This public opinion research report presents the results of an online survey conducted by Ekos Research Associates Inc. on behalf of the Public Health Agency of Canada. The research study was conducted between April 7 and June 21, 2021 with 1,008 Indigenous respondents or Non- Indigenous respondents who have provided care to an Indigenous person living with dementia.
Cette publication est aussi disponible en français sous le titre : Conseils en matière de démence et populations autochtones au Canada.
This publication may be reproduced for non-commercial purposes only. Prior written permission must be obtained from Health Canada. For more information on this report, please contact Health Canada at hc.cpab.por-rop.dgcap.sc@canada.ca or at:
Health Canada, CPAB
200 Eglantine Driveway, Tunney's Pasture
Jeanne Mance Building, AL 1915C
Ottawa, Ontario K1A 0K9
Catalogue Number:
H14-374/2021E-PDF
International Standard Book Number (ISBN):
978-0-660-39838-9
Related publications (registration number: POR 082-20)
Table 15: Measures to Ensure Culturally Appropriate Dementia Guidance – Paid Care Providers
Table 16: Response Rates
List of Charts
Chart 1: Awareness of Someone Living with Dementia – Indigenous Peoples (Other)
Chart 2: Taking Steps to Reduce Risk
Chart 3: Dementia Guidance Topics
Chart 4: First Sought-After Source of Dementia Guidance
Chart 5: Format Preferences
Chart 6: Gaps in Recommendations and Advice – Unpaid Care Providers
Chart 7: Gaps in Recommendations and Advice – Paid Care Providers
Chart 8: Challenges in Accessing Dementia Guidance for Indigenous Populations – Paid Care Providers
Chart 9: Challenges in Accessing Dementia Guidance for Indigenous Populations – Unpaid Care Providers
Chart 10: Use of Culturally Appropriate Guidance – Paid Care Providers
Executive Summary
A. Background and Objectives
Canada's first national dementia strategy, A Dementia Strategy for Canada: Together We Aspire, released in June 2019, identifies three national objectives: prevent dementia; advance therapies and find a cure; and improve the quality of life of people living with dementia and caregivers. The national strategy also identifies that Indigenous Peoples are a population at higher risk of developing dementia and may face barriers to diagnosis and care. Higher incidence of chronic conditions that are risk factors to dementia are prevalent in the Indigenous population[1]. Although dementia research in Indigenous populations is limited, some findings document a higher incidence of dementia among First Nations populations[2].
The primary objective of the research is to gather Indigenous perspectives on dementia guidance, including guidelines and best practices on prevention, diagnosis, treatment and management, stigma reduction, creating dementia inclusive communities, and emergency preparedness and response. Gathering Indigenous perspectives and experiences with dementia guidance is essential to move closer towards ensuring dementia guidance is culturally appropriate and culturally safe and reflects the distinctiveness across Indigenous Peoples, including geographic and other differences, as well as varying barriers and challenges
This research is intended to inform PHAC programs and initiatives, along with supporting information needs of others working on guidance. Results will also support annual reporting on the national dementia strategy to Parliament as required by the National Strategy for Alzheimer's Disease and Other Dementias Act.
B. Methodology
The survey is comprised of 1,008 completed cases of respondents, 18 years of age and older, including 111 paid care providers that have cared for an Indigenous person living with dementia in the last 10 years. These paid care providers may or may not be Indigenous themselves. Another 176 are unpaid care providers, defined as someone who provides unpaid care and support to an Indigenous person living with dementia, within the last 10 years. These unpaid care providers may or may not be Indigenous themselves. There is also a small sample of 28 individuals who reported themselves to be an Indigenous person living with dementia. The remaining 693 are Indigenous respondents who have identified themselves as not living with dementia and have not cared for an Indigenous person living with dementia in a paid or unpaid capacity in the last 10 years. This segment of respondents is referred to as Indigenous Peoples (Other) throughout the report.
The survey sample was drawn from multiple sources, including from the Probit panel, which is assembled using a random digit dial (RDD) process for sampling from a blended land-line cell-phone frame, which provides full coverage of Canadians with telephone access. The distribution of the recruitment process is meant to mirror the actual population in Canada (as defined by Statistics Canada). As such, our more than 120,000-member panel can be considered representative of the general public in Canada (meaning that the incidence of a given target population within our panel very closely resembles the public at large) and margins of error can be applied. We also relied on RDD of land and cell phones associated with geographic areas that include First Nation reserve communities. Respondents who had previously completed a survey of the general public in the spring of 2020, also participated if they were providing paid or unpaid care to an Indigenous person living with dementia. Further, a subset of respondents to a survey of dementia care providers, conducted in February-March 2021, also participated if they were providing care to an Indigenous person living with dementia. A small number of records were also completed as a result of referrals from other respondents within the sample.
The majority of the sample (76%) was collected by telephone, although 245 cases were completed online and mostly concentrated among those who are not individuals living with dementia. The interview length averaged 15 minutes online and 23 minutes by telephone. Cases were collected between April 7 and June 21, 2021, following extensive testing online and by telephone, in both English and French[3]. The rate of participation was 11% (14% online and 10% by telephone). Details on the rate of participation can be found in Appendix A and the questionnaire is provided in Appendix B.
This randomly recruited probability sample carries with it a margin of error of +/-3.1%. The margin of error for most target groups is between 5% and 10%. Results for those Indigenous respondents who are not living with dementia and have not provided paid or unpaid care to someone with dementia (i.e., "Indigenous Peoples (Other)") have been weighted to Indigenous population proportions for region, age, and Indigenous identity groupings (i.e., First Nations, Métis, Inuit). Chi-square tests were used to compare subgroups to the remaining sample. Where there was a sizable degree of association between sub-groups, multivariate analysis was used to further explore which independent variable (i.e., sub-groups such as Indigenous identify group, education, age, location) was most likely the strongest association and possible explanation for other associations. For scaled items (e.g., knowledge rating, degree to which the respondent agrees with a statement) linear regression was used and where the responses were not linear (i.e., response categories, such as yes and no), logistic regression was used.
C. Key Findings
Most Indigenous Peoples (Other)[4] in the survey know someone who is living with or has lived with dementia (66%); only 30% do not. Among this group, 42% said that they know an extended family member with dementia. Fewer said they know a friend, neighbour or colleague (19%), a community member (14%), Elder or Knowledge Keeper (12%) or parent (11%) living with dementia.
Survey respondents rated their knowledge regarding a variety of dementia topics, such as signs and symptoms, prevention, and dementia inclusive communities, on a 5-point scale, from not at all knowledgeable to very knowledgeable. Those who are paid to provide care to Indigenous Peoples living with dementia (i.e., paid care providers) tended to report higher knowledge on dementia topics than unpaid care providers. Those respondents who are Indigenous Peoples not living with dementia or providing paid or unpaid dementia care (i.e., Indigenous Peoples (Other)) self-reported the lowest levels of knowledge. Over three-quarters (77%) of paid care providers said they are moderately or very knowledgeable about the signs and symptoms of dementia. Over half of paid care providers said they are moderately or very knowledgeable of the ways to reduce the risk of developing dementia (54%) and how to make a community more welcoming and supportive of people living with dementia (52%). Over half (52%) of those respondents who are providing care to Indigenous Peoples living with dementia in an unpaid capacity (i.e., unpaid care providers) said they are moderately or very knowledgeable of the signs and symptoms of dementia. Nearly one-third (32%) of unpaid care providers felt knowledgeable about how to make the community more welcoming and supportive of people living with dementia and over one-quarter (28%) of unpaid care providers reported that they are moderately or very knowledgeable about the ways to reduce the risk of developing dementia. Among the Indigenous Peoples (Other) group, only about one-quarter (26%) felt moderately or very knowledgeable about the signs and symptoms of dementia. Fewer reported they were moderately or very knowledgeable about how to make a community more welcoming and supportive of people living with dementia (19%) or the ways to reduce the risk of developing dementia (14%).
Paid care providers are more likely than both the unpaid care providers and the Indigenous Peoples (Other) respondent groups to have selected harmful alcohol use (39%) more often as a key factor for an increased risk of developing dementia. The next most commonly identified factors, reported by all three respondent groups, are a diet lacking in healthy foods, lack of physical activity, and loneliness and social isolation.
Over half (59%) of unpaid care providers said they have taken steps to reduce their own risk of developing dementia, while two-thirds (66%) of paid care providers have done so. Only 39% of respondents within the Indigenous Peoples (Other) group said that they have taken steps to reduce their risk. The strongest barrier to reducing risk reported by unpaid care providers and Indigenous Peoples (Other) is a lack of awareness of what steps to take.
Paid care providers are less likely than unpaid care providers or the respondents from the Indigenous Peoples (Other) group to worry about the possibility of personally developing dementia (38%, compared to 56% and 50% respectively). Respondents were more concerned about someone close to them developing dementia than their own personal risk (55% of paid care providers, 68% of unpaid, and 67% of the general population).
Care provider respondents, including 70% of unpaid- and 69% of paid-, demonstrated a stronger preference than the general population for printed material such as brochures and pamphlets when looking for health recommendations or advice. Among Indigenous Peoples (Other), most indicated online resources as their preferred format (70%, compared to 57% of unpaid care providers and 62% of paid care providers).
Most paid care providers (77%) said they have used guidance on treatment and management of dementia. Half or more have used guidance on prevention (56%) or screening and diagnosis (50%). Overall, paid care providers would use primarily the websites of advocacy organizations (74%) for dementia guidance available online, followed by health care expert websites (68%) when looking for dementia guidance and recommendations. About half of paid care providers said they would be moderately or very likely to seek information online from the federal or provincial governments, or from regional or local Indigenous health authority websites. This is also the case for about four in ten unpaid care providers and the Indigenous Peoples (Other) group.
One-third of Indigenous Peoples (Other) living with dementia (32%) said they found or received dementia recommendations or advice. This respondent group indicated a need for dementia-related recommendations or advice on the different types of dementia, pharmacological and non-pharmacological treatments and therapies, and supports and services for people living with dementia.
Unpaid care provider respondents identified the strongest need for recommendations and advice on day-to-day care for people living with dementia (76%). About two-thirds reported the need for advice on screening and diagnosis of dementia (69%), ways to reduce the risk of developing dementia (68%), transitions in care (65%), or dementia-inclusive communities and negative stereotypes (64%).
About seven in ten paid care providers reported gaps or barriers in dementia guidance on the treatment and management of dementia (70%), how to make interactions feel safe and more supportive (69%), ways to reduce the risk of developing dementia (68%), or transitions in care (68%).
Less than half (47%) of paid care providers felt that the dementia guidance and related tools they use to provide care and support to Indigenous Peoples living with dementia are culturally appropriate and culturally safe. There is a strong consensus among paid and unpaid care providers as well as respondents in the Indigenous Peoples (Other) group that the development of dementia guidance should involve Indigenous communities and Elders in order to be culturally appropriate, and that training for care providers should be specific to Indigenous Peoples. Specifically, 81% of unpaid care providers, 79% of paid care providers, and 75% of respondents in the Indigenous Peoples (Other) group felt that in order to ensure that recommendations or advice about dementia are culturally appropriate and culturally safe for Indigenous Peoples, training for care providers should be specific to Indigenous Peoples living with dementia. Most respondents also felt that it is important to involve Indigenous Peoples in the development of recommendations or advice to ensure the material is culturally appropriate and safe for Indigenous populations (84% of paid care providers, 82% of the Indigenous Peoples (Other) group and 79% of unpaid care providers). About three-quarters said that material should involve Indigenous Elders, Healers, and Knowledge Keepers (79% of paid care providers, 77% of respondents in the Indigenous Peoples (Other) group and 75% among unpaid care providers).
D. Note to Readers
Detailed findings are presented in the sections that follow. Overall results are presented in the main portion of the narrative and are typically supported by graphic or tabular presentation of results. Results are presented separately for each of the four types of respondents:
Indigenous Peoples living with dementia – caution should be used in interpreting the findings because of relatively small sample size; (n=28);
Paid care providers – Indigenous and non-Indigenous individuals providing paid care to an Indigenous person living with dementia;
Unpaid care providers – Indigenous and non-Indigenous individuals providing unpaid care to an Indigenous person living with dementia; and,
Indigenous Peoples (Other)[5] – Indigenous respondents (including First Nations, Métis, Inuit and those who identified otherwise as Indigenous)[6] who are not living with dementia, nor providing paid or unpaid care to Indigenous Peoples living with dementia.
It should be noted that results are presented separately for each respondent group[7] in the charts, tables and introductory text. Results for the proportion of respondents in the sample who either said "don't know" or did not provide a response (i.e., DK/NR) may not be indicated in the graphic representation of the results in all cases, particularly where they are not sizable (e.g., 10% or less). Results may also not total to 100% due to rounding. Some questions invited respondents to indicate "other" and provide their own response. In some cases, these "other" responses were coded into existing response categories or new categories were added. In the case of the latter, these are indicated in the chart or table through the use of "(unprompted)" following the new category label.
Bulleted text presented below charts and/or tables is also used to point out any statistically and substantively significant differences between regional and demographic sub-groups of respondents. Regional and demographic sub-groups results are pooled for all respondents, across the four respondent types. Sub-groups include:
Three separate Indigenous identity groups (First Nations, Métis and Inuit) among the 88% of respondents who are Indigenous.
Results based on region, and urban/rural location[8];
Key demographic patterns of interest which are described based on gender, age, education, and sexual orientation. Since education is strongly correlated with type of respondent, with paid and unpaid care providers reporting higher levels of education than the other two respondent groups, results are only described for education where they do not seem to be explained by other differences among the main respondent groups.
Only differences that are statistically and substantively different (e.g., five percentage points from the overall mean) are presented, where there are at least 10 responses in a given cell.
Details of the methodology and sample characteristics can be found in Appendix A. The programmed survey instrument can be found in Appendix B.
E. Contract Value
The contract value for the POR project is $99,980.65 (including HST).
I hereby certify as Senior Officer of Ekos Research Associates Inc. that the deliverables fully comply with the Government of Canada political neutrality requirements outlined in the Communications Policy of the Government of Canada and Procedures for Planning and Contracting Public Opinion Research. Specifically, the deliverables do not include information on electoral voting intentions, political party preferences, standings with the electorate, or ratings of the performance of a political party or its leaders.
Signed by: Susan Galley (Vice President)
Detailed Findings
A. Profile
Of the 1,008 respondents in the survey sample, 28 indicated themselves to be Indigenous and living with dementia. Another 111 are Indigenous (23%) or non-Indigenous (75%) and paid to provide care to one or more Indigenous individuals who are living with dementia, either currently, or within the past 10 years. Another 176 are Indigenous (74%) or non-Indigenous (23%) and provided unpaid care or support to an Indigenous person living with dementia, either currently or within the past 10 years. The majority of the sample (693) identified as Indigenous Peoples who are not living with dementia, nor have they provided paid or unpaid care to an Indigenous person living with dementia within the last 10 years. This segment of respondents is referred to as Indigenous Peoples (Other) throughout the report. Of these, 24 Indigenous respondents provided unpaid care over 10 years ago. Also, among those who are paid to provide care to an Indigenous person living with dementia, one in four are also currently providing or have provided unpaid dementia care.
