This public opinion research report presents the results of an online survey conducted by Ekos Research Associates Inc. on behalf of the Public Health Agency of Canada. The research study included a survey with 1,500 paid and unpaid care providers of people living with dementia, as well as 50 in-depth interviews conducted between February and March 2021 with those providing dementia care or support.
Cette publication est aussi disponible en français sous le titre Connaissances, perspectives et expériences de fournisseurs de soins dans le domaine de la démence au Canada.
This publication may be reproduced for non-commercial purposes only. Prior written permission must be obtained from Public Services and Procurement Canada. For more information on this report, please contact the Public Health Agency of Canada at hc.cpab.por-rop.dgcap.sc@canada.ca or at:
Communications Branch
Public Services and Procurement Canada
Portage III Tower A
16A1-11 Laurier Street
Gatineau QC K1A 0S5
Catalogue Number:
H14-380/2021E-PDF
International Standard Book Number (ISBN):
978-0-660-39997-3
Related publications (registration number: POR 074-20):
Table 2: Family and Friend Caregivers – Type of Care
Table 3: Comfort with Providing Care
Table 4: Perceptions of Abilities of People Living With Dementia
Table 5: Perceived Discomfort Among Care Providers
Table 6: Perceptions Related to Stigma
Table 7: Risk/Protective Factors
Table 8: Self-rated Knowledge
Table 9: Knowledge
Table 10: Need for Training (Paid care Providers)
Table 11: Areas for Further Training (Family and Friend Caregivers)
Table 12: Resources
Table 13: Paid Care Providers - Access to Necessary Tools
Table 14: Factors Affecting Care
Table 15: Impact of COVID
Table 16: Challenges During COVID
Table 17: Challenges for Family and Friend Caregivers During COVID
List of Charts
Chart 1: Intensity of Care
Chart 2: Involvement of Family/Friend Caregivers
Chart 3: Degree of Comfort
Chart 4: Comfort with Providing Care in Presence of Co-morbidities
Chart 5: Family and Friend Caregivers - Care for Higher Risk Populations
Chart 6: Family and Friend Caregivers – Use of Culturally Appropriate Resources
1. Executive Summary
A. Background and Objectives
Dementia is characterized by a decline in cognitive abilities, including memory; awareness of person, place and time; language; basic math skills; judgment; and planning. Dementia can also affect mood and behaviour. Prevention of dementia, eliminating stigma, and enabling dementia-inclusive communities are critical objectives. Growing evidence supports recent guidance that around 40% of worldwide dementia cases could be prevented by addressing 12 risk factors: lower levels of early life education; hypertension; obesity; hearing loss; smoking; depression; physical inactivity; diabetes; social isolation; excessive alcohol consumption; traumatic brain injury; and air pollution[1]. In addition, stigma and a lack of understanding about dementia have been identified as significant barriers to receiving early and timely diagnosis, quality care, and the ability to engage meaningfully in one's community. Given Canada's growing and aging population, the number of Canadians living with dementia is expected to increase in future decades[2]. Creating safe, supportive, and inclusive communities across Canada for people living with dementia and family and friend caregivers is essential to improving quality of life.
Care providers play an integral role in supporting people living with dementia. They require sufficient knowledge and skills to be well-equipped and contribute to an improved quality of life for people living with dementia and caregivers. Professional care providers working with people living with dementia include:
developmental service workers who support those with disabilities;
health care professionals (e.g., physicians, nurses, technicians, and social workers);
personal care workers;
first responders; and
family and friend caregivers who support those living with dementia, often in an unpaid role.
Canada's first national dementia strategy, A Dementia Strategy for Canada: Together We Aspire, released in June 2019, identifies three national objectives: prevent dementia; advance therapies and find a cure, and improve the quality of life of people living with dementia and caregivers. The strategy sets out a vision of a Canada in which all people living with dementia and caregivers are valued and supported, quality of life is optimized, and dementia is prevented, well understood, and effectively treated. The current research is intended to address "several areas of focus noted in the strategy including: (a) address the importance of access to quality care, from diagnosis through end of life; (b) build the capacity of care providers, including through improved access to and adoption of evidence-based and culturally appropriate guidelines for standards of care; and (c) improve support for family and friend caregivers, including through access to resources and supports".
The primary objective of the research is to understand the perspectives, experiences, and knowledge of care providers in Canada. Care providers are critical information sources regarding:
risk factors and prevention related to dementia, dementia diagnosis, screening, and perceptions including stigma;
treatment and advance care planning for people living with dementia, and in particular for specialized and higher risk populations, as well as those with co-morbidities;
available dementia supports, education and training;
the priorities and needs to improve the quality of life of those living with dementia; and,
the impact of greater systemic pressures, such as exerted during the COVID-19 pandemic, on ability to provide care to those living with dementia
The information will be used to inform dementia-related initiatives and support annual reporting to Parliament on Canada's dementia strategy and international reporting obligations related to the Global Dementia Observatory.
B. Methodology
The study included a national survey of 1,593 paid care providers and unpaid family and friend caregivers, largely collected online, but with some completed by telephone, complemented by a series of 51 in-depth interviews with those providing dementia care or support.
Survey
The study included a national survey of paid care providers and family and friend caregivers of people living with dementia. The survey sample was randomly selected from a probability-based panel. The Probit panel, which is assembled using a random digit dial (RDD) process for sampling from a blended land-line cell-phone frame, provides full coverage of Canadians with telephone access. The distribution of the panel is meant to mirror the actual population in Canada (as defined by Statistics Canada). As such, our more than 100,000 member panel can be considered representative of the general public in Canada (meaning that the incidence of a given target population within our panel very closely resembles the public at large) and margins of error can be applied. Twenty percent of surveys were collected by trained, bilingual interviewers, while the rest were collected through online survey self-administration.
The survey was conducted online and by telephone from February 27 to March 30, 2021, in both official languages. This followed testing to make sure public understanding was clear and consistent. The survey length averaged 17 minutes online and 28 minutes by telephone. The overall rate of participation was 25% (27% online and 15% by telephone). Details on the rate of participation can be found in Appendix A, and the full questionnaire is provided in Appendix B.
Interviews
Using the Probit panel to recruit paid care providers and family and friend caregivers, a total of 51 interviews were conducted[3], each lasting roughly 60 minutes. On average, 10 participants were interviewed in each paid care provider category (health care professionals, developmental service workers, personal care workers), as well as among unpaid family and friend caregivers. Interview participants were included from each provincial region of the country4.
Participants in the interviews were asked to describe their experiences with and the nature of support or care they provide to those living with dementia, factors affecting care as well as challenges and rewards, impact on care during COVID, their views on the ability of people living with dementia to live independently, stigma encountered in dementia care, culturally appropriate tools, and any training and dementia guidance they have received that has helped them to provide dementia care. Paid care providers were provided with an incentive for their time. The interview guide can be found in Appendix C.
C. Key Findings
Role of Care Providers
Frequency of Care
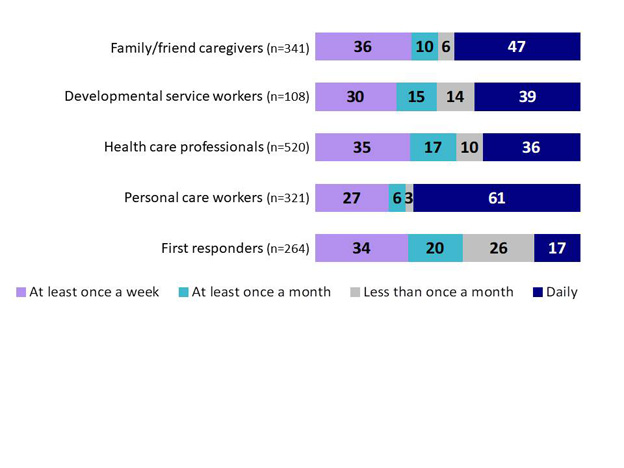
Among family and friend caregivers in the survey, nearly half (47%) provide daily care for someone living with dementia, and 36% do so at least once per week. For paid care providers, personal care workers provide care more regularly than developmental service workers or health care professionals; 61% provide support each day. Among health care professionals, 36% provide daily care, 35% at least once weekly. The pattern is similar among developmental service workers. First responders are less likely to provide support or care for people living with dementia on a regular basis, although nearly half (46%) provide care at least once a month (20%) or less often (26%).
Type of Care
Among health care professionals, many play multiple roles in the care of those living with dementia. Nearly half (49%) complete comprehensive history for those living with dementia, while 42% provide counselling or emotional support. One-third (33%) assist with daily living. Roughly, two in ten health care professionals administer medication (27%), provide non-pharmacological therapy (23%) or provide emergency treatment (20%).
Over half of developmental service workers provide counselling or emotional support (54%), and nearly half assist with daily living (46%). Nearly one-third of developmental support workers help complete comprehensive health history and assess patients (31%). One-quarter administer medication (25%) and slightly fewer provide first aid or emergency response (22%).
Most personal care workers (86%) assist with activities of daily living such as movement, bathing, dressing, meal preparation, and assistance with eating. Nonetheless, one-quarter said they administer medication (25%) or provide counselling and emotional support (25%).
Two in three first responders (67%) provide first aid to those living with dementia. Just less than half provide emergency treatment (47%) or rescue and locate missing persons (47%).
The role of family and friend caregivers is multipronged. About two in three family and friend caregivers currently or have in the past assisted with general health care and health monitoring such as overseeing medication usage, helping to administer medication or setting up appointments (68%) or assisting with financial affairs (66%). Over half assist with activities of daily living such as cooking, cleaning, bathing, or dressing (59%), or with transportation (56%). Over four in ten (43%) provide support with house maintenance or outdoor work. Fewer help with general social and mental health, social engagement, and outings (21%). In interviews, most family and friend caregivers said they provide care for a family member, most often a parent.
Comfort, Perceptions, Stigma
Comfort
Paid care providers who care for people living with dementia are much more likely than family and friend caregivers to say they are comfortable with their ability to provide quality care and support (i.e., indicating a 4 or 5 on a 5-point scale from uncomfortable to very comfortable). Personal care workers reported the highest level of comfort, with nine in ten (91%) indicating they are comfortable providing quality care or support to someone living with dementia. Two-thirds (64%) of family and friend caregivers reported being comfortable. Fewer first responders (58%) said they are comfortable in their ability to support care for someone living with dementia. In the presence of co-morbidities, health professionals reported the highest comfort (85%) of the four paid care provider groups in providing care for people living with dementia.
Perceptions
Survey respondents said they are relatively confident about the ongoing capabilities of people living with dementia in the years following diagnosis. Most health care professionals (81%) agree or strongly agree (4 or 5 on 5-point scale) that someone living with dementia can sometimes continue to live in their own homes for years following diagnosis; as do 75% of family and friend caregivers. About two-thirds of developmental service workers, personal care workers, or first responders agree.
Most also believe that people living with dementia can sometimes continue to be active in the community for years after the diagnosis, again with health care professionals most likely to agree (85%), followed by about three-quarters of developmental service workers, personal support workers and first responders, as well as family and friend caregivers saying the same.
Just over half of developmental service workers (57%), health care professionals (53%) and first responders (53%) agree that people living with dementia can sometimes continue to work for years following diagnosis. A lower proportion of personal care workers (41%) and family and friend caregivers (35%) agree.
Although few interview participants said they believe that dementia is a normal part of aging, many perceive that there are an increasing number of individuals living with dementia. These participants feel that increasing vascular issues and other illnesses such as diabetes are driving up the incidence of dementia. Some participants, however, feel that the increase in dementia can be attributed to both an increase in the diagnosis of dementia and greater life expectancy.
Interview participants perceive that people living with dementia can have a good quality of life; although, there were nuanced views of what contributes to quality of life. Many participants feel that contributors to quality of life can vary greatly depending on stages of dementia. For those who are in the early stages, for example, quality of life might come from a continued degree of activity and social connection. During later stages, most suggested that a higher quality of life might come from living among familiar surroundings and remaining in their home as long as possible.
Stigma
Over half of care providers agree or strongly agree that negative stereotypes about dementia are common within the health care system. This includes 53% of family and friend caregivers, and 56% to 57% of developmental service workers and health care professionals. Slightly fewer personal care workers (48%) and first responders (39%) agree. Notably, 65% of developmental service workers and 59% of health care professionals have witnessed a reduction in the quality of health care received by people living with dementia due to stigma.
Over half of health care professionals and developmental service workers (56%) feel they are knowledgeable about stigma related to dementia and how to reduce it. This is also the case among 47% of personal care workers. Among family and friend caregivers, 37% feel knowledgeable, although nearly as many (31%) said they feel less knowledgeable in this area. Only 28% of first responders rated themselves as knowledgeable in this area.
The majority of interview participants also identified stigma as a pervasive issue affecting the care received by people living with dementia. Stigma was often described in terms of misunderstanding or misjudging the abilities of people living with dementia. Interview participants feel that many paid care providers do not adequately understand how to assess the abilities of people living with dementia and are not adequately trained in how to communicate with people living with dementia.
Knowledge, Training and Resources
Knowledge of Risk and Protective Factors
Among the dementia prevention interventions presented in the survey, social Isolation is seen as the most important risk factor to be prioritized, according to family and friend caregivers (66%), personal care workers (60%), first responders (59%), health care professionals (55%), and developmental service workers (51%). Physical inactivity was noted by 51% of family and friend caregivers as an important risk factor that should be prioritized. Depression was noted as a priority by developmental service workers and personal care workers (41% each), but less so by health care professionals (28%). Higher levels of formal education were reported by about one-quarter of all care providers (22 to 27%) as an important risk or protective factor that should be prioritized in dementia prevention interventions.
Among interview participants, most believe social isolation is a key contributor to cognitive decline, and that continuing social connections, not living alone, and joining social groups could help delay the development of dementia symptoms. Many participants also said that keeping the mind active can help mitigate the onset or progression of dementia.
Overall, many interview participants pointed to a mixture of risks that can contribute to cognitive decline; most believing that there is not just one factor that determines the propensity to develop dementia. These participants identified a combination of genetics, lifestyle choices, social connection, and mental stimulation as contributors to the development of dementia.
Dementia Knowledge
Survey respondents rated their knowledge in a variety of areas related to dementia prevention, diagnosis, care, and treatment on a 5-point scale, from least knowledgeable to most knowledgeable. For reporting purposes, we refer to scores of 1 or 2 on the sale as less knowledgeable, a score of 3 as moderately knowledgeable and scores of 4 or 5 as more knowledgeable. Less than half of developmental services workers (43%), health care professionals (41%), and personal care workers (36%) said they feel more knowledgeable about dementia prevention and reducing risk. First responders and family and friend caregivers more often said they feel less knowledgeable in this area.
In terms of knowledge of screening for dementia or making a diagnosis, 41% of health care professionals, 32% of developmental service workers, and 31% of family and friend caregivers said they feel more knowledgeable; in each case a similar number of respondents rated themselves as less knowledgeable. Only 22% of personal care workers and 11% of first responders said they feel more knowledgeable in this area.
In terms of knowledge of treatments and care for those living with dementia, nearly three-quarters of personal care workers (72%) said they feel more knowledgeable. Health professionals (68%), developmental service workers (57%), and family and friend caregivers (46%) also rated themselves as more knowledgeable in this area. First responders more often said they are less knowledgeable in this area.
Regarding advance care planning and end-of-life care for those living with dementia, a higher proportion of health care professionals rated themselves as more knowledgeable (52%), compared with personal care workers (45%), developmental service workers (41%) and family and friend caregivers (39%). Among first responders, 63% said they feel less knowledgeable and only 15% said they are more knowledgeable in this area.
Training in Dementia Care
Survey respondents rated the extent to which they felt they could use more preparation/training in a variety of areas related to dementia prevention, diagnosis, care, and treatment on a 5-point scale, from 1 (needing the least additional preparation/training) to 5 (the most additional preparation/training). For reporting purposes, we refer to scores of 1 or 2 on the scale as needing minimal additional preparation/training, a score of 3 as needing a moderate amount of additional preparation/training and scores of 4 or 5 as needing much more preparation/training. The majority of developmental service workers (60%) and personal care workers (52%) feel they could use much more preparation or training in dementia prevention and reducing risk. Less than half of health care professionals (46%) and over one-third of first responders (38%) said they could use much more training in dementia prevention and reducing the risk.
Over half of developmental service workers (55%) reported that they could use much more preparation or training in screening for dementia or making a dementia diagnosis. Less than half of personal care workers (46%) and health care professionals (42%) said the same, as did more than one-third of first responders (35%).
Personal care workers (54%) are most likely to feel they could use much more training on the treatment and care of someone living with dementia. About four in ten developmental service workers (47%), first responders (41%), and health care professionals (40%) reported the same.
There is greater variation across care providers regarding their perceived need for much more training on advance care planning and end-of-life care for those living with dementia. This ranges from 56% among developmental service workers, and 52% among personal care workers, to 41% among health care professionals, and 31% among first responders.
Many developmental service workers (56%) feel they could use much more training on how to make interactions with care providers feel safer and more supportive. Just under half of personal care workers (49%), health care professionals (42%), and first responders (42%) also feel this is the case for them.
In interviews, few paid care providers reported receiving formal training on providing care for those living with dementia. Many shared that they have become capable of caring for those living with dementia as a result of on-the-job training. Among family and friend caregivers, many said they are not well trained to provide care for someone living with dementia. A few friends and family caregivers have asked for information during their doctor's appointments on how to care for the individual living with dementia, or consulted with other friends or acquaintances who are health care providers or who have experience caring for their own loved one living with dementia.
Dementia Guidance Resources
Two-thirds of health care professionals (68%) said they know where to find resources related to dementia prevention and reducing risk. About six in ten developmental service workers (60%) or personal care workers (59%) reported that they know where to find this information. A minority of friend and family caregivers (41%) and first responders (35%) said the same.
Nearly three-quarters of health care professionals (73%) know where to find information on dementia screening and diagnosis. Fewer developmental support workers (64%), family and friend caregivers (59%), and personal care workers (50%) said this, as did a minority of first responders (36%).
Most health care professionals (83%), personal care workers (79%), and developmental service workers (76%) know where to find resources on the treatment and care of someone living with dementia. Family and friend caregivers (65%) and first responders (53%) are least likely to have said this.
The majority of developmental service workers (58%) and health care professionals (55%) reported they would know where to find resources related to stigma reduction. Less than half of personal care workers (49%), family and friend caregivers (31%), and first responders (30%) said they would know where to find this information.
Health care professionals and developmental service workers (69% each) are more likely than other care providers to have said they know where to find information on advance care planning and end-of-life care. Nearly two-thirds of personal care workers (61%) also know where to find this information. Fewer family and friend caregivers (48%) and first responders (32%) said this.
In interviews, some participants said they try to stay current on the latest advice to provide care for people living with dementia. Aside from formal workshops and training, a few care providers identified resources from their employer or discussions with colleagues as ways to stay current. Some paid care providers pointed to non-profit organizations with a specific focus on dementia as a primary source of information.
Culturally Appropriate Care and Tools
Culturally appropriate care involves considering a patient's cultural background, personal experiences, and norms. Over half of developmental service workers (59%) and personal care workers (54%) said they would know where to find culturally appropriate tools. Nearly half of health care professionals (48%) and about one-quarter of first responders (26%) or family and friend caregivers (24%) said the same.
Culturally appropriate tools were reported to be available to provide care or support for specific segments of the population living with dementia, to varying degrees. These populations include:
People from ethnic and cultural minority communities - Less than 50% of paid care providers said that necessary tools are available to provide care for those living with dementia from ethnic and cultural minority communities.
People with intellectual/developmental disabilities – 69% of developmental service workers, 50% of personal care workers and health care professionals and 38% of first responders reported that tools are available;
Rural and remote communities - About 40% of personal care workers, health care professionals, and developmental service workers reported that tools are available, although fewer first responders said this;
Those living with young onset dementia - About 40% of personal care workers, health care professionals, and developmental service workers reported that tools are available, although fewer first responders said this is the case;
LGBTQ2+ community – Just over 33% of care providers reported that tools are available;
Indigenous People - Roughly 33% of care providers reported that tools are available; and,
Official language minority communities – About 33% of developmental service workers, personal care workers, and health care professionals reported that tools are available, although fewer first responders said the same.
Among the one-on-one interviews, a few participants said they are aware of culturally appropriate guidance, or have received culturally appropriate training, specifically designed for those living with dementia.
Factors Impacting Quality of Care and Challenges to Care
Quality of Care
Many challenges can affect the ability to provide quality dementia care or support. Mitigation strategies noted include better sharing of information across care providers or in care settings (57%) and more dementia care training (54%). Health care professionals reported the sharing of information as a key area for change (63%) that would improve quality of care.
Having more time to spend with those with dementia is another area where many care providers feel change is needed, particularly personal care workers (48%) and health care professionals (40%). Increased mental health supports is also considered a key area for positive change, particularly among family and friend caregivers (50%), but also among 39% of developmental service workers, 32% of first responders and 31% of health care professionals.
Having an advance care plan in place is also believed to have a positive impact on quality of care, particularly among family and friend caregivers (39%). Knowing the medical history of the individual is a key area for positive change, notably among personal care workers (33%) and first responders (32%). Better access to culturally appropriate information resources is also seen as having the potential to improve quality of care according to care providers (24%), particularly health care professionals (33%).
In interviews, family and friend caregivers said that improved access to programs that provide respite and information, such as day programs and support groups, would be valuable in providing care. Several said that they had to find dementia guidance on their own, and would welcome any communication of sources for dementia guidance. Improved access to paid care providers including doctors, psychologists, and home care (including consistency in home care staff) were noted by family and friend caregivers as necessary to support the overall care available for the person living with dementia.
According to interviews with personal care workers and health care professionals, adequate staffing and time to provide care, along with training specific to dementia care, are critical elements of providing quality care for persons living with dementia. Developmental service workers emphasized the need for training and dementia guidance to ensure well-informed and consistent approaches to care. Emergency responders noted fear and confusion experienced by those living with dementia in emergency situations and the difficulty of gaining compliance and gathering information on the scene.
Impact of COVID on Quality of Care
Care providers were asked about the impact of COVID-19 on ability to provide care. Results indicate that restrictions due to the COVID-19 pandemic negatively impacted communication methods and access to in-person care for those living with dementia. Among survey respondents, half of health care professionals and developmental service workers said they had to change how they communicate with patients when providing care, typically communicating through virtual methods. This was also noted by 30% of family and friend caregivers. Reducing in-person care because of concerns about transmission was similarly identified by higher proportions of health care providers (32%) and family and friend caregivers (30%) compared with other care providers. Health care professionals said they had less time to spend with people because of increased caseload and staffing issues (36%), also noted by 29% of developmental service workers. Not being able to provide in-person care because of visitation restrictions was reported by 33% of developmental service workers, 32% of family and friend caregivers, and 27% of health care professionals. Disruption of appointments was also noted by 30% of developmental service workers and 26% of family and friend caregivers.
Challenging Aspects of Providing Care
A systemic lack of resources was noted as a barrier to providing or receiving adequate care for those living with dementia. Both paid care providers and family and friend caregivers identified a lack of staff and adequate training to engage with and provide stimulation to people living with dementia as problematic. Access to specialists and physicians, and long wait times for some resources and programs were cited as barriers. Limited access to home care and other respite options for caregivers was also described as an area for improvement in supporting people living with dementia in the home. Finally, lack of coordination and sharing information were noted as other areas for improvement; with many highlighting interdisciplinary, holistic, approaches as the most desirable way to address the complex needs of people living with dementia, particularly those with co-morbidities.
D. Note to Readers
Detailed findings are presented in the sections that follow under the headings of Survey Findings and Interview Findings. Overall survey results are presented in the main portion of the narrative and are typically supported by graphic or tabular presentation of results. Bulleted text is used to point out any statistically significant and meaningful differences between sub-groups of respondents. If differences are not noted in the report, it can be assumed that they are either not statistically significant[4] in their variation from the overall result or that the difference was deemed to be too small to be noteworthy (e.g., less than 5% above or below the overall average).
Survey results for the proportion of respondents in the sample who either said "don't know" or did not provide a response may not be indicated in the graphic representation of the results in all cases, particularly where they are not sizable (e.g., 10% or less). These responses were, however, included in the calculations. Results may not total to 100% for this reason, and also due to rounding.
Overall themes are also described for interview responses, followed by anonymized, illustrative quotes. Quotes from participants are included first in the language of the speaker and then translated to the other language as needed. It should be noted that the results of the interviews are qualitative in nature. These results should not be used to estimate numeric proportion or number of individuals in the population who hold a particular opinion as they are not generalizable. That is, results should not be assumed to be representative of the experiences of the wider population of dementia care providers or family and friend caregivers in Canada. Responses from the interviews are meant to provide more detailed illustrations of experiences and perspectives. For this reason, terms such as "a few," "some" and "most" are used to broadly indicate views, rather than using specific percentages. To ensure a common understanding of the terms used in the analysis, the following guidelines were used in analysing and reporting on participant results:
"A few participants" = less than 25 per cent;
"Some participants" = 25 to 49 per cent;
"Many participants" = 50 to 75 per cent;
"Most participants" = over 75 per cent; and
"Almost all participants" = 95 per cent or more.
It should also be understood that the information provided by participants is subjective in nature, based on their own recollection, and perceptions and should not be interpreted as factual in nature.
E. Contract Value
The contract value for the POR project is $142,317.74 (including HST).
I hereby certify as Senior Officer of Ekos Research Associates Inc. that the deliverables fully comply with the Government of Canada political neutrality requirements outlined in the Communications Policy of the Government of Canada and Procedures for Planning and Contracting Public Opinion Research. Specifically, the deliverables do not include information on electoral voting intentions, political party preferences, standings with the electorate, or ratings of the performance of a political party or its leaders.
Signed by Susan Galley (Vice President)
2. Detailed Findings
A. Type of Care
Survey Findings
Role of Care Providers
Among paid care providers in the fields of health care or developmental services, most reported a role in nursing (23%), social work (18%), or occupational therapies (14%). One in ten said they work as a health technician or dietitian (11%), or as a physician (10%), and slightly fewer (7%) work as a pharmacist.
