PSPC POR number: 068-22
Final Report
HC POR-21-06
Prepared for The Public Health Agency of Canada
Supplier Name: The Strategic Counsel
Contract number: CW2245802
Contract Value: $249,969.36
Award Date: 2022-10-21
Delivery Date: May 2, 2023
Registration number: POR-068-22
For more information on this report, please contact Health Canada at:
hc.cpab.por-rop.dgcap.sc@canada.ca
Ce rapport est aussi disponible en français.
Prepared for:The Public Health Agency of Canada
Supplier: The Strategic Counsel
May 2023
This public opinion research report presents the results of a two-phased study including a hybrid telephone and online survey and a round of focus groups conducted by The Strategic Counsel on behalf of Health Canada and the Public Health Agency of Canada.
Cette publication est aussi disponible en français sous le titre: Points de vue des Canadiens sur le vieillissement en santé à l'aube de la Décennie pour le vieillissement en bonne santé 2021-2030
This publication may be reproduced for non-commercial purposes only. Prior written permission must be obtained from the Public Health Agency of Canada. For more information on this report, please contact Health Canada at hc.cpab.por-rop.dgcap.sc@canada.ca or at:
Public Health Agency of Canada
785 Carling Avenue
Ottawa, Ontario, K1A 0K9
Catalogue Number: H14-449/2023E-PDF
International Standard Book Number (ISBN): 978-0-660-67533-6
Related publications (registration number): H14-449/2023F-PDF
Points de vue des Canadiens sur le vieillissement en santé à l'aube de la Décennie pour le vieillissement en bonne santé 2021-2030 (Final Report, French) ISBN Number: 978-0-660-67534-3
©His Majesty the King in Right of Canada, as represented by the Minister of Health, 2023.
In recent years, Canada has experienced a significant demographic shift - the year 2016 marked the first time in Canadian history in which the number of seniors surpassed the number of children (14 and younger). It is estimated that by 2038 approximately 21% to 25% of Canadians will be over the age of 65. As greater numbers of the population live longer, it is vital that individuals understand the importance of healthy aging and that they are supported in their efforts to age well.
In 2020, Canada endorsed the United Nations Decade of Healthy Ageing (2021-2030), a coordinated global effort led by the World Health Organization (WHO), which outlines a vision of a world in which all people can live long and healthy lives. Four action areas were identified which focus on changing how we think, feel and act towards aging, cultivating age-friendly environments, creating integrated and responsive health care systems and services, and ensuring long-term care for people who need it.
The Decade of Healthy Ageing (2021-2030)provides a new opportunity for the Government of Canada and the Public Health Agency of Canada (PHAC) to champion healthy aging in Canada.
The goal of this public opinion research was to gather information on the factors that foster well-being in older age by exploring the perspectives of older Canadians on enablers and barriers that affect their quality of life in older age. More specifically, the research was designed to address the following overarching objectives:
Additionally, the insights from this study will inform reporting to the WHO on Canada's progress on healthy aging.
This research study was conducted in two phases: Phase 1: Quantitative Telephone and Online Survey; and Phase 2: Qualitative Post-Survey In-Depth Focus Groups. A hybrid approach was deployed in order to yield a more comprehensive and holistic perspective. Each phase of the research was conducted among Canadians aged 50 years or older.
It should be noted that for purposes of this research, an abbreviated definition of healthy aging was employed and shared with respondents which emphasized developing and maintaining the physical and cognitive abilities that enable wellbeing as one ages via supportive environment that allow people to do what they value as they age. The more formal and complete definition can be found on the World Health Organization website: https://www.who.int/news-room/questions-and-answers/item/healthy-ageing-and-functional-ability.
To address the above-noted program objectives, the study was carried out across two phases:
More detail on the methodology, including the demographic characteristics of the survey sample and composition of the focus groups, can be found in Section IV - Detailed Methodology.
Key insights from both phases of the study are highlighted below, focusing on overarching themes with supporting data and findings from both the quantitative and qualitative phases. The structure of this section generally adheres to the six main topic areas covered to varying degrees in both the survey and the focus groups: Outlook and Perspectives on Aging, The Concept of Healthy Aging, Enablers and Barriers to Healthy Aging, Developing Age-Friendly Communities, Awareness and Role of PHAC in Healthy Aging, and Communications and Outreach to Older Canadians.
The survey results (shown as percentages) provide the foundation for the discussion of the key findings. Additional commentary from the focus groups is reported on as relevant and where it helps to shed more light on results from the survey and draw out further important nuances. Note also that those who participated in the survey are referred to as survey respondents or respondents, while those who took part in the focus groups are referred to as participants. This distinction is helpful in identifying from which of the two phases a particular finding has been drawn.
Canadians aged 50+ are mostly positive in terms of their general outlook on aging (overall 73% are very/somewhat positive). Those aged 80+ (80%), are in fact the most positive although the vast majority of those aged 50-64 are also positively disposed (70%). This suggests that older adults looking back on the experience of aging tend to view their situation somewhat more favourably relative to younger adults who are facing the prospect of aging and the accompanying adjustments or transition to this next phase in their lives. Respondents' attitudes towards aging also correlate strongly with their perceptions regarding their quality of life specifically in relation to social networks, mental well-being and financial status. Again, we found that the older cohort (aged 80+) offer more positive ratings in each of these areas.
Focus group participants provided a more nuanced perspective on aging than survey participants. Those who tended to be more positive or optimistic explained that they were looking forward to having more time to focus on hobbies, interests, family and friends. Some remarked on being more confident and "settled" at this stage in their lives, expressed gratitude or felt a sense of privilege at reaching this milestone in their lives. Others were more stoic, accepting aging as impending and unavoidable while also suggesting that maintaining a positive attitude requires individuals to personally "invest more in your happiness as you get older." Those participants who reported one or more of the following generally tended to be more positive in their outlook on aging: being financially secure, employed and/or volunteering, in reasonably good health, and leading a more active social life.
Others who espoused more negative attitudes about aging pointed to a range of issues as impacting their views, such as low or declining levels of energy, chronic aches and pains or other health issues, the experience of losing loved ones and/or the responsibility of caring for another elderly person or a partner, as well as having to give up activities and pursuits they had previously enjoyed.
Results from the survey closely align with the views expressed by participants in focus groups. While attitudes towards aging are fairly consistent across all regions of Canada and most demographic groups, those respondents who have never been married are less positive about aging relative to others who are married or cohabiting with a partner (66% vs. 75%, respectively). This finding underscores the negative impact of isolation and the importance of companionship and engagement to maintaining a positive outlook on aging. Survey results also revealed health status as a driver of attitudes. Those who self-report as having a disability and/or medical condition are less likely to rate their quality of life as good or excellent compared to those who do not (60% vs. 89%, respectively). Similarly, the former group are less inclined to feel somewhat/very positive about aging, compared to the latter (64% vs. 79%, respectively).
The predominant concerns Canadians aged 50+ have about aging are twofold: the prospect of declining health for themselves or for their partners (58% of survey respondents raised this as a key concern on an unprompted basis), and having the financial resources required to sustain them throughout their senior years (30%). With respect to the issue of financial resources, it should be noted that just over half (52%) of all respondents to the survey are retired, although retirement status varies across age groups - 24% among those aged 50-64, 80% among those aged 65-79, and 88% of those aged 80+. Notably, almost one in five of survey respondents (17%) indicate they are holding off or uncertain about retirement: until sometime after they reach age 70 (4%), are not likely to retire at any point (4%) or are uncertain about the age at which they will or can retire (9%).
Results from the survey indicate an elevated level of concern about declining health and financial security as they age among those residing in multi-generational households and, in particular, those with responsibility for children either over or under the age of 18. The issue of financial security is also a higher preoccupation for renters, relative to homeowners, and for those with lower household incomes, specifically under $60,000 annually. Those in lower income households are less likely to anticipate being able to retire at age 65 or earlier.
Focus group participants expressed similar concerns about aging with a primary focus on their health, both cognitive and physical, and their personal financial situation. Some expressed anxiety about how quickly one's health status can change (e.g., due to falls). Others who have witnessed the decline of a parent with Alzheimer's or dementia were concerned about the prospect of experiencing a similar fate. Many worried about the state of Canada's health care system, specifically wait lists, access to care, and the prospect of privatization. Other challenges which focus group participants associated with aging included: maintaining social relationships, meeting new people, social isolation (a particular issue for those in rural areas), loneliness, age discrimination (especially in the workplace and mentioned more often by female participants), home maintenance and housing affordability, and being a burden on others.
The younger segment of focus groups participants aged 50 and older was also concerned about the dual challenge of simultaneously taking care of aging parents as well as children. Those in the LGBTQ2S+ community worried they may face isolation as they age, fearing the prospect of discrimination, exclusion, and prejudice along with the accompanying negative mental health impacts particularly in the event they are required to move into an institutional setting. Older immigrants observed that seniors in their country of origin would typically be able to rely on extensive family support systems while, in their view, these systems were far more limited in Canada forcing them to be more self-reliant.
The term 'healthy aging' had a wide range of associations based on a list of select aspects of healthy aging shown or read to survey respondents. In addition to cognitive and brain health, as well as mental and physical well-being, healthy aging was also strongly associated with maintaining independence, aging in place, being active and mobile and having opportunities to do the things one feels are important.
In focus groups, the concept of and term 'healthy aging' resonated with participants. Without prompting, participants top-of-mind descriptions of healthy aging aligned with the WHO's definition. Healthy aging was strongly associated with the goal of maintaining an active and engaged lifestyle as one ages. Participants viewed healthy aging as encompassing the notions of physical, spiritual, emotional and mental health. Healthy aging held several connotations for focus group participants: staying active, learning/staying informed about aging, a healthy mind and a positive mindset, good nutrition, and a strong support system and social network. Some participants felt that the term healthy aging assumed one would also have or require the financial means to age in a healthy way. Others associated it with an ability to gain more personal control and agency over the aging process.
Key associations with the term 'healthy aging' and how it is interpreted vary to some extent by gender, age and health status. This was evident both in focus group discussions and in responses to the survey. In the survey, women are more likely than men to interpret the term quite broadly and, in particular, to associate it with being socially connected and being valued. The younger cohort, aged 50 to 64, tended to associate healthy aging more strongly with mental and physical well-being, being able to do what they feel is important, and being a contributor to society. By contrast, those aged 80 or older are more likely to associate healthy aging with being able to age at home. Those with a medical condition and/or a disability are less likely to associate healthy aging with many of the attributes assessed, compared to those who do not have a medical condition and/or a disability, although the strongest associations among both groups are with being able to age at home, being independent, and maintaining mental, cognitive and physical health. In focus groups, those with disabilities also stressed a strong desire to remain in their homes. This group were of the view that institutionalization as an older person would result in a further loss of independence.
Survey respondents and focus group participants alike point to the importance of access to the health care system and services as a key determinant for healthy aging (51% identified this as one of the most important factors contributing to healthy aging). Family and social connections were also noted as important (44% and 25%, respectively).
In focus groups the discussion regarding the factors which support or enable healthy aging allowed for a more wide-ranging conversation. Conversations surfaced additional facilitators such as a basic level of income, allowing for the financial resources to support a healthy diet and exercise, opportunities for continuous learning, access to seniors' centres, transportation, and affordable housing.
Although there was no strong consensus among focus group participants that being valued and contributing to society is vital to being able to age in a healthy way, some firmly believed that being respected, as distinct from being valued, as an elder in society is paramount. Participants commented that older Canadians' experience through the pandemic has affected their views about how society treats the aged and their perceptions regarding age discrimination. They underscored the need for a much more compassionate view of aging among society at large and generally more respect for older people among health care practitioners.
A commonly held view among focus group participants was that planning for healthy aging should begin much earlier in life and should include activities to ensure one's financial security in addition to exercises and activities to maintain physical and cognitive health as one ages.
Technology was seen as a double-edged sword. Some focus group participants felt that technological advances offered opportunities to support people as they age by connecting them to health care resources and social networks. Participants also appreciated devices which would assist them in meeting their personal fitness goals, monitoring their health status and improving their overall quality of life. The downsides, however, related to the rate of technological change which participants felt presented a challenge for older Canadians in terms of staying apace with new developments, affordability and the impersonal nature of technology. Others commented on the issues of misinformation online which they felt created confusion for older Canadians and undermined confidence on advice and information they might receive related to healthy aging.
As noted above, access to the health care system and financial resources were often mentioned as concerns or challenges for those aged 50 and older and were viewed as the main barriers to healthy aging. Participants, particularly those in lower income groups and those without a pension or a robust personal savings plan, frequently mentioned their worries about having a financially sustainable future.
Most survey respondents (84%) describe the communities in which they currently reside as 'age-friendly' and rate them favourably in terms of having safe, easy to access buildings and public spaces (64% rate their community as excellent or good), accessible and affordable high-speed internet (60%), social and recreational activities (58%), opportunities for lifelong learning (57%), and exercise programs for older adults (50%). Ratings drop off significantly when it comes to assessments of their communities regarding the availability of in-home services that support independent living (38%) and affordable housing (21%). Focus group participants also prioritized the latter two areas when discussing the key features of an 'age-friendly' community in addition to access to health services, including healthcare, mental health and dental care, although many nevertheless described their community as being 'age-friendly.'
More in-depth discussions in the focus groups revealed the difficulties that some participants faced in finding a family doctor. Additionally, participants emphasized their view that affordable housing is a basic human right, regardless of age or financial ability. Focus group discussions also illuminated the strong desire of those aged 50+ to age in place, viewing this as key to maintaining older Canadians' positive mental health.
The extent to which each of the features of an age-friendly community was prioritized varied across the focus groups, although access to health services, affordable housing and in-home services were commonly identified as key priorities across most groups:
Awareness of and the role of PHAC in healthy aging was explored in more depth within the focus groups. Many participants were not highly familiar with PHAC or its mandate to prevent disease and injury and promote good physical and mental health. Regardless, they felt the Agency had some credibility in promoting healthy aging and addressing unmet needs, most particularly in the area of awareness raising and information on the topic. Participants identified several areas where PHAC could play a role:
Across the board results from the survey indicate that there is an interest in obtaining more information on maintaining physical and cognitive health (88% are somewhat or very interested), aging at home (86%), healthy aging (86%) and healthy nutrition (80%). Health professionals, specifically doctors and nurses, are viewed as trusted sources of information on healthy aging (mentioned by 70% of survey respondents as being among the two sources they trust most). While few survey respondents (25%) recall seeing anything from the Government of Canada or PHAC on this topic, as noted above, PHAC has some credibility to lead or partners in awareness-raising and educational initiatives.
In focus groups, participants also indicated they would rely primarily on their family doctor for tips, information, and advice on healthy aging, but also on a range of other sources, including:
Comments from focus group participants suggested that any information coming from PHAC should also provide links to other reputable resources. In terms of receiving information a combination 'push and pull' approaches were recommended, encompassing both traditional and social media as well as government websites.
Older Canadians are relatively positive and optimistic about aging even though concerns and worries about the prospect of growing older in Canadian society were expressed. In particular, concerns about declining health in later life, the state of the health care system in Canada and the ability to access health care services, along with having adequate financial resources to remain comfortable, healthy, housed and independent for as long as possible were commonly noted. Participants felt they have a reasonable quality of life and want to continue to maintain this as they age. What this means for older persons as they move through this stage of their lives tends to vary based on their present circumstances and life situation. However, virtually all segments of the older population feel that being respected, more so than being valued for their past and/or current contribution to society, is important.
Many are confident in their ability to age in a healthy way and generally understand the concept of healthy aging as well as the facilitators and enablers of healthy aging. They also believe that their communities are age-friendly and can accommodate their changing needs as they age. Affordable housing is, however, a significant issue for older Canadians across the board. Similarly, a substantial proportion of older Canadians offer lower ratings of their community on services that support independent living and affordable public transit, which are key to their goal of aging in place.
Older Canadians are interested in the topic of healthy aging - both generally and in terms of specific areas such as maintaining cognitive and physical health, as well as aging at home. PHAC and Health Canada are viewed by some as credible sources of information, although additional work to enhance name recognition and brand awareness for PHAC may be required in advance of or in parallel to any educational outreach and awareness-raising initiatives on the topic of healthy aging. This would also help to improve PHAC's credibility among those audiences which may have less trust in and question information coming from health agencies as a result of the divisive experience through the pandemic and the influence of misinformation campaigns.
The senior population in Canada is diverse and changing. Connecting with the 50+ audience is challenging as it is not homogenous - age-friendly tailored communications should consider the wide variability in views, needs and expectations by gender, age, ethnicity and cultural background, socio-economic status and across equity-seeking groups. While various sub-groups of the 50+ population present unique challenges with respect to their general attitudes, expectations, priorities and interests regarding healthy aging, views tend to vary primarily and more consistently on the basis of socio-economic and health status.
A short summary highlighting key distinctions for specific sub-groups is included below:
By gender identity and sexual orientation - Gender differences are apparent across many aspects of healthy aging explored in this study, although the differences are most striking in a few areas. While declining health status (for themselves or their partner) is a top concern for both men and women in terms of aging, it is a more prominent issue for men compared to women. In focus groups, women were more vocal about the effects of aging on their appearance, the prospect of losing their independence and their ability to remain in their home. In contrast to men, women appear to have a more expansive view of healthy aging, tending to associate it more strongly with opportunities for continuous learning, staying socially connected, being valued and being seen as a contributor to society. They also view being close to family as an enabler to healthy aging to a greater extent than do men. While both women and men are generally of the view that their communities are age-friendly, men are more inclined to rate their communities highly on the various features that contribute to age-friendly communities. Slightly more men than women rate their community positively with respect to safety, accessibility in general and to key services such as health care, mental health and dental services, as well as in-home services to support independent living. Overall, women exhibit more interest than men in various topics related to healthy aging, particularly aging at home, maintaining cognitive and physical health, general information on the topic, and healthy nutrition. While medical professionals are key to delivering information and messaging about healthy aging to both women and men, women appear to be somewhat more open to hearing from others (e.g., family or friends and pharmacists).
Given the small number of those who identified as non-binary in the survey, most of the findings for this group are drawn from the feedback provided in the one focus group which was held with individuals aged 50+ who self-identified as 2SLGBTQI+. While additional research is recommended with this community on the topic of healthy aging, this group did offer many useful insights specific to their unique perspectives and challenges. Several participants mentioned the need for alternatives to long-term care and/or more supportive care systems offering queer positive spaces for aging members of the community. Some mentioned that many organizations serving older people are not queer-friendly and that more training of staff is required particularly focused on improving interactions with and care for the trans community as they age. Issues of safety within their community and within institutions for the elderly, including retirement homes and long-term care facilities, were a common concern for this group with several commenting that some members of their community may be driven "back into the closet."The ability to age in a way that offers choice was important and some took issue with what they felt was an overly restrictive WHO definition of healthy aging which may not allow everyone to see themselves. Otherwise, many of their concerns, interests and issues about healthy aging were similar to other older Canadians, focusing on financial security, social connection, and affordable housing.
By socio-economic status - Results show that older Canadians believe a basic level of income is one of the main enablers of healthy aging and concerns were expressed about the additional challenges faced by those with fewer financial resources as they age. Financial insecurity was an even greater concern among older Canadians with lower household incomes. These individuals were also more likely to focus on basic needs and fundamentals such as access to housing, buildings and transit as important factors contributing to healthy aging. Improved access to information on healthy aging is also of greater interest to this group, specifically on topics such as aging at home, preventing elder abuse, and oral health.
In general, older Canadians with higher household incomes are more positive in terms of their outlook on aging and tend to prioritize access to health services, social networks and physical/cognitive supports as key enablers to be able to age in a healthy way. This group also puts more emphasis on community-based social and recreational activities and safe neighbourhoods as important facets of age-friendly communities.
Among visible minority and racialized groups - Visible minority groups and/or racialized Canadians have a similar perspective and outlook on aging as others with a few notable differences. Compared to others a smaller share of those who classify as a visible minority rate their quality of life, in terms of their financial well-being, as excellent/good. Family is extremely important to this group as they age, and they are more likely to place a great priority on being close to family as an enabler of healthy aging. In focus groups, racialized participants mentioned the need for more cultural supports for seniors, creating opportunities for individuals to connect regularly with their cultural community. In certain cultural communities the process of aging and elderly people is celebrated, and a desire was expressed by some to be able to share in these events with their peers. This was viewed as critical to their being able to maintain an optimistic outlook and positive mental health as they age. As with other older Canadians, racialized participants expressed concerns about their ability to support themselves financially as they age and to access affordable shelter - this group specifically mentioned the need for more subsidized housing for seniors. Several also noted concerns with the health care system based on previous negative experiences and interactions. Visible minorities express strong interest in information on the subject of healthy aging in general, as well as specific topic areas including healthy nutrition, oral health and preventing elder abuse, to a greater extent as compared to other Canadians, aged 50 and older. They also tend to invest more trust in Health Canada/PHAC as a source of information on these issues, while placing somewhat less confidence in medical professionals compared to others.
Among newcomers - In focus groups, newcomers to Canada were particularly concerned about being disconnected from family and support systems that would have been available to them in their senior years in their country of origin. For this group, limited support systems in Canada particularly from other family members was a concern especially for those with chronic health conditions. There was a sense that Canadians do not place the same value on community and supporting each other in the aging process. Language was also raised as a challenge for newcomers aging in Canada who are not fluent in either English or French. This group also emphasized the importance of maintaining cultural connections as one ages.
Among Indigenous people - Although being an Indigenous elder is viewed as conferring a certain degree of status, Indigenous focus group participants emphasized their interest in staying connected with or reconnecting with their community and their culture as they age. Many were concerned about the prospect of being isolated, either from their community or their family. With respect to PHAC's role in healthy aging, this group emphasized the need to implement programs and services directed at older Indigenous people and assistance in helping them navigate the system of care and supports available. Many felt that information was available but that it was challenging to know where to find it or how to access services. There was also a desire for Indigenous people to have more control over their own healthcare, viewing this as essential to ensuring better access to the health care system and in-home services. They also identified a need for more employment/volunteer opportunities and exercise programs for older Indigenous people. When considering the needs of Indigenous people as they age in terms of services and information on the topic of healthy aging, this group stressed that consideration should be given to variability in access to financial resources and the needs of those living in rural, remote and Northern areas. There was little enthusiasm expressed for more information without the corresponding resources to be able to access services for those who are aging. And, in terms of communications, this group was more likely to mention radio as an important channel.
By health status - Respondents to the survey who self-report a poorer health status or who identify as having a disability and/or a medical condition which adversely affects their immune response system have a distinct perspective both on the quality their life at present and they outlook on aging. In particular, those who rate their health status as fair or poor/very poor are much less likely than those whose health is good/excellent to also rate their perceived quality of life highly across many areas and most particularly in terms of their financial well-being and social engagement. This perspective is foundational to their attitudes and concerns about aging. This group tends to be more pessimistic across the board and more concerned about their finances and the prospect of more privatization within the health care system as well as having to pay out of pocket for assistive devices (e.g., hearing aids). They are also less inclined to associate a broad range of features with the idea of healthy aging, specifically being active and mobile, and offer lower ratings of their communities on many features associated with being age-friendly. In focus groups, some disabled participants anticipated their world "shrinking"as they age and felt that their disability would exacerbate a sense of isolation. They value their autonomy and express a desire for healthy aging programming and services to focus more in bolstering their ability to be independent to the extent possible.