The largest proportion of the sample are First Nations (48%: 456 individuals), of whom 75% are not living with dementia nor providing dementia care. Another 32% (331 individuals) are Métis, of whom 70% are not living with dementia nor providing dementia care. A smaller proportion are Inuit (7%: 75 individuals), of whom 59% are not living with dementia, nor providing dementia care[9]. A sizable proportion of the overall sample (12%: 127 individuals) are not Indigenous but are included as respondents who have provided or are currently providing paid or unpaid care to one or more Indigenous Peoples who are living with dementia.
The following are the sample characteristics of the sample for paid and unpaid care providers as well as for Indigenous Peoples (Other).
Table 1: Sample Characteristics – Care Providers and Other Indigenous Respondents Table
8th grade or less (equivalent to secondary II in Quebec)
3%
2%
2%
Some high school
5%
2%
9%
High school diploma or equivalent
20%
5%
1%
Registered apprenticeship or other trades certificate or diploma
6%
3%
5%
College, CEGEP or other non-university certificate or diploma
24%
30%
27%
University certificate or diploma below Bachelor's level
7%
8%
8%
Bachelor's degree
14%
32%
17%
Post graduate degree above Bachelor's level
19%
19%
11%
No response
2%
0%
1%
Urban/Rural
176
111
693
Urban
49%
48%
40%
Rural
35%
21%
30%
Language
176
111
693
English
90%
86%
93%
French
10%
14%
7%
Among the three Indigenous identity groups, those who are Métis are more likely than the other two groups to report a university level of education (42% vs. 20% among First Nations respondents and 19% among Inuit respondents). Métis respondents are also typically older (55% are 55 years of age or older compared with only 39% of First Nation and 20% of Inuit respondents who are 55 or older). Higher proportions of First Nations and Inuit respondents are under 35 (36% and 50% respectively, compared with only 20% of Métis respondents). There is also a higher concentration of urban residents among Métis respondents (61%) compared with 30% among First Nations respondents and 8% among Inuit respondents.
Knowing Someone with Dementia – Other Indigenous Peoples
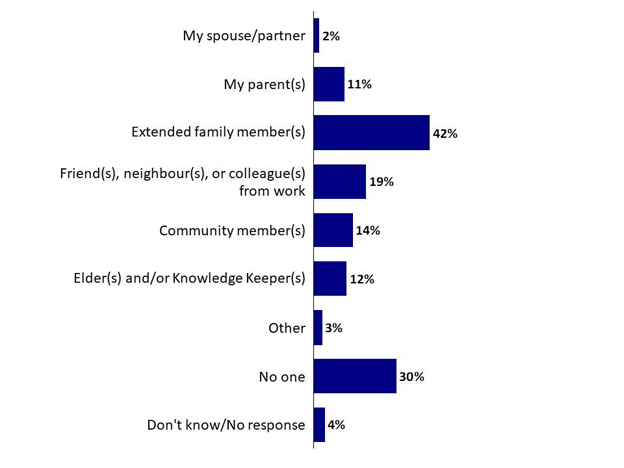
Forty-two per cent of respondents within the Indigenous Peoples (Other) respondent group said that they know an extended family member who is living with or has lived with dementia. Less than one in five know a friend, neighbour or colleague (19%), a community member (14%), or Elder or Knowledge Keeper (12%) who is living or has lived with dementia. Eleven per cent said that their parent is living with or has lived with dementia while two per cent named their spouse or partner. Thirty per cent responded that they do not know anyone living with or who has lived with dementia.
Chart 1: Know Someone Living with Dementia – Indigenous Peoples (Other)
Chart 1: Know Someone Living with Dementia – Indigenous Peoples (Other) - Text Version
This chart of single bars shows the percentage of results for responses to nine statements.
Respondents were asked: "Do you know anyone who is living/has lived with dementia?"
Respondents selected:
My spouse/partner: 2%
My parent(s): 11%
Extended family member(s): 42%
Friend(s), neighbour(s), or colleague(s) from work: 19%
Community member(s): 14%
Elder(s) and/or Knowledge Keeper(s): 12%
Other: 3%
No one: 30%
Don't know/no response: 4%
Base: GP n=682
Q6. Do you know anyone who is living/has lived with dementia?
Base: GP n=682
Métis respondents are more likely to know a friend, neighbour or colleague who is living or has lived with dementia (26%), First Nation respondents are less likely to say this (14%). Inuit respondents are more likely than Métis or First Nations to say they do not know anyone who is living or has lived with dementia (42%). Métis are also more likely than First Nation or Inuit respondents to say a parent is or was living with dementia (16% compared with 7% among the other two groups).
Urban residents are more likely than rural residents to say they know an extended family member (50%), friend (29%) or parent (18%) who is living or has lived with dementia. On the other hand, rural residents are more likely to say they know a community member who is living or has lived with dementia (18%).
Those in Atlantic Canada[12] (36%) are more likely than those in any other region to say they know a friend, neighbour or colleague who is living or has lived with dementia. Respondents in British Columbia (29%) are more likely to identify knowing an Elder or Knowledge Keeper who is living or has lived with dementia.
Respondents under age 35 years (40%) are more likely than those over 35 years of age to say they do not know anyone living with dementia. Those aged 55-74 years tend to say their parent is living with dementia (19% to 23%). Respondents aged 55 years and over (31% - 33%) are more likely than their younger counterparts to report they know a friend, neighbour or colleague who is living or has lived with dementia. Those over age 65 years (8%) tend to identify a spouse or partner as the individual they know who is living or has lived with dementia.
B. Knowledge and Perceptions Regarding Dementia
Perceived Knowledge Level
Three groups of survey respondents[13] rated their knowledge on a variety of dementia topics, such as signs and symptoms, prevention, and dementia inclusive communities, on a 5-point scale, from not at all knowledgeable to very knowledgeable. Over half (52%) of unpaid care providers said they are moderately or very knowledgeable of the signs and symptoms of dementia, while 18% felt they are not at all or a little knowledgeable. Over one-quarter (28%) of unpaid care providers reported that they are moderately or very knowledgeable about the ways to reduce the risk of developing dementia; a greater proportion said they are not at all or a little knowledgeable in this area (45%). About one-third (32%) of unpaid care providers felt moderately or very knowledgeable about how to make the community more welcoming and supportive of people living with dementia.
Paid care providers have a higher self-reported level of knowledge on dementia topics relative to unpaid care providers and the Indigenous Peoples (Other). Over three-quarters (77%) of paid care providers said they are moderately or very knowledgeable about the signs and symptoms of dementia. Over half of paid care providers said that they are moderately or very knowledgeable of the ways to reduce the risk of developing dementia (54%) or how to make a community more welcoming and supportive of people living with dementia (52%).
Among Indigenous Peoples (Other), only about one-quarter (26%) felt moderately or very knowledgeable about the signs and symptoms of dementia. Fewer reported themselves to be moderately or very knowledgeable about the ways to reduce the risk of developing dementia (14%) or how to make a community more welcoming and supportive of people living with dementia (19%).
How knowledgeable about the following dementia topics would you say you are?
Unpaid Providers
Paid Providers
Indigenous Peoples (Other)
Q1.a Signs and symptoms of dementia
n=176
n=111
n=693
A little/Not at all
18%
6%
42%
Somewhat
30%
17%
30%
Very/Moderately
52%
77%
26%
Don't know/No response
1%
0%
2%
Q1.b Ways to reduce the risk of developing dementia
n=176
n=111
n=693
A little/Not at all
45%
27%
62%
Somewhat
23%
19%
20%
Very/Moderately
28%
54%
14%
Don't know/No response
4%
0%
4%
Q1.c How to make a community more welcoming and supportive of people living with dementia
n=176
n=111
n=693
A little/Not at all
35%
23%
59%
Somewhat
31%
24%
17%
Very/Moderately
32%
52%
19%
Don't know / No response
2%
0%
5%
Among Indigenous respondents, Inuit and First Nations respondents are more likely than Métis respondents to say they are not knowledgeable about signs and symptoms of dementia (43% and 42% respectively compared with 31% among Métis). The same is also true about ways to reduce the risk of developing dementia (75% and 63% respectively indicated limited knowledge compared with 51% among Métis). A series of multivariate tests were performed to examine the influence of Indigenous identify group, education, age and urban/rural setting of respondents on self-rated knowledge. Results indicate that the pattern among Indigenous identity groups is likely explained by education since reported knowledge increases with education and the education profile is higher among Métis respondents than it is among the other two Indigenous groups in the sample.
Residents in urban areas are also more likely to be knowledgeable about signs and symptoms (42% versus 38%) as well as ways to reduce the risk of dementia (25% versus 17% in rural areas), although this is likely driven by the greater propensity of Métis respondents (who within this sample have comparatively higher education and are older; both associated with higher knowledge) to live in urban areas.
Residents of the Territories are more likely than others across the country to say they have a high knowledge of how to make a community more welcoming (40%).
Levels of knowledge about signs and symptoms and ways to reduce the risk of dementia increase with age. Those aged 55-64 years of age and 65-74 years of age (45% each) are more likely to say they are knowledgeable about the signs and symptoms of dementia while those aged 35 years and younger (21%) are least likely. Respondents aged 55-64 years of age or 65-74 years of age (25% each) are more likely to report higher knowledge of ways to reduce the risk, particularly compared to those aged 35 years and younger (13%).
Understanding of Contributing Factors
The top factors that come to mind to unpaid care providers when thinking about what increases the chances of developing dementia include a diet lacking in healthy foods (26%), loneliness and social isolation (24%), a lack of physical activity (23%), genetics (22%), and harmful alcohol use (19%).
Paid care providers are more likely than other respondent groups to have identified harmful alcohol use (39%) as a factor that increases the chances of developing dementia. Other top factors reported by paid care providers include a diet lacking in healthy foods (31%), loneliness and social isolation (25%), a lack of physical activity (23%), and genetics (29%). Paid care providers are also much more likely to have said that hypertension (18%) is a factor in increasing chances of developing dementia.
Among Indigenous Peoples (Other), the top factors reported include a diet lacking in healthy foods (26%), loneliness and social isolation (21%), genetics (23%), and a lack of physical activity (19%).
Table 3: Perception of Factors that Contribute to Dementia
Col1
Unpaid Providers
Paid Providers
Indigenous Peoples (Other)
Q2. What are the first three things that come to mind when thinking about what factors increase your chances of developing dementia?
n=176
n=111
n=693
Diet lacking in healthy foods
26%
31%
26%
Loneliness/social isolation
24%
25%
21%
Lack of physical activity
23%
23%
19%
Harmful alcohol use
19%
39%
17%
Genetics/hereditary (unprompted)
22%
29%
23%
Mental health (unprompted)
12%
4%
5%
Age/aging (unprompted)
9%
6%
9%
Sleep disruption
7%
7%
8%
Smoking
7%
11%
5%
Hypertension/high blood pressure
6%
18%
4%
Head trauma/injury/concussion (unprompted)
6%
6%
3%
Lack of cognitive stimulation (unprompted)
6%
3%
5%
Diabetes
5%
6%
4%
Chronic drug use/abuse (unprompted)
4%
5%
3%
Other illness/disease (unprompted)
4%
6%
2%
Fewer years of formal education
4%
3%
3%
Lifestyle (general mention, unprompted)
4%
5%
3%
Harmful chemical exposure (unprompted)
5%
1%
5%
Air pollution
3%
3%
2%
Hearing loss
3%
3%
2%
High cholesterol
2%
3%
2%
Health (general mention, unprompted)
3%
2%
2%
Environment (general mention, unprompted)
1%
3%
3%
Nothing comes to mind
7%
5%
12%
Other
5%
4%
5%
Don't know/No response
7%
5%
12%
Métis respondents are more likely to identify a diet lacking in healthy foods (31%), genetics (32%), or a lack of physical activity (26%), compared with First Nations or Inuit respondents, as factors that increase the chance of developing dementia. As previously described, based on multivariate testing of the influence of Indigenous identity group, age, education and urban/rural setting on the likelihood to identify these factors, this is likely related to the pattern of higher education level among Métis respondents. University educated respondents are also more likely than those with lower education to mention a diet lacking in healthy foods (33%), genetics (34%), lack of physical activity (27%) or social isolation (27%).
Those in urban areas are more likely than others to point to a diet lacking in healthy foods (31%) and heredity (34%), although this is likely driven by the greater propensity of Métis respondents to live in urban areas, who are also more likely to be university-educated.
Regionally, those in Alberta are more likely than others across the country to mention a diet lacking in healthy foods (39%) and genetics (33%). Residents of Quebec are more likely to say harmful alcohol use (29%) as a factor. Residents of the Territories[14] (21%) are more likely than other residents to say that nothing comes to mind.
Younger respondents, aged 35 years and under, are more likely to name sleep disruption such as sleep apnea (14%). Those 35-44 years of age are more apt to say hypertension (12%) or smoking (12%).
Women (25%) are more likely than men (18%) to point to social isolation as a factor that increases the chance of developing dementia.
Worry Regarding Dementia
Unpaid care providers and other Indigenous Peoples were each asked to respond to questions addressing personal concerns about dementia. There was the propensity to worry more about the possibility of someone close to them developing dementia, than personally developing dementia. Two-thirds (68%) of unpaid care providers agreed or strongly agreed that they worry about the possibility of someone close to them developing dementia. Over half (56%) agree that they worry about personally developing dementia.
Among Indigenous Peoples (Other), 67% agree or strongly agree that they worry about someone close to them developing dementia. Half (50%) agree that they worry about the possibility of personally developing dementia.
Table 4: Concern for Dementia
To what extent do you agree or disagree with the following?
Unpaid Providers
Indigenous Peoples (Other)
Q3.d I worry about the possibility of personally developing dementia
n=176
n=692
Strongly disagree/Disagree
26%
29%
Neither
16%
17%
Strongly agree/Agree
56%
50%
Don't know / No response
3%
4%
Q3.e I worry about the possibility of someone close to me developing dementia
n=176
n=692
Strongly disagree/Disagree
15%
17%
Neither
16%
11%
Strongly agree/Agree
68%
67%
Don't know / No response
2%
5%
Inuit respondents are more likely than First Nation or Métis respondents to say they are not worried about someone close to them developing dementia (31% compared with 17% and 15%, respectively).
Younger respondents (under age 35) (76%) are more likely to say they worry about the possibility of someone close to them developing dementia; older respondents are least likely (55% of those aged 65 years and older). Those 65 or older are also the least likely to say they are concerned about personally developing dementia (35% disagree that they are worried about personally developing dementia compared with 21% to 24% of younger age groups).
Women (71%) are more likely than men (60%) to say they worry about the possibility of someone close to them developing dementia.
LGBTQ2+ respondents (87%) are more likely than those who identify as heterosexual (65%) to worry about the possibility of someone close to them developing dementia.
Respondents with a high school education (57%) are more likely to say they worry about the possibility of personally developing dementia, when compared to those with college (47%) or university (52%) education.
Those in Atlantic Canada (67%) are more likely to say they worry about the possibility of personally developing dementia; those in the Territories (40%) are least likely.
