important? Why/why not?
PROBE: Do you think masks protect you against other illnesses other than COVID-19?
Now thinking about ventilation in particular…
What does it mean to you to improve ventilation in your home or at your place of work?
Have you already put measures in place to improve ventilation? If so, which ones?
Do you think that improving ventilation decreases the risk of COVID-19 transmission? Why or why not??
| BLOC 4 | Influence of a COVID-19 Infection |
|---|---|
| Length | 20 minutes |
Were you infected with COVID-19 at one point or another during the pandemic? More than once? Did you test to confirm your infection?
If you've previously been infected with COVID-19, did that experience influence your decision to get additional doses of the COVID-19 vaccine (i.e., booster doses), or not?
PROBE: How did it influence your decision?
(i.e., if you felt that getting COVID wasn't "that bad", did it influence you not to seek further vaccine doses?)
| BLOC 5 | Vaccines |
|---|---|
| Length | 20 Minutes |
What does it mean to you to stay up to date with your COVID-19 vaccines?
PROBE: How important is it to do so?
What would encourage you stay up to date with your COVID-19 vaccines?
Health Canada recently approved an updated COVID-19 vaccine as a booster dose for adults 18 years and older. The updated booster is called a bivalent vaccine. It targets the original COVID-19 virus from 2019 and the Omicron variant of concern. What are your views on bivalent vaccines? What would make you consider getting one?
Have you heard of bivalent vaccines before today?
| BLOC 6 | Message Testing |
|---|---|
| Length | 20 minutes |
I will now present you with different messages that you might see on social media, in advertisements, online etc. regarding different topics related to COVID-19. After each set of messages, we will discuss your impressions.
Message A:
Stay up to date with your COVID-19 vaccines to help protect against severe outcomes. Get all booster doses recommended for you.
Message B:
Stay up to date with your COVID-19 vaccines to help protect against severe outcomes. Get all vaccine doses recommended for you.
Which one has a clearer message? Why?
Which one would motivate you to stay up to date with your COVID-19 vaccines?
How can we improve the messages to make them clearer and more "motivational" to stay up to date on COVID-19 vaccines? What words should be used?
What would you change in the messages?
When talking about COVID-19 vaccination, do you know what the term "Primary Series" means?
How can we make this term clearer?
Next messages:
Message D:
Consult your local health care resources, or provincial or territorial public health authority to find out when you're due for your next COVID-19 vaccine dose.
Message E:
Check with your province or territory to find out when you're due for your next COVID-19 vaccine dose.
Which one has a clearer message? What if it said "COVID-19 booster, instead of COVID-19 vaccine dose?"
Do you know how to find out COVID-19 vaccine information from your province or territory?
| BLOC 7 | Mental health |
|---|---|
| Length | 25 minutes |
What factors/stressors are currently affecting your mental health, if any?
Have there been times when you haven't sought support when you have struggled with your mental health?
PROBE: What were some of the reasons for not seeking support?
Who/where do you look for information about mental health support and/or services?
Examples if needed: where you can find mental health support; tips for how you can support and improve your mental health; real-life stories about mental health from people with lived experiences to reduce potential stigma related to this topic; awareness/education materials on mental health
Now thinking about online resources…
Are you aware of any free virtually-delivered mental health services?
(Examples if needed: tools/resources accessed online, digital mental health apps, online mental health platforms, text-based services, etc.)
PROBE: Which ones? (name or type) / How did you become aware of them?
Would you consider using online resources if you felt the need or would you recommend them to a friend or family member?
PROBE : Please explain why.
Would you be more likely to consider using/recommending them if initially recommended to you by a trusted source?
PROBE: What is a trusted source for you?
(Examples if needed: friends, family, colleagues, physician, nurses, online resources, etc.)
What type of information related to mental health would you like to see from the Government of Canada?
| BLOC 8 | Conclusion |
|---|---|
| Durée | 5 minutes |
Do you have any final comments you would like to add on the topics we just discussed?
Conclude and end the meeting.
Thank you very much for your precious collaboration!
A.3.2 Vaccinated parents Groups
| BLOC 1 | Introduction and explanation |
|---|---|
| Length | 10 minutes |
Welcome and presentation
- Reception of participants
- Introduction of the moderator
- Presentation of Leger
Primary aim
- The research is being conducted by Léger Marketing on behalf of Health Canada. The objective of the meeting is to learn about your opinion and perception on different elements related to the COVID-19 pandemic to help inform government actions and decisions.
Rules of discussion
- Dynamics of the discussion (duration, discussion, round table)
- No wrong answers
- Importance of giving personal, spontaneous and honest opinions
- Importance of reacting respectfully to the opinions of others
- Importance of speaking one person at a time
Presentation of the group room
- Audio and video recording for subsequent analysis
- Presence of observers from the Government of Canada
- Presence of analyst to take notes
Results confidentiality
- The discussions we will have this evening will remain confidential at all times.
- Your name will never be mentioned in the report
- Information collected for study purposes only
Do you have any questions before we get started?
Introduction of participants
- What's your first name?
- Your place of residence (province and city)?
- What is your main occupation?
| BLOC 2 | Concerns about COVID-19 |
|---|---|
| Length | 10 minutes |
After more than two years of the pandemic, I would like to know…
What risks does COVID-19 represent for you and your children today?
Is/are your child(ren) vaccinated against COVID-19? How many doses have they received?
Do you think we are now out of the COVID-19 pandemic?
PROBE: why (or why not) do you think so?
Is the upcoming winter season make you more worried about COVID-19?
PROBE: why or why not?
| BLOC 3 | PUBLIC health measures |
|---|---|
| Length | 25 minutes |
We will now discuss the public health measures.
Will you continue to use individual public health measures now that they are no longer mandatory in most places? Which one(s)?
(If needed, examples of individual PHM include mask wearing, staying home when you are sick, respiratory etiquette, cleaning and disinfecting, ventilation, etc.)
PROBE: If so, why? Or why not?
Which one(s), if any, will your child(ren) continue using in their everyday life?
Are there specific situations when you or your children would use them?
(If needed, examples of situation include work, school, indoor or outdoor gathering, shopping, etc.)
Which ones do you feel offer the most protection against COVID-19, for youself? What about for your children?
Now thinking about wearing masks in particular…
When your children go to school will you encourage them to wear a mask?
Do you think masks protect you against other illnesses other than COVID-19? What about your children?
Will you keep your children home from school when they are sick with any illness? (i.e. including a cold)
Now thinking about ventilation in particular…
What does it mean to you to improve ventilation in your home or at your place of work?
Have you already put measures in place to improve ventilation? If so, which ones?
Do you think that improving ventilation decreases the risk of COVID-19 transmission? Why or why not?
| BLOC 4 | Influence of a COVID-19 Infection |
|---|---|
| Length | 15 minutes |
Were you infected with COVID-19 at one point or another during the pandemic? Did your child(ren) get COVID? Were you or your child(ren) infected more than once? Did you confirm your COVID-19 infection with a test?
If you've previously been infected with COVID-19, did that experience influence your decision to get additional doses of the COVID-19 vaccine (i.e., booster doses), or not?
Did it influence your decision to vaccinate your child or not?
PROBE: How did it influence your decision?
(i.e., if you felt that getting COVID wasn't "that bad", did it influence you not to seek further vaccine doses?)
| BLOC 5 | Vaccines |
|---|---|
| Length | 15 minutes |
What does it mean to you to stay up to date with your child's COVID-19 vaccines?
PROBE: How important is it to do so?
What would encourage you stay up to date with your child's COVID-19 vaccines?
| BLOC 6 | Message Testing |
|---|---|
| Length | 25 minutes |
I will now present you with different messages that you might see on social media, in advertisements, online etc. regarding different topics related to COVID-19. After each set of messages, we will discuss your impressions.
Message A:
Vaccinating children against COVID-19 is beneficial for their health and well-being. Research shows that vaccinating children with a COVID-19 vaccine provides very good protection against serious illness, hospitalization and death from COVID-19.
What are your impressions of this message? Is it clear?
Would this message motivate you to get your child(ren) vaccinated?
How can we improve the message to make it clearer and more "motivational" to get your child(ren) vaccinated?
Message B:
While most children who get COVID-19 experience mild or no symptoms, some, including previously healthy children, can experience severe disease and require hospitalization. Fortunately, severe COVID-19 outcomes, including hospitalization, are lower in children who are vaccinated against COVID-19.
What are your impressions of this message? Is it clear?
Would this message motivate you to get your child(ren) vaccinated?
How can we improve the message to make it clearer and more "motivational" to get your child(ren) vaccinated?
Message C:
Even if a child has already had COVID-19, vaccination is still important. While infection alone provides some protection, vaccination combined with infection helps improve the immune response. Studies in adults show that vaccination following infection provides stronger and longer-lasting protection.
What are your impressions of this message? Is it clear?
Would this message motivate you to get your child(ren) vaccinated?
How can we improve the message to make it clearer and more "motivational" to get your child(ren) vaccinated?
Message D:
When talking about COVID-19 vaccination, do you know what the term "Primary Series" means?
How can we make this term clearer? Does understanding the term help you feel more informed about vaccines?
Message E:
Consult your local health care resources, or provincial or territorial public health authority to find out when you're due for your next COVID-19 vaccine dose.
Message F:
Check with your province or territory to find out when you're due for your next COVID-19 vaccine dose.
Which one has a clearer message? What if it said "COVID-19 booster, instead of COVID-19 vaccine dose?"
Do you know how to find out COVID-19 information from your province or territory?
Message G:
Stay up to date with your COVID-19 vaccines to help protect against severe outcomes. Get all booster doses recommended for you.
Message H:
Stay up to date with your COVID-19 vaccines to help protect against severe outcomes. Get all vaccine doses recommended for you.
Which one has a clearer message?
Which one would motivate you to get stay up to date with your COVID-19 vaccines? What words should be used?
How can we improve the messages to make them clearer and more "motivational" to stay up to date on COVID-19 vaccines?
| BLOC 7 | Mental health |
|---|---|
| Length | 25 minutes |
What factors/stressors are currently affecting your mental health, if any?
Have there been times when you haven't sought support when you have struggled with your mental health?
PROBE: What were some of the reasons for not seeking support?
Examples if needed: where you can find mental health support; tips for how you can support and improve your mental health; real-life stories about mental health from people with lived experiences to reduce potential stigma related to this topic; awareness/education materials on mental health
Now thinking about online resources…
Are you aware of any free virtually-delivered mental health services?
(Examples if needed: tools/resources accessed online, digital mental health apps, online mental health platforms, text-based services, etc.)
PROBE: Which ones? (name or type) / How did you become aware of them?
Would you consider using online resources (for your child(ren) or for you) if you felt the need or would you recommend them to a friend or family member?
PROBE: Please explain why.
(Examples if needed: friends, family, colleagues, physician, nurses, online resources, etc.)
Would you be more likely to consider using/recommending them if initially recommended to you by a trusted source?
PROBE: What is a trusted source for you?
What type of information related to mental health would you like to see from the Government of Canada?
| BLOC 8 | Conclusion |
|---|---|
| Durée | 5 minutes |
Do you have any final comments you would like to add on the topics we just discussed?
Conclude and end the meeting.
Thank you very much for your precious collaboration!
Appendix E: Survey questionnaire – WAVE 18.
[QLANG] Would you prefer to complete the survey in English or French?
Préféreriez-vous répondre à ce questionnaire en anglais ou en français?
Condition: not(QLANG.selected)
Row:
[english] English / Anglais
[french] Français / French
Thank you for agreeing to take part in this survey. We anticipate that the survey will take approximately 12 minutes to complete.
Background information
This research is being conducted by Léger Marketing, a Canadian public opinion research firm on behalf of Health Canada.
The purpose of this online survey is to collect opinions and feedback from Canadians that will be used by the Government of Canada to help inform government actions and decisions.
How does the online survey work? You are being asked to offer your opinions and experiences through an online survey. You have to be 18 or over in order to participate in this survey. We anticipate that the survey will take 12 minutes to complete. Your participation in the survey is completely voluntary, and you are able to withdraw at any time during the survey if you no longer wish to participate. Your responses are confidential and will only ever be reported in aggregate – never in any way that can identify any individual respondent or their responses. Your decision on whether or not to participate will not affect any dealings you may have with the Government of Canada. How is your personal information protected? The personal information you provide to Health Canada is governed in accordance with the Privacy Act and is being collected under the authority of section 4 of the Department of Health Act in accordance with the Treasury Board Directive on Privacy Practices. We only collect the information we need to conduct the research project. Why is your personal information collected?We require your personal information such as demographic information to better understand the topic of the research. However, your responses are always combined with the responses of others for analysis and reporting; you will never be identified. What are your rights under the Privacy Act: In addition to protecting your personal information, the Privacy Act gives you the right to request access to and correction of your personal information.
If you are experiencing technical issues while responding to the survey, please contact Leger's technical support team at support@legeropinion.com.
Your help is greatly appreciated, and we look forward to receiving your feedback.
[GDR] What is your gender identity?
Gender refers to current gender which may be different from sex assigned at birth and may be different from what is indicated on legal documents.
Row:
[r1] Male
[r2] Female
[r96] Other
[r99] I prefer not to answer
[PROV] In which province or territory do you currently live?
Row:
[BC] British Columbia
[AB] Alberta
[SK] Saskatchewan
[MB] Manitoba
[ON] Ontario
[QC] Quebec
[NB] New Brunswick
[NS] Nova Scotia
[PE] Prince Edward Island
[NF] Newfoundland
[NT] Northwest Territories
[YK] Yukon
[NU] Nunavut
[YEAR] In what year and month were you born?
[AGE2] Would you be willing to indicate in which of the following age categories you belong?
Condition: (AGERef.r1)
Row:
[r0] Under 18
[r1] Between 18 and 24
[r2] Between 25 and 34
[r3] Between 35 and 44
[r4] Between 45 and 54
[r5] Between 55 and 64
[r6] 65 or older
[r9] I prefer not to answer
[ETHNIC] Do you identify as any of the following?
Select all that apply
Row:
[r1] Black
[r2] East Asian
[r3] Indigenous (First Nations, Inuk/Inuit, Métis)
[r4] Latin American
[r5] Middle Eastern
[r6] South Asian
[r7] Southeast Asian
[r8] White
[r96] Other (please specify)
[r97] None of the above
[r99] Prefer not to answer
[CHILD] Are you the parent or guardian of a child or children under 18 years of age living in your household?