While there is a higher proportion of women among health care professionals and developmental service workers in the sample (78% and 75% respectively), the concentration of men is higher than the average among physicians in the sample (41%). The concentration of women is highest (92%) among health technicians.
Physicians and nurses are typically older, with 40% to 42% being 55 or older. The youngest are technicians, where 43% are under 35.
Among first responders, more than four in ten (43%) are in policing, one-quarter (26%) are paramedics, and 14% are fire fighters. Other roles reported to a lesser extent include security (8%), roles at dispatch (5%), and search and rescue (2%).
While 61% of first responders are men, the gender split is more even among paramedics where 51% are women.
The age distribution is younger among police officers where 49% are under 35.
Paramedics are less likely to have attained a university level of education (23%) compared with 40% to 42% among other first responders
Among family and friends caregivers, 61% said they do not reside with the person they are caring for while 18% live in the same residence. A similar number (15%) reported they no longer live with the person they care for, or do not currently provide care for someone living with dementia.
Intensity
Respondents were asked to identify how frequently they provide support or care to people living with dementia. Among family and friend caregivers, 47% provide daily care, and 36% do so at least once per week. Only 16% provide support once each month (10%) or, less than once per month (6%).
Personal care workers provide care more regularly than those in other health or developmental service roles; 61% provide support each day, 27% at least once a week, and only 9% provide care once per month or less often. Among health care professionals, 36% provide daily care, 35% at least once weekly, 17% at least once each month, and 10% less than once a month. The pattern is similar among developmental service workers, where 39% provide support daily, 30% weekly, 15% monthly, and 14% once per month or less often. First responders are less likely to provide support or care for people living with dementia on a regular basis. Nearly half (46%) provide care at least once a month (20%) or less than once per month (26%).
Chart 1: Intensity of Care
Chart 1: Intensity of Care - Text Version
This stacked chart shows the percentage of results for responses of five groups across four categories: at least once a week, at least once a month, less than once a month, and daily.
Respondents were asked: "How frequently do you interact with or provide care or support to people living with dementia in your work? / How frequently do you provide care or support to people living with dementia?"
Respondents selected:
Family/friend caregivers (n=341)
Category "at least once a week": 36%
Category "at least once a month": 10%
Category "less than once a month": 6%
Category "daily": 47%
Developmental service workers (n=108)
Category "at least once a week": 30%
Category "at least once a month": 15%
Category "less than once a month": 14%
Category "daily": 39%
Health care professionals (n=520)
Category "at least once a week": 35%
Category "at least once a month": 17%
Category "less than once a month": 10%
Category "daily": 36%
Personal care workers (n=321)
Category "at least once a week": 27%
Category "at least once a month": 6%
Category "less than once a month": 3%
Category "daily": 61%
First responders (n=264)
Category "at least once a week": 34%
Category "at least once a month": 20%
Category "less than once a month": 26%
Category "daily": 17%
Q2. How frequently do you interact with or provide care or support to people living with dementia in your work? / How frequently do you provide care or support to people living with dementia?
Base: n=1593
Among health care professionals and developmental service workers, physicians are more likely to provide care at least once a week (51%) compared with those in other fields, and least likely to give daily support (16%). Those working as health technicians (20%) or as psychologists (19%) are more apt to provide care less than once a month.
Paramedics report providing more frequent care than other first responders; 51% said they do so at least once each week. Police are more likely to provide support at least once a month (26%) while other first responders typically provide care less than once a month (44%).
Considering the high proportion of women represented among personal care workers and family and friend caregivers in the sample (81 and 77%, respectively), and propensity of these same groups to provide daily support or care (61 and 47%, respectively), it is not surprising that 45% of women report providing daily care to support someone living with dementia.
Those with a graduate level of education are more likely to see dementia patients infrequently; 16% at least once per month and 13% less than once monthly. Conversely, those with a college education are more likely to provide care daily (45%).
Type of Service
When asked about the type of care or support they provide to support someone living with dementia, over half of developmental service workers said they provide counselling or emotional support (54%), and nearly half assist with daily living (46%). Nearly one-third of developmental support workers help complete comprehensive health history and assess patients (31%). One-quarter administer medication (25%) and slightly fewer provide first aid or emergency response (22%).
Among health care professionals, 49% complete a comprehensive history for those living with dementia, while 42% provide counselling or emotional support. One-third (33%) assist with daily living. Roughly, one-quarter of health care professionals administer medication (27%) or provide non-pharmacological therapy (23%). Two in ten provide emergency treatment (20%).
Most personal care workers (86%) assist with activities of daily living such as movement, bathing, dressing, meal preparation, and assistance with eating. One-quarter said they administer medication (25%) or provide counselling and emotional support (25%).
Two in three first responders (67%) provide first aid to those living with dementia. Just less than half provide emergency treatment (47%) or rescue and locate missing persons (47%).
Table 1: Paid Care Providers - Type of Care
Col1
Developmental service workers
Health care professionals
Personal care workers
First responders
Q7. What kind of care or support do you provide for people living with dementia?
n=108
n=520
n=321
n=264
Completing a comprehensive health history and assessing patients
Assisting with activities of daily living (movement, bathing, dressing/ undressing, meal prep, assistance with eating)
46%
33%
86%
7%
Education of care providers
0%
1%
0%
0%
Medical care/acute care or support
3%
8%
1%
0%
Coordination/connection to services, adapting/assessing environment
5%
5%
1%
3%
General engagement/stimulation, transportation
6%
2%
5%
2%
Other (please specify)
5%
2%
3%
2%
Don't know / No response
2%
2%
1%
6%
Among health care professionals and developmental service workers, physicians are more likely to say they prescribe medication (70%), formulate and communicate a diagnosis (69%), complete a comprehensive health history and assess the patient (69%), or provide emergency treatment (44%). Nurses are more likely to report administering medication (53%) or assisting with daily living (46%). Therapists are more apt to say they provide non pharmacological therapy (75%) or assist with daily living (47%). Technicians are more apt to report providing medical care or acute care and support (36%). Those working in psychological or social service roles are more likely to say they provide counselling or emotional support (74%).
Among first responders, paramedics are more likely to say they provide first aid (87%) or emergency treatment (84%). Police are more apt to say they provide rescue and location of missing persons (71%).
Women are more likely to assist with activities of daily living (50%), along with counselling and emotional support (35%) and completing a comprehensive health history and assessing patients (32%). Men are more apt to say they provide emergency aid (38%), provide emergency treatment (27%), and rescue and locate missing persons (23%).
Regionally, those in Atlantic Canada (47%) and Ontario (40%) are more likely to report they provide counselling and emotional support. Those in Atlantic Canada (37%) are more likely to say they help administer medication. Those in Ontario (21%) are more likely to say they provide non-pharmacological therapy.
About two in three family and friend caregivers said they assist with general health care and health monitoring such as overseeing medication usage, helping to administer medication or setting up appointments (68%) or assisting with financial affairs (66%). Over half assist with activities of daily living such as cooking, cleaning, bathing, or dressing (59%), or with transportation (56%). Over four in ten (43%) provide support with house maintenance or outdoor work. One in five (21%) help with general social and mental health, social engagement, and outings.
Table 2: Family and Friend Caregivers – Type of Care
Q8. What kind of care or support [do/did] you provide for someone living with dementia?
n=341
General health care and health monitoring such as overseeing medication usage or help administering medication or setting up appointments
68%
Assisted with activities of daily living such as cooking, cleaning, bathing, or dressing
59%
House maintenance or outdoor work
43%
Transportation
56%
Assisted with financial affairs
66%
Social/mental health/engagement/outings
21%
Other (please specify)
5%
Don't know / No response
1%
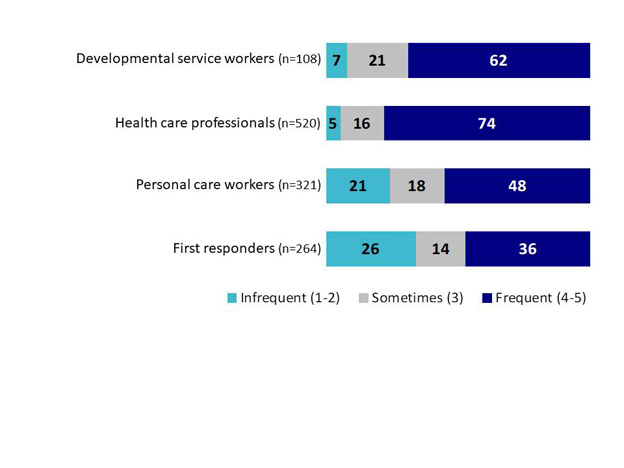
Nearly three in four health care professionals (74%) involve family and friend caregivers frequently (i.e., 4 or 5 on the scale) in the care planning of the person living with dementia. Over six in ten developmental service workers (62%) also said they frequently involve family and friend caregivers. This drops to half among personal care workers (48%) and just over one-third (36%) among first responders.
Chart 2: Involvement of Family/Friend Caregivers
Chart 2: Involvement of Family/Friend Caregivers - Text Version
This stacked chart shows the percentage of results for responses of four groups across three categories: infrequent, sometimes, and frequent. [1-Never to 5-Always]
Respondents were asked: "In your role, how frequently do you involve the family / friend caregivers of people living with dementia in care planning for the person living with dementia (i.e. contributing to decisions about care)?"
Respondents selected:
Developmental service workers (n=108)
Category "infrequent (1-2)": 7%
Category "sometimes (3)": 21%
Category "frequent (4-5)": 62%
Health care professionals (n=520)
Category "infrequent (1-2)": 5%
Category "sometimes (3)": 16%
Category "frequent (4-5)": 74%
Personal care workers (n=321)
Category "infrequent (1-2)": 21%
Category "sometimes (3)": 18%
Category "frequent (4-5)": 48%
First responders (n=264)
Category "infrequent (1-2)": 26%
Category "sometimes (3)": 14%
Category "frequent (4-5)": 36%
Q11. In your role, how frequently do you involve the family / friend caregivers of people living with dementia in care planning for the person living with dementia (i.e. contributing to decisions about care)? (1-Never to 5-Always)
Base: n=1252
Among first responders, paramedics are more likely to report involving family and friend caregivers frequently (63%).
Women (61%) are more likely than men (48%) to say they involve family and friend caregivers frequently in the care plan.
Regionally, care providers in Atlantic Canada (77%) are most likely to say they involve family and friend caregivers frequently, while those in Quebec (45%) are least likely to do so.
Care providers with graduate degrees or higher (71%) are more likely to say they involve family and friend caregivers frequently in care planning.
Interview Findings (Role of Care Providers)
Interview participants were also asked to describe their experiences providing care or support to people living with dementia. While they varied greatly, some common themes emerged among those in similar roles.
Family and Friend Caregivers
Among family and friend caregivers, for example, almost all said they provide care for a family member, most commonly a parent. Some did not specify how long they have provided care, but among those who did, the time period of care was between three and ten years. In most cases, the participant described themselves as the primary caregiver, though some noted they have secondary support from other family members, a licensed practical nurse or a personal care worker. Some share the overall responsibility of care more evenly with their partner or siblings. The location of care varies, with some saying they already shared a residence with the person living with dementia and no move was required, some who reported the person living with dementia moving into their residence or vice versa, and some who do drop-in visits to the residence of the person living with dementia.
Most family and friend caregivers described providing full-time care, or more specifically daily care including household chores, cooking, errands, and to a lesser extent dressing and hygiene. Some also mentioned assistance with physical and mental stimulation, emotional support, finances, and activity planning. Many described previous experience with dementia, either through prior work in personal care, a retirement facility, or from previously caring for someone else living with dementia.
Health Care Professionals
Among health care professionals who specified how long they have worked in their fields, experience ranged from 10 to 40 years. Most commonly, this experience was found in a hospital setting, though some mentioned work in the community, family or clinical practices, and a few said they are employed in long-term or home care. When describing what area of care they work in, many said they are involved in dementia patient care or long term care, others said they work in geriatrics or with seniors, and a few work in acute care. A couple of participants mentioned other areas; surgery and psychiatry. Nearly half of respondents had previously encountered dementia in their personal lives, either with family members or friends. A few mentioned their involvement in training or education, primarily of new nurses and other professionals, but in one case, also training family and friend caregivers on how to work with people living with dementia.
Personal Care Workers
Among personal care workers who specified how long they have worked in their field, experience ranged from 5 to 30 years. Most commonly this took place in a long-term care, or group home facility, though some mentioned involvement in private or one-on-one home care. A couple of participants noted work in community assisted living or with housing projects for seniors, the homeless, and the marginalized in which they would encounter people living with dementia. Not many participants described the details of the support they provide to people living with dementia, but most often references were made to the provision of daily assistance including moving patients, helping with eating , and monitoring. One participant said they primarily provide respite for other caregivers. A couple of participants noted previous experience with dementia among their family members, and a few had prior relevant work experience including in nursing, social work, and palliative care.
Developmental Service Workers
Although some of the developmental service workers interviewed did not specify how many years they have worked in their fields, those who provided this information had between 10 and 30 years of experience. Most described work in a long-term care facility, though several also worked in a hospital setting. A couple of respondents described roles in program or service coordination specifically. One participant noted employment in a community assisted living facility and another described one-on-one home care.
With such varied roles as social workers, program coordinators, and physiotherapists, the type of support provided to those living with dementia varied greatly. Those working in long-term care for example, described care, and activities planning/coordination, acute care, and development of mobility and daily living skills as among their duties. Those in hospitals described physical rehabilitation (including mobility and daily living skills development), transition planning for patients entering long-term care, acute care, and other assessment or investigative functions such as conducting incapability assessments or responding to concerns under the ‘BC Adult Guardianship Act'. Those working in community living or home care noted helping with daily tasks, accessing community resources like adult day programs, providing respite to caregivers, and providing stimulation such as physical exercise, socializing, and entertainment for people living with dementia. No developmental service workers mentioned prior experience with someone living with dementia in their personal lives.
First Responders
Most first responders did not specify how long they have worked in their given field, but among those who did, the range was between 20 and 30 years of experience. Among those who specified how often they are providing care to those living with dementia, paramedics reported the most contact, with some saying they provide care daily or multiple times per week. Conversely, one respondent in policing/search and rescue said contact could be as infrequent as a couple of times per year.
The type of care provided varied depending on the respondent's role. Paramedics for example, most often reported being called to long-term care facilities or private homes to address medical issues from cuts and injuries to lift assists or fall prevention and assessment, to more serious medical emergencies such as a heart attack or stroke. Many also described transporting patients to the hospital for medical assistance. Among police/search and rescue, the most common interaction described was finding patients who have walked away from their homes. One paramedic noted less common interactions such as providing home assessments and dealing with caregiver breakdowns. One first responder described their involvement in an ‘extended care' program which involves responding to calls in long-term care, providing health assessments, and working with on-site physicians to develop ongoing care planning. This program allows health care professionals and first responders to collaborate on care on-site as opposed to transporting people living with dementia to the hospital which can be confusing or agitating.
Involvement of Family in Care Plan
Many paid care providers[5] who were interviewed said they involve family in the health care planning process or decision-making of a person living with dementia. These interview participants explained that involving family can be beneficial in understanding the health history of the individual and in creating a care plan that corresponds to their needs appropriately. The health care plan can ensure that everyone involved in the care of the individual is aligned on the care goals. The plan is subsequently adjusted as changes arise in the individual's health status. The health care plan can help serve as a shared reference to decision-making, according to a few participants. As one participant explained, "if the family buys into the care plan, there is more support".
"It is very important to inform the family during the planning stage of the care plan, especially in psychiatry. They organize a meeting, ask questions to better understand the health problems of the patient, inform the family of the plan. After that initial stage, the nursing team decides on a daily basis without informing the family unless they are present." (Nurse)
"Yes, we involve family. [We] try to get them on the same page in terms of consistent care and engagement. We get information from family about patient history and background that helps us." (Physician)
"Yes, they work in long-term care facility in an interdisciplinary team to decide on care plan, and this includes a family member on the team. With COVID, these are now online meetings but they still occur." (Personal care worker)
"Yes, when developing treatment plan and decisions, there is a multi-disciplinary team and family are involved." (Occupational therapist/Physiotherapist)
"Unless I have a specific and compelling reason to not involve family, such as concerns about abuse or neglect, I do. Because they know their family member best and have been helping to manage the illness, sometimes for years." (Medical social worker)
Some paid care providers said they engage with families to more fully understand the person living with dementia and their history. This includes information or stories from their past that may help in providing comfort to the person living with dementia. For example, information from family about previous occupations, favourite pastimes or names of family members can assist care providers in interacting with the individual living with dementia and calming them in periods of distress.
"You need historical information about that individual from families. Trying to pull these things out can be so impactful if someone is distressed." (Nurse)
"It's important to recognize the value of family in care. I may have expertise that can help that individual, but the family really knows the individual." (Nurse)
"[Families] contribute a great deal. Background about other names of family members, things the client likes to do." (Personal care worker)
A few paid care providers said that involving family in the care plan can help the family understand the abilities of their loved one living with dementia and can help provide support and training to families to interact with their family member.
"Case managers would sit down with the families and give them more information about dementia. One man has a 35-year-old son who thinks that his dad is faking this whole thing because some days he acts normal. The son has watched me [in caring for dad] and learned what to do." (Personal care worker)
"[Use a care plan] to be able to assess their abilities, and for the family to realize what their abilities are." (Personal care worker)
Many paid care providers talked about the extent to which family and friends visit those who are living with dementia in care. While some patients living with dementia receive daily visits from family and friends, others may receive a visitor weekly or less. These participants feel that individuals living with dementia benefit from having someone come to visit and the resulting social interaction. Nonetheless, some of the participants said they understand that some family and friends may feel challenged in visiting their loved one with dementia, as the individual may not recognize or engage with their friends or family members.
"It's devastating for a family to see their parent or relative deteriorating. For some families, I've seen a daughter there every morning to give [their] parent breakfast. But a lot of residents don't have relatives. And some families are resistant to coming because when the patient does not recognize them or can even be angry and swear." (Nurse)
"Not having visitors is very difficult, probably only 20% of families come to visit. Not many can handle the stressors of seeing their parent or grandparent." (Psychiatric aide)
B. Comfort, Perceptions, Stigma
Comfort
Survey Findings
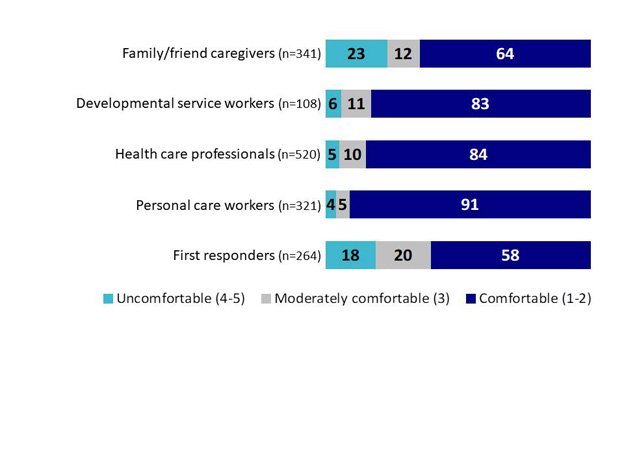
Paid care providers working in fields dedicated to the care of people living with dementia were much more likely than family and friend caregivers to say they are comfortable (i.e., 1 or 2 on the scale) with their ability to provide quality care and support. This includes 91% of personal care workers, 84% of health care professionals, and 83% of developmental service workers. In each case, only 4% to 6% indicated discomfort in their ability to provide care or support. Among paid care providers, first responders are considerably less likely to be comfortable in their ability to provide care or support to people living with dementia. Close to one in five (18%) said that they are uncomfortable and 20% are only moderately comfortable.
Among family and friend caregivers, 64% said they are comfortable with their ability. Close to one in four (23%), however, said they are not and another 12% said they are only moderately comfortable.
Chart 3: Degree of Comfort
Chart 3: Degree of Comfort - Text Version
This stacked chart shows the percentage of results for responses of five groups across three categories: uncomfortable, moderately comfortable, and comfortable. [1-Very comfortable, 3-Neutral, 5-Very uncomfortable]
Respondents were asked: "How comfortable do you feel with your ability to provide quality care or support to [people/someone] living with dementia?"
Respondents selected:
Family/friend caregivers (n=341)
Category "uncomfortable (4-5)": 23%
Category "moderately comfortable (3)": 12%
Category "comfortable (1-2)": 64%
Developmental service workers (n=108)
Category "uncomfortable (4-5)": 6%
Category "moderately comfortable (3)": 11%
Category "comfortable (1-2)": 83%
Health care professionals (n=520)
Category "uncomfortable (4-5)": 5%
Category "moderately comfortable (3)": 10%
Category "comfortable (1-2)": 84%
Personal care workers (n=321)
Category "uncomfortable (4-5)": 4%
Category "moderately comfortable (3)": 5%
Category "comfortable (1-2)": 91%
First responders (n=264)
Category "uncomfortable (4-5)": 18%
Category "moderately comfortable (3)": 20%
Category "comfortable (1-2)": 58%
Q9. How comfortable do you feel with your ability to provide quality care or support to [people/someone] living with dementia? (1-Very comfortable, 3-Moderately comfortable, 5-Very uncomfortable)
Base: n=1592
Among first responders, paramedics were most likely to indicate comfort in their ability to provide care and support (87%), although this is lower among police (46%) and other first responders (52%) including firefighters and security. Approximately 28% of other first responders said they are uncomfortable.
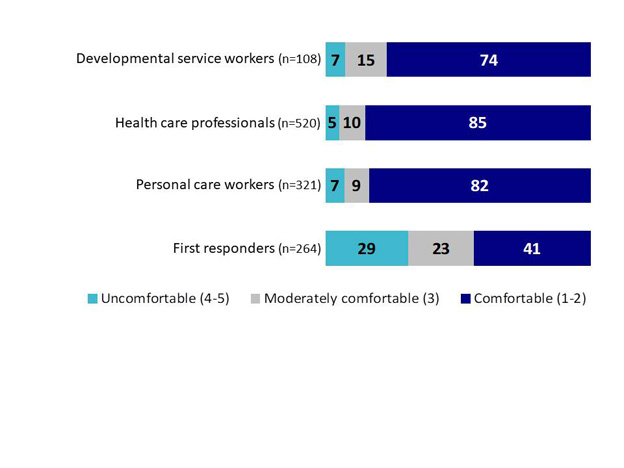
Among paid care providers, there is a similar level of comfort in their ability to provide dementia care where there are co-morbidities (i.e., providing a rating of 1 or 2 on a 5-point scale from very comfortable to very uncomfortable). The comfort level is about the same with and without co-morbidities among health care professionals (85% and 84% in either case). While high among personal care workers, it is not as high as comfort levels without the presence of co-morbidities (82% compared with 91%). Similarly, developmental service workers are also somewhat less likely to be comfortable with their ability to provide care in the presence of co-morbidities (74% vs. 83%). First responders are also less apt to be comfortable with their ability to provide support when the person has co-morbidities (41% comfortable compared with 58% where there are no co-morbidities). Close to one in three (29%) indicated discomfort.
Chart 4: Comfort with Providing Care in Presence of Comorbidities
Chart 4: Comfort with Providing Care in Presence of Comorbidities - Text Version
This stacked chart shows the percentage of results for responses of four groups across three categories: uncomfortable, moderately comfortable, and comfortable. [1-Very comfortable, 3-Neutral, 5-Very uncomfortable]
Respondents were asked: ". In your role, how comfortable do you feel providing quality care to / supporting people living with dementia who have additional health concerns (comorbidities) (e.g. treating multiple conditions, monitoring drug interactions, working with an interdisciplinary team, coordinating care)?"
Respondents selected:
Developmental service workers (n=108)
Category "uncomfortable (4-5)": 7%
Category "moderately comfortable (3)": 15%
Category "comfortable (1-2)": 74%
Health care professionals (n=520)
Category "uncomfortable (4-5)": 5%
Category "moderately comfortable (3)": 10%
Category "comfortable (1-2)": 85%
Personal care workers (n=321)
Category "uncomfortable (4-5)": 7%
Category "moderately comfortable (3)": 9%
Category "comfortable (1-2)": 82%
First responders (n=264)
Category "uncomfortable (4-5)": 29%
Category "moderately comfortable (3)": 23%
Category "comfortable (1-2)": 41%
Q10. In your role, how comfortable do you feel providing quality care to / supporting people living with dementia who have additional health concerns (comorbidities) (e.g. treating multiple conditions, monitoring drug interactions, working with an interdisciplinary team, coordinating care)? (1-Very comfortable, 3-Moderately comfortable, 5-Very uncomfortable)
Base: n=1252
Following the same pattern, paramedics are more likely to be comfortable with their ability to care for dementia patients with additional health concerns (74%), whereas only 27% to 32% of other first responders are comfortable, and 37% to 38% are not comfortable with their ability to provide support.
Among health care professionals and developmental service workers, nurses are the most likely to feel comfortable providing quality care to / supporting people living with dementia who have additional health concerns (90%).
Discomfort is also higher among men (15%), who are more likely to be first responders, as well as among care providers working in Alberta (19%). Care providers in the Atlantic (84%) are more likely than those in other areas to indicate comfort with this type of care.
When asked whether they are more comfortable providing care to a person without dementia than they are providing care to a person who is living with dementia, 52% of first responders said they agree or strongly agree (i.e., 4 or 5 on the scale). Four in ten (41%) family and friend caregivers said the same, and only 21% disagree or strongly disagree. Slightly fewer developmental service workers (34%) and health care professionals (33%) agree, although in each group the proportions agreeing and disagreeing are about the same. As many personal care workers (31%) agree, although nearly half (45%) disagree.
