Testing Marketing Concepts for Palliative Care Public Education Campaign
Prepared for Health Canada
Supplier name: Earnscliffe Strategy Group
November 2022
This public opinion research report presents the results of focus groups conducted by Earnscliffe Strategy Group on behalf of Health Canada. The qualitative research was conducted in November 2022.
Cette publication est aussi disponible en français sous le titre : Mise à l'essai de concepts de marketing pour une campagne d'information sur les soins palliatifs
This publication may be reproduced for non-commercial purposes only. Prior written permission must be obtained from Health Canada. For more information on this report, please contact Health Canada at: hc.cpab.por-rop.dgcap.sc@canada.ca or at:
Health Canada, CPAB
200 Eglantine Driveway, Tunney's Pasture
Jeanne Mance Building, AL 1915C
Ottawa Ontario K1A 0K9
Catalogue Number: H14-434/2023E-PDF International Standard Book Number (ISBN): 978-0-660-48076-3 Related publications (registration number): H14-434/2023F-PDF
Mise à l'essai de concepts de marketing pour une campagne d'information aux soins palliatifs (Final Report, French) ISBN Number 978-0-660-48077-0
Earnscliffe Strategy Group (Earnscliffe) is pleased to present this report to Health Canada summarizing the results of the qualitative research conducted to test marketing concepts for the 2022-2023 Palliative Care Public Education Campaign.
In late 2017, the Framework on Palliative Care in Canada Act was passed by Parliament with all-party support. In the spring and summer of 2018, Health Canada consulted with provincial and territorial governments, federal departments, palliative care providers, and other national stakeholders, as well as people living with serious illness, caregivers, and other people in Canada to develop the Framework on Palliative Care in Canada.
The Framework on Palliative Care in Canada was followed by the Action Plan on Palliative Care, which aims to improve quality of life for people living with serious illness, families, and caregivers, and enhance access, quality of care, and health care system performance. The Government of Canada invested funding in the implementation of the Action Plan on Palliative Care in Budget 2021.
As part of the Action Plan, Health Canada has prioritized raising awareness and understanding of palliative care. One of the key elements identified was the launch of an education campaign targeting the public and health care providers who are not palliative care specialists. This campaign will have two phases:
Phase 1 (2023 and beyond): Targeting health/social care providers who are not palliative care specialists to build capacity and promote awareness of the benefits of a palliative approach to care for patient outcomes and quality of end of life.
Phase 2 (2023-24 and beyond): Targeting persons living with serious illness (including underserved populations), their family members, friends, and unpaid caregivers to support the gradual normalization of death and dying, increase grief literacy, and increase awareness of benefits of early palliative care.
As part of this commitment, Health Canada is developing creative marketing concepts that will be used as part of the campaign scheduled to launch in winter of 2022-23. This campaign will first aim to increase awareness and understanding of the benefits of introducing palliative care early - and in conjunction with - the treatment process, as well as the non-medical aspects of palliative care. It will then aim to raise awareness of the benefits of palliative care, increase understanding of how palliative care can improve quality of life until the end of life, and increase grief literacy and awareness of how to access support among people in Canada.
To inform the campaign strategy, Health Canada engaged Earnscliffe to conduct a comprehensive wave of qualitative research to test draft campaign elements. The main objectives of the research were to collect feedback on creative concepts to inform final creative development and to ensure the advertising campaign resonates with its intended target audiences and meets its objectives. The research will inform final creative development by determining the potential for effectiveness and the resonance of messages and concepts with target audiences. The total contract value of the research was $124,836.75 including HST.
To meet these objectives, Earnscliffe conducted a series of eighteen (18) online discussion groups. The target audiences included members of the general population living with serious illness, including those with a physical disability; Black and other people of colour; Indigenous people living off reserve; family, friends and/or unpaid caregivers of someone living with serious illness; and health/social care providers. One discussion group among each target audience was conducted with residents of Eastern Canada (Atlantic Canada, Quebec, and Ontario) in English, Eastern Canada (Atlantic Canada, Quebec, and Ontario) in French, and Western Canada (Manitoba, Saskatchewan, Alberta, British Columbia, and the Territories). This approach ensured we were able to include those living in official language minority communities (OLMCs). The focus groups were approximately 90 minutes in length.
It is important to note that qualitative research is a form of scientific, social, policy, and public opinion research. Focus group research is not designed to help a group reach a consensus or to make decisions, but rather to elicit the full range of ideas, attitudes, experiences, and opinions of a selected sample of participants on a defined topic. Because of the small numbers involved, the participants cannot be expected to be thoroughly representative in a statistical sense of the larger population from which they are drawn, and findings cannot reliably be generalized beyond their number. As such, results are directional only.
The key findings can be summarized as follows:
Context and understanding
While neither of the creative concepts were deemed to be unacceptable or inappropriate for the Government of Canada to use, several participants – including both health/social care providers and those living with serious illness – questioned the timing of such a campaign given the current state of the health care system and a sense that for a variety of reasons it is not currently able to meet the ideal standard of care.
Participants viewed the concepts from the assumption that palliative care was exclusively "end of life" care and often only the very final stages of that. Despite being shown and read a more comprehensive definition of palliative care that included far more than just end of life, many still maintained a default understanding of palliative care that was at odds with some messages introduced in the creative concepts.
Creative concepts
Overall preference favoured Concept B, and it was the preferred concept for most of the campaign target audiences with only those living with serious illness and a physical disability preferring Concept A.
Participants gravitated towards the overall design of Concept B. Through the colours, photos, and graphic elements, it conjured up feelings of warmth, serenity, softness as well as conveying comfort and support.
The photos in Concept B were very well received by participants. They liked the depiction of human touch, as well as the diversity of individuals featured – this was especially true among Black or other people of colour. There was also a preference for seeing photos of at least two people rather than an individual on their own.
Unlike Concept A, reaction to the graphic element was mostly positive. Participants across all audiences were able to draw connections, derive meaning, and find relevance with palliative care.
When the headlines were reviewed separately from the concept, participants often selected messaging from Concept B as their preferred messaging noting that the headlines were both informative as well as encouraging.
With respect to Concept A, the messaging and the empowering sentiment of the words were appreciated by most participants who interpreted them as an empowering message that conveyed one could make their own choices about their journey. Conversely, some were uncomfortable with the notion of palliative care patients being encouraged to take power or control given how debilitating some of their conditions can be and/or overwhelming these decisions are.
Unlike the messaging, most participants did not appreciate the colours or graphic elements as much as they did for Concept B. Most participants did not like the turquoise or lime green colours, finding them reminiscent of hospitals, and were confused by the bar graphics.
Participants really liked most of the photos in Concept A. Echoing Concept B, they especially liked those featuring human touch and featuring multiple people. As with Concept B, some photos depicting people smiling were perceived as inappropriate.
Additional campaign elements
There was almost unanimous preference for a Health Canada-branded campaign as opposed to a Government of Canada-branded campaign. Given the topic, palliative care and grief, participants felt Health Canada sponsorship was much more intuitive and relevant.
The myths and facts approach employed in a couple of the creative examples for Concept B was tremendously popular. What participants most appreciated about this approach was the invitation to factual and/or more information. It was noted that this would be particularly useful for this campaign given the stigma around, and misinterpretation of, palliative care.
With respect to the social media examples, there was unanimous preference across all target audiences for posts and/or stories that include a headline with the image, rather than exclusively an image.
Most health/social care providers said they prefer the term "patients" and felt that it was most appropriate in the context of palliative care, while some who fell under the "other" health/social care professionals category explained that current thinking in the field of medicine preferred the term "clients" as it avoided stigma surrounding being unwell.
Additional messaging preferences
While the term palliative care was widely assumed to be understood, the actual meaning and especially the breadth of the definition was not commonly understood. Of the other messages offered, many had heard the term "comfort care" and associated it with pain management. A few were familiar with the term "compassionate care" and linked it with a sense of pity.
When it came to living with a serious illness over an extended period, there seemed to be a split between preference for the term "journey" or "experience" with the former being seen as more personal and the latter being perceived as more reflective of a moment in time.
There was no consensus on grief-related messaging, except in resistance to the terms "cope with grief," which implied one has to get over their grief, and "understand your grief" which implied making an already difficult process even more challenging. The two most positively received were "move through your grief" and "work through your grief".
Regarding wording intended for the website, participants gravitated towards the message "Grief is a normal response, and your experience of grief will be unique. No one can tell you what the process will be or how long it will take. Grief takes as long as it takes."
Communication needs of family/friends/unpaid caregivers
Few had looked for information about palliative care and/or grief. Among those who had, it was typically for services available in their communities. When asked what they would most like to know, participants indicated they would be interested in learning more about the accessibility of palliative services, how one qualifies, and what grief supports are available after a loved one passes.
In terms of their communications behaviours and preferences, participants suggested that Health Canada should consider a broad-based campaign leveraging multiple communications channels and having information available in pharmacies, hospitals, and doctor's offices.
Where QR codes are concerned, most noted they use them when required, and agreed that it would be helpful to include on informational resources.
Research firm: Earnscliffe Strategy Group (Earnscliffe) Contract number: CW2237798-HT372-224664 Contract value: $124,836.75 Contract award date: August 18, 2022
I hereby certify as a representative of Earnscliffe Strategy Group that the final deliverables fully comply with the Government of Canada political neutrality requirements outlined in the Communications Policy of the Government of Canada and Procedures for Planning and Contracting Public Opinion Research. Specifically, the deliverables do not include information on electoral voting intentions, political party preferences, standings with the electorate or ratings of the performance of a political party or its leaders.
Signed:
Date: November 25, 2022
Stephanie Constable
Principal, Earnscliffe
Introduction
Earnscliffe Strategy Group (Earnscliffe) is pleased to present this report to Health Canada summarizing the results of the qualitative research conducted to test marketing concepts for the 2022-2023 Palliative Care Public Education Campaign.
In late 2017, the Framework on Palliative Care in Canada Act was passed by Parliament with all-party support. In the spring and summer of 2018, Health Canada consulted with provincial and territorial governments, federal departments, palliative care providers, and other national stakeholders, as well as people living with serious illness, caregivers, and other people in Canada to develop the Framework on Palliative Care in Canada.
The Framework on Palliative Care in Canada was followed by the Action Plan on Palliative Care, which aims to improve quality of life for people living with serious illness, families, and caregivers, and enhance access, quality of care, and health care system performance. The Government of Canada invested funding in the implementation of the Action Plan on Palliative Care in Budget 2021.
As part of the Action Plan, Health Canada has prioritized raising awareness and understanding of palliative care. One of the key elements identified was the launch of an education campaign targeting the public and health care providers who are not palliative care specialists. This campaign will have two phases:
Phase 1 (2023 and beyond): Targeting health/social care providers who are not palliative care specialists to build capacity and promote awareness of the benefits of a palliative approach to care for patient outcomes and quality of end of life.
Phase 2 (2023-24 and beyond): Targeting persons living with serious illness (including underserved populations), their family members, friends, and unpaid caregivers to support the gradual normalization of death and dying, increase grief literacy, and increase awareness of benefits of early palliative care.
As part of this commitment, Health Canada is developing creative marketing concepts that will be used as part of the campaign scheduled to launch in winter of 2022-23. This campaign will first aim to increase awareness and understanding of the benefits of introducing palliative care early - and in conjunction with - the treatment process, as well as the non-medical aspects of palliative care. It will then aim to raise awareness of the benefits of palliative care, increase understanding of how palliative care can improve quality of life until the end of life, and increase grief literacy and awareness of how to access support among people in Canada.
To inform the campaign strategy, Health Canada engaged Earnscliffe to conduct a comprehensive wave of qualitative research to test draft campaign elements. The main objectives of the qualitative research were to collect feedback on creative concepts to inform final creative development and to ensure the advertising campaign resonates with its intended target audience and meets its objectives.
Specifically, the main objectives of the initial qualitative research were to ensure the advertising campaign resonates with its intended target audience and meets its objectives, by:
determining how well the main messages are understood and perceived;
determining whether the ad concepts grab people's attention and what components (design, vocabulary, imagery, tone) are successful or not successful;
assessing the clarity of the concepts;
assessing the strengths and weaknesses of the ad concepts;
generating other suggestions for improvements; and,
exploring audience media habits to further supplement or support the media mix data used to inform advertising campaign design.
The research will inform final creative development by determining the potential for effectiveness and the resonance of messages and concepts with target audiences.
To meet these objectives, Earnscliffe conducted a series of eighteen (18) online discussion groups. The target audiences included members of the general population living with serious illness, including those with a physical disability; Black and other people of colour; Indigenous people living off reserve; family, friends and/or unpaid caregivers of someone living with serious illness; and health/social care providers. One discussion group among each target audience was conducted with residents of Eastern Canada (Atlantic Canada, Quebec, and Ontario) in English, Eastern Canada (Atlantic Canada, Quebec, and Ontario) in French, and Western Canada (Manitoba, Saskatchewan, Alberta, British Columbia, and the Territories). This approach ensured we were able to easily include those living in official language minority communities (OLMCs). The focus groups were approximately 90 minutes in length.
The table below shows the number of participants in each group:
Exhibit 1. Number of focus group participants by group
Group
Audience
Region/Language
No of recruits
No of participants
1
Those living with serious illness
Eastern Canada (E)
8
7
2
Health/Social care providers
Eastern Canada (E)
8
8
3
Those living with serious illness and a physical disability
Eastern Canada (E)
8
7
4
Health/Social care providers
Western Canada (E)
8
8
5
Those living with serious illness
Western Canada (E)
8
8
6
Those living with serious illness and a physical disability
Western Canada (E)
8
8
7
Those living with serious illness
Eastern Canada (F)
8
6
8
Black and other people of colour living with serious illness
Eastern Canada (E)
8
9
9
Black and other people of colour living with serious illness
Eastern Canada (F)
8
8
10
Black and other people of colour living with serious illness
Western Canada (E)
8
7
11
Those living with serious illness and a physical disability
Eastern Canada (F)
8
5
12
Family, friends, or unpaid caregivers
Eastern Canada (E)
8
7
13
Health/Social care providers
Eastern Canada (F)
8
6
14
Family, friends, or unpaid caregivers
Western Canada (E)
8
7
15
Indigenous people living with serious illness
Eastern Canada (F)
8
4
16
Indigenous people living with serious illness
Eastern Canada (E)
8
6
17
Family, friends, or unpaid caregivers
Eastern Canada (F)
8
6
18
Indigenous people living with serious illness
Western Canada (E)
8
7
Appended to this report are the recruitment screener, discussion guide, and materials tested in the focus groups.