Row:
[r1] Yes
[r2] No
[r99] Prefer not to answer
[CHILD_AGE] How old is/are the child/children?
Condition: (CHILD.r1)
Select all that apply
Row:
[r1] Under 6 months of age
[r2] Between 6 months and LESS than 5 years of age
[r3] 5 to 11 years of age
[r4] 12 to 17 years of age
[r99] Prefer not to answer
[Q89] Have you ever been infected with COVID-19?
Row:
[r1] Yes
[r2] No
[r3] I think so (not confirmed by a positive test, PCR or rapid test)
[r98] Don't know
[r99] Prefer not to answer
[Q90] Do you know people in your immediate social network (i.e., friends or close family members) who have been infected with COVID-19?
Row:
[r1] Yes
[r2] No
[r3] I think so (not confirmed by a positive test, PCR or rapid test)
[r98] Don't know
[r99] Prefer not to answer
[Q130] Do you consider yourself to be at risk of more severe disease or outcomes from COVID-19 (e.g., are an older adult over age 60, are pregnant, have Down syndrome, have a chronic medical condition, are immunocompromised, or live with obesity, etc.)?
Row:
[r1] Yes
[r2] No
[r98] Unsure
[r99] Prefer not to answer
[Q155] How worried are you of becoming infected with COVID-19?
Row:
[r1] Very worried
[r2] Somewhat worried
[r3] A little worried
[r4] Not worried at all
[r98] Don't know
[Q156] Why are you not worried about becoming infected with COVID-19?
Condition: (Q155.r4 or Q155.r98)
Select all that apply.
Row:
[r1] I've contracted COVID-19 before and was not really sick
[r2] I've contracted COVID-19 before and know what to expect
[r3] I've contracted COVID-19, so I am immune
[r4] I am vaccinated, so I am immune
[r5] I am vaccinated so my symptoms would be mild
[r6] COVID-19 is not very dangerous
[r7] COVID-19 is just another flu
[r8] COVID-19 is here to stay
[r9] There are low levels of COVID-19 in my community
[r10] New variants of COVID-19 do not concern me
[r11] I have other, more important concerns.
[r96] Other (specify)
[r98] Don't know
[Q157] Why are you worried about becoming infected with COVID-19?
Condition: (Q155.r1 or Q155.r2 or Q155.r3)
Select all that apply.
Row:
[r1] I've contracted COVID-19 and was really sick (e.g. severely sick or hospitalized)
[r2] I am worried about getting really sick
[r3] I am worried about getting significant complications from COVID-19 (e.g. long COVID)
[r4] I am worried about getting others sick
[r5] I am worried it will impact my work
[r6] I am worried it will impact my plans (e.g. events, concerts, vacations etc.)
[r7] I am worried about new variants
[r96] Other (specify)
[r98] Don't know
[Q1] What is your most pressing concern at this time?
Select only one.
Row:
[r1] Physical health
[r2] Mental health
[r3] Health of family and/or friends
[r5] Economy
[r7] Personal financial situation
[r8] Returning to normal and/or uncertainty about the future
[r9] New COVID-19 variants
[r10] Death of a family member and/or friend
[r11] Social isolation and/or loneliness
[r12] Workplace vaccination policy not being applied
[r13] Having to comply with the workplace vaccination policy
[r15] Easing or lifting of public health restrictions
[r16] New or emerging viruses other than COVID-19
[r17] Work or school pressures
[r18] Relationships with family or friends
[r19] Current events
[r96] Other, please specify:
[r97] I have no pressing concern
[r98] Don't know
[Q3C] How would you rate your overall mental health?
Row:
[r1] Very good
[r2] Good
[r3] Average
[r4] Bad
[r5] Very bad
[r98] Don't know
[Q108] Please indicate your level of agreement with the following statement: I feel I have adequate access to mental health support services.
Condition: False
Row:
[r1] Strongly agree
[r2] Agree
[r3] Neither agree nor disagree
[r4] Disagree
[r5] Strongly disagree
[r97] Unsure/ Not applicable
[Q4] In the past month, have you received any support for your mental health?
Row:
[r1] Yes
[r2] No
[r98] Don't know
[Q4B] What type of support have your received?
Condition: (Q4.r1)
Select all that apply.
Row:
[r1] Online/virtual support from support workers, social workers, psychologists or other professionals
[r2] In person support from support workers, social workers, psychologists or other professionals
[r3] Phone (including text) support
[r4] Resources and tips for taking care of yourself
[r5] Your primary health care provider
[r6] Resources and/or services through your local government
[r7] Resources and/or services through your provincial/territorial government
[r8] Resources and/or services through the Government of Canada
[r9] Through digital apps or platforms, like Wellness Together Canada
[r10] Support from local, or a non-for profit organization
[r11] Employee assistance programs
[r12] Your faith or spiritual leaders
[r96] Other, please specify:
[Q4C] What is the main reason why have you not received any support for your mental health?
Condition: False
Row:
[r1] You preferred to manage yourself
[r2] You didn't know how or where to get this kind of help
[r3] You haven't gotten around to it (e.g., too busy)
[r4] Your job interfered (e.g., workload, hours of work or no cooperation from supervisor)
[r5] Access to care was limited (e.g., help was not readily available)
[r6] You didn't have confidence in the health care system or social services
[r7] You couldn't afford to pay
[r8] Insurance did not cover
[r9] You were afraid of what others would think of you
[r10] Language problems
[r11] You did not need support for your mental health
[r12] You felt the problem would go away on its own
[r13] You thought you could find your own resources instead of outside help
[r14] You feel your current day to day physical and mindful activities are enough to support your mental health (e.g., working out, walking, yoga, meditation, etc.)
[r96] Other, please specify:
[r98] Don't know
[Q10] When thinking about life after COVID-19, what makes you feel worried, if any?
Condition: False
Select all that apply
Row:
[r1] In-person interactions/socializing
[r2] Being in crowded places
[r3] Going back to the pre-pandemic routine
[r4] Giving up working from home
[r5] Not knowing if those around me are vaccinated
[r6] That we will never really end the COVID-19 pandemic
[r7] Confusion around public health measures
[r8] Being judged for wanting to wear a mask
[r9] Finding work
[r10] Being judged for being vaccinated
[r11] Accessing health care services
[r12] Being judged for not being vaccinated
[r13] Wearing a mask when others around me are not wearing one
[r14] Not wearing a mask when others around me are wearing one
[r15] Not knowing if those around me are vaccinated or are up to date with their vaccines
[r16] I am worried about a new pandemic
[r17] I am not worried about life after COVID-19
[r18] I am not worried about COVID-19 in general
[r96] Other, please specify
[Q158] To what extent do you agree or disagree with the following statements?
Column:
[c1] Strongly Agree
[c2] Somewhat Agree
[c3] Neither agree or disagree
[c4] Somewhat Disagree
[c5] Strongly disagree
[c6] Unsure / Not applicable
Row:
[r1] Mental health is interconnected with physical health, and central to overall health and well-being
[r2] I practice taking care of my mental health on a regular basis.
[r3] I have enough time to take care of my mental health.
[r4] I know when I need help with my mental health.
[r5] I think I can manage my mental health struggles on my own.
[r6] I am aware of free mental health and substance use resources online or by phone.
[r7] I feel I have adequate access to mental health support services.
[r8] It's hard to ask for help if I'm struggling with my mental health.
[r9] I know how or where to get help for my mental health.
[r10] I can afford mental health support.
[r11] I can afford to see a mental health therapist such as a social worker, psychologist, or counsellor.
[Q131] To what extent do you agree with the following statements?
Column:
[c1] Strongly agree
[c2] Somewhat agree
[c3] Somewhat disagree
[c4] Strongly disagree
[c98] Don't know
Row:
[r1] You can catch COVID-19 multiple times
[r2] You can get COVID-19 even if vaccinated
[r3] You are less likely to get seriously ill from COVID-19 if you are vaccinated (e.g. not be hospitalized)
[r4] It is important to stay up to date with COVID-19 vaccinations
[r5] Staying up to date with COVID-19 vaccinations includes boosters
[r6] The immunity provided by a COVID-19 infection is short-lived and not as effective
[r7] Protection against COVID-19 is longer with vaccination and is more effective than immunity from infection
[Q132] How many doses of a COVID-19 vaccine have you received?
Row:
[r1] 1 dose
[r2] 2 doses
[r3] 3 doses
[r4] 4 doses
[r5] 5 doses
[r97] None, I am not vaccinated against COVID-19
[r98] Not sure
[Q132B] Have you received a COVID-19 booster dose?
Condition: not(Q132.r97)
Row:
[r1] Yes, received one booster dose
[r2] Yes, received two booster doses
[r3] Yes, received three booster doses
[r4] No, have not received a booster dose
[Q159] When did you receive your most recent COVID-19 booster dose?
Condition: (Q132B.r1 or Q132B.r2 or Q132B.r3)
Row:
[r1] Less than 3 months ago
[r2] 3 – 6 months ago
[r3] 6 – months to a year ago
[r4] Over one year ago
[r5] I have not received a COVID-19 booster
[r98] Don't know
[Q154] How likely are you to keep your COVID-19 doses up to date (i.e. continue to receive them as you become eligible for additional doses)?
Condition: (Q132.r1 or Q132.r2 or Q132.r3 or Q132.r4 or Q132.r5)
Row:
[r1] Very likely
[r2] Somewhat likely
[r3] Not very likely
[r4] Not at all likely
[r98] Don't know
[Q93] What is the top reason you are unlikely or uncertain about keeping your COVID-19 doses up to date?
Condition: (Q154.r3 or Q154.r4 or Q154.r98)
Row:
[r1] I think I am protected enough with the current number of vaccine doses
[r2] I had side effects with the dose/doses I already got
[r3] I'm concerned about how long it will take to get it
[r4] I'm concerned about the safety of the booster dose
[r5] I'm concerned about getting a different vaccine type than my previous doses
[r6] I'm concerned about the long-term effects of the vaccine
[r7] I need more information on booster doses
[r8] I prefer to wait a while before getting vaccinated
[r9] I'm fed up with getting vaccinated
[r10] I don't need a booster because the new variant is less severe, even if it is more contagious
[r11] I think those who are most vulnerable should get their booster dose first
[r12] I think we should help developing countries get fully vaccinated first
[r13] I do not see the need to get a booster because I've contracted COVID-19 after being vaccinated
[r14] I recently got COVID-19 and I don't know when to get the booster dose
[r15] I don't need a booster because I have natural immunity from having had COVID
[r16] I had short term non-serious side effects with the dose/doses I already got and don't want a booster because of this
[r17] I'm tired of being told what to do to protect my health
[r18] I recently had COVID-19 and need to wait the recommended time before getting my booster dose
[r19] I feel that the vaccine does not provide much protection as you can still get COVID-19 even if vaccinated
[r20] I am not exposed to risks of COVID-19 in my daily life and therefore feel that I do not need to receive a booster dose
[r21] I had long term side effects with the dose/doses I already got and don't want a booster because of this
[r22] Booster doses are not available in my area
[r23] I think it is unlikely that I will get infected with COVID-19
[r96] Other, please specify:
[Q76] Among the following factors and thinking about the current COVID-19 situation, what would motivate you to get your booster dose?
Condition: (Q132B.r4)
Please select up to your top 3
Row:
[r1] Advice from my primary health care provider that it is recommended for me
[r2] Required to be able to travel within Canada
[r3] Required to be able to travel internationally
[r4] Helping to get things back to normal
[r5] Being able to more safely spend time with friends and family in-person
[r6] Knowing that the majority of new COVID-19 cases are among those who have not received a booster
[r7] Knowing that the majority of new COVID-19 hospitalizations are among those who have not received a booster
[r15] Knowing that family and friends and those in my community are getting vaccinated
[r16] Being able to get my flu shot and additional COVID-19 dose at the same time
[r8] Knowing that getting vaccinated could help protect the most vulnerable members of society
[r9] If getting boosted would make it more likely for my area to lift local public health restrictions (e.g. mandatory mask wearing, gathering limits, etc.)
[r10] Getting the vaccine at a convenient time and location
[r11] Receiving paid time off work to get a booster dose
[r12] A booster dose being made mandatory for all Canadians
[r13] Understanding the benefits and importance of booster doses
[r17] Understanding about the safety of booster doses
[r14] Knowing it is a new COVID-19 vaccine formulation that is specific to latest variants
[r97] None of the above
[Q160] Have you ever been reluctant or hesitated to get a COVID-19 booster dose?
Condition: (Q132B.r1 or Q132B.r2 or Q132B.r3)
Row:
[r1] Yes
[r2] No
[r98] Don't know
[Q161] For which reasons were you reluctant to get a COVID-19 booster dose?
Condition: (Q160.r1)
Select all that apply.
Row:
[r1] I have concerns about the safety and/or side effects of having a COVID-19 booster dose
[r2] I think COVID-19 vaccines are not effective in protecting me from the virus
[r3] I am well protected after receiving two doses/being fully vaccinated
[r4] I am not at high risk of getting COVID-19
[r5] I already had COVID-19
[r6] I had bad reactions to the previous doses
[r7] I have concerns getting it with the flu vaccine
[r8] I was waiting for an updated vaccine targeting new variants
[r96] Other reasons (please specify):
[Q162] What made you decide to get a COVID-19 booster dose despite your initial reluctance?
Condition: (Q160.r1)
Select all that apply.
Row:
[r1] High number of COVID-19 cases
[r2] I was recommended by a health care professional
[r3] I fear I may regret it later if I don't
[r4] It is required at my work place
[r5] Concerns over vaccination policies
[r6] Benefits are more important than risks
[r7] Advice from a friend or a family member
[r8] A vaccine targeting new variants (e.g. Omicron variant) is available
[r96] Other reasons (please specify):
[Q133] If recommended, how likely would you be to get a COVID-19 vaccine at the same time as a flu shot?
Condition: (Q154.r1 or Q154.r2)
Row:
[r1] Very likely
[r2] Somewhat likely
[r3] Not very likely
[r4] Not at all likely
[r5] I do not intend to get a flu shot
[r98] Don't know
[Q134] If COVID-19 vaccines were offered as a routine vaccine (e.g. annually), how likely would you be to get one?
Row:
[r1] Very likely
[r2] Somewhat likely
[r3] Not very likely
[r4] Not at all likely
[r98] Don't know
[Q134B] What is the top reason you are unlikely or uncertain about getting a routine COVID-19 vaccine (e.g. annually)?