Table 3: Comfort with Providing Care
To what extent do you agree with the following statements about dementia? (1-Strongly disagree, 5-Strongly agree)
Family/friend caregivers
Developmental service workers
Health care professionals
Personal care workers
First responders
Q28B. I am more comfortable providing care to a person without dementia than I am providing care to a person who is living with dementia
n=341
n=108
n=520
n=321
n=264
Disagree (1-2)
21%
32%
36%
45%
25%
Neutral (3)
27%
29%
30%
21%
18%
Agree(4-5)
41%
34%
33%
31%
52%
Don't know/ No response
10%
5%
1%
3%
5%
Among First responders, police are more likely than others to agree they are not as comfortable providing care to someone with dementia (63%).
Discomfort is more common among men (46% agreeing compared with 35% among women), as well as among those under 35 (45% agree) and care providers in Quebec (44%).
Interview Findings (Comfort with Providing Care)
The large majority of care providers said they are comfortable with their ability to provide care to people living with dementia. Many attributed this to personal experience as a caregiver to a parent or other family members or friends.
"There was dementia in own family and I saw what good regiment of diet and engagement of activities can do." (Physiotherapist)
"I was the primary caregiver for late mother, so I learned a lot from that." (Program coordinator and counsellor)
Some said it has been their years of experience on the job; learning about what works and through trial and error, that has increased their comfort.
"I have a 35+ year career in supportive settings with people with disabilities or addictions, or mental health. I have such a broad spectrum." (Nurse)
"I learned through experience and paying attention to what the patient seems to be asking for." (Nurse)
"I was not as comfortable in the beginning, especially when faced with responsive behaviours, but I have become very comfortable with time. I have gained confidence as I build relationships and learn on the ward." (Physiotherapist)
Some paid care providers, particularly health care professionals or developmental service workers, feel more comfortable because they have received training on the nature of dementia, and in dementia care that has increased their comfort.
"I wasn't very knowledgeable and only moderately comfortable at first. I feel much better now because I have a better understanding and better guidance on the approach to use in communications and daily activities." (Direct case manager)
"I feel qualified and have a good background, but I have taken many courses and training through different professional associations." (Occupational therapist)
"I had basic training from the center (home for the elderly) on how to help patients, manipulate (turn) them, and how to feed them. I also have past experience as a social worker that gives basic tools on how to interact with the patients." (Personal care worker)
A few unpaid caregivers said they have been provided with dementia guidance through day programs, organizations, or paid care providers. A few also said they would have liked to have a source for dementia guidance on a range of topics to help them learn.
"The day program taught me some things and I have looked up things on the Internet, so I know more now (e.g., sponge bath). I would like to have 1 stop shopping for information on all kinds of different topics related to dementia care. It's hard to find. I don't know where to look for something specific to dementia." (Family and friend caregivers)
"I don't know if I was equipped with all the tools needed. I talked to people to find the information, but it wasn't easily available." (Family and friend caregivers)
"I feel good about it because I have (homecare) help and access to someone to discuss difficulties and solutions with." (Family and friend caregivers)
Some feel they simply have a disposition that is well-suited to work with individuals with dementia, who require the assistance of care providers who are patient, and compassionate, who are willing to take the time to build the necessary trust and understanding. A number of care providers said the key is taking time to understand the world through the experience and perspective of someone living with dementia.
"My biggest strengths are patience and tolerance. Patients are going to take a swing at you, call you names." (Psychiatric aide)
"You need to approach patients with courtesy and compassion, respect and dignity." (Nurse)
"I learned long ago that you have to meet them where they are and on the level they can understand you. You can't argue with them or force them to your point of view, it won't work. They aren't able to process it." (Program coordinator, counsellor)
"You really want to engage them and see for who they are. Get to know them. Just spend time building the relationship and getting to know them and talking with them because that's what they need and it helps me to engage with them successfully in the long run." (Physiotherapist)
"The biggest thing is to be patient and not try to rush through things. You need to not move too fast for them and explain things more thoroughly." (Paramedic)
A considerably smaller number of interview participants said they are not very comfortable, either because they feel they do not have adequate information about the nature of dementia or how best to communicate with or approach care with someone living with dementia. A few said they find the need for explanation and repetition draining. One said simply that it is heart-wrenching to see.
"I'm fairly comfortable. It can get tiring though - the repetition of answering same questions over and over. It's mentally draining." (Personal care worker)
Perceptions of dementia
Survey Findings
Survey respondents were asked about their level of agreement with regard to the abilities of people living with dementia in the years following diagnosis on a 5-point scale, from strongly disagree to strongly agree. For reporting purposes, we refer to scores of 1 or 2 on the scale as agreeing, a score of 3 as being neutral and scores of 4 or 5 as disagreeing. In terms of living independently, 75% of family and friend caregivers said they agree or strongly agree that someone living with dementia can sometimes continue to live in their own homes for years following diagnosis. The highest level of agreement is among health care professionals (81%), while only 66% to 69% of developmental service workers, personal care workers, and first responders agree. In fact, 13% to 14% of personal care workers and first responders disagree.
Most also believe that people living with dementia can sometimes continue to be active in the community for years following diagnosis, again with health care professionals most likely to agree (85%), although three in four of developmental service workers, personal support workers and first responders, as well as family and friend caregivers, also agree (74% to 77%). Only 3% to 10% of each of the five segments disagree.
Approximately half of developmental service workers (57%), health care professionals (53%) and first responders (53%) agree that people living with dementia can sometimes continue to work for years following diagnosis. Personal care workers are somewhat less apt to agree (41%) and 26% disagree. Family and friend caregivers are least likely to believe this to be true (35%), although 15% said they do not know.
Table 4: Perceptions of Abilities of People Living With Dementia
To what extent do you agree with the following statements about dementia? (1-Strongly disagree, 5-Strongly agree)
Family/friend caregivers
Developmental service workers
Health care professionals
Personal care workers
First responders
Q28A. [People/Someone] living with dementia can sometimes continue to live in their own homes for years following diagnosis
n=341
n=108
n=520
n=321
n=264
Disagree (1-2)
11%
7%
4%
14%
13%
Neutral (3)
11%
21%
12%
17%
15%
Agree(4-5)
75%
69%
81%
66%
67%
Don't know/ No response
3%
3%
3%
3%
6%
Q28E. [People/Someone] living with dementia can sometimes continue to work for years following diagnosis
n=341
n=108
n=520
n=321
n=264
Disagree (1-2)
22%
20%
16%
26%
15%
Neutral (3)
28%
19%
27%
25%
21%
Agree(4-5)
35%
57%
53%
41%
53%
Don't know/ No response
15%
3%
5%
8%
11%
Q28G. [People/Someone] living with dementia are sometimes able to continue being active in their communities for years following diagnosis
n=341
n=108
n=520
n=321
n=264
Disagree (1-2)
10%
7%
4%
8%
3%
Neutral (3)
12%
12%
8%
13%
14%
Agree(4-5)
74%
77%
85%
74%
77%
Don't know/ No response
5%
4%
3%
5%
6%
Care providers under 35 are less likely to agree that people living with dementia can sometimes live in their homes for years following diagnosis (68%). This is also true of care providers in Quebec (68%), and among those with a high school or college level of education (60% and 69%, respectively). Care providers in the Atlantic (85%) and those with a graduate level of education (78%) are more likely to agree that they can.
Paramedics (87%) are more likely to agree than police (78%) or other first responders (68%) that people living with dementia are sometimes able to continue being active in their communities for years following diagnosis. Women are also more likely to agree (80%) than men (74%). Those care providers who are 55 or older are somewhat less likely to agree (75%), compared to younger care providers (79% to 81%). Those with a high school level of education are least apt to agree (64%) whereas those with a graduate degree are most likely to agree (83%).
As with living independently, those with a high school level of education are least likely to agree (33%) that people living with dementia can sometimes continue to work for years following diagnosis, while those with a graduate degree are most likely to agree (50%). Unlike the pattern for those under 35 regarding independent living, this younger segment is most likely to agree that people living with dementia can continue to work for years (53%).
When asked about their perceptions and experiences regarding the comfort of other care providers communicating directly with people living with dementia, 51% of first responders and 55% of family and friend caregivers agree (4 or 5 on the scale) that some care providers are not comfortable. Around two-thirds of personal care workers (63%) and health care professionals and developmental service workers (66%) agree that some care providers are not comfortable, while relatively few disagree with this statement (7%-12%), providing a 1 or 2 on the scale.
Table 5: Perceived Discomfort Among Care Providers
To what extent do you agree with the following statements about dementia? (1-Strongly disagree, 5-Strongly agree)
Family/friend caregivers
Developmental service workers
Health care professionals
Personal care workers
First responders
Q28H. Some paid care providers are not comfortable communicating directly with [people/someone] living with dementia
n=341
n=108
n=520
n=321
n=264
Disagree (1-2)
10%
7%
10%
12%
8%
Neutral (3)
17%
20%
18%
18%
24%
Agree(4-5)
55%
66%
66%
63%
51%
Don't know/ No response
18%
6%
6%
7%
17%
Paramedics are more likely to perceive discomfort among some care providers when communicating directly with a person with dementia (68%) compared with other first responders (45% to 47%).
Perceiving discomfort among care providers when communicating with a person with dementia is also more prevalent among women (62% compared with 55% among men).
Those with a graduate level of education are also more likely to agree that some care providers are uncomfortable (64%).
Interview Findings (Perceptions of Abilities)
Perceptions about Ability to Live Independently
Interview participants are largely unanimous in their views about people living with dementia living independently in the community. Almost everyone said they believe that people living with dementia have the ability to do so, and that they believe this is preferable in the early stages of the disease, when cognitive function is only mildly compromised. Basic supports with meal preparation and assistance with shopping were described as necessary in the early stages of the disease.
"There are some people at the beginning and it's very minor. With input from family, close care, checking on them daily, they can manage." (Family and friend caregivers)
"A big part of the picture of keeping people in their homes is weekly assistance with cleaning, shopping, and meal preparation. There used to be a lot more access to home care than there are the last few years. That was a service that allowed a lot of people to stay in their homes." (Physician)
"There are some that are still in their homes alone. But home care people may go in twice a day to help with medication and help with breakfast, lunch, and suppers." (Personal care worker)
"...it depends on the level of dementia and degree of support and monitoring they have in the community, from family or friend or anyone. They also need to stay socially connected in some way." (Occupational therapist)
"Even people with more moderate to advanced dementia, with the right supports and routines, can definitely live what looks like normal lives. What helps is homecare services, seniors focused housekeeping services, family supports, access to financial management through either a family member, or easier access to services like those offered by the Office of the Public Trustee and Guardian. Those services are available but can be quite difficult to access." (Social worker)
How long they can live independently in the community, however, is perceived to depend first on the pace of the disease progression and, second on the availability of supports. Ongoing monitoring is believed to be key in assessing whether the progression of the disease requires an increased level of supports and whether those supports can be put in place quickly. Increased disease progression, according to some care providers, is believed to require added assistance with medications and basic personal hygiene.
"Yes, provided there are the proper supports in place in the home. This needs care and support of family and also professional supports in the home on a regular basis for meals, bathing/dressing and daily care, as well as ensuring that stove disabled, etc. and regular check-ins throughout the day. A nanny cam/baby monitor is useful to check-in and ensure they are ok." (Nurse)
"In the early stages, yes, it is possible. There needs to be ongoing monitoring though for progression, and then family supports (monitoring, keeping watch for symptoms and risk) and adding supports as they are needed to match progression is important to maintain the consistency." (Physician)
The concern raised, however, was the rate or predictability of decline, which some believe can be sudden in some cases, leaving little time to react in terms of increased supports and safety. Most participants emphasized the need for regular monitoring and assessment related to safety issues that may present themselves. Reduced ability to safely operate a stove or microwave; to enter and exit their home safely, and to know how to find the way home are examples described of possible challenges affecting those with cognitive decline.
"At some point, it is not sustainable to be in the community if cognitive function is significantly impaired. When a person still has insight into their erosion and things they cannot do it helps. Once they lose that, it becomes harder if they are not aware." (Occupational therapist)
"There is not enough support for the individual in the community. Not enough home care options and not enough awareness that these options even exist. (They) can live alone but only in early stages. Then need more support from others, and even then, only while workable/sustainable. Many live in community, but it doesn't mean they should when their care is compromised. I've seen many decline in community because they are not supported enough and then improve when in long-term care because they are getting better care and attention, more social contact and stimulation. So, (it) depends on degree of dementia and on supports." (Nurse)
"It's an ongoing, everyday assessment and monitoring. You don't know when it's going to change or what danger/risk will present itself. And, as a family member you are guarded and watching and you are always questioning your own judgments which may be compromised because of being too close and emotional involved. It's hard to judge the right time for more support." (Family and friend caregivers)
"There needs to be support and monitoring for changes/assessment, and see what resources are needed and that the level of resources is increasing as the risk assessment is increasing, so that there is a steady/good match here. It's where this balance is out of whack and the needs are higher than the support to cover it that you get into a crisis situation, which is when bad things happen." (Nurse)
Sustainability of the situation, particularly for caregivers, is also perceived to be a key element in the decision to remain in the community or transition to a long-term care setting. As the disease progresses, and challenges affecting those with cognitive decline increase, home care and other respite options are believed to be important to avoid caregiver burnout over the longer term. Wandering and incontinence were both noted as triggers in the decision to enter long-term care. Increased unresponsive and uncooperative or aggressive behaviours were also described as a perceived third type of trigger.
"When the situation is sustainable (e.g., respite for caregivers) it works fine." (Nurse)
"They soon lose social references, not recognising even their closest ones, they lose the sense of orientation, get lost outside their room." (Nurse)
"Essentially, when the requirements for monitoring or medicating starts to become unsafe for the person with dementia or their partner, or if the person with dementia is a wanderer, that's a deal-breaker. "(Physician)
"(Disease) progression means more intensive care from caregivers (meals and meds and then personal care), and the family can become exhausted (burn out). Also, incontinence and violence can quickly push the needs past what family can provide or cope with. That is when long-term care becomes the next step." (Physician)
Another key concern with independent living for people living with dementia is perceived to be the stability of symptoms from day-to-day and even hour-to-hour. As a few described, a person with dementia can be managing symptoms and doing well one day, and wandering or aggressive on another day, making part-time support risky, given the lack of predictability.
"The situation needs to be individualized to meet that specific person's needs. That can be tricky because the level and needs can change day to day. But, generally, when the level/match is right, you can see it, that everything seems to be working. When it's not, it can come to a boil quickly and then there are unnecessary admissions to hospital/long-term care. It's always better when it's planned and the decisions are in place for when they need to be." (Nurse)
"The problem with living alone is that you don't know/can't predict when they will have good periods of time and bad ones. They can change in an hour and often do later in the day (sundowning)." (Personal care worker)
"The problem too is that they have good days and bad days, and you can't tell what is going to be what. It's not linear or predictable so they can be at risk. (It turns on a dime)." (Paramedic)
"It's about level of care and safety, but cognitive ability can fluctuate quickly, even day to day, or from a time in day to another time in day (e.g., sundowning)." (Paramedic)
Inevitable Part of Aging
Only a few of the interview participants said they believe that dementia is a normal part of aging, but even these individuals contextualized this with observations of increasing vascular issues and other illnesses such as diabetes, driving up the incidence of dementia. Many also said they perceive the rate of dementia to be increasing (i.e., that it seems to be more common than it used to be); however, some participants attribute the increase in dementia to both an increase in the diagnosis of dementia and in life expectancy.
"Starting to believe that it is inevitable more and more as we all age. My dad then my mom. With high BP and vascular issues it can be a big driver, then also other chronic diseases like Diabetes, it affects so many." (Family and friend caregivers)
"Residents are living longer and of course we are going to see more dementia now." (Recreation therapist)
Many perceive dementia as not being "inevitable" because many people in their 90's still have good cognitive function. Some participants described a wide variation between individuals who have already started to decline cognitively in their 60's compared with some who are still doing well decades later into their lives. A few participants pointed to a perceived dichotomy where some individuals enjoy good physical health but develop dementia, while others may experience more physical decline but be "sharp" cognitively. Overall, most participants believe there is no one path that determines an inevitable aging process.
"There are 90-year-old people who don't have anything wrong with their memory but their body is shot." (Family and friend caregivers)
"I wouldn't say it's normal or should happen. There can be people who are 100 and sharp, and people who are younger and have dementia." (Nurse)
"We have to get away from this type of labeling. It needs to be recognized as a disease process (i.e., symptoms of a disease and its progress). It is not normal, it is a disease. If it's "normal", it becomes your fault." (Physician)
"Common to have memory issues, but dementia is something else. It's more fundamental confusion and perception issue. But, it does seem to be becoming more and more common." (Paramedic)
In explaining that dementia is not a "normal" part of aging, most participants pointed to key risk factors such as vascular issues like high blood pressure and stroke as being connected with dementia. Others pointed to co-morbidities and other chronic illnesses such as diabetes. Some also believe that dementia is hereditary since a number of participants pointed to genetics as a risk factor. One physician included infections among the elderly as a contributor to developing dementia. A few participants believe that brain injuries have been linked to a subsequent onset of dementia.
"You see a fair amount of vascular dementia so you have to watch blood pressure, sugars, and cholesterol levels, as well as regular exercise and healthy diet and healthy weight. Diabetic epidemic is also showing up as dementia later in life as well." (Physician)
"Brain injury is another risk factor, although obviously less preventable." (Nurse)
"Be cognizant of family history and watch for indicators. Have your spouse know family history so that they are aware of things to look for." (Search and rescue)
Many participants said they perceive lifestyle choices as risk factors that could affect an individual's propensity to develop dementia. These participants perceive immoderate alcohol and drug use as risk factors. Some participants said that some physical lifestyle factors can help to prevent dementia such as eating healthy and exercising. A few participants pointed to "environmental" conditions as a perceived risk factor.
"Alcohol abuse for example, or cardiovascular disease, contribute hugely to dementia. And, I've seen examples of some reversal of symptoms as well, especially with removal of alcohol. So, risk can be increased or decreased, and actual onset or symptoms can also be ameliorated in some cases." (Nurse)
"It's mostly about lifestyle, I think. If you have had ongoing stress and a hard life, it is harder on your body over time. Having a lot of stress, and alcohol or drug abuse are contributors." (Direct support worker)
Quality of Life
Interview participants found the question of quality of life to be interesting. While they almost uniformly perceive that people living with dementia can have a good quality of life, there were layered views about what this means and what is needed to ensure it.
Many participants have varying beliefs on the concept of quality of life as it means different things to different people, and can vary greatly depending on stages of dementia. For those who are in the early stages, for example, quality of life might come from a continued degree of activity and social connection. This was noted by interview participants as providing a good quality of life, while also keeping cognitive decline at bay. Most suggested that a higher quality of life might come from living among familiar surroundings and remaining at home as long as possible. Participants said that for some people living with more advanced dementia, they believe quality of life can involve sitting by a window, sitting outside, or hearing their favourite music.
"(It's) about meeting them where they are. If their dementia is mild, and they have a good support system, they can have a good quality of life. Someone with more dementia and needs more care, if there is a place with more recreation activities for them and have people who are well trained and understand their needs so that they are not trying to reorient them and causing them stress. You want to see that they are happy, engaged in activities or the people around them, and have a bit of a social life, be it family or friends. Look out for people who are distressed or depressed, withdrawn or upset." (Personal care worker)
"(It) depends on severity, level of articulation and what stimulates them (what they like), but yes, they can be engaged and have enjoyment and feel belonging/involvement. Even in severe cases can have some quality of life (although diminished/narrowed), they can have moments of enjoyment in activity/music, food, etc. At some point (in severe cases) quality of life is just about being calm and not angry, upset, stressed and frustrated/agitated all the time. If not, then quality can be very poor." (Occupational therapist)
"If they are engaged and feel like they are contributing to something. If they have some kind of activity that gets them out and keeps them moving around a bit. They need to feel they are connecting and stimulated by something that gets their interest." (Day program counsellor & coordinator)
Participants described situations they believe need to be in place for people living with dementia to have a good quality of life. As described, this starts with the individual. The nature and rate of the progression is perceived to be a key factor in quality of life and many described eroding quality of life over time as symptoms become more severe. More severe symptoms are perceived to compromise ability to engage in activities and connect with others, and for some, increases the level of fear of and apathy about the world around them. Some participants, however, believe that quality of life can come from enjoyment or comfort in the moment, even if it is not remembered shortly afterwards.
"(We) used to take mother to Christmas concerts. She really enjoyed them even if she didn't remember them afterwards." (Family and friend caregivers)
"Isolation and loneliness can have a significant impact on dementia and decline." (Physician)
"As long as they are connecting and able to have some communications, have some visits and be active, have something to give them enjoyment." (Personal care worker)
"...some become trapped in their head. (It) depends on capacity. When they become non-verbal they don't have a ton of quality. But, you can still see sometimes that something draws them out or moves them (e.g., music). If you can give them something that comforts them (e.g., doll is their baby to care for) and they are contributing in some way then it gives them something and engages them." (Personal care worker)
"When they are in the moment and happy, they are content and have good quality of life. They don't know they are not correct or processing incorrectly, so as long as they don't feel challenged and you are meeting them where they are and not trying to bring them into your reality, they are quite content. When you challenge them on their reality (as not the right reality) they become confused and insulted, which is when they lash out and have responsive behaviours. If you are supporting and validating their perceptions/experiences and what they can contribute, they feel more confident and content, so are not angry and suffering." (Direct support manager)
A key element to quality of life, however, is perceived by some participants as the degree of acceptance or contentment of the person living with dementia regarding their situation, or their emotional state. For some people living with dementia, this is about how content and positive they are by nature (i.e., "happy people"), some believe. Some participants, however, perceive increasing contentment with the progression of dementia, where the person living with dementia is less aware of who they are and what they have lost, and therefore less frustrated and angry.
"Some people are very tortured in their dementia, but others are quite placid. But, if you are not overly frustrated by your decline, and generally going with the flow things are generally better. Having social connections and/or you have something to do/engage you with your time it helps a lot as well to feel not too frustrated." (Physician)
"(One of the) residents was very angry and ill-tempered. She swore and pushed everyone away, but now she is happier. In her case, I think that forgetting has actually helped her let go of some of the frustrations she had." (Personal care worker)
"They can be very happy. My father is now childlike and it is easy to make him happy. He is enjoying life, doesn't care that he is incontinent." (Nurse, Family and friend caregivers)
"They do as long as caregivers and care providers engage with them in a meaningful and consistent way. They need to be stimulated and reminded of the connection to their past and that they are still a person. That maintains quality of life. Otherwise, they withdraw and feel angry and/or isolated/alone and uninterested." (Physician)
"If (they are) content to sit in warm sunshine and relax, can easily thrive, but if need to be busy and contributing, it may be harder to accept and be content. If someone can be calm and relaxed and content in whatever they are able to do, they quality is good. When they are frustrated though and agitated, they quality is poor." (Occupational/Physiotherapist)
Many participants perceive quality of life to be associated with the quality of dementia care provided. Many said they believe that the best situation is when the person living with dementia has caregivers who are able to support them appropriately at their current stage of dementia, with the capacity to increase care as needed. This might mean family checking in on and bringing food to an individual during the early stages of dementia, as well as monitoring the situation closely for progression. As needed, it might mean caring for them in the same home, and keeping them in an environment they are comfortable in and know well. These situations, however, are perceived to require flexibility on the part of the caregiver to meet the increasing needs.
"(The situation has to be right) If services are available to the person. (Example) A couple where one spouse has dementia and both can live at home together." (Physician)
"As soon as we warehouse people in nursing homes, they are out of their environment. They are away from where they are comfortable, or even have physical objects they were used to. They are not as resilient as they used to be to adapt. But they can have a good quality of life, of course. It has to do with being amongst those who are your loved ones. Being part of a community and being respected." (Nurse)
"They could have a good quality of life, and it is more than likely at home. It's where they are most comfortable, no one likes being in the hospital for a period of time. They would need to have the proper supports at home, and ideally by family. That's not an option for every person, depends on their level of dementia and financial option. If you have lots of money you can find high end care homes or assisted living." (Paramedic)
"Yes, if they are with the right people (caring for them). Whether it's the family or the caregivers, you have to be very patient." (Personal care worker)
A few participants perceive that the quality of life of people living with dementia as largely influenced by care providers, not just for physical care, but also engagement, and that people living with dementia are not able to reach out and initiate engagement themselves. Similarly, some participants believe that the broader community also has a key role to play in engaging people living with dementia in the community, which requires a more widespread and deeper understanding of the nature of dementia and how to communicate with people living with dementia.
"They need a Champion to make it happen and meet their needs for involvement, contact and interaction/engagement." (Family and friend caregivers)
"They won't reach out and do that (engage) for themselves, someone else has to do it for them. That is why community is so important and has so much of a role to play. Everyone in the community can play a role in keeping people [living] with dementia engaged and active, but you also have to understand it well enough to communicate appropriately." (Family and friend caregivers)
"They can't generate their own quality of life, it has to be generated for them by others around them. They are often too afraid to be motivated to seek out stimulation. They are afraid to interact with the world around them so they withdraw unless others keep them engaged. If they have no social connection then quality of life is much lower and they fade." (Paramedic)
"....elderly can be overlooked in our society, particularly in the west. Some cultures care for elderly more than we do. We have more of a throw-away society. Attitudes need to change in that regard to value elderly. It's not just about lack of care in government/public institutions but among families as well." (Paramedic)
Stigma
Survey Findings
Stigma is defined as negative attitudes or discrimination against someone based on a distinguishing characteristic such as a mental illness, health condition, or disability. Care providers were asked to indicate their level of agreement with a number of statements regarding stigma about people living with dementia from 1-strongly disagree to 5-strongly agree. ,
Roughly half of care providers agree that negative stereotypes about dementia are common within the health care system. This includes 53% of family and friend caregivers, and 56% to 57% of developmental service workers and health care professionals who agree or strongly agree that negative stereotypes are common. Slightly fewer personal care workers agree (48%, with 22% disagreeing), and fewer than four in ten (39%) first responders agree. It is noteworthy, however, that 13% of first responders and 12% of family and friend caregivers said they did not know if negative stereotypes are common in health care or not.