It is important to note that qualitative research is a form of scientific, social, policy, and public opinion research. Focus group research is not designed to help a group reach a consensus or to make decisions, but rather to elicit the full range of ideas, attitudes, experiences, and opinions of a selected sample of participants on a defined topic. Because of the small numbers involved, the participants cannot be expected to be thoroughly representative in a statistical sense of the larger population from which they are drawn, and findings cannot reliably be generalized beyond their number. As such, results are directional only.
Detailed findings
This qualitative report is divided in five sections that summarize the overall context and understanding as well as specific reactions to the creative concepts, additional campaign elements and messaging, as well as communication needs.
The findings across region and demographics were generally consistent. Except where specifically identified, the findings also represent the combined results regardless of audience, region, or language (English and French). Quotations used throughout the report were selected to bring the analysis to life and provide unique verbatim commentary from participants across the country.
Context and understanding
There were overarching views shared that serve as important context for understanding the lens through which participants viewed the concepts.
While none of the concepts were deemed to be unacceptable or inappropriate for the Government of Canada to use in any way, several participants, including both health/social care providers and members of the general population living with life-liming illness (primarily in Western Canada), questioned the timing of such a campaign. Asked to explain their hesitation, these participants explained that the care described and conveyed in the concepts was the ideal, but not realistically possible given the current state of the health care system. Others were hopeful that this campaign signals increased focus and priority for the government around palliative care.
At a minimum, they felt that it was important to educate Canadians about palliative care; especially about how to be more empathetic in our society. For some health/social care providers, the emphasis of the campaign - and Concept B in particular - on having earlier conversations about palliative care was important and seemed to assuage any concerns about the timing of the campaign.
"My mother just passed under palliative care. The staff were amazing, but they didn't have access to the doctors they would have otherwise. This campaign is interesting timing with everything going on with healthcare. It's important in some ways, but it also should be fully accurate as to what is accessible and possible." - Family, friends, or unpaid caregivers; Western Canada in English
"I take away and I am hoping that government is putting priority into palliative care and more supports. There have been many failures during COVID for patients and clients." - Those living with serious illness and a physical disability; Western Canada in English
"I'm puzzled as to why the government feels it has to sell this to health care providers. The problem is access." - Health/Social care provider; Western Canada in English
"Right now the challenge is accessing palliative care. I worry about this campaign. Unless there is a plan to bolster care and access, this comes off as tone deaf. It is not easy to connect people to palliative care." - Health/Social care provider; Western Canada in English
Most participants began from the assumption that the concept of palliative care was exclusively "end of life" care and for many, the very final stages of that. This persisted over the course of the group discussions despite the fact participants were shown and read a definition that clearly articulated that palliative care extends far beyond just end of life and is available to more than just the patient. While several participants ended up remarking that one or both concepts provided new information about palliative care, most still maintained a default understanding that was at odds with some of the messages communicated in the concepts and which sometimes served to limit the effectiveness of the concept and did not seem to alter their understanding of the term.
"I was under the same impression of palliative care being for the end of life, particularly because I have a brother living with ALS for the past 14 years. He recently moved into hospice care this year. Good to know the difference between palliative and 'hospice' care." - Black or other people of colour living with serious illness; Eastern Canada in English
Creative concepts
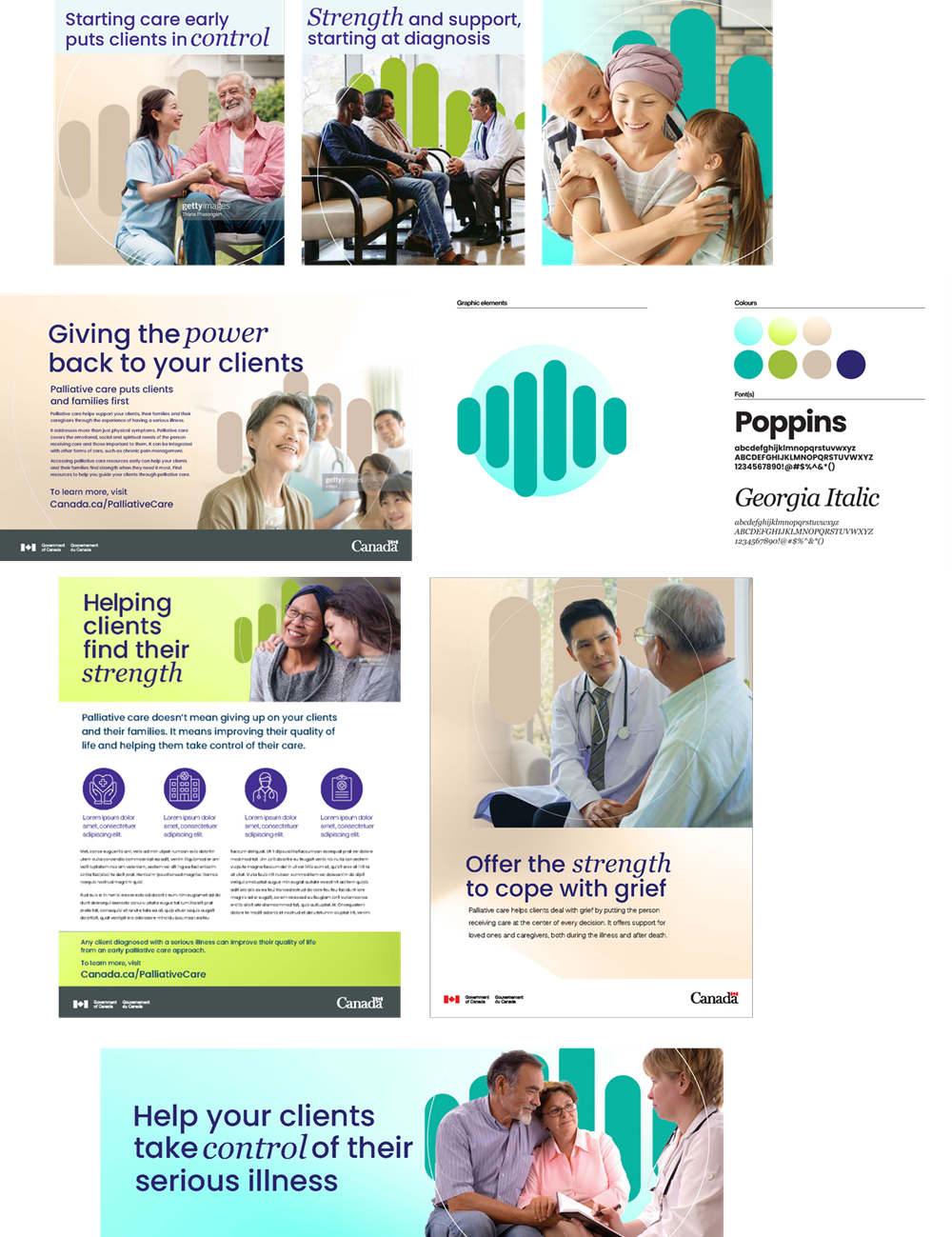
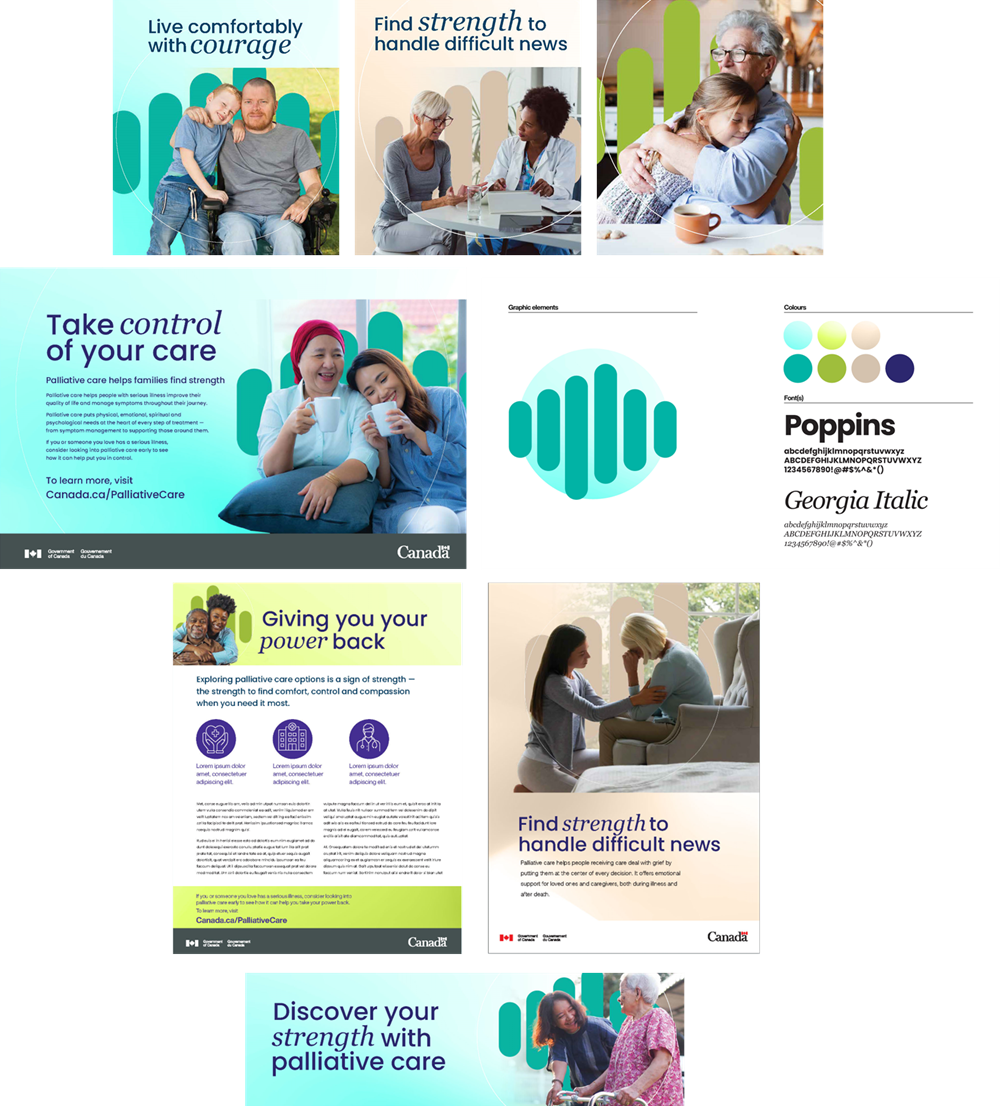
Participants were presented with two creative concepts which contained both visuals and wording. For each concept, a variety of examples of visual treatments were used to convey the overall look and feel of the concept. These examples included a style guide depicting the graphic elements, colours, and fonts; two posters; an information sheet; social media stories; and a website banner. Participants were asked to discuss their overall reactions to each concept, in the context of both the visuals and wording messages, and then to select their preferred concept.
The majority of participants, including most of the campaign target audiences, preferred Concept B. Those living with serious illness and a physical disability preferred Concept A; and family, friends, or unpaid caregivers were evenly split between the two concepts.
*One participant in the Black and other people of colour living with serious illness group in Eastern Canada in English did not respond to the preference question.
"Concept B is giving us the message we really needed." - Black and other people of colour living with serious illness; Eastern Canada in English
"This one [Concept B] shows what palliative care is really like; it shows more the reality of the patients. [Concept A] is more like a campaign; staged." - Those living with serious illness; Eastern Canada in English
"Concept B is friendlier and for everyone. It is more inclusive of everybody not just the patient. Concept A is for the person getting care. Concept B makes you want to read the words. It will reach a greater audience." - Those living with serious illness and a physical disability; Western Canada in English
"What attracted me most about Concept B is that we usually think of it at the end, but this is more about the journey. It's informative, educational. It raises public awareness. The colours are attractive. There are lots of ages and people of all disabilities." - Black and other people of colour living with serious illness; Eastern Canada in French
Though not presented with this option, some expressed a preference for a combination of both concepts.
"A hybrid would definitely work better." Black or other people of colour living with serious illness; Western Canada in English
"Can I get a third concept that combines Concept A and B?" - Family, friends, or unpaid caregivers; Eastern Canada in English
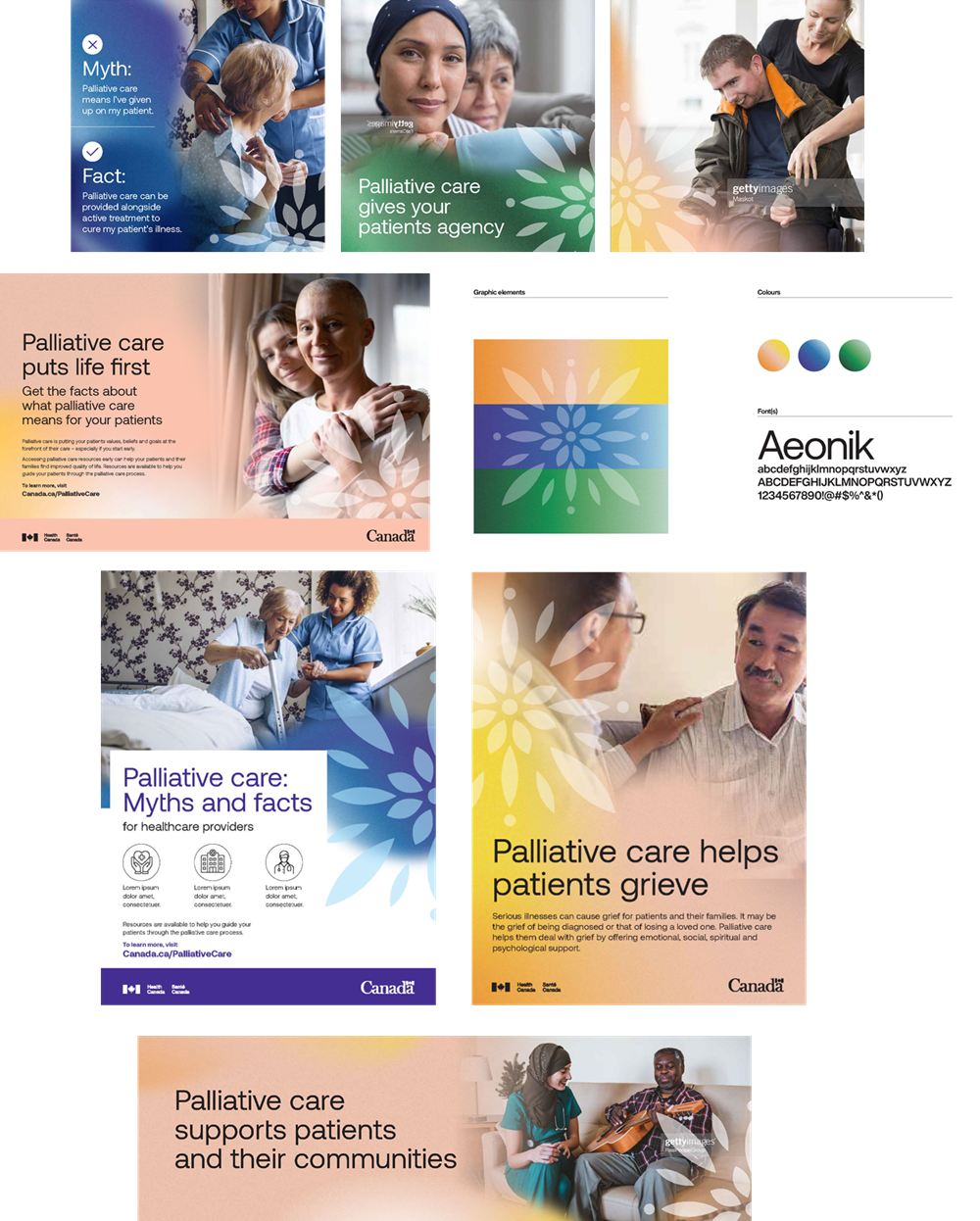
Concept B
More often than not, what participants appreciated most about Concept B was the overall design. Through the colours, photos, and graphic elements, it conjured up feelings of warmth, serenity, softness and was seen to convey comfort, and, more importantly, support which participants very much appreciated in the context of palliative care.