Condition: (Q134.r3 or Q134.r4 or Q134.r98)
Row:
[r1] I think I am protected enough with the current number of vaccine doses
[r2] I had side effects with the dose/doses I already got
[r3] I think I am protected enough because I had COVID-19
[r4] I'm concerned about the safety of an annual COVID-19 vaccine
[r5] I think I am protected enough because I was vaccinated AND I had COVID-19
[r6] I'm concerned about the long-term effects of the vaccine
[r7] I need more information on annual doses (e.g. why they are needed, benefits, safety, effectiveness, etc.)
[r8] I'm fed up with getting vaccinated
[r9] I'm tired of being told what to do to protect my health
[r10] I don't think the vaccine is effective enough against the spread of COVID-19
[r11] I feel that the vaccine does not provides enough protection against severe outcomes from COVID-19
[r12] I feel that the vaccine does not provide much protection as you can still get COVID-19 even if vaccinated
[r13] I am not exposed to risks of COVID-19 in my daily life and therefore feel that I do not need to receive a routine COVID-19 vaccine
[r14] I don't think COVID-19 infection is serious enough anymore to need routine COVID-19 vaccine (e.g. annually)
[r96] Other, please specify:
[Q163] And what about if the COVID vaccines were offered twice a year, how likely would you be to get them?
Condition: (Q134.r1 or Q134.r2 or Q134.r98)
Row:
[r1] Very likely
[r2] Somewhat likely
[r3] Not very likely
[r4] Not at all likely
[r98] Don't know
[Q164] Have you seen, read or heard anything about the bivalent COVID-19 vaccine?
Row:
[r1] Yes
[r2] No
[r98] Don't know
[Q165] The bivalent COVID-19 vaccine targets the original COVID-19 and the omicron variant, which helps provide further protection against omicron strains. Based on this explanation, are you more or less likely to get a COVID-19 bivalent booster dose?
Row:
[r1] I am more likely
[r2] I am less likely
[r3] My opinion hasn't changed since I was going to get a bivalent booster dose anyways
[r4] My opinion hasn't changed since I do not intend to get a bivalent booster dose
[r98] Don't know
[Q135] Thinking about your child(ren) aged 12-17, how many doses of a COVID-19 vaccine have they received?
Condition: (CHILD_AGE.r4)
Select all that apply
Row:
[r1] 1 dose
[r2] 2 doses
[r3] 3 doses
[r7] 4 doses
[r4] None. I will wait a bit before getting my child(ren) vaccinated
[r5] None. I will not get my child(ren) vaccinated
[r6] Not sure
[Q95] Thinking about your child(ren) aged 12-17, how likely are you to have them receive a booster dose of the COVID-19 vaccine?
Condition: (Q135.r1 or Q135.r2)
Row:
[r1] Very likely
[r2] Somewhat likely
[r3] Not very likely
[r4] Not at all likely
[r5] My child(ren) 12-17 has/have already received a booster dose
[r98] Don't know
[Q136] Thinking about your child(ren) aged 5-11, how many doses of a COVID-19 vaccine have they received?
Condition: (CHILD_AGE.r3)
Select all that apply
Row:
[r1] 1 dose
[r2] 2 doses
[r3] 3 doses
[r4] None. I will wait a bit before getting my child(ren) vaccinated
[r5] None. I will not get my child(ren) vaccinated
[r6] Not sure
[Q136B] Thinking about your child(ren) aged 5-11, now that a booster has been authorized for them how likely are you to have them receive one?
Condition: (Q136.r1 or Q136.r2 or Q136.r6)
Row:
[r1] Very likely
[r2] Somewhat likely
[r3] Not very likely
[r4] Not at all likely
[r5] My child(ren) 5-11 has/have already received a booster dose
[r98] Don't know
[Q110] Why are you not likely or not sure to have your child(ren) get a booster dose of a COVID-19 vaccine?
Condition: (Q95.r3 or Q95.r4 or Q95.r98) or (Q136B.r3 or Q136B.r4 or Q136B.r98)
Select up to 3 reasons.
Row:
[r1] I think they are protected enough with the current dose schedule
[r2] They had side effects with the dose/doses they already got
[r3] I'm concerned about how long it will take to get it
[r4] I'm concerned about the safety of the booster dose
[r5] I'm concerned about the long-term effects of the vaccine
[r6] I need more information on booster doses
[r7] I prefer to wait a while before getting vaccinated
[r15] I'm confused about when they should get a booster
[r8] I'm fed up with getting my children vaccinated
[r9] They don't need a booster because the new variants are becoming less severe
[r10] I think those who are most vulnerable should get their booster dose first
[r11] I think we should help developing countries get fully vaccinated first
[r12] I do not see the need to get a booster because my child(ren) have already contracted COVID-19 after being vaccinated
[r13] They recently got COVID-19 and I don't know when to get their booster dose
[r16] I think adolescents have stronger immunity that protects them
[r14] My child is very anxious or fearful of vaccinations
[r96] Other, please specify:
[Q98B] Thinking about your child(ren) between the ages of 6 months and under 5, have they received at least one dose of a COVID-19 vaccine?
Condition: (CHILD_AGE.r2)
Row:
[r1] Yes
[r2] No, I will wait a bit before getting my child(ren) vaccinated
[r3] No, I will not get my child(ren) vaccinated
[r98] Not sure
[Q28] Which of the following factors would make you more likely to vaccinate your child(ren) against COVID-19?
Condition: (Q98B.r2 or Q98B.r3 or Q98B.r98)
Please choose your top three.
Row:
[r1] Assurance from my health professional that the vaccines are safe for my children
[r2] More information on the COVID-19 vaccine clinical trials involving children, including data on safety and effectiveness
[r3] Vaccinating my child(ren) would contribute to the collective benefit of ending the pandemic
[r4] Health Canada announces the vaccine is safe for kids and shares details of their findings from reviewing clinical trials
[r5] International health organizations say the vaccine is safe for kids based on findings from testing around the world
[r6] Being able to get my child vaccinated at a convenient location in my community
[r7] Assurance that I can be with my child(ren) during the vaccination
[r8] Encouragement from my child's school or school board that parents vaccinate their children
[r9] Seeing or hearing about friends, family or others I know personally getting their child(ren) vaccinated
[r10] Understanding the benefits of vaccinating children
[r11] Seeing or hearing about people that are "like" my child(ren) (i.e., similar age, health status, ethnicity, etc.) getting safely vaccinated
[r12] Getting more information about COVID cases and hospitalizations among children
[r13] My child(ren) can return to activities and socialization that they miss and need
[r14] My child(ren)'s mental health has suffered during the pandemic and I want them to get their regular lives back
[r15] Nothing would make me more likely to vaccinate my child(ren) against COVID-19
[r16] Receiving a financial incentive
[r17] If there was a financial penalty for not being vaccinated
[r18] More information on the potential long-term effects of my children being infected with COVID-19
[r19] More information on children who have received the COVID-19 vaccine, e.g. from clinical trials involving children or from real world use, including data on safety and effectiveness
[r20] International health organizations say the vaccine is safe for kids based on findings from testing around the world
[r21] More information on the benefits of vaccinating children, i.e. protection from severe illness and long COVID
[r22] More information on how vaccines work and build immunity in children
[r23] Getting more information about risks to children from COVID-19 (e.g. "Long COVID") and hospitalizations
[r24] Information about best timing of another dose, based on the risk in my community
[r25] If there is a COVID-19 outbreak in my child (children)'s school
[r96] Other, please specify:
[r98] Don't know
[Q166] The bivalent COVID-19 vaccine targets the original COVID-19 virus strain and the omicron variant, which helps provide further protection against omicron strains. Based on this explanation, are you more or less likely to have your child(ren) get a COVID-19 bivalent booster dose?
Condition: (CHILD.r1)
Row:
[r1] I am more likely
[r2] I am less likely
[r3] My opinion hasn't changed since I was going to have my child(ren) get a bivalent booster dose anyways
[r4] My opinion hasn't changed since I do not intent to have my child(ren) get a bivalent booster dose
[r98] Don't know
[Q111] Have any of your child's regular childhood vaccinations been missed/delayed as a result of the pandemic?
Condition: (CHILD.r1)
Childhood vaccinations are defined as routine vaccines given in childhood to protect against serious diseases such as diphtheria, tetanus, pertussis (whooping cough), polio, Haemophilus influenzae type B (Hib), rotavirus, hepatitis B, measles, mumps, rubella, chickenpox, pneumococcal and meningococcal diseases, and human papillomavirus virus (HPV).
Row:
[r1] Yes
[r2] No
[r98] Don't know
[Q112] Do you intend to catch up on your child's missed/delayed regular childhood vaccinations?
Condition: (Q111.r1)
Row:
[r1] Yes
[r2] No
[r98] Don't know
[Q137] Why do you not plan for your children to get the recommended childhood vaccines?
Condition: (Q112.r2)
Row:
[r1] I am concerned about potential side effects from the vaccine
[r2] I am concerned about the long-term effects of the vaccine
[r3] I believe that children have strong immune systems and do not need vaccines
[r4] I do not think the diseases they protect against are common in Canada
[r5] I do not think the diseases they protect against are serious enough to warrant vaccination
[r6] I do not want my child(ren) to receive any more vaccines
[r7] I had not planned for my child(ren) to get the recommended childhood vaccines
[r8] I do not believe that vaccines work
[r9] The COVID-19 pandemic and related vaccines have changed my views on vaccines
[r96] Other, please specify:
[Q138] Adult routine vaccinations are defined as routine vaccines and/or boosters given in adulthood to protect against serious diseases such as shingles (recommended for 50+), tetanus, pertussis (whooping cough), influenza (flu) and pneumococcal (recommended for 18+ with chronic medical conditions and healthy adults aged 65+).
Have you missed/delayed any routine vaccinations as a result of the pandemic?
Condition: False
Row:
[r1] Yes
[r2] No
[r3] I don't think this is applicable to me
[r98] Don't know
[Q139] Do you intend to catch up on your missed/delayed routine vaccinations?
Condition: False
Row:
[r1] Yes
[r2] No
[r98] Don't know
[Q140] Why do you not intend to catch up on your missed/delayed routine vaccinations?
Condition: False
Row:
[r1] I am concerned about potential side effects from vaccines
[r2] I am concerned about the long-term effects of vaccines
[r3] I do not think the diseases they protect against are common in Canada
[r4] I do not think the diseases they protect against are serious enough to warrant vaccination
[r5] Do not want to receive any more vaccines
[r6] Belief that immune system is strong without vaccines
[r7] I do not believe that vaccines work
[r8] The COVID-19 pandemic and related vaccines have changed my views on vaccines
[r96] Other, please specify:
[Q142] How has the recent COVID-19 pandemic had an impact on your confidence in vaccinations in general?
Row:
[r1] I am a lot less confident now
[r2] I am somewhat less confident now
[r3] About the same as before
[r4] Somewhat more confident now
[r5] A lot more confident now
[r98] I don't know
[Q143] Why are you less confident in vaccinations?
Condition: (Q142.r1 or Q142.r2)
Select all that apply
Row:
[r1] COVID-19 vaccines have negatively impacted my view on vaccines in general
[r2] I have more concerns about the safety of vaccines in general
[r3] I now believe that vaccines do not have as much benefit in preventing severe outcomes
[r4] I now believe that vaccines in general does not have as much benefit in stopping the spread of viruses
[r5] The COVID-19 pandemic has shown that we have strong immune systems without vaccines
[r6] The COVID-19 pandemic has shown that vaccines do not work very well
[r96] Other:
[Q144] Do you intend to get the flu vaccine this year?
Row:
[r1] Yes
[r2] No
[r3] I have already received the flu vaccine this year
[r98] Don't know
[Q145] Why do you not intend to get your flu shot this year?
Condition: (Q144.r2 or Q144.r98)
Select all that apply
Row:
[r1] I have never gotten a seasonal flu shot before
[r2] I am healthy, and/or never get the flu
[r3] Getting the flu doesn't make me that sick
[r4] I have concerns about side effect from getting the flu shot
[r5] The flu shot does not work
[r6] I have concerns about interactions with the COVID-19 vaccines
[r7] No one got the flu last year
[r8] I've had enough vaccines this year
[r9] I'm not eligible for the flu shot in my area
[r10] I feel I am protected as I had the flu this year
[r11] I had side effects the last time I received the flu shot
[r12] I had side effects the last time I received a vaccine other than the flu shot
[r13] Individual public health measures like frequent handwashing and wearing a mask are enough to protect me from the flu
[r15] I believe the flu shot can give me the flu
[r96] Other, please specify:
[r14] No specific reason, I just won't get it
[Q168] Among the following factors, what would motivate you to get a flu shot this year?
Condition: (Q144.r2 or Q144.r98)
Please select up to 3 reasons.
Row:
[r1] Advice from my primary health care provider that it is recommended for me
[r2] Being able to more safely spend time with friends and family
[r3] Knowing that the majority of flu cases are among those who have not received a flu shot
[r4] Knowing that the majority of flu hospitalizations are among those who have not received flu shot
[r5] Knowing that getting a flu shot could help protect myself from severe outcomes
[r6] Knowing what severe outcomes or complications could result from being infected with the flu
[r7] Knowing if I am more at risk of severe outcomes from being infected with the flu
[r8] Knowing that I can reduce spreading the flu to those around me who are at higher risk of severe outcomes from being infected with the flu
[r9] Getting the flu shot at a convenient time and location
[r10] Receiving paid time off work to get a flu shot
[r11] A flu shot being made mandatory for all Canadians
[r12] Understanding the benefits and importance of a flu shot
[r97] None of the above
[Q1B] How often do you follow each of the following public health measures?
Individual public health measures are actions you can use every day to help reduce the spread of COVID-19 and other respiratory illnesses. These measures are also sometimes called personal preventive practices. Examples include: staying home when sick; wearing a well-fitting respirator or mask, especially in public indoor settings; improving indoor ventilation in home or co-living settings; practicing respiratory etiquette and frequent hand hygiene; and cleaning and disinfecting high-touch surfaces and objects.
NOTE: In any questions below that refer to masks, the word mask refers to a respirator (e.g., N95, KN95), medical mask or non-medical mask.