Reducing the Risk of Dementia
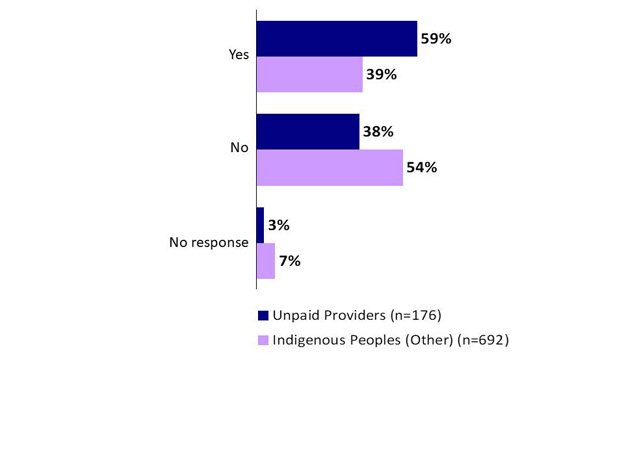
The majority (59%) of unpaid care providers said they have taken steps to reduce their own risk of developing dementia. Only 39% of Indigenous Peoples (Other) respondents said that they have taken steps to reduce their risk.
Chart 2: Taking Steps to Reduce Risk
Chart 2: Taking Steps to Reduce Risk - Text Version
This chart with single bars shows the percentage of results for responses to three statements: yes, no, and no response across two groups: Unpaid Providers and Indigenous Peoples (Other).
Respondents were asked: "Have you taken steps to reduce your own risk of developing dementia?"
Q14. Have you taken steps to reduce your own risk of developing dementia?
Métis (50%) respondents are more likely than First Nations (38%) or Inuit (20%) respondents to say they have taken steps to reduce their risk of developing dementia. This may be related to comparatively higher education levels since the incidence of not taking steps is highest among those with a high school level of education (57% compared with 49% and 46% among those with college and university levels of education ).
Similarly, residents of urban areas are also more likely to have taken steps (54% versus 40% in rural areas), although this is likely driven by the greater propensity of Métis respondents, who have comparatively higher education levels, to live in urban areas.
Those 55-64 years of age (54%) and 65-74 years of age (53%) are more likely than those older or younger to say they have taken steps to reduce their own risk of developing dementia. Those under 35 are least likely to have taken steps (30%). This age pattern also helps to explain the pattern among the three Indigenous identity groups since Métis respondents are older than First Nations and Inuit respondents.
Among those who have not taken steps to reduce their risk of developing dementia, one-third (34%) of unpaid care providers said that they did not because they are not aware of what to do to reduce risk. One in four unpaid care providers felt that they were either not personally concerned about developing dementia (16%) or dementia advice did not seem relevant to their situation (10%).
Over half (57%) of Indigenous Peoples (Other) said that they did not take steps because they are not aware of what to do to reduce their risk of developing dementia. One in five either do not consider themselves to be at risk of developing dementia (10%), are not personally concerned about it (7%), or generally do not find the advice relevant for them personally (4%). Another 8% said they do not feel it will make a difference.
Table 5: Barriers to Reducing Risk
Col1
Unpaid Providers
Indigenous Peoples (Other)
Q15 What has prevented you from taking steps to reduce your risk of developing dementia?
n=67
n=369
I am not aware of what to do to reduce my risk
34%
57%
I am not concerned/never think or worry about it (general, unprompted)
16%
7%
The advice doesn't seem relevant to my situation
10%
4%
I am not sure it will make a difference
4%
8%
Resources are not available in my community
4%
2%
Do not consider myself at risk (unprompted)
4%
10%
I am busy with other responsibilities (unprompted)
4%
3%
I am dealing/living with other health or mental health issues (unprompted)
6%
1%
It is too hard to make the changes
1%
2%
Other
6%
2%
Don't know
12%
12%
No response
1%
3%
Métis respondents who have not taken any steps are more likely to say they are not aware of what to do to reduce risk of developing dementia (62%) compared with First Nations (52%) or Inuit (40%) respondents.
Related to the pattern among Indigenous identifying groups, the incidence of citing lack of awareness of steps to take was considerably higher among those with a university level of education. (The education profile of Métis respondents in the sample is higher than it is for the other two Indigenous groups).
Those living in rural areas are somewhat more likely to say they do not feel at risk (13%).
The likelihood of pointing to lack of awareness of the steps to take is also higher in Alberta (67%) and lowest in Quebec (38%) compared with other parts of the country.
Perceptions of Community Supports
Forty-two per cent of unpaid care providers agreed or strongly agreed that people in their community are knowledgeable, respectful, and supportive of people living with dementia, although 36% believe their community is not supportive. Less than one-quarter of unpaid care providers felt that the physical environment of their community, such as housing or transportation, is supportive of people living with dementia (23%) or that there are sufficient resources in their community (23%).
Half (50%) of paid care providers agreed or strongly agreed that people in their community are knowledgeable, respectful, and supportive of people living with dementia. About one-quarter of paid care providers said that the physical environment of their community is supportive of people living with dementia (28%) or that there are sufficient resources (25%).
Among Indigenous Peoples (Other), 34% of respondents agreed or strongly agreed that people in their community are knowledgeable, respectful, and supportive of people living with dementia.
Table 6: Perception of Community Support for People Living with Dementia
To what extent is your community each of the following?
Unpaid Providers
Paid Providers
Indigenous Peoples (Other)
Q3.c People in my community are knowledgeable, respectful and supportive of people living with dementia
n=176
n=111
n=693
Strongly disagree/Disagree
36%
24%
25%
Neither
16%
23%
22%
Strongly agree/Agree
42%
50%
34%
Don't know/No response
5%
3%
19%
Q5.a The physical environment of my community is supportive of people living with dementia
n=176
n=111
NA
Not at all/Limited
47%
35%
--
Moderate
24%
33%
--
Considerable/Great
23%
28%
--
Don't know/No response
7%
4%
--
Q5.b There are sufficient resources
n=176
n=111
NA
Not at all/Limited
53%
41%
--
Moderate
21%
32%
--
Considerable/Great
23%
25%
--
Don't know / No response
3%
1%
--
Among Indigenous respondents, Inuit (57%) and First Nations (42%) are more apt to say people in their community are knowledgeable, respectful and supportive. Only 25% of Métis respondents believe this to be the case, while 33% disagree. Multivariate analysis tests were performed to examine the influence of Indigenous identity group, age, education and urban vs rural setting on the tendency to agree regarding knowledge, supportiveness and respectfulness of their community. Results indicate that this is likely related to education, since those with a high school level of education are most likely to believe their community is supportive; an incidence that is higher among Inuit respondents and lowest among Métis. Métis respondents are also more likely than the other two Indigenous identity groups to disagree (53%) that the physical environment in their community is supportive.
While rural residents more often agree that people in their community are knowledgeable, respective and supportive (45% agree vs. 34%), those in urban areas are more likely than rural residents to disagree (32% versus 28%).
Regionally, those living in the Territories (55%) and Quebec (48%), are more likely than others across the country to agree that people in their community are knowledgeable, respectful, and supportive of people living with dementia. Residents of Alberta are more likely than others to disagree (37%). Those in Quebec are also more likely than others across the country to agree that the physical environment in their community is supportive (38%)
Those with a high school level of education are more likely than those with more education to agree that there are sufficient resources in their community to support people living with dementia and their caregivers (37% compared with only 22% among those with post-secondary education).
Perceptions of Limitations of People Living with Dementia
Among unpaid care providers, 55% agreed or strongly agreed that people living with dementia can sometimes continue working for years after the onset of symptoms. However, two-thirds agreed that people living with dementia generally face a lower quality of life than people who are not living with dementia.
Two-thirds (68%) of paid care providers agreed or strongly agreed that people living with dementia can sometimes continue working for years after the onset of symptoms, while slightly more (71%) agreed that people living with dementia generally face a lower quality of life than people who are not living with dementia.
Indigenous Peoples (Other) were less likely to agree or strongly agree with both statements. Less than half (45%) agreed that people living with dementia are sometimes able to continue working after the onset of symptoms. Sixty-two per cent agreed that people living with dementia face a lower quality of life.
Table 7: Perception of Capacity of People Living with Dementia
To what extent do you agree or disagree with the following?
Unpaid Providers
Paid Providers
Indigenous Peoples (Other)
Q3.a People living with dementia are sometimes able to continue working for years after the onset of symptoms
n=176
n=111
n=693
Strongly disagree/Disagree
21%
13%
18%
Neither
18%
18%
27%
Strongly agree/Agree
55%
68%
45%
Don't know/No response
6%
1%
11%
Q3.b People living with dementia generally face a lower quality of life than people without dementia
n=176
n=111
n=693
Strongly disagree/Disagree
14%
13%
12%
Neither
18%
15%
20%
Strongly agree/Agree
66%
71%
62%
Don't know/No response
2%
1%
7%
Among Indigenous respondents, Métis peoples are more likely to agree that people living with dementia generally face a lower quality of life (69%) compared with First Nations (60%) or Inuit respondents. In fact, Inuit respondents are almost as likely to disagree (34%) as agree (45%).
Similarly, those respondents who are university-educated are more likely to agree that people living with dementia generally face a lower quality of life (74%) compared with 56% of those with a high school level of education.
Urban residents (who are also more likely to be university-educated) are also more likely to agree that people with dementia face a lower quality of life (68%) and can continue to work for years (56%) compared with rural residents (55% and 43%, respectively).
Residents of Ontario are most likely across the country to agree that people with dementia generally face a lower quality of life (69%), while those in British Columbia are least likely to agree (55%). Residents of the Territories are more likely to disagree that people living with dementia are sometimes able to continue working for years after the onset of symptoms (32%).
Respondents aged 35-44 (63%) are more likely than any other age group to agree that people with dementia are sometimes able to continue working. This is least likely among those under 35 years of age (41%).
Women are more likely than men to agree that people with dementia generally face a lower quality of life (66% versus 60% among men).
Quality of Life for People Living with Dementia
Over one-third (38%) of unpaid care providers said that having frequent support and visits with family and friends contributes most to the quality of life of those living with dementia. Twenty per cent of unpaid care providers indicated good physical health and 22% indicated living with loved ones as top factors that contribute to quality of life. Slightly fewer unpaid care providers perceived that being able to stay in their own home as long as possible (16%), having access to good quality staff and supports (18%), and having enough access to health care services (14%) were top factors.
Four in ten (41%) paid care providers likewise said that having frequent support and visits with family and friends was a top factor in the quality of life of those living with dementia. Over one-quarter (27%) of paid care providers felt that good physical health was a top factor that contributes to quality of life. Slightly fewer paid care providers perceived that living with loved ones (20%), feeling like they belong to a community (18%), being able to stay in their own home as long as possible (17%), having access to good quality staff and supports (17%), and having enough access to health care services (15%) were top factors.
Table 8: Contributors to a Good Quality of Life – Care Providers
Col1
Unpaid Providers
Paid Providers
Q7 Thinking about the Indigenous peoples living with dementia who you have provided care to, what are the top three factors you believe contribute the most to their quality of life?
n=176
n=111
Having frequent (weekly or more often) support and visits with family and friends
38%
41%
Living with loved ones (family and friends)
22%
20%
Good physical health
20%
27%
Improve access to good quality/adequate support staff/services, supports for respite care (unprompted)
18%
17%
Being able to stay in their own home as long as possible
16%
17%
Having enough access to health care services
14%
15%
Feeling like they belong to a community
12%
18%
Good mental health
11%
12%
Good spiritual health
8%
8%
Having a sense of purpose, that their life is useful
8%
9%
Access/transportation to activities (mental/physical stimulation) (unprompted)
8%
3%
Compassion/understanding (unprompted)
7%
5%
Being able to express their culture through language and other ways
6%
13%
Being independent in their daily living needs
6%
9%
Not having to worry about money
5%
9%
Being able to move around their community as much as they want
5%
4%
Consistency/routine (unprompted)
4%
5%
Living in safe homes/facilities, living in an supportive environment (unprompted)
3%
6%
Culturally appropriate care (holistic/alternatives/Indigenous approaches, more respect for their culture/history...) (unprompted)
3%
5%
Knowledge/awareness/training for caregivers and family/friends (unprompted)
3%
5%
Being able to be out on the land
1%
2%
Other
3%
1%
Don't know
7%
2%
Regionally, those in Quebec are more likely than those in other provinces or territories to say having frequent support and visits from family and friends (51%) is a top factor contributing to the good quality of life for Indigenous Peoples living with dementia. Those in Ontario (16%) are more likely to name good spiritual health.
Those under age 35 years of age are more likely than older cohorts to name good physical health (41%). Those aged 55-64 years of age are apt to say access to good quality support staff and service and supports for respite care (29%). Individuals who are 65 or older are most likely to point to staying in their home as long as possible (24%) as a top factor.
Individuals who are university-educated are somewhat more likely than other respondents to say a top factor is being able to express their culture through language and other ways (13%).
Among Indigenous Peoples living with dementia, one-third (32%) said that good physical health is an important factor in quality of life, followed by 29% who felt that good mental health was important. Having frequent support and visits with family and friends, and having basic needs met were each important aspects of quality of life, according to 18% of those living with dementia. Fourteen per cent of Indigenous Peoples living with dementia listed not having to worry about money good spiritual health, feeling like they belong to a community, being able to stay in their own home as long as possible, having a sense of purpose and living with loved ones as one of their top three factors in having a good quality of life.
Table 9: Contributors to a Good Quality of Life – People Living With Dementia
Q8 What are three things that are most important for you in having a good quality of life?
n=28
Good physical health
32%
Good mental health
29%
Having frequent (weekly or more often) support and visits with family and friends
18%
Basic needs met (safe housing/food...)
18%
Not having to worry about money
14%
Good spiritual health
14%
Feeling like I belong to a community
14%
Being able to stay in my own home as long as possible
14%
Living with loved ones (family and friends)
14%
Having a sense of purpose, that my life is useful
14%
Being able to be out on the land
11%
Being independent in my daily living needs (e.g., preparing my own food, laundry, shopping)
7%
Being able to express my culture through language and other ways
4%
Being able to move around my community as much as I want
4%
Having enough access to health care services
4%
Compassion/understanding (unprompted)
4%
Improved access to doctor/care (unprompted)
4%
Other
7%
Among Indigenous Peoples living with dementia, 43% said their quality of life is excellent or very good. Another 18%, however rate it as fair to poor. Overall health is rated as excellent or very good by 32%, 33% say this is true with regard to their ability to socialize, and 35% say this about their happiness. On the other hand, 32% say their health is fair to poor, 29% say the same about their happiness, and 22% say this about their ability to socialize. Two in three (64%) Indigenous Peoples living with dementia said they have enough of a say in decisions about their medical and day-today care, although 32% do not believe they do.