By urban vs rural living - Perhaps not surprisingly social isolation as one ages is a challenge raised more frequently by those residing in rural communities. Qualitative discussions uncovered that a lack of access to public transportation in these communities is seen as further "isolating" for many. Similarly, access to healthcare services (in the context of acceptable distances to a healthcare facility, the time it would take to receive emergency care if needed, and reasonable wait times for health services) is mentioned as an important feature of age-friendly communities for those residing in rural areas. By comparison, urban dwellers are more likely prioritize safe neighbourhoods.
Results from the two phases of the study are reported separately in the Detailed Findings (Sections II and III).
Phase 1 reporting, which highlights the findings from the online and telephone surveys, is structured to provide the reader with an initial overview of the results by theme or question, and typically includes a graphical or tabular representation of these results. The tables which have been included throughout this section show the total results on a question by question basis, as well as the break-out by gender and age across three cohorts - respondents between the ages of 50 to 64, 65 to74 and 80+. As a standard, results are also broken out for those who identified as having a disability and/or medical condition which would affect their body's ability to ward off infection (i.e., diabetes, heart disease, HIV, asthma) and these are compared to others and the overall totals. These tables offer an 'at a glance' perspective on how results may vary by gender, age and disability/medical status.
Immediately following the table, key demographic and regional differences of interest are more fully described, as relevant or applicable. These are shown under specific headings (gender, age, education, household income, household composition, employment status, language, region, community type, etc.) and include other statistically significant variations based on self-reported health and caregiver status, and perceptions of their overall quality of life. In some cases, due to the absence of any statistically significant differences or as a result of small sample sizes, no additional sub-group reporting has been included. The final sample for the combined telephone and online survey results included a small percentage who identified as non-binary, Indigenous or of a particular ethnic background and, as a result, sub-group analysis on these variables was limited.
Phase 2 reporting covers the findings from the focus groups. While generally adhering to the structure of the moderator's guide used to facilitate each discussion, the results are presented more thematically. Given the nature of focus groups discussions, which allow for issues to be explored in-depth and in a less filtered and structured fashion relative to surveys, findings are more open to interpretation. Moreover, given the relatively few individuals who participated in the focus groups as compared to the survey, the findings cannot be quantified or generalized to the broader population of Canadians aged 50 and older. That said, feedback from qualitative exercises such as this do offer valuable insights which help to contextualize or illuminate results from the survey and add to our overall understanding of older Canadians' views on various aspects of healthy aging.
Supplier Name: The Strategic Counsel
Contract Number: CW2245802
Contract Award Date: 2022-10-21
Contract Value: $249,969.36
For more information, please contact Health Canada at hc.cpab.por-rop.dgcap.sc@canada.ca
Statement of Political Neutrality
I hereby certify as Senior Officer of The Strategic Counsel that the deliverables fully comply with the Government of Canada political neutrality requirements outlined in the Government of Canada's Policy on Communications and Federal Identity and Directive on the Management of Communications. Specifically, the deliverables do not include information on electoral voting intentions, political party preferences, party standings with the electorate, or ratings of the performance of a political party or its leaders.
Signed: ___________________________________
Donna Nixon, Partner
Phase 1 of this study involved the administration of a 20-minute survey among 2,500 Canadians, aged 50 and older. The primary methodology was a telephone-based interview (n=2000) supplemented by an online survey (n=500). The dual-mode approach was undertaken in order to assess any modal differences in attitudes for this target population and to ascertain whether future surveys could be shifted to a fully online methodology.
The totals referred to below and throughout this part of the report reflect the merged results from both the telephone and online surveys. The sample design for each mode was configured to ensure that the final results reflected a cross-section of Canadians in the 50+ age group by gender, age and region.
As noted in the Executive Summary a detailed methodology, including a full demographic profile of respondents and a discussion of any variations in the findings across the two modes, can be found in Section IV of this report.
A high-level profile of respondents to the survey is outlined below and includes self-reported information about the respondents' health and caregiver status along with their perceived quality of life and level of engagement in various activities. This overview, along with the demographic profile included in the Methodology, offers important context when interpreting findings from the survey given that respondents' own health and circumstances may impact their views on and interest in the topic of healthy aging.
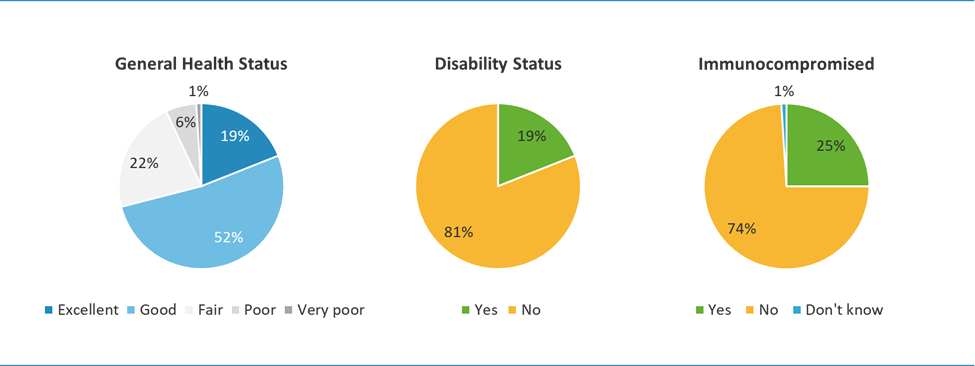
Respondents report being in generally good health. About one in five identify as having a disability and slightly more - one-quarter - indicate having a chronic health condition which affects their body's ability to fight off infections. The age of respondents does not appear to have a particularly strong bearing on health status, however there is a slight shift to those reporting their health as good, rather than excellent, as one ages.
Respondents with disabilities are typically at greater risk for other health problems and the results from the survey underscore the presence of comorbidity - a higher proportion of this group are also immunocompromised. Although a smaller percentage than people without disabilities and/or those who are immunocompromised, many respondents with a disability and/or a chronic medical condition nevertheless report their health to be good.
The vast majority of respondents also report having access to a family doctor. Access does vary depending on where one lives in Canada. It is lowest in Quebec and highest in Ontario.
One in five respondents are caregivers, providing primary care for someone else with a health condition, physical or mental disability or who is experiencing problems related to aging. There is a slight gender and age skew - a higher proportion of women and respondents in the youngest age cohort (50-64 years of age) are more likely to say they are a caregiver.
Most respondents to the survey claim to be in generally good health (see Figure 1) - the majority say their health is either good or excellent. Similarly, most indicate they do not have a disability or some type of medical condition that would weaken their body's ability to ward off disease or infection.
| Rating | Percentage |
|---|---|
| Excellent | 19 |
| Good | 52 |
| Fair | 22 |
| Poor | 6 |
| Very poor | 1 |
| Identify as a person with a disability | Percentage |
|---|---|
| Yes | 19 |
| No | 81 |
| Immunocompromised | Percentage |
|---|---|
| Yes | 25 |
| No | 74 |
| Don't know | 1 |
As shown in the following table, while most respondents rate their general health as good(52%) or excellent (19%), just over one in five rate their health as fair (22%), and a small percentage report being in poor (6%) or very poor (1%) health.
| TOTAL | Male | Female | Age 50-64 |
Age 65-79 |
Age 80+ |
Medical condition and/or disability YES |
Medical condition and/or disability NO |
|
|---|---|---|---|---|---|---|---|---|
| n= | 2500 | 1175 | 1325 | 1300 | 900 | 300 | 885 | 1604 |
| % | % | % | % | % | % | % | % | |
| NET - EXCELLENT/GOOD | 70 | 69 | 72 | 71 | 70 | 70 | 44 | 85 |
| Excellent | 19 | 19 | 19 | 20 | 18 | 14 | 4 | 27 |
| Good | 52 | 50 | 53 | 50 | 52 | 56 | 40 | 59 |
| Fair | 22 | 24 | 21 | 21 | 24 | 23 | 39 | 13 |
| Poor | 6 | 6 | 6 | 6 | 5 | 6 | 14 | 1 |
| Very Poor | 1 | 1 | 1 | 1 | 1 | 1 | 3 | <1 |
| NET - POOR | 7 | 7 | 7 | 8 | 6 | 7 | 17 | 2 |
| Prefer not to answer | <1 | <1 | <1 | <1 | <1 | <1 | 1 | <1 |
Q5. Would you say your health in general is …?
Base: Total sample
Self-reported health status varies minimally, as noted below.
Age
Health Status
Among respondents who completed the survey, about one in five (19%) identify as a person with a disability. This proportion is relatively consistent across demographic groups and regions, with a few exceptions.
| TOTAL | Male | Female | Age 50-64 |
Age 65-79 |
Age 80+ |
|
|---|---|---|---|---|---|---|
| n= | 2500 | 1175 | 1325 | 1300 | 900 | 300 |
| % | % | % | % | % | % | |
| Yes | 19 | 18 | 20 | 20 | 17 | 22 |
| No | 81 | 82 | 79 | 80 | 83 | 78 |
| Don't know | <1 | - | <1 | <1 | <1 | - |
| Prefer not to answer | <1 | - | <1 | - | <1 | - |
Q6a. Do you identify as a person with a disability?
Base: Total sample
Household Income
Marital Status
Language
Region
Compared to the percentage of respondents who identify as having a disability, a slightly higher proportion of respondents say they have a medical condition (such as heart disease, diabetes, HIV or asthma) that weakens the body's ability to fight off infections (25%).
| TOTAL | Tele-phone | Online | Male | Female | Age 50-64 |
Age 65-79 |
Age 80+ |
|
|---|---|---|---|---|---|---|---|---|
| n= | 2500 | 2000 | 500 | 1175 | 1325 | 1300 | 900 | 300 |
| % | % | % | % | % | % | % | % | |
| Yes | 25 | 25 | 25 | 24 | 26 | 24 | 25 | 29 |
| No | 74 | 74 | 75 | 75 | 74 | 76 | 74 | 70 |
| Don't know | 1 | 1 | - | 1 | 1 | <1 | 1 | 1 |
| Prefer not to answer | <1 | <1 | - | <1 | <1 | <1 | <1 | - |
Q6b. Do you identify as someone with a medical condition that weakens your body's ability to fight off infections (such as heart disease, diabetes, HIV, asthma)?
Base: Total sample
Sexual Orientation
Age
Marital Status
Language
Disability Status
To obtain a better understanding of respondents' ability to access medical care on a regular or as needed basis, they were asked whether or not they have a family doctor or physician - 86% do, 14% do not (see Table 4). This variable was also examined in terms of the extent to which it correlates with certain perspectives on healthy aging and is reported on in later sections, as relevant.
| TOTAL | Male | Female | Age 50-64 |
Age 65-79 |
Age 80+ |
Medical condition and/or disability YES |
Medical condition and/or disability NO |
|
|---|---|---|---|---|---|---|---|---|
| n= | 2500 | 1175 | 1325 | 1300 | 900 | 300 | 885 | 1604 |
| % | % | % | % | % | % | % | % | |
| Yes | 86 | 85 | 87 | 83 | 89 | 92 | 91 | 83 |
| No | 14 | 15 | 13 | 17 | 11 | 8 | 9 | 16 |
| Prefer not to answer | <1 | <1 | <1 | <1 | - | 1 | <1 | <1 |
Q22. Do you have a family doctor/physician?
Base: Total sample
Age
Language
Region
One in five respondents (20%) report being a caregiver, specifically having responsibility for the primary care of someone with a long-term health condition, physical or mental disability or problems related to aging.
| TOTAL | Male | Female | Age 50-64 |
Age 65-79 |
Age 80+ |
Medical condition and/or disability YES |
Medical condition and/or disability NO |
|
|---|---|---|---|---|---|---|---|---|
| n= | 2500 | 1175 | 1325 | 1300 | 900 | 300 | 885 | 1604 |
| % | % | % | % | % | % | % | % | |
| Yes | 20 | 17 | 22 | 23 | 16 | 16 | 20 | 20 |
| No | 80 | 82 | 78 | 76 | 84 | 83 | 80 | 80 |
| Prefer not to answer | <1 | <1 | <1 | <1 | 1 | <1 | <1 | <1 |
Q23. Are you responsible for the primary care of someone with a long-term health condition, physical or mental disability, or problems related to aging?
Base: Total sample
Gender
Age
Household Composition
Language
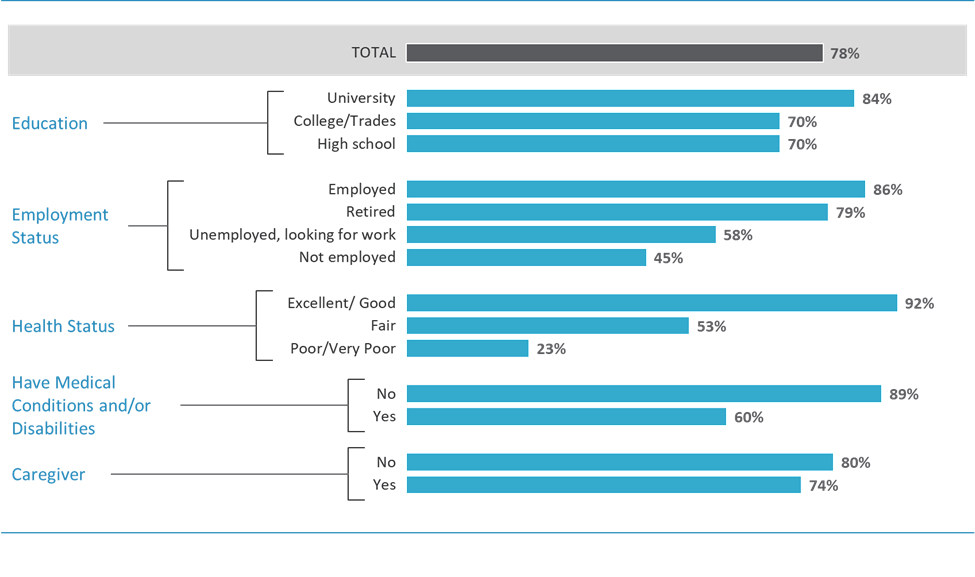
Combined, almost four in five respondents rate their overall quality of life quite positively and this is consistent by gender, across age groups, and most other demographics. Perceptions of one's quality of life vary primarily based on one's health and socio-economic status. Ratings are not as positive among those whose health status is poorer or compromised and respondents with lower incomes or who are unemployed/not in the workforce (rather than working or retired).
| Base | Percentage reporting Excellent/Good |
|---|---|
| Total sample | 78 |
| Education | Percentage reporting Excellent/Good |
|---|---|
| University | 84 |
| College/Trades | 70 |
| High school | 70 |
| Employment Status | Percentage reporting Excellent/Good |
|---|---|
| Employed | 86 |
| Retired | 79 |
| Unemployed, looking for work | 58 |
| Not employed | 45 |
| Health Status | Percentage reporting Excellent/Good |
|---|---|
| Excellent/Good | 92 |
| Fair | 53 |
| Poor/Very Poor | 23 |
| Medical Condition and/or Disability | Percentage reporting Excellent/Good |
|---|---|
| No | 89 |
| Yes | 60 |
| Caregiver Status | Percentage reporting Excellent/Good |
|---|---|
| No | 80 |
| Yes | 74 |
Respondents offer generally favourable ratings when it comes to their current quality of life, with over half rating it as good (53%) and another quarter as excellent(25%). Just under one in five (17%) offer a more neutral rating, describing their quality of life as fair. Very few older Canadians (3%) feel they have a poor (4%) or very poor(1%)quality of life at present.
| TOTAL | Male | Female | Age 50-64 |
Age 65-79 |
Age 80+ |
Medical condition and/or disability YES |
Medical condition and/or disability NO |
|
|---|---|---|---|---|---|---|---|---|
| n= | 2500 | 1175 | 1325 | 1300 | 900 | 300 | 885 | 1604 |
| % | % | % | % | % | % | % | % | |
| NET - EXCELLENT/GOOD | 78 | 77 | 79 | 77 | 81 | 78 | 60 | 89 |
| Excellent | 25 | 25 | 25 | 26 | 26 | 20 | 12 | 33 |
| Good | 53 | 53 | 54 | 51 | 55 | 58 | 47 | 56 |
| Fair | 17 | 18 | 17 | 18 | 16 | 19 | 31 | 10 |
| Poor | 3 | 3 | 3 | 4 | 3 | 3 | 7 | 1 |
| Very Poor | 1 | 1 | 1 | 1 | <1 | <1 | 2 | <1 |
| NET - POOR | 4 | 4 | 4 | 5 | 3 | 3 | 9 | 2 |
| Prefer not to answer | <1 | - | <1 | - | - | <1 | - | <1 |
Q7. Overall, how would you rate your quality of life? Would you say it is ...?
Base: Total sample
Age
Education
Household Income
Employment Status
Visible Minority
Health Status
Type of Community
To further evaluate older Canadians' perceptions of their quality of life, respondents were asked to provide ratings in six different areas. Positive ratings (of excellent orgood) are provided by over four in five respondents in regard to their relationships (87%), mental well-being (82%) and/or sense of purpose in life (80%). Fewer, but still a significant proportion, rate their physical or financial well-being as excellent/good (68% and 67%, respectively). Ratings drop back to with respect to perceptions of their quality of life related to participating in social/community activities (55%).
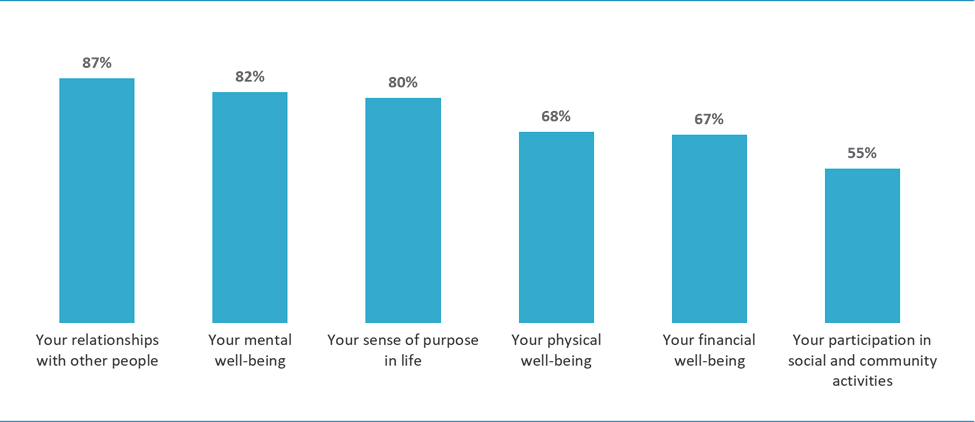
| Your relationships with other people | 87% |
| Your mental well-being | 82% |
| Your sense of purpose in life | 80% |
| Your physical well-being | 68% |
| Your financial well-being | 67% |
| Your participation in social and community activities | 55% |
Table 7 shows the ratings for quality of life in these same areas broken out by gender, age and for those with/without a disability and/or medical condition. More detail on the demographic and regional variations are also provided below the table. Some patterns are evident, specifically that those with a medical condition or disability generally tend to rate their quality of life in each area lower compared to those without - ratings for the former group range from 41% to 79%, while ratings for the latter group range from 63% to 92%. More positive ratings also tend to be offered by respondents with a higher socio-economic status (i.e., higher annual household income, higher educational attainment, employed, and homeowners).
| TOTAL | Male | Female | Age 50-64 |
Age 65-79 |
Age 80+ |
Medical condition and/or disability YES |
Medical condition and/or disability NO |
|
|---|---|---|---|---|---|---|---|---|
| n= | 2500 | 1175 | 1325 | 1300 | 900 | 300 | 885 | 1604 |
| % | % | % | % | % | % | % | % | |
| Your relationships with other people | 87 | 84 | 90 | 86 | 88 | 91 | 79 | 92 |
| Your mental well being | 82 | 82 | 81 | 79 | 84 | 86 | 71 | 88 |
| Your sense of purpose in life | 80 | 80 | 81 | 80 | 81 | 81 | 69 | 87 |
| Your physical well being | 68 | 69 | 68 | 68 | 69 | 69 | 43 | 82 |
| Your financial well-being | 67 | 67 | 66 | 65 | 66 | 72 | 53 | 74 |
| Your participation in social and community activities | 55 | 54 | 56 | 54 | 57 | 55 | 41 | 63 |
Q8A. How, would you rate your quality of life in each of the following areas...?
Base: Total sample
Statistically significant variations in quality of life ratings across the six areas are highlighted below:
Gender
Age
Education
Household Income
Home Ownership
Household Composition and Marital Status
Visible Minority
Language
Health Status
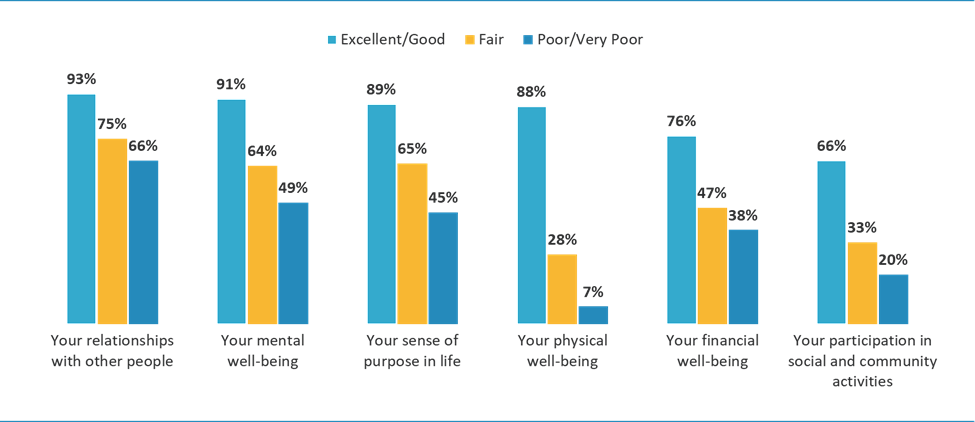
| Area | Excellent/Good | Fair | Poor/Very poor |
|---|---|---|---|
| Your relationships with other people | 93% | 75% | 66% |
| Your mental well-being | 91% | 64% | 49% |
| Your sense of purpose in life | 89% | 65% | 45% |
| Your physical well-being | 88% | 28% | 7% |
| Your financial well-being | 76% | 47% | 38% |
| Your participation in social and community activities | 66% | 33% | 20% |
Region
Type of Community
Canadians aged 50 and older are a highly engaged group, both socially and physically active on a regular basis. A much smaller percentage are regularly engaged in volunteering or in activities at local community centres.