"I like the logo. It's zen. I like the colours. I like the images and seeing people helping people. There are more action shots of people helping and supporting others. It says to me that you can be sick but keep living." - Those living with serious illness; Eastern Canada in French
Participants were initially drawn to the colours. They were described as muted hues of primary colours. They were seen to be soft and complimentary to the photos and notably helped the people featured in the photos stand out. There was a further connection for several participants between the colours - yellow, blue, and green - to the sun, water, and the earth.
"I like the imagery in Concept B better. It uses warming tones. I particularly like the green, blue, and yellow. It's like the earth, sky, and sun." - Indigenous people living with serious illness; Eastern Canada in English
Most of the photos in Concept B were well received. Participants very much appreciated the depictions of human touch. This was seen to convey the message that those in palliative care would be supported, whether by health/social care providers, their family/loved ones, or caregivers. Participants also noted and appreciated the diversity of representation depicted throughout the concept: diversity of race, diversity of health/social care professionals, diversity of age, and diversity of ability.
"It's comforting. You feel like you aren't left alone. There's someone to help." - Family, friends, or unpaid caregivers; Eastern Canada in English
"I actually like Concept B. I am more of a visual learner, and this is more focused on the pictures than the words. Everything seems warming. There's always someone there touching." - Black and other people of colour living with serious illness; Eastern Canada in English
"All the pictures don't have someone in a white coat. It's showing different people and more different types of clinicians." - Health/Social care provider; Eastern Canada in English
Having noted that, there was a sense that some of the photos featured individuals who are too happy given the circumstances. A few also felt the photo on the fact sheet was a little more staged and did not convey the same warm and fuzzy feeling as the rest of the photos. Some appreciated the positive and encouraging feeling this conveyed while others were concerned that this did not align with all palliative care journeys.
"I don't think everyone going through palliative care is smiling that much. I think it's more serious." Black and other people of colour living with serious illness; Western Canada in English
"The photos are of people who don't need palliative care. They're smiling a lot." - Those living with serious illness and a physical disability; Eastern Canada in French
In contrast with Concept A, reaction to the graphic element was mostly positive. Participants across all audiences were able to find meaning, relevance, and connection with the graphic element (often referred to by participants as the logo) and palliative care. It was likened to the sun, a flower, a light, and the Big Bang and was interpreted as conveying hope, support, and warmth. Several Black or other people of colour felt it had human and religious significance. They described it as an explosion that brings one to eternity or the afterlife; and, for those who continue to live on in the absence of their loved one, it signifies a rebirth and new beginning.
"The flower reminds me of the mandala. Reminds me of the spiritual side of healing." - Those living with serious illness and a physical disability; Eastern Canada in English
"The logo comes from the bottom, and it explodes. It's like the Big Bang. It brings you to eternity. It's an explosion, a renaissance, and a rebirth for those left behind." - Black and other people of colour living with serious illness; Eastern Canada in French
"I see the before and after death." - Those living with serious illness and a physical disability; Eastern Canada in French
In terms of the graphic elements, the element that was received less favourably was the font. It was perceived as being too sharp-edged and not round enough. Those who felt this way, argued it was inconsistent with the soft feeling conveyed by the other design elements.
Where the messaging was concerned, while participants initially felt the headlines were a little wordy and lacked the punch of the headlines of Concept A, when reviewed in isolation, messages from Concept B were often felt to be more compelling and appropriate.
"The language is definitely more supportive in Concept B than Concept A." - Family, friends, or unpaid caregivers; Western Canada in English
"What I took away was that palliative care starts earlier than you think. It's not just at the end. It also goes beyond pain management and helps you grieve." - Those living with serious illness and a physical disability; Western Canada in English
"In my culture, it is taboo to talk about palliative care. We don't talk about it. Those who live this, do so in secret. Concept B strikes the right balance. The headlines help." - Black and other people of colour living with serious illness; Eastern Canada in French
The headline that seemed to resonate most for health/social care providers was "Palliative care puts life first". They described it as memorable and appreciated that it offered a different connotation than is traditionally associated with palliative care, i.e., life rather than death.
They also appreciated the messages "Palliative care supports clients/patients and their communities" and "Palliative care helps clients/patients grieve," as these put the focus on patients desire for support.
The headline "Palliative care gives your clients/patients agency" did not resonate with health/social care providers. They felt it was confusing and did not have much meaning.
For those living with serious illness and family, friends, or unpaid caregivers, the preferred headlines were "Palliative care starts earlier than you think" and "Palliative care may be more than you think". These were appreciated for the fact that they were informative, encouraging, and provided new information or a different interpretation about palliative care. Worth noting, a few, were uncomfortable with the interpretation that the end may be coming sooner than one would like to think.
"I like the statement that palliative care may start earlier than you think. From a paediatric community perspective there are services available that families have no idea about until they experience palliative care." - Family, friends, or unpaid caregivers; Western Canada in English
Those living with serious illness also appreciated the messages "Palliative care goes beyond pain management" and "Palliative care helps you grieve". For many, this was new information and information that they thought would be helpful. As we will see later, where grief is concerned, almost all are well aware of its individual and unpredictable nature.
Reaction to the message, "Find ways to live life to the fullest" was a little more mixed. Some, especially Black and other people of colour living with serious illness appreciated the sentiment that one is living until the very moment they die. Others felt that it was not always possible for those in palliative care.
Concept A
With regards to Concept A, participants most appreciated the messaging (headlines) and the empowering sentiments conveyed in the words: strength, power, courage, and control.
The sentiment was interpreted as an empowering message that conveyed one could make their own choices about their journey. Those appreciative of this sentiment, particularly those living with serious illness and a disability, or family, friends, and unpaid caregivers, rallied behind the notion that palliative care does not necessarily mean end-of-life. As mentioned above, this sentiment was also particularly relevant for Black and other people of colour living with serious illness. The empowering sentiment conveyed by the messaging was particularly relevant as a reminder that one has to advocate for their own health in Canada.
"I like the words used. They are words of empowerment. Palliative care is not actually related to death and dying. It's involved with treatment without curative. I am diabetic, there's no cure, so my care is palliative." Those living with serious illness; Western Canada in English
"I like the use of the very strong words - control, strength, and courage. It feels like you don't have those, and this shows that you do." - Those living with serious illness; Eastern Canada in English
Not all participants agreed that the messaging was appropriate, however, some were uncomfortable with the ideas of strength and power, and courage or control to a lesser extent, being associated with palliative care. Some spoke of their own experiences with care - or with providing care for patients in the case of health/social care providers - and noted that these were moments in which patients did not have the strength to conjure power, courage, or strength whether they wanted to or not. To illustrate this, one participant living with serious illness spoke of being in a coma.
A number of participants living with serious illness were uncomfortable with the notion of the patient being encouraged to take control. They offered examples of how overwhelming the decisions surrounding living with serious illness or end-of-life could be, and how much control doctors had over what healthcare options they had access to. Some highlighted the stress they felt, and the unfortunate need for a patient to have to advocate on their own behalf at a time when they were at their weakest and least able to handle this responsibility.
"Take control of your care is a very aggressive statement. Folks are in a very vulnerable state. Words like 'discover' appeals to me." Family, friends, or unpaid caregivers; Western Canada in English
"I am not sure about 'Take control of your care'. Some people can't get control of parts of their care." - Those living with serious illness; Eastern Canada in English
When asked about alternate language options that did not draw on the concepts of strength, participants offered notions of autonomy, independence, resilience. Many participants also stressed the importance of support from healthcare providers, family, friends, and loved ones more generally.
"They say I'm courageous, but we are all kind of courageous because you just deal with what's in front of you. I really think support is what is important and should be there." - Those living with serious illness; Western Canada in English
"I think the messaging is a little bit vague, and I think that sometimes we forget that it's not just for people who have the illness but it's also for their caregivers and their loved ones. So, it should say somewhere in there something for the support for the family and caregivers." Black or other people of colour living with serious illness; Western Canada in English
With regards to the graphical elements of Concept A, paralleling comments about Concept B, the depiction of human touch was identified as important. What participants appreciated a little bit more in the images in Concept A was that no one appeared alone in any of the photos. As with Concept B, some photos depicted smiling people in a way that some participants felt was too much given the circumstances. Others associated the photos with a corporate advertisement, such as something they might see from a life insurance company.
"The pictures are comforting, warming, close. It makes me feel comforted. It makes me feel happy that somebody is there, close by." - Those living with serious illness; Eastern Canada in English
"I feel like I am getting mixed signals from the imagery. Some are very happy, and some are very sad. Some we don't know what's going on." - Indigenous people living with serious illness; Eastern Canada in English
The bar graphic used in the images was confusing to most participants who felt that it distracted from the people featured in the images. When asked to interpret what the bars meant, many struggled and were not able to provide a response while a few others made comparison to other corporate logos or the cellular signal bars on a smartphone. Among those who made a connection to health and palliative care, they compared the bars to a pulse or a heartrate monitor, fingers on a hand, people standing together, the ups-and-downs of one's illness, or the stages of life.
"The starburst [Concept B] seems more jazzy. I felt like I didn't understand what the heart rate graphic was." - Those living with serious illness; Western Canada in English
"When I saw the graphic, it reminded me of cellular data. It's really busy and I don't know what it represents." - Those living with serious illness; Eastern Canada in English
"Feels like an advertisement from a private company providing these services, but it's supposed to be from the federal government. It doesn't look accessible to everyone." - Indigenous people living with serious illness; Eastern Canada in English
The colour scheme used in Concept A received a lukewarm reception. Those with more positive reactions highlighted that the colours were vibrant and eye-catching. That being said, most did not like the turquoise or lime green hues which were seen to be too jarring and to evoke unwelcome reminders of hospital settings. Of all the colours employed in Concept A, the beige was the best received. It was felt to be soft and comforting and the bars blended more into the background than the others.
"The colours are more institutional. It's more of a fact sheet. It's generic." - Indigenous people living with serious illness; Western Canada in English
"I'm struggling with it. It's almost a little bit too playful, and as much as I love the colours I don't like them for this." Black and other people of colour living with serious illness; Western Canada in English
"The colouring is too much." - Family, friends, or unpaid caregivers; Eastern Canada in English
Additional campaign elements
Following discussions of both concepts, participants were asked to provide their reaction to a number of different campaign elements.
When it came to the branding of the campaign, there was almost unanimous preference for a Health Canada-branded campaign as opposed to a Government of Canada-branded campaign. In light of the topic, palliative care and grief, participants felt Health Canada sponsorship was much more intuitive and relevant. It is worth noting that the distinction between Health Canada and the Government of Canada was identified as important - in particular for those with critical views of the latter.
"I didn't notice, but Health Canada makes more sense." - Those living with serious illness; Eastern Canada
"Health Canada is more relevant." - Family, friends, or unpaid caregivers; Eastern Canada in English
When it came to specific features of the concepts tested, the myths and facts approach employed in a couple of the examples in Concept B was tremendously popular. Some participants mentioned liking this approach spontaneously when reviewing it, while others agreed when they were specifically prompted. The invitation to additional information was appreciated, particularly since the group discussions demonstrated that there were misunderstandings surrounding a type of care that was previously believed to be well understood. The contrast of myths and facts was additionally seen as an effective way to foster curiosity in the subject, encourage further conversations, and to address some of the stigma and misinterpretations surrounding palliative care. Health/social care providers noted it would provide an opportunity to open the conversation with their patients/clients.
"Palliative care myths and facts are important. Patients have lots of questions. This opens the conversation with the patient." - Health/Social care provider; Eastern Canada in English
"This is a powerful tool. It's a good idea. There is lots of misunderstanding. I like to explain things to my patients." - Health/Social care provider; Eastern Canada in English
"Myths and facts is a punchier way to convey information." - Family, friends, or unpaid caregivers; Eastern Canada in English
"I really like the myth and fact element of it. It provides an element for people who don't know a lot about palliative care. And the photos are more realistic." - Those living with serious illness; Western Canada in English
"We all carry the misconception that palliative care is for end of life. That's why we all like the myths and facts approach because it highlights those and helps us to understand better." - Family, friends, or unpaid caregivers; Eastern Canada in English
"The myths really help explain my situation." - Those living with serious illness and a physical disability; Eastern Canada in English
Regarding social media examples, there was a unanimous preference across all target audiences for posts and stories that included a headline in addition to an image. This was felt by participants to provide important context for the ad and that ads without it were susceptible to misinterpretation. It was also noted that they would be more likely to scroll past an ad that did not have a headline.