Table 10: Ratings of Quality of Life and Health – Indigenous Persons Living with Dementia
Q9. How would you rate your quality of life?
n=28
Excellent
25%
Very good
18%
Good
39%
Fair
14%
Poor
4%
Q10. Would you say your overall health is excellent, very good, good, fair or poor?
n=28
Excellent
14%
Very good
18%
Good
36%
Fair
21%
Poor
11%
Q11. Would you say your overall happiness is excellent, very good, good, fair or poor?
n=28
Excellent
14%
Very good
21%
Good
36%
Fair
18%
Poor
11%
Q12. Would you say your ability to socialize and/or spend time with other people is excellent, very good, good, fair or poor?
n=28
Excellent
21%
Very good
11%
Good
43%
Fair
11%
Poor
11%
Don't know
4%
Q13. Do you think you have enough of a say in decisions about your medical and day-to-day care?
n=28
Yes
64%
No
32%
Don't know
4%
C. Dementia Guidance
Topics of Interest
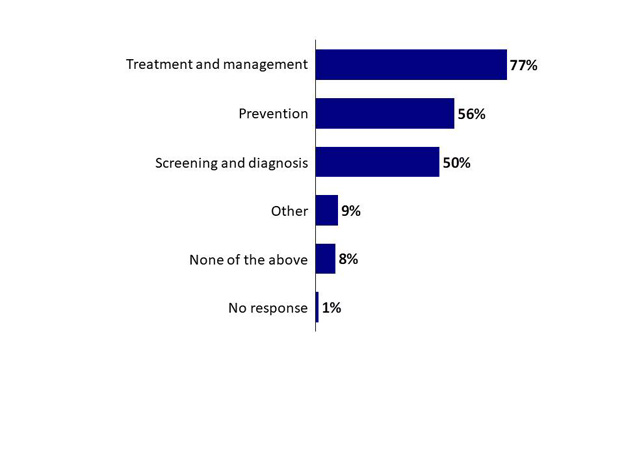
Over three-quarters (77%) of paid care providers said they have used guidance on treatment and management of dementia. Half or more used guidance on prevention (56%) or screening and diagnosis (50%).
Chart 3: Dementia Guidance Topics (Paid Care Providers)
Chart 3: Dementia Guidance Topics (Paid Care Providers) - Text Version
This chart of single bars shows the percentage of results for responses to twelve statements.
Respondents were asked: "Which of the following dementia guidance topics did you/do you use on a regular basis?"
Respondents selected:
Treatment and management: 77%
Prevention: 56%
Screening and diagnosis: 50%
Other: 9%
None of the above: 8%
No response: 1%
Base: Paid care providers (n=111)
Q16. Which of the following dementia guidance topics did you/do you use on a regular basis? (Paid care providers, n=111)
First Sought-After Source of Dementia Guidance
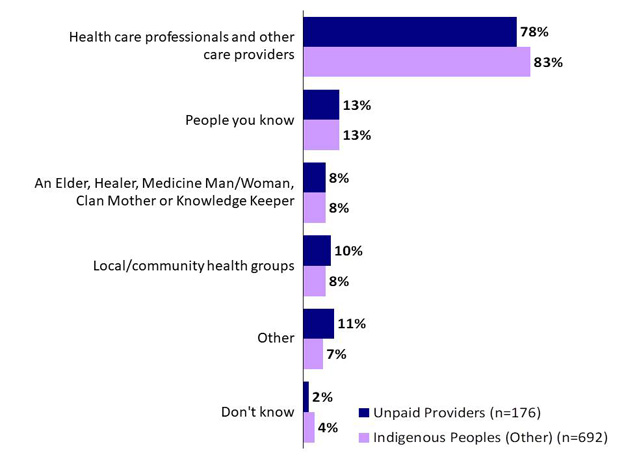
Most unpaid care providers (78%) said they would go to health care professionals and other care providers first to get recommendations and advice on dementia. Roughly one in ten would go to people they know (13%), local or community health groups (10%) or an Elder, Healer, Medicine Man/Women, Clan Mother, or Knowledge Keeper (8%).
As with the care provider respondent groups, most (83%) Indigenous Peoples (Other) said they would go to a health care professional and other care providers for recommendations and advice. About one in ten would go to people they know (13%), an Elder, Healer, Medicine Man/Women, Clan Mother, or Knowledge Keeper (8%), or local community or health groups (8%).
Chart 4: First Sought-After Source of Dementia Guidance
Chart 4: First Sought-After Source of Dementia Guidance - Text Version
This chart with single bars shows the percentage of results for responses to six statements across two groups: Unpaid Providers and Indigenous Peoples (Other).
Respondents were asked: "Who would you talk to first to get recommendations or advice about dementia?"
Respondents selected:
Health care professionals and other care providers
Group "Unpaid Providers": 78%
Group "Indigenous Peoples (Other)": 83%
People you know
Group "Unpaid Providers": 13%
Group "Indigenous Peoples (Other)": 13%
An Elder, Healer, Medicine Man/Woman, Clan Mother or Knowledge Keeper
Q17. Who would you talk to first to get recommendations or advice about dementia?
Métis respondents are more likely than First Nations or Inuit respondents to say they would talk to a health care professional (88%) first to get recommendations or advice about dementia. First Nations respondents are somewhat more likely than the other two Indigenous groups to identify an Elder, Healer, Medicine Man/Woman, Clan Mother or Knowledge Keeper (12%). There were no significant patterns of note among Inuit respondents.
Respondents in Manitoba and Saskatchewan[15] (91%) are more likely to say they would talk first to health care professionals. Those in Quebec (12%) are more likely to go to an Elder, Healer, Medicine Man/Women, Clan Mother or Knowledge Keeper. Those in Ontario (13%) are more apt to say local/community health groups.
Younger respondents (age 35 years and younger) are more likely than older counterparts to talk to people they know (21%) or an Elder, Healer, Medicine Man/Women, Clan Mother or Knowledge Keeper (18%) first to get recommendations or advice about dementia.
Those who identify as members of the LGBTQ2+ community are more likely to say they would talk to an Elder, Healer, Medicine Man/Women, Clan Mother or Knowledge Keeper (22%) or a local/community health group (25%), compared to those who identify as heterosexual.
Online Sources of Dementia Guidance
When looking for dementia guidance for Indigenous populations online, two-thirds (67%) of unpaid care providers would be likely or very likely to look to advocacy organizations for dementia. Over half (51%) would be likely or very likely to seek health care expert websites for dementia guidance. Regional or local Indigenous health authority websites would be a likely or very likely source for dementia guidance, according to 42% of unpaid care providers. Federal (40%) or provincial (43%) government websites were also viewed as likely or very likely sources by unpaid care providers.
About three-quarters (74%) of paid care providers said they would be likely or very likely to seek out websites of advocacy organizations for dementia when looking for guidance. About two-thirds (68%) would be likely or very likely to go to health care expert websites. Half or more would likely or very likely go to provincial or territorial government websites (53%), regional or local Indigenous health authority websites (52%), or federal government websites (50%).
Nearly two-thirds (64%) of the Indigenous Peoples (Other) said that they would likely or very likely look for websites of advocacy organizations for dementia when seeking guidance, while over half (53%) felt they would likely or very likely go to health care expert websites. Less than half said they would likely or very likely search online for dementia guidance using federal government websites (49%), provincial or territorial websites (43%), or regional or local Indigenous health authority websites (41%).
Other online resources noted across the three respondent groups who answered this question are Google, Alzheimer Society and other dementia-specific websites, Indigenous/culturally-specific websites, age-related sites, pages on Facebook, general health-related sites (e.g., WebMB, Mayo Clinic) and scientific/research sites.
Table 11: Online Sources of Dementia Guidance
If you were looking for dementia guidance/recommendations or advice online for Indigenous populations, how likely would you be to use each of the following types of websites?
Unpaid Providers
Paid Providers
Indigenous Peoples (Other)
Q18.a Federal government websites
n=176
n=111
n=693
Not at all/Not very
35%
23%
24%
Moderately
21%
26%
21%
Likely/Very likely
40%
50%
49%
Don't know/No response
5%
0%
5%
Q18.b Provincial/Territorial government websites
n=176
n=111
n=693
Not at all/Not very
28%
23%
25%
Moderately
25%
23%
27%
Likely/Very likely
43%
53%
43%
Don't know/No response
4%
2%
5%
Q18.c Regional/local Indigenous health authority websites
n=176
n=111
n=693
Not at all/Not very
36%
21%
28%
Moderately
16%
24%
23%
Likely/Very likely
42%
52%
41%
Don't know/No response
6%
3%
7%
Q18.d Advocacy organizations for dementia websites
n=176
n=111
n=693
Not at all/Not very
20%
10%
14%
Moderately
9%
15%
17%
Likely/Very likely
67%
74%
64%
Don't know / No response
3%
1%
5%
Q18.e Health care expert websites
n=176
n=111
n=693
Not at all/Not very
23%
14%
21%
Moderately
19%
16%
21%
Likely/Very likely
51%
68%
53%
Don't know / No response
7%
3%
5%
Among Indigenous respondents, Métis respondents are more likely than First Nations or Inuit respondents to say they would use advocacy organizations for dementia websites (74%). Inuit respondents were less likely than the other two Indigenous identity groups to indicate provincial or territorial government websites as a source (41% said they were unlikely to do use this source). The same is true for regional or local Indigenous health authority websites (46% said they would be unlikely to do so), advocacy organizations for dementia (28% said unlikely to use this source), or health experts (36% said they would be unlikely to do so). A higher proportion of First Nations also said they would be unlikely to use the websites of health experts (23%) compared with Métis respondents (17%).
Results for Métis respondents' stronger use of advocacy organization sites is likely related to education[16]. Those with a university (73%) or college (70%) education are more likely than those with a high school (53%) education to say they would seek an advocacy organization for dementia website. Métis respondents in the sample have a higher incidence of university education. Those who are high school educated are least likely to look in federal (31%) or provincial/territorial (30%) government websites
Urban residents are more likely to say they would look for regional/local health authority websites (47% versus 38% among rural residents), or advocacy groups websites (69% versus 62%). Rural residents are also less likely to say they would look for information on health care experts' websites (28%).
Regionally, respondents in Atlantic Canada are more likely to identify federal (67%) or provincial (67%) government websites. The same is true among residents of Manitoba and Saskatchewan (55% federal and 52% provincial government websites).
Those aged 45-54 years of age (52%) or 55-64 years of age (48%) are more apt to say they would go to a regional/local Indigenous health authority website, such as the British Columbia First Nations Health Authority. Those 65 years of age or older are less likely than younger respondents to go to a federal government website (34% said they would be unlikely to do so), provincial/territorial government websites (31% would be unlikely to do so), regional/local health authority sites (35% unlikely), or advocacy organization websites (22% unlikely).
Preferred Languages and Formats
Most respondents said that they would need dementia guidance tools in English, including Indigenous Peoples living with dementia (86%), unpaid care providers (91%), paid care providers (80%), and other Indigenous respondents (87%). French was the second-most mentioned language in each of the respondent groups, including Indigenous Peoples living with dementia (14%), unpaid care providers (10%), paid care providers (29%), and the Indigenous Peoples (Other) group (10%). The need for dementia guidance tools in many Indigenous languages was identified most often by paid care providers.
Table 12: Preferred Languages for Dementia Guidance Tools
Col1
People Living With Dementia
Unpaid Providers
Paid Providers
Indigenous Peoples (Other)
Q19 In what languages do you need dementia guidance tools for the populations you provide care or support to? / What is your preferred language for receiving health recommendations or advice?
n=28
n=176
n=111
n=693
English
86%
91%
80%
87%
French
14%
10%
29%
10%
Cree
11%
3%
12%
3%
Inuktitut (Nunavik)
11%
1%
4%
0%
Inuinnaqtun
7%
1%
1%
0%
Inuktitut (Nunatsiatvut)
7%
1%
3%
0%
Atikamekw
4%
1%
3%
0%
Dene
4%
1%
1%
1%
Michif
4%
1%
5%
1%
Mi'kmaq
4%
1%
3%
0%
Montagnais (Innu)
4%
1%
2%
0%
Ojibway
4%
1%
6%
0%
Plains Cree
4%
1%
5%
0%
Blackfoot
0%
1%
3%
0%
Inuktitut (Baffin)
0%
1%
4%
0%
Oji-Cree
0%
1%
5%
0%
Other language
7%
3%
14%
1%
No response
0%
1%
5%
2%
Métis respondents are somewhat more likely to cite English as their preferred language (92%), compared with First Nations (85%) or Inuit (80%). One in four Inuit respondents (27%) indicated Inuinnaqtun and Inuktitut (including Baffin, Nunatsiatvut, Nunavik and Inuinnaqtun).
Preferences for languages vary by region. The preference for English is more concentrated in the Territories (97%), Alberta (95%), Ontario (95%) and BC (93%) than it is in other regions. French is more popular in Quebec (59%). Twelve percent of Manitoba and Saskatchewan residents prefer Cree (12%). Inuktitut is far more prominently preferred in the territories, concentrated largely in Nunavut (13%).
Preference for French is higher among women (15% compared with 9% among men).
Preference for French is higher among those with a post-secondary level of education (15% to 17%) compared with those high school (4%).
Preference for French is also more likely among those under 35 years of age (20%) compared with older age cohorts.
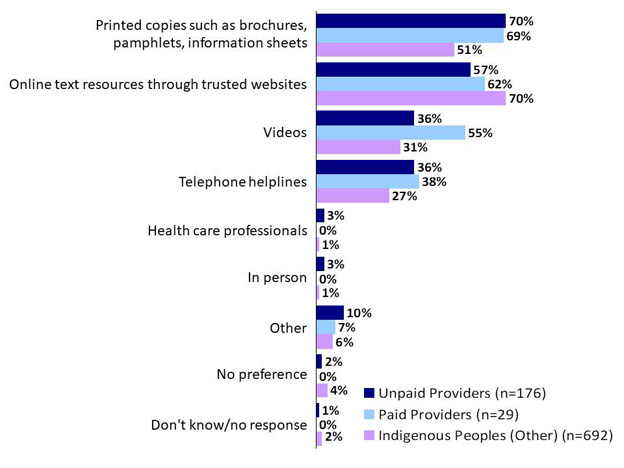
Most (70%) unpaid care providers said they would prefer printed copies such as brochures, pamphlets and information sheets when looking for health recommendations or advice. Over half (57%) would prefer online text resources through trusted websites. Over one-third would prefer videos (36%) or telephone helplines (36%).
Among paid care providers, most (69%) would prefer printed copies of health recommendation or advice, such as brochures, pamphlets and information sheets. Paid care providers would also prefer online text resources through trusted websites (62%), or videos (55%). Thirty-eight percent would prefer telephone helplines.
Respondents in the Indigenous Peoples (Other) identified their preferred source as online text resources through trusted websites (70%). About half (51%) would prefer printed copies such as brochures, pamphlets, and information sheets. Over one quarter would prefer videos (31%) or telephone helplines (27%).
Chart 5: Format Preferences
Chart 5: Format Preferences - Text Version
This chart with single bars shows the percentage of results for responses to nine statements across three groups: Unpaid Providers, Paid Providers, and Indigenous Peoples (Other).
Respondents were asked: "Which of the following format options do you prefer when looking for health recommendations or advice, for yourself or others?"
Respondents selected:
Printed copies such as brochures, pamphlets, information sheets
Q20. Which of the following format options do you prefer when looking for health recommendations or advice, for yourself or others?