The vast majority of older Canadians engage in social interactions with family and/or friends at least weekly (88%), with almost half saying they do so daily (48%). Other activities in which respondents engage regularly include physical activities - 79% say they engage in activities such as swimming, walking, dancing, or gardening at least once a week - and undertaking hobbies related to their interests (70%). Fewer volunteer (23%) and/or participate in activities put on by their local community centre (20%) on a weekly basis.
| TOTAL | Male | Female | Age 50-64 |
Age 65-79 |
Age 80+ |
Medical condition and/or disability YES |
Medical condition and/or disability NO |
|
|---|---|---|---|---|---|---|---|---|
| n= | 2500 | 1175 | 1325 | 1300 | 900 | 300 | 885 | 1604 |
| % | % | % | % | % | % | % | % | |
| Connecting with family and friends | 88 | 85 | 91 | 87 | 89 | 90 | 82 | 92 |
| Physical activity (swimming, walking, dance, gardening) | 79 | 81 | 77 | 80 | 80 | 73 | 67 | 86 |
| Hobbies or personal interests (painting, photography, birdwatching, music, taking a class) | 70 | 69 | 70 | 70 | 71 | 68 | 64 | 73 |
| Volunteering | 23 | 22 | 24 | 18 | 28 | 29 | 19 | 25 |
| Activities at a local community centre (either in-person or virtual) | 20 | 19 | 21 | 17 | 22 | 26 | 17 | 21 |
Q9. How often do you engage in each of the following... ?
Base: Total sample
Participation rates vary to some extent across key demographics and by region, as follows.
Gender
Age
Education
Household Income
Employment Status
Household Composition and Marital Status
Language
Health Status and Quality of Life
Region
Type of Community
When it comes perspectives on aging, respondents generally feel positive about the prospect of getting older. However, concerns center mainly on the prospect of declining health associated with aging and their personal finances. Looking across demographic groups, characteristics of those who appear more concerned with their own (or their partner's) health declining are typically men, younger (aged 50-64), are employed, have a post-secondary educational attainment, are in a married/common law relationship, are living with their children, and do not have a medical condition or disability. Those who have greater concern about their personal finances as they age are also more likely to be younger, but also have lower household incomes (less than $60,000 annually), have children living at home, and have a medical condition or disability.
Just over half (52%) of older Canadians are retired while the other half is made up of those still in the workforce (41%) or e not in the workforce (7%). While many of those currently working intend to retire between the ages of 60 and 65, a significant proportion are not sure or indicate they have no plans to retire at any time in the future.
Almost three quarters (73%) of Canadians aged 50 and older feel positive either about the general prospect or their current experience with regards to aging. As per Figure 5 below, two in five (20%) hold a verypositive view while, a larger proportion (over half of respondents) (53%) have somewhat positive views. Still a significant proportion, approximately one quarter of respondents (26%), have more negative views.
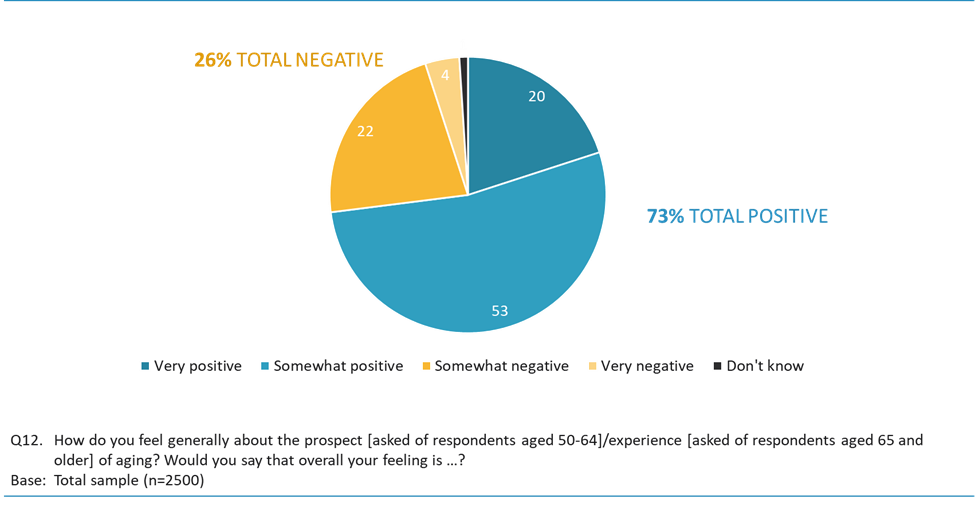
| Very positive | 20% |
| Somewhat positive | 53% |
| Total positive | 73% |
| Somewhat negative | 22% |
| Very negative | 4% |
| Total negative | 26% |
| Don't know | 1% |
Views on aging do vary across select demographic groups including gender, age and presence of a medical condition/disability as indicated in Table 9 below.
| TOTAL | Male | Female | Age 50-64 |
Age 65-79 |
Age 80+ |
Medical condition and/or disability YES |
Medical condition and/or disability NO |
|
|---|---|---|---|---|---|---|---|---|
| n= | 2500 | 1175 | 1325 | 1300 | 900 | 300 | 885 | 1604 |
| % | % | % | % | % | % | % | % | |
| TOTAL - VERY/SOMEWHAT POSITIVE | 73 | 73 | 74 | 70 | 76 | 80 | 64 | 79 |
| Very positive | 20 | 19 | 21 | 17 | 21 | 29 | 17 | 22 |
| Somewhat positive | 53 | 53 | 54 | 53 | 55 | 51 | 47 | 57 |
| Somewhat negative | 22 | 22 | 21 | 24 | 20 | 17 | 27 | 18 |
| Very negative | 4 | 4 | 4 | 5 | 3 | 2 | 8 | 2 |
| TOTAL - VERY/SOMEWHAT NEGATIVE | 26 | 27 | 25 | 29 | 24 | 19 | 35 | 21 |
| Don't know/Not sure | 1 | 1 | 1 | 1 | <1 | 1 | 1 | <1 |
| Prefer not to answer | <1 | <1 | <1 | <1 | <1 | <1 | <1 | <1 |
Q12. How do you feel generally about the prospect [asked of respondents aged 50-64]/experience [asked of respondents aged 65 and older] of aging? Would you say that overall your feeling is …?
Base: Total sample
Figure 6, and the accompanying narrative below, highlights some of the key demographic differences in terms of those who hold more positive views overall about aging.
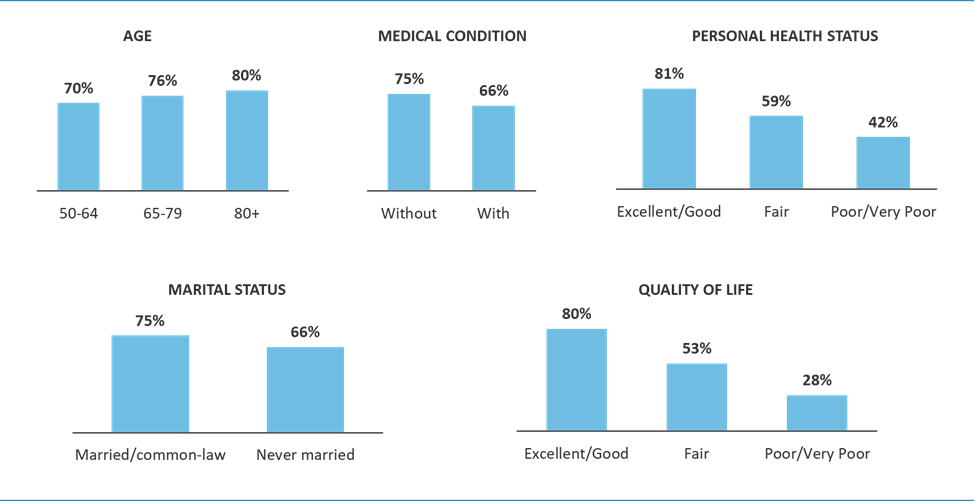
| Age | Percentage reporting Very/Somewhat positive |
|---|---|
| 50-64 | 70 |
| 65-79 | 76 |
| 80+ | 80 |
| Medical Condition | Percentage reporting Very/Somewhat positive |
|---|---|
| Without | 75 |
| With | 66 |
| Personal Health Status | Percentage reporting Very/Somewhat positive |
|---|---|
| Excellent/Good | 81 |
| Fair | 59 |
| Poor/Very poor | 42 |
| Marital Status | Percentage reporting Very/Somewhat positive |
|---|---|
| Married/Common-law | 75 |
| Never married | 66 |
| Quality of Life | Percentage reporting Very/Somewhat positive |
|---|---|
| Excellent/Good | 80 |
| Fair | 53 |
| Poor/Very poor | 28 |
Age
Marital Status
Health Status and Quality of Life
Region
When asked in an open-ended format what two things most concern them as they age, respondents focused on two issues: declining health affecting themselves or their partners (58%) and finances (30%). Other concerns are mentioned with far less frequency, including losing their independence (14%), accessing medical services (8%), isolation or loneliness (7%), physical decline (7%), and not being able to live at home (5%). Fear of falls or getting hurt was mentioned infrequently (3%) as was not being able to drive (3%). Other issues were mentioned by 2% or fewer respondents.
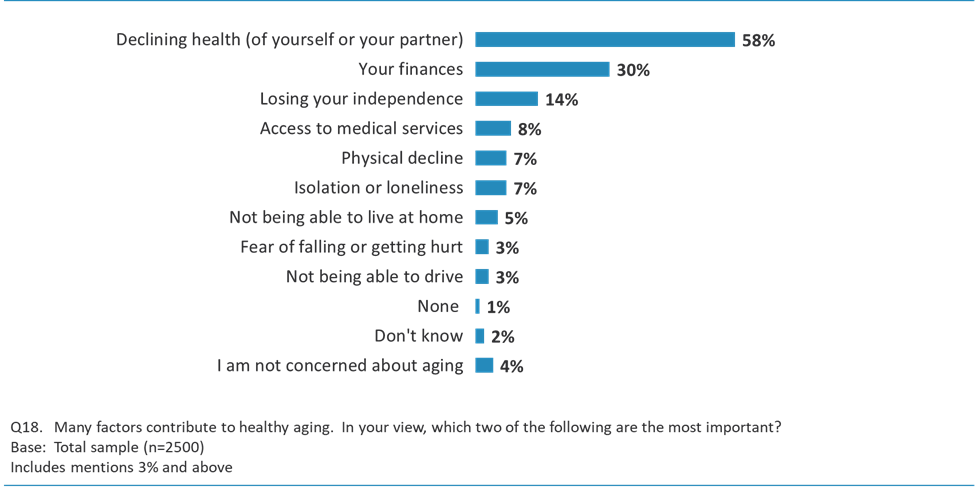
| Declining health (of yourself or your partner) | 58% |
| Your finances | 30% |
| Losing your independence | 14% |
| Access to medical services | 8% |
| Physical decline | 7% |
| Isolation or loneliness | 7% |
| Not being able to live at home | 5% |
| Fear of falling or getting hurt | 3% |
| Not being able to drive | 3% |
| None | 1% |
| Don't know | 2% |
| I am not concerned about aging | 4% |
There are some significant differences when it come's to one's concerns about aging based on the demographic characteristics, as highlighted in Table 10 below and described in the narrative that follows.
| TOTAL | Male | Female | Age 50-64 |
Age 65-79 |
Age 80+ |
Medical condition and/or disability YES |
Medical condition and/or disability NO |
|
|---|---|---|---|---|---|---|---|---|
| n= | 2500 | 1175 | 1325 | 1300 | 900 | 300 | 885 | 1604 |
| % | % | % | % | % | % | % | % | |
| Declining health (of yourself or your partner) | 58 | 62 | 54 | 61 | 56 | 48 | 56 | 59 |
| Your finances | 30 | 32 | 29 | 37 | 26 | 11 | 35 | 27 |
| Losing your independence | 14 | 12 | 15 | 12 | 15 | 15 | 12 | 14 |
| Access to medical services | 8 | 6 | 10 | 8 | 8 | 6 | 9 | 8 |
| Physical decline | 7 | 7 | 7 | 6 | 8 | 9 | 7 | 7 |
| Isolation or loneliness | 7 | 6 | 8 | 7 | 8 | 7 | 8 | 7 |
| Not being able to live at home | 5 | 4 | 7 | 4 | 7 | 9 | 5 | 5 |
| Fear of falling or getting hurt | 3 | 2 | 3 | 2 | 4 | 5 | 4 | 2 |
| Not being able to drive | 3 | 2 | 3 | 1 | 3 | 7 | 3 | 2 |
| None | 1 | 1 | 1 | 1 | <1 | 2 | 1 | 1 |
| Don`t Know | 2 | 2 | 1 | 1 | 2 | 4 | 2 | 2 |
| I am not concerned about aging | 4 | 4 | 3 | 3 | 4 | 7 | 4 | 4 |
Q13. What 2 things are you most concerned about as you age?
Base: Total sample
Includes mentions 3% and above
Gender
Age
Education
Household Income
Employment Status
Home Ownership Status
Household Composition and Marital Status
Visible Minority
Language
Health Status and Quality of Life
Region
Respondents were asked about their current employment status and a subsequent question, among those still in the workforce, regarding the age at which they anticipated retiring.
Of the total sample, just over half (52%) are retired. A small proportion (7%) are not in the workforce and not seeking employment.
Among the remainder, which includes all those still working either full-time or part-time, just under one in five (18%) anticipate retiring at age 65 or earlier (6% at age 60 or before; 12% between the ages of 61 and 65). Another 7% expect to retire between the ages of 66 and 70, while a small percentage (4%) anticipate retiring some time over the age of 70. Similar numbers (4%) do not expect to retire, at any age, and another 9% are uncertain about the age at which they will retire.
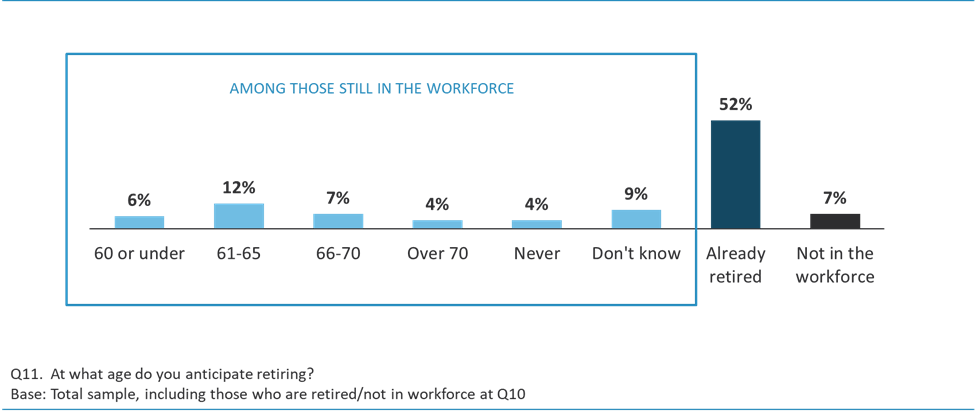
| 60 or under | 6% |
| 61-65 | 12% |
| 66-70 | 7% |
| Over 70 | 4% |
| Never | 4% |
| Don't know | 9% |
| Already retired | 52% |
| Not in the workforce | 7% |
Table 11, and the text provided below, outlines a breakdown of one's anticipated retirement age across the various demographics groups analyzed in this research study.
| TOTAL | MALE | FEMALE | AGE 50-64 |
AGE 65-79* |
AGE 80+* |
MEDICAL COND-ITION YES |
MEDICAL COND-ITION NO |
|
|---|---|---|---|---|---|---|---|---|
| n= | 2500 | 1175 | 1325 | 1300 | 900 | 300 | 885 | 1604 |
| % | % | % | % | % | % | % | % | |
| 60 or under | 6 | 6 | 6 | 12 | <1 | - | 5 | 7 |
| 61-65 | 12 | 13 | 11 | 22 | <1 | - | 9 | 14 |
| 66-70 | 7 | 8 | 6 | 10 | 4 | <1 | 6 | 8 |
| Over 70 | 4 | 4 | 4 | 3 | 5 | 2 | 3 | 4 |
| Never | 4 | 4 | 3 | 5 | 3 | 2 | 3 | 5 |
| Don't know/Not sure (Volunteered) | 9 | 8 | 9 | 13 | 5 | 2 | 7 | 10 |
| I am already retired | 52 | 51 | 53 | 24 | 80 | 88 | 55 | 51 |
| Not in the workforce | 7 | 5 | 9 | 10 | 2 | 6 | 13 | 3 |
Q11. At what age do you anticipate retiring?
Base: Total sample, including those who are retired/not in workforce at Q10
*Responses to this question appear to indicate that a very small number of respondents may have misunderstood the question to be asking about the age they expected to retire rather than the age they anticipate retiring. Further analysis shows that this issue occurred among several respondents to the telephone survey.
Gender
Age
Education
Household Income
Household Composition and Marital Status
Visible Minority
Language
Health Status and Quality of Life
Region
The World Health Organization defines healthy aging as the following:
Healthy ageing is the process of developing and maintaining the functional ability that enables wellbeing in older age. Functional ability is about having the capabilities that enable all people to be and do what they have reason to value. This includes a person's ability to:
They further define functional ability as consisting of the intrinsic capacity of an individual (meaning mental and physical capacities) as well as relevant environmental characteristics (meaning environments such as home, community and broader society), and the interaction between these two.
Respondents were asked a short series of questions to gauge their top-of-mind perspectives on the concept of healthy aging, specifically key associations with the term, and what they believe to be the primary enablers of healthy aging. Overwhelmingly, healthy aging is associated with the ability to remain active, self-sufficient and independent into one's senior years. Respondents are focused primarily on ensuring their physical and mental well-being as well as cognitive performance, while they are less inclined to strongly associate healthy aging with making a societal contribution, being valued, socially connected or continuous learning. Although many respondents view aging at home as being clearly linked to the concept of healthy aging, the connection between the two is more strongly felt among the older age cohort (those aged 65+) and among Francophones relative to Anglophones. The degree to which respondents associate various abilities with healthy aging also varies quite dramatically based on one's self-assessed health status and perceived quality of life, and specifically whether one is disabled or has a medical condition. Those with a disability and/or medical condition are, for example, much less likely to strongly associate healthy aging with being active and mobile.
Prior to providing respondents with a brief definition of healthy aging, they were asked how much they associate healthy aging with a range of elements (10 in total), using a scale of a lot, somewhat, not very much ornot at all. As shown in the two charts below, respondents associate the term healthy aging with a variety of abilities that are factors of their individual capacity and characteristics, as well as the wider environment.
Based on the proportion of respondents who responded a lot on this question, over three-quarters strongly associate healthy aging with the various abilities or competencies which support the goal of remaining self-sufficient, including:
The ability to do what one feels is important is also strongly associated with the process of healthy aging (76%).
By comparison, certain aspects related to individual growth, social interactions, and how one is perceived by others are less strongly associated with the process of healthy aging. About six in ten closely associate healthy aging with:
The strength of association declines further when it comes to being a contributor to society, with just over two in five seeing this as closely linked to the process of healthy aging (43%).
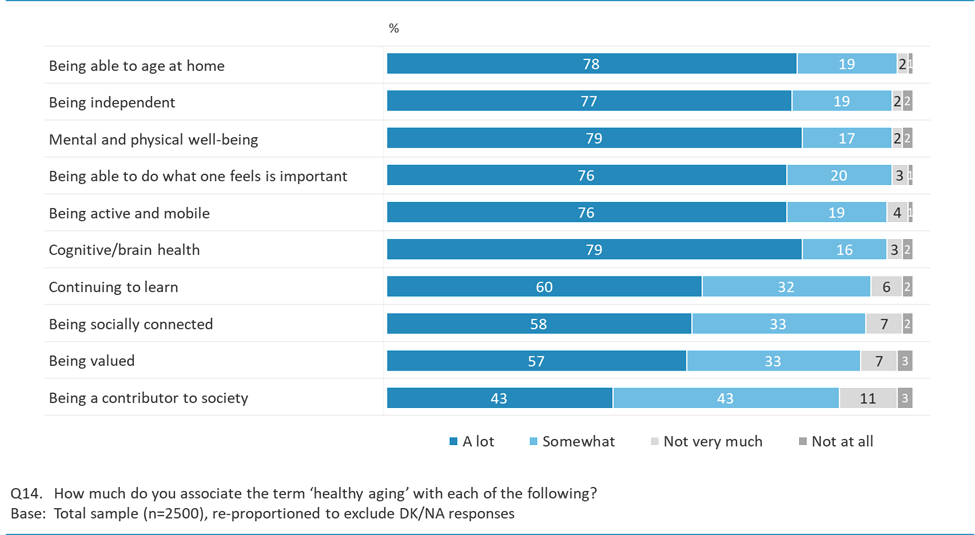
| Element | A lot | Somewhat | Not very much | Not at all |
|---|---|---|---|---|
| Being able to age at home | 78% | 19% | 2% | 1% |
| Being independent | 77% | 19% | 2% | 2% |
| Mental and physical well-being | 79% | 17% | 2% | 2% |
| Being able to do what one feels is important | 76% | 20% | 3% | 1% |
| Being active and mobile | 76% | 19% | 4% | 1% |
| Cognitive/brain health | 79% | 16% | 3% | 2% |
| Continuing to learn | 60% | 32% | 6% | 2% |
| Being socially connected | 58% | 33% | 7% | 2% |
| Being valued | 57% | 33% | 7% | 3% |
| Being a contributor to society | 43% | 43% | 11% | 3% |
Table 12, below, shows a further break-out across select demographic sub-groups for those who strongly associate each of the above-noted aspects with healthy aging (i.e., % saying they associate each of the 10 elements a lot with healthy aging).
| TOTAL | Male | Female | Age 50-64 |
Age 65-79 |
Age 80+ |
Medical condition and/or disability YES |
Medical condition and/or disability NO |
|
|---|---|---|---|---|---|---|---|---|
| n= | 2500 | 1175 | 1325 | 1300 | 900 | 300 | 885 | 1604 |
| % | % | % | % | % | % | % | % | |
| Mental and physical well-being | 79 | 76 | 81 | 80 | 79 | 74 | 70 | 84 |
| Cognitive/brain health | 79 | 76 | 81 | 80 | 78 | 77 | 71 | 83 |
| Being able to age at home | 78 | 77 | 79 | 74 | 82 | 81 | 74 | 79 |
| Being independent | 78 | 74 | 80 | 76 | 80 | 79 | 71 | 81 |
| Being active and mobile | 76 | 75 | 76 | 76 | 77 | 70 | 64 | 82 |
| Being able to do what one feels is important | 76 | 74 | 77 | 77 | 77 | 66 | 68 | 80 |
| Continuing to learn | 60 | 54 | 65 | 60 | 61 | 56 | 57 | 61 |
| Being socially connected | 58 | 50 | 65 | 59 | 59 | 56 | 50 | 63 |
| Being valued | 58 | 48 | 66 | 57 | 58 | 55 | 53 | 60 |
| Being a contributor to society | 43 | 38 | 47 | 43 | 44 | 36 | 37 | 46 |
Q14. How much do you associate the term 'healthy aging' with each of the following?
Base: Total sample
Gender
Age
Education
Household Income
Language
Health Status and Quality of Life
Region
All respondents were given an opportunity, on an unprompted basis, to offer additional suggestions in terms of anything else they associated with healthy aging. Most (55%) did not have anything else to add. Among those who provided suggestions, responses were quite varied with under one in ten commenting that they associate healthy aging with generally staying healthy and caring for oneself (7%) and staying engaged whether that is through hobbies and interests (7%) or via social and family connections (7%). A very small percentage of respondents associate healthy aging with financial stability (4%), a positive mental outlook (4%), the ability to access medical services (4%) and general self-sufficiency or independence (4%). Other responses were offered, but only by 2% or fewer respondents.