Finally, asked whether they prefer the term "patients" or "clients", most health/social care providers said they prefer the term "patients" and felt that it was most appropriate in the context of palliative care. There were some, often "other" health/social care professionals (for example, pharmacist, therapist, personal support worker), who explained that current thinking in the field of medicine preferred the term "clients". They argued that "patient" has a negative connotation and implies people who are sick or unwell.
Additional messaging preferences
Participants were asked their understanding and preference for different wording options.
While the term palliative care was widely assumed to be understood, the actual meaning and especially the breadth of the definition were not widely or commonly understood. Asked whether there were other terms that they use or had heard before, health/social care providers often volunteered "supportive care", whereas, those living with serious illness or family, friends, or unpaid caregivers often volunteered "end-of-life care". Many across all audiences had heard the term "comfort care", which was closely linked to pain management and making sure that those living with serious illness are as comfortable as possible in their final days. Few across all audiences were familiar with the term "compassionate care". When asked, they offered that it conveyed a sense of pity.
"Specifically pain management, giving someone the ability to pass peacefully." - Those living with serious illness; Eastern Canada in English
"They try to make you comfortable, the patient and the loved ones. So 'comfort care' is more like it." - Black and other people of colour living with serious illness; Eastern Canada in English
To describe living with a serious illness from the beginning (diagnosis) to end of life or transition into the spirit world, there seemed to be a split between preference for the term "journey" or "experience". A "journey" seemed to have a beginning and an end and was more personal or individual. A few expressed that the fact a journey has an ending made it a less appealing term. Indigenous people living with serious illness tended to prefer the term "journey". An "experience" was interpreted as an activity or a moment in time.
With respect to grief-related language, there did not seem to be real consensus except in resistance to the term, "cope with grief" which implied one has to get over their grief and now. Most were not all that fond of "understand your grief" either as that suggested a difficult and painful process.
The two that were more positively received were, "move through your grief" and "work through your grief". They both captured what participants understand about grief: that grief is different for everyone, it takes time, as well as the (mis)perception that it involves different stages. Participants felt these were a little softer and appreciated that neither conveyed an expectation.
"'Work through grief' is good. Everyone works through it differently. Coping makes it seem like you need to be better now." - Those living with serious illness, Eastern Canada in English
"'Move through' implies that you don't need to do anything special with it." - Black and other people of colour living with serious illness; Eastern Canada in English
"I like 'move through.' There's lots of stages of grief, and that's what you actually do. It's a better description of the process." - Those living with serious illness; Eastern Canada in English
Among the messages intended for the website, participants resonated with the message, "Grief is a normal response, and your experience of grief will be unique. No one can tell you what the process will be or how long it will take. Grief takes as long as it takes." Those with more recent or powerful experiences with grief often noted that this statement really resonated with them.
"It's bang on. No one can tell you how to grieve." - Those living with serious illness; Western Canada in English
"This one is perfect." - Family, friends, or unpaid caregivers; Western Canada in English
It was also at this time that a number of participants offered that the power and impact of grief is not well understood or accommodated by employers. In these cases, participants usually raised the details of corporate policies that allowed for three days of grieving, which seemed remarkably insufficient for some cases of grief.
"It also needs to resonate with employers too. Grief is not always understood. Some people will need longer, and some people will need a couple days." - Black and other people of colour living with serious illness; Eastern Canada in English
"Three days just isn't enough. You're supposed to go back and act like everything is ok." - Family, friends, or unpaid caregivers; Western Canada in English
Communication needs of family/friends/unpaid caregivers
When time permitted some participants were asked a series of questions related to their information needs and preferences.
Few have looked for information about palliative care and/or grief. Those who had, typically looked for services available in their communities. Indeed, when asked what they would most like to know, participants indicated they would be interested in learning more about accessibility of palliative services, how one qualifies, and what grief supports are available for after a loved one passes.
In terms of their communications behaviours and preferences, they suggested information in pharmacies, hospitals, and doctor's offices given how much idle time they tend to spend in these facilities. They also suggested Health Canada should consider a broad-based campaign leveraging multiple communications channels (for example, television, radio, social media) to reach a more diverse population. Some also suggested providing information on public transit.
Where QR codes are concerned, most said they use them when they have to but are not in the habit of doing so. Asked if it would be helpful on some of the products they had reviewed, participants did think it would be. There was a sense that a QR code on a poster or pamphlet would be helpful for directed access to specific information; much easier than trying to remember a website address or typing a website address into a browser (and the need to type it correctly).
"I only use them when I have to. I'm not in the habit. But I do think they would be helpful on a pamphlet to get information. Much more efficient and direct then having to remember or type a website address; discourages typos." - Family, friends, or unpaid caregivers; Eastern Canada in French
"I've used QR codes. They're marvelous. I don't have to take the time to read the poster. I can get the information directly to my phone." - Those living with serious illness and a physical disability; Eastern Canada in French
Conclusions
To the extent that the purpose of this qualitative phase was to test creative concepts (both the visuals and wording messages) to gauge whether they were appealing, memorable, and motivating in terms of encouraging the intended audiences to seek out information about palliative care or grief, the findings suggest that there were compelling and persuasive elements worth considering. And, while there were preferences across the two creative concepts, there did not appear to be any major negative sentiment or reactions. It is certainly acceptable and appropriate for the Government of Canada to communicate in this way, though several questioned the timing of such a campaign given the current state of the health care system and the perceived limited access to palliative care.
Regardless of the specific concept, several key points emerged as particularly relevant for participants across audiences. First, that there is support and resources available for those who are seeking it. Second, that there is interest in raising public awareness to counter some of the misinterpretations and stigmas that currently exist surrounding palliative care. Third, that humanizing this experience and underscoring human connection is especially important. Finally, almost all participants, particularly those living with serious illness, do attach meaning to the term palliative care, however, it is somewhat inconsistent with Health Canada's broader definition and is very narrowly focused on end-of-life care.
In terms of the creative concepts, Concept B was preferred overall. The colours used in Concept B were described as more warm, comforting, and supportive and participants were able to draw connections between palliative care and the symbol used. Participants particularly appreciated the diversity of individuals featured in the photos and the scenes of human connection that conveyed the importance of support for those in palliative care. While participants also appreciated the human connection that featured in some of the photos in Concept A, the reactions to the graphic element and colours were lukewarm. Participants noted that, while the colours were attention grabbing, they also evoked unwelcome memories of hospitals. As for the bar graphic, it was met with confusion by many participants who likened it to - and all of Concept A - to something more appropriate for a corporate advertisement.
With regards to the wording messages, participants initially perceived those from Concept B to be less compelling than those in Concept A, mainly because they were not as concise and lacked punch. However, when the wording messages were reviewed on their own, participants often gravitated to the sentiment expressed in those of Concept B. Health/social care providers found that the messages that emphasised life rather than death resonated with them most, while those living with serious illness gravitated towards those that underlined the need for support. With respect to Concept A, the use of language focused on strength, courage, and taking control was somewhat polarizing. For some this was seen to be empowering and emphasized that one could make their own choices about their journey. For others who noted the vulnerability of those in these situations, this strong language was seen as out of touch and insensitive.
As for the additional messaging considered, health/social care providers offered the term "supportive care," while those living with serious illness, or family, friends, or unpaid caregivers often volunteered "end-of-life care". Comfort care was linked in the minds of many across all audiences to notions of pain management. When it came to language surrounding grief, the only consensus was in resistance to the suggestion to "cope with" grief which implied an imperative to get over their grief.
Also worth noting, the myths and facts approach used in Concept B was very well received with participants appreciating that it simultaneously worked to combat some of the misinterpretations surrounding palliative care while also inviting readers to search out more information. As for social media examples, there was a unanimous preference for those which featured a headline in addition to an image. With respect to the overall branding of the campaign, there was almost unanimous preference for a Health Canada-branded campaign as opposed to one associated with Government of Canada.
Finally, participants noted that their preference for a broad-based communication campaign that leveraged multiple communication channels (for example, television, radio, social media) and which overlapped with the physical spaces of care (for example, pharmacies, hospitals, doctor's offices).
Appendix A - Focus group methodology report
Methodology
The target audiences included health/social care providers who are not palliative care specialists; people in Canada living with serious illness, including those with physical disabilities; Black, Indigenous and Other People of Colour (BIPOC); and family, friends, or unpaid caregivers.
The groups were conducted with residents of Eastern Canada, including Atlantic Canada, Quebec, Ontario, and Western Canada, including the Prairies, British Columbia, and the Territories. Some of the groups with residents of Eastern Canada (NF, PE, NS, NB, QC, ON) were conducted in English, while some were conducted with residents of Eastern Canada (NB, QC, ON) in French.
Exhibit 2. Schedule and composition of the groups
Group
Audience
Region/Language
No of recruits
No of participants
Date/Time
1
Those living with serious illness
Eastern Canada (E)
8
7
Monday, November 7, 2022
4:00 pm ET / 5:00 pm AT / 5:30 pm NT
2
Health/Social care providers
Eastern Canada (E)
8
8
Monday, November 7, 2022
6:00 pm ET / 7:00 pm AT / 7:30 pm NT
3
Those living with serious illness and a physical disability
Eastern Canada (E)
8
7
Monday, November 7, 2022
6:00 pm ET / 7:00 pm AT / 7:30 pm NT
4
Health/Social care providers
Western Canada (E)
8
8
Monday, November 7, 2022
8:00 pm ET / 7:00 pm CT / 6:00 pm MT / 5:00 pm PT
5
Those living with serious illness
Western Canada (E)
8
8
Monday, November 7, 2022
8:00 pm ET / 7:00 pm CT / 6:00 pm MT / 5:00 pm PT
6
Those living with serious illness and a physical disability
Western Canada (E)
8
8
Tuesday, November 8, 2022
3:00 pm ET / 2:00 pm CT / 1:00 pm MT / 12:00 pm PT
7
Those living with serious illness
Eastern Canada (F)
8
6
Tuesday, November 8, 2022
5:00 pm ET / 6:00 pm AT
8
Black and other people of colour living with serious illness
Eastern Canada (E)
8
9
Tuesday, November 8, 2022
6:00 pm ET / 7:00 pm AT / 7:30 pm NT
9
Black and other people of colour living with serious illness
Eastern Canada (F)
8
8
Tuesday, November 8, 2022
7:00 pm ET / 8:00 pm AT
10
Black and other people of colour living with serious illness
Western Canada (E)
8
7
Monday, November 14, 2022
8:00 pm ET / 7:00 pm CT / 6:00 pm MT / 5:00 pm PT
11
Those living with serious illness and a physical disability
Eastern Canada (F)
8
5
Monday, November 14, 2022
5:00 pm ET / 6:00 pm AT
12
Family, friends, or unpaid caregivers
Eastern Canada (E)
8
7
Wednesday, November 9, 2022
6:00 pm ET / 7:00 pm AT / 7:30 pm NT
13
Health/Social care providers
Eastern Canada (F)
8
6
Wednesday, November 9, 2022
7:00 pm ET / 8:00 pm AT
14
Family, friends, or unpaid caregivers
Western Canada (E)
8
7
Wednesday, November 9, 2022
8:00 pm ET / 7:00 pm CT / 6:00 pm MT / 5:00 pm PT
15
Indigenous people living with serious illness
Eastern Canada (F)
8
4
Monday, November 14, 2022
7:00 pm ET / 8:00 pm AT
16
Indigenous people living with serious illness
Eastern Canada (E)
8
6
Thursday, November 10, 2022
6:00 pm ET / 7:00 pm AT / 7:30 pm NT
17
Family, friends, or unpaid caregivers
Eastern Canada (F)
8
6
Thursday, November 10, 2022
7:00 pm ET / 8:00 pm AT
18
Indigenous people living with serious illness
Western Canada (E)
8
7
Thursday, November 10, 2022
8:00 pm ET / 7:00 pm CT / 6:00 pm MT / 5:00 pm PT
The focus group participants received an honorarium of as a token of appreciation for their time:
Specialists: $700
Family physicians/general practitioners: $400
Nurses and other health/social care providers: $350
Those living with serious illness and a physical disability: $150
Those living with serious illness, including Black or other people of colour, Indigenous peoples as well as family, friends, or unpaid caregivers: $125
All focus groups were conducted between November 7 and November 14, 2022.
Recruitment
Participants were recruited using a recruitment screener (see Appendix B for health/social care providers and Appendix C for those living with serious illness).
The target audiences included health/social care providers who are not palliative care specialists; people in Canada living with serious illness, including those with physical disabilities; Black, Indigenous and Other People of Colour (BIPOC); and family, friends, or unpaid caregivers of those living with serious illness.
For the groups with health/social care providers, we aimed for two family physicians or general practitioners, two specialists, two nurses and two who meet the criteria for "other health/social care provider". "Other health/social care provider" referred to those who work in/as: social work, occupational therapists, physiotherapists, speech therapy, respiratory therapists, spiritual counsellors, other counsellors, pharmacists, other long-term care and home care staff, case managers/workers, or shelter workers. Additionally, we ensured a good mix of care settings.
For the groups with those living with serious illness or family, friends, or unpaid caregivers, we ensured a good mix of other demos (province within regions, age, gender, income, education, household type, urban/suburban/rural, etc.).
Our field work subcontractor, Quality Response, and their selected suppliers reached out to members of their respective databases first via email and followed up with telephone calls to pre-qualify participants. They then conducted telephone recruitment to supplement in each market.
Moderation
Given the accelerated timeline, two moderators were used to conduct the focus groups. Each moderator took notes and summarized their groups and subsequently met to provide the other with a debrief on the groups, including the key findings.
A note about interpreting qualitative research results
It is important to note that qualitative research is a form of scientific, social, policy, and public opinion research. Focus group research is not designed to help a group reach a consensus or to make decisions, but rather to elicit the full range of ideas, attitudes, experiences, and opinions of a selected sample of participants on a defined topic. Because of the small numbers involved the participants cannot be expected to be thoroughly representative in a statistical sense of the larger population from which they are drawn, and findings cannot reliably be generalized beyond their number.
Glossary of terms
The following is a glossary of terms used throughout the report. These phrases are used when groups of participants share a specific point of view. Unless otherwise stated, it should not be taken to mean that the rest of participants disagreed with the point; rather others either did not comment or did not have a strong opinion on the question.
Exhibit 3. Glossary of qualitative terms
Generalization
Interpretation
Few
Few is used when less than 10% of participants have responded with similar answers.
Several
Several is used when fewer than 20% of the participants responded with similar answers.
Some
Some is used when more than 20% but significantly fewer than 50% of participants with similar answers.
Many
Many is used when nearly 50% of participants responded with similar answers.