Approximately two-thirds of developmental service workers (65%) and 59% of health care professionals believe they have witnessed a reduction in the quality of care that people living with dementia have received due to stigma. This is also true of 54% of personal care workers and 50% of family and friend caregivers, although 21% to 22% disagree or strongly disagree. While 44% of first responders said they have witnessed a reduction in the quality of care due to stigma, larger proportions were either neutral (25%) or said they do not know if this is the case (15%), compared with other care providers.
Table 6: Perceptions Related to Stigma
To what extent do you agree with the following statements about dementia?
Family/friend caregivers
Developmental service workers
Health care professionals
Personal care workers
First responders
Q28C. Negative stereotypes (stigma) about [people/someone] living with dementia are common within the health care system
n=341
n=108
n=520
n=321
n=264
Disagree (1-2)
15%
11%
16%
22%
18%
Neutral (3)
20%
27%
24%
24%
30%
Agree(4-5)
53%
56%
57%
48%
39%
Don't know/ No response
12%
6%
3%
7%
13%
Q28F. I have witnessed negative stereotypes (stigma) reduce the quality of health care received by those living with dementia
n=341
n=108
n=520
n=321
n=264
Disagree (1-2)
22%
18%
16%
21%
16%
Neutral (3)
18%
13%
21%
17%
25%
Agree(4-5)
50%
65%
59%
54%
44%
Don't know/ No response
10%
5%
4%
8%
15%
Among first responders, paramedics are most likely to agree (53%) that negative stereotypes are common within the health care system.
Women (53%), those with a graduate degree (56%) and care providers in Ontario (57%) are also more likely to agree that negative stereotypes are common within the health care system.
Among first responders, paramedics are most likely to have witnessed stigma reduce the quality of care received by those living with dementia (65%).
Care providers with a graduate degree (58%) are also more likely than other care providers to have witnessed negative impacts on quality of care.
Interview Findings (Stigma)
Across all five types of care providers, about one in four did not perceive stigma as a pervasive issue, while the majority did. Most focused on stigma among paid care providers, although some paid care providers spoke about stigma among family members or in the community. A few family and friend caregivers mentioned stigma in terms of other family and friends feeling uncomfortable interacting with, or visiting less often, the person living with dementia. Stigma was often described by care providers in terms of misunderstanding or misjudging the abilities of people living with dementia. Only a few talked about discomfort in being around or not knowing what to do or say to a person with dementia.
Many participants said they believe that some paid care providers do not adequately understand how to assess the abilities of people living with dementia and are not adequately trained in how to recognize and modulate communications and care to the level of the specific individual with dementia. Some described interactions where care providers ignore or do not include the individual in conversations or in decisions and information they should have. Others described situations of care providers doing too much for the individual, robbing them of the opportunity to do things for themselves.
"I see people talking over someone or talking about their disease in front of them, or correcting them. Talk about them like they aren't in the room. Or getting frustrated with them. They need to be included and treated like a person and engaged." (Family and friend caregivers)
"You see the lack of communications of some, the impatience and eye rolling and gritting of teeth of staff at LTC. Many don't want to be there." (Family and friend caregivers)
"Some care providers are very quick to jump in and do things for people with dementia instead of seeing what they can do for themselves and assessing and sitting back and letting them do it. It may be quicker and easier to do it for them, but then they don't have the chance to do for themselves and feel they are independent and have pride in accomplishment and they disengage and let everyone do everything for them. It's very important for them to feel that they are respected enough and asked/expected to try to do what they can for themselves." (Physiotherapist)
Some interview participants pointed to what they believe are pressures on the system, understaffing and a lack of time, as the primary reasons for paid care providers to sometimes make assumptions or take shortcuts. They also said this lack of time results in a lack of opportunity to engage with patients, reducing the level of stimulation they receive.
"It's too hard and they don't have enough time. Between the lack of training and the caseload there is exhaustion and burn out, so patients suffer." (Family and friend caregivers)
"Workers are all short on time and so some will find it easier to take shortcuts in the commitment to their care. There is generally far too much burden on the system and there are daily, real life situations so many are faced with making decisions about getting it all done." (Nurse)
"The bigger issue is simply the lack of resources and time to be able to spend any time with them to engage them." (Personal care worker)
"Busy staff don't have time to engage them, and don't have time to let people with dementia do things for themselves (faster to just do it for them), but this robs them of opportunity to take responsibility and do things for themselves (e.g., wash face). You need to have them do things for themselves as much as possible, and they want to be able to do things for themselves as well. Need to avoid the reduction in independence, which is so easy to fall into." (Personal care worker)
Some family and friend caregivers and paid care providers perceive that some people working in the industry may not have the right disposition to work with people living with dementia, and possibly people with reduced cognitive function for any reason. Many, however, pointed to a lack of training and information about dementia, and how to communicate with and care for dementia patients.
"Some people are good at that and others can be almost uncomfortable to watch in terms of their interaction with people with dementia. They are not cut out for this population and some are not well trained." (Physician)
"Care providers need to understand the critical importance of consistency in engaging with/stimulating. Personal beliefs infiltrate the quality of care and that's a slippery slope. You start to not stimulate as much and the patient starts to withdraw, the provider gets bored and ignores the person living with dementia more, and patient withdraws even more, (and the erosion continues)." (Physician)
"I love working with elderly and am very comfortable around dementia. We just connect and laugh, but for many it's not comfortable and they don't understand it." (Paramedic)
When talking about stigma among family members of people living with dementia, some paid care providers described a perceived lack of fundamental understanding among families about dementia and the impacts on perception, cognitive function, and memory. They described perceptions of family talking over or excluding the individual, as though they are not in the room, resulting in resentment and withdrawal on the part of the person with dementia. In some cases, families were described as having trouble accepting or denying the degree of disease progression. Some said that friends can also drop away over time because of a lack of understanding, but also because of discomfort in not knowing what to say or difficulty facing their personal fears regarding dementia.
"Family don't always recognize/understand where the person with dementia is currently at re: abilities, so they are not always well versed/prepared in how to care for family." (Nurse)
"People can underestimate their capabilities or diminish respectful treatment. This not only demeans but also undermines cooperation (e.g., grabbing by the arm to bring somewhere will only result in further confusion and resistance whereas gentle and straight forward talk will get you where you need to go). It requires understanding of abilities and communication skills." (Nurse)
"This is a huge issue, especially with family not engaging them. People with dementia feel it and know they are being excluded." (Personal care worker)
"Lots of people with dementia don't have family and friends who want to visit them anymore. They don't know what to say or do. It's hard for them." (Personal care worker)
"Some people even in the same age group will react. It's a reminder to them, that it could be them, and they don't want to think about it." (Personal care worker)
Some care providers feel that stigma can impact quality of care as care providers may underestimate the abilities of the person living with dementia or perhaps rush their care / interaction with the patient. These care providers described situations where other care providers would approach a person living with dementia in a manner that is brisk and not adaptive to the situation. As described, some people living with dementia may not be able to get out of bed in the morning as quickly as other health patients for a bath or to eat. By not adapting care for people living with dementia, the patient can become agitated and it further affects the type of interaction between care providers and a person living with dementia. Further, some care providers described that stigma can result in care providers assuming that a person living with dementia does not know or care how they are being treated.
"They don't have a voice so people are just running over them. You can't build a relationship of trust like that!" (Family and friend caregivers)
"They feel shut out and criticized or dismissed for their disease symptoms. They don't feel included or wanted. It is a very frustrating disease because you feel lost and useless. You feel unable to be connected with the world and you feel you can no longer contribute." (Physician)
"There is a stigma when you label the individual as unable. It can be really distressing to a dementia patient when they are losing their feeling of control and being valued." (Nurse)
"It is demoralizing to people with dementia and hampers the rapport built up (or no rapport builds up)." (Occupational therapist)
"I may have built a connection and relationship with a patient and then from 1 day to the next they have changed and are more distant, distrusting and frustrated. They have seen someone else in between and sometimes that doesn't go well. They feel dismissed and not seen, and they get frustrated or disconnect. So, I have to start all over again to build that trust and draw them out again." (Physiotherapist)
C. Knowledge, Training and Resources
Risk and Protective Factors
Survey Findings
Among dementia prevention interventions, social isolation was identified as the most important risk or protective factor that should be prioritized, according to family and friend caregivers (66%), personal care workers (60%), first responders (59%), health care professionals (55%) and developmental service workers (51%). Physical inactivity was noted by 51% of family and friend caregivers as an important risk factor that should be prioritized. Depression was recognized by developmental service workers and personal care workers (41% each), but less so by health care professionals (28%). Education was reported by about one-quarter of all care providers (22 to 27%) as an important protective factor that should be prioritized in dementia prevention interventions.
Table 7: Risk/Protective Factors
Col1
Family/friend caregivers
Developmental service workers
Health care professionals
Personal care workers
First responders
Q27. Based on your knowledge, what are the three most important risk or protective factors that should be prioritized in dementia prevention interventions?
n=341
n=108
n=520
n=321
n=264
Education
27%
25%
26%
25%
22%
Hearing loss
17%
11%
12%
12%
6%
Hypertension
11%
6%
9%
3%
3%
Obesity
2%
6%
7%
3%
6%
Smoking
3%
6%
9%
3%
5%
Depression
39%
41%
28%
41%
36%
Physical inactivity
51%
33%
38%
33%
31%
Social isolation
66%
51%
55%
60%
59%
Diabetes
6%
5%
9%
4%
3%
Air pollution
0%
0%
1%
1%
0%
Alcohol consumption
13%
24%
25%
21%
27%
Traumatic brain injury
14%
31%
23%
28%
29%
Genetics/family history
1%
1%
1%
1%
1%
Drug abuse
1%
0%
2%
0%
0%
Diet/nutrition/oral care
1%
1%
3%
2%
0%
Dementia education and assessment/monitoring
0%
1%
1%
0%
0%
Social/brain stimulation
0%
2%
2%
2%
0%
Stress, instability (housing, poverty)
0%
1%
1%
1%
0%
Other (please specify)
9%
10%
8%
8%
2%
Not sure
6%
2%
3%
7%
9%
Don't know / No response
4%
3%
4%
4%
9%
Among health care professionals and developmental service workers, physicians (26%) are more likely than others to identify smoking as a risk.
Among first responders, police (66%) are most likely to identify social isolation as a risk factor. Women (61%) are also more likely than men (54%) to identify social isolation as a risk factor.
Younger care providers (under age 35) are more likely to identify traumatic brain injury (34%) and alcohol consumption (30%), while older care providers (55 and over) are more likely to say education (29%) or hearing loss (14%).
Regionally, those in Ontario are apt to say physical inactivity (44%) or education (34%), while those in Quebec are more likely to identify social isolation (66%), traumatic brain injury (33%) or alcohol consumption (32%) as risk or protective factors.
Those with a college education (29%) are most likely to name a traumatic brain injury as an important risk factor.
Interview Findings (Risk/Protective Factors)
Social connection and general brain stimulation were raised as important factors that could slow the pace of dementia progression. Most participants said they believe social isolation is a contributor to cognitive decline, therefore, continuing social connections, not living alone, and joining social groups can help delay the development of dementia symptoms. Many participants also noted a "use it or lose it" attitude towards cognitive function, and said that keeping the mind active through puzzles, card games, and bingo can all help increase focus and concentration and generally mitigate the onset or progression of dementia.
"Engagement and stimulation of the brain, memory, cognition and social interaction are huge factors. Need to keep the brain exercised. Social isolation is a big factor in decline." (Occupational therapist/Physiotherapist)
"Social connection and engagement are also factors that can mitigate the onset or progression of dementia." (Physician)
"Socialization is key. Isolation is a key driver. If on their own in (the) community and do not have contact it gets worse, especially if they live alone." (Nurse)
"There are [genetic] risk factors, and some you can control. You may not be able to control whether you get dementia, but you can do some mindfulness things and brain agility - puzzles, minimizing distractions. I worry about dementia, so I try to stay active and not isolate." (Nurse)
"Community involvement is number one. Get out and volunteer. Join groups, church groups or meditation group or walking group." (Recreation therapist)
Many participants pointed to a mixture of risks that can contribute to cognitive decline; noting there is not just one factor that determines the propensity to develop dementia. These participants identified a combination of genetics, lifestyle choices, social connection, and mental stimulation as contributors to the development of dementia.
"Heredity you can't do anything about. That's one of the first determinants - if there was a family history. The other is taking care of self in terms of exercise, maintaining physical strength and agility, and mental strength and agility. Making a point of having regular interactions with other people, social interactions." (Physician)
"It's linked with concussion, stroke, genetics, lifestyle factors like stress and exercise, social connection." (Personal care worker)
"I don't think it's normal. But it seems to be that there are a lot more people being diagnosed with dementia at younger ages. I've seen different kinds of dementia, like due to drinking. Usually younger people, alcoholics. A few had strokes so vascular dementia." (Personal care worker)
"Its related to general health and co-morbidities, previous health issues, diet, use of drugs and alcohol, but also a personality thing - outlook and attitudes - whether engaged and have sense of purpose or distancing and disengaging from life." (Occupational therapist/Physiotherapist)
"No, not normal, co-morbidities contribute - cardiovascular, diabetes, but also lifestyle (stress, exercise, social connection and stimulation in community within circle is key). Use it or lose it." (Occupational therapist/Physiotherapist)
A moderate number of interview participants said they are not aware of factors associated with the risk or prevention of dementia. This is most prevalent among family and friend caregivers, and first responders. Some personal care workers also said they do not feel knowledgeable about dementia risk factors; although many personal care workers identified social connections and cognitive activity as viable methods of slowing cognitive decline.
"Have not looked into it. I fall into the category of not very knowledgeable about it." (Firefighter)
"I don't feel too knowledgeable. I look at the brain as a muscle, work out your brain to stay as strong as it can." (Paramedic)
"I really don't know if there is anything. Don't know if it's food related, or environment related, or what are the causes of dementia." (Family and friend caregivers)
"Never thought of that. Do you want to send me something that would do that?" (Family and friend caregivers)
"Would not say I'm terribly knowledgeable about dementia prevention. You hear that it is good to keep your brain active, and be physically active." (Personal care worker)
"[Do] not know if dementia can be prevented but mental exercises as simple as crossword puzzles can maybe help." (Personal care worker)
Self-Rated Knowledge
Survey Findings
Respondents were asked to rate themselves from 1 (least knowledgeable) to 5 (most knowledgeable) in a variety of areas related to dementia prevention, diagnosis, care, and treatment. For reporting purposes, we refer to scores of 1 or 2 on the scale as less knowledgeable, a score of 3 as moderately knowledgeable and scores of 4 or 5 as more knowledgeable. Regarding dementia prevention and reducing risk, developmental services workers (43%), health care professionals (41%), and to a lesser extent, personal care workers (36%) feel more knowledgeable. Conversely, first responders (64%) and family and friend caregivers (43%) said more often that they are less knowledgeable about dementia prevention and risk reduction.
When assessing their knowledge of screening for dementia or making a diagnosis, 41% of health care professionals, 32% of developmental service workers, and 31% of family and friend caregivers said they are more knowledgeable, however, in each case a similar number of respondents rated themselves as less knowledgeable (33%, 36%, and 40%, respectively). Only 22% of personal care workers and 11% of first responders said they are more knowledgeable about screening for and diagnosis of dementia (47% and 64%, respectively rated themselves as less knowledgeable).
Related to stigma and how to reduce it, over half of the health care professionals and developmental service workers (56%)said they are more knowledgeable. This is also the case among 47% of personal care workers. Among family and friend caregivers, 37% said they are more knowledgeable, and another 31% said they are less knowledgeable in this area. Only 28% of first responders rated themselves as more knowledgeable in this area as high, while 42% described themselves as less knowledgeable.
When assessing their knowledge of treatments and care for those living with dementia, nearly three-quarters of personal care workers (72%) said they are more knowledgeable. Health professionals (68%), developmental service workers (57%), and family and friend caregivers (46%) also rated themselves as more knowledgeable. Only 26% of first responders said they are more knowledgeable in this area, and 44% said they are less knowledgeable.
Regarding advance care planning and end-of-life care for those living with dementia, health care professionals rated themselves as more knowledgeable the most often (52%), followed by personal care workers (45%), developmental service providers (41%) and family and friend caregivers (39%). Among first responders, 63% said they are less knowledgeable and only 15% said they are more knowledgeable in this area.
Table 8: Self-rated Knowledge
How would you rate your knowledge in each of the following areas? (1-Least knowledgeable, 5-Most knowledgeable)
Family/friend caregivers
Developmental service workers
Health care professionals
Personal care workers
First responders
Q15A. Dementia prevention / reducing risk
n=341
n=108
n=520
n=321
n=264
Less knowledgeable (1-2)
43%
29%
27%
33%
64%
Moderately knowledgeable (3)
28%
23%
29%
23%
18%
More knowledgeable (4-5)
23%
43%
41%
36%
11%
Don't know/ No response
5%
6%
3%
7%
8%
Q15B Screening for dementia / Making a dementia diagnosis
n=341
n=520
n=108
n=321
n=264
Less knowledgeable (1-2)
40%
36%
33%
47%
64%
Moderately knowledgeable (3)
26%
25%
21%
21%
16%
More knowledgeable (4-5)
31%
32%
41%
22%
11%
Don't know/ No response
3%
6%
5%
10%
8%
Q15C Stigma related to dementia and how to reduce it
n=341
n=520
n=108
n=321
n=264
Less knowledgeable (1-2)
31%
13%
15%
22%
42%
Moderately knowledgeable (3)
27%
27%
26%
24%
22%
More knowledgeable (4-5)
37%
56%
56%
47%
28%
Don't know/ No response
5%
5%
4%
7%
8%
Q15D Treatment and care of someone living with dementia
n=341
n=520
n=108
n=321
n=264
Less knowledgeable (1-2)
25%
17%
11%
8%
44%
Moderately knowledgeable (3)
28%
22%
18%
17%
24%
More knowledgeable (4-5)
46%
57%
68%
72%
26%
Don't know/ No response
1%
4%
2%
3%
6%
Q15E Advance care planning and end-of-life care for those living with dementia
n=341
n=520
n=108
n=321
n=264
Less knowledgeable (1-2)
35%
31%
24%
28%
63%
Moderately knowledgeable (3)
23%
22%
20%
20%
13%
More knowledgeable (4-5)
39%
41%
52%
45%
15%
Don't know/ No response
3%
6%
4%
7%
9%
Dementia prevention / reducing risk
Among health care professionals and developmental service workers , nurses and pharmacists are more likely to say they are more knowledgeable (48%) while health technicians are the least likely to say this (50% rated themselves as less knowledgeable in this area).
Among first responders, police are most likely to rate themselves as less knowledgeable (71%).
Women self-rated as having more knowledge in this area (34% report themselves to be knowledgeable versus 23% for men). However, women make up a higher proportion of personal care workers, health care professionals and developmental service workers sampled (81%, 78% and 75% respectively). It is also noteworthy that workers in these sectors typically rated themselves as more knowledgeable in all listed categories compared to first responders, 61% of whom are men. The pattern of women reporting more often reporting themselves to be more knowledgeable compared with men follows in all subject matter areas being self-assessed. The variation between men and women among those who rated themselves as more knowledgeable ranges from 6% to 18% depending on the list item.
Those in Quebec more often rated themselves as more knowledgeable compared with those in other regions.
Screening for dementia / Making a dementia diagnosis
Among health care professionals and developmental service workers, physicians are the most likely to describe themselves as more knowledgeable in this area (67%). Those working as technicians are the most likely to rate themselves as less knowledgeable (61%).
Those with high school or college levels of education are more likely to rate themselves as less knowledgeable (55% and 48% respectively), while those with a graduate level more likely to describe themselves as more knowledgeable (37%).
Stigma related to dementia and how to reduce it
Among health care professionals and developmental service workers, psychologists and social workers are more likely to say they are more knowledgeable in this area (69%), as are therapists (67%). Those working as health technicians are least likely to do so (30% reported they are knowledgeable).
Paramedics are more likely than other first responders to see themselves as more knowledgeable (43% compared with 20%-25% among those working in other first responder roles).
Those living in Atlantic Canada (60%) are more likely to describe themselves as more knowledgeable compared with those residing in other regions. Conversely, those in Quebec more often described themselves as less knowledgeable in this area (29% rated low).
Knowledge of treatments and care
Among health care professionals and developmental services workers, nurses and pharmacists (78%) along with therapists (77%) are most likely to rate themselves as more knowledgeable in this area. Health technicians along with psychologists and social workers are more likely than others to say they are less knowledgeable (29% and 20%, respectively).
Paramedics are the most likely among first responders to rate themselves as more knowledgeable (60% rated high), while police officers most often rated themselves less knowledgeable (60% rated low).
Regionally, those in Quebec and Alberta rated themselves as less knowledgeable compared with those living in other areas of the country (24%) .
Those who completed graduate studies are more likely to see themselves as more knowledgeable in this area (60%), while those with a high school education are least likely to do so (28% rated themselves as less knowledgeable).
Advance care planning and end-of-life care for those living with dementia
Among health care professionals and developmental service workers, physicians (66%), along with nurses and pharmacists (63%) are more likely to have rated themselves as more knowledgeable. Those working as technicians as well as those in other roles are least likely (52% and 35%, respectively rated themselves as less knowledgeable).
Police officers are the least likely among first responders to describe themselves to be more knowledgeable in this area (74% rated low), while paramedics are the most likely to do so (29% rated themselves as more knowledgeable).
Those under the age of 35 are more likely to rate themselves as less knowledgeable (43%), as are those residing in Quebec (41%).
Those who completed graduate programs are more likely to describe themselves as more knowledgeable (46%) while those with an undergraduate degree are less likely to do so (45% rated themselves as less knowledgeable).
Knowledge
In terms of thinking about dementia and its symptoms through the lens of a disease process compared to viewing it as a normal part of aging, most care providers generally agree or strongly agree it is not a normal part of aging. Health care professionals are most likely to believe that dementia is not an inevitable part of aging (68%), as is also the case among 62% of family and friend caregivers. Fewer developmental service workers (54%), personal care workers (51%), and first responders (48%) believe that dementia is not a normal part of aging. In fact, 27% of personal care workers and 25% of first responders and developmental service workers believe it is inevitable.
Table 9: Knowledge
To what extent do you agree with the following statements about dementia?
Family/friend caregivers
Developmental service workers
Health care professionals
Personal care workers
First responders
Q28D. Dementia is a normal/inevitable part of ageing (1-Strongly disagree, 5-Strongly agree)
n=341
n=108
n=520
n=321
n=264
Disagree (1-2)
62%
54%
68%
51%
48%
Neutral (3)
18%
19%
15%
18%
20%
Agree(4-5)
15%
25%
16%
27%
25%
Don't know/ No response
5%
3%
2%
4%
7%
Among health care professionals and developmental service workers, physicians are least likely to view dementia as a normal part of aging (7%), with 80% disagreeing with this idea.
Men (26%), and those under 35 (25%) as well as care providers in Quebec (25%) are more likely to see dementia as a normal part of aging than their counterparts.
Training in Dementia Care
Survey Findings
Survey respondents rated the extent they felt they could use more preparation/training in a variety of areas related to dementia prevention, diagnosis, care, and treatment on a 5-point scale, from 1 (needing the least additional preparation/training) to 5 (the most additional preparation/training). For reporting purposes, we refer to scores of 1 or 2 on the scale as needing minimal additional preparation/training, a score of 3 as needing a moderate amount of additional preparation/training and scores of 4 or 5 as needing much more preparation/training.
The majority of developmental service workers (60%) and personal care workers (52%) felt they could use much more preparation or training in dementia prevention and reducing risk. Close to half of health care professionals (46%) and over one-third of first responders (38%) said they could use much more training in dementia prevention and reducing the risk.
Over half of developmental service workers (55%) reported that they could use much more preparation or training in screening for dementia or making a dementia diagnosis. Less than half of personal care workers (46%) and health care professionals (42%) feel they could use much more training in these areas. Just over one-third of first responders (35%) feel they would benefit from much more training on screening and diagnosis for dementia.
Personal care workers (54%) were most likely to report they could use much more training on the treatment and care of someone living with dementia. Roughly four in ten developmental service workers (47%), first responders (41%), or health care professionals (40%) reported they could use much more training on treatment and care.
Results vary more greatly among types of care providers when it comes to training on advance care planning and end-of-life care for those living with dementia. This ranges from 56% of developmental service workers, 52% of personal care workers, 41% of health care professionals, and a low of 31% among first responders reporting that they need much more training and preparation on this topic.
Many developmental service workers (56%) feel they could use much more training on how to make interactions with care providers feel safer and more supportive. Nearly half of personal care workers (49%), and closer to four in ten health care professionals (42%), and first responders (42%) feel the same.
Table 10: Need for Training (Paid care Providers)
To what extent do you feel you could use more preparation/training in each of these same areas? (1-Need the least preparation/training, 5-Need the most)
Developmental service workers
Health care professionals
Personal care workers
First responders
Q16A. Dementia prevention / reducing risk
n=108
n=520
n=321
n=264
Minimal additional preparation/training (1-2)
10%
20%
15%
23%
Moderate amount of additional preparation/training (3)
20%
25%
20%
16%
Much more preparation/training (4-5)
60%
46%
52%
38%
Not applicable
6%
7%
7%
17%
Don't know/ No response
3%
2%
6%
6%
Q16B Screening for dementia / Making a dementia diagnosis
n=520
n=108
n=321
n=264
Minimal additional preparation/training (1-2)
18%
24%
17%
23%
Moderate amount of additional preparation/training (3)
17%
21%
14%
17%
Much more preparation/training (4-5)
55%
42%
46%
35%
Not applicable
7%
12%
16%
19%
Don't know/ No response
4%
2%
7%
6%
Q16C Treatment and care of someone living with dementia
n=520
n=108
n=321
n=264
Minimal additional preparation/training (1-2)
19%
29%
22%
20%
Moderate amount of additional preparation/training (3)
28%
26%
17%
20%
Much more preparation/training (4-5)
47%
40%
54%
41%
Not applicable
3%
4%
3%
15%
Don't know/ No response
3%
1%
3%
5%
Q16D Advance care planning and end-of-life care for those living with dementia
n=520
n=108
n=321
n=264
Minimal additional preparation/training (1-2)
18%
27%
16%
28%
Moderate amount of additional preparation/training (3)
21%
22%
18%
16%
Much more preparation/training (4-5)
56%
41%
52%
31%
Not applicable
3%
9%
8%
20%
Don't know/ No response
3%
1%
5%
5%
Q16E How to make interactions with care providers feel safer and more supportive
n=520
n=108
n=321
n=264
Minimal additional preparation/training (1-2)
17%
28%
19%
18%
Moderate amount of additional preparation/training (3)
23%
25%
21%
24%
Much more preparation/training (4-5)
56%
42%
49%
42%
Not applicable
2%
3%
7%
11%
Don't know/ No response
2%
2%
5%
5%
Regionally, those in Quebec are more likely to say they could use much more preparation/training in all five areas.