Métis respondents are more likely to prefer online resources (74%) compared with the other two Indigenous groups (65% among First Nations and 53% among Inuit).
The pattern among Indigenous identity groups is likely explained by the education pattern[17]. Those with a university education (80%) are more likely than those with a high school education (53%) to prefer online resources through trusted websites, and the education profile is higher among Métis respondents.
Respondents in Manitoba and Saskatchewan (65%) or Atlantic Canada (67%) are more likely to prefer printed copies. Those in Atlantic Canada (44%) and Ontario (36%) are more likely to prefer telephone helplines.
Those aged 65 years of age or older are more likely than other age cohorts to prefer printed copies (65%), as well as telephone lines (36%).
Women were also more likely than men to express a preference for telephone helplines (32% versus 26%).
Those who identify as members of the LGBTQ2+ community (6%) are more likely than those who identify as heterosexual (0%) to say they prefer word of mouth.
Availability of Guidance for those Living with Dementia
Less than one-third (32%) of Indigenous Peoples living with dementia said they have found or received dementia recommendations or advice; 64% have not.
The majority of respondents living with dementia said they need recommendations or advice on the different types of dementia (57%), or non-pharmacological treatments and therapies (54%). Over one-third (36%) reported that they need recommendations or advice on the supports and services available for people living with dementia, while 29% said they would like information on pharmacological treatments. Fourteen per cent felt that they do not need any recommendations or advice[18].
Table 13: Availability of Guidance for Indigenous Persons Living with Dementia
Col1
People Living With Dementia
Q23 Have you found or received dementia recommendations or advice?
n=28
Yes
32%
No
64%
Don't know/No response
4%
Q22 Which topics, if any, do you need recommendations or advice on when it comes to dementia?
n=28
Different types of dementia
57%
Non-pharmacological treatments and therapies
54%
Supports and services for people living dementia
36%
Pharmacological treatment (i.e., medication)
29%
Other
4%
Do not need any recommendations or advice
14%
Don't know/No response
4%
Gaps in Dementia Guidance
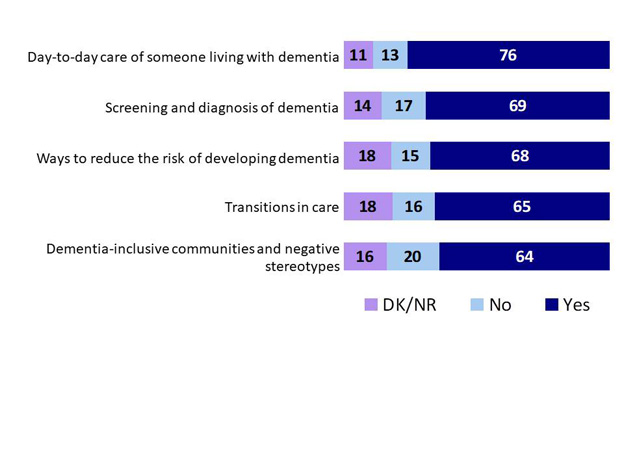
Among unpaid care providers, 76% said that there are gaps or barriers in dementia recommendations and advice for Indigenous populations in the day-to-day care of someone living with dementia. Roughly two-thirds reported that there are gaps in ways to reduce the risk of developing dementia (68%), in screening and diagnosis of dementia (69%), transitions in care (65%), or dementia-inclusive communities and negative stereotypes (64%).
Other gaps or barriers noted by unpaid care providers relate to guidance that is in Indigenous languages, or culturally specific to Indigenous Peoples, and issues related to access, particularly in remote communities.
Chart 6: Gaps in Recommendations and Advice – Unpaid Care Providers
Chart 6: Gaps in Recommendations and Advice – Unpaid Care Providers - Text Version
This stacked bar chart shows the percentage of results for responses to five statements across three categories: DK/NR, no, and yes.
Respondents were asked: "From your experience, are there any gaps/barriers with dementia recommendations and advice (i.e., guidance) for Indigenous populations in the following areas?1"
Respondents selected:
Day-to-day care of someone living with dementia
Category "DK/NR": 11%
Category "No": 13%
Category "Yes": 76%
Screening and diagnosis of dementia
Category "DK/NR": 14%
Category "No": 17%
Category "Yes": 69%
Ways to reduce the risk of developing dementia
Category "DK/NR": 18%
Category "No": 15%
Category "Yes": 68%
Transitions in care
Category "DK/NR": 18%
Category "No": 16%
Category "Yes": 65%
Dementia-inclusive communities and negative stereotypes
Category "DK/NR": 16%
Category "No": 20%
Category "Yes": 64%
Base: Unpaid providers (n=176)
Q27a-e. From your experience, are there any gaps/barriers with dementia recommendations and advice (i.e., guidance) for Indigenous populations in the following areas?[19] (Unpaid care providers, n=176)
Métis respondents are more likely to say there are gaps in recommendations on the ways to reduce the risk of developing dementia (80%) compared with First Nations (63%)[20] and Inuit (55%) respondents.
Those respondents who are between 55 and 64 years of age (89%) are more likely than other age groups (75% for those 45 to 54 and 65 or older and less than 70% for those under 45) to point to gaps in day-to-day care for someone living with dementia.
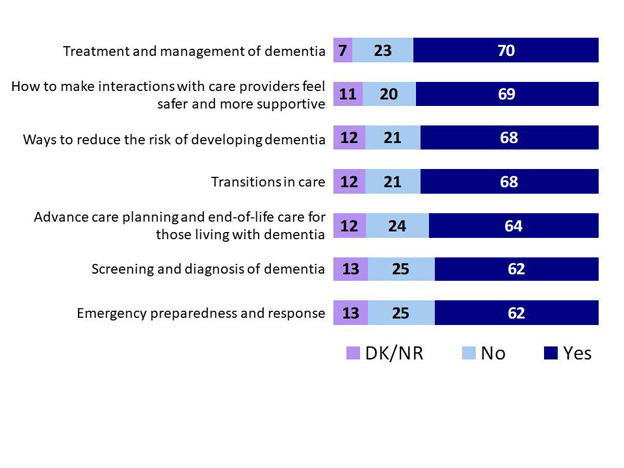
Among paid care providers, 70% felt there are gaps or barriers in dementia guidance for Indigenous populations in the treatment and management of dementia. Roughly two-thirds reported that there are gaps in ways to reduce the risk of developing dementia (68%), how to make interactions with care providers feel safer and more supportive (69%), or transitions in care (68%). Slightly fewer said that there are gaps in dementia guidance about advance care planning and end-of-life care for those living with dementia (64%), screening and diagnosis of dementia (62%), or emergency preparedness and response (62%).
Other gaps indicated by paid care providers relate to guidance in Indigenous languages, and/or grounded in Indigenous specific cultures, knowledge and spirituality.
Chart 7: Gaps in Recommendations and Advice – Paid Care Providers
Chart 7: Gaps in Recommendations and Advice – Paid Care Providers - Text Version
This stacked bar chart shows the percentage of results for responses to seven statements across four categories: DK/NR, no, and yes.
Respondents were asked: "From your experience, are there any gaps/barriers with dementia guidance for Indigenous populations in the following areas?"
Respondents selected:
Treatment and management of dementia
Category "DK/NR": 7%
Category "No": 23%
Category "Yes": 70%
How to make interactions with care providers feel safer and more supportive
Category "DK/NR": 11%
Category "No": 20%
Category "Yes": 69%
Ways to reduce the risk of developing dementia
Category "DK/NR": 12%
Category "No": 21%
Category "Yes": 68%
Transitions in care
Category "DK/NR": 12%
Category "No": 21%
Category "Yes": 68%
Advance care planning and end-of-life care for those living with dementia
Category "DK/NR": 12%
Category "No": 24%
Category "Yes": 64%
Screening and diagnosis of dementia
Category "DK/NR": 13%
Category "No": 25%
Category "Yes": 62%
Emergency preparedness and response
Category "DK/NR": 13%
Category "No": 25%
Category "Yes": 62%
Base: Paid care providers (n=111)
Q28a-g. From your experience, are there any gaps/barriers with dementia guidance for Indigenous populations in the following areas? (Paid care providers, n=111)
Challenges in Accessing Dementia Guidance
Several challenges or barriers were noted by paid care providers when accessing or using dementia guidance for Indigenous populations, including that guidance is not culturally appropriate or culturally safe (34%). Just over one in ten said that the guidance is too complicated to understand or communicate (15%), guidance is not in the right language (14%) or the guidance is too expensive to obtain (10%). Nearly one-quarter (23%) said they have not encountered any challenges in accessing or using dementia guidance for Indigenous populations.
Chart 8: Challenges in Accessing Dementia Guidance for Indigenous Populations – Paid Care Providers
Chart 8: Challenges in Accessing Dementia Guidance for Indigenous Populations – Paid Care Providers - Text Version
Indigenous Populations – Paid Care Providers
This chart of single bars shows the percentage of results for responses to ten statements.
Respondents were asked: "What challenges or barriers, if any, have you encountered when accessing or using dementia guidance for Indigenous populations?"
Respondents selected:
Guidance is not culturally appropriate or culturally safe for those to whom I provide care or support: 34%
I have not encountered any challenges or barriers: 23%
Guidance is too complicated to understand or communicate: 15%
Guidance is not in the right language: 14%
Guidance not readily available/not sure where to look/hard to access: 12%
Guidance is too expensive to obtain: 10%
Response related challenges with dementia, not Indigenous dementia guidance: 7%
N/A No need for dementia guidance: 3%
Other: 3%
Don't know/no response: 5%
Base: Paid care providers (n=111)
Q29. What challenges or barriers, if any, have you encountered when accessing or using dementia guidance for Indigenous populations? (Paid care providers, n=111)
Challenges or barriers were noted by about one in ten unpaid care providers when accessing or using dementia guidance for Indigenous populations, including advice that does not consider the cultural context (19%), advice that is too complicated to understand (16%), the advice is not in the right language (12%), the advice is too expensive to obtain (9%) or the advice comes from an untrustworthy source (7%). Nearly one-quarter (24%) said they have not encountered any challenges in accessing or using dementia guidance for Indigenous populations.
Chart 9: Challenges in Accessing Dementia Guidance for Indigenous Populations – Unpaid Care Providers
Chart 9: Challenges in Accessing Dementia Guidance for Indigenous Populations – Unpaid Care Providers - Text Version
This chart of single bars shows the percentage of results for responses to twelve statements.
Respondents were asked: "What challenges or barriers, if any, have you encountered when accessing or using dementia recommendations and advice for Indigenous populations?"
Respondents selected:
I have not encountered any challenges or barriers: 24%
Advice does not consider the cultural context: 19%
Response related challenges with dementia, not Indigenous dementia guidance: 18%
Advice is too complicated to understand or communicate: 16%
Advice is not in the right language: 12%
Advice is too expensive to obtain: 9%
Do not trust the source of the advice: 7%
N/A No need for dementia guidance: 5%
Guidance not readily available/not sure where to look/hard to access: 2%
Difficult to find the information: 1%
Other: 11%
Don't know/no response: 13%
Base: Unpaid providers (n=176)
Q29.b. What challenges or barriers, if any, have you encountered when accessing or using dementia recommendations and advice for Indigenous populations? (Unpaid care providers, n=176)
Those with a university education are more likely than those with a high school education to encounter most challenges, including advice that does not consider cultural context (31%), advice that is too complicated (29%), advice that is not in the right language (19%) and advice from a source they do not trust (16%).
Care providers and respondents in the Indigenous Peoples (Other) group were asked for suggested actions that would help to ensure that recommendations or advice about dementia are as culturally appropriate and culturally safe for Indigenous peoples as possible. There is a strong consensus among unpaid care providers and respondents in the Indigenous Peoples (Other) group that the development of dementia guidance should involve Indigenous communities and Elders in order to be culturally appropriate, and that training for care providers should be specific to Indigenous Peoples.
Among unpaid care providers, the most often noted benefit would come from training for care providers that is specific to Indigenous peoples living with dementia (81%). Almost as many also suggested that Indigenous involvement (79%), and more specifically the involvement of Indigenous Elders, Healers, and Knowledge Keepers (75%) would be helpful in developing culturally appropriate and safe guidance. About the same proportion also said that recommendations should reflect the distinct nature and lived experience of Indigenous Peoples (74%), consider the geography of the population (73%), and reflect the Indigenous perspectives of aging well (73%) in order to be culturally appropriate and safe. Just over two-thirds said that it would be helpful if recommendations recognized and responded to historical experiences of Indigenous Peoples (69%) and reflected the Indigenous ways of knowing (69%).
Most Indigenous Peoples (Other) (82%) also felt that it is important to involve Indigenous Peoples in the development of recommendations or advice to ensure the material is culturally appropriate and culturally safe for Indigenous populations. About three-quarters said that it would be helpful to involve Indigenous Elders, Healers, and Knowledge Keepers (77%), and that training for care providers should be specific to Indigenous Peoples living with dementia (75%). Slightly fewer said that it would be best if recommendations or advice reflected Indigenous perspectives of aging well (70%), considered the geography of the population (70%), and recognized and responded to historical experiences of Indigenous peoples (69%). About two-thirds believe that materials that reflect the distinct nature and lived experience of Indigenous Peoples (68%) and reflect Indigenous ways of knowing (66%) would help to make them culturally appropriate and safe.
Q30 In your opinion, what should be done to ensure that recommendations or advice about dementia are culturally appropriate and culturally safe for Indigenous populations?
n=176
n=692
Training for care providers specific to Indigenous Peoples living with dementia
81%
75%
Involve Indigenous Peoples in development
79%
82%
Involve Indigenous Elders, Healers, Medicine Men/Women, and/or Knowledge Keepers in development
75%
77%
Reflect the distinct nature and lived experience of First Nations, Inuit and Métis
74%
68%
Reflect Indigenous perspectives of aging well
73%
70%
Consider the geography of the population (e.g. urban, remote, northern)
73%
70%
Reflect Indigenous ways of knowing
69%
66%
Recognize and respond to historical experiences of Indigenous Peoples
69%
69%
Other
14%
7%
Nothing needs to be done
1%
2%
Don't know/No response
6%
5%
Among Indigenous respondents, Métis respondents are more likely than First Nations or Inuit to say recommendations should recognize and respond to historical experiences (74%), consider the geography of the population (77% compared with 69% among First Nations and 64% among Inuit) and provide training for care providers specific to Indigenous peoples (81% compared with 74% among First Nations and 69% among Inuit) to ensure that dementia recommendations or advice are culturally appropriate and culturally safe for Indigenous populations. Métis and Inuit respondents (78%) are more likely than First Nations (67%) to say recommendations should reflect Indigenous perspectives of aging well.
Perhaps related to this pattern among Métis respondents where the education profile is comparatively higher, those with a university education are more likely than those with a high school education to say advice should recognize and respond to historical experiences (77%), reflect Indigenous perspectives of aging well (81%). The same is true in terms of reflecting Indigenous ways of knowing (73%), considering the geography of the population (76%) and training for care providers should be specific to Indigenous Peoples (81%).