Additional analysis by demographic sub-groups is limited given the small cell sizes in terms of the various responses offered.
| TOTAL | Male | Female | Age 50-64 |
Age 65-79 |
Age 80+ |
Medical condition and/or disability YES |
Medical condition and/or disability NO |
|
|---|---|---|---|---|---|---|---|---|
| n= | 2477 | 1167 | 1310 | 1285 | 897 | 296 | 880 | 1587 |
| % | % | % | % | % | % | % | % | |
| Take care of yourself/Staying healthy/Diet/Mentally astute | 7 | 8 | 7 | 7 | 8 | 8 | 7 | 8 |
| Active/Hobbies/Doing stuff for yourself | 7 | 7 | 7 | 6 | 8 | 9 | 7 | 7 |
| Social life/Community/Friends and family | 7 | 5 | 9 | 6 | 8 | 12 | 8 | 7 |
| Financial Stability/Independence | 4 | 4 | 5 | 5 | 4 | 4 | 5 | 4 |
| Good outlook/Positive mentality/Happy | 4 | 4 | 4 | 3 | 4 | 9 | 4 | 4 |
| Able to access medical help/Able to deal with medical concerns | 4 | 4 | 4 | 4 | 4 | 3 | 4 | 3 |
| Independence/Agency | 4 | 3 | 4 | 3 | 4 | 5 | 4 | 4 |
| Have support | 2 | 1 | 3 | 2 | 2 | 2 | 2 | 2 |
| Being a positive role model/Contribute to society/Valued by people | 1 | 1 | 2 | 1 | 2 | 1 | 1 | 1 |
| Live in your own home | 1 | <1 | 1 | <1 | 1 | 2 | 1 | <1 |
| Not concerned about death/aging | 1 | 1 | 1 | <1 | 1 | 1 | <1 | 1 |
| No, there is nothing else I associate with healthy aging / None* | 55 | 59 | 51 | 59 | 53 | 42 | 53 | 56 |
| Other (including <1% mentions) | 4 | 3 | 4 | 3 | 4 | 7 | 4 | 3 |
| Don't Know | 6 | 6 | 6 | 6 | 5 | 7 | 6 | 6 |
Q15. Is there anything else that you associate with 'healthy aging?'
Base: Total sample who answered the open end.
There are a number of factors which contribute to one's ability to age in a healthy way. These include social and family connections as well as community-based infrastructure and access to services that help to maintain and improve physical, mental and social health, promote independence and quality of life as one ages.
Respondents were read (or shown in the case of the online survey) a select list of factors which enable healthy aging and asked whichtwothey felt were most important. They were also prompted to provide responses in addition to those read or shown to them if they felt the list provided excluded other factors which they deemed to be important to healthy aging.
As shown in Figure 10 below, just over half identify access to health services (51%) as one of the two most important factors contributing to healthy aging, followed by being close to family (44%). Between one in five and one in four respondents identify social networks and friends (25%), being able to get outdoors (22%), and accessible housing, buildings and transit (20%) among their top two choices. Physical and cognitive supports is identified as a 'top two' factor enabling healthy aging by just over one in ten (16%), while access to cultural events is identified by relatively few respondents (6%).
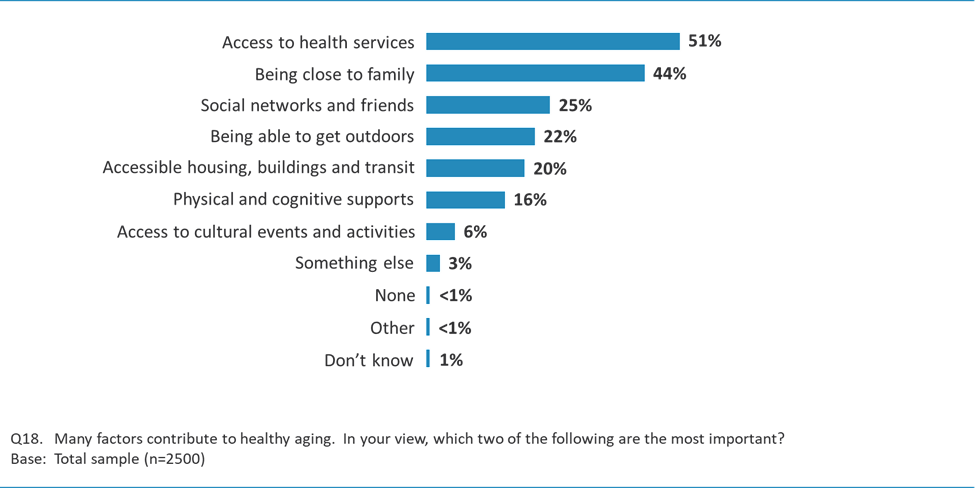
| Access to health services | 51% |
| Being close to family | 44% |
| Social networks and friends | 25% |
| Being able to get outdoors | 22% |
| Accessible housing, buildings and transit | 20% |
| Physical and cognitive supports | 16% |
| Access to cultural events and activities | 6% |
| Something else | 3% |
| None | <1% |
| Other | <1% |
| Don't know | 1% |
There are several variations of note in responses to this question as shown in Table 14 and described in the analysis below.
| TOTAL | Male | Female | Age 50-64 |
Age 65-79 |
Age 80+ |
Medical condition and/or disability YES |
Medical condition and/or disability NO |
|
|---|---|---|---|---|---|---|---|---|
| n= | 2500 | 1175 | 1325 | 1300 | 900 | 300 | 885 | 1604 |
| % | % | % | % | % | % | % | % | |
| Access to health services | 51 | 52 | 51 | 52 | 52 | 48 | 52 | 51 |
| Being close to family | 44 | 40 | 48 | 43 | 43 | 51 | 42 | 45 |
| Social networks and friends | 25 | 25 | 26 | 25 | 26 | 24 | 23 | 27 |
| Being able to get outdoors | 22 | 25 | 19 | 19 | 26 | 23 | 21 | 22 |
| Accessible housing, buildings and transit | 20 | 19 | 21 | 22 | 18 | 17 | 24 | 18 |
| Physical and cognitive supports like educational and exercise programs | 16 | 17 | 16 | 19 | 15 | 11 | 15 | 17 |
| Access to cultural events and activities | 6 | 6 | 6 | 6 | 5 | 6 | 5 | 6 |
| Something else (includes mentions <1%) | 3 | 4 | 3 | 3 | 4 | 4 | 4 | 3 |
| None | <1 | <1 | <1 | <1 | <1 | - | 1 | <1 |
| Other | <1 | <1 | <1 | <1 | <1 | 1 | <1 | <1 |
| Don't Know | 1 | 1 | 1 | 1 | 1 | 2 | 1 | 1 |
Q18. Many factors contribute to healthy aging. In your view, which two of the following are the most important? Is it...?
Base: Total sample
Gender
Age
Education
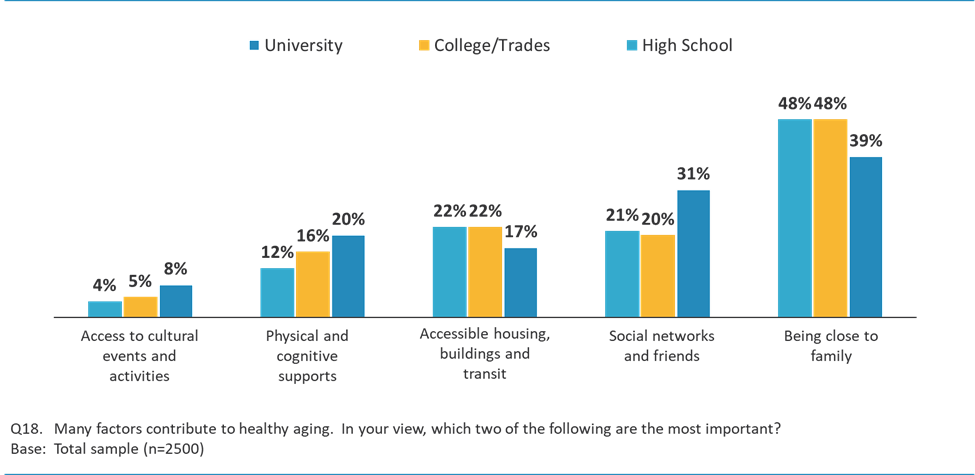
| Factor | University | College/Trades | High School |
|---|---|---|---|
| Access to cultural events and activities | 8% | 5% | 4% |
| Physical and cognitive supports | 20% | 16% | 12% |
| Accessible housing, buildings and transit | 17% | 22% | 22% |
| Social networks and friends | 31% | 20% | 21% |
| Being close to family | 39% | 48% | 48% |
Household Income
Employment Status
Visible Minority
Language
Health Status and Quality of Life
Region
Respondents were asked several questions regarding the extent to which they view their community as age-friendly, and to assess the availability of and access to various services and features within their community which support healthy aging. Responses to these questions illuminate where there are perceived gaps and/or barriers to healthy aging at the community level.
Most respondents view their community as age-friendly (84%), with one-third describing their community as very age-friendly (33%) and just over half describing it as at least somewhat age-friendly (51%). Just over one in ten feel their community is not particularly age-friendly (15%), describing it as not very age-friendly (12%) or not age-friendly at all (2%).
| TOTAL | Male | Female | Age 50-64 |
Age 65-79 |
Age 80+ |
Medical condition and/or disability YES |
Medical condition and/or disability NO |
|
|---|---|---|---|---|---|---|---|---|
| n= | 2500 | 1175 | 1325 | 1300 | 900 | 300 | 885 | 1604 |
| % | % | % | % | % | % | % | % | |
| TOTAL - VERY/SOMEWHAT AGE-FRIENDLY | 84 | 84 | 83 | 80 | 88 | 87 | 82 | 85 |
| Very age-friendly | 33 | 32 | 33 | 28 | 35 | 46 | 32 | 33 |
| Somewhat age-friendly | 51 | 52 | 50 | 52 | 53 | 41 | 50 | 52 |
| Not very age-friendly | 12 | 12 | 12 | 15 | 9 | 10 | 13 | 12 |
| Not age-friendly at all | 2 | 2 | 3 | 3 | 2 | 1 | 4 | 2 |
| TOTAL - NOT VERY/NOT AT ALL AGE-FRIENDLY | 15 | 14 | 15 | 18 | 12 | 10 | 17 | 14 |
| Don't know | 2 | 2 | 2 | 2 | 1 | 3 | 2 | 1 |
Q16. Healthy aging is about developing and maintaining the physical and cognitive abilities that enable wellbeing as one ages. It is supported by environments that allow people to do what they value as they age. Overall, would you describe the community in which you currently live as being...?
Base: Total sample (n=2500)
Across all regions and demographic sub-groups, a majority of respondents rate their community as age-friendly. There are very few variations of note, other than those mentioned below.
Age
Home Ownership Status
Language
Health Status and Quality of Life
Region
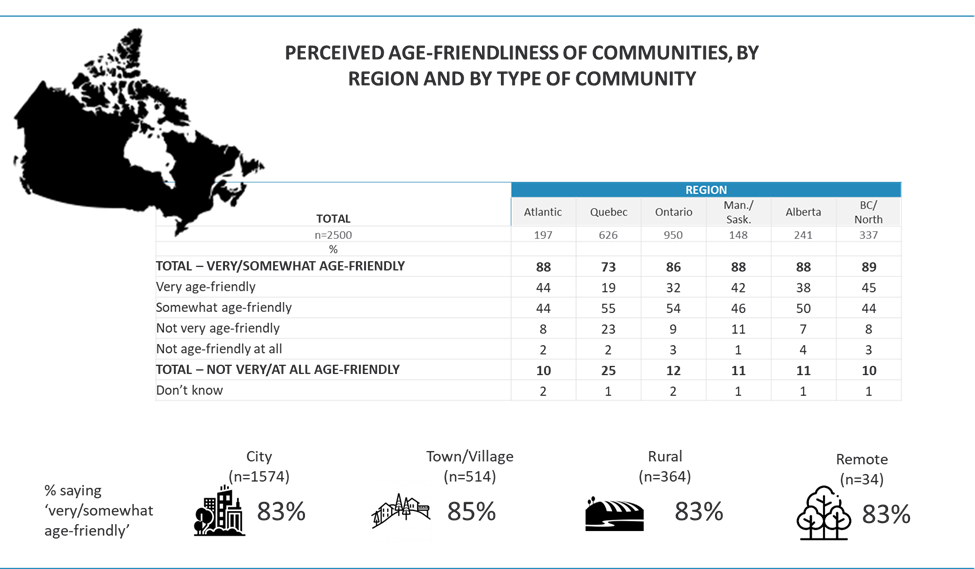
| Rating | Atlantic | Quebec | Ontario | Manitoba/ Saskatchewan | Alberta | British Columbia/ North |
|---|---|---|---|---|---|---|
| Total very/somewhat age-friendly | 88% | 73% | 86% | 88% | 88% | 89% |
| Very age-friendly | 44% | 19% | 32% | 42% | 38% | 45% |
| Somewhat age-friendly | 44% | 55% | 54% | 46% | 50% | 44% |
| Not very age-friendly | 8% | 23% | 9% | 11% | 7% | 8% |
| Not age-friendly at all | 2% | 2% | 3% | 1% | 4% | 3% |
| Total not very/at all age-friendly | 10% | 25% | 12% | 11% | 11% | 10% |
| Don't know | 2% | 1% | 2% | 1% | 1% | 1% |
| Community Type | Base size (n) | Very/Somewhat age-friendly |
|---|---|---|
| City | 1574 | 83% |
| Town/Village | 514 | 85% |
| Rural | 364 | 83% |
| Remote | 34 | 83% |
To further evaluate the perceived age-friendliness of communities across Canada, respondents were asked to provide ratings of their community in 11 areas related to aspects of community services, infrastructure, employment and volunteer opportunities, among others. Most respondents tend to offer a rating of good or fairon many of the features evaluated.
When examining only that proportion of respondents who provide the highest rating - a rating of good or excellent - it is clear that the features fall into at least three categories or tiers based on these ratings (see Figure 13 below):
Communities receive high ratings (i.e., more than half offer a rating of good or excellent) for being safe and providing easy access to buildings and public spaces (64%), having accessible and affordable high-speed internet (60%), community-based social and recreational activities and events (58%), and opportunities for lifelong learning (57%).
The ratings of communities drop slightly (to between 4 and 5 in ten respondents saying good/excellent) for exercise programs for older adults (50%), employment and volunteer opportunities for older adults (50%), although it is notable that one in ten respondents express some uncertainty in assessing their community on these features. Similar numbers rate their community as good or excellent with respect to access to health care, mental health and dental care services (49%), well-maintained sidewalks (46%) and accessible and affordable transit (41%).
Lower ratings are obtained regarding in-home services that support independent living (38%), with 17% saying they are unsure how to rate their community on this feature. The lowest rating is with respect to affordable housing where just one in five (21%) evaluate their community as good or excellent.
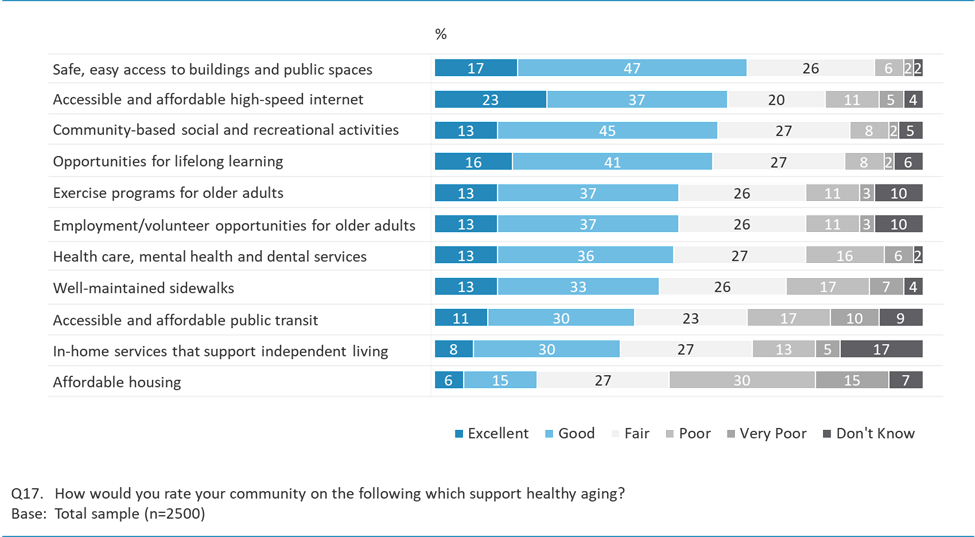
| Area | Excellent | Good | Fair | Poor | Very Poor | Don't know |
|---|---|---|---|---|---|---|
| Safe, easy access to buildings and public spaces | 17% | 47% | 26% | 6% | 2% | 2% |
| Accessible and affordable high-speed internet | 23% | 37% | 20% | 11% | 5% | 4% |
| Community-based social and recreational activities | 13% | 45% | 27% | 8% | 2% | 5% |
| Opportunities for lifelong learning | 16% | 41% | 27% | 8% | 2% | 6% |
| Exercise programs for older adults | 13% | 37% | 26% | 11% | 3% | 10% |
| Employment/volunteer opportunities for older adults | 13% | 37% | 26% | 11% | 3% | 10% |
| Health care, mental health and dental services | 13% | 36% | 27% | 16% | 6% | 2% |
| Well-maintained sidewalks | 13% | 33% | 26% | 17% | 7% | 4% |
| Accessible and affordable public transit | 11% | 30% | 23% | 17% | 10% | 9% |
| In-home services that support independent living | 8% | 30% | 27% | 13% | 5% | 17% |
| Affordable housing | 6% | 15% | 27% | 30% | 15% | 7% |
Table 16 highlights select demographic variations on this question, followed by additional detailed analysis across the wider range of demographic and regional variables.
| TOTAL | Male | Female | Age 50-64 |
Age 65-79 |
Age 80+ |
Medical condition and/or disability YES |
Medical condition and/or disability NO |
|
|---|---|---|---|---|---|---|---|---|
| n= | 2500 | 1175 | 1325 | 1300 | 900 | 300 | 885 | 1604 |
| % | % | % | % | % | % | % | % | |
| Safe, easy to access buildings and public spaces | 64 | 67 | 62 | 58 | 70 | 71 | 58 | 68 |
| Accessible and affordable high-speed Internet | 60 | 64 | 56 | 56 | 65 | 62 | 56 | 62 |
| Community-based social and recreational activities and events | 58 | 60 | 56 | 56 | 59 | 63 | 52 | 61 |
| Opportunities for lifelong learning | 57 | 58 | 56 | 56 | 57 | 61 | 52 | 59 |
| Exercise programs for older adults | 50 | 50 | 51 | 49 | 51 | 54 | 44 | 54 |
| Employment and volunteer opportunities for older adults | 50 | 51 | 49 | 50 | 51 | 45 | 43 | 54 |
| Health care, mental health and dental care services | 49 | 52 | 45 | 43 | 50 | 65 | 46 | 50 |
| Well-maintained sidewalks | 46 | 48 | 43 | 42 | 48 | 54 | 43 | 47 |
| Accessible and affordable public transit | 41 | 43 | 38 | 40 | 40 | 45 | 39 | 41 |
| In-home services that support independent living | 38 | 41 | 35 | 36 | 37 | 47 | 38 | 38 |
| Affordable housing | 21 | 23 | 19 | 17 | 23 | 32 | 20 | 22 |
Q17. How would you rate your community on the following, which support healthy aging?
Base: Total sample
Gender
Education
Household Income
Home Ownership Status
Household Composition and Marital Status
Visible Minority
Language
Health Status and Quality of Life
| TOTAL | Personal Health Status | Quality of Life | ||||
|---|---|---|---|---|---|---|
| Excellent/Good | Poor/Very Poor | Excellent/Good | Poor/Very Poor | |||
| n= | 2500 | 1761 |
175 | 1959 | 103 | |
| % | % | % |
% | % | ||
| Safe, easy to access buildings and public spaces | 64 | 69 | 43 |
69 | 35 | |
| Accessible and affordable high-speed Internet | 60 | 64 | 45 |
64 | 40 | |
| Community-based social and recreational activities and events | 58 | 63 | 38 |
64 | 27 | |
| Opportunities for lifelong learning | 57 | 61 | 36 |
61 | 24 | |
| Exercise programs for older adults | 50 | 56 | 29 |
56 | 22 | |
| Employment and volunteer opportunities for older adults | 50 | 55 | 24 |
56 | 19 | |
| Health care, mental health and dental care services | 49 | 52 | 36 |
52 | 27 | |
| Well-maintained sidewalks | 46 | 48 | 38 |
48 | 24 | |
| Accessible and affordable public transit | 41 | 43 | 33 |
42 | 32 | |
| In-home services that support independent living | 38 | 40 | 30 |
39 | 22 | |
| Affordable housing | 21 | 23 | 17 |
23 | 8 | |
Q17. How would you rate your community on the following, which support healthy aging?
Base: Total sample
Region
Type of Community
Respondents are interested in receiving more information on the topic of healthy aging, specifically information related to aging at home and maintaining physical and cognitive health as one ages. However, only one quarter recall having seen anything related to healthy aging from the Government of Canada in recent years.
Medical professionals are viewed as key to delivering this type of information, although allied health professionals such as pharmacists, the Public Health Agency and Health Canada, as well as experts on the topic also have a role to play. Additionally, friends and family members and health-related sources are viewed by some as reliable conduits of information on this topic.
One quarter (25%) of Canadians aged 50 and older claim to have seen something from the Government of Canada or PHAC on the topic of healthy aging within the last two years. It is important to note that the level of recall may be a factor of the respondent having either sought out information proactively or having received it without necessarily being able to accurately recall the jurisdiction or agency which was responsible for producing and disseminating the information.
| TOTAL | Male | Female | Age 50-64 |
Age 65-79 |
Age 80+ |
Medical condition and/or disability YES |
Medical condition and/or disability NO |
|
|---|---|---|---|---|---|---|---|---|
| n= | 2500 | 1175 | 1325 | 1300 | 900 | 300 | 885 | 1604 |
| % | % | % | % | % | % | % | % | |
| Yes | 25 | 22 | 29 | 23 | 29 | 24 | 24 | 26 |
| No | 67 | 71 | 64 | 71 | 63 | 66 | 69 | 67 |
| Don't know | 7 | 7 | 7 | 6 | 8 | 10 | 7 | 8 |
Q20. Do you recall seeing anything from the Government of Canada or the Public Health Agency of Canada on the topic of healthy aging in the last 2 years?
Base: Total sample
Gender
Age
Language
Region
There is significant interest in information related to healthy aging, although the level of interest varies considerably by topic (see Figure 14). In particular, respondents want to know more about maintaining physical and cognitive health and about aging at home - a majority (54%) say they are very interested in learning more about both of these aspects of healthy aging. Similarly, a near majority (48%) are very interested in general information about healthy aging.
About two in five respondents express a high level of interest in information regarding healthy nutrition (42%) and immunization (40%). The recent pandemic, particularly the impact of COVID-19 on the elderly population and the initial priority placed on vaccinations for people 60 years of age and older, may have influenced older adults' vaccination attitudes and behaviours and thus their level of interest in the topic of immunization. Additional work in this area would be useful in terms of better understanding the nature of the correlation and the degree to which any changes in attitudes have resulted in older adults taking a greater interest in the importance of vaccines.