Psychologists/social workers (52%) are more likely to say they could use much more training in screening for dementia, while physicians (25%) are least likely to say the same. Women (45%) are also more likely to say this.
Younger care providers (under age 35) (49%), along with women (45%), are more likely to say they could use much more training in advance care planning and end-of-life care.
Younger care providers (under age 35) (52%) are more likely to say they could use much more training on how to make interactions with care providers feel safer and more supportive.
Using the same scale, family and friend caregivers were most likely to say they need much more preparation or training in dementia subtypes and states of progression (54%) and advance care planning and end-of-life care (54%). Fewer feel they could use much more training in the day-to-day care of someone living with dementia (48%), dementia screening and diagnosis (43%) or dementia signs and symptoms (43%).
Table 11: Areas for Further Training (Family/Friend Caregivers)
To what extent do you feel you [could use/could have used] more preparation/ training in each of these areas? (1-Need the least preparation/training, 5-Need the most)
Family/friend caregivers
Q17A. Dementia signs and symptoms
n=341
Minimal additional preparation/training (1-2)
29%
Moderate amount of additional preparation/training (3)
21%
Much more preparation/training (4-5)
43%
Not applicable
5%
Don't know/ No response
1%
Q17B Dementia screening and diagnosis
n=341
Minimal additional preparation/training (1-2)
24%
Moderate amount of additional preparation/training (3)
21%
Much more preparation/training (4-5)
43%
Not applicable
9%
Don't know/ No response
3%
Q17C Dementia subtypes and stages of progression
n=341
Minimal additional preparation/training (1-2)
16%
Moderate amount of additional preparation/training (3)
24%
Much more preparation/training (4-5)
54%
Not applicable
4%
Don't know/ No response
2%
Q17D Day-to-day care of someone living with dementia
n=341
Minimal additional preparation/training (1-2)
23%
Moderate amount of additional preparation/training (3)
21%
Much more preparation/training (4-5)
48%
Not applicable
5%
Don't know/ No response
4%
Q17E Advance care planning and end-of-life care
n=341
Minimal additional preparation/training (1-2)
24%
Moderate amount of additional preparation/training (3)
15%
Much more preparation/training (4-5)
54%
Not applicable
5%
Don't know/ No response
2%
Family and friend caregivers in Quebec are more likely to say they could use much more training in advance care planning and end-of-life care (75%), dementia subtypes and states of progression (71%), dementia screening and diagnosis (67%), and dementia signs and symptoms (63%).
Interview Findings (Training)
In interviews, some paid care providers said they received training for the type of dementia care they are providing. This included course-work or modules throughout their formal education that provided information on dementia and adapting care for those living with dementia. Training, in a few cases, was provided through their employer in the form of job orientation or delivered through in-service learning days or other training opportunities. Physicians particularly noted the availability of training programs that can be offered to staff, although staff turnover can limit the ability to build knowledge in a facility.
"Yes, have a good background but have had quite a lot of training. Often 1-2 day courses with modules. Much easier now online. Have specific training in elderly and dementia - movement, organization, cognition, communications, dealing with aggression." (Occupational therapist/Physiotherapist)
"They offer two types of training where I work and have taken them both. One is called 'gentle persuasive approaches'. It's about noticing when someone is agitated and trying to change their focus. The other is non-violent crisis intervention. If a resident was trying to grab your hair, tricks to get away. Feel well trained. I took my course and I'm licensed. You update the two training (sessions) at work every two years." (Personal care worker)
"Received a one-day training on aggressive behaviour of dementia patients." (Personal care worker)
"Have had certificate course on communicating with PWD to engage and support them in respectful and friendly way to build trust and establish relationship (so they open up to you), and you can engage and stimulate." (Personal care worker)
"There are many programs one can take for staff training. Pieces program is offered to everyone. You First program is there for everyone who starts to work with elderly/dementia. [...]Training is something that should be a focus but there is also staff turnover that can get in the way." (Physician)
While the mention of any specific training was diverse, Alzheimer's Society organizations were referenced by some care providers as a resource for training needs for both paid care providers and family and friend caregivers of those living with dementia. One first responder (search and rescue) said that they invited a representative from the provincial chapter of the Alzheimer's Society to conduct training on how to interact with individuals living with dementia.
"[Alzheimer's] Society has been a big help because they lead us to so many other online learning, websites/resources." (Direct support manager)
"We recently had a Zoom talk that was geared towards 'how do we interact with a person with dementia', put on by a lady from the Alzheimer's Society. We had another session about 5 years ago." (Search and rescue)
Many paid care providers reported that they have become capable of caring for those living with dementia as a result of on-the-job training. Although a few of these care providers have received formal training on providing care for those living with dementia, many said that their experience caring for patients on the job has served as training and resulted in an aptitude for providing relevant and appropriate care. This on-the-job training has helped them to assess different situations and adapt their care depending on the individual, the level of dementia, and the response of the individual throughout their care.
"There are some basic competency requirements when graduated, but mostly it's ongoing training and by far the biggest contribution is on the job training." (Nurse)
"Have absolutely no training at all in care in general let alone dementia care. We are completely untrained. Just learning as we go on the job. It would be good to have training, some tips and tricks on communicating better or getting better compliance or how to engage and stimulate effectively." (Personal care worker)
"Have learned on the job and sharing with clients and families, so see more of what to do, what works, and see some families managing really well, with good strategies." (Personal care worker)
Most family and friend caregivers indicated that they do not feel well trained to provide care for someone living with dementia. A few family and friend caregivers had received some training to care for someone living with dementia through their job, or generally had experience in providing health care as a result of their employment. A few said that they used visits with the doctor of the person living with dementia as an avenue to ask for information on how to care for the individual, or consulted with other friends or acquaintances who may be a health care professional or have experience caring for their own loved one living with dementia. Many family and friend caregivers feel that they now have enough experience to feel that they can provide adequate care for their loved ones. This experience was gained through learning what works and what does not for the person living with dementia and was adapted as needs changed, rather than through formal training. A few family and friend caregivers said that they received some handouts or brochures at the time of diagnosis to learn more about dementia. Some reported that they could use more resources on how to care for someone living with dementia, and feel that the resources available tend to include general information on dementia and not practical information or "training" on how to care for someone living with dementia.
"Need actual help with stimulation and engagement and caring for and solutions. Like a family or caregiver management program with all kinds of themes and how to and tips and tricks to use to get things done." (Family and friend caregivers)
"They would give you a pamphlet at the hospital, saying if you have dementia, these are some of the things you may experience. There was a lack of understanding among our family about what dementia does." (Family and friend caregivers)
"Speak with LPN who gives me guidance and information. [...] The rest is just trial and error, and you find what works." (Family and friend caregivers)
Many paid care providers said they would like to have the opportunity for more specialized training in caring for people living with dementia. Many nurses said that there should be more of an emphasis on dementia in nursing programs. Some paid care providers said that they would like to take more training, but it is not offered by their employer. A few reported that while some quick training options, such as one day or ‘lunch and learn' sessions, are available, it is difficult to fit this type of training into the day or to build enough knowledge based on only several hours of training.
"It's when you have half day and day long sessions that it works and staff have to sign up and are paid for that time so they take it. Then you can have better focus on a theme/several related areas. Best to be scenario-based and grounded in shared experiences of some things staff commonly face. Then they have real life examples and actual context." (Nurse)
"If you seek it out, there is lots there you can take/pick up, but you have to know about it first of all and then you have to be able to fit it into your day, around your caseload. Sometimes you can and sometimes you can't. There is no time set aside for professional learning." (Occupational therapist/Physiotherapist)
"It's almost all on the job training. There is "in service" which is a regular update type of training we do in off hours to recap on issues and protocols and learn of something new." (Paramedic)
Dementia Guidance Resources
Survey Findings
Two in three health care professionals (68%) said that they know where to find resources related to dementia prevention and reducing risk. About six in ten developmental service workers (60%) or personal care workers (59%) reported that they know where to find this information. Fewer family and friend caregivers (41%) or first responders (35%) know where to find resources on dementia prevention and reducing risk.
Nearly three in four health care professionals (73%) know where to find information on dementia screening and diagnosis. Fewer developmental support workers (64%), family and friend caregivers (59%), or personal care workers (50%) know where to find information on dementia screening and diagnosis; the minority of first responders (36%) know where to go for this information.
Most health care professionals (83%), personal care workers (79%), and developmental service workers (76%) know where to find resources on the treatment and care of someone living with dementia. Family and friend caregivers (65%) and first responders (53%) are least likely.
The majority of developmental service workers (58%) and health care professionals (55%) know where to find resources related to stigma reduction. Less than half of personal care workers (49%), family and friend caregivers (31%), and first responders (30%) said they would know where to find this information.
Health care professionals and developmental service workers (69% each) were more likely to report they know where to find information on advance care planning and end-of-life care. Nearly two-thirds of personal care workers (61%) also know where to find this information. Fewer family and friend caregivers (48%) and first responders (32%) said they would know where to go for this information.
Over half of developmental service workers (59%) and personal care workers (54%) said they would know where to find culturally appropriate tools that give consideration to a patient's cultural background, personal experiences, and norms. Nearly half of health care professionals (48%) and about one-quarter of first responders (26%) or family and friend caregivers (24%) said they know where to find culturally appropriate tools.
Table 12: Resources
Would you know where to find resources related to dementia on these topics if you needed them to support your care providing role?
Family/friend caregivers
Developmental service workers
Health care professionals
Personal care workers
First responders
Q18A. Dementia prevention / reducing risk
n=341
n=108
n=520
n=321
n=264
Yes
41%
60%
68%
59%
35%
No
48%
25%
23%
27%
44%
Not applicable
7%
10%
4%
7%
13%
Don't know/ No response
5%
5%
4%
7%
8%
Q18B Dementia screening and diagnosis
n=341
n=520
n=108
n=321
n=264
Yes
59%
64%
73%
50%
36%
No
30%
21%
17%
27%
43%
Not applicable
6%
9%
6%
13%
15%
Don't know/ No response
5%
6%
4%
10%
6%
Q18C Treatment and care of someone living with dementia
n=341
n=520
n=108
n=321
n=264
Yes
65%
76%
83%
79%
53%
No
27%
13%
12%
12%
31%
Not applicable
4%
6%
3%
2%
9%
Don't know/ No response
4%
6%
3%
6%
7%
Q18D Stigma reduction
n=341
n=520
n=108
n=321
n=264
Yes
31%
58%
55%
49%
30%
No
51%
29%
36%
33%
47%
Not applicable
9%
4%
3%
7%
13%
Don't know/ No response
9%
9%
6%
11%
9%
Q18E Advance care planning and end-of-life care
n=341
n=520
n=108
n=321
n=264
Yes
48%
69%
69%
61%
32%
No
40%
19%
20%
21%
45%
Not applicable
6%
7%
7%
11%
16%
Don't know/ No response
6%
5%
4%
7%
7%
Q18G Culturally appropriate tools
n=341
n=520
n=108
n=321
n=264
Yes
24%
59%
48%
54%
26%
No
46%
27%
44%
33%
55%
Not applicable
22%
2%
3%
5%
11%
Don't know/ No response
7%
12%
5%
8%
8%
Those with a graduate degree are more likely to say they know where to find resources on all topics, with the exception of culturally appropriate tools.
Dementia prevention / reducing risk
Physicians (84%), along with police (46%) are more likely to say they know where to find resources for dementia prevention/reducing risk.
Dementia screening and diagnosis
Physicians (93%), along with women (60%) and police (46%) are more likely to say they know where to find resources for dementia screening and diagnosis.
Stigma reduction
Psychologists/social workers (72%), those in Ontario (50%), and police (38%) are more likely to say they know where to find information on stigma reduction.
Advance care planning and end-of-life care
Physicians (80%), along with women (59%) and paramedics (50%) are more likely to say they know where to find resources for advance care planning and end-of-life care.
Culturally appropriate tools
Police (32%) are more likely than other first responders to indicate they know where to find culturally appropriate tools.
Interview Findings (Guidance Resources)
Some paid care providers said they try to stay current on the latest dementia advice to provide care for people living with dementia. Aside from workshops and training mentioned previously, a few care providers reported that their employer has material available that outlines guidelines and best practices to provide care for people living with dementia, or that they discuss best care practices and garner advice from their colleagues. A few care providers said that due to the information provided through their employer, along with on-the-job knowledge they have attained, they do not tend to look for any further information.
"There's always something out there, they come up with new best practices to improve it. The private company I worked with sent out emails all the time." (Personal care worker)
"Some reading but nothing specific. Just treat with humanity and understanding and try to place things as much as you can on their terms. Need to try to find solutions and brainstorm with teammates about best care." (Personal care worker)
"Where I am presently, the staff and manger are pretty good at coming up with solutions. We brainstorm and come up with what works as changes in patients happen." (Personal care worker)
"Hospital library has search so queue in OT and dementia and sent list of new articles every month to sift through." (Occupational therapist/Physiotherapist)
Some paid care providers pointed to sources of information that they have accessed or would trust to learn about the latest dementia advice. Most mentioned non-profit organizations with a specific focus on dementia as a primary source of information. A few said that videos from Teepa Snow have been a practical and useful resource. A few said that if they were going to look for information on dementia care, they would generally search online, or go to Health Canada, provincial or regional health departments.
"The Alzheimer's Society would be an excellent resource to start." (Psychiatric aide)
"An excellent resource has been the Alzheimer's Society." (Physician)
"One resource is Teepa Snow who has videos that are down to earth and practical solutions on providing care to persons living with dementia. Hands on, easy approaches to make it lighter." (Personal care worker)
"I would trust things that came from Health Canada, government and regulatory agencies like [municipal] Health Authority or [provincial] Health." (Firefighter)
Some paid care providers feel that there is guidance available if you look for it. Some others said they are not aware of and would like access to guidance on the ways to mitigate the progression of the disease, how to manage aggressive behaviours, as well as care practices (i.e. how to improve the quality of life of those living with dementia). These paid care providers predominantly said that they would like practical "how to" information, demonstrating best practices and advice on providing care in the form of courses or videos.
"Having how to videos of tips and tricks for daily things like personal care or engaging/communicating would be really good to have. Would want it to be real life situations." (Personal care worker)
"Need to know how to make the quality of life better for them when working with them. Courses would be the best. Online, the videos are good so you can actually see something to relate to." (Personal care worker)
Most family and friend caregivers said they get most of their dementia advice from doctors and nurses providing care for their loved one, or from support groups. A few reported receiving brochures from the doctor assessing the person living with dementia or that they wait until an appointment with the doctor, or when a nurse may attend the home every month or two, to ask questions about providing care and what to expect as the dementia progresses. A few said that they get advice on providing care by attending "sharing groups", meetings through non-profit organizations with a specific focus on dementia, and particularly during COVID-19 restrictions, online support groups. A few family and friend caregivers said they are not sure where to go for information. A few identified specific areas in which they could use more information. These included a guide to community resources, what care is available for different stages of dementia, and generally understanding the different stages of dementia.
"Didn't really look up information because it was easier to talk to a nurse about how to handle situations." (Family and friend caregivers)
"We go ahead with what we have and if something comes up we go to the doctor." (Family and friend caregivers)
"For families, it would help to get information on the resources available, the roles of each player [doctor, nurse, social worker], as well as a guide to community resources." (Family and friend caregivers)
"Went down to the Alzheimer's Society. They are great, but there's nothing available [in person] right now. I told them that when they open up we'll be back." (Family and friend caregivers)
"My sister got a pamphlet and is reading up. Got to see the criteria to assess the stage that my mom is at." (Family and friend caregivers)
D. Culturally Appropriate Care/Tools
Survey Findings
Culturally appropriate care involves considering a patient's cultural background, personal experiences, and norms. Respondents were asked if they have the necessary tools in order to provide culturally appropriate care or support for people living with dementia for certain populations. Among paid care providers, 41% of developmental service workers, 37% of health care professionals and personal care workers, and 34% of first responders said that they had the necessary tools available to provide care for ethnic and cultural minority communities.
Culturally appropriate tools to provide care or support for Indigenous People living with dementia were reported to be available according to 36% of personal care workers, 35% of first responders, 33% of health care professionals, and 31% of developmental service workers.
Results are more varied among types of care providers when it comes to the availability of tools to care for people with intellectual/developmental disabilities. This ranges from a high of 69% of developmental service workers, 53% of personal care workers, and 49% of health care professionals, down to 38% among first responders.
Tools to support LGBTQ2+ were reported to be available according to 40% of developmental service workers, 38% of health care professionals, 36% of first responders, and 34% of personal care workers.
Culturally appropriate guidance for official language minority communities were reported to be available according to 37% of developmental service workers, 33% of personal care workers, 32% of health care professionals, and 27% of first responders.
Tools were reported to be available to provide care for rural and remote communities for 42% of personal care workers, 39% of health care professionals, 39% of developmental service workers, and 34% of first responders.
Culturally appropriate tools for those living with young onset dementia were reported to be available for 42% of personal care workers, 42% of developmental service workers, and 38% of health care professionals, but only among 28% of first responders.
Table 13: Paid Care Providers - Availability of Necessary Tools
Do you have the necessary tools in order to provide culturally appropriate care or support for people living with dementia for the following populations?
Developmental service workers
Health care professionals
Personal care workers
First responders
Q22A. Ethnic and cultural minority communities
n=108
n=520
n=321
n=264
Yes
41%
37%
37%
34%
No
44%
51%
45%
45%
Not applicable
6%
4%
10%
11%
Don't know/ No response
9%
8%
7%
9%
Q22B Indigenous peoples
n=520
n=108
n=321
n=264
Yes
31%
33%
36%
35%
No
56%
55%
47%
45%
Not applicable
6%
5%
9%
11%
Don't know/ No response
6%
8%
8%
9%
Q22C People with intellectual/developmental disabilities
n=520
n=108
n=321
n=264
Yes
69%
49%
53%
38%
No
27%
39%
34%
43%
Not applicable
2%
4%
6%
9%
Don't know/ No response
3%
7%
7%
10%
Q22D LGBTQ2+
n=520
n=108
n=321
n=264
Yes
40%
38%
34%
36%
No
46%
48%
44%
42%
Not applicable
6%
4%
12%
11%
Don't know/ No response
8%
10%
11%
10%
Q2E Official language minority communities
n=520
n=108
n=321
n=264
Yes
37%
32%
33%
27%
No
51%
54%
48%
52%
Not applicable
6%
6%
9%
12%
Don't know/ No response
6%
8%
10%
9%
Q2F Rural and remote communities
n=520
n=108
n=321
n=264
Yes
39%
39%
42%
34%
No
48%
43%
38%
41%
Not applicable
7%
12%
11%
16%
Don't know/ No response
6%
6%
9%
9%
Q2G Young onset dementia
n=520
n=108
n=321
n=264
Yes
42%
38%
42%
28%
No
45%
50%
40%
53%
Not applicable
6%
4%
11%
9%
Don't know/ No response
6%
7%
7%
11%
Ethnic and cultural minority communities
Nurses and pharmacists are less likely than other health care professionals and developmental service workers (32%) to say they have tools available for ethnic and cultural minority communities.
Among first responders, police are more likely to report that tools are available (42%) compared with other first responders.
Indigenous peoples
Among first responders, paramedics were more likely to report the availability of these tools (46%) compared with others.
Care providers in Alberta (44%) and the Prairies (44%) are more likely to say they have culturally appropriate tools for Indigenous Peoples.
Those with a college (37%) background are more likely to say they have the necessary tools, particularly compared with those with higher levels of education.
People with intellectual/developmental disabilities
Among health care professionals and developmental service workers, nurses and pharmacists are less apt to say they have to the necessary tools (45%).
LGBTQ2+
Among health care professionals and developmental service workers, availability of the tools necessary to provide culturally appropriate care or support for LGBTQ2+ people living with dementia was most likely to be reported among those providing psychological or social services (48%).
Younger care providers (under age 35) are more likely than older care providers to say they have the necessary tools for LGBTQ2+ populations (41%).
Official language minority communities
Results do not vary significantly between different types of paid care providers in terms of availability of tools adapted for official language minority communities.
Rural and remote communities
Paramedics (56%) are much more likely than other first responders to say they have tools available for rural and remote communities.
Regionally, those in Atlantic Canada (57%) are more apt to have the necessary tools for rural and remote communities. This is least often reported to be the case in Quebec (34%).
Young onset dementia
Those with a college education (42%) are more likely than those with other levels of education to have tools on young onset dementia.
Culturally Appropriate Guidance Use among Family and Friend Caregivers
Survey respondents were asked if they have the necessary tools in order to provide culturally appropriate care or support for people living with dementia who are also likely to be at higher risk of developing dementia and who may experience barriers to care, including to diagnosis and access to dementia supports and services. These populations include: ethnic and cultural minority communities, Indigenous peoples, people with intellectual / developmental disabilities, LGBTQ2+, official language minority communities, rural and remote communities and young onset dementia.
Among family and friend caregivers for someone living with dementia, 10% have provided care or support for someone living with dementia in an ethnic and cultural minority community, among Indigenous peoples, or in LGBTQ2+ communities who has been identified as being likely to be at a higher risk for developing dementia.
Chart 5: Family and Friend Caregivers - Care for Higher Risk Populations
Chart 5: Family and Friend Caregivers - Care for Higher Risk Populations - Text Version
This pie chart shows the percentage of results for responses to one question across three categories: yes, no, and DK/NR.
Respondents were asked: "[Do/Did] you provide care or support for someone living with dementia in any of the following populations (e.g., ethnic and cultural minority communities, Indigenous peoples, LGBTQ2+, etc.)?"
Respondents selected:
Category "yes": 10%
Category "no": 85%
Category "DK/NR": 5%
Base: n=331
Q24. [Do/Did] you provide care or support for someone living with dementia in any of the following populations (e.g., ethnic and cultural minority communities, Indigenous peoples, LGBTQ2+, etc.)?
Base: n=331
Family and friend caregivers age 35-54 (21%) are more likely to say they provided care or support for LGBTQ2+ communities, however, the sample size for family and friend caregivers in that age group was small (n=48).
Among a relatively small number of family and friend caregivers who have provided care for someone in the higher risk populations (n=48), 42% said they used culturally appropriate resources.
Chart 6: Family and Friend Caregivers– Use of Culturally Appropriate Resources
Chart 6: Family and Friend Caregivers– Use of Culturally Appropriate Resources - Text Version
This pie chart shows the percentage of results for responses to one question across three categories: yes, no, and DK/NR.
Respondents were asked: [Do/Did] you use any culturally appropriate resources when providing care or support? (Culturally appropriate resources include advice or recommendations that give consideration to a patient's cultural background, personal experiences and norms.)"
Respondents selected:
Category "yes": 42%
Category "no": 40%
Category "DK/NR": 19%
Base: n=48
Q25. [Do/Did] you use any culturally appropriate resources when providing care or support? (Culturally appropriate resources include advice or recommendations that give consideration to a patient's cultural background, personal experiences and norms.)
Few participants were aware of culturally appropriate guidance specifically designed for higher risk groups living with dementia. A few have received general culturally appropriate training, in terms of interacting with patients who are from cultures other than their own; however, the training was not specific to caring for those living with dementia. To support cultural needs, a few participants noted that their facility tries to connect care providers with patients of the same language or culture, which helps the patient feel more comfortable, and the care provider to better understand their needs.
"You need to work with people's beliefs and cultural background to be able to work with them in a respectful and useful manner. We emphasize this in training all the time. You have to focus on what the patient believes, and much of this can come from cultural background." (Physician)
"Yes, the culture really affects their behaviour. As a care giver you need to be aware of the culture to know what is the norm. We were given training, we had in-service days by the [facility] all the time." (Personal care worker)
This training was provided to help co-workers understand the culture of one another, to work more effectively together. A few participants said that culturally appropriate guidance was provided for care providers who are new Canadians to better understand the culture and needs of their patients. For example, one participant described providing training to new care providers on dementia diagnosis and care, as some care providers were from cultures that did not recognize dementia as being "real".
"What I noticed is that some international nurses would say that dementia is non-existent in their culture. Maybe these international nurses don't see people who are generally older and develop dementia. Those who said they didn't have dementia in their elderly, they said they felt that it was preventative in diet, such as using turmeric. For some cultures, elderly is respected and taken into their homes as they age. In Canada, there are many who can't live on their own and then go into care homes. Culturally, elderly people in Canada don't want to be a burden on their family. Nurses from other countries would say, 'how could you put your family in a nursing home'. It's a shock to some people." (Nurse)
Some participants said that they would like to have access to culturally appropriate guidance in providing care to those living with dementia. These participants feel that having these tools would help to provide care in a manner that builds trust and understanding with the person living with dementia, and for adapting care based on a patient's cultural or religious background. This could include formal training, written materials or handouts, or access to information online. In the absence of formal training, some participants said that they rely on interactions with the family of the person living with dementia to learn about their culture, in addition to their specific history and needs.