Column:
[c1] Always
[c2] Often
[c3] Sometimes
[c4] Rarely
[c97] Never
[c98] Don't know/Not applicable
Row:
[r1] Washing hands for at least 20 seconds with soap and warm water
[r2] Using hand sanitizer containing at least 60% alcohol, if soap and water aren't available
[r3] Staying home and away from others if you feel sick
[r4] Practising physical distancing
[r5] Limiting the number of people you have contact with outside of your household
[r6] Avoiding closed spaces and crowded places
[r7] Wearing a mask–when indoors in a public space or in an indoor space with people from outside your immediate household
[r8] Wearing a mask– when outside in a public space
[r9] Improving ventilation when people from outside your immediate household are in your home (as examples: open windows and doors regularly, use a heating, ventilation and air conditioning (HVAC) system or run kitchen or bathroom exhaust fans)
[r10] Using individual public health measures when interacting with someone who is at risk of more severe disease or outcomes from COVID-19 (e.g., are an older adult over age 60, are pregnant, have Down syndrome, have a chronic medical condition, are immunocompromised, or live with obesity etc.)
[r11] Wearing a mask – inside with others when you're feeling sick
[Q115] Many individual public health measures (e.g., staying home when sick, handwashing, wearing a mask) were recommended in 2020 to help control the spread of COVID-19. How much do you think these individual public health measures could help reduce the spread of other respiratory infectious diseases, such as seasonal influenza (the flu)?
Row:
[r1] A great deal
[r2] Somewhat
[r3] Not very much
[r4] Not at all
[r98] Don't know
[Q169] To what extent would you agree or disagree with reinstating mandatory public health measures (e.g. policies on masking, or capacity limits)?
Row:
[r1] Strongly agree
[r2] Somewhat agree
[r3] Neither agree or disagree
[r4] Somewhat disagree
[r5] Strongly disagree
[r98] Don't know
[Q170] Under what conditions would you support reinstating mandatory public health measures (e.g. policies on masking, or capacity limits).
Select all that apply.
Row:
[r1] If there is a local outbreak of COVID-19 cases
[r2] If there are a rising number of hospitalizations related to COVID-19
[r3] If there are a rising number of deaths related to COVID-19
[r4] If the health care or public health capacities are becoming overloaded
[r5] If the spread of COVID-19 is increasing
[r6] If there are new COVID-19 variants of concern
[r7] If there are other respiratory viruses in circulation (eg. seasonal flu)
[r8] I am not supportive at all to reinstate the mandatory PHMs
[Q146] What is the top reason you rarely or never practice any individual public health measures to reduce the spread of other respiratory diseases?
Condition: False
Row:
[r1] I don't think it helps reduce the spread of other respiratory diseases
[r2] I am okay with getting other respiratory diseases
[r3] I want to build acquired immunity by being infected with other respiratory diseases
[r4] The individual public health measures cause too much disruption in my life
[r5] I don't want to have others criticize or ridicule me for practicing individual public health measures
[r98] Don't know
[r96] Other, please specify:
[Q147] How confident, if at all, do you feel about making your own decisions with respect to choosing to practice any or all of the individual public health measures mentioned in the previous questions (i.e. wearing a mask, staying home when sick, hand hygiene, etc)?
Condition: False
Row:
[r1] Very confident
[r2] Somewhat confident
[r3] A little confident
[r4] Not confident at all
[r98] I don't know
[Q148] Which of the following would be useful to help your decision making about using any or all of the individual public health measures mentioned in the previous question (i.e. wearing a mask, staying home when sick, hand hygiene, etc)?
Condition: False
Select all that apply.
Row:
[r1] Information about potential risks to myself personally (i.e. infection, severe illness, etc.)
[r2] Information on the effectiveness of individual public health measures
[r3] Information on the spread of COVID-19 in my community
[r4] Information on the spread of a cold, flu or other respiratory illness going around in my community
[r5] If I knew of a family member or friend who became seriously ill from COVID-19
[r6] Clear communications from the government/public health officials on when and which individual public health measures should be used
[r96] Other, please specify:
[r98] Don't know
[Q149] Where would you go for these types of information?
Condition: False
Select all that apply.
Row:
[r1] Conversations with family/friends/colleagues
[r2] Conversations with a health care provider
[r3] Government of Canada websites
[r4] Provincial/territorial government websites
[r5] Provincial/territorial public health authorities
[r6] Local or regional health authorities
[r7] Federal public health authorities
[r8] Non-Canadian health authorities, e.g. the CDC, WHO
[r9] Social media
[r10] Your workplace
[r11] Media outlets/news
[r96] Other sources, please specify:
[r98] Don't know
[Q150] To what extent do you feel pressured by others to practice or not practice individual public health measures?
Condition: False
Row:
[r1] A lot
[r2] Somewhat
[r3] A little
[r4] Not at all
[r98] Don't know
[Q151] How familiar are you with the potential long-term effects of having COVID-19 (also known as "long-COVID" or "post COVID-19 condition")?
Row:
[r1] Very familiar
[r2] Somewhat familiar
[r3] Not very familiar
[r4] Not at all familiar
[r98] Don't know
[Q152] How worried are you/would you be about developing longer-term symptoms from a COVID-19 infection?
Row:
[r1] Very worried
[r2] Somewhat worried
[r3] Not very worried
[r4] Not at all worried
[r98] Don't know
[Q153] What makes/would make you feel worried about long-term symptoms of COVID?
Condition: (Q152.r1 or Q152.r2)
Select all that apply.
Row:
[r1] Limitations to my working life
[r2] Limitations to my leisure/personal life
[r3] Uncertainty about my future health prospects
[r4] Being judged for my condition
[r5] Not knowing if others (friends, colleagues, employers, healthcare providers, etc.) will take my condition seriously
[r6] Difficulty in formally indicating my condition to employers, healthcare providers, and/or others
[r7] Difficulty in accessing benefits related to my condition (e.g. sick leave, disability)
[r8] Being terminated by my employer for my condition
[r9] Lack of information/resources on my condition
[r10] Lack of public acknowledgement from authority figures (government, etc.) on my condition
[r96] Other, please specify:
The last few questions are strictly for statistical purposes. All of your answers are completely confidential.
[LANGU] What is the language you first learned at home as a child and still understand?
Row:
[r1] English
[r2] French
[r96] Other
[r99] I prefer not to answer
[MINO] Do you identify as any of the following?
SELECT ALL THAT APPLY
Row:
[r3] A member of the LGBTQ2 community
[r4] A person with a disability
[r97] None of the above
[r99] I prefer not to answer
[IMM] Where were you born?
Row:
[r1] Born in Canada
[r2] Born outside Canada
[r99] I prefer not to answer
[YIMM] In what year did you move to Canada?
Condition: (IMM.r2)
[MainAutoCountry] What is your country of origin?
Condition: (IMM.r2)
[PAYS] What is your country of origin?
Condition: IMM.r2 and not(MainAutoCountry.r99)
[SCOL] What is the highest level of formal education that you have completed?
Select one only
Row:
[r1] Some high school or less
[r2] High school diploma or equivalent
[r3] Registered Apprenticeship or other trades certificate or diploma
[r4] College, CEGEP or other non-university certificate or diploma
[r5] University certificate or diploma below bachelor's level
[r6] Bachelor's degree
[r7] Postgraduate degree above bachelor's level
[r99] I prefer not to answer
[OCCUP] Which of the following categories best describes your current employment status? Are you...
Select one only
Row:
[r1] Working full-time (35 or more hours per week)
[r2] Working part-time (less than 35 hours per week)
[r3] Self-employed
[r4] Unemployed, but looking for work
[r5] A student attending school full-time
[r6] Retired
[r7] Not in the workforce (full-time homemaker, full-time parent, or unemployed and not looking for work)
[r96] Other employment status. Please specify.
[r99] I prefer not to answer
[REVEN] Which of the following categories best describes your total household income? That is, the total income of all persons in your household combined, before taxes?
Select one only
Row:
[r1] Under $20,000
[r2] Between $20,000 and under $40,000
[r3] Between $40,000 and under $60,000
[r4] Between $60,000 and under $80,000
[r5] Between $80,000 and under $100,000
[r6] Between $100,000 and under $150,000
[r7] $150,000 and above
[r99] I prefer not to answer
[HH_SIZE] How many people, including yourself, are supported by your total household income?
[FSA] Please indicate the first 3 characters of your postal code.
If you would rather not provide it, please select I don't know/I prefer not to answer
The present study deals with topics that you might have found distressing. If you found participation distressing, we want to encourage you to consider free mental health services including the following:
Appendix F: Screening guide – WAVE 19.
The groups will be held online via CMNTY.
The objective is to have 8-10 participants per focus group except for group 1 and 2 (2SLGBTQI+) with 4-6 (OR MORE IF POSSIBLE) participants per group.
| Date/Time | Participants | Language | Region | |
|---|---|---|---|---|
| GROUP 1 4-6 participants Or more if possible | Feb 7, 2023, 5pm | 2SLGBTQI+ populations 18 to 55 | ENG | BC + AB+SK+MB+ON |
| GROUP 2 4-6 participants or more if possible | Feb 7, 2023, 5pm | 2SLGBTQI+ populations 18 to 55 | FRE | QC + NB |
| GROUP 3 8-10 participants | Feb 7, 2023, 7pm | Racialized populations 18 to 55 | ENG | ON |
| GROUP 4 8-10 participants | Feb 7, 2023, 7pm | Racialized populations 18 to 55 | FRE | QC + NB |
| GROUP 5 8-10 participants | Feb 9, 2023, 7pm | Young adults 18 to 34 | ENG | AB + SK + MB |
| GROUP 6 8-10 participants | Feb 8, 2023, 7pm | Parents (children under 18) and people who are pregnant | ENG | ON + ATL |
| GROUP 7 8-10 participants | Feb 8, 2023, 5pm | Parents (children under 18) and people who are pregnant | ENG | BC + Prairies+ Territories |
| GROUP 8 8-10 participants | Feb 8, 2023, 5pm | Parents (children under 18) and people who are pregnant | FRE | QC + NB |
Recognizing challenges with regards to recruitment, it would be best if we are able to also include Indigenous participants in some groups. Would be nice to aim for at least three participants spread throughout the different sessions.
For each participant, collect the following information:
Participant name:
Phone number at home:
Cell phone:
Email address:
Recruitment date:
Recruiter :
Group #:
Confirmation (date):
Introduction
Hello/Bonjour, I'm ___________ of Leger, a marketing research company. We are organizing a research project on behalf of Health Canada. The research's objective is to collect opinions and feedback from Canadians that will be used by Health Canada to understand Canadians' behaviours and attitudes with respect to mental health and COVID-19, which may include vaccination and public health measures.
One of the project objectives is to better understand the perspectives of Canadians accessing or trying to access mental health services and/or supports and mental health in general, as well as the perspectives of their family members and friends. You do not have to have experienced a mental health challenge or mental illness to participate in our focus groups, nor do you have to have used or attempted to access mental health services or support. Nor do you need to be an expert.
We are preparing to hold a few research sessions with people like yourself. Participation is completely voluntary. We are interested in your opinions. The format is an "online" discussion led by a research professional with up to ten participants. All opinions will remain anonymous and will be used for research purposes only in accordance with laws designed to protect your privacy. We don't have anything to sell and we don't advertise and it's not an opinion poll on current events or politics. We are organizing several of these discussions. We would be interested in possibly having you participate.
Your participation is voluntary. All information collected, used and/or disclosed will be used for research purposes only and the research is entirely confidential. We are also committed to protecting the privacy of all participants. The names of the participants will not be provided to any third party. May I continue?
[Interviewer note: If asked about privacy laws, say: "The information collected through the research is subject to the provisions of the Privacy Act, the legislation of the Government of Canada, and to the provisions of relevant provincial privacy legislation.]
The focus group would take place online on the (INSERT DATE/TIME) and will be a maximum of 2 hours. You will be compensated $135 for your time.
I repeat that participation is entirely voluntary, and all information you provide is completely confidential. The full names of participants will not be provided to any third party.
A1. Are you interested in participating?
| Yes | 1 | Continue |
|---|---|---|
| No | 2 | Thank and conclude |
I would now like to ask you a few questions to see if you meet our eligibility criteria to participate.
When you conclude at A2-A3 -Intro 1, say: Thank you for your cooperation but unfortunately, we cannot invite you in the groups we organize.
When you conclude on other screening questions, say: Thank you for your collaboration. We have already reached the number of participants with a profile similar to yours. Therefore, we cannot invite you to participate.
A2. The group discussions we are organizing are going to be held over the Internet. They are going to be "online focus groups". Participants will need to have a computer, a high-speed Internet connection, and a WebCam in order to participate in the group. Would you be able to participate under these conditions?
| Yes | 1 | Continue |
|---|---|---|
| No | 2 | Thank and conclude |
A3. Are you comfortable discussing mental health, whether it's your own, your family's or friends', in a focus group setting with several people?
| Yes | 1 | Continue |
|---|---|---|
| No | 2 | Thank and conclude |
Profiling
INTRO1.
Do you or anyone in your immediate family work or have you ever worked in...?
| Marketing Research | 1 Thank and conclude |
|---|---|
| Marketing and Advertising | 2 Thanks and conclude |
| Public relations, communications | 3 Thanks and conclude |
| Media (newspapers, television, radio, etc.) | 4 Thanks and conclude |
| Telecommunications | 5 Thanks and conclude |
| Healthcare sector | 6 Thanks and conclude |
| Mental health sector | 7 Thanks and conclude |
| None of the above | 9 |
Gender
Please indicate your gender
| Male or man | 1 |
|---|---|
| Female or woman | 2 |
| Another gender | 3 |
| Gender: Ensure a good mix during the recruitment, Another gender is not a screening criteria | |
Province
In which province or territory do you live?
| British Columbia | 1 |
|---|---|
| Alberta | 2 |
| Saskatchewan | 3 |
| Manitoba | 4 |
| Ontario | 5 |
| Quebec | 6 |
| New Brunswick | 7 |
| Nova Scotia | 8 |
| Prince Edward Island | 9 |
| Newfoundland | 10 |
| Northwest Territories | 11 |
| Yukon | 12 |
| Nunavut | 13 |
Area
Which of the following best describes the area in which you live?
| Urban area | 1 |
|---|---|
| Rural area | 2 |
Try for a good mix |
|
Language
What is your first official language spoken?
Note for recruiter if respondent asks: In Canada, 'first official language spoken' is specified within the framework of the Official Languages Act. It refers to the first official language (i.e., English or French) that is spoken by an individual.
| French | 1 |
|---|---|
| English | 2 |
AGE.