Those in British Columbia are more likely than those in other regions to say recommendations should involve Indigenous Elders, Healers, Medicine Men/Women and Knowledge Keepers (87%), consider the geography of the population (80%), and recognize and respond to historical experiences (78%). Those in Atlantic Canada are also more likely than others across the country to identify the need for training for care providers specific to Indigenous Peoples living with dementia (86%), as well as reflecting Indigenous perspectives of aging well (80%) and Indigenous ways of knowing (79%). Those in the Territories are more likely than others to emphasize the need to reflect the distinct nature and lived experience of First Nations, Métis and Inuit (79%).
Respondents aged 55 years of age or older are the most likely age cohorts to identify each recommendation.
Those who identify as members of the LGBTQ2+ community are more likely than those who identify as heterosexual to recommend each piece of advice (83% to 93% recommend each type of advice).
According to most paid care providers (84%), Indigenous Peoples should be involved in the development of dementia guidance to ensure it is culturally appropriate and culturally safe for Indigenous populations. Most also felt that guidance should involve Indigenous Elders, Healers, Knowledge Keepers (79%), include cultural competency training for care providers of Indigenous Peoples living with dementia (79%), recognize and respond to historical experiences of Indigenous Peoples (78%), or reflect Indigenous perspectives of aging well (78%). About three-quarters said that dementia guidance can be made culturally appropriate by reflecting Indigenous ways of knowing (76%), reflecting the distinct nature and lived experience of Indigenous peoples (76%), or considering the geography of the population (75%).
Table 15: Measures to Ensure Culturally Appropriate Dementia Guidance – Paid Care Providers
Q31 In your opinion, what should be considered to ensure dementia guidance is culturally appropriate and culturally safe for Indigenous populations?
n=111
Involve Indigenous Peoples in development
84%
Involve Indigenous Elders, Healers, Medicine Men/Women, and/or Knowledge Keepers in development
79%
Cultural competency training for care providers of Indigenous Peoples living with dementia
79%
Recognize and respond to historical experiences of Indigenous peoples
78%
Reflect Indigenous perspectives of aging well
78%
Reflect Indigenous ways of knowing
76%
Reflect the distinct nature and lived experience of First Nations, Inuit and Métis
76%
Consider the geography of the population (e.g. urban, remote, northern)
75%
Other
12%
Nothing needs to be done
2%
Don't know/No response
1%
Women are more likely than men to say dementia guidance should recognize and respond to historical experiences of Indigenous Peoples (84% of women, 66% of men) and reflect Indigenous perspectives of aging well (82% of women, 66% of men).
Urban residents are more likely than those in rural areas to point to the value of reflecting the distinct nature and lived experience of First Nations, Métis and Inuit (87% compared with 79% among rural respondents).
Paid care providers who are between 55 and 64 are more likely than other age groups to emphasize the need to involve Indigenous peoples in the development of dementia guidance (94%), reflect Indigenous perspectives of aging well (94%), and ways of knowing (91%), as well as distinct nature of and lived experience of First Nations, Métis and Inuit (91%), and the geography of the population (88%).
Nearly half (47%) of paid care providers felt that the dementia guidance and related tools they use to provide care and support to Indigenous Peoples living with dementia are culturally appropriate and culturally safe.
Chart 10: Use of Culturally Appropriate Guidance – Paid Care Providers
Chart 10: Use of Culturally Appropriate Guidance – Paid Care Providers - Text Version
This chart of single bars shows the percentage of results for responses to four statements.
Respondents were asked: "Do you feel that the dementia guidance and related tools that you have used or currently use to provide care and support to Indigenous peoples living with dementia are culturally appropriate and culturally safe?"
Respondents selected:
Yes: 47%
No: 33%
Don’t know: 17%
No response: 3%
Base: Paid care providers (n=111)
Q32. Do you feel that the dementia guidance and related tools that you have used or currently use to provide care and support to Indigenous peoples living with dementia are culturally appropriate and culturally safe? (Paid care providers, n=111)
Appendices
A. Methodological Details
The survey was developed cooperatively between the Ekos Research team and the Project Authority. The average time it took respondents to complete the survey was 15 minutes online and 23 minutes by telephone. The survey was pre-tested with 48 respondents (36 in English, 12 in French), including 25 collected online and 23 by telephone. Since no significant changes were made as a result of survey pre-testing, the cases were retained in the final sample. The survey was administered in English and French, as well as with an accessible link for those using a mobile phone or screen reading technology.
Respondents to the survey were 18 years of age and older and indicated themselves to be Indigenous, or a care provider[21] to one or more Indigenous persons living with dementia, in a paid or unpaid role, within the last 10 years[22]. The sample included individuals living in all provinces and territories. The survey sample was drawn from multiple sources, including from Probit panel, which is assembled using a random digit dial (RDD) process for sampling from a blended land-line cell-phone frame, which provides full coverage of Canadians with telephone access. The distribution of the recruitment process is meant to mirror the actual population in Canada (as defined by Statistics Canada). As such, our more than 120,000-member panel can be considered representative of the general public in Canada (meaning that the incidence of a given target population within our panel very closely resembles the public at large) and margins of error can be applied. We also relied on RDD of land and cell phones associated with geographic areas that include a First Nation reserve communities. Also, respondents who had previously completed a survey of the general public in the spring of 2020 participated if they were providing paid or unpaid care to an Indigenous person living with dementia in order to augment the cases in these two target groups. Further, a subset of respondents to a survey of dementia care providers, conduced in February-March 2021 participated if they were providing care to an Indigenous person. A small number of records were also completed as a result of a referral from another respondent within the sample. Initially there was an intent to target higher proportions of respondents who are Indigenous Peoples living with dementia, or those who have provided care to an Indigenous person with dementia, either in a paid or unpaid role. Because the incidence of finding these individuals within the sample sources used was much lower than expected, even including the sample sources described, the final sample includes a higher than expected proportion of respondents who are not living with dementia or caring for an Indigenous person living with dementia (i.e., Indigenous Peoples (Other). A total of 1,008 cases were completed between April 7 and June 21, 2021. The associated margin of error is up to plus or minus 3.1%, at a .95 confidence interval (i.e., 19 times out of 20). The margin of error for most target groups is between 5% and 10%.
Survey data collection adhered to the Government of Canada standard for public opinion research as well as all applicable industry standards. Ekos informed respondents of their rights under the Privacy Act and the Access to Information Act and ensured that those rights were protected throughout the research process. This included: informing respondents of the purpose of the research; identifying both the sponsoring department and the research supplier; informing respondents that their participation in the study is voluntary, and that the information provided would be administered according to the requirements of the Privacy Act.
Once the survey data was collected, the database was reviewed for data quality. Coding was also completed. Results for those Indigenous respondents who were not living with dementia, nor providing paid or unpaid care to someone with dementia (i.e., "Indigenous Peoples (Other)") were weighted to Indigenous population proportions for region, and age, as well as by Indigenous identity groupings (i.e., First Nations, Métis, Inuit). Data tables were created to isolate results for each of the four types of respondents (i.e., Indigenous Peoples living with dementia, those providing dementia care to one or more Indigenous Peoples in a paid role within the last 10 years, those providing dementia care to the same population in an unpaid role within the last 10 years, and Indigenous Peoples who are not living with dementia and have not provided dementia care within the last 10 years (Indigenous Peoples (Other)). Other demographic variables used in the analysis related to Indigenous populations include region, age, education, gender, and sexual orientation. Chi-square tests were used to compare subgroups to the remaining sample. Where there was a sizable degree of association between sub-groups, multivariate analysis was used to further explore which independent variable (i.e., sub-groups such as Indigenous identify group, education, age, location) was most likely the strongest association and possible explanation for other associations. For scaled items (e.g., knowledge rating, degree to which the respondent agrees with a statement) linear regression was used and where the responses were not linear (i.e., response categories, such as yes and no), logistic regression was used.
Response Rates and Non-Response Bias
The response rate for the survey was 11% (14% in the sample collected online and 10% in the sample collected by telephone), using the Government of Canada public opinion research standards for online and telephone research. Online, a total of 15,307 invitations were sent by email, of which 347 were returned as undeliverable, for a resulting valid sample of 14,960. A total of 245 interviews were completed, and 1,825 were found to be ineligible or within a quota that had been filled, resulting in a response rate of 13.8%.
In the telephone sample, a total of 39,031 telephone numbers were attempted. Of these, 8,143 telephone numbers were invalid, resulting in a remaining valid sample of 30,888. Of these, 2,361 were found to be out of scope (under 18) while 763 cases were completed, for a resulting response rate of 10.1%.
Table 16 – Response Rates
Col1
Online
Telephone
Total
Total Invited
15,307
39,031
54,338
Invalid
347
8,143
8,490
Total valid
14,960
30,888
45,848
Unresolved (U) – no response
12,846
21,144
33,990
In-scope responding units (IS) – Refusals, early break off
The unweighted sample of Indigenous Peoples who are not living with dementia and have not provided dementia care (i.e., "Indigenous Peoples (Other)") was compared with figures for Indigenous populations from Statistics Canada (2016 Census). Results suggest that there are similar sources of systematic sample bias in the survey, following patterns typically found in most general public surveys. The survey sample for this group was more educated than the Indigenous population, with 35% reporting university degrees, compared with the actual percentage of 9% found in the Indigenous population (2016 Census). There was also an under representation of those under 35 years of age (11% compared with 29% in the Indigenous population). There was also a slight underrepresentation of the Indigenous population in British Columbia and Manitoba and Saskatchewan , and a slight overrepresentation in Quebec.
B. Survey Questionnaire
Web Introduction
Online
Thank you for agreeing to complete this survey. The Government of Canada has hired Ekos Research to conduct a public opinion survey on behalf of the Public Health Agency of Canada.
Si vous préférez répondre au sondage en français, veuillez cliquer sur français. The purpose of the survey is to gather information from Indigenous peoples and care providers of Indigenous peoples on their experiences and perspectives related to dementia.
The survey takes 15 minutes to complete. Your participation is voluntary and your responses will be kept entirely confidential. It is being administered according to the requirements of the Privacy Act. Results will not be reported on an individual basis, but rolled into groups of 20 or more to preserve confidentiality. To view our privacy policy, click here.
The survey is registered with the Research Verification Service of the Canadian Insights Research Council (CIRC), if you wish to verify the legitimacy of this research.
A few points before beginning...
Please consider the questions and your answers carefully.
Definitions to some terms are provided. Hover your mouse over the underlined terms as you move through the survey in order to see the definition.
If you leave the survey before completing it, you can return to the survey URL later, and you will be returned to the page where you left off. Your answers up to that point in the survey will be saved.
If you have any questions about how to complete the survey, please call Ekos at 1-866-211-8881 or email us at online@ekos.com. Thank you in advance for your participation.
Telephone Introduction
Phone
Hello, my name is [name of interviewer] and I'm calling from Ekos Research Associates.
The Government of Canada has hired Ekos Research to conduct a public opinion survey on behalf of the Public Health Agency of Canada. The purpose of the survey is to gather information from Indigenous peoples and care providers of Indigenous peoples on their experiences and perspectives related to dementia.
Would you prefer to be interviewed in English or French?/ Préférez-vous répondre en français ou en anglais?
The survey will take 15 minutes to complete. Your participation is voluntary and completely confidential. Your answers will remain anonymous. Any information you provide will be administered in accordance with the Privacy Act, the Access to Information Act, and other applicable privacy laws. Results will not be reported on an individual basis, but rolled into groups of 20 or more to preserve confidentiality. The survey is registered with the Research Verification Service of the Canadian Insights Research Council (CIRC).
Continue: 1
Refuse (Thank & terminate): 9
Privacy
Phone
This call may be recorded for quality control or training purposes.
SC1
Non-01521 Respondent
Have you provided care or support to people living with dementia, through paid work (e.g. in the area of health care, psychological or support services, personal care services or emergency response services) in the past 10 years?
Yes: 1
No: 2
No response: 9
PSC2
01521 respondent
You participated in a survey in March and indicated that you provide care or support to people living with dementia, through your paid work, in the area of health care, pyschological or social support services, personal care services or emergency response services.
SC2
01521 respondent OR SC1 = Yes
Has this paid work ever included regular or occasional care or support to Indigenous peoples living with dementia?
Yes: 1
No: 2
No response: 9
SC3
Yes SC2
Are you currently providing ongoing paid care or support or was this in the past 10 years and you no longer do?
I am currently providing paid care or support: 1
I provided care or support in the past 10 years but no longer do: 2
No response: 9
PSC4
01521 respondent
You participated in a survey in March and indicated that you provide care or support to people living with dementia as an unpaid caregiver.
SC4 [1,8]
An unpaid caregiver may do a range of things to care for someone living with dementia.
Have you done any of the following in the last 10 years for a person living with dementia, without getting paid?
[Phone] Please read each item in the list and select each one that applies [Else] (Select all that apply)
Assisted with financial affairs: 1
Assisted with activities of daily living including cooking, cleaning, shopping for food and other essentials, bathing or dressing: 2
General health care and health monitoring including overseeing medication usage or help administering medication, setting up appointments: 3
Driving/escorting to health or other necessary appointments: 4
Monitoring their safety, or checking in on them: 5
Other types of care (Please specify): 77
None of these – no assistance to a person living with dementia: 98
Don't know: 97
Prefer not to answer: 99
SC5
SC4 does not = DK/PNA
At any point in the last 10 years was this unpaid care or support provided to an Indigenous person living with dementia?
Yes: 1
No: 2
No response: 9
SC6
SC5 = Yes
Are you currently providing ongoing unpaid care or support or was this in the past 10 years and you no longer do?
I am currently providing care or support: 1
I provided care or support in the past 10 years but no longer do: 2
No response: 9
SC7
Are you an Indigenous person living with dementia?
Yes: 1
No: 2
No response: 9
CALCS1 [1,5]
Calculation:
If paid in last 10 years (SC1) or 01521 Respondent (SAGE_V2) and paid to care for indigenous people with dementia (SC2) and paid in last 10 years (SC3) return "paid";
If selected any SC4 answer and provide care for indigenous people with dementia (SC5) currently (SC6) return "current unpaid";
If do not currently provide care, but have in last 10 years (SC6) return "unpaid, last 10 years";
If selected any SC4 answer and did not provide care for indigenous people with dementia in last 10 years (SC5) return "unpaid, over 10 years ago";
If an Indigenous person living with dementia return "an Indigenous person living with dementia";
If none of the above, return "None"
I am an Indigenous person living with dementia: 1
I am currently providing care to an Indigenous person living with dementia, in an unpaid role.: 2
In the past 10 years, I used to provide care to an Indigenous person living with dementia in an unpaid role.: 3
More than 10 years ago, I provided care to an Indigenous person living with dementia in an unpaid role.: 4
I am currently or have in the past 10 years been paid to provide care to and/or support Indigenous peoples living with dementia.: 5
None of the above: 6
No response: 7
S1B
Paid care
Which of the following best describes your paid role?