Relative to the above-noted aspects of healthy aging, fewer respondents (about one third) are keenly interested topics such as oral health (34%), preventing elder abuse (34%), and falls and injuries (33%).
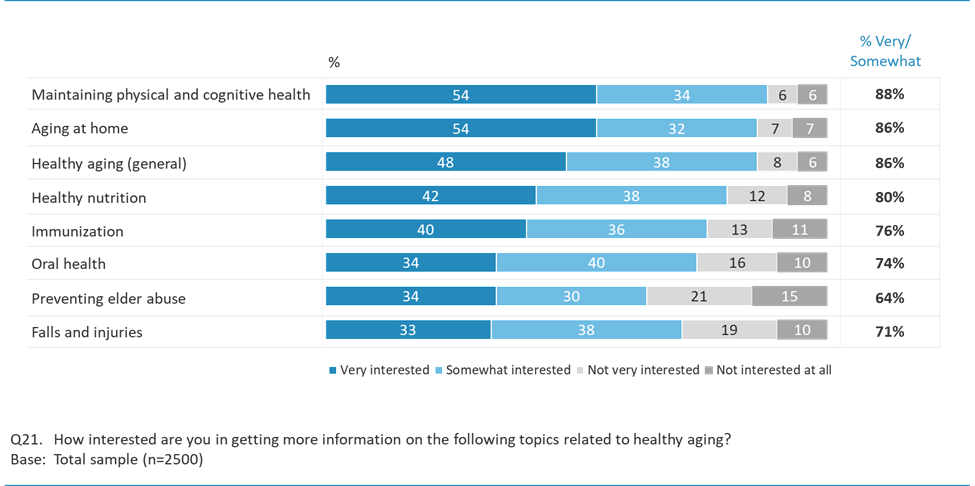
| Topic | Very interested | Somewhat interested | Not very interested | Not interested at all | Total very/somewhat interested |
|---|---|---|---|---|---|
| Maintaining physical and cognitive health | 54% | 34% | 6% | 6% | 88% |
| Aging at home | 54% | 32% | 7% | 7% | 86% |
| Healthy aging (general) | 48% | 38% | 8% | 6% | 86% |
| Healthy nutrition | 42% | 38% | 12% | 8% | 80% |
| Immunization | 40% | 36% | 13% | 11% | 76% |
| Oral health | 34% | 40% | 16% | 10% | 74% |
| Preventing elder abuse | 34% | 30% | 21% | 15% | 64% |
| Falls and injuries | 33% | 38% | 19% | 10% | 71% |
Interest varies across demographic groups as highlighted in the table below and in the additional information that follows.
| TOTAL | Male | Female | Age 50-64 |
Age 65-79 |
Age 80+ |
Medical condition and/or disability YES |
Medical condition and/or disability NO |
|
|---|---|---|---|---|---|---|---|---|
| n= | 2500 | 1175 | 1325 | 1300 | 900 | 300 | 885 | 1604 |
| % | % | % | % | % | % | % | % | |
| Maintaining physical and cognitive health | 54 | 49 | 58 | 52 | 56 | 57 | 54 | 54 |
| Aging at home | 54 | 50 | 58 | 49 | 58 | 66 | 57 | 53 |
| Healthy aging (general) | 48 | 42 | 53 | 46 | 49 | 54 | 48 | 48 |
| Healthy nutrition | 42 | 38 | 45 | 40 | 43 | 46 | 44 | 41 |
| Immunization | 40 | 38 | 42 | 32 | 46 | 55 | 45 | 37 |
| Oral health | 34 | 29 | 38 | 31 | 36 | 42 | 39 | 32 |
| Preventing elder abuse | 34 | 30 | 37 | 32 | 35 | 39 | 37 | 32 |
| Falls and injuries | 33 | 28 | 37 | 28 | 35 | 45 | 39 | 29 |
Q21. How interested are you in getting more information on the following topics related to healthy aging?
Base: Total sample
Gender
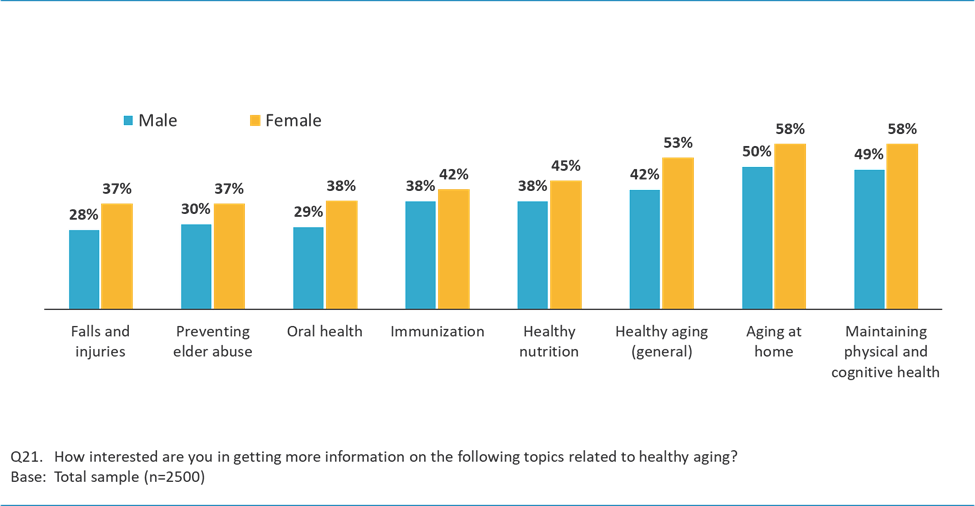
| Topic | Male | Female |
|---|---|---|
| Falls and injuries | 28% | 37% |
| Preventing elder abuse | 30% | 37% |
| Oral health | 29% | 38% |
| Immunization | 38% | 42% |
| Healthy nutrition | 38% | 45% |
| Healthy aging (general) | 42% | 53% |
| Aging at home | 50% | 58% |
| Maintaining physical and cognitive health | 49% | 58% |
Age
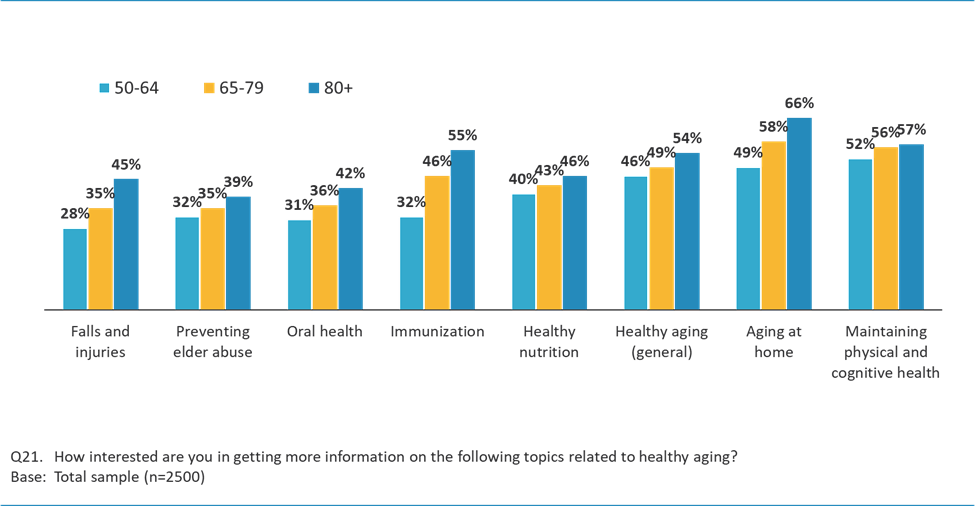
| Topic | 50-64 | 65-79 | 80+ |
|---|---|---|---|
| Falls and injuries | 28% | 35% | 45% |
| Preventing elder abuse | 32% | 35% | 39% |
| Oral health | 31% | 36% | 42% |
| Immunization | 32% | 46% | 55% |
| Healthy nutrition | 40% | 43% | 46% |
| Healthy aging (general) | 46% | 49% | 54% |
| Aging at home | 49% | 58% | 66% |
| Maintaining physical and cognitive health | 52% | 56% | 57% |
Education
Household Income
Home Ownership Status
Household Composition and Marital Status
Visible Minority
Language
Health Status and Quality of Life
Region
Type of Community
Interest varies significantly between those who recall seeing something from the Government of Canada or the Public Health Agency of Canada on the topic of healthy aging over the last two years and those who do not, with the former group more likely to be very interested in all of the topics. While public recall of informational campaigns may not be entirely accurate, and there is often some degree of confusion as to the sponsoring agency or level of government, these results do suggest that educational marketing has had an impact in terms of generating further interest on important and useful topics for Canadians in the 50+ demographic.
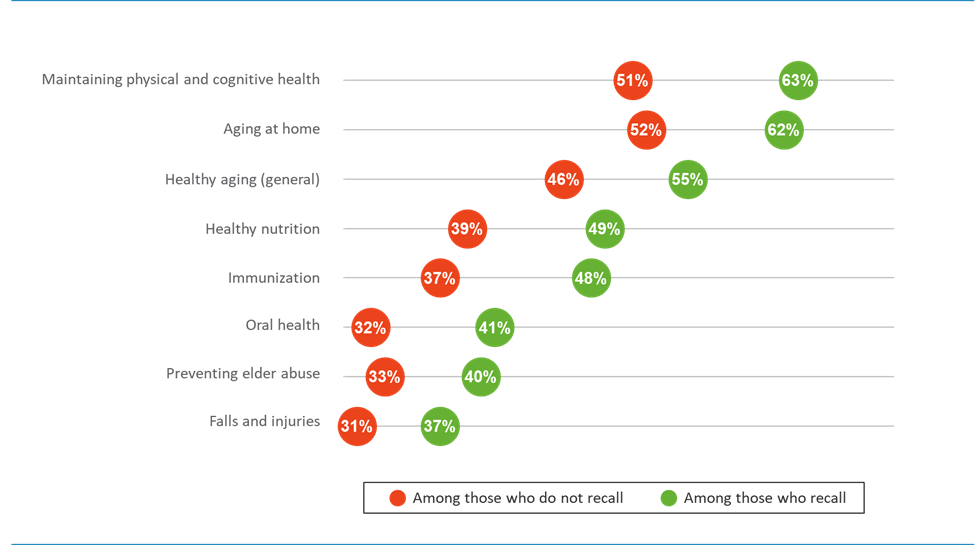
| Topic | Among those who do not recall | Among those who recall |
|---|---|---|
| Maintaining physical and cognitive health | 51% | 63% |
| Aging at home | 52% | 62% |
| Healthy aging (general) | 46% | 55% |
| Healthy nutrition | 39% | 49% |
| Immunization | 37% | 48% |
| Oral health | 32% | 41% |
| Preventing elder abuse | 33% | 40% |
| Falls and injuries | 31% | 37% |
All respondents were given an opportunity to identify from a list of possible sources of information on the topic of healthy aging the two they most trust. By a wide margin, respondents (70%) selected medical professionals, including doctors and nurses, as one of the two most trusted sources. About one in five identified family and friends (19%) or pharmacists (18%). Just over one in ten indicate they trust the Public Health Agency of Canada/Health Canada (13%), researchers or experts in the area (12%) and health-related websites (12%). With much less frequency, some respondents indicated trusting their provincial/territorial or municipal government (6%), the Government of Canada (4%), the news media (4%) and online media (3%). Other sources were mentioned by 1% or fewer respondents.
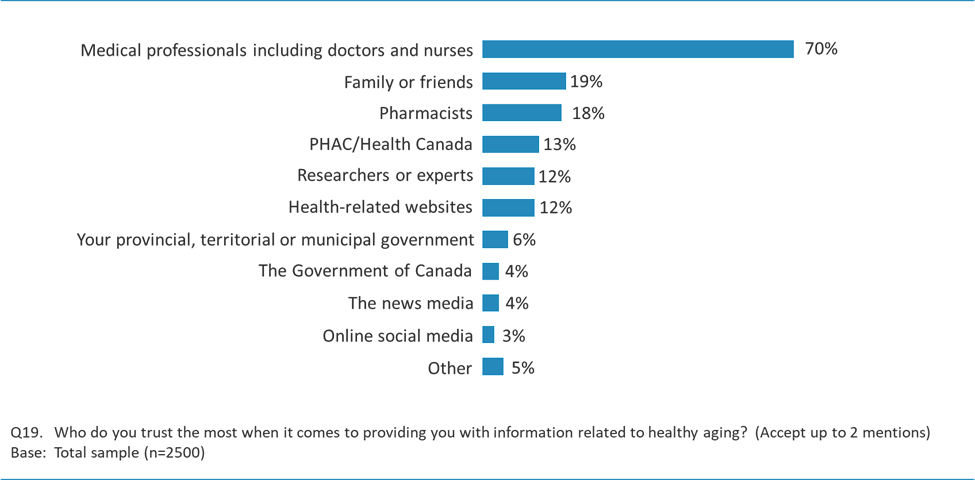
| Medical professionals including doctors and nurses | 70% |
| Family or friends | 19% |
| Pharmacists | 18% |
| PHAC/Health Canada | 13% |
| Researchers or experts | 12% |
| Health-related websites | 12% |
| Your provincial, territorial or municipal government | 6% |
| The Government of Canada | 4% |
| The news media | 4% |
| Online social media | 3% |
| Other | 5% |
Trust in various sources varies across demographic groups and regions, as detailed below.
| TOTAL | Male | Female | Age 50-64 |
Age 65-79 |
Age 80+ |
Medical condition and/or disability YES |
Medical condition and/or disability NO |
|
|---|---|---|---|---|---|---|---|---|
| n= | 2500 | 1175 | 1325 | 1300 | 900 | 300 | 885 | 1604 |
| % | % | % | % | % | % | % | % | |
| Medical professionals including doctors and nurses | 70 | 71 | 69 | 68 | 72 | 71 | 72 | 69 |
| Family or friends | 19 | 17 | 21 | 19 | 17 | 27 | 20 | 18 |
| Pharmacists | 18 | 16 | 20 | 16 | 20 | 22 | 19 | 17 |
| The Public Health Agency of Canada/Health Canada | 13 | 11 | 14 | 13 | 13 | 10 | 12 | 13 |
| Researchers or experts | 12 | 10 | 13 | 14 | 10 | 6 | 11 | 13 |
| Health-related websites | 12 | 11 | 12 | 13 | 12 | 6 | 11 | 13 |
| Your provincial, territorial or municipal government | 6 | 8 | 4 | 6 | 5 | 5 | 5 | 7 |
| The Government of Canada | 4 | 5 | 3 | 4 | 4 | 3 | 3 | 4 |
| The news media | 4 | 3 | 4 | 2 | 4 | 6 | 3 | 4 |
| Online social media | 3 | 3 | 3 | 3 | 4 | 2 | 3 | 3 |
| Other | 5 | 4 | 5 | 5 | 4 | 6 | 5 | 5 |
| All of the above | <1 | <1 | 1 | <1 | <1 | 1 | <1 | <1 |
| Trust themselves/Do their own research | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 2 |
| Alternative medicine | <1 | - | <1 | <1 | <1 | - | - | <1 |
| Books/Written content | <1 | <1 | 1 | 1 | - | 1 | 1 | <1 |
| Community centres | <1 | <1 | <1 | <1 | <1 | 2 | <1 | 1 |
| World Health Organization | <1 | <1 | <1 | <1 | - | - | <1 | - |
| None | 1 | 1 | <1 | 1 | 1 | 1 | 1 | <1 |
| Other | <1 | - | <1 | <1 | <1 | - | <1 | <1 |
| Don`t Know | 1 | 1 | 1 | 1 | 1 | 2 | 1 | 1 |
Q19. Who do you trust the most when it comes to providing you with information related to healthy aging? (UP TO TWO MENTIONS)
Base: Total sample
Gender
Age
Education
Household Income
Visible Minority
Language
Health Status and Quality of Life
Recall of Information on Healthy Aging from Government of Canada/PHAC
Region
Type of Community
As a final question on each of the telephone and online surveys, respondents were invited to share additional comments about healthy aging with a particular focus on areas that may not have been covered within the questionnaire.
While most participants (61% overall - 86% of those who completed the online survey and 55% of those who responded to the telephone survey) did not provide any additional thoughts, those who did offered an array of commentary. Feedback focused on several areas: issues related to health care and home care (8%); general support for and services aimed at an aging population (6%), as well as the cost of living and financial pressures affecting seniors (5%). Other concerns were mentioned by fewer than 5% of respondents but reflect the many aspects of and challenges related to aging that are on the minds of those aged 50 and older in Canada.
| TOTAL | Male | Female | Age 50-64 |
Age 65-79 |
Age 80+ |
Medical condition and/or disability YES |
Medical condition and/or disability NO |
|
|---|---|---|---|---|---|---|---|---|
| n= | 2500 | 1175 | 1325 | 1300 | 900 | 300 | 885 | 1604 |
| % | % | % | % | % | % | % | % | |
| Better access to health care is needed/Access to home care/Not enough healthcare/medical professionals (e.g., nurses, do | 8 | 7 | 10 | 8 | 9 | 7 | 9 | 8 |
| Accommodating the aging population/Community support/Access to public services (i.e., assistance for seniors, leisure ac | 6 | 4 | 7 | 5 | 5 | 7 | 7 | 5 |
| Cost of living/Financial costs of aging/Expenses/Seniors not having enough money to live | 5 | 4 | 6 | 5 | 5 | 3 | 6 | 4 |
| Aging gracefully/Looking after yourself/Exercising/Keeping physically and mentally active | 4 | 4 | 4 | 4 | 4 | 7 | 4 | 4 |
| Government not doing enough/Doesn't care about aging/Should be government focus | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 3 |
| Learning to accept aging/Positive attitude/Being happy | 2 | 2 | 2 | 1 | 3 | 4 | 2 | 2 |
| Long term care/Regulations on private seniors homes/Fear of having to live in care homes | 2 | 1 | 3 | 2 | 2 | 1 | 1 | 2 |
| Affordable housing/Seniors housing/Making it easier financially to stay in my home | 1 | 1 | 2 | 1 | 2 | 1 | 3 | 1 |
| Food/Nutrition/Healthy diet | 1 | 1 | 1 | 1 | 1 | 2 | 1 | 1 |
| Mental health/Mental health issues | 1 | 1 | 1 | 1 | 1 | 1 | 2 | 1 |
| Respect/More respect for seniors/A sense of responsibility to the elderly | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Spirituality/Faith/Religious beliefs | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Prescription drugs from doctors/Seniors on pills/Cost of drugs | 1 | <1 | 1 | <1 | 1 | 1 | 1 | <1 |
| Safety at home/Feeling safe | <1 | - | 1 | 1 | <1 | 1 | 1 | <1 |
| Assisted suicide/Assisted dying/MAID (medical assistance in dying) | <1 | <1 | 1 | <1 | <1 | 1 | <1 | <1 |
| Concerns about disability/Tax credits/Additional services for people with disabilities | <1 | <1 | <1 | 1 | <1 | 1 | 1 | <1 |
| Dementia is a huge fear/More resources need to be put towards dementia | <1 | <1 | <1 | <1 | <1 | 1 | <1 | <1 |
| Alcohol/Drugs/Smoking/No smoking and no drinking | <1 | - | <1 | - | <1 | 1 | <1 | <1 |
| Other | 4 | 4 | 4 | 5 | 4 | 3 | 5 | 4 |
| Don't know/Refused/Not applicable | 6 | 7 | 6 | 5 | 7 | 9 | 6 | 7 |
| Nothing else/Nothing/All Good/Covered it all | 61 | 64 | 58 | 64 | 59 | 55 | 58 | 63 |
| Prefer not to answer/No Answer | 1 | 1 | 1 | 1 | 1 | 2 | 1 | 1 |
Q33. What didn't we ask as part of this survey, that you would like us to know about healthy aging?
Base: Total sample
Other than this broad thematic analysis of the feedback provided, additional analysis on this question has not been undertaken as part of the quantitative survey due to the wide variety of responses received. Any further review should be undertaken applying techniques which are more suitable to qualitative analysis.
Participants in nineteen groups engaged in conversations regarding their perspectives and outlook towards aging. All groups were comprised of participants aged 50 and older.
To begin, participants were asked to share how they felt about getting older, including any words or images that came to mind when they thought about aging. Across all groups participants shared a wide range of perspectives related to both the positive and negative aspects of getting older.
Several expressed that aging was not something that personally worried them and a number commented that they were looking forward to embarking upon this chapter of their lives. Among these participants, it was felt that so long as one maintained a positive attitude and acknowledged that getting older is a natural part of life, that aging could be an enjoyable and fulfilling process. A number commented that they had worked hard to maintain their physical health and had also been taking steps to ensure they engaged in mentally stimulating activities on a daily basis. A few spoke of the importance of continuing to establish goals related to one's physical health and personal pursuits, believing it was important for individuals to have something they were working towards as they aged. A large number also spoke of the importance of having family and other loved ones in their lives as they get older. It was thought that time with family provided a great deal of fulfillment and that experiences such as playing with their grandchildren and enjoying holidays with family were among the things they looked forward to the most in the years to come. Some also believed that getting older would provide them with more time to focus on relaxing and pursuing their passions as they entered into their retirement years.
Many also spoke of the negative aspects of getting older and their concerns related to how their lives may change as they age. Several were worried about experiencing a loss of mobility, diminished energy, and a general slowing down of their daily lives. Related to this, some commented that they were already dealing with chronic health conditions such as arthritis that had begun to impede their movements and physical activity. A number also mentioned concerns related to how their physical appearance may change, including common signs of aging such as graying hair and wrinkles. Some expressed fears related to the potential of suffering a sudden medical event (such as a stroke or heart attack) that may unexpectedly and drastically alter their quality of life going forward. Several voiced concerns about their cognitive abilities as they age, with a number who expressed disquietude about memory loss and degenerative diseases such as Alzheimer's and dementia. Financial concerns were also top of mind among participants who were worried about their ability to live on a fixed income, especially during periods of high inflation and economic uncertainty. Among those participants, there was a feeling of uncertainty around their ability to physically and/or financially support themselves as they age. In relation to this, some expressed fears that a decline in their physical and financial health may result in them having to enter a long-term care (LTC) facility. A few also raised concerns related to systemic issues such as the ability of the healthcare system to support a growing number of seniors in the decades to come. Related to this, some commented that the perceived strain placed on the healthcare system as a result of the COVID-19 pandemic had heightened their concerns that there would not be enough resources to accommodate them as they aged.
When asked whether, on balance, they felt mostly positive or negative about the prospect of aging, a much larger number indicated feeling optimistic about getting older compared to those who were more negative in their outlooks. Several spoke positively of their experience watching their children become adults as well as spending time with their grandchildren. Among those who were retired or working less, a number spoke about their ability to better enjoy their time at home and in their community, as well as having more time for hobbies, travel, and other recreational pursuits. The view was also shared that aging is unavoidable, so it was best to embrace the process and enjoy the time they had left. A few expressed feeling privileged to have had the chance to age into their senior years, commenting that not everyone has the opportunity. Among those who felt more negatively about aging, several reiterated issues related to diminished mobility, compounding issues related to their mental health, decreased ability to partake in activities they once enjoyed, and the financial challenges of surviving on a fixed income. Participants also reported feeling less visible as they aged, believing that they now were generally paid less attention to by those around them. Regarding their financial health, a number expressed concerns about the difficulties they would likely encounter if they attempted to return to the workforce, believing it was very difficult for seniors to find well paying jobs given their older age.