Majority/Plurality
Majority or plurality are used when more than 50% but fewer than 75% of the participants responded with similar answers.
Most
Most is used when more than 75% of the participants responded with similar answers.
Vast majority
Vast majority is used when nearly all participants responded with similar answers, but several had differing views.
Unanimous/Almost all
Unanimous or almost all are used when all participants gave similar answers or when the vast majority of participants gave similar answers and the remaining few declined to comment on the issue in question.
Appendix B - Recruitment screener - Health/Social care providers
Focus Group Summary
Recruit 8 participants per group
Groups are 90 minutes in length
Three groups with health/social care providers
Aim for two family physicians/GPs, two specialists, two nurses and two who meet the criteria for other "health care/social care professionals"
Ensure good mix of care settings
Group #
Audience
Region/Language
Time
Monday, November 7, 2022
1 (SC)
General population with a serious illness
East - NL, PEI, NS, NB, QC, ON (EN)
4:00 pm ET / 5:00 pm AT / 5:30 pm NT
2 (SC)
Health/Social care providers
East - NL, PEI, NS, NB, QC, ON (EN)
6:00 pm ET / 7:00 pm AT / 7:30 pm NT
3 (DA)
Those with a serious illness and a physical disability
East - NL, PEI, NS, NB, QC, ON (EN)
6:00 pm ET / 7:00 pm AT / 7:30 pm NT
4 (SC)
Health/Social care providers
West - MB, SK, AB, BC, Territories (EN)
8:00 pm ET / 7:00 pm CT / 6:00 pm MT / 5:00 pm PT
5 (DA)
General population with a serious illness
West - MB, SK, AB, BC, Territories (EN)
8:00 pm ET / 7:00 pm CT / 6:00 pm MT / 5:00 pm PT
Tuesday, November 8, 2022
6 (SC)
Those with a serious illness and a physical disability
Interviewer:
Date:
Validated:
Quality Central:
On list:
On quotas:
Hello/Bonjour, this is [ ] calling on behalf of Earnscliffe, a national public opinion research firm. We are organizing a series of discussion groups on issues of importance on behalf of the Government of Canada, specifically Health Canada. The Government of Canada would like to understand people in Canada's views to help inform the development of a future advertising campaign. We are looking for health and social care providers who would be willing to participate in a 90-minute online discussion group. Up to 8 participants will be taking part and for their time, participants will receive an honorarium. May I continue?
Yes CONTINUE
No THANK AND TERMINATE
Participation is voluntary. We are interested in hearing your opinions; no attempt will be made to sell you anything or change your point of view. The format is a 'round table' discussion led by a research professional. All opinions expressed will remain anonymous and views will be grouped together to ensure no particular individual can be identified. I would like to ask you a few questions to see if you or someone in your household qualify to participate. This will take about three minutes. May I continue?
Yes CONTINUE
No THANK AND TERMINATE
Monitoring text:
READ TO ALL: "This call may be monitored or audio taped for quality control and evaluation purposes.
ADDITIONAL CLARIFICATION IF NEEDED:
To ensure that I (the interviewer) am reading the questions correctly and collecting your answers accurately;
To assess my (the interviewer) work for performance evaluation;
To ensure that the questionnaire is accurate/correct (i.e. evaluation of CATI programming and methodology - we're asking the right questions to meet our clients' research requirements - kind of like pre-testing)
If the call is audio taped, it is only for the purposes of playback to the interviewer for a performance evaluation immediately after the interview is conducted or it can be used by the Project Manager/client to evaluate the questionnaire if they are unavailable at the time of the interview - all audio tapes are destroyed after the evaluation.
Are you a specialist in palliative care? That is, do you have postgraduate training/specific advanced credentialing in palliative care and/or does your practice focus on palliative care and consultation for people and families or caregivers affected by serious conditions, especially those with complex needs?
Yes [THANKS AND TERMINATE]
No [CONTINUE]
Which of the following best describes your professional designation?
Physician - general practitioner [2 PER GROUP]
Physician - specialist [2 PER GROUP]
Registered nurse [2 PER GROUP]
Nurse practitioner [2 PER GROUP]
Licenced practical nurse/Registered practical nurse [2 PER GROUP]
None of the above
[IF NONE OF THE ABOVE] Which of the following, if any, describe your line of work or profession? [CHECK ALL THAT APPLY] 2 FROM ANY OF THE FOLLOWIING PER GROUP, AIM FOR A MIX
In which care setting do you spend most of your time? [ENSURE GOOD MIX]
Primary care
Outpatient clinic
Long-term care facility/Residential care
Home care
Community care
Hospital/Rehabilitation centre
Shelter
Community health centre/ clinic
Another care setting
In which province or territory do you live?
Newfoundland and Labrador
Nova Scotia
New Brunswick
Prince Edward Island
Quebec
Ontario
Manitoba
Saskatchewan
Alberta
British-Columbia
Nunavut
Northwest Territories
Yukon
EAST (EN): 1 FROM ATLANTIC CANADA, 3 FROM QUEBEC, 4 FROM ONTARIO EAST (FR): 1 FROM ATLANTIC CANADA, 5 FROM QUEBEC, 2 FROM ONTARIO WEST (EN): 1 FROM MANITOBA, 1 SASKATCHEWAN, 2 FROM ALBERTA, 3 FROM BRITISH COLUMBIA, 1 FROM TERRITORIES
What is your racial and/or ethnic background? [SELECT ALL THAT APPLY.]
Black (African, Afro-Caribbean, African-Canadian descent)
East Asian (Chinese, Korean, Japanese, Taiwanese descent)
Indigenous (First Nations, Inuit, Métis)
Latin American (Hispanic descent)
Middle Eastern (West Asian or North African descent, e.g. Afghan, Egyptian, Iranian)
South Asian (Indian, Pakistani, Sri Lankan, Indo-Caribbean descent)
Southeast Asian (Filipino, Vietnamese, Cambodian, Thai descent)
White (European descent)
Prefer not to answer
In what year did you start practising/working in your profession? [RECORD YEAR] ENSURE GOOD MIX
What gender do you identify with? [ENSURE GOOD MIX]
Male
Female
Non-binary person
Two spirit
Another gender identify
Prefer not to answer
Would you describe the area in which you work as… ENSURE GOOD MIX
Urban
Suburban
Rural
Prefer not to answer
Have you participated in a discussion or focus group before? A discussion group brings together a few people in order to know their opinion about a given subject.
Yes [MAX 2 PER GROUP, ASK S11, S12, S13]
No [SKIP TO S14]
Don't know/Prefer not to answer [THANK AND TERMINATE]
When was the last time you attended a discussion or focus group?
If within the last 6 months [THANK AND TERMINATE]
If not within the last 6 months [CONTINUE]
Don't know/Prefer not to answer [THANK AND TERMINATE]
How many of these sessions have you attended in the last five years?
If 4 or less [CONTINUE]
If 5 or more [THANK AND TERMINATE]
Don't know/Prefer not to answer [THANK AND TERMINATE]
This research will require participating in a video call online.
Do you have access to a computer, smartphone or tablet with high-speed internet which will allow you to participate in an online discussion group?
Yes [CONTINUE]
No [THANK AND TERMINATE]
Does your computer/smartphone/tablet have a camera that will allow you to be visible to the moderator and other participants as part of an online discussion group?
Yes [CONTINUE]
No [THANK AND TERMINATE]
Do you have a personal email address that is currently active and available to you?
Yes [CONTINUE, PLEASE RECORD EMAIL]
No [THANK AND TERMINATE]
INVITATION
Participants in discussion groups are asked to voice their opinions and thoughts. How comfortable are you in voicing your opinions in front of others? Are you…? (READ LIST)
Very comfortable [MINIMUM 4 PER GROUP]
Fairly comfortable [CONTINUE]
Comfortable [CONTINUE]
Not very comfortable [THANK AND TERMINATE]
Not at all comfortable [THANK AND TERMINATE]
Don't know/Prefer not to answer [THANK AND TERMINATE]
Sometimes participants are asked to read text, review images, or type out answers during the discussion. Is there any reason why you could not participate?
Yes [ASK S19]
No [SKIP TO S20]
Don't know/Prefer not to answer [THANK AND TERMINATE]
Is there anything we could do to ensure that you can participate?
Yes [ASK S20]
No [THANK AND TERMINATE]
Don't know/Prefer not to answer [THANK AND TERMINATE]
What specifically? [OPEN END] INTERVIEWER TO NOTE FOR POTENTIAL ONE-ON-ONE INTERVIEW
Based on your responses, it looks like you have the profile we are looking for. I would like to invite you to participate in a small group discussion, called an online focus group, we are conducting at [TIME], on [DATE]. As you may know, focus groups are used to gather information on a particular subject matter. The discussion will consist of about 6 people and will be very informal.
It will last up to 90 minutes and you will receive an incentive of… [FAMILY/GENERAL PRACTITIONER] $400; [SPECIALIST] $700; [NURSES AND OTHER] $350
…as a thank you for your time. Would you be willing to attend?
Yes [RECRUIT]
No [THANK AND TERMINATE]
Don't know/Prefer not to answer [THANK AND TERMINATE]
PRIVACY QUESTIONS
Now I have a few questions that relate to privacy, your personal information and the research process. We will need your consent on a few issues that enable us to conduct our research. As I run through these questions, please feel free to ask me any questions you would like clarified.
P1) First, we will be providing a list of respondents' first names and profiles (screener responses) to the moderator so that they can sign you into the group. Do we have your permission to do this? I assure you it will be kept strictly confidential.
Yes [GO TO P2]
No [GO TO P1A]
We need to provide the first names and background of the people attending the focus group because only the individuals invited are allowed in the session and this information is necessary for verification purposes. Please be assured that this information will be kept strictly confidential. GO TO P1A
P1a) Now that I've explained this, do I have your permission to provide your first name and profile?
Yes [GO TO P2]
No [THANK & TERMINATE]
P2) A recording of the group session will be produced for research purposes. The recordings will be used by the research professional to assist in preparing a report on the research findings and may be used by the Government of Canada to inform their work in this subject area.
Do you agree to be recorded for research and reporting purposes only?
Yes [THANK & GO TO P3]
No [READ RESPONDENT INFO BELOW & GO TO P2A]
It is necessary for the research process for us to record the session as the researchers need this material to complete the report.
P2a) Now that I've explained this, do I have your permission for recording?
Yes [THANK & GO TO P3]
No [THANK & TERMINATE]
P3) Employees from the Government of Canada and the creative agency working with the Government of Canada to develop the advertising campaign may also be online to observe the groups.
Do you agree to be observed by Government of Canada employees and employees of the creative agency?
Yes [THANK & GO TO INVITATION]
No [GO TO P3A]
P3a) It is standard qualitative procedure to invite clients, in this case, Government of Canada employees, and employees of the creative agency hired to develop an advertising campaign by the Government of Canada, to observe the groups online. They will be there simply to hear your opinions firsthand although they may take their own notes and confer with the moderator on occasion to discuss whether there are any additional questions to ask the group.
Do you agree to be observed by Government of Canada employees and employees of the creative agency?
Yes [THANK & GO TO INVITATION]
No [THANK & TERMINATE]
INVITATION
Wonderful, you qualify to participate in one of our discussion sessions. As I mentioned earlier, the group discussion will take place on [DATE] at [TIME] for up to 90 minutes.
Group #
Audience
Region/Language
Time
Monday, November 7, 2022
1 (SC)
General population with a serious illness
East - NL, PEI, NS, NB, QC, ON (EN)
4:00 pm ET / 5:00 pm AT / 5:30 pm NT
2 (SC)
Health/Social care providers
East - NL, PEI, NS, NB, QC, ON (EN)
6:00 pm ET / 7:00 pm AT / 7:30 pm NT
3 (DA)
Those with a serious illness and a physical disability
East - NL, PEI, NS, NB, QC, ON (EN)
6:00 pm ET / 7:00 pm AT / 7:30 pm NT
4 (SC)
Health/Social care providers
West - MB, SK, AB, BC, Territories (EN)
8:00 pm ET / 7:00 pm CT / 6:00 pm MT / 5:00 pm PT
5 (DA)
General population with a serious illness
West - MB, SK, AB, BC, Territories (EN)
8:00 pm ET / 7:00 pm CT / 6:00 pm MT / 5:00 pm PT
Tuesday, November 8, 2022
6 (SC)
Those with a serious illness and a physical disability
Black and other people of colour with a serious illness
East - NL, PEI, NS, NB, QC, ON (EN)
6:00 pm ET / 7:00 pm AT / 7:30 pm NT
9 (SC)
Black and other people of colour with a serious illness
East - NB, QC, ON (FR)
7:00 pm ET / 8:00 pm AT
10 (DA)
Black and other people of colour with a serious illness
West - MB, SK, AB, BC, Territories (EN)
8:00 pm ET / 7:00 pm CT / 6:00 pm MT / 5:00 pm PT
Wednesday, November 9, 2022
11 (SC)
Those with a serious illness and a physical disability
East - NB, QC, ON (FR)
5:00 pm ET / 6:00 pm AT
12 (DA)
Family/Friends/Caregivers
East - NL, PEI, NS, NB, QC, ON (EN)
6:00 pm ET / 7:00 pm AT / 7:30 pm NT
13 (SC)
Health/Social care providers
East - NB, QC, ON (FR)
7:00 pm ET / 8:00 pm AT
14 (DA)
Family/Friends/Caregivers
West - MB, SK, AB, BC, Territories (EN)
8:00 pm ET / 7:00 pm CT / 6:00 pm MT / 5:00 pm PT
Thursday, November 10, 2022
15 (SC)
Indigenous people with a serious illness
East - NB, QC, ON (FR)
5:00 pm ET / 6:00 pm AT
16 (DA)
Indigenous people with a serious illness
East - NL, PEI, NS, NB, QC, ON (EN)
6:00 pm ET / 7:00 pm AT / 7:30 pm NT
17 (SC)
Family/Friends/Caregivers
East - NB, QC, ON (FR)
7:00 pm ET / 8:00 pm AT
18 (DA)
Indigenous people with a serious illness
West - MB, SK, AB, BC, Territories (EN)
8:00 pm ET / 7:00 pm CT / 6:00 pm MT / 5:00 pm PT
Can I confirm your email address so that we can send you the link to the online discussion group?
We ask that you login a few minutes early to be sure you are able to connect and to test your sound (speaker and microphone). If you require glasses for reading, please make sure you have them handy as well.