What age category do you fall into?
| 18 to 24 | 1 Prioritize Group 5 |
|---|---|
| 25 to 34 | 2 Prioritize Group 5 |
| 35 to 44 | 3 |
| 45 to 55 | 4 |
| 55 and over | 5 Thank and conclude |
| Age: Ensure a good mix of age during the recruitment | |
MINO
Do you identify as any of the following?
| Yes | No | Prefer not to answer | |
|---|---|---|---|
| A member of the 2SLGBTQ+ community | Prioritize Group 1 and 2 | - | - |
| A visible minority or racialized person | Prioritize Group 3 and 4 | - | - |
ETHN.
What is your ethnic origin?
| Black - African, African Canadian, Afro-Caribbean descent | 1 |
|---|---|
| East Asian - Chinese, Japanese, Korean, Taiwanese, or other East Asian descent | 2 |
| Indigènes - First Nations, Inuk/Inuit, Métis descent | 3 |
| Latin American - Hispanic or Latin American descent | 4 |
| Middle Eastern - Arab, Persian, West Asian descent (e.g., Afghan, Egyptian, Iranian, Kurdish, Lebanese, Turkish) | 5 |
| South Asian - South Asian descent (e.g., Bangladeshi, Indian, Indo-Caribbean, Pakistani, Sri Lankan) | 6 |
| Southeast Asian - Cambodian, Filipino, Indonesian, Thai, Vietnamese, or other Southeast Asian descent | 7 |
| White - European descent | 8 |
| Another category — please specify: | 9 |
| Includes values not described above | 10 |
| Do not know | 11 |
| Prefer not to answer/Not applicable | 12 |
ETHN: There should be at least three Indigenous/First Nations/Inuk/Métis (code 3) in the groups (does not matter what group)
ETH: For group 3 -4 – ETH must not be white (code 8)
Following section from PREG to VACC B – only for GROUP 6-7-8
PREG. – Ask all
Are you currently expecting a child for whom you would be the primary decision maker about the child's health? If women or another gender add - Or are you personally pregnant?
| Yes | 1 Prioritze group 6-7-8 |
|---|---|
| No | 2 |
ADOP – Ask only if no at PREG
Are you currently planning to adopt a child in the next year?
| Yes | 1 Prioritze group 6-7-8 |
|---|---|
| No | 2 |
PREG 2 – ask only if PREG = yes (1) or if ADOP = yes (1)
Do you intend to have your child(ren) vaccinated with routine immunizations?
| Yes, I intend to have my child(ren) vaccinated with routine immunizations | 1 Continue to education |
|---|---|
| No, I have no intention to have my child(ren) vaccinated with routine immunizations | 2 Thanks and conclude |
CHILD.
How many children under 18 do you have?
| None | 1 Thanks and conclude |
|---|---|
| [ ] enter number of child/children | GO TO VACCB |
VACCB.
Thinking about your child(ren) under 18, are they up to date with their routine vaccinations?
| Yes, my child(ren) are up to date with their routine immunizations | 1 Continue to education |
| No, my child(ren) is(are) not vaccinated but I intend to have my child(ren) vaccinated with routine immunizations | 2 Continue to education |
| No, they have missed or experienced delays getting their routine immunizations and have not caught up yet but I intend to have them catch up their missed vaccination. | 3 Continue to education |
| I have no intention to have my child(ren) vaccinated with routine immunizations | 4 Thanks and conclude |
If the participant has more than one child under 18 at child, ask vaccb for each child
We need a good mix of participants with children up to date and some who have experienced delay in their routine vaccination for group 6-7-8
EDUCATION.
What is the highest level of education you completed?
| Some high school or less | 1 |
|---|---|
| High school diploma or equivalent | 2 |
| Registered Apprenticeship or other trades certificate or diploma | 3 |
| College, CEGEP or other non-university certificate or diploma | 4 |
| University certificate or diploma below bachelor's level | 5 |
| Bachelor's degree | 6 |
| Postgraduate degree above bachelor's level | 7 |
| Ensure a good mix for all groups if possible during the recruitment | |
OCCUP.
Which of the following categories best describes your current employment status? Are you…
| Working full-time (35 or more hours per week) | 1 |
|---|---|
| Working part-time (less than 35 hours per week) | 2 |
| Self-employed | 3 |
| Unemployed, but looking for work | 4 |
| A student attending school full-time | 5 |
| Retired | 6 |
| Not in the workforce (full-time homemaker, full-time parent, or unemployed and not looking for work) | 7 |
| Other employment status. Please specify. | 8 |
GROUP ATTRIBUTION
| Group 1 | Province: 1-2 -3-4-5 (BC – AB –SK –MB--ON) Language: English Age: code 1 to 5 (18 to 55 y.o.) Mino : 2SLGBTQ+ = yes |
|---|---|
| Group 2 | Province: 6-7 (QC-NB) Language: French Age: code 1 to 5 (18 to 55 y.o.) Mino : 2SLGBTQ+ = yes |
| Group 3 | Province: 5 (Ontario) Language: English Age: code 1 to 5 (18 to 55 y.o.) Mino : Visible minority =yes Ethn =code 1 to 7 |
| Group 4 | Province: 6-7 (QC-NB) Language: French Age: code 1 to 5 (18 to 55 y.o.) Mino : Visible minority =yes Ethn =code 1 to 7 |
| Group 5 | Province: 2-3-4 (AB-SK-MB) Language: ENG Age: code 1-2 (18 to 34 y.o.) |
| Group 6 | Province: 5, 7-8-9-10 (ON-ATL) Language: ENG MIX PREG 2= 1 AND VACCB =1-2-3 (IMPORTANT TO HAVE SOME PARTICIPANTS WITH VACCB =3 IN THIS GROUP) PREG2= 1 OR VACCB=MIX OF PARENT AT VACCB PROFILE 1-2-3 |
| Group 7 | Province: 1-2-3-4; 11-12-13 (BC-Prairies-Territories) Language: ENG MIX PREG 2= 1 AND VACCB =1-2-3 (IMPORTANT TO HAVE SOME PARTICIPANTS WITH VACCB =3 IN THIS GROUP) PREG2= 1 OR VACCB=MIX OF PARENT AT VACCB PROFILE 1-2-3 |
| Group 8 | Province: 6-7 (QC-NB) Language: French MIX PREG 2= 1 AND VACCB =1-2-3 (IMPORTANT TO HAVE SOME PARTICIPANTS WITH VACCB =3 IN THIS GROUP) PREG2= 1 OR VACCB=MIX OF PARENT AT VACCB PROFILE 1-2-3 |
PSPC POR1
Have you ever attended a discussion group or taken part in an interview on any topic that was arranged in advance and for which you received money for participating?
| Yes | 1 |
|---|---|
| No | 2 Go to PSPC POR |
PSPC POR2
When did you last attend one of these discussion groups or interviews?
| Within the last 6 months | 1 Thanks and conclude |
|---|---|
| Over 6 months ago | 2 |
PSPC POR 3
Thinking about the groups or interviews that you have taken part in, what were the main topics discussed?
RECORD: _______________ THANK/TERMINATE IF RELATED TO HEALTH CARE OR MENTAL HEALTH
PSPC POR4
How many discussion groups or interviews have you attended in the past 5 years?
| Fewer than 5 | 1 |
|---|---|
| Five or more | 2 Thanks and conclude |
Conclusion
Q1.
By participating in this focus group, you will be asked to discuss with other participants and share your opinion on various topics related to mental health, mental health services and supports, regarding health care and public health measures. Please note that you do not need to be an expert to participate. You may also be asked to read during the meeting.
How comfortable do you feel in such an environment?
Read the answer choices.
| Very comfortable | 1 |
|---|---|
| Somewhat comfortable | 2 |
| Not very comfortable | 3 Thanks and conclude |
| Not at all comfortable | 4 Thanks and conclude |
Invitation
Thank you. We'd like to invite you to participate in this focus group.
We are thrilled to have you as one of our participants in this study; your profile perfectly fits the target respondent we are looking for. We would like to invite you to participate in an online focus group that will be facilitated by an experienced professional moderator and will last approximately 120 minutes. The session will take place at [XX], on____XX____ (date/time) __XX__.
For your participation, you will receive a financial incentive of $135.
Please note that the session will be recorded. Your interview may also be observed by people who are directly working on the research study.
Just a quick reminder that the groups of discussion are going to be held over the Internet. They are going to be "online focus groups". You will need a computer, a high-speed Internet connection, and a WebCam in order to participate in the group.
INV1.
Are you still interested in participating in this research study?
| Yes | 1 |
|---|---|
| No | 2 Thanks and conclude |
The information provided by you will be kept confidential and will only be disclosed to those who are directly working on the research that is relevant to the topic of discussion.
INV2.
Representatives from Health Canada may observe the discussion, but will not have access to any of your private information. You will be asked to sign a consent form in order to participate in this research. Would you be willing to do this?
| Yes | 1 |
|---|---|
| No | 2 Thanks and conclude |
Privacy section
Now I have a few questions that relate to privacy, your personal information and the research process. We will need your consent on a few issues that enable us to conduct our research. As I run through these questions, please feel free to ask me any questions you would like clarified.
P1) First, we will provide the online platform and session moderator with a list of respondents' names and profiles (screener responses) so that they can sign you into the group. Do we have your permission to do this? I assure you it will be kept strictly confidential.
| Yes | 1 Go to P2 |
|---|---|
| No | 2 Read information below and P1A |
We need to provide the online platform and session moderator with the names and background of the people attending the focus group because only the individuals invited are allowed in the session and the facility and moderator must have this information for verification purposes. Please be assured that this information will be kept strictly confidential. GO TO P1A
P1a) Now that I've explained this, do I have your permission to provide your name and profiles to the online platform and moderator?
| Yes | 1 Go to P2 |
|---|---|
| No | 2 Thanks and conclude |
P2) A recording of the group session will be produced for research purposes. The recording will only be used by the team of researchers at Léger to assist in preparing a report on the research findings.
Do you agree to be recorded for research purposes only?
| Yes | 1 Go to invitation |
|---|---|
| No | 2 Read information below and P2A |
It is necessary for the research process for us to record the session as the researcher needs this material to complete the report.
P2a) Now that I've explained this, do I have your permission for recording?
| Yes | 1 Go to invitation |
|---|---|
| No | 2 Thanks and conclude |
As we are only inviting a small number of people to take part, your participation is very important to us. If for some reason you are unable to participate, please call so that we can get someone to replace you. You can reach us at ____ at our office. Please ask for ____.
To ensure that the focus groups run smoothly, we remind you:
- To make sure you are connected to the Internet and logged on 15 minutes in advance of the group
- To turn off your cellular phones – to avoid disruptions during the group.
- Make sure your WebCam is ON and functional
- To bring reading glasses, if necessary, to be able to go over the material.
- To make sure you will be located in a clear room (luminous)
- That the session will be recorded for analysis purposes only.
Email address: __________________________________________________________________
Thank you very much for your assistance!
Contact information
Someone from our company will contact you to confirm the group. Could you leave me a phone number where we can reach you in the evening as well as during the day?
Name:
Phone number:
Cell phone:
Recruited by:
Confirmed by:Appendix G: Discussion guide – WAVE 19.
| BLOC 1 | Introduction and explanation |
|---|---|
| Length | 10 Minutes |
While participants log in
- Share MH resources links in the chat
During the discussion, one of the topics we will address is mental health. While we have tried to minimize any potential risks and discomfort, due to the nature of the questions pertaining to one's mental health, some participants may feel uneasy or uncomfortable when answering questions about their own experiences or listening to the experiences of others. If you feel uncomfortable during this part of the discussion, feel free to not answer the questions asked. You can also mute the conversation, or even leave and rejoin after the mental health portion that will last around an hour.
The present study deals with topics that you might have found distressing. If you feel the need to talk, here is a list of mental health resources you can consult:
- Mental health support: Get help
- Wellness Together Canada
- Get Help | Talk Suicide Canada
- The Hope for Wellness Helpline
Welcome and presentation
- Reception of participants
- Introduction of the moderator
- Presentation of Leger
Primary aim
- The research is being conducted by Léger Marketing on behalf of Health Canada (HC). The objective of the meeting is to learn about your opinion and perception on different elements related to mental health, vaccines and the COVID-19 pandemic to help inform government actions and decisions.
Rules of discussion
- Dynamics of the discussion (duration, discussion, round table)
- No wrong answers
- Importance of giving personal, spontaneous and honest opinions
- Importance of reacting respectfully to the opinions of others
- Importance of speaking one person at a time
Presentation of the group room
- Audio and video recording for subsequent analysis
- Presence of observers from HC
- Presence of analyst to take notes
Results confidentiality
The discussions we will have this evening will remain confidential at all times.
- Your name will never be mentioned in the report
- Information collected for study purposes only
- The information collected will help Health Canada get a better understanding of Canadians' mental health situation, as well as their attitudes towards vaccines and public health measures.
Do you have any questions before we get started?
Introduction of participants
- What's your first name?
- Your place of residence (province and city)?
- What is your main occupation?
| BLOC 2 | Mental health |
|---|---|
| Length | 60 minutes |
Warm-up (brief, no need for specific recall of pub ed campaign)
Have you seen or heard anything about the mental health of Canadians lately?
IF YES, what was it? What was most striking? What do you remember?
Mental health
If we jump right in, what does mental health mean to you? Does it have a positive or negative meaning?
Explore why positive and why negative meaning.
PROBE: What does good mental health mean to you? Why?
PROBE: What does poor mental health mean to you? Why?
In general, what does it mean for someone to take care of their mental health?
What actions can you take to care for your own mental health? To improve your mental health? To maintain your mental health?
Examples if needed: exercising, sleeping well, doing something you enjoy, connecting with loved ones, seeking support when needed, I take part in local events and get to know my neighbours, I find ways to get involved and give back to my community, etc.
Do you follow through on these actions regularly to take care of your mental health? If not, why? What are some of the reasons or barriers?
Examples if needed: not enough time in the day, other competing priorities such as housework, physical activity, caretaking of children, etc.)
What kinds of information or support would help you take care of your mental health?
Do you only think of your mental health in times when you feel you are struggling?
What can have a negative impact on your mental health?
Examples if needed: biological (genetics, prenatal damage, brain injury), behavioural (being isolated, not engaging with friends, engaging in negative thinking patterns), structural (economic hardship, lack of food and poor nutrition, unsafe living conditions, lack of access to mental health resources, stigma, lower health/mental health literacy, etc).
What signs or symptoms would prompt you to seek help with your mental health? Explore why.
Examples if needed: feeling overwhelmed by intense emotions; physical symptoms such as fatigue, stomach pain, headaches, weight loss/gain, racing heart; trouble with daily functioning, feeling anxious/nervous.