[Phone] (Interviewer: Read list)
Providing first response services (e.g. police, paramedics, firefighters, etc.): 1
Providing primary health care (e.g. primary care providers): 2
Providing specialized dementia care (e.g. specialists such as geriatrician, psychiatrist): 3
Providing paid general care for a person living with dementia (e.g. personal support worker, home care support, etc.): 4
Other (specify): 77
No response: 99
S1C
Unpaid care
Thinking of the most recent month you provided unpaid care to an Indigenous person living with dementia, what would you say is the average number of hours per week you provided the unpaid care?
Hours : 77
Don't know: 98
Prefer not to answer: 99
S4
Are you First Nations (North American Indian), Métis, or Inuk (Inuit)?
First Nations: 1
Métis: 2
Inuk (Inuit): 3
Other (specify): 77
CALCS1 not = 1
Not Indigenous: 5
No response: 99
CALCSCREENOUT
Calculation : Discontinue survey if CALCS1=1, 4, 6 or 7 (PWD or GP or No response), and S4=5, 9
Terminate: 1
Continue: 2
S4B
S4 = First Nations
Do you live in an Indigenous or First Nation community for at least 6 months of the year?
Yes: 1
No: 2
Prefer not to answer: 99
Q4
CALCS1=5 Paid Care
How frequently did you provide or do you provide paid care or support to Indigenous peoples living with dementia?
Never: 1
Daily: 2
At least once a week: 3
Once a month: 4
Less than once a month: 5
No response: 9
CALCSCREENOUTB
Calculation : Q4 = 1 never, no longer categorized as paid care provider. If not Indigenous, discontinue survey, unless also unpaid care
Terminate: 1
Continue: 2
Q1A
CALCS1 not=1 not PLWD
How knowledgeable about the following dementia topics would you say you [Phone] are on a scale from 1 - not at all knowledgeable; 2 – a little knowledgeable; 3 – somewhat knowledgeable; 4 – moderately knowledgeable; 5 - very knowledgeable? [Else] are?
Signs and symptoms of dementia
Not at all knowledgeable: 1
A little knowledgeable: 2
Somewhat knowledgeable: 3
Moderately knowledgeable: 4
Very knowledgeable: 5
Don't know/No response: 9
Q1B
CALCS1 not=1 not PLWD
Ways to reduce the risk of developing dementia
Not at all knowledgeable: 1
A little knowledgeable: 2
Somewhat knowledgeable: 3
Moderately knowledgeable: 4
Very knowledgeable: 5
Don't know/No response: 9
Q1C
CALCS1 not=1 not PLWD
How to make a community more welcoming and supportive of people living with dementia
Not at all knowledgeable: 1
A little knowledgeable: 2
Somewhat knowledgeable: 3
Moderately knowledgeable: 4
Very knowledgeable: 5
Don't know/No response: 9
Q2 [1,3]
CALCS1 not=1 not PLWD
What are the first three things that come to mind when thinking about what factors increase your chances of developing dementia?
[Phone] (Interviewer: Do not read - accept up to 3)
Hypertension/high blood pressure: 1
Harmful alcohol use: 2
Lack of physical activity: 3
Diet lacking in healthy foods: 4
Sleep disruption (e.g. sleep apnea): 5
Smoking: 6
Diabetes: 7
High cholesterol: 8
Loneliness/social isolation: 9
Fewer years of formal education: 10
Too much screen time: 11
Air pollution: 12
Hearing loss: 13
Unsafe exposure to the sun: 14
Other (specify): 77
Nothing comes to mind: 15
Don't know/No response: 99
Q3A
CALCS1 not=1 not PLWD; Q3D/E, Unpaid, GP
To what extent do you agree or disagree with the [Phone] following on a scale from 1-5? (Interviewer: read scale - 1 - strongly disagree; 2 – disagree; 3 – neither; 4 – agree; 5 - strongly agree, don't know)[Else] following?
People living with dementia are sometimes able to continue working for years after the onset of symptoms
Strongly disagree: 1
Disagree: 2
Neither: 3
Agree: 4
Strongly agree: 5
Don't know/No response: 9
Q3B
CALCS1 not=1 not PLWD; Q3D/E, Unpaid, GP
People living with dementia generally face a lower quality of life than people without dementia
Strongly disagree: 1
Disagree: 2
Neither: 3
Agree: 4
Strongly agree: 5
Don't know/No response: 9
Q3C
CALCS1 not=1 not PLWD; Q3D/E, Unpaid, GP
People in my community are knowledgeable, respectful and supportive of people living with dementia
Strongly disagree: 1
Disagree: 2
Neither: 3
Agree: 4
Strongly agree: 5
Don't know/No response: 9
Q3D
CALCS1 not=1 not PLWD; Q3D/E, Unpaid, GP
I worry about the possibility of personally developing dementia
Strongly disagree: 1
Disagree: 2
Neither: 3
Agree: 4
Strongly agree: 5
Don't know/No response: 9
Q3E
CALCS1 not=1 not PLWD; Q3D/E, Unpaid, GP
I worry about the possibility of someone close to me developing dementia
Strongly disagree: 1
Disagree: 2
Neither: 3
Agree: 4
Strongly agree: 5
Don't know/No response: 9
Q5A
CALCS1=2-3, 5 paid and unpaid care
To what extent is your community each of the [Phone] following on a scale from 1-5? Interviewer: read scale - (1-Not at all, 2-Limited extent, 3-Moderate extent, 4-Considerable extent and 5 - Great extent)[Else] following?
The physical environment of my community is supportive of people living with dementia (e.g. housing, transportation)
Not at all: 1
Limited extent: 2
Moderate extent: 3
Considerable extent: 4
Great extent: 5
Don't know/No response: 9
Q5B
CALCS1=2-3, 5 paid and unpaid care
There are sufficient resources (e.g. services, facilities) to support people living with dementia and their caregivers in my community
Not at all: 1
Limited extent: 2
Moderate extent: 3
Considerable extent: 4
Great extent: 5
Don't know/No response: 9
Q6 [1,9]
CALCS1 = 4, 6 GP
Do you know anyone who is living/has lived with dementia?
(Select all that apply)
My spouse/partner: 1
My parent(s): 2
Extended family member(s): 3
Friend(s), neighbour(s), or colleague(s) from work: 4
Community member(s): 5
Elder(s) and/or Knowledge Keeper(s): 6
Other (please specify): 77
No one 98
Don't know/No response: 99
Q7 [1,3]
CALCS1=2-3, 5 paid and unpaid care
Thinking about the Indigenous peoples living with dementia who you have provided care to, what are the top three factors you believe contribute the most to their quality of life?
[Phone] (Interviewer: Do not read - accept up to 3)
Good physical health: 1
Good mental health: 2
Good spiritual health: 3
Having frequent (weekly or more often) support and visits with family and friends: 4
Feeling like they belong to a community: 5
Having a sense of purpose, that their life is useful: 6
Being able to stay in their own home as long as possible: 7
Being independent in their daily living needs (e.g., preparing their own food, laundry, shopping): 8
Living with loved ones (family and friends): 9
Being able to be out on the land: 10
Being able to express their culture through language and other ways: 11
Not having to worry about money: 12
Being able to move around their community as much as they want: 13
Having enough access to health care services: 14
Other (specify): 77
Don't know: 98
No response: 99
Q8 [1,3]
CALCS1=1 PLWD
Different people value things in different ways. In other words, some people think some things are important that others may not. This question explores what you value and what is important to you. What are three things that are most important for you in having a good quality of life?
(Select all that apply) [Phone] (Interviewer: Do not read - accept up to 3)
Good physical health: 1
Good mental health: 2
Good spiritual health: 3
Having frequent (weekly or more often) support and visits with family and friends: 4
Feeling like I belong to a community: 5
Having a sense of purpose, that my life is useful: 6
Being able to stay in my own home as long as possible: 7
Being independent in my daily living needs (e.g., preparing my own food, laundry, shopping): 8
Living with loved ones (family and friends): 9
Being able to be out on the land: 10
Being able to express my culture through language and other ways: 11
Not having to worry about money: 12
Being able to move around my community as much as I want: 13
Having enough access to health care services: 14
Other (specify): 77
Don't know: 98
No response: 99
Q9
CALCS1=1 PLWD
How would you rate your quality of life?
[Phone] (Interviewer: Read list)
Excellent: 1
Very good: 2
Good: 3
Fair: 4
Poor: 5
Don't know: 98
No response: 99
Q10
CALCS1=1 PLWD
Would you say your overall health is excellent, very good, good, fair or poor?
[Phone] (Interviewer: Read list)
Excellent: 1
Very good: 2
Good: 3
Fair: 4
Poor: 5
Don't know: 98
No response: 99
Q11
CALCS1=1 PLWD
Would you say your overall happiness is excellent, very good, good, fair or poor?
[Phone] (Interviewer: Read list)
Excellent: 1
Very good: 2
Good: 3
Fair: 4
Poor: 5
Don't know: 98
No response: 99
Q12
CALCS1=1 PLWD
Would you say your ability to socialize and/or spend time with other people is excellent, very good, good, fair or poor?
[Phone] (Interviewer: Read list)
Excellent: 1
Very good: 2
Good: 3
Fair: 4
Poor: 5
Don't know: 98
No response: 99
Q13
CALCS1=1 PLWD
Do you think you have enough of a say in decisions about your medical and day-to-day care?
Yes: 1
No: 2
Don't know: 98
No response: 99
Q14
CALCS1=2-4, 6 GP and Unpaid care
Have you taken steps to reduce your own risk of developing dementia?
Yes: 1
No: 2
No response: 99
Q15 [1,8]
Q14=no
What has prevented you from taking steps to reduce your risk of developing dementia?
(Select all that apply) [Phone] (Interviewer: Do not read)
I am not aware of what to do to reduce my risk: 1
It is too hard to make the changes: 2
I am not sure it will make a difference: 3
The advice doesn't seem relevant to my situation: 4
Resources are not available in my community: 5
Other (specify): 77
Don't know: 98
No response: 99
Q16 [1,6]
CALCS1=5 Paid care
Dementia guidance includes recommendations and advice on various topics such as prevention, diagnosis, treatment, [hover="A negative stereotype often influenced by public attitudes, misconceptions and fear. Stigmatizing language and behaviours related to dementia may include: making assumptions about a person's abilities; ageism or implying that dementia is a normal part of aging; and dementia-related jokes."] stigma reduction, and [hover="Communities that allow people living with dementia and caregivers to optimize their health and wellbeing; live as independently as possible; be understood and supported; safely navigate and access their local communities; and maintain their social networks."] dementia-inclusive communities that are based on evidence.
Which of the following dementia guidance topics did you or do you use on a regular basis?
(Select all that apply) [Phone] Interviewer: read each one and accept yes/no for each
Prevention (i.e. actions taken to promote and preserve health and to reduce the chance of developing dementia): 1
Screening and diagnosis (i.e. testing for the presence/absence of a condition (screening) and the identification of the nature of the condition (diagnosis)): 2
Treatment and management (i.e. provision of services such as medications, devices, counselling, etc.): 3
Other (specify): 77
None of the above: 97
No response: 99
Q17 [1,6]
CALCS1=2-4, 6 GP and Unpaid care
Dementia recommendations or advice can include various topics such as prevention, diagnosis, treatment, [hover="A negative stereotype often influenced by public attitudes, misconceptions and fear. Stigmatizing language and behaviours related to dementia may include: making assumptions about a person's abilities; ageism or implying that dementia is a normal part of aging; and dementia-related jokes."] stigma reduction, and [hover="Communities that allow people living with dementia and caregivers to optimize their health and wellbeing; live as independently as possible; be understood and supported; safely navigate and access their local communities; and maintain their social networks."] dementia-inclusive communities that are based on evidence.
Who would you talk to first to get recommendations or advice about dementia?
[Phone] (Interviewer: Do not read)
Health care professionals and other care providers: 1
People you know (friends and family): 2
An Elder, Healer, Medicine Man/Woman, Clan Mother or Knowledge Keeper: 3
Local/community health groups: 4
Other (specify): 77
Don't know: 98
Q18A
CALCS1 not=1 Exclude PLWD
If you were looking for [CALCS1 = 5 and Q4 not = 1] dementia guidance [Else] dementia recommendations or advice online for Indigenous populations, how likely would you be to use each of the following types of [Phone] websites on a scale where 1- Not at all likely, 2-Not very likely, 3-Moderately likely, 4-Likely and 5- Very likely? [Else] websites?
Federal government websites (e.g. First Nations and Inuit Health Branch (Indigenous Services Canada), Health Canada, Public Health Agency of Canada)
Not at all likely: 1
Not very likely: 2
Moderately likely: 3
Likely: 4
Very likely: 5
Don't know/No response: 9
Q18B
CALCS1 not=1 Exclude PLWD
Provincial/Territorial government websites (health department websites)
Not at all likely: 1
Not very likely: 2
Moderately likely: 3
Likely: 4
Very likely: 5
Don't know/No response: 9
Q18C
CALCS1 not=1 Exclude PLWD
Regional/local Indigenous health authority websites (e.g. British Columbia First Nations Health Authority)
Not at all likely: 1
Not very likely: 2
Moderately likely: 3
Likely: 4
Very likely: 5
Don't know/No response: 9
Q18D
CALCS1 not=1 Exclude PLWD
Advocacy organizations for dementia websites (e.g. Alzheimer Society)
Not at all likely: 1
Not very likely: 2
Moderately likely: 3
Likely: 4
Very likely: 5
Don't know/No response: 9
Q18E
CALCS1 not=1 Exclude PLWD
Health care expert websites
Not at all likely: 1
Not very likely: 2
Moderately likely: 3
Likely: 4
Very likely: 5
Don't know/No response: 9
Q18F [1,3]
CALCS1 not=1 Exclude PLWD
Are there any other types of websites you would go to?
Yes (please specify): 77
No: 98
Don't know/No response: 99
Q19 [1,19]
[CALCS1 = 5 and Q4 not = 1] In what languages do you need dementia guidance tools for the populations you provide care or support to? [Else] What is your preferred language for receiving health recommendations or advice (for example, from a health care provider or in a written resource, for yourself or to share with others)?
(Select all that apply) [Phone] (Interviewer: Do not read)
Atikamekw: 1
Blackfoot: 2
Cree: 3
Dene: 4
English: 5
French: 6
Inuinnaqtun: 7
Inuktitut (Baffin): 8
Inuktitut (Nunatsiatvut): 9
Inuktitut (Nunavik): 10
Michif: 11
Mi'kmaq: 12
Montagnais (Innu): 13
Ojibway: 14
Oji-Cree: 15
Plains Cree: 16
Other language (specify): 77
No response: 99
Q20 [1,7]
Which of the following format options do you prefer when looking for health recommendations or advice, for yourself or others?
(Select all that apply) [Phone] (Interviewer: Read list)
Printed copies such as brochures, pamphlets, information sheets: 1
Online text resources through trusted websites: 2
Videos (rather than text) available online: 3
Telephone helplines: 4
Other (specify): 77
No preference 98
Don't know/No response: 99
Q21 [1,10]
CALCS1=1 PLWD
Would you prefer to get recommendations or advice on dementia through...?