As we are only inviting a small number of people, your participation is very important to us. If for some reason you are unable to attend, please call us so that we may get someone to replace you. You can reach us at [INSERT PHONE NUMBER] at our office. Please ask for [NAME]. Someone will call you in the days leading up to the discussion to remind you.
So that we can call you to remind you about the discussion group or contact you should there be any changes, can you please confirm your name and contact information for me?
First name
Last Name
email
Daytime phone number
Evening phone number
If the respondent refuses to give his/her first or last name, email or phone number please assure them that this information will be kept strictly confidential in accordance with the privacy law and that it is used strictly to contact them to confirm their attendance and to inform them of any changes to the discussion group. If they still refuse THANK & TERMINATE.
Appendix C - Recruitment screener - Those living with serious illness
Focus Group Summary
Recruit 8 participants per group
Groups are 90 minutes in length
All must have a serious illness
15 groups in total:
Three groups with members of the general public with a serious illness
Three groups with those with a serious illness and a physical disability
Three groups with Black and other people of colour with a serious illness
Three groups with Indigenous peoples with a serious illness
Three groups with family, friends or unpaid caregivers of someone with a serious illness or of someone who succumbed to a serious illness within the last year
Ensure good mix of other demos (province within regions, age, gender, income, education, household type, urban/suburban/rural etc.)
Group #
Audience
Region/Language
Time
Monday, November 7, 2022
1 (SC)
General population with a serious illness
East - NL, PEI, NS, NB, QC, ON (EN)
4:00 pm ET / 5:00 pm AT / 5:30 pm NT
2 (SC)
Health/Social care providers
East - NL, PEI, NS, NB, QC, ON (EN)
6:00 pm ET / 7:00 pm AT / 7:30 pm NT
3 (DA)
Those with a serious illness and a physical disability
East - NL, PEI, NS, NB, QC, ON (EN)
6:00 pm ET / 7:00 pm AT / 7:30 pm NT
4 (SC)
Health/Social care providers
West - MB, SK, AB, BC, Territories (EN)
8:00 pm ET / 7:00 pm CT / 6:00 pm MT / 5:00 pm PT
5 (DA)
General population with a serious illness
West - MB, SK, AB, BC, Territories (EN)
8:00 pm ET / 7:00 pm CT / 6:00 pm MT / 5:00 pm PT
Tuesday, November 8, 2022
6 (SC)
Those with a serious illness and a physical disability
Interviewer:
Date:
Validated:
Quality Central:
On list:
On quotas:
Hello/Bonjour, this is [...] calling on behalf of Earnscliffe, a national public opinion research firm. We are organizing a series of discussion groups on issues of importance on behalf of the Government of Canada, specifically Health Canada. The Government of Canada would like to understand people in Canada's views to help inform the development of a future advertising campaign. We are looking for people who would be willing to participate in a 90-minute online discussion group. Up to 8 participants will be taking part and for their time, participants will receive an honorarium. May I continue?
Yes CONTINUE
No THANK AND TERMINATE
Participation is voluntary. We are interested in hearing your opinions; no attempt will be made to sell you anything or change your point of view. The format is a 'round table' discussion led by a research professional. All opinions expressed will remain anonymous and views will be grouped together to ensure no particular individual can be identified. I would like to ask you a few questions to see if you or someone in your household qualify to participate. This will take about three minutes. May I continue?
Yes CONTINUE
No THANK AND TERMINATE
Monitoring text:
READ TO ALL: "This call may be monitored or audio taped for quality control and evaluation purposes.
ADDITIONAL CLARIFICATION IF NEEDED:
To ensure that I (the interviewer) am reading the questions correctly and collecting your answers accurately;
To assess my (the interviewer) work for performance evaluation;
To ensure that the questionnaire is accurate/correct (i.e. evaluation of CATI programming and methodology - we're asking the right questions to meet our clients' research requirements - kind of like pre-testing)
If the call is audio taped, it is only for the purposes of playback to the interviewer for a performance evaluation immediately after the interview is conducted or it can be used by the Project Manager/client to evaluate the questionnaire if they are unavailable at the time of the interview - all audio tapes are destroyed after the evaluation.
Do you or does anyone in your immediate family or household work in any of the following areas?
Yes
No
A marketing research firm
A magazine or newspaper, online or print
A radio or television station
A public relations company
An advertising agency or graphic design firm
An online media company or as a blog writer
In health care
The government, whether federal, provincial or municipal
IF "YES" TO ANY OF THE ABOVE, THANK AND TERMINATE
In which province or territory do you live?
Newfoundland and Labrador
Nova Scotia
New Brunswick
Prince Edward Island
Quebec
Ontario
Manitoba
Saskatchewan
Alberta
British Columbia
Nunavut
Northwest Territories
Yukon
EAST (EN): 2 FROM ATLANTIC CANADA, 2 FROM QUEBEC, 4 FROM ONTARIO EAST (FR): 2 FROM ATLANTIC CANADA, 4 FROM QUEBEC, 2 FROM ONTARIO WEST (EN): 1 FROM MANITOBA, 1 SASKATCHEWAN, 2 FROM ALBERTA, 3 FROM BRITISH COLUMBIA, 1 FROM TERRITORIES
Do you have a life-impacting health condition or illness? What is it? [DO NOT READ ANSWER CATEGORIES, USE PRE-CODED LIST]
ALS ("Lou Gehrig's Disease")
Alzheimer and other dementias (e.g., Lewy Body dementia, vascular dementia, Creutzfeldt-Jakob disease, etc.)
Inflammatory central nervous system disease (e.g., chronic meningitis, central nervous system vasculitis, neurosarcoidosis, etc.)
Leukemia
Liver disease (e.g., liver cirrhosis, Hepatitis A, B, and C, Wilson disease, etc.)
Malignant neoplasm
Malnutrition
Multiple sclerosis
Musculoskeletal disorder
Non-ischemic heart disease
Neurological disease (e.g., Alexander disease, Ataxia, Multiple system atrophy (MSA), Muscular dystrophy, etc.)
Neuropathy
Parkinson's disease
Progressive supranuclear palsy
Tuberculosis
None of the above [GO TO Q4]
Don't know/Prefer not to answer [GO TO Q4]
IF HAS A LIFE-IMPACTING HEALTH CONDITION OR ILLNESS, SKIP TO Q7
Do you provide currently or have you provided within the past year unpaid care and/or assistance to a person living with a life-impacting health condition or illness?
Yes [CONTINUE]
No [THANK AND TERMINATE]
Don't know/Prefer not to answer [THANK AND TERMINATE]
What life-impacting health condition or illness does the person you provide/provided care and/or assistance to live with? [DO NOT READ ANSWER CATEGORIES, USE PRE-CODED LIST]
ALS ("Lou Gehrig's Disease")
Alzheimer and other dementias (e.g., Lewy Body dementia, vascular dementia, Creutzfeldt-Jakob disease, etc.)
Inflammatory central nervous system disease (e.g., chronic meningitis, central nervous system vasculitis, neurosarcoidosis, etc.)
Leukemia
Liver disease (e.g., liver cirrhosis, Hepatitis A, B, and C, Wilson disease, etc.)
Malignant neoplasm
Malnutrition
Multiple sclerosis
Musculoskeletal disorder
Non-ischemic heart disease
Neurological disease (e.g., Alexander disease, Ataxia, Multiple system atrophy (MSA), Muscular dystrophy, etc.)
Neuropathy
Parkinson's disease
Progressive supranuclear palsy
Tuberculosis
NONE OF THE ABOVE [THANK AND TERMINATE]
Don't know/Prefer not to answer [THANK AND TERMINATE]
IF PROVIDES/PROVIDED CARE AND/OR ASSISTANCE TO A PERSON LIVING WITH A LIFE-IMPACTING ILLNESS (Q4) AND PERSON LIVING WITH A LIFE-IMPACTING ILLNESS QUALIFIES WITH ONE OF THE ILLNESSES IN Q5, QUALIFIES AS FAMILY, FRIEND OR CAREGIVER (GROUPS 12, 14, AND 17)
What is your relationship with that person? [ENSURE GOOD MIX]
Family member
Friend
Unpaid caregiver
Prefer not to answer [THANK AND TERMINATE]
Do you identify as a person with a physical disability?
Yes [RECRUIT FOR GROUPS (3, 6, AND 11)]
No
Prefer not to answer
What is your racial and/or ethnic background? [SELECT ALL THAT APPLY.]
Black (African, Afro-Caribbean, African-Canadian descent)
East Asian (Chinese, Korean, Japanese, Taiwanese descent)
Indigenous (First Nations, Inuit, Métis)
Latin American (Hispanic descent)
Middle Eastern (West Asian or North African descent, e.g. Afghan, Egyptian, Iranian)
South Asian (Indian, Pakistani, Sri Lankan, Indo-Caribbean descent)
Southeast Asian (Filipino, Vietnamese, Cambodian, Thai descent)
White (European descent)
Prefer not to answer
IF Q8 = 1,2,4,5,6,7 RECRUIT FOR BLACK AND OTHER PEOPLE OF COLOUR GROUPS (GROUPS 8, 9, AND 10) IF Q8=3, RECRUIT FOR INDIGENOUS GROUPS (GROUPS 15, 16, AND 18) ALL ARE ELIGIBLE FOR ALL OTHER GROUPS
Which of the following age categories do you fall in to? Are you…? ENSURE GOOD MIX
Under 18 years [THANK AND TERMINATE]
18-24 years
25-29 years
30-34 years
35-44 years
45-54 years
55-65 years
66-74
75+
What gender do you identify with? [ENSURE GOOD MIX]
Male
Female
Non-binary person
Two-spirit
Another gender identify
Prefer not to answer
What is your current employment status? ENSURE GOOD MIX
Working full-time
Working part-time
Self-employed
Retired
Unemployed
Student
Other
Prefer not to answer [THANK AND TERMINATE]
Which of the following categories best describes your total household income; that is, the total income of all persons in your household combined, before taxes? [READ LIST] ENSURE GOOD MIX
Under $20,000
$20,000 to under $40,000
$40,000 to under $60,000
$60,000 to under $80,000
$80,000 to under $100,000
$100,000 to under $150,000
$150,000 or more
Prefer not to answer [THANK AND TERMINATE]
What is the last level of education that you have completed? ENSURE GOOD MIX
Some high school only
Completed high school
Some college/university
Completed college/university
Post-graduate studies
Prefer not to answer [THANK AND TERMINATE]
Would you describe the area in which you live as… ENSURE GOOD MIX
Urban
Suburban
Rural
Prefer not to answer
Have you participated in an in-depth interview or focus group before? A discussion group brings together a few people in order to know their opinion about a given subject.
Yes [MAX 4 PER AUDIENCE]
No [SKIP TO S18]
Don't know/Prefer not to answer [THANK AND TERMINATE]
When was the last time you attended a discussion or focus group?
If within the last 6 months [THANK AND TERMINATE]
If not within the last 6 months [CONTINUE]
Don't know/Prefer not to answer [THANK AND TERMINATE]
How many of these sessions have you attended in the last five years?
If 4 or less [CONTINUE]
If 5 or more [THANK AND TERMINATE]
Don't know/Prefer not to answer [THANK AND TERMINATE]
INVITATION
Participants in in-depth interviews are asked to voice their opinions and thoughts. How comfortable are you in voicing your opinions in front of others? Are you…? (READ LIST)
Very comfortable [MINIMUM 4 per group]
Fairly comfortable [CONTINUE]
Comfortable [CONTINUE]
Not very comfortable [THANK AND TERMINATE]
Not at all comfortable [THANK AND TERMINATE]
Don't know/Prefer not to answer [THANK AND TERMINATE]
The discussion groups will be about palliative care and grief/bereavement. Are you comfortable speaking about this topic with a research professional?
Yes [CONTINUE]
No [THANK AND TERMINATE]
Would you prefer to participate in the discussion group alone or would you prefer to participate with the support of a family member or care partner?
Alone
With a care partner or family member
IF PREFERS TO PARTICIPATE WITH A CARE PARTNER/FAMILY MEMBER, SPECIFY: Your care partner or family member would be permitted to attend, at your request, to provide support during the discussion group. They would not be permitted to respond to any of the questions and would merely attend to listen and provide support. They will need to be available on the scheduled date/time and will not be incented/compensated for their attendance.
Do you have access to the technology necessary to participate in this interview by phone?
Yes
No
[IF NO] Is there anything we could do to ensure that you can participate? What specifically? INTERVIEWER TO NOTE INTERVIEWEE'S NEEDS AND CONSULT WITH EARNSCLIFFE ON APPROACH
Based on your responses, it looks like you have the profile we are looking for. I would like to invite you to participate in a small group discussion, called an online focus group, we are conducting at [TIME], on [DATE]
As you may know, focus groups are used to gather information on a particular subject matter. The discussion will consist of about 8 people and will be very informal.
It will last up to 90 minutes and you will receive [IF IN GROUP WITH PERSONS WITH DISABILITY] $150/ [ALL OTHER GROUPS] $125 as a thank you for your time. Would you be willing to attend?
Yes [RECRUIT]
No [THANK AND TERMINATE]
Don't know/Prefer not to answer [THANK AND TERMINATE]
PRIVACY QUESTIONS
Now I have a few questions that relate to privacy, your personal information and the research process. We will need your consent on a few issues that enable us to conduct our research. As I run through these questions, please feel free to ask me any questions you would like clarified.
P1) First, we will be providing a list of respondents' first names and profiles (screener responses) to the moderator so that they can sign you into the group. Do we have your permission to do this? I assure you it will be kept strictly confidential.
Yes [GO TO P2]
No [GO TO P1A]
We need to provide the first names and background of the people attending the focus group because only the individuals invited are allowed in the session and this information is necessary for verification purposes. Please be assured that this information will be kept strictly confidential. GO TO P1A
P1a) Now that I've explained this, do I have your permission to provide your first name and profile?
Yes [GO TO P2]
No [THANK & TERMINATE]
P2) A recording of the group session will be produced for research purposes. The recordings will be used by the research professional to assist in preparing a report on the research findings and may be used by the Government of Canada to inform their work in this subject area.
Do you agree to be recorded for research and reporting purposes only?
Yes [THANK & GO TO P3]
No [READ RESPONDENT INFO BELOW & GO TO P2A]
It is necessary for the research process for us to record the session as the researchers need this material to complete the report.
P2a) Now that I've explained this, do I have your permission for recording?