"Yes, have occasion to have clients with different cultures, religions and languages all the time. Don't really have any culturally appropriate tools and resources at all. You only have access to family and talking to others about culture, expectations, to try and figure it out. And, you can misstep if you don't know. It would be great to have tips, scenarios, for different cultures and access to some tools in different languages." (Occupational therapist/Physiotherapist)
"I would like culturally appropriate guidance, it would be useful, but not something that I've been provided. We are asked to take the more broad cultural training we are given and then try and apply it the best we can to the work we are doing at any given moment. Would like the training, because often with dementia patients that have reached an advanced stage, it is a challenge. With patients who have their faculties, we put a strong emphasis on their autonomy and choice. With dementia, there is difficulty with this. I'm not comfortable directing them [with what they should do] because it rubs against my other cultural training." (Medical social worker)
Some participants explained that they encounter challenges relating to language barriers with those living with dementia; for example, an individual may speak English as a second language but have progressed in their disease to the point of communicating only in their original language. In these instances, access to someone who can speak their language is required to communicate. A few participants said that dementia guidance available in various languages would be helpful to provide to patients and families, including how to provide support to a family member living with dementia.
"Language barriers are a problem, especially as patient starts to lose language anyway. Need questions, diagnostic tools, support and care language and questions in many languages. Always walking around with your phone to access Google translate, which is very helpful. ‘Here is the bathroom, this is your bed, good morning!'" (Nurse)
"It would be good to have more educational tools for family that is culturally appropriate, in different languages and cultural references, because the family sometimes doesn't understand what is happening either, so having the ability to explain to them or give them a handout for them to read through to help them understand what is going on would be helpful." (Occupational therapist/Physiotherapist)
"Yes, occasionally need these tools in different languages in particular. Have access to interpreters who can be on the phone or in live online call. We use a circulating iPad to connect with them and patient at same time. Less need for cultural context, since rely on families when this is needed. They can fill you in." (Occupational therapist/Physiotherapist)
Some participants said they do not have access to culturally appropriate guidance; nor do they feel that they need this guidance as they are working with a population that is not culturally diverse.
"In my workplace, there is little cultural or ethnic diversity." (Recreation therapist)
"Not applicable with the residents we have." (Program counsellor/coordinator)
E. Factors Impacting Quality of Care and Challenges
Factors Affecting Quality of Care
Survey Findings
Among potential challenges affecting the ability to provide quality dementia care or support, listed in the survey, better sharing of information across care providers or in care settings (57%) and more dementia care training (54%) were noted most often as making a significant difference. In particular, health care professionals reported the sharing of information as a key area for change (63%) to have a positive impact, notably more than half of each type of provider agreed (52-56%).
Having more time to spend with those with dementia is another area where many care providers feel change is needed, particularly personal care workers (48%) and health care professionals (40%). Increased mental health supports is also considered a key area for positive change, particularly among family and friend caregivers (50%), but also among 39% of developmental service providers, 32% of first responders and 31% of health care professionals.
Having an advance care plan in place was also noted to have a positive impact on quality of care, particularly among family and friend caregivers (39%). Knowing the medical history of the individual is a key area for positive change, particularly among personal care workers (33%) and first responders (32%). Better access to culturally appropriate information resources is also seen as making a positive difference to quality of care according to one in four care providers (24%), particularly health care professionals (33%).
Table 14: Factors Affecting Care
Col1
Family/friend caregivers
Developmental service workers
Health care professionals
Personal care workers
First responders
Q29. Based on your experience, which of the following would most [make/have made] a significant difference to your ability to provide quality dementia care or support?
n=341
n=108
n=520
n=321
n=264
Better sharing of information across care providers and/or care settings
55%
53%
63%
52%
56%
Better access to culturally-appropriate information resources
6%
30%
33%
26%
25%
More dementia care training
55%
52%
53%
56%
53%
More time to spend with the person(s) I care for
32%
36%
40%
48%
13%
Mental health supports for care providers
50%
39%
31%
28%
32%
Having an advanced care plan in place
39%
23%
26%
28%
23%
Knowing the medical history of the person living with dementia
10%
20%
27%
33%
32%
Family support/home care
5%
1%
0%
0%
1%
Access to specialized/community services/supports/resources
2%
0%
1%
0%
0%
Knowing social/cultural history, disrupted connection to family information
1%
2%
1%
2%
0%
Money, number and quality/ training of staff
1%
0%
1%
1%
1%
Other (please explain)
2%
2%
1%
1%
2%
Don't know / No response
5%
4%
2%
1%
8%
Sharing of information is more often emphasized among care providers in the Prairies (67%) compared with care providers in other parts of the country and among those with a graduate degree (60%).
Among health care professionals and developmental service workers, technicians are most likely to advocate for increased dementia care training (65%).
Increased mental health supports is an area more often listed among psychologists and social workers (43%), compared with other health care professionals and developmental service workers. This is also more often indicated among women (37%), and care providers 55 or older (39%), compared with other care providers. Regionally, mental health supports is noted more often among care providers in the Atlantic (50%) or Ontario (40%) than in other parts of the country.
Women (38%), care providers who are 35 to 54 (39%) and those in Quebec (41%) are more likely than others to see added time spent with the individual as having a positive impact on quality of care.
Among health care professionals and developmental service workers, technicians (36%) are more likely to see the value in knowing the medical history of the individuals. Among first responders, this is more often the case among paramedics (44%).
An advance care plan is more often seen as making a positive contribution to quality of care among those with a graduate degree (31%) compared with other care providers.
Having better access to culturally appropriate information is more often seen as a valuable contribution to quality of care among those under 35 (31%), and those in Quebec (31%), compared with other care providers.
Interview Findings (Factors Affecting Quality of Care)
Family and Friend Caregivers
In terms of factors affecting the ability to provide quality dementia care, family and friend caregivers spoke of access to programs that provided respite and information, such as day programs and support groups. Several said that they had to find dementia guidance on their own, and would welcome any communication of sources for dementia guidance. Access to paid care providers including doctors, psychologists, and home care was also noted as an area that friend and family caregivers would like to see improved in order to support the overall care available for the person living with dementia. Several said there is a need for new or increased government financial support for primary caregivers to support the sustainability of ongoing care within the community. One family member referred to COVID health restrictions, which prevented family visits, as hampering the ability to provide care, while two others said that programs were closed as a result of COVID, leaving them to provide care without community support. Consistency of home care providers in terms of assignment to specific clients, as well as consistency of training and approach were also noted.
"There's no time to do something you wanted to do, and if you did, you would feel so worried and so guilty. The burn out takes a big toll." (Family and friend caregivers)
"Being able to access doctors, psychologists, to come to the home was difficult." (Family and friend caregivers)
"Finances. Working full-time is the plan, but I'm currently on a one-year, unpaid leave of absence. We are in our 60's and want to get out of debt and safe for retirement." (Family and friend caregivers)
"Home care is great and gives good respite, but there is a consistency issue. Not everyone is well prepared to do this work and you could see the differences between some who were well prepared and suited and some who weren't." (Family and friend caregivers)
Some paid care providers believe that in the case of families caring for someone living with dementia at home, the caregiver should also have access to support from programs and the community. This would help them to become educated on how to provide quality care for a person living with dementia (e.g., physical care, cognitive and emotional engagement, and appropriate communications and interaction). Related to this, the caregiver is perceived to need respite support from community programs to ensure they are able to sustain their caregiver role.
"(It helps to have) assistance of community services like home care, and Alzheimer's Society to provide reassurance and support for the spouse who is providing care — provides advice to the spouse of ways to care for the person living with dementia." (Physician)
"Yes, (it) depends on level of dementia though. If in the beginning and they have supports, then yes. But, who supports the caregiver? That is all part of the equation as well. Have to have respite or burn out. Could be the (person) with dementia lasts longer than the caregiver who burns out/becomes worn out first. That is why adult day programs are so valuable to offset care and provide respite as well as support and learning for caregiver. Home care is good, but can be hard too. Patient has strangers coming in (and so does family). An issue also is when there is fragmentation between home care providers (i.e., each time a new care provider coming in and never getting to know the patient and family well enough and person with dementia always seeing a new person). Disjointed and confusing for patient. There needs to be consistency which is a problem with homecare - that consistency is not there as much as it should be (i.e., always trying to keep the same match in place)." (Nurse)
"Day programs for example are great. They get people out and engaged, stimulated (memory, motor function), doing something, connecting with others (social interaction), feeling useful and contributing to something. Organized programs in the community that are age appropriate, well trained and staffed are huge." (Nurse)
Personal Care Workers
The factor mentioned most often that affects quality of dementia care, according to personal care workers, is having adequate staffing and time to provide care. Many said that more time is needed in working with this population because of the need to not rush the interaction, explain things slowly and maintain trust, in order to gain confidence and compliance, and not cause confusion, anxiety or aggression.
"People with dementia really require a higher staffing level. You may need to re-approach them several times. You can't rush them. It's a more time-consuming care and need adequate amount of time." (Personal care worker)
"We become task-oriented instead of people-oriented because there's so much to do, but then you forget about the patients and how they are doing/capacity, kind of day they are having." (Personal care worker)
Having training that is specific to dementia care is another key pillar of providing quality care for persons living with dementia, according to personal care workers. Those who are not adequately trained in the nature of dementia and dementia care are less likely to successfully establish a relationship and gain the trust of the person living with dementia needed to provide quality care.
"Team education and understanding of dementia and how to relate to/understand and work with people with dementia. It would be great to have a consistent level of understanding across the team." (Personal care worker)
Similarly, several said that one needs the right personality to do this work, and anyone lacking patience and empathy are not likely to be well suited to provide good quality dementia care.
"The number one is personality. You have to have the patience to work with them, you have to have the desire to work with them, and you have to want to make their day the best you can." (Personal care worker)
Some personal care workers reiterated the need to have consistency in personnel who are assigned to specific persons living with dementia. Matching care providers with patients, where possible, is helpful to build rapport, get to know likes and dislikes and how best to approach specific individuals, as well to maintain a good, consistent routine. Constant turnover of care providers is, therefore, not conducive to quality dementia care.
"They try to have most of us go in to stay with the same person all the time. Patients get more confused when new caregivers go in. They don't know the routine." (Personal care worker)
"Keeping the same personnel in place helps build relationships with the patients and to better interact with them and serve their needs." (Personal care worker)
Developmental Service Workers
By and large, developmental service care workers outlined the same factors as noted by personal care workers, with particular emphasis on the need for training and dementia guidance to ensure well-informed and consistent approaches to care. A few providers also emphasized the need for information about the types of programs that are available in the community for people living with dementia and their families. One care provider articulated that a dementia diagnosis is beneficial in accessing services, and in accessing funding to provide care at a higher staff to patient ratio.
"Having a diagnosis is also a helpful support because it leads us to be able to use a different designation for some residents so that they could access a higher level of care (better ratio of staff to patient)." (Direct support manager)
"Until I accessed the Dementia Society I didn't know a lot about dementia care, but finding it, led to many other discoveries (information, resources, tools, access to expertise in community). Even the doctors didn't know what was available in terms of these programs." (Direct support manager)
A few care providers believe that a lack of coordinated approach to care can affect the quality of care provided to people living with dementia. Although they acknowledged the need for privacy, they also suggested that having access to shared information can be very helpful for care providers to better understand the patients' recent history and cognitive assessments. They pointed out that this could, for example, include sharing of information from physicians or emergency responders, and long-term care facilities, and vice versa, so that information stays with patients across transitions, to better inform staff.
"For caregivers it's hard to navigate the system. It's disjointed and fragmented. It's hard to find reliable and consistent care/support." (Occupational therapist)
"It would be better to have better and more coordinated/complete information on a case. This is a huge problem in transfers as well (e.g., go into acute care then come back out and have home care, but don't get file on what happened, why went to hospital, how it went), so it's fragmented and you are guess and trying to assess when info would be very helpful. It would be so valuable for workers but mostly for the patient, if information were shared more widely and systematically." (Occupational therapist)
Several care providers talked about the benefits of well-designed dementia care programs that use an interdisciplinary approach and also try to create a calming, home-like environment that is less institutional in look and organization. The Butterfly Program in particular was noted by two care providers.
"The Butterfly Program uses a multidisciplinary team to create better relationship with and focus on patients. Everyone is more engaged now in this program - staff who are more trained and focused on patient as priority, and patients. It's less task oriented and more patient oriented, with lots of focus on improving engagement, memory and sensory input." (Physiotherapist)
Health Care Professionals
Similar factors were raised related to the ability to provide quality dementia care, highlighting the importance of staffing ratios and time to spend with patients, as well as training and the right disposition. One physician described the Care by Design Program which creates added skill capacity among emergency responders, supported by physicians, and a re-design in how physicians are assigned to patients to increase cohesiveness across teams in long-term care facilities, and improve relationships with patients.
"The ratio of health care provider to the elderly is ridiculous. It's a conveyor belt... wash this person, wash that person. They don't have the time to sit and talk to elderly patients." (Nurse)
"Doctors and other health care providers, who have even higher caseloads, only see people with dementia for a very short time so focus on one narrow aspect. Also, having (or not having) an actual diagnosis is a barrier." (Nurse)
"I see some long-term care facilities where the built structure is just setting them up to fail. When staffing ratios are not high enough and they are not able to create enough of an environment that is positive for dementia care, and there is a density of patients with aggressive/responsive behaviour in the unit it requires more resources." (Physician)
Two health care professionals also raised the issue of a need for increased awareness and guidance regarding dementia and the need for increased understanding of the disease.
"Take the fear away. People perceive it as an immediate death sentence. I would be able to see from office visits, very early signs starting up. When I would bring it up to the spouse, the inevitable reaction was denial." (Physician)
"There is not enough awareness about the risks, patient background/history, and signs and symptoms of dementia. There is not enough understanding that it is a disease and has a progression. There is not enough understanding of dementia care. Most family/friends (and society), and even care providers don't have enough grounding in what to look for and assessment (diagnosis) to know that what they are seeing is dementia, and therefore it is not treated as such and proper care is not sought/available. Not recognizing this means that people living with dementia are not treated with the dignity they deserve. There is stigma because they (and others) believe they are doing something wrong (i.e., blamed for symptoms) when it is a disease (i.e., a labelling issue)." (Physician)
First Responders
Emergency responders noted the difficulty of gaining compliance and gathering information from those on the scene who are living with dementia. They also talked about fear and confusion experienced by those with dementia in these types of emergency situations (i.e. when strangers and in some cases full teams arrive in the home). Knowing in advance that they are responding to a call involving a person living with dementia helps. One respondent said their dispatcher will typically inform them if a call involves a person living with dementia, giving them time to consider their approach. Others talked about the challenges when they do not have this information until they arrive on the scene and conduct an assessment.
"Information going into the scene is always helpful. The more you know the better the success outcomes in finding person. (You) need clues on where have been/might go, how long gone for exactly and so on." (Police)
Having training specific to dementia, particularly in emergency situations, was described as something that would improve their ability to gain trust and establish rapport quickly. A few participants described personal experience with family or friends living with dementia or past work experience as helpful to better understand approaches that work to reduce anxiety and resistance, and increase compliance.
"I can't force or coerce or even really touch the patient in a way that is leading or forcing. So, this can be very challenging if the person with dementia doesn't understand. So, for example if they have to go to hospital but they don't want to, I have to try and reason with them." (Paramedic)
Several first responders emphasized the importance of primary caregivers understanding common dangers, including wandering, driving, cooking, and so on, to increase the development of safety strategies and having information ready for first responders in the event of an emergency. Having quick access to health records and the ability to consult with health care professionals was also seen as helpful.
A couple of respondents noted that COVID-19 regulations for masks have complicated some encounters, causing added confusion and increased difficulties in communication with those living with dementia.
Impact of COVID on Quality of Care
Survey Findings
When asked about the impact of COVID on the care or support provided to people living with dementia, communications, and in-person care were noted as among the areas most affected. Half of the health care professionals (51%) and developmental service workers (50%) said they had to change how they communicated with patients when providing care, typically communicating through virtual methods. This was also noted among 30% of family and friend caregivers. Reducing in-person care because of concerns about transmission was similarly identified by higher proportions of health care professionals (32%) and family and friend caregivers (30%). Health care professionals said that they had less time to spend with people because of increased caseload and staffing issues (36%), also noted by 29% of developmental service workers. Not being able to provide in-person care because of visitation restrictions was reported by 33% of developmental service workers, and 32% of family and friend caregivers, followed by 27% of health care professionals. Disruption of appointments was noted by 30% of developmental service workers and 26% of family and friend caregivers. First responders (47%), and to a lesser extent, personal care workers (29%) were more likely than other care providers to say there was no impact on how care or support was provided during COVID.
Table 15: Impact of COVID
Col1
Family/friend caregivers
Developmental service workers
Health care professionals
Personal care workers
First responders
Q14. How has COVID-19 impacted how you provide care or support to [people/someone] living with dementia?
n=341
n=108
n=520
n=321
n=264
Changes in how I communicate when providing care (e.g. over the phone, video calls instead of meeting in-person)
30%
50%
51%
17%
13%
Less time to spend with the person receiving care (e.g. due to increased workload, changes in staffing)
22%
29%
36%
28%
10%
Not able to provide care in person (visitation restrictions)
32%
33%
27%
12%
8%
Reducing in person care due to concern with transmission of the virus
30%
27%
32%
22%
14%
Not having appointments that would otherwise take place
26%
30%
18%
16%
5%
COVID-19 has not impacted how I provide care
14%
9%
12%
29%
47%
Fewer services/programs/ resources available
1%
2%
1%
1%
0%
PPE, loss of communications/ contact
1%
6%
4%
8%
5%
Disruption in procedures, routine, care providers, care
1%
0%
1%
2%
1%
Isolation, lack of family visits, deteriorating mental health from withdrawal
6%
6%
6%
3%
1%
Other (please explain)
2%
3%
3%
2%
0%
Not applicable
26%
4%
7%
5%
17%
Don't know / No response
0%
1%
2%
4%
3%
Among health care professionals and developmental service workers, psychologists and social workers were more likely to note changes in the way they communicated to provide care (67%). A disruption in appointments was also more often reported by these care providers (29%). Among this group, physicians were most likely to report reduced in-person care to mitigate transmission (43%).
Paramedics and health technicians were the most likely to report no impact in the way they delivered care (60% and 27%, respectively).
When asked about the most challenging part of providing care or support to people living with dementia during COVID, a lack of staff was most often noted across paid care providers. It was a particular issue among personal care workers (49%), although also cited by 45% of health care professionals and 41% of developmental service workers. Even among first responders, it was the most often noted challenge (38%). For developmental service workers (46%) and health care professionals (40%), the migration of services to more virtual methods of delivery (e.g., telehealth) during COVID represented a key challenge in providing care to people living with dementia.
A lack of information, guidance, and training on how to safely perform care duties was also reported as a significant challenge among 34% of personal care workers, as well as 32% of first responders and 31% of developmental service workers. It was somewhat less of an issue for health care professionals (26%). The nature of the group or assisted living, including crowded and shared spaces, was indicated as a key challenge during COVID according to 25% to 30% of all paid care providers.
Staff working in multiple settings was indicated by 33% of personal care workers, and 21% to 25% of other care providers as one of the most challenging aspects of providing dementia care during COVID. Infection control and availability of protective equipment was similarly noted by 27% to 30% of developmental service workers and health care professionals, as well as personal care workers. It was less of an issue for first responders (20%).
Among family and friend caregivers providing unpaid care during COVID, the restrictions on visits (54%) and loss of activities loved ones could participate in, including adult day programs (49%), were reported as the most challenging part of providing care during COVID. The cancellation or reduction of support services such as home care and the need for interactions to take place while wearing protective equipment were also key challenges reported by 39% and 24% of family and friend caregivers, respectively.
Table 16: Challenges During COVID
Col1
Developmental service workers
Health care professionals
Personal care workers
First responders
Q30.What have you found to be the most challenging part of providing care or support to people living with dementia during COVID-19?
n=108
n=520
n=321
n=264
Lack of information, guidance and training on how to safely perform care duties
31%
26%
34%
32%
Infection control and availability of protective equipment
30%
27%
27%
20%
Adaptation of services (e.g. moving to telehealth and virtual care services)
46%
40%
21%
20%
Understaffing
41%
45%
49%
38%
The nature of group and assisted living (e.g. crowding and shared rooms)
30%
27%
26%
25%
Staff working in multiple settings
25%
23%
33%
21%
Disruption/inconsistency of staff/routine
1%
0%
1%
0%
Isolation, lack of family supports/visits
2%
9%
6%
1%
Disrupted access to services
2%
2%
1%
0%
Confusion/communications with people living with dementia about pandemic & changes
0%
1%
1%
0%
Other (please explain)
9%
6%
3%
4%
Not applicable
0%
0%
1%
0%
Don't know / No response
9%
8%
9%
21%
Table 17: Challenges for Family and Friend Caregivers During COVID
Col1
Family/friend caregivers
Q31. What have you found to be the most challenging part about caring for someone living with dementia during COVID-19?
n=341
Lack of information and clear guidance on how to safely perform care duties
15%
Cancellation or reduction of support services (e.g. home care)
39%
Loss of activities that the person I provide care to can participate in (e.g. day programs)
49%
Visitation restrictions
54%
Interacting with people living with dementia while using personal protective equipment (PPE) such as masks, gowns and gloves
24%
Other (please explain)
9%
Not applicable
20%
Don't know / No response
3%
Among health care professionals and developmental service workers, psychologists and social workers were more likely to report adaptation of services to virtual delivery as a challenge (50%).
Among first responders, firefighters and those involved in dispatch, search and rescue or security are more likely than others to point to a lack of information, guidance or training (42%).
Interview Findings (Challenges)
Challenging Aspects of Providing Care
Lack of resources in the system
Both paid care providers and family and friend caregivers spoke of the challenges of a system that is under-resourced. Many described a lack of staff and therefore a lack of adequate time to engage with and provide stimulation to people living with dementia. A few said this is because geriatrics, and in particular dementia care, may not be seen as highly desirable areas to work in. Several said that some people are not well suited for providing care to this population. One paid provider said that salaries are higher in acute care and therefore long-term care facilities have trouble finding staff.
"As nurses, and even health care aids, you don't have enough time to focus on the individual or mental state." (Nurse)
"Not enough trained staff, particularly in long-term care and the community to assist so many end up in acute care, which is more expensive. They system is short of resources, especially in long-term care, so the burden falls to the family. There's a lack of capacity (beds) in long-term care and wait lists are long. There is 20% less pay for same work in community compared with hospital so that robs community of trained resources." (Nurse)
"I struggle with feeling pressured and task-oriented and I have to not show it at all, which is also hard when you have that pressure all day, every day." (Personal care worker)
"You need to be so inventive. And, it's really all about understanding their point of view, but of course that's challenging when you don't stop to think of it and everyone is so busy, you don't have time." (Direct support manager)
Another example of the pressure on resources is the lack of access to specialists and physicians, and long wait times for some resources and some programs (e.g., adult day programs, mental health support). A few care providers spoke of treatments limited to only the most urgent needs, rather than fully addressing all needs of patients, resulting in return visits (i.e., patients coming back to acute care over and over).
"Lack of access to a physician and care in general before it reaches a boiling point. But, sadly coming in through ER is often the fastest/shortest route to seeing someone/accessing care, so this is how situations end up. But this is not the best use of ER resources and it's not the best for person with dementia to get to that point." (Nurse)
"The wait lists are extremely long and our health care seems to rely on family or friend care at home." (Family and friend caregivers)
"That churn of people in and out when not yet at best capacity means that you will probably see them again since they are not as good as they could be when you released them, and you may not have been releasing them to the best set up/environment. So, that rushing to meet numbers isn't really helping since they will be back - you're just pushing it farther down the line, but not solving. That part is frustrating." (Occupational therapist)
"Things being swept under the rug because of lack of time. Not dealing with all elements of situation so person with dementia keeps coming back into care again." (Nurse)
"There is not enough service or programming and supports in the community for after the level of dementia [increases]. Once they progress to a point beyond how we can keep them busy, there needs to be more dedicated and concentrated/focused attention to keep them feeling like they are connecting and contributing and doing something, and there isn't enough of that out there." (Program counsellor & coordinator)
Both family and friend caregivers and paid care providers spoke of the lack of home care and other respite options for caregivers supporting people living with dementia in the home. Several described the intensive level of needs to be addressed, increasing with the progression of the disease, sometimes resulting in exhaustion and burn out among caregivers. A few family and friend caregivers also spoke of the factors that need to be weighed in making difficult decisions about timing of transition to long term care.
"Having at least one other person involved (other friend) would be a relief for intensity." (Family and friend caregivers)
"Being physically alone to do everything is hard physically and mentally, as well during COVID. Very isolating." (Family and friend caregivers)
"(For caregivers) it doesn't stop. You are so lucky when the person falls asleep so you can rest. If you were the sole caregiver you could get chronic fatigue." (Nurse)
"There is terrible pressure and guilt around keeping family member at home and not sending to long-term care, but if not enough support, they get better care in a facility (more interaction/social time/stimulation) and caregivers do not get worn out." (Nurse)
Lack of training and guidance/information on dementia
The other main area described in terms of challenges in providing dementia care is related to lack of training and guidance specific to dementia. This ranged from training for staff to provide routine care, as well as training or access to information for families to better understand dementia, appropriate methods of communicating, and assessment for the purposes of decision-making. First responders also spoke of the need for training to better understand dementia and to have appropriate guidance on effective communications in emergency situations. One physician spoke of the need for centralized expertise on dementia that could be accessed by physicians for assessments and referrals, including assessments of a range of practical tasks, such as driving.