Participants over the age of 70 were asked whether their experience with aging had thus far aligned with their expectations. For several, aging had been more enjoyable than expected, with a number feeling that they had acquired considerable perspective as they had gotten older as well as undergoing spiritual growth. A few who identified as Indigenous mentioned that they had taken steps towards reconnecting with their culture in recent years. Some mentioned that the aging process had been difficult due to the sadness associated with losing loved ones, including parents, spouses, and close friends. A number, however, indicated that this had made the time they spent with their remaining loved ones all the more precious to them. A small number discussed having encountered difficulties related to health conditions such as arthritis and other chronic issues, which had made the aging process more complicated than they had anticipated.
Discussing the goals they had for getting older, many reported focusing more on their physical health and fitness. Maintaining their personal fitness had been a long-term goal for several while others indicated that they had recently renewed efforts to get back into shape as a way to lead a more active lifestyle. A few commented that they wanted to stay as physically fit as possible in their senior years in order to remain in their own homes for longer and continue to take care of themselves without the assistance of a personal support worker (PSW). A large number also mentioned wanting to spend as much time as possible with their children and grandchildren, believing this to be a very fulfilling experience. Other goals mentioned by participants included travelling more, learning new languages and skills, and becoming more involved in charitable and non-profit organizations as a way to enact positive change in their communities.
Asked to identify the key challenges individuals faced as a result of aging, comments focused primarily on three key areas. These included:
Questioned whether there were some groups of seniors more likely to face these challenges than others, it was largely expected that those living alone, low-income individuals, and persons living with disabilities would likely struggle more than others. Additionally, it was also expected that those unfamiliar with technology or who did not speak English or French would likely face a higher degree of difficulty in having their financial and health-related needs met.
Focusing next on the concept of healthy aging, participants were asked whether they were familiar with the term. On balance, roughly similar numbers reported having heard of the term healthy aging relative to those who had not. Among those who were aware, participants mentioned having heard about it from their doctor, through family and friends, as well as on television and social media. It was largely believed that the concept of healthy aging referred to maintaining both their physical and mental health as they age. When asked to describe what healthy aging meant to them, many believed the concept referred to living an active lifestyle, exercising regularly, and maintaining a balanced and nutritional diet. It was felt by several that the term also referred to staying cognitively sharp and focused on continued education for oneself as well as learning new skills. A few also believed that healthy aging involved maintaining a sense of purpose, establishing goals to work towards, and sustaining a positive mindset. Questioned whether they had heard of other terms such as 'active aging' and 'successful aging', very few had. Speculating on what these concepts referred to, most felt that active aging was associated with physical activity while successful aging likely had more to do with financial success and keeping busy in one's senior years. A smaller number interpreted these terms as being mostly synonymous with healthy aging, feeling there was little difference among them.
To aid in conversation, participants were provided with the following information related to healthy aging:
The World Health Organization (WHO) defines healthy aging as "the process of developing and maintaining the functional ability that enables wellbeing in older age." Functional ability is about having the capabilities that enable all people to be and do what they have reason to value. This includes a person's ability to:
Asked whether they felt this definition was clear, most believed that it was, with many commenting that it aligned with what they had perceived healthy aging to involve. A smaller number felt differently, believing that healthy aging should be viewed as a subjective concept, with a variety of meanings relative to each individuals' personal situation. The view was added that by defining healthy aging through criteria such as this, the WHO may serve to devalue the lifestyles of those whose priorities may not align with this list. A number, including those living with disabilities, commented that the criteria of being mobile was difficult for some to achieve and felt that individuals who may struggle with mobility should not be made to feel like they are not living healthy lives as a result. A few felt that the list did not incorporate enough aspects related to mental health and emotional fulfillment, while others believed it did not sufficiently address the financial challenges seniors may encounter as they age.
Discussing the factors and activities they felt were most important towards facilitating healthy aging, participants put forward a range of ideas.
Those mentioned most frequently included:
"The government needs to control for inflation. Food needs to be affordable."
(Nationwide Older Men)
In addition, most participants felt that remaining physically active and fit contributed greatly to healthy aging in terms of maintaining their strength and mobility. Some emphasized the importance of being able to access exercise programs, classes and/or a membership to a gym, while others spoke about exercise in a more low-impact way, such as getting out for walks or gardening.
"If the government wants us to age well, they should facilitate access to a gym."
(Nationwide Older Women)
"Your mental health is key to your physical health." (Nationwide Indigenous Older Adults)
Other factors, cited by some participants, but with less frequency than those listed above included:
Overall, participants did not feel that being valued and/or contributing to society was a key factor when it came to healthy aging. This was overall less important than many of the other factors listed above. However, when it came to being valued, participants were less concerned about their value to society in general but instead the value they provide to those close to them. They felt the greatest importance was that they feel valued and respected by their own family, including specifically their spouse, children, grandchildren, and other relatives they may be close to. Many viewed themselves as having committed their life to raising and supporting their families and wanted to feel valued in this regard as they age.
"I [have] invested my life into my children and grandchildren. I want to be valued and supported by them." (Nationwide Older Women)
On balance, participants believed for the most part that the ability to age healthily was within their control, as opposed to solely systemic factors. They viewed adhering to healthy behaviours and habits, such as a healthy and nutritious diet, being physically active, getting proper sleep and other basic fundamentals as within their own control. Simultaneously, participants recognized that there were other factors, outside of their control, that also played a role in one's ability to age healthily. For example, economic factors such as inflationary pressures could limit one's ability to pay for healthier foods (compared to cheaper, more processed foods) or limit their access to a gym.
"Groceries are expensive. People can't afford to buy fresh produce and foods, so they buy junk."
(Quebec Rural)
Genetics and predispositions to certain hereditary illnesses were viewed as out of their control. In this regard, they placed importance on healthcare services for prevention and treatment. Not being able to access health care services was seen as something that could prevent Canadians from being able to take control of their aging.
When asked about their thoughts on the role of technology in healthy aging and its benefits, participants spoke about the various types of devices they use and their associated benefits including the ability to easily connect with friends and family and quickly access information and services. Furthermore, participants felt that technology helped them to both set health related goals for themselves and keep their mind and bodies active.
With respect to various technologies, participants mentioned most frequently video conferencing platforms, wearables, various health apps and social media. The following provides an all-encompassing list of the different types of devices/technologies mentioned throughout the groups, along with the noted benefits each provides.
While participants viewed many benefits to using technology, a number cited several drawbacks or concerns as well.
"Right now, I don't trust it. It feels invasive. I don't know what they are doing to do with that information." (Nationwide Older Adults Identifying as 2SLGBTQI+)
More generally, some participants spoke about not wanting to feel as though technology was being forced upon. A few mentioned that some seniors' programs had moved to an online only format.
"I would like to be a choice, not a requirement." (Prairies Urban)
Next, participants were shown a list (outlined below) and asked to identify, in their view, which of the 14 factors or features they believed to be the most important in terms of making a community age-friendly. Participants were allowed to select up to five, but no more than five options. They were also given the option to select 'other' if they felt there was a feature not included on the list.
Based on participant's evaluations of the various characteristics associated with age-friendly communities, the results can be easily grouped into three tiers as indicated below. Tier 1 features were those identified most often as being important, while Tier 2 features were mentioned by many, but not most, and Tier 3 features were far less frequently mentioned. Among the various features that could help make cities and towns more age-friendly, participants placed a higher priority on improved access to health services, affordable housing, and in-home services to support independent living. While participants generally acknowledged that all of the features were important in ensuring one's community was age-friendly, much of the rationale for priorities in the top tiers was often made on the basis of what participants believed was vital to healthy aging or what was lacking in their own communities. More details regarding commentary for each feature and reasons for prioritization order (as provided by participants) are provided below. Results from this polling exercise can also be found in section A of the Appendix.
Access to health services including healthcare, mental health and dental care was seen as fundamental to aging. When citing their reason for selecting this option, many focused-on aspects related to health care services. They particularly placed importance on the need for every senior to be able to access a family physician. There was a general perception among participants that finding a family physician willing to take on new patients was becoming increasingly more difficult, especially in certain provinces/territories. Participants discussed the importance of access given that there is an increased dependency on these services as one gets older. Others discussed the mental health crisis across Canada and believed that more seniors needed access to support services for their mental health. With regards to dental services, some believed that there should be more government funding to support seniors in taking care of their dental needs, as oral health is a key element of one's overall health.
"Access to healthcare services is important because people can't get doctors. {And] even if you have a doctor, it is hard to see them." (Prairies Rural)
"There are a lot of people in distress. Their mental health is not taken care of." (Quebec Rural)
Affordable housing was seen as a requirement in order to facilitate all other necessary aspects of aging healthily, including eating/cooking, sleeping, etc. Reasons for selecting this as important was also related to inflationary pressures at present, making it more difficult for Canadians, especially seniors, to live comfortably. Some described feeling that their current pensions would not keep up with the rising costs of living and that inflation was a serious threat for seniors living on a fixed budget. Those in rural areas specifically commented on increasing rates for rental properties in their communities. Notably, women were more vocal about affordable housing, in addition to racialized participants.
"This is the most important! Everything starts with housing." (Ontario Rural)
"Affordable housing is a basic fundamental right." (Atlantic Urban)
When it came to in-home services, participants placed importance on the idea of 'aging in place'. They believed that, to the extent possible, allowing one to remain at home for as long as possible provided a more consistent lifestyle, better mental health state and increased access to close social connections (e.g., family and friends) for older Canadians. Many themselves had concerns about entering a long-term care facility and felt that by providing in-home services to support aging in place, it could potentially reduce the financial burden on long-term care and the healthcare system. Some also discussed the idea of in-home services reducing their exposure to communicable diseases, compared to in group settings, particularly in light of the COVID-19 pandemic. Notably, Indigenous participants placed less importance, compared to the average, on these types of services.
"The longer you can keep people in their own homes, the better [their] mental health will be, and it will be a lower cost to society." (Nationwide Higher SES)
"Nurses who come a couple times a week can be a lower cost then going into a long-term care home... and they allow people to age in place." (Prairies Urban)
Features of age-friendly communities that were cited by many participants, but with less frequency than Tier 1 features, are listed below.
Participants felt that community-based activities were important in terms of motivating seniors to get out and connect with other people in order to further promoting healthy aging. They mentioned recreational activities such as book clubs, art programs, and other similar activities to be of interest. On the social front, they also discussed general groups like dinner clubs and hobby-related social groups. Groups that focused on physical exercise, such as walking groups, were also viewed as important towards remaining physically active. All of these group activities were seen as providing an opportunity for seniors to connect with others like them and continue to increase their own social networks. Key subgroups who placed more emphasis on the importance of these activities included newcomers, racialized participants, those who identified as 2SLGBTQI+, women and those with a higher SES.
In a similar regard, many felt that building meaningful social connections was essential to healthy aging. They described their social networks as providing significant value to their lives, allowing them to feel less isolated and contributing to a more positive state of mind. It was discussed that a good social network helps to ensure that one has the support they need as they age. Older men tended to emphasize the importance of this more so than participation in community-based activities.
"Friends are really important because they are connections with those who surround us. We are a remedy for one another." (Quebec Rural)
Other features, which were mentioned with much less frequency are cited below in Tier 3.
Although mentioned less frequently, a few important takeaways for the above factors include:
When further prompted about the main challenges, obstacles, or barriers to aging healthily, the discussion aligned with the characteristics of age-friendly communities mentioned above. Commonly identified barriers, from most to least mentioned, stated across all groups included:
On balance, most participants describe the community where they live as age-friendly. Participants said they felt well-served by their community as an older Canadian and specifically pointed to a few characteristics they believed made their area age-friendly, including:
However, there were a number of gaps identified, which align with earlier rankings of factors that contribute to healthy aging. These included:
Across all groups participants were not very familiar with the Public Health Agency of Canada (PHAC) or it's role in terms of preventing disease and injuries, responding to public health threats, and promoting good physical and mental health. Nevertheless, after describing PHAC's role to participants, many did believe the organization could play a role in terms of supporting healthy aging for Canadians.
Asked where PHAC should be focusing its efforts, most felt it should be in terms of developing, supporting, and implementing both existing and new programs/ services for seniors. However, awareness raising and providing information on healthy aging were also viewed as important.
When it comes to awareness raising, participants felt it was important that PHAC continue to work to enhance its name and brand recognition as there was low familiarity overall with the organization and its mandate. Some felt this was an important step to undertake in advance, or in parallel, with other initiatives such as educational outreach or programs to ensure the information and/or services were viewed as trusted and with credibility. This was particularly important in light of the COVID-19 pandemic, as some participants held a more negative view of public health agencies post-pandemic.
Education about healthy aging continues to be important to certain groups. Participants noted the importance of information being accessible to seniors through a variety of means including online, in addition to more traditional methods. Helping seniors to navigate through this information, including where they can go for further help was important to some. In particular, providing resources to other organizations, like senior's associations, who are already interacting with this demographic was an approach seen to be effective. However, some participants felt that more creative approaches, outside of providing information on websites and brochures, should be considered for reaching and distributing this information to this group, although no specific recommendations were made.
By far, most believed that PHAC should focus its efforts around offering and supporting specific programs and services for seniors related to healthy aging, as they felt that this would have the most impact. Many believed the support provided by these programs would encourage Canadians to age in a healthy way, thus supporting the prevention or prolonging of illness and injuries as one ages. Participants suggested that any programs that would be supported and/or developed should be coordinated and targeted to best meet the needs of the population of older Canadians at present.
Participants rely on a host of sources for information about healthy aging, although many indicated having a high level of trust primarily in their family doctor and other health professionals. That said, several participants commented that while they appreciate their family doctor would offer them an honest assessment of their health, physicians can be somewhat dismissive of the various conditions and ailments that are commonly associated with aging.
"My doctor just says, 'you're getting older … what can you expect?'" (Ontario Rural)
The broader group of allied health professionals are also viewed as reliable sources of information on the topic of healthy aging. In this regard, pharmacists, dieticians, physiotherapists, chiropractors and massage therapists were mentioned. In particular, some participants commented on the trust they place in practitioners who have experience working with aging bodies and/or an older demographic.
"Pharmacists are incredible. Sometimes I trust them more than the doctor." (Nationwide Lower SES)
"I trust the dietitian that works in the grocery story because they tell me what I can afford." (Nationwide Lower SES)
There were mixed views across the groups on the extent to which participants identified alternative health care providers as reliable sources on healthy aging. While older women and participants who identified as LGBTQ2S+ were somewhat more inclined to trust the advice of naturopaths and homeopaths, some others, including those with disabilities, had less confidence in these types of resources or were concerned about the cost of accessing alternative health care providers.
Additionally, participants mentioned utilizing online resources, often indicating that they do their own research based on key word searches or research on specific health conditions and issues which are personally relevant.
"I would take what my doctor gives me and delve into it further on the Internet." (Nationwide Older Women)
"If I want to know anything, I go to Google." (Nationwide Older Men)
Specific websites were mentioned, including local health sciences centres, health institutes, as well as medical and/or health-related websites (e.g., University Health Network, Harvard Health (Harvard Medical School), Mayo Clinic, Johns Hopkins Medicine, WebMD, Heart and Stroke Foundation, Diabetes Canada). Provincial and federal government health websites were also referenced, with the caveat that government sites are not viewed as easy to navigate. A few participants commented that government websites are trusted and offer voluminous information on health and topics related to healthy living or healthy lifestyles. And, while relatively few participants had heard of the Public Health Agency of Canada, most indicated that it would be seen as credible. In discussion about reliance on the Internet for information on healthy aging, some participants raised the issue of misinformation, particularly when googling information. While the Internet is often considered a 'go to' first source for information, participants' comments suggested some hesitancy regarding its reliability unless it is clearly from respected, authenticated and evidence-based scientific sources.
"I go to the Internet first, but I don't always trust the sites I visit completely." (BC/North Rural/Urban)
It's hard to tell what's reliable, and what's not." (Ontario Rural)
Several participants spoke about having signed up to receive health newsletters from experts and institutions - McMaster Health Forum was mentioned in this regard. Across almost all groups, several commented on social media as a frequently used source of information, including Facebook, YouTube, Instagram and Telegram Messenger. Others commented that they would be inclined to trust seniors themselves, seniors' advocates, or organizations which provide services to seniors such as VON Canada or community-based seniors clubs.
"I think it would be helpful if the information was provided by seniors' organizations. It's better to hear information from a senior than a young person." (Atlantic Urban)
"I work with an agency called VON that provides classes for seniors. I would go there." (Nationwide Indigenous Older Adults)
"I try to find people who have been there and done it - people who are 90 to 100 years old." (Ontario Rural)
Family and friends were seen as trusted sources of health information by a number of participants who referred to reliance on their spouses or partners if they were seeking information about healthy aging.
"I rely on family … they'll be honest with me." (Ontario Rural)
Beyond the sources noted above and with less frequency, participants also mentioned traditional media (e.g., radio, TV), newsletters and pamphlets that are mailed to them or delivered to their door, as well as magazines targeting the older demographic (e.g., Zoomer magazine). In this context, pharmaceutical companies were explicitly mentioned by a few participants as lacking in credibility as a source of information about healthy aging.
When asked specifically about the credibility of the Public Health Agency of Canada, most participants did view the agency as trustworthy even if they were not necessarily familiar with it. PHAC's credibility stems from an understanding or perception that it has a key role to play in promoting health and sharing information with Canadians about health and healthy living as well and the fact that the information it produces is based on the advice of agency specialists and professionals with expertise in the area of healthy aging. Others saw PHAC as having a mandate to provide the facts in an unbiased manner.
"PHAC will tell us what's true, not just what we want to hear." (Quebec Urban)
The main criticisms of information from PHAC centered mainly on participants' lack of awareness of the agency and on past experience with government websites, specifically the requirement for visitors to government websites to have to parse large amounts of content in order to address questions they need answered or get to the information of interest to them. Others expressed concerns that PHAC may not have the capacity to disseminate information to the Canadian public or that it would duplicate the information coming from other sources within the health care system. Any other concerns or criticism about the credibility of information coming from PHAC centered on the following:
Relatively few participants commented on the ease of finding information about healthy aging, but those who did underscored the need to ensure that it is provided in a way that is easily understood by Canadians with varying levels of ability to read, consume and absorb information. In addition to taking into consideration literacy levels, participants also suggested that formatting should consider visual acuity particularly among the older population. Several took the opportunity to emphasize that any information on healthy aging should target those who are nearing retirement in order to prompt people to think about the topic in a timely fashion. Suggestions were also brought forward to ensure that information supports the goal of living independently and/or making decisions for oneself.
"It should recognize that senior people are autonomous and value their own autonomy. Healthy aging programs should be focused on facilitating that." (Nationwide Older Adults Living with Disabilities)
Participants' preferences for receiving information on the topic of healthy aging aligned, for the most part, with the sources and channels they trusted and/or viewed as convenient, relatively easy and quick to access. They included the following:
In commenting on their preferences, participants stressed that information should come from credible sources, such as the World Health Organization (WHO) or the federal government and that it should incorporate information that is presented visually and in a way that is appealing and grabs one's attention. Some also stated a preference for information which is delivered via an interactive format. Others wanted to ensure that contact information (e.g., a telephone number) is included in the event that the reader wished to follow up.
Indigenous participants made the point that information is useful, but that resources are required to be able to follow the advice given or implement the strategies for healthy aging that are offered.
"Sending out information to people who don't have access to resources is pointless." (Nationwide Indigenous Older Adults)
Participants were asked about the most appropriate way to refer to people aged 50 and older in communications about healthy aging. In a polling exercise, participants across the 19 groups selected what they believed was the best way to refer to individuals in this demographic and then provided some commentary to elaborate on their choice.
Results from this exercise were mixed, although similar to the results from the quantitative survey, many were comfortable being referred to as a 'senior'. About as many also favoured the term 'older adult,' while fewer preferred 'elder' or 'older person.' Each term generated both positive and negative commentary. While many viewed the label 'senior' as commonly used and one that people 'grow into as they age,' others felt it applied more so to those aged 65 or 70 and older. The opportunity to obtain discounts as a senior was viewed as an advantage. The main objection to the term 'senior' came from those in their 50s who felt they were too young to be considered a part of this demographic. There was also a sense that the term seniors held negative connotations for younger people.
"Younger people think of seniors as old and crotchety. They see them in a negative way." (BC/North Rural/Urban)
By contrast, the term 'older adult' was viewed as less value-laden and more appropriate for those in their 50s or early 60s who did not yet see themselves as seniors. Those who favoured this term felt it was appropriate for individuals who may still be active or more youthful in terms of their mindset, despite their chronological age. Those who objected to this term or disliked it simply didn't feel it appropriate to refer to people as old or older. Again those in their 50s and 60s were more inclined to feel this way. By contrast, some felt that referring to those aged 50 and older as seniors was more acceptable in that it suggested a level of life experience that yields knowledge and wisdom.
'Elder' was preferred by some, although less so as compared to the terms 'senior' or 'older adult.' The term 'elder' conferred a certain status based on life knowledge and experience and was viewed as a respectful way of referring to individuals who have reached this stage in their life. Some commented that they have seen the term used more commonly as a way of referring to individuals with considerable life experience. Others expressed concerns that the term is too closely associated with 'elderly' to which they objected. Some participants in a group held among those residing in the Prairies noted that it has religious connotations and, as such could be inappropriate for use more widely in discussions referring to Canada's aging demographic.
The term 'older person' was viewed as acceptable by some who felt that it positioned individuals in more relative terms. Others, however, were of the view that the term was somewhat incomplete in the sense that one could be older than others at age 30. As in the case of older adult, many also objected to the stigma associated with being labeled as old. Some also expressed concerns that the terms 'older adult,' 'older person,' and 'senior' all lack compassion, while 'elder' has connotations of wisdom and thoughtfulness.
A number of participants either preferred to avoid the use of labels entirely or felt none of the labels or terms discussed were appropriate, especially given the breadth of the demographic group (from age 50 on) being referred to. Several participants questioned why a label was required at all, preferring to be called a person. Some of these participants also noted that applying a term to such a wider swath of society did not account for the different circumstances and situations of individuals within the 50+ age group.
"We're all people. We all have the same rights and we might have different needs. But, we're all people." (Quebec Urban)
"I don't want to be called by any of these labels. My age is irrelevant." (Nationwide Indigenous Older Adults)
A few participants volunteered other labels or terms picking up on the idea of 'mature citizens,' or 'mature adults.' Others felt that any term should imply or infer wisdom based on the life experience of those who reach this stage in their lives.
At the conclusion of each focus group participants were given an opportunity to share any final thoughts related to healthy aging, including additional guidance they wished to relay to the Public Health Agency of Canada on this topic. The suggestions and comments provided by participants fall into a number of categories with a particular focus on planning and taking care of oneself in order to enhance the prospect of a higher quality of life at this stage. The range of themes which arose from participants' comments is highlighted below:
Two methodologies were employed for the quantitative phase of the research, as follows:
The survey was conducted in both official languages, English and French.
The final sample, as shown in the tables below is reflective of a proportionate sample based on population demographics in terms of gender, age, and region of the target audience from the 2021 Census by Statistics Canada.