What actions would you take if you felt you were experiencing poor mental health?
PROBE: Who/where would you go to first for support with your mental health?
Examples if needed: family doctor/primary care physician, crisis line, spiritual leader, emergency services at a hospital, psychologist, online resources, friend, relatives, local community health centre, community agency, etc.
Do you find it hard to seek help or support when you feel you are experiencing poor mental health?
PROBE: What barriers, if any, would make it challenging to seek help?
Examples if needed: not knowing where to go, cost, finding the time, unsure if problem is serious enough, embarrassment, wait lists, access to care or supports was limited, do not have a family doctor, etc.
Ask only if time permits:
- Do you feel comfortable talking about your mental health with family, friends, others close to you?
- Why, or why not?
- Why comfortable/uncomfortable with these people and not others?
- Do you know where to access mental health resources or services? Can you name them?
- What types of information or resources would you like to find on a Government of Canada mental health website?
Exercise 1 – polling questions + discussion
You should now see a pop up appear on your screen. Please read the statement and indicate to what extent you agree or disagree with the statement [Agree, Disagree] Discuss:
- Inequality of any kind (such as social, economic, health, etc.) can have an impact on one's mental health.
- Only adults have mental health challenges.
- The sooner mental challenges are identified and treated, the better.
[Repeat for each statement] Discuss: Those who agree, why? Those who disagree, why?
Exercice 2 – polling questions + discussion
I will now present you with different messages that you might see on social media, in advertisements, online etc. regarding different topics related to mental health. After each message, we will discuss your impressions.
Share screen
Message 1:
If you are struggling with mental health challenges and addiction, please know that you are not alone. There are programs and services that can help, including Wellness Together Canada which is free and confidential, and available 24/7.
Is this message clear? Polling answer scale: Very clear, somewhat clear, somewhat unclear, very unclear
How can we improve the message?
What do you think of the phrase "you are not alone"?
PROBE: Do you find the phrase problematic? Why, or why not?
Message 2:
We all know that the past few years have been challenging. The pandemic has disproportionately affected already marginalized populations, such as women, youth, racialized communities, 2SLGBTQIA+, First Nations, Inuit and Métis. There have been, and continues to be, significant impacts on peoples' mental well-being.
Is this message clear? Polling answer scale: very clear, somewhat clear, somewhat unclear, very unclear
How can we improve the message?
Are you tired of hearing "the past few years have been challenging"? Do you think the past few years still have an impact on Canadian's mental health?
Message 3:
If you need help, please reach out. If you are struggling, know that you can access the Wellness Together Canada (WTC) portal and its companion app PocketWell for free 24/7 educational content, and self-guided and moderated peer-to-peer support, as well as one-to-one counselling with qualified health professionals.
Is this message clear? Polling answer scale:: very clear, somewhat clear, somewhat unclear, very unclear
How can we improve the message?
What do you think about the phrase "If you need help, please reach out. If you are struggling know that you can access.."?
PROBE: Are you tired of hearing that you can reach out if you need help or are struggling? Do you see any problems with the suggested phrasing? What do you think of the word "struggling"? Is there another word you'd prefer to be used here?
Are the types of support available, accessible, clear and easy to understand? Would they encourage you to reach out and get more information or access these services?
We are now going to change the subject from mental health to vaccination.
| BLOC 3 | Vaccine |
|---|---|
| Length | 25 minutes |
Read to all
The seasonal flu shot is your best protection from severe outcomes from the flu, and even healthy people can experience serious illness or pass that illness to someone at higher risk of hospitalization (children, seniors, people with chronic illnesses). You cannot get the flu from the flu shot.
Knowing these facts, do you think everyone should get a flu shot?
PROBE: If so, why? Or why not? Who should get it? Who should not get it?
Are you motivated by keeping yourself safe, your family and/or keeping your community healthier to get your flu shot?
Ask parents groups only: How has the situation with overcrowded childrens' hospitals due to respiratory illness through the fall and winter, impacted your decision to get your child the flu shot?
Ask all: How has the situation with overcrowded childrens' hospitals due to respiratory illness through the fall and winter, impacted your decision to get the flu shot?
Now thinking about vaccines in general…
Before the COVID-19 pandemic, did you usually get your recommended routine vaccinations? Why or why not?
(If needed, examples of recall vaccines include tetanus, hepatitis.)
What about now? Will you keep up to date with your recommended adult routine vaccinations, why or why not?
Ask parents groups only: What about your children's recommended routine vaccinations? Did you usually get your child's recommended routine vaccinations? Why or why not?
Ask parents groups only: What about your children's vaccination? Will you keep up to date with their recommended vaccinations? Why, or why not?
Exercice 3 – polling questions + discussion
You should now see a pop up appear on your screen. Please read the statement and indicate to what extent you agree or disagree with the statement [Agree, Disagree] Discuss:
- Recommended vaccinations provide adequate protection against vaccine preventable diseases.
- PROBE: Why? Why not?
- Ask parents group only: Recommended vaccinations provide my child with adequate protection against vaccine preventable diseases.
- PROBE: Why? Why not?
Has the COVID-19 pandemic increased your confidence in vaccines? Has it decreased your confidence in vaccines?
PROBE: If so, are their specific areas your confidence has increased or decreased? Such as vaccines' effectiveness of protection against illness, their safety, their necessity, etc?
Ask if time permits:
Before travelling to foreign countries, do you look up the recommended vaccines? And do you get the recommended vaccinations?
- PROBE: Why or why not?
Ask parents groups only: Has your opinion towards recommended routine vaccination for your child changed over time?
Ask parents groups only: Do you feel as if the COVID-19 vaccines and booster shots changed your opinion and intentions on your child's recommended routine vaccination?
IF NOT COVID-19: what made you change your mind in that regard?
Ask parents groups only: Whether you do get your children vaccinated or not, could you tell me more about what you base your vaccination decisions on?
- Do you have any concerns about side effects and safety?
- Do your concerns about side effects and safety change when your children reach a certain age?
- Does your view on PHMs have anything to do with it?
- Do social and personal factors such as culture, religion, or stigma associated with being vaccinated have anything to do with your decisions?
Examples if needed: external risk factors (i.e, perceived individual risk, disease profile, transmission levels in community, etc) or vaccine-specific fears/considerations (I.e., not enough testing concerns, MiDi (mis- and disinformation) about vaccine, action bias for medical interventions, etc)
Ask parents groups only: Has the increase in hospitalizations due to RSV, Flu and COVID-19 made you more likely to vaccinate your children against respiratory illnesses, why or why not?
If not covered previously by the participants
Ask only if time permits:
- Ask parents groups only: For those who were pregnant in the past 2 years and those trying to get pregnant, did this change your opinion on getting the COVID-19 vaccine and boosters? How did it affect your decision? Did you have any concern regarding breastfeeding?
- Did you research information prior to making your decision to get the COVID-19 vaccine/boosters? Where did you get your information from?
- Probe: Health professionals, internet in general, health Canada website, etc.
Ask all – not just women:Are you/were you afraid the vaccine would have an impact on your fertility? Why?
Now, Let's talk about public health measures.
| BLOC 4 | Public health measures |
|---|---|
| Length | 20 minutes |
Before we move on to the next questions, I'm going to show you videos - (I'll show you two videos in total for this section of our discussion) – Only show one video if short on time
During the holidays, you may have seen one of these ads [show the ads]
- Video 1: Help make our season's greeting safe (test, mask, wash hands)
- Video 2: Help make our season's greeting safe (test, improve ventilation, get vaccinated)
Do you think the public health measures guidance provided in the videos was relevant throughout the holiday season? Why or why not?
Do you think these types of ads should be repeated before other key holidays? Why or why not?
Did you follow any of the guidance provided in the videos above throughout the holiday season?
IF SO, which public health measures did you adhere to and why? Why not?
Do you think the public health measures guidance provided in the videos above are relevant when there is increase in circulation of respiratory viruses (e.g. flu, RSV, COVID-19)? Why, or why not?
| BLOC 5 | Conclusion |
|---|---|
| Length | 5 minutes |
That was all I wanted to discuss with you today. Before I let you go, do you have any final comments you would like to add on the topics we just discussed?
Resend MH resources in the chat section, conclude and end the meeting.
Thank you very much for your precious collaboration!
The present study deals with topics that you might have found distressing. If you feel the need to talk, here is a list of mental health resources you can consult:
- Mental health support: Get help
- Wellness Together Canada
- Get Help | Talk Suicide Canada
- The Hope for Wellness Helpline
Appendix H: Survey questionnaire – WAVE 20.
Thank you for agreeing to take part in this survey. We anticipate that the survey will take approximately 12 minutes to complete.
Background information
This research is being conducted by Léger Marketing, a Canadian public opinion research firm on behalf of Health Canada.
The purpose of this online survey is to collect opinions and feedback from Canadians that will be used by the Government of Canada to help inform government actions and decisions.
How does the online survey work? You are being asked to offer your opinions and experiences through an online survey. You have to be 18 or over in order to participate in this survey. We anticipate that the survey will take 12 minutes to complete. Your participation in the survey is completely voluntary, and you are able to withdraw at any time during the survey if you no longer wish to participate. Your responses are confidential and will only ever be reported in aggregate – never in any way that can identify any individual respondent or their responses. Your decision on whether or not to participate will not affect any dealings you may have with the Government of Canada. How is your personal information protected? The personal information you provide to Health Canada is governed in accordance with the Privacy Act and is being collected under the authority of section 4 of the Department of Health Act in accordance with the Treasury Board Directive on Privacy Practices. We only collect the information we need to conduct the research project. Why is your personal information collected?
We require your personal information such as demographic information to better understand the topic of the research. However, your responses are always combined with the responses of others for analysis and reporting; you will never be identified. What are your rights under the Privacy Act: In addition to protecting your personal information, the Privacy Act gives you the right to request access to and correction of your personal information.
If you are experiencing technical issues while responding to the survey, please contact Leger's technical support team at support@legeropinion.com.
Your help is greatly appreciated, and we look forward to receiving your feedback.
[GDR] What is your gender identity?
Gender refers to current gender which may be different from sex assigned at birth and may be different from what is indicated on legal documents.
Row:
[r1] Male
[r2] Female
[r96] Other
[r99] I prefer not to answer
[PROV] In which province or territory do you currently live?
Row:
[BC] British Columbia
[AB] Alberta
[SK] Saskatchewan
[MB] Manitoba
[ON] Ontario
[QC] Quebec
[NB] New Brunswick
[NS] Nova Scotia
[PE] Prince Edward Island
[NF] Newfoundland
[NT] Northwest Territories
[YK] Yukon
[NU] Nunavut
[YEAR] In what year and month were you born?
Choice:
[MONTH] MONTH
Choice:
[ch1] January
[ch2] February
[ch3] March
[ch4] April
[ch5] May
[ch6] June
[ch7] July
[ch8] August
[ch9] September
[ch10] October
[ch11] November
[ch12] December
[r1] I prefer not to answer
[AGE2] Would you be willing to indicate in which of the following age categories you belong?
Condition: (AGERef.r1)
Row:
[r0] Under 18
[r1] Between 18 and 24
[r2] Between 25 and 34
[r3] Between 35 and 44
[r4] Between 45 and 54
[r5] Between 55 and 64
[r6] 65 or older
[r9] I prefer not to answer
[ETHNIC] Do you identify as any of the following?
Select all that apply
Row:
[r1] Black
[r2] East Asian
[r3] Indigenous (First Nations, Inuk/Inuit, Métis)
[r4] Latin American
[r5] Middle Eastern
[r6] South Asian
[r7] Southeast Asian
[r8] White
[r96] Other (please specify)
[r97] None of the above
[r99] Prefer not to answer
[CHILD] Are you the parent or guardian of a child or children under 18 years of age living in your household?
Row:
[r1] Yes
[r2] No
[r99] Prefer not to answer
[CHILD_AGE] How old is/are the child/children?
Condition: (CHILD.r1)
Select all that apply
Row:
[r1] Under 6 months of age
[r2] Between 6 months and LESS than 5 years of age
[r3] 5 to 11 years of age
[r4] 12 to 17 years of age
[r99] Prefer not to answer
[Q89] Have you ever been infected with COVID-19?
Row:
[r1] Yes
[r2] No
[r3] I think so (not confirmed by a positive test, PCR or rapid test)
[r98] Don't know
[r99] Prefer not to answer
[Q130] Do you consider yourself to be at risk of more severe disease or outcomes from COVID-19 (e.g., are an older adult over age 60, are pregnant, have Down syndrome, have a chronic medical condition, are immunocompromised, or live with obesity, etc.)?
Row:
[r1] Yes
[r2] No
[r98] Unsure
[r99] Prefer not to answer
[Q155] How worried are you of becoming infected with COVID-19?
Row:
[r1] Very worried
[r2] Somewhat worried
[r3] A little worried
[r4] Not worried at all
[r98] Don't know
[Q156] Why are you not worried about becoming infected with COVID-19?
Condition: (Q155.r4 or Q155.r98)
Select all that apply.
Row:
[r1] I've contracted COVID-19 before and was not really sick
[r2] I've contracted COVID-19 before and know what to expect
[r3] I've contracted COVID-19, so I am immune
[r4] I am vaccinated, so I am immune
[r5] I am vaccinated so my symptoms would be mild
[r6] COVID-19 is not very dangerous
[r7] COVID-19 is just another flu
[r8] COVID-19 is here to stay
[r9] There are low levels of COVID-19 in my community
[r10] New variants of COVID-19 do not concern me
[r11] I have other, more important concerns
[r96] Other (specify)
[r98] Don't know
[Q157] Why are you worried about becoming infected with COVID-19?
Condition: (Q155.r1 or Q155.r2 or Q155.r3)
Select all that apply.
Row:
[r1] I've contracted COVID-19 and was really sick (e.g. severely sick or hospitalized)
[r2] I am worried about getting really sick
[r3] I am worried about getting significant complications from COVID-19 (e.g. long COVID)
[r4] I am worried about getting others sick
[r5] I am worried it will impact my work
[r6] I am worried it will impact my plans (e.g. events, concerts, vacations etc.)