"Lack of education of staff and families about dementia and what to be looking for, what to be assessing and how to assess it re: risk and safety." (Nurse)
"Initial diagnosis and what does that mean and what does it look like? Are family physicians comfortable with this, and if not, do they have resources/centralized groups where they can access support? As the pace of dementia increases and as population ages, doctors need this (more access to assistance and capacity building) rather than having to wait for geriatric specialist/referrals (e.g., driving assessments)." (Physician)
"Nurses also need more training in assessing/diagnosing and what is available in the community/services to access. Many don't know very much about home care options in particular - not given the background." (Nurse)
"Family can be hard. They don't understand and can't accept the decline of the person with dementia and their capacity, (its hard) to comprehend. You can't push or will them to be where you want them to be, you move with them in their decline. When family can't see or understand that they push and cause greater confusion, stress and anxiety for patient." (Physiotherapist)
"Trying to get the compliance or information you need as fast as possible. Try to go in smaller teams to reduce confusion, but there are big teams in one place (fire, EMT, etc.), so keeping PWD calm and less confused is critical. Big and loud surprise makes for worst in confusion and lack of compliance." (Firefighter)
"I like the idea of a training program especially with an aging population. We are going to be experiencing a lot more of it. We get a lot of training with homeless, drug addicts and aggressive people, but none on dementia." (firefighter)
"More information is needed on the resources needed to support those supporting people with dementia. Doctors and nurses need to have access to information about dementia that they can hand out to families and others." (Program counsellor & coordinator)
Lack of coordinated approach
The third area of challenges is related to the lack of coordination in the approach to providing overall care for people living with dementia. For example, one provider emphasized the need for an interdisciplinary, holistic, approach to address the complex needs of people living with dementia, particularly those with co-morbidities. Another spoke of the lack of shared information between different types of organizations and care providers, considered beneficial in assessing and making decisions about care, or in supporting a person in emergency situations.
"Homecare also needs better access to an inter-disciplinary team of professionals to assist in assessment and care planning, as they do in long-term care." (Nurse)
"There is a lack of access to interdisciplinary teams for advice and support (e.g., diet, memory stimulation) – finding solutions that work for specific problems (e.g., ensure and shakes in cup to give if won't eat). There isn't enough coverage of expertise drawn on for these kinds of supports/solutions in community." (Nurse)
"Facility transfer notes can be slim and the patient may not be able to tell you very much. Often there are no family members around to provide information, so you have to guess." (Paramedic)
"Having as much information as possible is key. Not having it is a challenge. Most of the time don't have enough information going onto a call like that. A lack of information is a problem in emergency situation - need it fast, and not having compromises safety/successful outcome, but don't have access to information often. If more access to thing like health records, would help." (Police/Search and rescue)
Challenges of caring for people living with dementia
The last main theme is related to the nature of dementia, as well as its impact on cognition. One provider talked about the difficulty in providing care for a population with a degenerative disease, where there is no improvement, only decline. Others, particularly those providing daily care, talked about the intensity and difficulty in caring for individuals with compromised ability to comprehend and articulate their needs (e.g., how they are feeling). The lack of comprehension and for some, the resulting frustration, can also lead to violent behaviours from those living with dementia that can be challenging for care providers to deal with. For some care providers, particularly first responders who are trying to obtain information and compliance in emergency situations, the lack of comprehension and potential for violent behaviour can be particularly challenging. For families, there is the added concern of trying to establish the individual's medical wishes, as making advance care directives is important to set up early, before the disease progression makes it impossible for the individual to clearly articulate their wishes.
"Knowing that there will be no improvement and that they will continue to degenerate. Fear of the unknown for person and for family is hard to see." (Personal care worker)
"It's a chronic disease process, so it's hard to care for/meet patient's needs. It's not like acute care where there is a solution. There is no cure and it's always progressing. It's very discouraging." (Physician)
"Feeling like I've lost my mom. Hoping that you've provided appropriate care - she's going to get the care she needs. Some days she knows who I am and sometimes not." (Family and friend caregivers)
"Understanding the needs of patients when they cannot express it/communicate it to you. You are trying to decipher their actions/responsive behaviours to meet their needs. You are interpreting, it's a guessing game." (Physiotherapist)
"It's also hard to deal with violent outbursts which can happen, and not take it personally and not let it show or interfere with your relationship with them or their care." (Personal care worker)
"The (reduced) capacity of a person to understand and rely on information, so it's often all guesswork to decipher what is going on, especially in home/community situations." (Paramedic)
"It really helped that I knew when she expressed her wishes well before that she did not want to have us children caring for her when she got to a point where she couldn't get out of bed." (Family and friend caregivers)
"You are trying to help them but they don't realize they need the help/that they are sick. Checking blood pressure, finger prick, or IV, is so hard when they don't understand what you are doing to them and why. They get mad and they fight you and you feel terrible and it goes badly sometimes." (Paramedic)
"Not all paid care givers are capable of providing good care. Just not the type of person who should be working with dementia clients." (Personal care)
Challenges in Delivering Care During COVID
Most interview participants described a wide variety of impacts and challenges experienced during COVID. Many of these stemmed from increased restrictions and, consequently withdrawal of support and assistance for people living with dementia, beginning with the reduction or complete absence of family visits. This was described by some as devastating for many patients, resulting in a lack of stimulation, greater isolation, and reduced care.
"The separation from family was terrible. Patients lost their only connection to the world, their engagement and stimulation, and the presence of people who care about them. It contributed significantly to the decline of many." (Physician)
"Not having family there is really hard for residents. They declined and there were mental health issues." (Personal care)
"I am limited to when and how often I can see her. With her living in a centre, I was hoping she would have more interaction, but with COVID they can't." (Family and friend caregivers)
"They want to go out and to see family. They are constantly asking ‘When can I go outside?' ‘When is my family coming?'" (Personal care worker)
Many participants also described shutdowns in support programs that provided stimulation for those with dementia, and withdrawal of respite for caregivers. Additional restrictions resulted in a vastly reduced range of options for activities, making it difficult to achieve needed stimulation, enjoyment and daily structure.
"It's terrible right now with not having day programs to go to." (Family and friend caregivers)
"Mainly because a lot of the community resources weren't available. You can't take people out for walks in the winter in the mall." (Nurse)
"All outings are gone and that is so unfortunate since it is an activity, and stimulates them and adds structure and they enjoy it. So, now we can't go anywhere and they don't understand why not. You have to explain over and over why not and it confuses them." (Direct case manager)
"They are not getting out as much so reduces mobility and physical strength." (Physiotherapist)
Some care providers described increased mental health issues such as disengagement and depression, as well as increased frustration and aggression.
"Having no visitors is raising the aggression of the patents." (Psychiatric aide)
"There were more cases of depression from isolation." (Nurse)
A second source of challenges introduced by the pandemic relates to the inability of people living with dementia to comprehend the situation. Personal protective equipment (PPE) was often described as a significant barrier to communication as it masks facial cues used to assist with communications and comprehension. First responders also spoke of PPE impeding their ability to connect with and calm people living with dementia, adding to already heightened fear and confusion in emergency circumstances. The use of online communications for consultations was also described as more difficult and compromising to care.
"When I go in I have to be fully garbed with PPE and the only thing she can see is my eyes and that's hard for her to even understand if I'm her daughter or just another worker." (Family and friend caregivers)
"COVID meant fewer visits and more virtual visits which is not ideal, as some people with dementia didn't communicate well this way (e.g., hearing well on the phone)." (Physician)
"PPE is a problem (gas masks and face shields and gowns and what not). It's very scary for them. Causes more confusion. And, they can't understand you through the PPE as well." (Paramedic)
"All the PPE, hospital gown and N95 mask, shield and blue gloves; you look like something from the apocalypse." (Firefighter)
Some paid care providers talked about the difficulty in trying to explain, and re-explain, the pandemic, and the need for restrictions to people living with dementia. Similarly, the need to explain, and ensure that health protocols are met, including the wearing of masks, social distancing, and sanitizing, was described as very challenging.
"Try to tell that to someone with dementia. [Name of health unit] didn't seem to envision this problem; the risk of COVID is life threatening, but to lock someone with dementia in their room is traumatizing to them." (Nurse)
"They don't understand the pandemic and when they do, they may forget. It's unfathomable to them, so they feel forgotten and they decline from lack of social contact." (Personal care worker)
"They don't understand why you are wearing a mask and look at you funny. They don't understand the whole COVID problem." (Personal care worker)
"Getting them to wear masks every day and wear them properly (over nose and mouth). They don't remember to do it and they don't understand sometimes why and they get frustrated and sometimes angry that I am always harping on them to do this." (Personal care worker)
The third set of challenges described relates to pressures on the health care system. This included significant understaffing, because of resources needed to respond to the pandemic, as well as due to illness and/or general fear of COVID. In long-term care, as well as in acute care settings, understaffing, and related burnout were described as significant and compromising to quality of care, leaving no time for connecting with dementia residents or patients. The added absence of family and volunteers to assist with care also contributed to the pressure.
"Staff shortages were also a significant factor in the decline of quality of care. Also, fewer family there meant more work and staff had no time to be contributing to engagement." (Physician)
"Resources are stretched even thinner. It's all been exposed that system was under resourced before, but now with COVID, testing, vaccinations, etc, it's drawing even more resources away and nurses are leaving in droves as well, so system is very strained. There's a huge shortage of staff everywhere." (Nurse)
"Not having the volunteers and families to assist and help the people with dementia stay engaged and connected socially (stimulated), so it's all up to nurses. PPE gets in the way/barrier to communication and comprehension and connection with them. Not being able to understand about COVID and why no one is coming or they can't leave." (Physiotherapist)
"The team is more stressed. We are understaffed like everyone especially on the daily care side so everyone has to pitch in more. In the spring it was so bad I couldn't get to the daily physio exercises because basic care was missing and everyone had to focus attention there, so physio suffered, there was no choice." (Physiotherapist)
In the homecare setting, a few mentioned that care providers are not often matched with the same clients on a regular basis, disrupting established relationships and routine, and quality of care. Some families were fearful of a greater risk of COVID with visiting home care workers (particularly with changing care providers), and therefore discontinued service, leaving them to try to meet all care needs on their own.
"At home there is a lot of fear of home care workers coming in and out and possible COVID infection risk/exposure. There is also disjointed care (different person each time) so each time worry about level of risk." (Occupational therapist)
Suggested Improvements from COVID Experience
Survey Findings
Survey respondents offered suggestions that would improve their ability to provide quality dementia care or support during COVID-19. The most prevalent theme focuses on adding resources into the system. Care providers primarily suggested the need for more (front line) staff, so that care providers would have more time to spend with those in their care. Many said there simply was not enough time, particularly during COVID, to give people living with dementia the attention they need. Many said that understaffing during COVID, the absence of family assistance because of restrictions, and the added time needed because of safety protocols takes away from time to provide care. Some spoke of the need for increased pay to attract and retain staff, and to reduce work in multiple locations. In home care environments, added staff would increase the continuity of home care providers, possibly reducing the risk and fear among families of COVID coming into the home.
"Plus de ressources de localisation. Meilleur contrôle de l'environnement des personnes atteintes de démence pour réduire les risques, plus de temps de la part des ressources pour garder les personnes atteintes de démence active et faire de la surveillance." ("More localization resources. Better control of the environment of people with dementia to reduce risk, more time on the part of resources to keep people with dementia active and monitor.")
"We don't have enough time in the day to give residents the time they need and deserve. We need a proper patient/staff ratio."
"More staff and living with more space to adequately provide separations between residents."
"Plus de PAB sur les unités avec démence plus de temps a leur consacrer, formation sur la démence et réaction au comportement agressif et hostile." ("More PAB on units with dementia more time for them, training on dementia and responding to aggressive and hostile behavior.")
"There needs to be more staff that are paid better. Staff are run down especially now."
"Have more RN nurses vs. health care aids in the facilities."
"Ensure staff are paid a living wage so they don't need to work at several different locations."
Others noted the reduced access to referrals, experts, and programs (e.g., health care, day programs, respite care), and the need to keep these open to ensure continued access to these much-needed services. Family and friend caregivers spoke of cancelled and reduced access to health care appointments and day/respite programs.
"The people we support are declining while not being able to see appropriate doctors and have proper assessments."
"Services for those with dementia or mental disabilities should not be closed. These people and the family care giver still live everyday and these services are essential for the well-being of the person and family."
"Increased DSP visiting, even during lockdown. Compulsory use of technology to have frequent virtual visits. Virtual Grand Rounds' throughout the facility when in-person supervisory visits are not possible."
"Provide more in home emergency care as often patients are dropped at hospitals as caregivers are burnt-out or unable to care."
"More informal resources, day services for adults with dementia and families."
Other care providers talked about cancelled appointments and the withdrawal of programs and activities as factors that decreased access to care and stimulation among those with dementia. They suggested that with better planning, this might not have been necessary.
"The care centre should have made a better plan on how to continue with physical and recreational therapy programs while keeping residents distant and safe."
"Avoir plus de temps avoir des équipements adaptés et aller au rythme des gens y veux passer la journée en pyjama ben qu'on le laisse faire." ("Have more time, have adapted equipment and go at the pace of people want to spend the day in pajamas, but let it be .")
"Having more help to organize activities to keep the patients active mentally and physically."
"Care homes should be required to provide outdoor spaces that are interesting, attractive and safe for residents."
The second main theme is related to equipment and protection for infection control and health safety guidance. Many said that there should have been more and better access to personal protective equipment, more rapid testing and turnaround of results for care providers, patients and residents, as well as quicker access to vaccines.
"There should have been rapid testing of all staff daily to keep the virus out. I believe thousands of Canadian elders died needlessly because care staff brought the virus into facilities when they came to work."
"Having proper PPE, having enough face shields/masks, availability of rapid COVID testing to swab people more quickly, more stringent infection prevention measures in LTC settings to avoid outbreaks when transferred to and from hospital and back."
Many care providers suggested improved access to clear, and consistent information about safety protocols and management of the crisis. This also includes better and more informed understanding among public health experts about the nature of dementia, the ability of those living with the disease to comprehend and comply with safety measures, and the significant impact that social isolation due to restrictions was having on cognitive abilities and mental health. The impact of restrictions meant that communications were hampered (through PPE), people living with dementia were more confused and frightened, and escorts were no longer allowed to accompany dementia patients to appointments. Training for all staff and caregivers with regard to infection control and safety protocols, along with workarounds for those with dementia were also suggested.
"More training on how to provide quality care to people with dementia with safety protocols in place related to infection control and COVID-19."
"The ministry and my agency has seemingly gone overboard with COVID care guidelines. We have stricter policy than the local hospitals. This is useless and causes strain on the care workers."
"At the beginning when no one really knew exactly what they were supposed to do in relation to COVID-19 it was difficult, there were lots of disagreements and misunderstandings. More practical training along with reminders and maybe a quick phone or text line for health care workers to ask questions to clarify what safety measures are to be taken in health care facilities in given jurisdictions."
"Consistency in public health and infection control guidelines. Forethought about the huge impact of social isolation on patients with dementia."
"Better communication and clearer guidelines for workers and patients and their families more communication."
"Public health officials aware of dementia care issues."
"Alternative PPE options for non-compliant dementia clients."
A third, related set of suggestions focuses on not restricting family access so severely, and generally better planning to ensure that caregivers may still visit and assist with engagement and care for their loved ones. Isolation was described as the most damaging aspect of COVID for people living with dementia, and the restrictions placed on family visits was the most significant contributor, followed by restrictions to activities and socializing within care facilities. The creation of safe spaces to congregate, socialize and engage in activities, in a way that followed safety protocols was suggested by a number of care providers. Some suggested, for example, the need for more dedicated staff to assist with coordination of activities, general engagement and coordination of socializing, and access to the outdoors. Others suggested that more technological equipment and staff to assist people living with dementia in virtual visits with family, although not ideal, could have helped to increase some social connection.
"Better planning to allow family visits."
"Locking someone with dementia in a room isolated for two weeks is not good for anyone."
"Accepter que plus d'un membre de la famille puisse visiter régulièrement son proche et permettre de porter seulement une visière car le masque est une embûche à la communication."("Accept that more than one family member can visit their loved one regularly and allow only a visor to be worn because the mask is a communication obstacle .")
"Frequently testing care givers. Allow care if patients are COVID free. Allow care with social distancing."
"Early access to COVID-19 testing to enable family or care givers to have nursing home visits."
Interview Findings (Suggested Improvements from COVID Experience)
Interview participants were asked to describe what makes providing care to people living with dementia rewarding. For family and friend caregivers , the reward often centers around keeping the person at home for as long as possible, and generally being able to respond to their needs as well as they could, for as long as they could. Some adult children spoke of reciprocating the care provided to them as they were growing up. Several spoke of honouring and respecting their loved ones.
"You are making the commitment to take care of the person who took care of you. You are doing the right thing. Treating them as they deserve and with respect." (Family and friend caregivers)
"I was happy to have her with me and to care for her as she did for me when I was young. I was able to provide for her. And, I got to know her even better in that time we had, so I was honoured to do it. It was a hard time but a cherished time all the same. I was able to give her happiness, care, dignity and respect and I will always be able to draw on that." (Family and friend caregivers)
Among paid care providers, many talked about being able to provide solutions and remediation that reduces the progression of the disease in terms of decline in physical or cognitive function. The end goal was described as maintaining independence for as long as possible or holding off the need for transition to long term care for as long as possible.
"If you feel you are conquering challenges and solving problems that feels good." (Nurse)
"Knowing I can help them a little bit, to be able to do something meaningful for themselves (able to take a meaningful action that feels like independence). I am helping them do things for themselves." (Physiotherapist)
"Helping them to achieve their own goals and increase / max out capacity is great. If they can maintain some independence and I've helped them with that, I'm rewarded. They get to have some pride." (Occupational therapist)
"I am helping them with mobility and to keep at bay all manner of complications (e.g., bed sores) for as long as possible, which is preventing life-altering erosion in them. They don't know that, but I do, and I am rewarded." (Physiotherapist)
Some first responders described a similar goal of successfully averting danger or decline, including finding those who are missing, and providing on-site medical crisis intervention that avoided a transition to acute care.
"They are sick and confused and scared, and if you can make them a bit better, or have an interaction that is not all about confusion and fear and anger, where you can talk to them and get them to a place where they are happy (e.g. you have treated them and left their home or left them at the hospital) and they are smiling and waving to you, and you know they feel ok, it makes everything better." (Paramedic)
"Hopefully we are getting them found and back to families safe and sound." (Search and rescue)
Many paid care providers focused on the well-being of the person with dementia and giving them moments of joy for as long as possible. Providing happy moments, even if not remembered for long, was often described as the primary goal and being able to provide this was described as very rewarding for care providers.
"The satisfaction of being able to bring happiness to someone. There are plenty of opportunities to give joy to someone." (Nurse)
"My favourite thing used to be taking second stage dementia patients to bingo. When they won a little coupon for ice cream it's like they won the lottery." (Psychiatric aide)
"They like music and might get up and dance or tap their feet, clap their hands. They might try singing, even if they don't talk anymore. Those are special moments." (Personal care worker)
"It is so rewarding to make them happy and content. Maybe you are or aren't making a long-term difference, but you are making them happy in the now, and you are findings solutions that work (e.g., gentle communications, foods they will eat, task they can do to stay independent and contributing) and that makes it all very rewarding." (Case management worker)
"I see what they feel like when contributing to something, seeing progress, there is real joy. They see they can do something and feel worthwhile and have pride." (Physiotherapist)
Similarly, some health care professionals and first responders spoke of the reward in helping a person with dementia to remain calm and feel at ease in a crisis.
"Connecting with them and keeping them calm. Making it go well. Anything that is uneventful is a good interaction. As long as it doesn't go bad its good." (Firefighter)
"To be a familiar face in dementia and level of trust they have with me is good for them. Dementia is palliative so I want to make the progression and end of life care as easy as possible for them and for family. I try to give them the tools and resource that are helpful to them to be able to be ready and make the transition. And to be a support to them right to the end if I can." (Physician)
Many spoke of the fun they have when working with people living with dementia. They talked about the laughter and enjoyment they experience at work, hearing the jokes and stories their patients tell.
"It's not all gloom and doom. Even if someone [has dementia], there may be something on TV, or a song comes on, you'll see them laugh. You might not know what it is about but they are remembering something pleasant. There is joy everywhere even if someone is leaving us cognitively." (Care management worker)
"Some are so funny, have a sense of humour. Their long-term memory can be quite good and they can tell stories from their childhood." (Recreation therapist)
"We laugh a lot. It's also fun to work with people with dementia. They like to laugh and tell jokes and stories." (Physician)
"I like to talk to them and let them start to talk, ask questions and they will tell you their stories. They love to talk!" (Paramedic)
Support for the families of people living with dementia was also described by many as a source of reward. This includes knowing that they have given families some much needed time to relax and re-charge, or some helpful advice or solutions to make their lives a little bit easier.
"Getting to know and support/share with families and what they are going through and share ideas/solutions and give advice from what you see (from outside looking in). Families are often feeling overwhelmed and worn out." (Personal care worker)
"With respite, for the caregiver to be able to go out and know that their family member is cared for while they are away. That was so rewarding to know that you made a difference in their lives that day." (Personal care worker)
"You also know that you are giving respite to families that need to have time away to do other things or just have a break and that's nice too." (Program counsellor & coordinator)
"The families. They are always extremely grateful. We take care of their loved ones the best we can and show them respect." (Paramedic)
3. Appendices
A. Methodological Details
The survey was developed cooperatively between the Ekos Research team and the Project Authority. The average time it took respondents to complete the survey was 17 minutes online and 28 minutes by telephone. The survey was pre-tested with 28 respondents (24 in English, 5 in French), including 19 collected online and 9 by telephone. These cases were retained in the final sample. The survey was administered in English and French, as well as with an accessible link for those using a mobile phone or screen reading technology.
The survey included a sample of 1,593 individuals providing paid or unpaid care or support to individuals living with dementia. This included 1,252 paid care providers and 341 family and friend caregivers. The survey sample was drawn from multiple sources, including from Probit panel, which is assembled using a random digit dial (RDD) process for sampling from a blended land-line cell-phone frame, which provides full coverage of Canadians with telephone access. The distribution of the recruitment process is meant to mirror the actual population in Canada (as defined by Statistics Canada). As such, our more than 120,000-member panel can be considered representative of the general public in Canada (meaning that the incidence of a given target population within our panel very closely resembles the public at large) and margins of error can be applied. We also relied on RDD of land and cell phones associated with geographic areas that include First Nation reserves. Also, respondents who had previously completed a baseline dementia survey of the general public in the spring of 2020, and indicated themselves to be either a paid or unpaid care provider to those living with dementia, were also re-contacted to participate in the current survey on dementia guidance in order to augment the cases in these two target groups. A small number of records were also completed (53) as a result of a referral from another respondent within the sample. When these sources were found to be insufficient to complete the intended 1,500 cases, additional sample was drawn from LegerWeb. Roughly 400 paid care providers were included in the final sample.
Initially there was an intent to complete roughly 300 cases within each of the five target groups of care providers or family and friend caregivers. Because the low incidence of first responders, the final sample was only 264. A total of 628 care providers indicated that they provided care as either a health care professional or developmental service worker. Developmental service workers were grouped with the health care professional category due to the limited number of respondents.
The survey was conducted online and by telephone from February 27 to March 30, 2021, in both official languages. Survey data collection adhered to the Government of Canada standard for public opinion research as well as all applicable industry standards. Ekos informed respondents of their rights under the Privacy Act and the Access to Information Act and ensured that those rights were protected throughout the research process. This included: informing respondents of the purpose of the research; identifying both the sponsoring department and the research supplier; informing respondents that their participation in the study is voluntary, and that the information provided would be administered according to the requirements of the Privacy Act.
Once the survey data was collected, the database was reviewed for data quality, and coding of verbatim responses was also completed. Data tables were created to isolate results for each of the five types of care providers, as well as among sub-groups of health care professionals and developmental service workers and first responders. Other subgroups used in the analysis included gender, age, education and region. Chi-square tests were used to compare subgroups to the remaining sample.
Response Rates and Non-Response Bias
Using the Government of Canada public opinion research standards for online and telephone research, the overall rate of participation was 30% (31% online and 18% by telephone),. Online, a total of 34,323 invitations were sent by email, of which 156 were returned as undeliverable, for a resulting valid sample of 34,167. A total of 1,414 interviews were completed, and 9,234 were found to be ineligible or within a quota that had been filled, resulting in a response rate of 31.2%.
In the telephone sample, a total of 4,070 telephone numbers were attempted. Of these, 635 telephone numbers were invalid, resulting in a remaining valid sample of 3,435. Of these, 426 were found to be out of scope (not providing dementia care or support) while 179 cases were completed (i.e., 29% of those agreeing to participate were eligible), for a resulting response rate of 17.8% (i.e., those agreeing to participate out of valid sample).
There are no known population figures from which to derive a useful comparison, and no comparison was made to the broader Canadian population. Nor was any weighting was applied to the data for the purposes of the analysis.
In-depth Interviews with Care Providers and Family and Friend Caregivers
Using the Probit panel to recruit paid care providers and family and friend caregivers, a total of 51 interviews were conducted, each lasting roughly 60 minutes. On average, 10 participants were interviewed in each care provider/caregiver category. Three physicians were interviewed (1 in the Atlantic, 1 in Ontario and 1 in the Prairies) among the 10 health care professionals. In the case of developmental service workers, 11 were interviewed.
Across the 51 participants, 15 were located in Ontario, eight were in the Atlantic, eight were in Quebec, seven in the Prairies, including Alberta, and six were in BC. Following is a breakdown of the 51 interviews.
Table 19 – Focus Groups
Care Providers
Atlantic
Quebec
Ontario
Prairies
Alberta
BC
Total
Family/friend caregivers
2
2
2
1
1
2
10
Health care professionals
2
1
2
2
2
1
10
Personal care workers
1
2
3
2
1
1
10
Developmental service workers
1
2
4
1
2
1
11
First responders
2
1
4
1
1
1
10
Total
8
8
15
7
7
6
51
Participants were asked to describe their experiences with and the nature of support or care they provide to those living with dementia, factors affecting care as well as challenges and rewards, impact on care during COVID, their views on the ability of people living with dementia to live independently, stigma encountered in dementia care, culturally appropriate tools, and any training and dementia guidance they have received that has helped them to provide dementia care. Paid care providers were provided with a $175 incentive for their time, although the three physicians interviewed were provided with $350. Family and friend caregivers were given $100. The interview guide can be found in Appendix C.