Yes [THANK & GO TO P3]
No [THANK & TERMINATE]
P3) Employees from the Government of Canada and the creative agency working with the Government of Canada to develop the advertising campaign may also be online to observe the groups.
Do you agree to be observed by Government of Canada employees and employees of the creative agency?
Yes [THANK & GO TO INVITATION]
No [GO TO P3A]
P3a) It is standard qualitative procedure to invite clients, in this case, Government of Canada employees, and employees of the creative agency hired to develop an advertising campaign by the Government of Canada, to observe the groups online. They will be there simply to hear your opinions firsthand although they may take their own notes and confer with the moderator on occasion to discuss whether there are any additional questions to ask the group.
Do you agree to be observed by Government of Canada employees and employees of the creative agency?
Yes [THANK & GO TO INVITATION]
No [THANK & TERMINATE]
INVITATION
Wonderful, you qualify to participate in one of our discussion sessions. As I mentioned earlier, the group discussion will take place on [DATE] at [TIME] for up to 90 minutes.
Group #
Audience
Region/Language
Time
Monday, November 7, 2022
1 (SC)
General population with a serious illness
East - NL, PEI, NS, NB, QC, ON (EN)
4:00 pm ET / 5:00 pm AT / 5:30 pm NT
2 (SC)
Health/Social care providers
East - NL, PEI, NS, NB, QC, ON (EN)
6:00 pm ET / 7:00 pm AT / 7:30 pm NT
3 (DA)
Those with a serious illness and a physical disability
East - NL, PEI, NS, NB, QC, ON (EN)
6:00 pm ET / 7:00 pm AT / 7:30 pm NT
4 (SC)
Health/Social care providers
West - MB, SK, AB, BC, Territories (EN)
8:00 pm ET / 7:00 pm CT / 6:00 pm MT / 5:00 pm PT
5 (DA)
General population with a serious illness
West - MB, SK, AB, BC, Territories (EN)
8:00 pm ET / 7:00 pm CT / 6:00 pm MT / 5:00 pm PT
Tuesday, November 8, 2022
6 (SC)
Those with a serious illness and a physical disability
Black and other people of colour with a serious illness
East - NL, PEI, NS, NB, QC, ON (EN)
6:00 pm ET / 7:00 pm AT / 7:30 pm NT
9 (SC)
Black and other people of colour with a serious illness
East - NB, QC, ON (FR)
7:00 pm ET / 8:00 pm AT
10 (DA)
Black and other people of colour with a serious illness
West - MB, SK, AB, BC, Territories (EN)
8:00 pm ET / 7:00 pm CT / 6:00 pm MT / 5:00 pm PT
Wednesday, November 9, 2022
11 (SC)
Those with a serious illness and a physical disability
East - NB, QC, ON (FR)
5:00 pm ET / 6:00 pm AT
12 (DA)
Family/Friends/Caregivers
East - NL, PEI, NS, NB, QC, ON (EN)
6:00 pm ET / 7:00 pm AT / 7:30 pm NT
13 (SC)
Health/Social care providers
East - NB, QC, ON (FR)
7:00 pm ET / 8:00 pm AT
14 (DA)
Family/Friends/Caregivers
West - MB, SK, AB, BC, Territories (EN)
8:00 pm ET / 7:00 pm CT / 6:00 pm MT / 5:00 pm PT
Thursday, November 10, 2022
15 (SC)
Indigenous people with a serious illness
East - NB, QC, ON (FR)
5:00 pm ET / 6:00 pm AT
16 (DA)
Indigenous people with a serious illness
East - NL, PEI, NS, NB, QC, ON (EN)
6:00 pm ET / 7:00 pm AT / 7:30 pm NT
17 (SC)
Family/Friends/Caregivers
East - NB, QC, ON (FR)
7:00 pm ET / 8:00 pm AT
18 (DA)
Indigenous people with a serious illness
West - MB, SK, AB, BC, Territories (EN)
8:00 pm ET / 7:00 pm CT / 6:00 pm MT / 5:00 pm PT
Can I confirm your email address so that we can send you the link to the online discussion group?
We ask that you login a few minutes early to be sure you are able to connect and to test your sound (speaker and microphone). If you require glasses for reading, please make sure you have them handy as well.
As we are only inviting a small number of people, your participation is very important to us. If for some reason you are unable to attend, please call us so that we may get someone to replace you. You can reach us at [INSERT PHONE NUMBER] at our office. Please ask for [NAME]. Someone will call you in the days leading up to the discussion to remind you.
So that we can call you to remind you about the discussion group or contact you should there be any changes, can you please confirm your name and contact information for me?
First name
Last Name
email
Daytime phone number
Evening phone number
If the respondent refuses to give his/her first or last name, email or phone number please assure them that this information will be kept strictly confidential in accordance with the privacy law and that it is used strictly to contact them to confirm their attendance and to inform them of any changes to the discussion group. If they still refuse THANK & TERMINATE.
Appendix D - Discussion guide - Health/Social care providers
Moderator introduces herself/himself and her/his role: role of moderator is to ask questions, make sure everyone has a chance to express themselves, keep track of the time, be objective/no special interest.
Good afternoon/Good evening and welcome everyone! My name is Stephanie/Doug and I use [she/he/they] pronouns. I will be leading our conversation today.
I would like to acknowledge that I am joining from the traditional, unceded territory of the Algonquin Anishinaabe nation. I recognize that we are all joining from different places and encourage you to share the Indigenous traditional territory you are joining from as part of your introduction later.
As mentioned, when we invited you to participate in this discussion group, we're conducting research on behalf of the Government of Canada and Health Canada, more specifically. The main focus of our discussion is to better understand perspectives on the topic of palliative care and grief and to gather your reactions to a series of draft advertising concepts for an upcoming campaign.
It is important for you to know that I am not a subject matter expert and do not have lived experience of taking care of or been in palliative care, hospices, etc.
I am very appreciative of the opportunity to better understand your thoughts/views through your lived experiences.
I also want to acknowledge the diversity of experiences for participants, and that we value these differences and welcome insight from people of all racial and/or ethnic backgrounds, genders, sexual orientations, abilities, faiths, family structures, and cultural backgrounds.
Your perspectives are very important and will help Health Canada in their efforts to develop messaging, educational resources, promotional materials, and marketing tools to strengthen the understanding of how palliative care can improve quality of life until the end of life.
I also want to acknowledge the sensitive nature of our conversation today and to reassure you that you should feel completely at ease declining to answer any questions you prefer not to answer. What you share will be treated respectfully.
If our conversation today causes you to feel distress, please feel free to take a moment for yourself, and re-join us if you are able to continue. You can also feel free to share your thoughts in the chat if you prefer.
Role of moderator: to ask questions, make sure everyone has a chance to express themselves, keep track of the time, assures participants that moderator has no special interest in, or knowledge of, the issues discussed.
Role of participants: speak openly and frankly about opinions, remember that there are no right or wrong answers and no need to agree with each other. [Emphasize that this is a safe space.]
Results are confidential and reported all together/individuals are not identified/participation is voluntary. No personal identifiers will be reported to Health Canada.
The length of the session (1.5 hours).
The presence of any observers, their role and purpose, and the means of observation (observers viewing and listening in remotely).
Confirm participants are comfortable with the platform and some of the specific settings such as: how to mute and unmute themselves; where the hand raise button is; and the chat box. Don't be afraid to use the chat box if you have something to contribute but are having trouble jumping in verbally.
Are there any questions about what I have just explained? Are you comfortable with all of this?
Moderator will go around the table and ask participants to introduce themselves.
Introduction of participants: To get started, let us introduce ourselves.
As you know, my name is Stephanie. I am 50 years old and have been happily married for 25 years. I have two grown children and a sweet old chocolate lab named Beau. I have been in public opinion research for 25 years and have a passion for qualitative research and getting to meet and speak with interesting people like yourselves. My hobbies include running, hiking and paddleboarding.
As you know, my name is Doug. I am 54 years old and the proud father of two adult sons. I got into public opinion research by accident 30 years ago and I have come to truly love finding out what people think about all kind of different topics and issues. One of my favourite hobbies is newly found. It's called padel. If you haven't played before, it's sort of a cross between tennis and racquetball.
Now let us go around the virtual room. Please tell us your first name, your line of work or profession, on which traditional territory you reside (if comfortable sharing) and one of your favourite interests or hobbies. Please feel free to introduce yourselves in the chat as well if you're more comfortable.
Context and understanding
To begin, I would like to read to you a couple of definitions in order to set the context for our discussions today:
Palliative care can be offered at any point during a serious illness and includes grief support for all those affected, including family, friends, and caregivers, and bereavement after a loved one passes. It includes services such as pain and symptom management, addresses psychological and spiritual concerns, informational needs, supports family and caregivers, and enhances quality of life. It can be given alongside curative treatments.
Palliative care addresses the physical, psychosocial, cultural, and spiritual needs of individuals of all ages. It may be delivered by a wide variety of care providers, including primary health care providers, disease specialists, and palliative care specialists.
A palliative approach to care integrates the core elements of palliative care into the care provided by non-specialists in primary care, long-term care, home and community care, and other health settings (for example, family physicians, nurse practitioners, physiotherapists, social workers, spiritual leaders, etc.). This approach builds capacity for generalist palliative care in a broader base of health care providers with the skills, knowledge and attitudes required to provide people and their families with palliative care whenever and wherever they need it.
In the coming months, the Government of Canada is launching a campaign aimed at raising awareness of palliative care and grief.
The purpose of our discussion today/tonight is to show you a series of draft creative concepts, which refers to visuals and wording messages, to gauge your reactions. We've got two concepts to show you. For each concept, there are a variety of examples of how that concept would be applied (i.e., social media posts, posters and a fact sheet). We will go through each concept one at a time and I will ask you to review them in silence and then we will discuss reactions as a group.
Before we begin, it is important to note that as these are still in the draft stage. I want you to use your imagination to consider them as final products.
[MODERATOR TO DISPLAY EACH CONCEPT IN ROTATED ORDER ONE AT A TIME ON SCREEN. MODERATOR TO LEAD A DISCUSSION TO UNDERSTAND REACTIONS TO EACH CONCEPT. MODERATOR TO PROBE FOR EACH]
Overall, what is your impression of this concept?
What, if anything, do you like? What, if anything, do you dislike? Why?
How does it make you feel, especially about palliative care and/or grief? Why?
What do you think of the design? Imagery? Graphic elements? Why?
What tone did it convey? Did you like it? Why or why not?
What did you interpret from the icons/symbols? Why?
What did you think of the photos? Why?
Would you notice it/Would it capture your attention? Is it memorable? Why or why not?
If you saw one of these products, would you be motivated to do anything? Why or why not?
If yes, what would you be motivated to do?
If you saw it on social media, would you be likely to like it or share it? Why or why not?
As far as you're concerned, is it appropriate to communicate about palliative care and/or grief in this way? Why or why not?
Was it credible/believable? Why or why not?
Was anything confusing or unclear? How so?
Does the concept raise any concerns or questions for you?
How could it be improved? Is there anything missing that should be communicated through products like these?
CONCEPT WRAP-UP:
Now that we have reviewed each of the concepts, I'd like to understand your overall preferences.
[POLL] Overall, which concept did you prefer? Why?
Would either be unacceptable or inappropriate for the Government to use? Why?
Which would be most likely to motivate you to do something? Why?
Which, if any, makes you think differently (in a positive way) about palliative care and/or grief? Why?
In the social posts, some used a headline, while one did not. Do you have a preference? Is one more attention-grabbing than another? Why?
What about the myth/fact approach of Concept A? Do you like that approach? Why or why not?
In one concept, they referred to "clients", while in the other, they referred to "patients". Which do you prefer? Why?
In one concept, the branding referred to the Government of Canada, while in the other it referred to Health Canada. Which do you prefer? Is one more credible than the other? Why?
Message testing
The messages conveyed in the two concepts were different.
[MODERATOR TO SHOW TWO VERSIONS OF COMPARABLE MEDIUMS ON SCREEN SIMULTANEOUSLY (I.E., BOTH POSTERS, BOTH FACT SHEETS, ETC.]
What do you think of this messaging?
What really stood out for you? Did any have a stronger impact than others?
Which specific words or phrases (if any) were particularly compelling? Why?
Were there any that were not all that compelling or problematic in some way? Which ones? Why?
Specific words/phrases:
Sometimes people use different words to describe the kind of care we are talking about today.
Are there other terms that you use with your patients/clients and/or find more relatable?
How about the term, "comfort care"? What does that term mean to you?
Do you feel it means something different or would it refer to the same type of care?
What about the term, "compassionate care"? What does that term mean to you?
What does the phrase, "palliative care gives your clients agency", mean?
What do you think of the grief-related language? Would 'move through or work through grief' or 'understand your grief' be preferred over 'cope with grief'?
What about the reference to 'strength' or 'power' - would there be other terms you would prefer?
What about the term "journey" or "experience" instead when we describe living with a serious illness all the way from the beginning (diagnosis) to end of life (death) or transition into the spirit world (depending on your beliefs)?
What do you think about the tone of the messages?
Was anything confusing or unclear?
Before today, had you heard this information? What information is new?
Is it credible? Believable? Why or why not?
Health Canada is also considering language for the website:
Talking to your clients/patients about their serious illness is not easy. We can help.
You might already by providing a palliative approach to care for your clients/patients with serious illness. Learn more about how you can best support your clients/patients.
You provide compassionate care for your clients/patient….and its important to acknowledge your own mental health.
What do you think about these messages?
Was anything confusing or unclear?
Reactions to the concept headlines/taglines (10-minute section / 50 minutes total)
Now let's focus on the headlines/taglines. There were different headlines/taglines used throughout the concepts:
Giving the power back to your clients/patients
Palliative care puts clients/patients and families first
Helping clients/patients find their strength
Starting care early puts clients/patients in control
Strength and support, starting at diagnosis
Help your clients/patients take control of their serious illness
Offer the strength to cope with grief
Palliative care puts life first
Get the facts about what palliative care means for your clients/patients
Palliative care gives your clients/patients agency
Palliative care supports clients/patients and their communities
Palliative care helps clients/patients grieve
Overall, what did you think of this headline/tagline? Why?
What thoughts/feelings did it evoke for you?
Does it fit with the concepts? Does it fit with some better than others? Why?
Is it memorable? Why or why not?
What did this headline/tagline mean or suggest to you, particularly about palliative care and/or grief? Why?
Is it appropriate to communicate about palliative care and/or grief in this way? Why or why not?
How, if at all, could it be improved? Why?