[r7] I am worried about new variants
[r8] I'm worried to contribute to an already overwhelmed healthcare system
[r9] I'm worried about not being treated correctly because the healthcare system is overwhelmed
[r96] Other (specify)
[r98] Don't know
While we have tried to minimize any potential risks and discomfort, due to the nature of the questions pertaining to one's mental health, some participants may feel uneasy or uncomfortable when answering questions about their experiences. If at any time you feel uncomfortable during this part of the survey, you may choose to skip questions by selecting "prefer not to answer" or "don't know". At the end of this section, and the study, you will be provided contact information for free mental health services.
[Q1] What is your most pressing concern at this time?
Select only one.
Row:
[r1] Physical health
[r2] Mental health
[r3] Health of family and/or friends
[r5] Economy
[r11] Social isolation and/or loneliness
[r7] Personal financial situation
[r8] Returning to normal and/or uncertainty about the future
[r9] New COVID-19 variants
[r16] New or emerging viruses other than COVID-19
[r15] Easing or lifting of public health restrictions
[r17] Work or school pressures
[r18] Relationships with family or friends
[r19] Current events
[r20] Climate change
[r21] Overwhelmed healthcare system
[r96] Other, please specify:
[r97] I have no pressing concern
[r98] Don't know
[Q3C] How would you rate your overall mental health?
Row:
[r1] Very good
[r2] Good
[r3] Average
[r4] Bad
[r5] Very bad
[r98] Don't know
[Q171] Which of the following actions, if any, do you take to maintain good mental health on a regular basis?
Select all that apply.
Row:
[r1] I make sleep a priority
[r2] I exercise regularly
[r3] I engage in activities that I enjoy
[r4] I eat a healthy, well balanced diet
[r5] I take part in local events and get to know my neighbours
[r6] I find ways to get involved and give back to my community
[r7] I set realistic goals for myself
[r8] I create healthy, trusting relationships with people who accept and support me
[r9] I don't do anything, since I don't see the need
[r10] I do not know how to maintain good mental health
[r96] Other, please specify:
[r99] Prefer not to answer
[Q172] When you experience a challenge or something in your life that affects your mental health, how easy or difficult is it for you to manage a mental health challenge?
Row:
[r1] Very easy
[r2] Easy
[r3] Neither easy or difficult
[r4] Difficult
[r5] Very difficult
[r98] Don't know
[r99] Prefer not to answer
[Q173] How do you take care of your mental health when you experience a challenge or something in your life that affects your mental health?
Select all that apply.
Row:
[r1] I seek professional support from support workers, social workers, psychologists or other professionals
[r2] I reach out to friends and family
[r3] I exercise
[r4] I make sleep a priority
[r5] I participate in a relaxing activity (meditation, hobby, wellness app etc)
[r6] I search online for resources and support
[r7] I reach out to my faith or spiritual leaders
[r8] I use my employee assistance programs
[r9] I don't do anything or seek help
[r10] I do not know how to take care of my mental health when I am affected by experience or challenge
[r11] My mental health has never been affected by experience or challenge
[r96] Other, please specify:
[r99] Prefer not to answer
[Q174] What factors, if any, influence the services or resources you use to manage a mental health challenge?
Select all that apply.
Row:
[r1] Monetary cost
[r2] Availability of services or resources
[r3] Time needed to use a service or resource
[r4] Recommendations from primary health care provider or a general practitioner at a walk-in clinic
[r5] Recommendations from friends and family
[r6] It depends on how serious I feel the mental health challenge is at that specific moment (i.e., not very serious, somewhat serious, or very serious)
[r7] Worry of what others think
[r8] Shame that I need help
[r9] Fear of asking for help
[r10] I have never been in a situation where I would have needed to use mental health services or resources
[r96] Other, please specify:
[r99] Prefer not to answer
[Q175] Who or what would be your first step when seeking help for mental health support, if needed?
Select only one.
Row:
[r1] Your primary health care provider or a general practitioner at a walk-in clinic
[r2] Emergency services at a hospital
[r3] An urgent care clinic
[r4] Online resources/web-based services
[r5] Digital apps or platforms
[r6] Phone (including text) services
[r7] Your local government
[r8] Your provincial/territorial government
[r9] The Government of Canada
[r10] Community services
[r11] Family/friends
[r12] Employee assistance program
[r13] Your faith or spiritual leader
[r14] Search on Internet
[r96] Other, please specify:
[r99] Prefer not to answer
[Q176] For each of the following mental health supports, please tell us if you would know how to access them if you needed to.
Column:
[c1] Yes
[c2] No
[c98] Unsure
[c99] Prefer not to answer
Row:
[r1] Online/virtual support from support workers, social workers, psychologists or other professionals
[r2] In person support from support workers, social workers, psychologists or other professionals
[r3] Phone (including text) support
[r4] Resources and tips for taking care of yourself
[r5] Resources and/or services through your local government
[r6] Resources and/or services through your provincial/territorial government
[r7] Resources and/or services through the Government of Canada
[r8] Support from a local, or non-for profit organization
[r9] Digital apps or platforms
[Q177] How comfortable do you feel talking about your mental health needs with those closest to you?
Row:
[r1] Very comfortable
[r2] Somewhat comfortable
[r3] Neither comfortable nor uncomfortable
[r4] Somewhat uncomfortable
[r5] Very uncomfortable
[r97] I don't feel I have mental health needs
[r98] Don't know
[r99] Prefer not to answer
[Q4] In the past month, have you received any support for your mental health?
Row:
[r1] Yes
[r2] No
[r98] Don't know
[Q4B] What type of support have your received?
Condition: (Q4.r1)
Select all that apply.
Row:
[r1] Online/virtual support from support workers, social workers, psychologists or other professionals
[r2] In person support from support workers, social workers, psychologists or other professionals
[r3] Phone (including text) support
[r4] Resources and tips for taking care of yourself
[r5] Your primary health care provider
[r6] Resources and/or services through your local government
[r7] Resources and/or services through your provincial/territorial government
[r8] Resources and/or services through the Government of Canada
[r9] Through digital apps or platforms, like Wellness Together Canada
[r10] Support from local, or a non-for profit organization
[r11] Employee assistance programs
[r12] Your faith or spiritual leaders
[r96] Other, please specify:
[Q4C] Why have you not received any support for your mental health?
Condition: (Q4.r2)
Row:
[r1] You preferred to manage yourself
[r5] Access to care or support was limited (e.g., help was not readily available when I needed it)
[r15] I am currently on a waiting list or referral for support
[r2] You didn't know how or where to get this kind of help
[r3] You haven't gotten around to it (e.g., too busy)
[r4] Your job interfered (e.g., workload, hours of work or no cooperation from supervisor)
[r6] You didn't have confidence in the health care system or social services
[r7] You couldn't afford to pay
[r8] Insurance did not cover
[r9] You were afraid of what others would think of you
[r10] Language problem
[r11] I do not need support for my mental health
[r96] Other, please specify:
[r98] Don't know
[Q178A] To what extent do you agree or disagree with the following statements?
Column:
[c1] Strongly Agree
[c2] Somewhat Agree
[c3] Neither agree or disagree
[c4] Somewhat Disagree
[c5] Strongly disagree
[c98] Unsure / Not applicable
Row:
[r1] Mental health is interconnected with physical health, and central to overall health and well-being
[r2] I practice taking care of my mental health on a regular basis.
[r3] Doing something enjoyable contributes to good mental health.
[r4] Factors such as resiliency and coping contribute to good mental health.
[r5] Spirituality contributes to good mental health.
[r6] Perceived control over life contributes to good mental health.
[r7] I have enough time to take care of my mental health.
[r8] I know when I need help with my mental health
[Q178B] To what extent do you agree or disagree with the following statements?
Column:
[c1] Strongly Agree
[c2] Somewhat Agree
[c3] Neither agree or disagree
[c4] Somewhat Disagree
[c5] Strongly disagree
[c98] Unsure / Not applicable
Row:
[r1] I think I can manage my mental health struggles on my own.
[r2] I am aware of free mental health and substance use resources online or by phone.
[r3] I feel I have adequate access to mental health support services.
[r4] It's hard to ask for help if I'm struggling with my mental health.
[r5] I know how or where to get help for my mental health.
[r6] I can afford mental health support.
[r7] I can afford to see a mental health therapist such as a social worker, psychologist, or counsellor.
[Q179] Why do you think it is hard to ask for help if you are struggling with your mental health?
Condition: (Q178B.r4.c1 or Q178B.r4.c2 or Q178B.r4.c3 or Q178B.r4.c98)
Select all that apply
Row:
[r1] I am worried of what others would think of me
[r2] I am worried it will impact my job
[r3] I think I cannot afford mental health support
[r4] I do not think there are resources that could help me
[r5] I am not sure where to look for help
[r6] I don't have time
[r7] I'm not sure my concern would be understood
[r8] I don't trust the practitioners available to me
[r9] I don't think my concern warrants outside help
[r10] I am worried no one would understand
[r96] Other, please specify:
[r99] Prefer not to answer
[Q180] What kind of information would you like to find on a Government of Canada mental health website?
Please select up to 3 choices.
Row:
[r1] Links to crisis lines or distress centres
[r2] Links to organizations providing online counselling
[r3] Links to free support services
[r4] Violence and abuse information
[r5] Suicide prevention information
[r6] Tips for improving your mental health
[r7] Tips on how to cope with stress and life's challenges
[r8] How to talk about mental health
[r9] Information on substance use
[r10] Information on mental illness
[r96] Other, please specify:
[r99] Prefer not to answer
Because of the sensitive nature of mental health, the questions you were just asked in this survey may have upset you. If you were (or are) upset, please consider using free mental health services such as those listed below:
Get Help Here: https://www.canada.ca/mental-health Wellness Together Canada: https://www.wellnesstogether.ca/en-CA Talk Suicide Canada: https://talksuicide.ca/ The Hope for Wellness Helpline: https://www.hopeforwellness.ca/
[Q132] How many doses of a COVID-19 vaccine have you received?
Row:
[r1] 1 dose
[r2] 2 doses
[r3] 3 doses
[r4] 4 doses
[r5] 5 doses
[r97] None, I am not vaccinated against COVID-19
[r98] Not sure
[Q132B] Have you received a COVID-19 booster dose?
Condition: not(Q132.r97)
Row:
[r1] Yes, received one booster dose
[r2] Yes, received two booster doses
[r3] Yes, received three booster doses
[r4] No, have not received a booster dose
[Q159] When did you receive your most recent COVID-19 booster dose?
Condition: (Q132B.r1 or Q132B.r2 or Q132B.r3)
Row:
[r1] Less than 3 months ago
[r2] 3 – 6 months ago
[r3] 6 – months to a year ago
[r4] Over one year ago
[r5] I have not received a COVID-19 booster
[r98] Don't know
[Q154] How likely are you to keep your COVID-19 doses up to date (i.e. continue to receive them as you become eligible for additional doses)?
Condition: (Q132.r1 or Q132.r2 or Q132.r3 or Q132.r4 or Q132.r5)
Row:
[r1] Very likely
[r2] Somewhat likely
[r3] Not very likely
[r4] Not at all likely
[r98] Don't know
[Q93] What is the top reason you are unlikely or uncertain about keeping your COVID-19 doses up to date?
Condition: (Q154.r3 or Q154.r4 or Q154.r98)
Row:
[r1] I think I am protected enough with the current number of vaccine doses
[r16] I had short term non-serious side effects with the dose/doses I already got and don't want a booster because of this
[r21] I had long term side effects with the dose/doses I already got and don't want a booster because of this
[r4] I'm concerned about the safety of the booster dose
[r6] I'm concerned about the long-term effects of the vaccine
[r8] I prefer to wait a while before getting vaccinated
[r9] I'm fed up with getting vaccinated
[r17] I'm tired of being told what to do to protect my health
[r18] I recently had COVID-19 and need to wait the recommended time before getting my booster dose
[r19] I feel that the vaccine does not provide much protection as you can still get COVID-19 even if vaccinated
[r20] I am not exposed to risks of COVID-19 in my daily life and therefore feel that I do not need to receive a booster dose
[r22] Booster doses are not available in my area
[r23] I think it is unlikely that I will get infected with COVID-19
[r24] I have a fear of needles
[r25] It is no longer mandated for activities I do
[r96] Other, please specify:
[Q76] Among the following factors and thinking about the current COVID-19 situation, what would motivate you to get your booster dose?
Condition: (Q132B.r4)
Please select up to your top 3
Row:
[r1] Advice from my primary health care provider that it is recommended for me
[r4] Helping to get things back to normal
[r5] Being able to more safely spend time with friends and family in-person
[r6] Knowing that the majority of new COVID-19 cases are among those who have not received a booster
[r7] Knowing that the majority of new COVID-19 hospitalizations are among those who have not received a booster
[r15] Knowing that family and friends and those in my community are getting vaccinated
[r16] Being able to get my flu shot and additional COVID-19 dose at the same time
[r9] If getting boosted would make it more likely for my area to lift local public health restrictions (e.g. mandatory mask wearing, gathering limits, etc.)
[r10] Getting the vaccine at a convenient time and location
[r11] Receiving paid time off work to get a booster dose
[r12] A booster dose being made mandatory for all Canadians
[r13] More knowledge of the benefits and importance of booster doses
[r17] More knowledge about the safety of booster doses
[r14] Knowing it is a new COVID-19 vaccine formulation that is specific to latest variants
[r97] None of the above
[Q160] Have you ever been reluctant or hesitated to get a COVID-19 booster dose?
Condition: (Q132B.r1 or Q132B.r2 or Q132B.r3)
Row:
[r1] Yes
[r2] No
[r98] Don't know
[Q161] For which reasons were you reluctant to get a COVID-19 booster dose?
Condition: (Q160.r1)
Select all that apply.
Row:
[r1] I have concerns about the safety and/or side effects of having a COVID-19 booster dose
[r2] I think COVID-19 vaccines are not effective in protecting me from the virus
[r3] I am well protected after receiving two doses
[r4] I am not at high risk of getting COVID-19
[r9] I am not worried about COVID-19
[r5] I already had COVID-19
[r6] I had bad reactions to the previous doses
[r7] I have concerns getting it with the flu vaccine
[r8] I was waiting for an updated vaccine targeting new variants
[r96] Other reasons (please specify):
[Q162] What made you decide to get a COVID-19 booster dose despite your initial reluctance?
Condition: (Q160.r1)
Select all that apply.