Interviews were recorded for notetaking purposes and used to describe overall themes of responses and anonymized, illustrative quotes. Results are reported based on content analysis conducted from a review of the notes. No formalized coding of responses took place. It should be noted that the results of the interviews are meant to be qualitative in nature. As per section 10.2.3 of Public Services and Procurement Canada's Qualitative Research Standards, "Qualitative research is designed to reveal a rich range of opinions and interpretations rather than to measure what percentage of the target population holds a given opinion. These results cannot be used to estimate the numeric proportion or number of individuals in the population who hold a particular opinion because they are not statistically projectable"[7]. Responses from the interviews nonetheless provide considerable added detail, and illustrate care providers' individual backgrounds, experiences and perspectives in providing care to people living with dementia. In order to avoid portraying these results as generalizable to the population, terms such as "a few," "some" and "most" are used to broadly indicate views, rather than using specific percentages. It should also be understood that the information provided by participants is subjective in nature, based on their own recollection, and perceptions of interactions with people living with dementia.
B. Survey Questionnaire
Online Introduction
Thank you for agreeing to complete this survey. The Government of Canada has hired Ekos Research to conduct a public opinion survey on behalf of the Public Health Agency of Canada. Si vous préférez répondre au sondage en français, veuillez cliquer sur « Français ». The purpose of the survey is to gather information on the experiences and perspectives of paid and unpaid care providers to people living with dementia. Findings will contribute to supporting a skilled workforce, informing dementia awareness, and improving tools that support the ability to provide evidence-informed care, as part of Canada's national dementia strategy.
The survey takes 15 minutes to complete. Your participation is voluntary and your responses will be kept entirely confidential. It is being administered according to the requirements of the Privacy Act. Results will not be reported on an individual basis, but rolled into groups of 20 or more to preserve confidentiality. To view our privacy policy, click the Privacy Policy link below.
The survey is registered with the Research Verification Service of the Canadian Insights Research Council (CIRC).
A few reminders before beginning...
If you leave the survey before completing it, you can return to the survey URL later, and you will be returned to the page where you left off. Your answers up to that point in the survey will be saved.
If you have any questions about how to complete the survey, please call Ekos at 1-866-211-8881 or email us at online@ekos.com. Thank you in advance for your participation.
Phone Introduction
Hello, my name is [name of interviewer] and I'm calling from Ekos Research Associates. May I speak with [name of respondent]?
The Government of Canada has hired Ekos Research to conduct a public opinion survey on behalf of the Public Health Agency of Canada. The purpose of the survey is to gather information on the experiences and perspectives of paid and unpaid care providers to people living with dementia. Findings will contribute to supporting a skilled workforce, informing dementia awareness, and improving tools that support the ability to provide evidence-informed care, as part of Canada's national dementia strategy.
The survey will take 15 minutes to complete. Your participation is voluntary and completely confidential. Your answers will remain anonymous. Any information you provide will be administered in accordance with the Privacy Act, the Access to Information Act, and other applicable privacy laws. Results will not be reported on an individual basis, but rolled into groups of 20 or more to preserve confidentiality. The survey is registered with the Research Verification Service of the Canadian Insights Research Council (CIRC).
Pivacy
This call may be recorded for quality control or training purposes.
Q1
Do you provide care or support to people living with dementia, through your paid work or as an unpaid caregiver to family or friends (currently or within the last 5 years)?
Yes: 1
No: 2
Q2
How frequently do you provide care or support to a person living with dementia?
Never: 1
Daily: 2
At least once a week: 3
At least once a month: 4
Less than once a month: 5
Don't know / No response: 99
Q3
Which of the following best describes your role as a care provider?
Family / friend caregivers of someone living with dementia (defined as someone who has provided care and support to someone with dementia in the past five years, who is not a paid care professional or personal support worker): 1
Developmental service workers (defined as someone who provides support to individuals who have intellectual or developmental disabilities. Support can be provided in homes, at work, in schools and to families): 2
Health professionals: 3
Personal care workers (Also referred to as health care aides, home support workers, personal support workers, and attendants): 4
First responders (i.e. police officers, paramedics, fire fighters, etc.): 5
Other (please specify): 77
Q5
Health professionals
Which of the following best describes your role?
[Phone version]Interviewer: Read list
Physician: 1
Nurse practitioner: 2
Nurse: 3
Pharmacist: 4
Occupational therapist: 5
Psychologist: 6
Social worker: 7
Other (please specify): 77
Don't know / No response: 99
Q6
First responders
Which of the following best describes your role as a first responder?
[Phone version]Interviewer: Read list
Police officer: 1
Paramedic: 2
Fire fighter: 3
Other (please specify): 77
Don't know / No response: 99
Q7 [1,11]
Paid only
What kind of care or support do you provide for people living with dementia?
Select all that apply
[Phone version]Interviewer: Do not read list, prompt as needed
Completing a comprehensive health history and assessing patients: 1
Assisting with activities of daily living (movement, bathing, dressing/undressing, meal prep, assistance with eating): 10
Other (please specify): 77
Don't know / No response: 99
Q8 [1,6]
Unpaid only
What kind of care or support [Q4 = 3]did[Else]do you provide for someone living with dementia?
Select all that apply
[Phone version]Interviewer: Do not read list, prompt as needed
General health care and health monitoring such as overseeing medication usage or help administering medication or setting up appointments: 1
Assisted with activities of daily living such as cooking, cleaning, bathing, or dressing: 2
House maintenance or outdoor work: 3
Transportation: 4
Assisted with financial affairs: 5
Other (please specify): 77
Don't know / No response: 99
Q9
[Q3 = 1]There are a variety of situations in which someone may [Q4 = 3]have provided[Else]be providing care to someone living with dementia. If any of the questions in the survey seem like they do not apply to you, please feel free to select not applicable or don't know/no response.>
How comfortable do you feel with your ability to provide quality care or support to [Q3 = 1]someone[Else]people living with dementia?
[Phone version]Interviewer: Read scale
Very comfortable: 1
Somewhat comfortable: 2
Neutral: 3
Somewhat uncomfortable: 4
Very uncomfortable: 5
Don't know / No response: 99
Q10
Paid only
In your role, how comfortable do you feel providing quality care to / supporting people living with dementia who have additional health concerns (comorbidities) (e.g. treating multiple conditions, monitoring drug interactions, working with an interdisciplinary team, coordinating care)?
[Phone version]Interviewer: Read scale
Very comfortable: 1
Somewhat comfortable: 2
Neutral: 3
Somewhat uncomfortable: 4
Very uncomfortable: 5
Don't know / No response: 99
Q11
Paid only
In your role, how frequently do you involve the family / friend caregivers of people living with dementia in care planning for the person living with dementia (i.e. contributing to decisions about care)?
[Phone version]Interviewer: Read scale
Never: 1
Rarely: 2
Sometimes: 3
Often: 4
Always: 5
Not applicable: 98
Don't know / No response: 99
Q12 [1,3]
Paid only, involve caregivers
Under what circumstances or in which situations do you involve caregivers of people living with dementia in care planning?
Please specify: 77
Don't know / No response: 99
Q13 [1,3]
Paid only, never involve caregivers
Why is that?
Please specify: 77
Don't know / No response: 99
Q14 [1,7]
How has COVID-19 impacted how you provide care or support to [Q3 = 1]someone[Else]people living with dementia?
Select all that apply
[Phone version]Interviewer: Do not read list, prompt as needed
Changes in how I communicate when providing care (e.g. over the phone, video calls instead of meeting in-person): 1
Less time to spend with the person receiving care (e.g. due to increased workload, changes in staffing): 2
Not able to provide care in person (visitation restrictions): 3
Reducing in person care due to concern with transmission of the virus: 4
Not having appointments that would otherwise take place: 5
COVID-19 has not impacted how I provide care: 6
Other (please explain): 77
Not applicable: 98
Don't know / No response: 99
PREQ15
How would you rate your knowledge in each of the following areas? PQ15: [Phone version]Interviewer: On a scale from 1-5 with 1 being the least knowledgeable and 5 being the most knowledgeable?
Q15A
Dementia prevention / reducing risk
Least knowledgeable 1: 1
2: 2
3: 3
4: 4
Most knowledgeable 5: 5
Don't know/ No response: 99
Q15B
Screening for dementia / Making a dementia diagnosis
Least knowledgeable 1: 1
2: 2
3: 3
4: 4
Most knowledgeable 5: 5
Don't know/ No response: 99
Q15C
Stigma related to dementia and how to reduce it [Rollover text: (Stigma is defined as negative attitudes or discrimination against someone based on a distinguishing characteristic such as a mental illness, health condition, or disability.)]
Least knowledgeable 1: 1
2: 2
3: 3
4: 4
Most knowledgeable 5: 5
Don't know/ No response: 99
Q15D
Treatment and care of someone living with dementia
Least knowledgeable 1: 1
2: 2
3: 3
4: 4
Most knowledgeable 5: 5
Don't know/ No response: 99
Q15E
Advance care planning and end-of-life care for those living with dementia
Least knowledgeable 1: 1
2: 2
3: 3
4: 4
Most knowledgeable 5: 5
Don't know/ No response: 99
PREQ16
Paid only
To what extent do you feel you could use more preparation/training in each of these same areas? [Phone version]Interviewer: On a scale from 1-5 with 1 indicating needing the least preparation/training and 5 indicating needing the most preparation/training?
Q16A
Paid only
Dementia prevention / reducing risk
Need the least preparation/ training 1: 1
2: 2
3: 3
4: 4
Need the most preparation/ training 5: 5
Not applicable: 98
Don't know/ No response: 99
Q16B
Paid only
Screening for dementia / Making a dementia diagnosis
Need the least preparation/ training 1: 1
2: 2
3: 3
4: 4
Need the most preparation/ training 5: 5
Not applicable: 98
Don't know/ No response: 99
Q16C
Paid only
Treatment and care of someone living with dementia
Need the least preparation/ training 1: 1
2: 2
3: 3
4: 4
Need the most preparation/ training 5: 5
Not applicable: 98
Don't know/ No response: 99
Q16D
Paid only
Advance care planning and end-of-life care for those living with dementia
Need the least preparation/ training 1: 1
2: 2
3: 3
4: 4
Need the most preparation/ training 5: 5
Not applicable: 98
Don't know/ No response: 99
Q16E
Paid only
How to make interactions with care providers feel safer and more supportive
Need the least preparation/ training 1: 1
2: 2
3: 3
4: 4
Need the most preparation/ training 5: 5
Not applicable: 98
Don't know/ No response: 99
Q16F [0,1]
Paid only
Other (please specify)
Need the least preparation/ training 1: 1
2: 2
3: 3
4: 4
Need the most preparation/ training 5: 5
Not applicable: 98
Don't know/ No response: 99
PREQ17
Unpaid only
To what extent do you feel you [Q4 = 3]could have used[Else]could use more preparation/training in each of these areas? [Phone version]Interviewer: On a scale from 1-5 with 1 indicating needing the least preparation/training and 5 indicating needing the most preparation/training?
Q17A
Unpaid only
Dementia signs and symptoms
Need the least preparation/ training 1: 1
2: 2
3: 3
4: 4
Need the most preparation/ training 5: 5
Not applicable: 98
Don't know/ No response: 99
Q17B
Unpaid only
Dementia screening and diagnosis
Need the least preparation/ training 1: 1
2: 2
3: 3
4: 4
Need the most preparation/ training 5: 5
Not applicable: 98
Don't know/ No response: 99
Q17C
Unpaid only
Dementia subtypes and stages of progression
Need the least preparation/ training 1: 1
2: 2
3: 3
4: 4
Need the most preparation/ training 5: 5
Not applicable: 98
Don't know/ No response: 99
Q17D
Unpaid only
Day-to-day care of someone living with dementia
Need the least preparation/ training 1: 1
2: 2
3: 3
4: 4
Need the most preparation/ training 5: 5
Not applicable: 98
Don't know/ No response: 99
Q17E
Unpaid only
Advance care planning and end-of-life care
Need the least preparation/ training 1: 1
2: 2
3: 3
4: 4
Need the most preparation/ training 5: 5
Not applicable: 98
Don't know/ No response: 99
Q17F [0,1]
Unpaid only
Other (please specify)
Need the least preparation/ training 1: 1
2: 2
3: 3
4: 4
Need the most preparation/ training 5: 5
Not applicable: 98
Don't know/ No response: 99
PREQ18
Would you know where to find resources related to dementia on these topics if you needed them to support your care providing role?
Q18A
Dementia prevention / reducing risk
Yes: 1
No: 2
Not applicable: 98
Don't know/ No response: 99
Q18B
Dementia screening and diagnosis
Yes: 1
No: 2
Not applicable: 98
Don't know/ No response: 99
Q18C
Treatment and care of someone living with dementia
Yes: 1
No: 2
Not applicable: 98
Don't know/ No response: 99
Q18D
Stigma reduction [Rollover text: (Stigma is defined as negative attitudes or discrimination against someone based on a distinguishing characteristic such as a mental illness, health condition, or disability.)]
Yes: 1
No: 2
Not applicable: 98
Don't know/ No response: 99
Q18E
Advance care planning and end-of-life care
Yes: 1
No: 2
Not applicable: 98
Don't know/ No response: 99
Q18G
Culturally appropriate tools (Culturally appropriate tools give consideration to a patient's cultural background, personal experiences and norms)
Yes: 1
No: 2
Not applicable: 98
Don't know/ No response: 99
Q19 [1,3]
Yes to any Q18A-Q18H
Please provide some examples of resources that have been most helpful to you in your care providing role:
Please specify: 77
Don't know / No response: 99
Q21 [1,3]
Please provide examples of any resources or services to support [Q3 = 1]someone[Else]people living with dementia and caregivers that you think are lacking.
Please specify: 77
Don't know / No response: 99
PREQ22
Paid only
Do you have the necessary tools in order to provide culturally appropriate care or support for people living with dementia for the following populations? (Culturally appropriate care involves giving consideration to a patient's cultural background, personal experiences and norms)
Q22A
Paid only
Ethnic and cultural minority communities
Yes: 1
No: 2
Not applicable: 98
Don't know/ No response: 99
Q22B
Paid only
Indigenous peoples
Yes: 1
No: 2
Not applicable: 98
Don't know/ No response: 99
Q22C
Paid only
People with intellectual / developmental disabilities
Yes: 1
No: 2
Not applicable: 98
Don't know/ No response: 99
Q22D
Paid only
LGBTQ2+
Yes: 1
No: 2
Not applicable: 98
Don't know/ No response: 99
Q22E
Paid only
Official language minority communities
Yes: 1
No: 2
Not applicable: 98
Don't know/ No response: 99
Q22F
Paid only
Rural and remote communities
Yes: 1
No: 2
Not applicable: 98
Don't know/ No response: 99
Q22G
Paid only
Young onset dementia
Yes: 1
No: 2
Not applicable: 98
Don't know/ No response: 99
Q22H [0,1]
Paid only
Other (please explain)
Yes: 1
No: 2
Not applicable: 98
Don't know/ No response: 99
Q23 [1,3]
Paid only and yes to any Q22A-Q22H
Please list some of these tools.
Please specify: 77
Don't know / No response: 99
Q24
[Q4 = 3]Did[Else]Do you provide care or support for someone living with dementia in any of the following populations (e.g., ethnic and cultural minority communities, Indigenous peoples, LGBTQ2+, etc.)?
Yes, please specify: 1
No: 2
Don't know / No response: 99
Q25
Unpaid only and yes to Q24
[Q4 = 3]Did[Else]Do you use any culturally appropriate resources when providing care or support? (Culturally appropriate resources include advice or recommendations that give consideration to a patient's cultural background, personal experiences and norms.)
Yes: 1
No: 2
Don't know / No response: 99
Q26 [1,3]
Unpaid only and yes to Q24 and use culturally appropriate resources in Q25
Please list some of these resources.
Please specify: 77
Don't know / No response: 99
Q27 [1,3]
Based on your knowledge, what are the three most important risk or protective factors that should be prioritized in dementia prevention interventions?
[Phone version]Interviewer: Do not read list, prompt as needed
Education: 1
Hearing loss: 2
Hypertension: 3
Obesity: 4
Smoking: 5
Depression: 6
Physical inactivity: 7
Social isolation: 8
Diabetes: 9
Air pollution: 10
Alcohol consumption: 11
Traumatic brain injury: 12
Other (please specify): 77
Not sure: 98
Don't know / No response: 99
PREQ28
To what extent do you agree with the following statements about dementia?
[Phone version]Interviewer: Read scale
Q28A
[Q3 = 1]Someone[Else]People living with dementia can sometimes continue to live in their own homes for years following diagnosis
Strongly disagree 1: 1
Disagree 2: 2
Neutral: 3: 3
Agree 4: 4
Strongly agree 5: 5
Don't know/ No response: 99
Q28B
I am more comfortable providing care to a person without dementia than I am providing care to a person who is living with dementia
Strongly disagree 1: 1
Disagree 2: 2
Neutral: 3: 3
Agree 4: 4
Strongly agree 5: 5
Don't know/ No response: 99
Q28C
Negative stereotypes (stigma) about [Q3 = 1]someone[Else]people living with dementia are common within the health care system [Rollover text: (Stigma is defined as negative attitudes or discrimination against someone based on a distinguishing characteristic such as a mental illness, health condition, or disability.)]
Strongly disagree 1: 1
Disagree 2: 2
Neutral: 3: 3
Agree 4: 4
Strongly agree 5: 5
Don't know/ No response: 99
Q28D
Dementia is a normal/inevitable part of ageing
Strongly disagree 1: 1
Disagree 2: 2
Neutral: 3: 3
Agree 4: 4
Strongly agree 5: 5
Don't know/ No response: 99
Q28E
[Q3 = 1]someone[Else]people living with dementia can sometimes continue to work for years following diagnosis
Strongly disagree 1: 1
Disagree 2: 2
Neutral: 3: 3
Agree 4: 4
Strongly agree 5: 5
Don't know/ No response: 99
Q28F
I have witnessed negative stereotypes (stigma) reduce the quality of health care received by those living with dementia [Rollover text: (Stigma is defined as negative attitudes or discrimination against someone based on a distinguishing characteristic such as a mental illness, health condition, or disability.)]
Strongly disagree 1: 1
Disagree 2: 2
Neutral: 3: 3
Agree 4: 4
Strongly agree 5: 5
Don't know/ No response: 99
Q28G
[Q3 = 1]someone[Else]people living with dementia are sometimes able to continue being active in their communities for years following diagnosis
Strongly disagree 1: 1
Disagree 2: 2
Neutral: 3: 3
Agree 4: 4
Strongly agree 5: 5
Don't know/ No response: 99
Q28H
Some paid care providers are not comfortable communicating directly with [Q3 = 1]someone[Else]people living with dementia
Strongly disagree 1: 1
Disagree 2: 2
Neutral: 3: 3
Agree 4: 4
Strongly agree 5: 5
Don't know/ No response: 99
Q29 [1,3]
Based on your experience, which of the following would most [Q4 = 3]have made[Else]make a significant difference to your ability to provide quality dementia care or support?
Please select your top 3.
[Phone version]Interviewer: Read list
Better sharing of information across care providers and/or care settings: 1
Better access to culturally-appropriate information resources: 2
More dementia care training: 3
More time to spend with the person(s) I care for: 4
Mental health supports for care providers: 5
Having an advanced care plan in place: 6
Knowing the medical history of the person living with dementia: 7
Other (please explain): 77
Don't know / No response: 99
Q30 [1,7]
Paid only
What have you found to be the most challenging part of providing care or support to people living with dementia during COVID-19?
Select all that apply
[Phone version]Interviewer: Do not read list, prompt as needed
Lack of information, guidance and training on how to safely perform care duties: 1
Infection control and availability of protective equipment: 2
Adaptation of services (e.g. moving to telehealth and virtual care services): 3
Understaffing: 4
The nature of group and assisted living (e.g. crowding and shared rooms): 5
Staff working in multiple settings: 6
Other (please explain): 77
Don't know / No response: 99
Q31 [1,6]
Unpaid only
What have you found to be the most challenging part about caring for someone living with dementia during COVID-19?
Select all that apply
[Phone version]Interviewer: Do not read list, prompt as needed
Lack of information and clear guidance on how to safely perform care duties: 1
Cancellation or reduction of support services (e.g. home care): 2
Loss of activities that the person I provide care to can participate in (e.g. day programs): 3
Visitation restrictions: 4
Interacting with people living with dementia while using personal protective equipment (PPE) such as masks, gowns and gloves: 5
Other (please explain): 77
Not applicable: 98
Don't know / No response: 99
Q32 [1,2]
Could you provide 1 or 2 suggestions of things that could have been done differently to improve your ability to provide quality dementia care or support during COVID-19?
Please explain: 77
Don't know / No response: 99
QGENDR
What is your gender?
Male: 1
Female: 2
Another gender, please specify: 77
I prefer not to say: 99
QAGE
What is your age?
18-24: 1
25-34: 2
35-44: 3
45-54: 4
55-64: 5
65-74: 6
75-84: 7
85 or older: 8
QPROV
In which province or territory do you live?
Alberta: 2
British Columbia: 1
Manitoba: 4
New Brunswick: 7
Newfoundland and Labrador: 10
NorthWest Territories: 12
Nova Scotia: 8
Nunavut: 13
Ontario: 5
Prince Edward Island: 9
Quebec: 6
Saskatchewan: 3
Yukon: 11
QEDUC
What is the highest level of education that you have completed?
Grade 8 or less: 1
Some high school: 2
High school diploma or equivalent: 3
Registered apprenticeship or other trades certificate or diploma: 4
College, CEGEP or other non-university certificate or diploma: 5
University certificate or diploma below Bachelor's level: 6
Bachelor's degree: 7
Post graduate degree above Bachelor's level: 8
Prefer not to answer: 99
QETHN [1,16]
Other than Canadian, which ethnic or cultural group do you identify with?
Select all that apply
British (English, Scottish, Irish, Welsh): 1
French (includes Quebecois, Franco-Ontarian, Franco-Manitoban, Acadian, etc.): 2
We are conducting a series of interviews to further discuss information on the experiences and perspectives of paid and unpaid care providers to people living with dementia. It does not require that you have any specific knowledge. We are offering an incentive for participation in this added component. Would you be interested in possibly participating in one of these follow-up interviews?
Yes: 1
No: 2
Name:
Email:
Telephone:
Ext.:
Thank You
Those are all the questions we have for you. Thank you very much for taking the time to complete this survey, it is greatly appreciated. Your answers have been saved and you may now close your browser window.
THNK2
Screened-out
Unfortunately, based on your responses you are ineligible to participate in this survey. Thank you for your time!
C. Interview Guide
The Health Promotion and Chronic Disease Prevention Branch, Public Health Agency of Canada (PHAC), has commissioned this study to provide evidence-based data and key insights into the perspectives and experience of Canadian care providers’ in terms of dementia. PHAC has commissioned Ekos Research Associates (Ekos) to collect baseline data of the experiences and perspectives of dementia care providers. Findings from this study will contribute to supporting a skilled workforce, informing dementia awareness, and improving tools that support the ability to provide evidence-informed care. More broadly, this research supports the implementation of Canada’s national dementia strategy.
As part of this study, Ekos is conducting a number of in-depth interviews with various dementia care providers, including: family and friend caregivers of those living with dementia, developmental service workers, health care professionals , personal care workers, and first responders. The interview is expected to last about 60 minutes. Participation is voluntary and your confidentiality will be respected. No information that might directly or indirectly reveal your identity will be released or published without your specific consent to the disclosure. The interview will, however, be recorded to allow the interviewer to prepare summary notes from the interview. The recording will be destroyed once the project has been completed.
Thank you for taking the time to talk with us today and share your experiences. Your views and opinions are extremely important. Feel free to stop me at any time for a break or if you have any questions.
Experience Providing Care for People Living With Dementia
Please tell me about your experience in caring for someone living with dementia.
What kind of care do you provide?
How long have you been involved in dementia care (e.g., less than 1 year, 1-5 years, more than 5 years)?
About how much of your time/work hours are spent caring for someone living with dementia, or on dementia related care before COVID-19? Has this changed since COVID-19 (since March 2020)?
About how many people do you provide dementia care for in a typical month?
What kinds of population groups do you typically provide dementia care for (age, diversity)?
What do you feel are the top two or three factors that affect your ability to provide quality care to people living with dementia?
In your work, do you need culturally appropriate guidance to effectively support people living with dementia? (Culturally appropriate guidance may involve adapting tools and information in ways that consider cultural background, personal experiences, and norms and help to make it easier to use and more effective.) If yes....
Are you able to obtain the culturally appropriate guidance you need?
What makes it culturally appropriate?
Is this guidance available in the languages you need for those you support?
Do you use these tools/information often? Are they helpful?
What else is needed (i.e., gaps)?
Knowledge, Experiences and Perceptions
Before the COVID 19 pandemic, how comfortable/confident did you feel in your ability to provide adequate care for people living with dementia?
Do you agree that dementia is a normal / inevitable part of aging? Why or why not?
Do you think people living with dementia can live independently (on their own)? Why or why not?
To what extent do you think people living with dementia can have a good quality of life? (e.g., by staying active in the community)
To what extent do you involve family/friend caregivers in the health care planning process / decision making of a person living with dementia? Please describe why.
People living with dementia often report experiencing stigma – such as people underestimating their abilities or excluding them from activities. To what extent do you think stigma impacts the nature or quality of health care for those living with dementia?
Training and guidance
How knowledgeable do you feel about dementia risk factors and prevention?
In your opinion, what is most important when it comes to reducing the risk of developing dementia?
Do you feel well trained for the type of dementia care you are providing? Why or why not?
Have you received any specialized training in caring for people living with dementia? What kinds of training? Has this specialized training made you feel better equipped to provide quality care?
How do you stay current on dementia guidance (i.e.., guidelines and best practices) to provide care for people living with dementia?
Which sources have you found most helpful? Why is that?
What, if anything, is missing to help care providers stay up to date on dementia guidance and other important information?
Overall
What is the most challenging part of providing care to a person living with dementia?
If you have encountered significant new challenges in providing care for people living with dementia related to COVID-19 (since March 2020)? (e.g., transitions in care, telehealth, personal protective equipment, staffing), please tell me about them.
What is most rewarding about providing care to a person living with dementia?