Additional prompts [IF TIME PERMITS]
Health Canada is also interested in understanding views related to the use of QR codes for communications purposes.
Would anyone like to share their experiences using QR codes? Why?
Would it be helpful if some of the products (i.e., posters, brochures, fact sheets) include a QR code to help you find more information? Why or why not?
What information would you like to know about palliative care, the palliative approach to care and/or grief?
Have any of you ever looked for information about palliative care, the palliative approach to care and/or grief?
Were you able to find what you were looking for? Why or why not?
Where would you like to receive information about palliative care to make products more applicable? Probe for more than a Google search, more specific sources.
Probe: TV ads; Internet ads; YouTube videos; social media platforms; information on a website; posters/brochures/pamphlets in hospitals, doctor's offices, pharmacies, etc.; other
Conclusion (5-minute section / 90 minutes total)
[MODERATOR TO REQUEST ADDITIONAL QUESTIONS ARE SENT VIA THE CHAT BOX DIRECTLY TO THE MODERATOR AND PROBE ON ANY ADDITIONAL AREAS OF INTEREST]
This concludes what we needed to cover tonight.
Do you have any final thoughts or any advice for Health Canada and/or their creative agency as they move to the production stage?
Moderator introduces herself/himself and her/his role: role of moderator is to ask questions, make sure everyone has a chance to express themselves, keep track of the time, be objective/no special interest.
Good afternoon/Good evening and welcome everyone! My name is Stephanie/Doug and I use [she/he/they] pronouns. I will be leading our conversation today.
I would like to acknowledge that I am joining from the traditional, unceded territory of the Algonquin Anishinaabe nation. I recognize that we are all joining from different places and encourage you to share the Indigenous traditional territory you are joining from as part of your introduction later.
As mentioned, when we invited you to participate in this discussion group, we're conducting research on behalf of the Government of Canada and Health Canada, more specifically. The main focus of our discussion is to better understand perspectives on the topic of palliative care and grief and to gather your reactions to a series of draft advertising concepts for an upcoming campaign.
It is important for you to know that I am not a subject matter expert and do not have lived experience of taking care of or been in palliative care, hospices, etc.
I am very appreciative of the opportunity to better understand your thoughts/views through your lived experiences.
I also want to acknowledge the diversity of experiences for participants, and that we value these differences and welcome insight from people of all racial and/or ethnic backgrounds, genders, sexual orientations, abilities, faiths, family structures, and cultural backgrounds.
Your perspectives are very important and will help Health Canada in their efforts to develop messaging, educational resources, promotional materials, and marketing tools to strengthen the understanding of how palliative care can improve quality of life until the end of life.
I also want to acknowledge the sensitive nature of our conversation today and to reassure you that you should feel completely at ease declining to answer any questions you prefer not to answer. What you share will be treated respectfully.
If our conversation today causes you to feel distress, please feel free to take a moment for yourself, and re-join us if you are able to continue. You can also feel free to share your thoughts in the chat if you prefer.
Role of moderator: to ask questions, make sure everyone has a chance to express themselves, keep track of the time, assures participants that moderator has no special interest in, or knowledge of, the issues discussed.
Role of participants: speak openly and frankly about opinions, remember that there are no right or wrong answers and no need to agree with each other. [Emphasize that this is a safe space.]
Results are confidential and reported all together/individuals are not identified/participation is voluntary. No personal identifiers will be reported to Health Canada.
The length of the session (1.5 hours).
The presence of any observers, their role and purpose, and the means of observation (observers viewing and listening in remotely).
Confirm participants are comfortable with the platform and some of the specific settings such as: how to mute and unmute themselves; where the hand raise button is; and the chat box. Don't be afraid to use the chat box if you have something to contribute but are having trouble jumping in verbally.
Are there any questions about what I have just explained? Are you comfortable with all of this?
Moderator will go around the table and ask participants to introduce themselves.
Introduction of participants: To get started, let us introduce ourselves.
As you know, my name is Stephanie. I am 50 years old and have been happily married for 25 years. I have two grown children and a sweet old chocolate lab named Beau. I have been in public opinion research for 25 years and have a passion for qualitative research and getting to meet and speak with interesting people like yourselves. My hobbies include running, hiking and paddleboarding.
As you know, my name is Doug. I am 54 years old and the proud father of two adult sons. I got into public opinion research by accident 30 years ago and I have come to truly love finding out what people think about all kind of different topics and issues. One of my favourite hobbies is newly found. It's called padel. If you haven't played before, it's sort of a cross between tennis and racquetball.
Now let us go around the virtual room. Please tell us your first name, your line of work or profession, on which traditional territory you reside (if comfortable sharing) and one of your favourite interests or hobbies. Please feel free to introduce yourselves in the chat as well if you're more comfortable.
Context and understanding
To begin, I would like to read to you a couple of definitions in order to set the context for our discussions today:
Palliative care can be offered at any point during a serious illness and includes grief support for all those affected, including family, friends, and caregivers, and bereavement after a loved one passes. It includes services such as pain and symptom management, addresses psychological and spiritual concerns, informational needs, supports family and caregivers, and enhances quality of life. It can be given alongside curative treatments.
Palliative care addresses the physical, psychosocial, cultural, and spiritual needs of individuals of all ages. It may be delivered by a wide variety of care providers, including primary health care providers, disease specialists, and palliative care specialists.
A palliative approach to care integrates the core elements of palliative care into the care provided by non-specialists in primary care, long-term care, home and community care, and other health settings (for example, family physicians, nurse practitioners, physiotherapists, social workers, spiritual leaders, etc.). This approach builds capacity for generalist palliative care in a broader base of health care providers with the skills, knowledge and attitudes required to provide people and their families with palliative care whenever and wherever they need it.
In the coming months, the Government of Canada is launching a campaign aimed at raising awareness of palliative care and grief.
The purpose of our discussion today/tonight is to show you a series of draft creative concepts, which refers to visuals and wording messages, to gauge your reactions. We've got two concepts to show you. For each concept, there are a variety of examples of how that concept would be applied (i.e., social media posts, posters and a fact sheet). We will go through each concept one at a time and I will ask you to review them in silence and then we will discuss reactions as a group.
Before we begin, it is important to note that as these are still in the draft stage. I want you to use your imagination to consider them as final products.
[MODERATOR TO DISPLAY EACH CONCEPT IN ROTATED ORDER ONE AT A TIME ON SCREEN. MODERATOR TO LEAD A DISCUSSION TO UNDERSTAND REACTIONS TO EACH CONCEPT. MODERATOR TO PROBE FOR EACH]
Overall, what is your impression of this concept?
What, if anything, do you like? What, if anything, do you dislike? Why?
How does it make you feel, especially about palliative care and/or grief? Why?
What do you think of the design? Imagery? Graphic elements? Why?
What tone did it convey? Did you like it? Why or why not?
What did you interpret from the icons/symbols? Why?
What did you think of the photos? Why?
Would you notice it/Would it capture your attention? Is it memorable? Why or why not?
If you saw one of these products, would you be motivated to do anything? Why or why not?
If yes, what would you be motivated to do?
If you saw it on social media, would you be likely to like it or share it? Why or why not?
As far as you're concerned, is it appropriate to communicate about palliative care and/or grief in this way? Why or why not?
Was it credible/believable? Why or why not?
Was anything confusing or unclear? How so?
Does the concept raise any concerns or questions for you?
How could it be improved? Is there anything missing that should be communicated through products like these?
CONCEPT WRAP-UP:
Now that we have reviewed each of the concepts, I'd like to understand your overall preferences.
[POLL] Overall, which concept did you prefer? Why?
Would either be unacceptable or inappropriate for the Government to use? Why?
Which would be most likely to motivate you to do something? Why?
Which, if any, makes you think differently (in a positive way) about palliative care and/or grief? Why?
In the social posts, some used a headline, while one did not. Do you have a preference? Is one more attention-grabbing than another? Why?
What about the myth/fact approach of Concept A? Do you like that approach? Why or why not?
In one concept, they referred to "clients", while in the other, they referred to "patients". Which do you prefer? Why?
In one concept, the branding referred to the Government of Canada, while in the other it referred to Health Canada. Which do you prefer? Is one more credible than the other? Why?
Message testing
The messages conveyed in the two concepts were different.
[MODERATOR TO SHOW TWO VERSIONS OF COMPARABLE MEDIUMS ON SCREEN SIMULTANEOUSLY (I.E., BOTH POSTERS, BOTH FACT SHEETS, ETC.]
What do you think of this messaging?
What really stood out for you? Did any have a stronger impact than others?
Which specific words or phrases (if any) were particularly compelling? Why?
Were there any that were not all that compelling or problematic in some way? Which ones? Why?
Specific words/phrases:
Sometimes people use different words to describe the kind of care we are talking about today.
Are there other terms that you use with your patients/clients and/or find more relatable?
How about the term, "comfort care"? What does that term mean to you?
Do you feel it means something different or would it refer to the same type of care?
What about the term, "compassionate care"? What does that term mean to you?
What does the phrase, "palliative care gives your clients agency", mean?
What do you think of the grief-related language? Would 'move through or work through grief' or 'understand your grief' be preferred over 'cope with grief'?
What about the reference to 'strength' or 'power' – would there be other terms you would prefer?
What about the term "journey" or "experience" instead when we describe living with a serious illness all the way from the beginning (diagnosis) to end of life (death) or transition into the spirit world (depending on your beliefs)?
What do you think about the tone of the messages?
Was anything confusing or unclear?
Before today, had you heard this information? What information is new?
Is it credible? Believable? Why or why not?
Health Canada is also considering language for the website:
Talking to your clients/patients about their serious illness is not easy. We can help.
You might already by providing a palliative approach to care for your clients/patients with serious illness. Learn more about how you can best support your clients/patients.
You provide compassionate care for your clients/patient….and its important to acknowledge your own mental health.
What do you think about these messages?
Was anything confusing or unclear?
Reactions to the concept headlines/taglines (10-minute section / 50 minutes total)
Now let's focus on the headlines/taglines. There were different headlines/taglines used throughout the concepts:
Giving the power back to your clients/patients
Palliative care puts clients/patients and families first
Helping clients/patients find their strength
Starting care early puts clients/patients in control
Strength and support, starting at diagnosis
Help your clients/patients take control of their serious illness
Offer the strength to cope with grief
Palliative care puts life first
Get the facts about what palliative care means for your clients/patients
Palliative care gives your clients/patients agency
Palliative care supports clients/patients and their communities
Palliative care helps clients/patients grieve
Overall, what did you think of this headline/tagline? Why?
What thoughts/feelings did it evoke for you?
Does it fit with the concepts? Does it fit with some better than others? Why?
Is it memorable? Why or why not?
What did this headline/tagline mean or suggest to you, particularly about palliative care and/or grief? Why?
Is it appropriate to communicate about palliative care and/or grief in this way? Why or why not?
How, if at all, could it be improved? Why?
Additional prompts [IF TIME PERMITS]
Health Canada is also interested in understanding views related to the use of QR codes for communications purposes.
Would anyone like to share their experiences using QR codes? Why?
Would it be helpful if some of the products (i.e., posters, brochures, fact sheets) include a QR code to help you find more information? Why or why not?
What information would you like to know about palliative care, the palliative approach to care and/or grief?
Have any of you ever looked for information about palliative care, the palliative approach to care and/or grief?
Were you able to find what you were looking for? Why or why not?
Where would you like to receive information about palliative care to make products more applicable? Probe for more than a Google search, more specific sources.
Probe: TV ads; Internet ads; YouTube videos; social media platforms; information on a website; posters/brochures/pamphlets in hospitals, doctor's offices, pharmacies, etc.; other
Conclusion (5-minute section / 90 minutes total)
[MODERATOR TO REQUEST ADDITIONAL QUESTIONS ARE SENT VIA THE CHAT BOX DIRECTLY TO THE MODERATOR AND PROBE ON ANY ADDITIONAL AREAS OF INTEREST]
This concludes what we needed to cover tonight.
Do you have any final thoughts or any advice for Health Canada and/or their creative agency as they move to the production stage?
Thank you very much for your participation. We really appreciate you taking the time to share your views. Your input is very important.
Appendix F - Focus group testing materials
Creative concepts
For each creative concept, participants were initially shown a slide focused on the graphic elements of the approach and which contained the logo, theme colours, and fonts. Following this, participants were shown a poster; information sheet; three examples of social media posts, two of which contained slogans and one of which did not; a website banner; and another poster.
Concept A
This concept featured a graphic element that was a mint green circle with six rounded green bars of various lengths and sizes layered over top. There were seven colours featured including different shades of green, beige, and blue. The two proposed fonts were: Poppins and Georgia Italic. The concepts featured images of people interacting with health/social care providers, family, friends, or unpaid caregivers.
Exhibit 4. Concept A - Health/Social care providers
Description:
In the concept "The Power of Palliative Care", patients are shown receiving support from caregivers and healthcare professionals. The concept uses empowering language to position palliative care as a form of strength, and a graphic asset with variable line lengths is used to represent the spectrum of palliative care. These assets were targeted towards health and social care providers.
Exhibit 5. Concept A - Those living with serious illness
Description:
In the concept “The Power of Palliative Care”, patients are shown receiving support from loved ones, caregivers and healthcare professionals. The language used in is concept is empowering and uplifting, and graphic assets with variable line lengths are used to show the variety of palliative care options available. These assets were targeted towards those living with a serious illness.
Concept B
This concept featured a graphic element that was a square with three horizontal coloured and shaded with green on the bottom, blue in the middle and orange/yellow on the top. Superimposed over the coloured square was a white flower with petals that extended out from the centre. There were three colours featured including different green, blue and orange/yellow. The proposed font was: Aeonik. The concepts featured images of people interacting with health/social care providers, family, friends, or unpaid caregivers.
Exhibit 6. Concept B - Health/Social care providers
Description:
The concept "Demystifying Palliative Care" features language that gives direct, factual information about palliative care to improve Canadians' knowledge about the subject, with imagery showing patients receiving support from loved ones and healthcare professionals. A dandelion graphic is overlayed on all images to convey a sense of hope and healing. These assets were targeted towards health and social care providers.
Exhibit 7. Concept B - Those living with serious illness
Description:
In the concept "Demystifying Palliative Care", straightforward, factual language is used to immediately teach Canadians about palliative care. Imagery shows patients being supported by loved ones and healthcare professionals, and a dandelion graphic is overlayed on the images to represent hope, happiness and healing. These assets were targeted towards those living with a serious illness.