Row:
[r1] High number of COVID-19 cases
[r2] I was recommended by a health care professional
[r3] I fear I may regret it later if I don't
[r4] It is required at my work place
[r5] Concerns over vaccination policies
[r6] Benefits are more important than risks
[r7] Advice from a friend or a family member
[r8] A vaccine targeting new variants (e.g. Omicron variant) is available
[r9] It was readily available to me nearby
[r10] Fear of being infected with COVID-19
[r11] Being pressured by a friend or a family member
[r96] Other reasons (please specify):
[Q134] If COVID-19 vaccines were offered as a routine vaccine (e.g. annually), how likely would you be to get one?
Row:
[r1] Very likely
[r2] Somewhat likely
[r3] Not very likely
[r4] Not at all likely
[r98] Don't know
[Q134B] What is the top reason you are unlikely or uncertain about getting a routine COVID-19 vaccine (e.g. annually)?
Condition: (Q134.r3 or Q134.r4 or Q134.r98)
Row:
[r1] I think I am protected enough with the current number of vaccine doses
[r2] I had side effects with the dose/doses I already got
[r3] I think I am protected enough because I had COVID-19
[r4] I'm concerned about the safety of an annual COVID-19 vaccine
[r5] I think I am protected enough because I was vaccinated AND I had COVID-19
[r6] I'm concerned about the long-term effects of the vaccine
[r7] I need more information on annual doses (e.g. why they are needed, benefits, safety, effectiveness, etc.)
[r8] I'm fed up with getting vaccinated
[r9] I'm tired of being told what to do to protect my health
[r10] I don't think the vaccine is effective enough against the spread of COVID-19
[r11] I feel that the vaccine does not provides enough protection against severe outcomes from COVID-19
[r12] I feel that the vaccine does not provide much protection as you can still get COVID-19 even if vaccinated
[r13] I am not exposed to risks of COVID-19 in my daily life and therefore feel that I do not need to receive a routine COVID-19 vaccine
[r14] I don't think COVID-19 infection is serious enough anymore to need routine COVID-19 vaccine (e.g. annually)
[r15] I have a fear of needles
[r16] I do other things to improve me immunity (eg. vitamins, sleep, supplements etc.)
[r96] Other, please specify:
[Q163] And what about if the COVID vaccines were offered twice a year, how likely would you be to get them?
Condition: (Q134.r1 or Q134.r2 or Q134.r98)
Row:
[r1] Very likely
[r2] Somewhat likely
[r3] Not very likely
[r4] Not at all likely
[r98] Don't know
[Q164] Have you seen, read or heard anything about the bivalent COVID-19 vaccine?
Row:
[r1] Yes
[r2] No
[r98] Don't know
[Q165] The bivalent COVID-19 vaccine targets the original COVID-19 and the omicron variant, which helps provide further protection against omicron strains. Based on this explanation, are you more or less likely to get a COVID-19 bivalent booster dose?
Row:
[r1] I am more likely
[r2] I am less likely
[r3] My opinion hasn't changed since I was going to get a bivalent booster dose anyways / Since I received a bivalent booster dose anyways
[r4] My opinion hasn't changed since I do not intend to get a bivalent booster dose
[r98] Don't know
[Q135] Thinking about your child(ren) aged 12-17, how many doses of a COVID-19 vaccine have they received?
Condition: (CHILD_AGE.r4)
Select all that apply
Row:
[r1] 1 dose
[r2] 2 doses
[r3] 3 doses
[r7] 4 doses
[r4] None. I will wait a bit before getting my child(ren) vaccinated
[r5] None. I will not get my child(ren) vaccinated
[r6] Not sure
[Q95] Thinking about your child(ren) aged 12-17, how likely are you to have them receive a booster dose of the COVID-19 vaccine?
Condition: (Q135.r1 or Q135.r2)
Row:
[r1] Very likely
[r2] Somewhat likely
[r3] Not very likely
[r4] Not at all likely
[r5] My child(ren) 12-17 has/have already received a booster dose
[r98] Don't know
[Q136] Thinking about your child(ren) aged 5-11, how many doses of a COVID-19 vaccine have they received?
Condition: (CHILD_AGE.r3)
Select all that apply
Row:
[r1] 1 dose
[r2] 2 doses
[r3] 3 doses
[r4] None. I will wait a bit before getting my child(ren) vaccinated
[r5] None. I will not get my child(ren) vaccinated
[r6] Not sure
[Q136B] Thinking about your child(ren) aged 5-11, now that a booster has been authorized for them how likely are you to have them receive one?
Condition: (Q136.r1 or Q136.r2 or Q136.r6)
Row:
[r1] Very likely
[r2] Somewhat likely
[r3] Not very likely
[r4] Not at all likely
[r5] My child(ren) 5-11 has/have already received a booster dose
[r98] Don't know
[Q110] Why are you not likely or not sure to have your child(ren) get a booster dose of a COVID-19 vaccine?
Condition: (Q95.r3 or Q95.r4 or Q95.r98) or (Q136B.r3 or Q136B.r4 or Q136B.r98)
Select up to 3 reasons.
Row:
[r1] I think they are protected enough with the current dose schedule
[r2] They had side effects with the dose/doses they already got
[r4] I'm concerned about the safety of the booster dose
[r5] I'm concerned about the long-term effects of the vaccine
[r6] I need more information on booster doses
[r7] I prefer to wait a while before getting vaccinated
[r15] I'm confused about when they should get a booster
[r8] I'm fed up with getting my children vaccinated
[r9] They don't need a booster because the new variants are becoming less severe
[r12] I do not see the need to get a booster because my child(ren) have already contracted COVID-19 after being vaccinated
[r13] They recently got COVID-19 and I don't know when to get their booster dose
[r16] I think adolescents have stronger immunity that protects them
[r14] My child is very anxious or fearful of vaccinations
[r17] COVID-19 is mild in children, so a booster is unnecessary
[r96] Other, please specify:
[Q98B] Thinking about your child(ren) between the ages of 6 months and under 5, have they received at least one dose of a COVID-19 vaccine?
Condition: (CHILD_AGE.r2)
Row:
[r1] Yes
[r2] No, I will wait a bit before getting my child(ren) vaccinated
[r3] No, I will not get my child(ren) vaccinated
[r98] Not sure
[Q28] Which of the following factors would make you more likely to vaccinate your child(ren) against COVID-19?
Condition: (Q98B.r2 or Q98B.r3 or Q98B.r98)
Please choose your top three.
Row:
[r1] Assurance from my health professional that the vaccines are safe for my children
[r6] Being able to get my child vaccinated at a convenient location in my community
[r7] Assurance that I can be with my child(ren) during the vaccination
[r9] Seeing or hearing about friends, family or others I know personally getting their child(ren) vaccinated
[r16] Receiving a financial incentive
[r18] More information on the potential long-term effects of my children being infected with COVID-19
[r19] More information on children who have received the COVID-19 vaccine, e.g. from clinical trials involving children or from real world use, including data on safety and effectiveness
[r20] International health organizations say the vaccine is safe for kids based on findings from testing around the world
[r21] More information on the benefits of vaccinating children, i.e. protection from severe illness and long COVID
[r22] More information on how vaccines work and build immunity in children
[r23] Getting more information about risks to children from COVID-19 (e.g. "Long COVID") and hospitalizations
[r24] Information about best timing of another dose, based on the risk in my community
[r25] If there is a COVID-19 outbreak in my child (children)'s school
[r26] If required for my child(ren) to attend school
[r15] Nothing would make me more likely to vaccinate my child(ren) against COVID-19
[r96] Other, please specify:
[r98] Don't know
[Q166] The bivalent COVID-19 vaccine targets the original COVID-19 virus strain and the omicron variant, which helps provide further protection against omicron strains. Based on this explanation, are you more or less likely to have your child(ren) get a COVID-19 bivalent booster dose?
Condition: (CHILD.r1)
Row:
[r1] I am more likely
[r2] I am less likely
[r3] My opinion hasn't changed since I was going to have my child(ren) get a bivalent booster dose anyways / Since my child(ren) already received the bivalent booster anyways
[r4] My opinion hasn't changed since I do not intent to have my child(ren) get a bivalent booster dose
[r98] Don't know
[Q142] How has the recent COVID-19 pandemic had an impact on your confidence in vaccinations in general?
Row:
[r1] I am a lot less confident now
[r2] I am somewhat less confident now
[r3] About the same as before
[r4] Somewhat more confident now
[r5] A lot more confident now
[r98] I don't know
[Q143] Why are you less confident in vaccinations?
Condition: (Q142.r1 or Q142.r2)
Select all that apply
Row:
[r1] COVID-19 vaccines have negatively impacted my view on vaccines in general
[r2] I have more concerns about the safety of vaccines in general
[r3] I now believe that vaccines do not have as much benefit in preventing severe outcomes
[r4] I now believe that vaccines in general does not have as much benefit in stopping the spread of viruses
[r5] The COVID-19 pandemic has shown that we have strong immune systems without vaccines
[r6] The COVID-19 pandemic has shown that vaccines do not work very well
[r7] The changing recommendations in vaccine schedules impacted my view on vaccines
[r96] Other:
[Q1B] How often do you follow each of the following public health measures?
Individual public health measures are actions you can use every day to help reduce the spread of COVID-19 and other respiratory illnesses. These measures are also sometimes called personal preventive practices. Examples include: staying home when sick; wearing a well-fitting respirator or mask, especially in public indoor settings; improving indoor ventilation in home or co-living settings; practicing respiratory etiquette and frequent hand hygiene; and cleaning and disinfecting high-touch surfaces and objects.
NOTE: In any questions below that refer to masks, the word mask refers to a respirator (e.g., N95, KN95), medical mask or non-medical mask.
Column:
[c1] Always
[c2] Often
[c3] Sometimes
[c4] Rarely
[c97] Never
[c98] Don't know/Not applicable
Row:
[r3] Staying home and away from others if you feel sick
[r7] Wearing a mask - when indoors in a public space or in an indoor space with people from outside your immediate household
[r8] Wearing a mask - when outside in a public space
[r11] Wearing a mask - inside with others when you're feeling sick
[r9] Improving ventilation when people from outside your immediate household are in your home (as examples: open windows and doors regularly, use a heating, ventilation and air conditioning (HVAC) system or run kitchen or bathroom exhaust fans)
[r10] Using individual public health measures when interacting with someone who is at risk of more severe disease or outcomes from COVID-19 (e.g., are an older adult over age 60, are pregnant, have Down syndrome, have a chronic medical condition, are immunocompromised, or live with obesity etc.)
[Q169] To what extent would you agree or disagree with reinstating mandatory public health measures (e.g. policies on masking, or capacity limits)?
Row:
[r1] Strongly agree
[r2] Somewhat agree
[r3] Neither agree or disagree
[r4] Somewhat disagree
[r5] Strongly disagree
[r98] Don't know
[Q170] Under what conditions would you support reinstating mandatory public health measures (e.g. policies on masking, or capacity limits).
Select all that apply.
Row:
[r1] If there is a local outbreak of COVID-19 cases
[r2] If there are a rising number of hospitalizations related to COVID-19
[r3] If there are a rising number of deaths related to COVID-19
[r4] If the health care or public health capacities are becoming overloaded
[r5] If the spread of COVID-19 is increasing
[r6] If there are new COVID-19 variants of concern
[r7] If there are other respiratory viruses in circulation (eg. seasonal flu)
[r8] I am not supportive at all to reinstate the mandatory PHMs
[Q151] How familiar are you with the potential long-term effects of having COVID-19 (also known as "long-COVID" or "post COVID-19 condition")?
Row:
[r1] Very familiar
[r2] Somewhat familiar
[r3] Not very familiar
[r4] Not at all familiar
[r98] Don't know
[Q152] How worried are you/would you be about developing longer-term symptoms from a COVID-19 infection?
Row:
[r1] Very worried
[r2] Somewhat worried
[r3] Not very worried
[r4] Not at all worried
[r98] Don't know
[Q153] What makes/would make you feel worried about long-term symptoms of COVID?
Condition: (Q152.r1 or Q152.r2)
Select all that apply.
Row:
[r1] Limitations to my working life
[r2] Limitations to my leisure/personal life
[r3] Uncertainty about my future health prospects
[r4] Being judged for my condition
[r5] Not knowing if others (friends, colleagues, employers, healthcare providers, etc.) will take my condition seriously
[r6] Difficulty in formally indicating my condition to employers, healthcare providers, and/or others
[r7] Difficulty in accessing benefits related to my condition (e.g. sick leave, disability)
[r8] Being terminated by my employer for my condition
[r9] Lack of information/resources on my condition
[r10] Lack of public acknowledgement from authority figures (government, etc.) on my condition
[r96] Other, please specify:
The last few questions are strictly for statistical purposes. All of your answers are completely confidential.
[LANGU] What is the language you first learned at home as a child and still understand?
Row:
[r1] English
[r2] French
[r96] Other
[r99] I prefer not to answer
[MINO] Do you identify as any of the following?
SELECT ALL THAT APPLY
Row:
[r3] A member of the LGBTQ2 community
[r4] A person with a disability
[r97] None of the above
[r99] I prefer not to answer
[IMM] Where were you born?
Row:
[r1] Born in Canada
[r2] Born outside Canada
[r99] I prefer not to answer
[YIMM] In what year did you move to Canada?
Condition: (IMM.r2)
[PAYS] What is your country of origin?
Condition: IMM.r2 and not(MainAutoCountry.r99)
[SCOL] What is the highest level of formal education that you have completed?
Select one only
Row:
[r1] Some high school or less
[r2] High school diploma or equivalent
[r3] Registered Apprenticeship or other trades certificate or diploma
[r4] College, CEGEP or other non-university certificate or diploma
[r5] University certificate or diploma below bachelor's level
[r6] Bachelor's degree
[r7] Postgraduate degree above bachelor's level
[r99] I prefer not to answer
[OCCUP] Which of the following categories best describes your current employment status? Are you...
Select one only
Row:
[r1] Working full-time (35 or more hours per week)
[r2] Working part-time (less than 35 hours per week)
[r3] Self-employed
[r4] Unemployed, but looking for work
[r5] A student attending school full-time
[r6] Retired
[r7] Not in the workforce (full-time homemaker, full-time parent, or unemployed and not looking for work)
[r96] Other employment status. Please specify.
[r99] I prefer not to answer
[REVEN] Which of the following categories best describes your total household income? That is, the total income of all persons in your household combined, before taxes?
Select one only
Row:
[r1] Under $20,000
[r2] Between $20,000 and under $40,000
[r3] Between $40,000 and under $60,000
[r4] Between $60,000 and under $80,000
[r5] Between $80,000 and under $100,000
[r6] Between $100,000 and under $150,000
[r7] $150,000 and above
[r99] I prefer not to answer