(Select all that apply) [Phone] (Interviewer: Read 1 at a time)
Video or telephone call with a care provider: 1
In-person conversation with a care provider (with physical distancing precautions in place): 2
Printed documents: 3
Online web chat: 4
Educational videos to watch online: 5
Telephone helplines: 6
Radio: 7
Other (specify): 77
Do not want any recommendations or advice: 97
No preference: 98
Don't know/No response: 99
Q22 [1,7]
CALCS1=1 PLWD
Which topics, if any, do you need recommendations or advice on when it comes to dementia?
(Select all that apply) [Phone] Interviewer read: I'm going to read the following list, please let me know if you would like me to repeat anything or if you need more information about the topics I am going to share Please stop me when I get to a topic you need advice on (Read 1 at a time)
Pharmacological treatment (i.e. medication): 1
Non-pharmacological treatments and therapies (e.g., physical therapy, lifestyle changes, music and art therapy): 2
Different types of dementia (e.g., Alzheimer's disease, vascular dementia, frontotemporal dementia): 3
Supports and services for people living dementia: 4
Other (specify): 77
Do not need any recommendations or advice: 98
Q23
CALCS1=1 PLWD
Dementia recommendations or advice can include various topics such as prevention, diagnosis, treatment, [hover="A negative stereotype often influenced by public attitudes, misconceptions and fear. Stigmatizing language and behaviours related to dementia may include: making assumptions about a person's abilities; ageism or implying that dementia is a normal part of aging; and dementia-related jokes."] stigma reduction, and [hover="Communities that allow people living with dementia and caregivers to optimize their health and wellbeing; live as independently as possible; be understood and supported; safely navigate and access their local communities; and maintain their social networks."] dementia-inclusive communities that are based on evidence.
Have you found or received dementia recommendations or advice?
Yes: 1
No: 2
Don't know/No response: 99
Q24
CALCS1=1 PLWD and Q23=1 yes
Were you able to follow it?
Yes, completely: 1
Yes, somewhat: 2
No: 3
Don't know/No response: 99
Q25 [1,7]
CALCS1=1 PLWD and Q24=2,3
Why were you not able to follow the recommendations or advice?
(Select all that apply) [Phone] Interviewer read: I'm going to read the following list, please let me know if you would like me to repeat anything and please stop me when I get to one problem that you have had (Read list)
Not available in my preferred language which made it harder to understand: 1
Does not consider my cultural context / not adapted to my situation: 2
Too expensive to take the recommended steps: 3
I didn't trust the source of the advice: 4
Other (specify): 77
Don't know/No response: 99
Q26 [1,7]
Q1=1 PLWD and Q24=1
What made it possible for you to follow the recommendations or advice?
(Select all that apply) [Phone] Interviewer read: I'm going to read the following list, please let me know if you would like me to repeat anything and please stop me when I get to one feature that made the advice easier to follow (Read list)
In my preferred language which made it easier to understand: 1
Considered by cultural context / adapted to my situation: 2
The recommended steps were affordable: 3
I trusted the source of advice: 4
It was easy for me to follow the recommended advice: 5
Other (specify): 77
Don't know/No response: 99
Q27A
CALCS1= 2, 3 Unpaid care
From your experience, are there any gaps/barriers with dementia recommendations and advice (i.e. guidance) for Indigenous populations in the following areas?
Ways to reduce the risk of developing dementia
Yes: 1
No: 2
Don't know/No response: 9
Q27B
CALCS1= 2, 3 Unpaid care
From your experience, are there any gaps/barriers with dementia recommendations and advice (i.e. guidance) for Indigenous populations in the following areas?
Screening and diagnosis of dementia
Yes: 1
No: 2
Don't know/No response: 9
Q27C
CALCS1= 2, 3 Unpaid care
From your experience, are there any gaps/barriers with dementia recommendations and advice (i.e. guidance) for Indigenous populations in the following areas?
Day-to-day care of someone living with dementia
Yes: 1
No: 2
Don't know/No response: 9
Q27D
CALCS1= 2, 3 Unpaid care
From your experience, are there any gaps/barriers with dementia recommendations and advice (i.e. guidance) for Indigenous populations in the following areas?
[hover="Communities that allow people living with dementia and caregivers to optimize their health and wellbeing; live as independently as possible; be understood and supported; safely navigate and access their local communities; and maintain their social networks."] Dementia-inclusive communities and negative stereotypes (i.e. [hover="A negative stereotype often influenced by public attitudes, misconceptions and fear. Stigmatizing language and behaviours related to dementia may include: making assumptions about a person's abilities; ageism or implying that dementia is a normal part of aging; and dementia-related jokes."] stigma)
Yes: 1
No: 2
Don't know/No response: 9
Q27E
CALCS1= 2, 3 Unpaid care
From your experience, are there any gaps/barriers with dementia recommendations and advice (i.e. guidance) for Indigenous populations in the following areas?
Transitions in care
Yes: 1
No: 2
Don't know/No response: 9
Q27F [1,3]
CALCS1= 2, 3 Unpaid care
Are there any other gaps/barriers with dementia recommendations and advice (i.e. guidance) for Indigenous populations?
Yes (please specify): 77
No: 98
Don't know/No response: 99
Q28A
CALCS1= 5 Paid care
From your experience, are there any gaps/barriers with dementia guidance for Indigenous populations in the following areas?
Ways to reduce the risk of developing dementia
Yes: 1
No: 2
Don't know/No response: 9
Q28B
CALCS1= 5 Paid care
Screening and diagnosis of dementia
Yes: 1
No: 2
Don't know/No response: 9
Q28C
CALCS1= 5 Paid care
Treatment and management of dementia
Yes: 1
No: 2
Don't know/No response: 9
Q28D
CALCS1= 5 Paid care
Advance care planning and end-of-life care for those living with dementia
Yes: 1
No: 2
Don't know/No response: 9
Q28E
CALCS1= 5 Paid care
How to make interactions with care providers feel safer and more supportive
Yes: 1
No: 2
Don't know/No response: 9
Q28F
CALCS1= 5 Paid care
Emergency preparedness and response (e.g. fire, flood, earthquake, pandemic, etc.)
Yes: 1
No: 2
Don't know/No response: 9
Q28G
CALCS1= 5 Paid care
Transitions in care
Yes: 1
No: 2
Don't know/No response: 9
Q28H [1,3]
CALCS1= 5 Paid care
Are there any other gaps/barriers with dementia guidance for Indigenous populations?
Yes (please specify): 77
No: 98
Don't know/No response: 99
Q29 [1,8]
CALCS1=5 Paid caregivers
What challenges or barriers, if any, have you encountered when accessing or using dementia guidance for Indigenous populations?
(Select all that apply) [Phone] (Interviewer: Do not read)
Guidance is not in the right language: 1
Guidance is not culturally appropriate or culturally safe for those to whom I provide care or support: 2
Guidance is too expensive to obtain: 3
Guidance is too complicated to understand or communicate: 4
Other (specify): 77
I have not encountered any challenges or barriers: 5
Don't know/No response: 99
Q29B [1,8]
CALCS1= 2, 3 Unpaid care
What challenges or barriers, if any, have you encountered when accessing or using dementia recommendations and advice for Indigenous populations?
(Select all that apply) [Phone] (Interviewer: Do not read)
Advice is not in the right language: 1
Advice does not consider the cultural context for those to whom I provide care or support: 2
Advice is too expensive to obtain: 3
Advice is too complicated to understand or communicate: 4
Do not trust the source of the advice: 6
Other (specify): 77
I have not encountered any challenges or barriers: 5
Don't know/No response: 99
Q30 [1,11]
CALCS1=2-4, 6 GP and Unpaid care
In your opinion, what should be done to ensure that recommendations or advice about dementia are [hover="Culturally appropriate and safe recommendations and advice acknowledge and include an understanding of cultural differences (e.g. Indigenous perspectives of aging well), personal experiences, norms and power imbalances in the health care system to help make health-related advice easier and safer for Indigenous populations."] culturally appropriate and culturally safe for Indigenous populations?
(Select all that apply) [Phone] Read list and accept yes/no for each one
Involve Indigenous peoples in development: 1
Involve Indigenous Elders, Healers, Medicine Men/Women, and/or Knowledge Keepers in development: 2
Recognize and respond to historical experiences of Indigenous peoples: 3
Reflect Indigenous perspectives of aging well: 4
Reflect Indigenous ways of knowing: 5
Reflect the distinct nature and lived experience of First Nations, Inuit and Métis: 6
Consider the geography of the population (e.g. urban, remote, northern): 7
Training for care providers specific to Indigenous peoples living with dementia: 8
Other (specify): 77
Nothing needs to be done: 98
Don't know/No response: 99
Q31 [1,11]
CALCS1=5 Paid care
In your opinion, what should be considered to ensure dementia guidance is [hover="Culturally appropriate and safe recommendations and advice acknowledge and include an understanding of cultural differences (e.g. Indigenous perspectives of aging well), personal experiences, norms and power imbalances in the health care system to help make health-related advice easier and safer for Indigenous populations."] culturally appropriate and culturally safe for Indigenous populations?
(Select all that apply) [Phone] (Interviewer: Read list and obtain yes/no for each one)
Involve Indigenous peoples in development: 1
Involve Indigenous Elders, Healers, Medicine Men/Women, and/or Knowledge Keepers in development: 2
Recognize and respond to historical experiences of Indigenous peoples: 3
Reflect Indigenous perspectives of aging well: 4
Reflect Indigenous ways of knowing: 5
Reflect the distinct nature and lived experience of First Nations, Inuit and Métis: 6
Consider the geography of the population (e.g. urban, remote, northern): 7
Cultural competency training for care providers of Indigenous people living with dementia: 8
Other (specify): 77
Nothing needs to be done 98
Don't know/No response: 99
Q32
CALCS1=5 Paid care
Do you feel that the dementia guidance and related tools that you have used or currently use to provide care and support to Indigenous peoples living with dementia are [hover="Culturally appropriate and safe recommendations and advice acknowledge and include an understanding of cultural differences (e.g. Indigenous perspectives of aging well), personal experiences, norms and power imbalances in the health care system to help make health-related advice easier and safer for Indigenous populations."] culturally appropriate and culturally safe?
Yes: 1
No: 2
Don't know: 98
No response: 99
QPROV
Which province or territory do you live in?
Alberta: 1
British Columbia: 2
Manitoba: 3
New Brunswick: 4
Newfoundland and Labrador: 5
Northwest Territories: 6
Nova Scotia: 7
Nunavut: 8
Ontario: 9
Prince Edward Island: 10
Quebec: 11
Saskatchewan: 12
Yukon: 13
No response: 99
QAGE
Which of the following age categories do you belong to?
CALCS1 not = 1
18-24 years: 1
CALCS1 not = 1
25-34 years: 2
CALCS1 not = 1
35-44 years: 3
45-54 years: 4
55-64 years: 5
65-69 years: 6
70-74 years: 7
75-79 years: 8
80-84 years: 9
85 years and older: 10
No response: 99
QSEX
What is your gender?
Male: 1
Female: 2
Another gender (specify): 77
No response: 99
QSEXB
CALCS1 not 1 excludes PLWD
Do you consider yourself to be...?
[Phone] (Interviewer: Read list)
Heterosexual (straight): 1
Homosexual (lesbian or gay): 2
Bisexual: 3
Two-spirit: 4
Other (specify): 77
No response: 99
QEDUC
What is the highest level of education that you have completed?
[Phone] (Interviewer: Do not read)
8th grade or less (equivalent to secondary II in Quebec): 1
Some high school: 2
High school diploma or equivalent: 3
Registered apprenticeship or other trades certificate or diploma: 4
College, CEGEP or other non-university certificate or diploma: 5
University certificate or diploma below Bachelor's level: 6
Bachelor's degree: 7
Post graduate degree above Bachelor's level: 8
No response: 99
QHHOLD
CALCS1=1 PLWD
Which of the following best describes where you reside?
[Phone] (Interviewer: Read list)
In a private household by myself: 1
In a private household with at least one other person: 2
In supportive housing providing minimal to moderate support or care, such as homemaking or personal care: 3
In an institution or care home providing moderate to advanced care, such as a hospital, nursing home, long term care and group home: 4
Other (specify): 77
No response: 99
QCARE
CALCS1=1 PLWD
Who is your primary caregiver?
My spouse/life partner: 1
Another family member: 2
My neighbour: 3
A friend: 4
I do not have a primary caregiver: 5
Other (specify): 77
No response: 99
QCONSENT
May we share your contact information (including your name, email address and telephone number) with the Public Health Agency of Canada so they can contact you for participation in future work on dementia? Please note that your contact information will in no way be linked to your survey responses.
Yes: 1
No: 2
QCONTACTA
Please provide or confirm the following. [Phone]
(Interviewer: Read and make corrections if needed.)
Name:
Correct: 1
Incorrect (please provide name) : 77
QCONTACTB
Telephone:
Correct: 1
Incorrect (please provide telephone) : 77
QCONTACTC
Email:
EMAIL is not empty
Correct: 1
[EMAIL is not empty] Incorrect (please provide email address) : [Else] Please provide email address: 77
QREF
[CALCS1 = 5 and Q4 not = 1] Do you think that one of the people you are providing dementia care for would be able and willing to also participate in this research, through a similar, but much smaller set of questions, that could be completed online or with a telephone interviewer, with or without your assistance?[Else] Do you think that the person you are providing dementia care for would be able and willing to also participate in this research, through a similar, but much smaller set of questions, that could be completed online or with a telephone interviewer, with or without your assistance?
[Phone] (Interviewer, if yes, ask: Would it better to contact this person directly by phone, through you by phone, directly by email, or through you by email?)
Yes, contact this person directly by telephone: 1
Yes, contact them through me by telephone so that I may assist them: 2
Yes, send this person an email invitation directly with a link to the survey: 3
Yes, send me an email invitation with a link to the survey so that I may assist them: 4
No: 5
QREFA
What is this person's name?
Please provide name: 77
Prefer not to say: 99
QREFB
What is this person's telephone number?
Please provide telephone: 77
Prefer not to say: 99
QREFC
Please confirm your telephone number:
Correct: 1
Incorrect (please provide telephone): 77
QREFD
What is this person's email address?
Please provide email address: 77
Prefer not to say: 99
QREFE
Please provide, or confirm your email address:
EMAIL is not empty
Correct: 1
[EMAIL is not empty] Incorrect (please provide email address): [Else] Please provide email address: 77
QREF2
We are also interested in hearing from paid and unpaid dementia care providers in this survey. Do you know someone who provides care or support to people living with dementia, including Indigenous peoples, in a paid or unpaid capacity? If so, would you be willing to forward an email invitation to this person on our behalf, so that we may extend an invitation to them to participate in this research, through a similar, set of questions, that could be completed online or with a telephone interviewer?
EMAIL is not empty
Yes, send me an email invitation to [EMAIL] and I will forward it to them: 1
[EMAIL is not empty] Yes, please send the invitation to another email address (please specify): [Else] Yes, send me an email invitation and I will forward it to them (please provide email): 77
No: 98
Thank You
Those are all the questions we have for you. Thank you very much for taking the time to complete this survey, it is greatly appreciated. Your answers have been saved and you may now close your browser window.
THNK2
Screened out
Unfortunately, based on your responses you are not eligible to participate in this survey. Thank you for your time!