The tables below outline separately the distribution of telephone and online surveys based on age and gender. Accompanying weights, which were applied to age/gender to ensure the final data set closely reflected the distribution of the population, aged 50 and above, are included below for Table 22 and Table 23.
| Proportionate Sample (Source: Statistics Canada, 2021 Census) | Final Survey Completes (Weighted) |
Weight | |||
|---|---|---|---|---|---|
| Age | Male | ||||
| % | n= | % | n= | ||
| 50-64 | 25 | 500 | 25 | 500 | 1.340481233 |
| 65-79 | 17 | 340 | 17 | 340 | 0.815346906 |
| 80+ | 5 | 100 | 5 | 100 | 0.751878947 |
| TOTAL | 47 | 940 | 47 | 940 | |
| Female | |||||
| % | n= | % | n= | ||
| 50-64 | 27 | 540 | 27 | 540 | 1.189426123 |
| 65-79 | 19 | 380 | 19 | 380 | 0.820733521 |
| 80+ | 7 | 140 | 7 | 140 | 0.858894847 |
| TOTAL | 53 | 1060 | 53 | 1060 | |
| Proportionate Sample (Source: Statistics Canada, 2021 Census) |
Final Survey Completes (Weighted) |
Weight | |||
|---|---|---|---|---|---|
| Age | Male | ||||
| % | n= | % | n= | ||
| 50-64 | 25 | 125 | 25 | 125 | 0.999999 |
| 65-79 | 17 | 85 | 17 | 85 | 0.999999 |
| 80+ | 5 | 25 | 5 | 25 | 1.041665625 |
| TOTAL | 47 | 240 | 47 | 240 | |
| Female | |||||
| % | n= | % | n= | ||
| 50-64 | 27 | 135 | 27 | 135 | 0.999999 |
| 65-79 | 19 | 95 | 19 | 95 | 0.999999 |
| 80+ | 7 | 35 | 7 | 35 | 0.999999 |
| TOTAL | 53 | 260 | 53 | 260 | |
After weighting for age and gender, the regional data closely aligned with Statistics Canada 2021 Census data, so no further weighting was applied. Results by region are provided below.
| Region | Percent of Population (Source: Statistics Canada, 2021 Census) |
Proportionate Sample (Source: Statistics Canada, 2021 Census) |
Final Survey Completes % (Weighted) |
Final Survey Completes n= (Weighted) |
|---|---|---|---|---|
| Atlantic |
8% NFLD 2% PEI <1% NS 3% NB 2% |
200 |
8% NFLD 2% PEI 1% NS 3% NB 2% |
197 |
| Quebec | 24% | 600 | 25% | 626 |
| Ontario | 38% | 950 | 38% | 950 |
| Manitoba | 3% | 75 | 3% | 75 |
| Saskatchewan | 3% | 75 | 3% | 74 |
| Alberta | 10% | 250 | 10% | 241 |
| British Columbia | 14% | 350 | 13% | 337 |
| TOTAL | 100% | 2,500 | 100% | 2,500 |
Respondents for the online survey were profiled and selected to participate in the survey through the use of a nationally representative online panel. Although research conducted via online panels does not follow the protocols for a random, representative survey (and as such will not have a margin of error applied to the results), we monitored variables listed above to ensure a good representation in accordance with the overall 2021 Statistics Canada Census data as per the variables above.
Following the Government of Canada's Standards for Public Opinion Research for Telephone and Online Surveys, pre-testing was undertaken prior to fully launching the survey. The telephone survey was pretested among n=26 respondents (14 in English and 12 in French) on January 31, 2023, prior to running live. For the online survey, a total of 22 survey completions were attained (11 in English and 11 in French) in a pretest on February 7, 2023.
The survey was intended to be 20 minutes in length, although fielding of the telephone survey during the pretest ran slightly over the expected length, averaging 22 minutes per interview. In discussions with the field supplier, it was predicted that the length would decrease as interviewers became more familiar with the survey. Online, the average length of the interview during pre-testing was 12 minutes, which was expected and under the allotted length of 20 minutes. With a hybrid telephone/online approach, a 20-minute telephone questionnaire can often be completed within a shorter length of time online.
Pre-test respondents were asked to provide feedback on various aspects of the experience completing the questionnaire, including overall ease of completion, comprehension, length, general interest in the topic and new learnings. Overall, the feedback from respondents who completed the survey was quite positive. The vast majority of respondents surveyed agreed, either somewhat or strongly, that:
Asked, on an open-ended basis, if the respondent had any other comments about the survey or their experience taking the survey, limited feedback was provided.
Results from the pre-test for both modes were provided to the Public Health Agency of Canada and given the positive findings, no modifications to the telephone or online survey were made.
Following the pre-test, the fieldwork for this survey was conducted from February 8th to March 5th, 2023 (telephone) and February 8-15th, 2023 (online). On average, the telephone survey took about 22 minutes to complete and ran anywhere between 10 and 44 minutes in length. Online, the median survey length was 11 minutes, with a range of completion times between 4 to 38 minutes.
In total n=2,000 respondents completed the telephone survey, with an incidence rate of 68%. At a confidence level of 95%, the margin of error for the telephone survey is ± 2.2%.
The survey resulted in an overall response rate of 2.69%, which has been calculated according to the Empirical Method formula of R / (U + IS + R). Additional details on the response rate calculation can be found in the Call Dispositions section of the Appendix.
In total n=500 respondents completed the online survey, with an incidence rate of 90%. The overall response rate was 24%. A total of 2,460 invitations were sent, of which 592 respondents started the survey. The overall completion rate achieved across all sample sources was 89%. As the online panel is opt-in and not considered to be a random sample, a margin of error can not be calculated.
The following outlines the calculations:
| Response Rate = (Interviews Started) / (Respondents E-mailed) | Completion Rate = (Completes + Screen outs + Quota full) / (Total # of Click Ins) |
|---|---|
| 24% = 592 / 2,460 | 89% = ((500 + 21 + 37) = 558) / 627 |
As noted in the above section "Sample Design", both the telephone and online methodologies were designed to obtain an age distribution reflective of Canada's population aged 50 and older - 52% aged 50-64, 36% aged 65-79 and 12% aged 80+. Although the proportion of respondents between the ages of 50 and 64 remained the same across both methodologies, online respondents skewed younger (aged 50-54) while telephone respondents skewed older (aged 60-64). Other demographic differences to note between modes are as follows:
Some differences were also noted in the results between those who completed the survey by telephone (interview administered) and those who completed the survey online (self-administered). Broadly speaking respondents who completed a telephone interview, relative to those who completed the survey online, were more:
These differences suggest that there are a variety of issues that can be introduced with interview-led surveys, which include social desirability bias and, overall, responses to scaled questions generally being more positive. There is a body of research which shows that mode effects are likely to occur under several scenarios and this may be contributing to some of the differences evident in this dataset. For example, on questions of a sensitive nature self-administered polls undertaken online tend to yield data that is less skewed toward socially desirable responses versus interviewer-led polls. Similarly, on questions that feature a ratings scale, telephone poll respondents are more likely than those responding online to select more positive answer categories but are not more likely to give extremely negative responses. For more detailed data by mode, please refer to the data tables. The differences seen in this study, otherwise known as mode effects, reflect much of the current research on why respondent's answers differ when the interview is undertaken in a different format. For example, Pew Research recently conducted a large-scale experiment that tested the effects of the mode of survey interview between with an interviewer vs. a self-administered online survey. Results indicated that lines of questioning around ratings of family or social life, produced significant differences between these two modes (18% and 14%, respectively). Should PHAC decide to undertake this survey in the future, deploying a self-administered (online) approach will likely provide more accurate results, reflecting respondents' more thoughtful and honest responses to attitudinal-based questions. However, if and when this shift is made further analysis should be conducted to assess the implications of a change to the methodology and this should be noted in the reporting. For additional details regarding the demographic makeup of both online and telephone respondents, please refer to the section below 'Respondent Profile - Additional Details' and the data tables.
One of the strengths of this study is the multi-modal approach to the methodology undertaken. Conducting interviews by telephone (using landline and mobile numbers) and online achieved a robust sample with a good mix of older Canadians, some of whom may only be reachable through one of these methods and would have otherwise been excluded. This approach was also employed to allow for comparisons between the two modes, as discussed above, should PHAC wish to move this study fully online in the future.
Survey research is a reliable means of gauging attitudes and behaviours at a specific point in time among the general public and specific target audiences. However, there are certain limitations in this approach which could be a factor of the methodology and questionnaire design or related to the target audience itself. While a number of steps have been taken to mitigate any deficiencies, it is nevertheless important that the limitations of the current study be fully explained. Some limitations of the data exist:
In addition to the respondent profile provided in Section A of the report, the following outline the total and modal responses for all other demographic questions asked as part of the survey.
| TOTAL | Telephone | Online | |
|---|---|---|---|
| n= | 2500 | 2000 | 500 |
| % | % | % | |
| Online | 20 | - | 100 |
| Telephone | 80 | 100 | - |
| TOTAL | Telephone | Online | |
|---|---|---|---|
| n= | 2500 | 2000 | 500 |
| % | % | % | |
| 50-64 | 52 | 52 | 52 |
| 65-79 | 36 | 36 | 36 |
| 80+ | 12 | 12 | 12 |
| 50-54 | 14 | 11 | 24 |
| 55-59 | 16 | 16 | 14 |
| 60-64 | 21 | 22 | 14 |
| 65-69 | 14 | 14 | 15 |
| 70-74 | 11 | 11 | 12 |
| 75-79 | 10 | 10 | 9 |
| 80+ | 12 | 12 | 12 |
| NOT SPECIFIED IN DETAIL | 3 | 3 | - |
| TOTAL | Telephone | Online | |
|---|---|---|---|
| n= | 2500 | 2000 | 500 |
| % | % | % | |
| Male | 47 | 47 | 47 |
| Female | 53 | 53 | 53 |
| Non-binary | <1 | <1 | <1 |
| Prefer to self-identify | <1 | <1 | - |
| Prefer not to answer | <1 | <1 | - |
| TOTAL | Telephone | Online | |
|---|---|---|---|
| n= | 2500 | 2000 | 500 |
| % | % | % | |
| Newfoundland and Labrador | 2 | 2 | 2 |
| Prince Edward Island | 1 | 1 | 1 |
| Nova Scotia | 3 | 3 | 3 |
| New Brunswick | 2 | 2 | 2 |
| Quebec | 25 | 25 | 24 |
| Ontario | 38 | 38 | 38 |
| Manitoba | 3 | 3 | 3 |
| Saskatchewan | 3 | 3 | 3 |
| Alberta | 10 | 10 | 10 |
| British Columbia | 13 | 13 | 14 |
| Atlantic | 8 | 8 | 8 |
| Quebec | 25 | 25 | 24 |
| Ontario | 38 | 38 | 38 |
| Manitoba/Saskatchewan | 6 | 6 | 6 |
| Alberta | 10 | 10 | 10 |
| BC/North | 13 | 13 | 14 |
| TOTAL | Telephone | Online | |
|---|---|---|---|
| n= | 2500 | 2000 | 500 |
| % | % | % | |
| Less than a High School diploma or equivalent | 5 | 5 | 3 |
| High School diploma or equivalent | 20 | 20 | 22 |
| Registered Apprenticeship or other trades certificate or diploma | 6 | 6 | 6 |
| College, CEGEP or other non-university certificate or diploma | 24 | 23 | 28 |
| University certificate or diploma below bachelor's level | 9 | 9 | 7 |
| Bachelor's degree | 20 | 20 | 20 |
| Post graduate degree above bachelor's level | 15 | 16 | 12 |
| Prefer not to answer | 1 | 1 | 1 |
| HS or less | 25 | 25 | 25 |
| College/Trades | 30 | 29 | 35 |
| University | 44 | 45 | 39 |
| TOTAL | Telephone | Online | |
|---|---|---|---|
| n= | 2500 | 2000 | 500 |
| % | % | % | |
| Western European (UK, Spain, Portugal, France, Italy, Germany, Austria, Switzerland, etc.) | 52 | 50 | 61 |
| Eastern European (Poland, Hungary, Romania, Ukraine, Russia, etc.) | 9 | 9 | 10 |
| African (Nigeria, Ethiopia, Tanzania, etc.) | 1 | 1 | <1 |
| Middle Eastern (Israel, Syria, Jordan, Egypt, Iran, Iraq, etc.) | 1 | 1 | 1 |
| South Asian (India, Afghanistan, Pakistan, Sri Lanka, etc.) | 1 | 1 | 2 |
| Southeast Asian (Thailand, Vietnam, Singapore, the Philippines, Indonesia, Cambodia, etc.) | 1 | 1 | 1 |
| East Asian (China, Korea, Japan, Taiwan, etc.) | 2 | 1 | 4 |
| South/Central/Latin American (Argentina, Mexico, Brazil, etc.) | 1 | 1 | 1 |
| West Indian (Caribbean) | 2 | 2 | <1 |
| Indigenous (First Nations, Metis, Inuit (Inuk), etc.) | 3 | 3 | 2 |
| Other | 28 | 32 | 14 |
| North American | 2 | 2 | <1 |
| Canadian | 18 | 20 | 10 |
| American | <1 | <1 | - |
| Australian | <1 | <1 | - |
| Black | <1 | <1 | - |
| White | 5 | 5 | 2 |
| French Canadian | 3 | 4 | 2 |
| Jewish | <1 | <1 | <1 |
| Mixed | <1 | <1 | - |
| Other | <1 | <1 | - |
| None/Not specified | 1 | 1 | 1 |
| Don't know | 2 | 1 | 4 |
| Prefer not to answer | 2 | 2 | 2 |
| TOTAL | Telephone | Online | |
|---|---|---|---|
| n= | 76 | 64 | 12 |
| % | % | % | |
| First Nations (on/off reserve) | 46 | 43 | 58 |
| Metis | 36 | 35 | 42 |
| Inuk | 4 | 5 | - |
| Other | 7 | 8 | - |
| Prefer not to answer/No answer | 7 | 9 | - |
| TOTAL | Telephone | Online | |
|---|---|---|---|
| n= | 72 | 60 | 12 |
| % | % | % | |
| Yes | 13 | 13 | 8 |
| No | 85 | 84 | 92 |
| Prefer not to answer | 2 | 3 | - |
| TOTAL | Telephone | Online | |
|---|---|---|---|
| n= | 2500 | 2000 | 500 |
| % | % | % | |
| Yes | 82 | 82 | 83 |
| No | 17 | 17 | 17 |
| Prefer not to answer | <1 | <1 | <1 |
| TOTAL | Telephone | Online | |
|---|---|---|---|
| n= | 427 | 341 | 85 |
| % | % | % | |
| Less than 5 years | 1 | 1 | 2 |
| 5-9 years | 1 | 2 | 1 |
| 10 years or more | 96 | 96 | 96 |
| Prefer not to answer | 1 | 1 | - |
| TOTAL | Telephone | Online | |
|---|---|---|---|
| n= | 2500 | 2000 | 500 |
| % | % | % | |
| Married | 49 | 48 | 50 |
| Living common-law | 9 | 9 | 11 |
| Separated | 4 | 4 | 4 |
| Divorced | 12 | 12 | 13 |
| Widowed | 13 | 14 | 8 |
| Never married | 12 | 12 | 13 |
| Prefer not to answer | 1 | 1 | 1 |
| TOTAL | Telephone | Online | |
|---|---|---|---|
| n= | 2500 | 2000 | 500 |
| % | % | % | |
| Under $20,000 | 7 | 7 | 4 |
| $20,000 to just under $40,000 | 16 | 16 | 17 |
| $40,000 to just under $60,000 | 17 | 16 | 21 |
| $60,000 to just under $80,000 | 14 | 13 | 14 |
| $80,000 to just under $100,000 | 10 | 10 | 12 |
| $100,000 to just under $150,000 | 12 | 12 | 14 |
| $150,000 and above | 12 | 13 | 8 |
| Prefer not to answer | 11 | 12 | 9 |
| TOTAL | Telephone | Online | |
|---|---|---|---|
| n= | 2500 | 2000 | 500 |
| % | % | % | |
| Retired | 51 | 51 | 51 |
| Employed (FT/PT/Self-employed) | 39 | 39 | 39 |
| Working full-time (that is 35 or more hours per week) | 25 | 26 | 24 |
| Working part-time (that is less than 35 hours per week) | 7 | 6 | 9 |
| Self-employed | 7 | 7 | 5 |
| Unemployed, but looking for work | 2 | 2 | 3 |
| OTHER | |||
| Not in the workforce (full-time homemaker, not employed, not looking for work) | 7 | 7 | 5 |
| A student attending school full-time | <1 | <1 | - |
| Other (do not specify) | 1 | 1 | 2 |
| Prefer not to answer | <1 | <1 | - |
| TOTAL | Telephone | Online | |
|---|---|---|---|
| n= | 2500 | 2000 | 500 |
| % | % | % | |
| A city | 63 | 62 | 68 |
| A town or village | 21 | 21 | 17 |
| A rural area | 15 | 15 | 14 |
| A remote area | 1 | 2 | 1 |
| Other | <1 | <1 | - |
| Don't know | <1 | <1 | - |
| Prefer not to answer | <1 | <1 | <1 |
| TOTAL | Telephone | Online | |
|---|---|---|---|
| n= | 2500 | 2000 | 500 |
| % | % | % | |
| Live in a retirement home | 2 | 2 | 1 |
| Rent your home | 20 | 19 | 23 |
| Own your home | 74 | 75 | 73 |
| Live in someone else's home | 2 | 2 | 1 |
| Other | 1 | 1 | 1 |
| Co-op | <1 | <1 | <1 |
| Rent subsidized facility | <1 | <1 | <1 |
| Camper/trailer | <1 | <1 | - |
| Homeless | <1 | <1 | <1 |
| Other | <1 | <1 | - |
| Prefer not to answer | 1 | 1 | 1 |
| TOTAL | Telephone | Online | |
|---|---|---|---|
| n= | 2500 | 2000 | 500 |
| % | % | % | |
| English | 75 | 77 | 66 |
| French | 25 | 23 | 34 |
The qualitative phase of this research was used to provide context to the survey results as a way to explore and better understand diverse views on what constitutes healthy aging. This phase of the research consisted of 19 online focus groups. The research instruments in English and French, including the recruiting script and moderators guide can be found in the Appendix.
The target audience for this research consisted of Canadians aged 50 and older.
All participants were recruited adhering to the Standards for the Conduct of Government of Canada Public Opinion Research - Qualitative Research. This included the following:
To ensure that the recruiting process was inclusive and supported the specific needs of those with disabilities, efforts were made to provide accommodations to any individual who expressed concern over their ability to actively participate online (e.g., providing an additional incentive for a caregiver to assist the participant with the technology required or providing an additional incentive for a translator).
A total of 19 focus groups were conducted from March 13th to March 23rd, 2023, across 5 regions of Canada (Atlantic, Ontario, Quebec, Prairies, British Columbia/North). For each group, 8 participants were recruited with the goal of ensuring 6 participants at a minimum attended each session. Just over half (10) of the focus groups were segmented by region - both by region within Canada and location with respect to urban and rural areas. The remaining nine focus groups were conducted nationwide with diverse sub-groups of the population. Details for each group, such as language, region, and group composition are outlined in the table below.
| Date | Language | Location | Composition | Number of Participants |
|---|---|---|---|---|
| March 13, 2023 | EN | Atlantic | Residing in Urban Areas | 8 |
| March 13, 2023 | EN | Atlantic | Residing in Rural Areas | 8 |
| March 13, 2023 | EN | Nationwide | Older Men | 7 |
| March 14, 2023 | EN | Ontario | Residing in Urban Areas | 7 |
| March 14, 2023 | EN | Ontario | Residing in Rural Areas | 6 |
| March 14, 2023 | EN | Nationwide | Older Adults with High Socio-economic Status | 7 |
| March 15, 2023 | FR | Quebec | Residing in Urban Areas | 8 |
| March 15, 2023 | FR | Quebec | Residing in Rural Areas | 7 |
| March 15, 2023 | EN | Nationwide | Older Women | 8 |
| March 16, 2023 | EN | Prairies | Residing in Urban Areas | 6 |
| March 16, 2023 | EN | Prairies | Residing in Rural Areas | 8 |
| March 20, 2023 | EN | Nationwide | Older Adults Identifying as Racialized | 8 |
| March 20, 2023 | EN | Nationwide | Older Adults with Low Socio-economic Status | 6 |
| March 21, 2023 | EN | British Columbia/North | Residing in Urban Areas | 7 |
| March 21, 2023 | EN | Nationwide | Indigenous Older Adults | 7 |
| March 22, 2023 | EN | British Columbia/North | Residing in Urban and Rural Areas | 7 |
| March 22, 2023 | EN | Nationwide | Older Adults Living with Disabilities | 8 |
| March 23, 2023 | EN | Nationwide | Older Adults Identifying as LGBTQ2S+ | 6 |
| March 23, 2023 | EN | Nationwide | Older Adult Newcomers to Canada | 7 |
| Total Number of Participants | 136 |
On a best-efforts basis, each focus group aimed to include a mix by gender, age, ethnicity, household income, educational attainment, and employment status (as applicable).
During the screening process and at the beginning of each group, participants were informed that the research was being conducted on behalf of the Public Health Agency of Canada (PHAC) and that their responses would be kept completely confidential. Furthermore, consent to audio and video record the session was obtained at both the time of recruitment and the beginning of each triad.
Participants were recruited in their official language of choice using either a random digit dialing (RDD) approach or through leveraging online panels. For audiences with a relatively high incidence in the overall population such as the regionally specific urban and rural groups, a RDD telephone approach was used. For lower incidence groups such as older adults identifying as LGBTQ2S+ or those with lower socio-economic status, an online panel was leveraged where profiling information was used to help more cost effectively target individuals meeting the criteria for each group. Participants identified through the online panel were then screened via telephone to ensure they met all the requirements.
To complete 19 focus groups over two weeks, three separate moderators were used. During fieldwork, the moderators met at least twice to discuss high level findings and trends and share perspectives. During these meetings any adjustments to the moderators' guides in terms of the flow of discussion, additional probing questions and other fine tuning to optimize the generation of key insights were discussed. Ultimately, no changes to the discussion guide were made.
In total, 152 participants were recruited and 136 participated. Each group was conducted online via Zoom, lasting approximately 90 minutes in length. All participants received an honorarium of $100 in appreciation of their time.
After completion of the focus groups and in discussion with the Project Authority, it was decided that additional one-on-one interviews would be conducted with older Canadians living with disabilities in order to achieve a broader representation among this group. A total of 5 in-depth interviews were conducted either online via Zoom or by telephone. No modifications to the discussion guide were made. Each interview lasted approximately 30-45 minutes and participants received a $100 honorarium in appreciation of their time.
Across the focus groups and one-on-one interviews, a total of 141 Canadians aged 50 and older participated.
The semi-structured nature of these focus groups discussions combined with the limited number of participants engaged in the research means that findings are not statistically representative and should be considered more directional in nature. As such, the findings from the qualitative research should not be considered statistically projectable to the broader population across Canada.
| Option | Total |
|---|---|
| Affordable housing | 80 |
| Safe neighbourhoods | 33 |
| Access to health services (health care, mental health and dental care) | 100 |
| In-home services that support independent living | 75 |
| Well-maintained sidewalks | 10 |
| Accessible and affordable public transit | 31 |
| Employment and volunteer opportunities for older people | 33 |
| Community-based social and recreational activities | 67 |
| Accessible and affordable high-speed Internet | 30 |
| Exercise programs for older people | 42 |
| Opportunities for lifelong learning | 32 |
| Accessible buildings | 22 |
| Access to the outdoors/natural environment | 31 |
| Walkable neighbourhoods | 29 |
| Social networks and friends | 64 |
| Something else (not listed) | 4 |
| Option | Total |
|---|---|
| Older person | 15 |
| Older adult | 31 |
| Senior | 39 |
| Elder | 17 |
| In another way (not listed) | 28 |
| N | |
|---|---|
| Total numbers attempted | 202,609 |
|
UNRESOLVED NUMBERS (U) Busy /No answer/ Voicemail |
73,897 |
| RESOLVED NUMBERS (Total minus U) | 128,712 |
|
OUT OF SCOPE (invalid/non-eligible) Not-in-service (NIS)/Non-res/business/ Fax/modem/ Cell/pager/ Duplicates |
90,125 |
|
IN SCOPE NON-RESPONDING (IS) Refusals/break-offs/language barrier/callback missed/respondent not available/illness/incapable |
35,561 |
| IN SCOPE RESPONDING (R) | 3,026 |
| Disqualified/Quote filled | 1,012 |
| Completed | 2,014 |
| RESPONSE RATE [R / (U + IS + R)] | 2.69% |
The response rate was calculated according to the standard Empirical Method, as follows:
DIVIDED BY
Health Canada/PHAC - Healthy Aging Research Study
DRAFT TELEPHONE Questionnaire (Jan. 23, 2023)
INTRODUCTION
Hello/Bonjour, my name is INSERT NAME from The Strategic Counsel, a professional public opinion research company. Would you prefer that I continue in English or French? Préférez-vous continuer en français ou en anglais? [IF FRENCH, CONTINUE IN FRENCH OR ARRANGE A CALL BACK WITH FRENCH INTERVIEWER: Nous vous rappellerons pour mener cette entrevue de recherche en français. Merci. Au revoir].
We are conducting a survey on behalf of the Public Health Agency of Canada regarding your views on aging. It should take no longer than about 15-20 minutes to complete. Your participation is voluntary and completely confidential. Your answers will remain anonymous. May I continue? IF UNABLE TO READ ENTIRE INTRODUCTION INTERVIEWER MUST PROVIDE LENGTH OF INTERVIEW TO EVERY RESPONDENT .
IF YES, QUALIFY AND CONTINUE.May I please speak to the person, 50 years of age or older, living in this household? Would that be you or someone else?
IF NO, BUT SOMEONE ELSE AT THIS NUMBER, ASK:May I speak with that person, please?
IF REFERRED TO ANOTHER PERSON, START FROM THE TOP. IF PERSON IS NOT AVAILABLE, TERMINATE.
IF DON'T KNOW, TERMINATE.
Before I begin, please note this call may be monitored or recorded for quality control purposes. The first few questions are about you.
SCREENING QUESTIONS
1. Record language of interview. [DO NOT ASK]
2. In what year were you born? [RECORD YEAR - YYYY] [PN: MANAGE QUOTAS FOR AGE]
2a. Would you be willing to tell me in which of the following age categories you belong? [PN: MANAGE QUOTAS FOR AGE]
3. What is your gender? [PN: MANAGE QUOTAS FOR GENDER OVERALL - 48 MALE/52 FEMALE - AND FOR GENDER BY AGE]
4. May I have the first 3 digits of your postal code? [PN: REASSIGN TO PROVINCES/TERRITORIES AND MANAGE QUOTAS BY REGION]
5. Would you say your health in general is …?
6. Do you identify as any of the following?
QUALITY OF LIFE AND CURRENT ACTIVITIES
The next few questions ask about your life, current routine, and the types of activities in which you are involved.
7. Overall, how would you rate your quality of life? Would you say it is …
8. How, would you rate your quality of life in each of the following areas … excellent, good, fair, poor or very poor? [READ AND ROTATE ITEMS A-F.]
9. How often do you engage in each of the following … at least once a day, at least once a week, at least once a month, at least once a year, never? [READ AND ROTATE ITEMS A-E]
10. Which of the following best describes your current employment status? Are you … [READ LIST. ACCEPT ONE ANSWER ONLY.]
11. [IF 'RETIRED' OR 'NOT IN THE WORKFORCE,' SKIP TO Q.12. ALL OTHERS, ASK] At what age do you anticipate retiring?
12. How do you feel generally about the [IF 50-64: PROSPECT / IF 65+: EXPERIENCE] of getting older? Would you say that overall your feeling is:
13. What 2 things are you most concerned about as you age? [ACCEPT UP TO TWO RESPONSES. IF POSSIBLE, PRE-CODE USING LIST BELOW.]
14. How much do you associate the term 'healthy aging' with each of the following? [READ AND ROTATE ITEMS A-J]
15. Is there anything else that you associate with 'healthy aging?' [OPEN-END]
ENABLERS AND BARRIERS TO HEALTHY AGING
[INTERVIEWERS TO READ TO RESPONDENTS]Healthy aging is about developing and maintaining the physical and cognitive abilities that enable wellbeing as one ages. It is supported by environments that allow people to do what they value as they age.
16. Overall, would you describe the community in which you currently live as being … ? [READ LIST. ACCEPT ONE RESPONSE ONLY.]
17. How would you rate your community on the following, which support healthy aging? [READ AND ROTATE ITEMS A-K]
18. Many factors contribute to healthy aging. In your view, which two of the following are the most important? Is it … [READ LIST AND ROTATE. ACCEPT UP TO TWO RESPONSES. PROMPT FOR ANYTHING ELSE LAST.]
COMMUNICATIONS AND TECHNOLOGICAL LITERACY/PROFICIENCY
Now we have a couple of questions about how you do or would access information on the topic of healthy aging.
19. Who do you trust the most when it comes to providing you with information related to healthy aging? [READ LIST AND ROTATE. ACCEPT UP TO TWO RESPONSES. PROMPT FOR 'OTHER, PLEASE SPECIFY LAST'.]
20. Do you recall seeing anything from the Government of Canada or the Public Health Agency of Canada on the topic of healthy aging in the last 2 years?
[DO NOT READ] Don't know
21. How interested are you in getting more information on the following topics related to healthy aging? [READ AND ROTATE ITEMS A-H]
Not interested at all
DEMOGRAPHICS
These last few questions will allow us to compare the survey results among different groups of respondents. Your answers will remain anonymous and confidential.
22. Do you have a family doctor/physician?
[DO NOT READ] Prefer not to answer
23. Are you responsible for the primary care of someone with a long-term health condition, physical or mental disability, or problems related to aging?
[DO NOT READ] Prefer not to answer
24. What is your sexual orientation? [READ LIST. ACCEPT ONE RESPONSE ONLY]
25. Which of the following best describes your marital status? [READ LIST. ACCEPT ONE RESPONSE ONLY.]
26. Do you live alone?
[DO NOT READ] PREFER NOT TO ANSWER
26a. [IF 'NO' AT Q.26, ASK] Please indicate whether you are living with any of the following? [READ LIST. SELECT ALL THAT APPLY.]
27. What is the highest level of formal education that you have completed? [READ LIST.]
28. Which of the following best describes your total household income last year, before taxes, from all sources for all household members? [READ LIST. ACCEPT ONLY ONE RESPONSE.]
29. Which of the following ethnicity(ies) do you identify as? [ACCEPT ALL THAT APPLY.]
29a. [IF INDIGENOUS AT Q.29, ASK:]Are you … READ LIST. SELECT ONE RESPONSE ONLY. ?
29b.[IF INDIGENOUS AT Q.29, ASK]Do you live on a reserve or First Nation community for at least 6 months of the year?
30. Were you born in Canada?
30a. [IF NO AT Q.30, ASK] How many years have you lived in Canada?
31. How would you describe the area in which you reside? Is it …
32. Which of the following best describes your current living situation? Do you …
33. What didn't we ask as part of this survey, that you would like us to know about healthy aging? [OPEN-END]
Santé Canada/ASPC - Étude de recherche sur le vieillissement en santé
ÉBAUCHE du questionnaire par TÉLÉPHONE (le 23 janvier 2023)
INTRODUCTION
Hello/Bonjour, my name is INSERT NAME, from Strategic Counsel, a professional public opinion research company. Would you prefer that I continue in English or French? Préférez-vous continuer en français ou en anglais? [IF FRENCH, CONTINUE IN FRENCH OR ARRANGE A CALL BACK WITH FRENCH INTERVIEWER: Nous vous rappellerons plus tard pour mener cette entrevue de recherche en français. Merci. Au revoir].
Nous réalisons un sondage au nom de l'Agence de la santé publique du Canada portant sur votre opinion sur le vieillissement. La participation à ce sondage ne devrait pas prendre plus de 15 à 20 minutes. Votre participation se fait sur une base volontaire et restera totalement confidentielle. Vos réponses demeureront anonymes. Puis-je poursuivre? SI L'INTERVIEWEUR NE PEUT PAS LIRE TOUTE L'INTRODUCTION, IL DOIT INDIQUER LA DURÉE DE L'ENTRETIEN À CHAQUE PERSONNE INTERROGÉE.
SI OUI, PRÉCISER LE RÉPONDANT ET CONTINUER.Puis-je parler à la personne âgée de 50 ans ou plus qui vit dans ce ménage? Est-ce que c'est vous ou quelqu'un d'autre?
SI NON, MAIS IL Y A QUELQU'UN D'AUTRE À CE NUMÉRO, DEMANDER : Puis-je parler à cette personne, s'il vous plaît?
S'IL S'AGIT D'UNE AUTRE PERSONNE, COMMENCER PAR LE DÉBUT. SI LA PERSONNE N'EST PAS DISPONIBLE, METTRE FIN À L'APPEL.
SI LA PERSONNE RÉPOND « JE NE SAIS PAS », METTRE FIN À L'APPEL.
Avant de commencer, veuillez noter que cet appel peut être surveillé ou enregistré à des fins de contrôle de la qualité. Les premières questions portent sur vous-même.
QUESTIONS DE SÉLECTION
1. Indiquer la langue choisie pour l'entretien. [NE PAS LIRE DE VIVE VOIX]
2. En quelle année êtes-vous né(e)? [INDIQUER L'ANNÉE - AAAA] [Note : GÉRER LES QUOTAS PAR AGE]
SI AGÉ DE MOINS DE 50 ANS (NÉ APRÈS 1972), METTRE FIN À l'APPEL
[Note : SI LE RÉPONDANT PRÉFÈRE NE PAS PRÉCISER SA DATE DE NAISSANCE, PASSER À LA Q.2A]
2a. Voudriez-vous me dire à quelle catégorie d'âge suivante vous appartenez? [Note : GÉRER LES QUOTAS PAR AGE]
3. Quel est votre genre? [Note : GÉRER LES QUOTAS PAR GENRE GLOBAL - 48 MASCULIN/52 FÉMININ - ET PAR GENRE SELON L'AGE]
4. Puis-je avoir les 3 premiers caractères de votre code postal? [Note : RÉATTRIBUER AUX PROVINCES-TERRITOIRES ET GÉRER PAR RÉGION]
5. Diriez-vous que votre santé en général est...?
6. Vous identifiez-vous à l'un des groupes suivants?
QUALITÉ DE VIE ET ACTIVITÉS PRÉSENTES
Les quelques questions qui suivent portent sur votre vie, votre routine et les types d'activités auxquelles vous participez.
7. Dans l'ensemble, comment évalueriez-vous votre qualité de vie? Diriez-vous qu'elle est…?
8. Comment évalueriez-vous votre qualité de vie dans chacun des domaines suivants? Est-elle excellente, bonne, acceptable, mauvaise ou très mauvaise? [LIRE ET RÉPÉTER DE A à F.]
9. À quelle fréquence pratiquez-vous chacune des activités suivantes? Les pratiquez-vous au moins une fois par jour, au moins une fois par semaine, au moins une fois par mois, au moins une fois par année, jamais? [LIRE ET RÉPÉTER DE A à E]
10. Quelle affirmation parmi les suivantes décrit le mieux votre situation d'emploi actuelle? Est-ce que vous…? [LIRE LA LISTE. ACCEPTER UNE SEULE RÉPONSE.]
11. [SI « RETRAITÉ » OU « NE FAIT PAS PARTIE DE LA POPULATION ACTIVE », PASSER À Q.12. SI « AUTRE », DEMANDER] À quel âge pensez-vous prendre votre retraite?
À PROPOS DU VIEILLISSEMENT
Maintenant, nous avons quelques questions concernant votre opinion sur le vieillissement.
12. Que pensez-vous en général de [si âgé de 50 à 64 ans : LA PERSPECTIVE DE VIEILLIR / si âgé de 65 ans et plus: L'EXPÉRIENCE DU VIEILLISSEMENT]? Diriez-vous que votre sentiment général est :
13. Quelles sont les 2 choses qui vous préoccupent le plus en vieillissant? [ACCEPTER JUSQU'À DEUX RÉPONSES. SI POSSIBLE, PRÉ-CODER À L'AIDE DE LA LISTE CI-DESSOUS.]
14. Dans quelle mesure associez-vous le « vieillissement en santé » à chacun des éléments suivants? [LIRE ET RÉPÉTER DE A à J]
15. Y a-t-il autre chose que vous associez au « vieillissement en santé »? [QUESTION OUVERTE]
FACTEURS HABILITANTS ET OBSTACLES AU VIELLISSEMENT EN SANTÉ
[À LIRE PAR L'INTERVIEWEUR À L'ATTENTION DU RÉPONDANT]Le vieillissement en santé consiste à développer et maintenir les capacités physiques et cognitives qui favorisent le bien-être en vieillissant. Il est favorisé par des environnements qui permettent aux gens de faire ce qu'ils aiment en prenant de l'âge.
16. De façon générale, décririez-vous la collectivité dans laquelle vous vivez actuellement comme étant… ? [LIRE LA LISTE. ACCEPTER UNE SEULE RÉPONSE.]
17. Comment évalueriez-vous votre collectivité sur les points suivants qui favorisent un vieillissement en santé? [LIRE ET RÉPÉTER DE A à K]
18. De nombreux facteurs contribuent à un vieillissement en santé. Selon vous, quels sont les deux facteurs suivants qui sont les plus importants? Est-ce…? [LIRE LA LISTE ET RÉPÉTER. ACCEPTER JUSQU'À DEUX RÉPONSES. INCITER À FOURNIR TOUTE AUTRE RÉPONSE EN DERNIER.]
LITÉRACIE/COMPÉTENCES EN MATIRE DE COMMUNICATIONS ET DE TECHNOLOGIE
Nous avons maintenant quelques questions sur la façon dont vous accédez ou souhaiteriez accéder à l'information sur le thème du vieillissement en santé.
19. À qui faites-vous le plus confiance lorsqu'il s'agit de vous fournir de l'information sur le vieillissement en santé? [LIRE LA LISTE ET RÉPÉTER. ACCEPTER JUSQU'À DEUX RÉPONSES. INCITER À FOURNIR TOUTE AUTRE RÉPONSE EN DERNIER.]
20. Vous souvenez-vous d'avoir vu quelque chose de la part du gouvernement du Canada ou de l'Agence de la santé publique du Canada sur le thème du vieillissement en santé au cours des 2 dernières années?
21. Dans quelle mesure souhaitez-vous obtenir davantage d'informations sur les sujets suivants liés au vieillissement en santé? [LIRE ET RÉPÉTER DE A à H]
COMPOSANTE DÉMOGRAPHIQUE
Ces quelques dernières questions nous permettront de comparer les résultats du sondage entre différents groupes de répondants. Vos réponses demeureront anonymes et confidentielles.
22. Avez-vous un médecin de famille?
23. Êtes-vous responsable des soins primaires d'une personne souffrant d'une maladie de longue durée, d'un handicap physique ou mental, ou de problèmes liés au vieillissement?
24. Quelle est votre orientation sexuelle?
25. Laquelle des catégories suivantes décrit le mieux votre état matrimonial? [LIRE LA LISTE. ACCEPTER UNE SEULE RÉPONSE.]
26. Vivez-vous seul(e)?
26a. [SI « NON » À LA Q.26, DEMANDER] Veuillez indiquer si vous vivez avec l'une des personnes suivantes? [LIRE LA LISTE. SÉLECTIONNER TOUTES LES RÉPONSES QUI CORRESPONDENT. SI LA PERSONNE INTERROGÉE HABITE SEULE, SÉLECTIONNER UNE SEULE RÉPONSE]
27. Quel est le plus haut niveau de scolarité que vous ayez atteint? [LIRE LA LISTE.]
28. Laquelle des catégories suivantes décrit le mieux le revenu total de votre ménage avant impôts déclaré l'an dernier, provenant de toutes les sources pour tous les membres du ménage? [LIRE LA LISTE. ACCEPTER UNE SEULE RÉPONSE.]
[NE PAS LIRE] Je préfère ne pas répondre
29. À laquelle ou lesquelles des ethnies suivantes vous identifiez-vous? [ACCEPTER TOUTES LES RÉPONSES QUI CORRESPONDENT.]
29a. [SI L'ON RÉPOND PAR « AUTOCHTONE » À LA Q.29, DEMANDER :] Faites-vous partie des…? LIRE LA LISTE. SÉLECTIONNER UNE SEULE RÉPONSE.
29b. [SI L'ON RÉPOND PAR « AUTOCHTONE » À LA Q.29, DEMANDER :] Vivez-vous dans une réserve ou collectivité des Premières Nations pendant au moins 6 mois au cours de l'année?
30. Êtes-vous né(e) au Canada?
30a. [SI L'ON RÉPOND « NON » À LA Q.30, DEMANDER :] Depuis combien d'années habitez-vous au Canada?
31. Comment décririez-vous la région dans laquelle vous vivez? Est-ce...?
32. Laquelle des affirmations suivantes décrit le mieux vos conditions de vie actuelles? Est-ce que vous… ?
33. Qu'est-ce que nous n'avons pas demandé dans le cadre de ce sondage que vous aimeriez que nous sachions en parlant de vieillissement en santé? [QUESTION OUVERTE]
Health Canada/PHAC - Healthy Aging Research Study
DRAFT ONLINE Questionnaire (Feb. 1, 2023)
INTRODUCTION
Thanks for agreeing to participate in this survey. It is being conducted by The Strategic Counsel on behalf of The Public Health Agency of Canada to gauge your views on aging. It should take no more than 15-20 minutes to complete. All of your answers will be kept completely confidential and anonymous, and your participation is voluntary.
If you would like to request an alternative format of the survey, please contact:
Matt Proulx
Phone: 844-207-7527 ext. 4032
Email: Matthew.Proulx@logitgroup.com
Click here [POP UP IN NEW BROWSER WINDOW*] to verify its authenticity.
This research is sponsored by The Public Health Agency of Canada. Note that your participation will remain completely confidential and it will not affect your dealings with the Government of Canada, including The Public Health Agency of Canada, in any way. You may contact Trista Heney, Associate, The Strategic Counsel at 416-975-4465 ext. 272 to verify the legitimacy of this survey. TEXT TO SHOW ONCE RESPONDENT CLICKS:
Click here [POP-UP IN NEW BROWSER WINDOW*] for more information about how any personal information collected in this survey is handled.
The personal information you provide to The Public Health Agency of Canada is governed in accordance with the Privacy Act and is being collected under the authority of Section 4 of the Department of Health Act in accordance with the Treasury Board Directive on Privacy Practices. We only collect the information we need to conduct the research project.
Purpose of collection: We require your personal information such as demographic information to better understand the topic of the research. However, your responses are always combined with the responses of others for analysis and reporting; you will never be identified. For more information: This personal information collection is described in the standard personal information bank Public Communications - PSU 914, available online here.
Your rights under the Privacy Act: In addition to protecting your personal information, the Privacy Act gives you the right to request access to and correction of your personal information. You also have the right to file a complaint with the Privacy Commissioner of Canada if you think your personal information has been handled improperly. TEXT TO SHOW ONCE RESPONDENT CLICKS:
Click here [POP-UP IN NEW BROWSER WINDOW*] for more information about what happens after the survey is completed.
The final report, written by The Strategic Counsel, will be available to the public from Library and Archives Canada http://www.bac-lac.gc.ca/. TEXT TO SHOW ONCE RESPONDENT CLICKS
SCREENING QUESTIONS
1. In what language would you prefer to continue the survey?
2. In what year were you born? [PN: MANAGE QUOTAS FOR AGE]
[PN: INSERT DROPDOWN LIST]
In what month were you born?
[PN: DROPDOWN WITH MONTHS JAN-DEC]
IF UNDER 50 (BORN AFTER JAN 1973), TERMINATE
3. What is your gender? [PN: MANAGE QUOTAS FOR GENDER OVERALL - 48 MALE/52 FEMALE - AND FOR GENDER BY AGE]
4. Please provide the first 3 characters of your postal code. [PN: REASSIGN TO PROVINCES/TERRITORIES AND MANAGE QUOTAS BY REGION]
__ __ __
GENERAL HEALTH INFORMATION
5. Would you say your health in general is … ?
QUALITY OF LIFE AND CURRENT ACTIVITIES
The next few questions ask about your life, current routine, and the types of activities in which you are involved.
7. Overall, how would you rate your quality of life? Would you say it is …
| RANDOMIZE | Excellent | Good | Fair | Poor | Very Poor |
|---|---|---|---|---|---|
| Your mental well-being | ☐ | ☐ | ☐ | ☐ | ☐ |
| Your physical well-being | ☐ | ☐ | ☐ | ☐ | ☐ |
| Your relationships with other people | ☐ | ☐ | ☐ | ☐ | ☐ |
| Your participation in social and community activities | ☐ | ☐ | ☐ | ☐ | ☐ |
| Your sense of purpose in life | ☐ | ☐ | ☐ | ☐ | ☐ |
| Your financial well-being | ☐ | ☐ | ☐ | ☐ | ☐ |
| RANDOMIZE | At least once a day | At least once a week | At least once a month | At least once a year | Never |
|---|---|---|---|---|---|
| Physical activity (swimming, walking, dance, gardening) | ☐ | ☐ | ☐ | ☐ | ☐ |
| Hobbies or personal interests (painting, photography, birdwatching, music, taking a class) | ☐ | ☐ | ☐ | ☐ | ☐ |
| Activities at a local community centre (either in-person or virtual) | ☐ | ☐ | ☐ | ☐ | ☐ |
| Connecting with family and friends | ☐ | ☐ | ☐ | ☐ | ☐ |
| Volunteering | ☐ | ☐ | ☐ | ☐ | ☐ |
10. Which of the following best describes your current employment status? [PN: ACCEPT ONE ANSWER ONLY.]
11. [IF 'RETIRED' OR 'NOT IN THE WORKFORCE,' SKIP TO Q.12. ALL OTHERS, ASK] At what age do you anticipate retiring?
[PN: INSERT DROPDOWN LIST - 50 AND ABOVE]
OUTLOOK ON AGING
Now, we have a few questions about your views on aging.
12. How do you feel generally about the [PN: IF 50-64: prospect / IF 65+: experience] of getting older? Would you say that overall your feeling is …
13. What 2 things are you most concerned about as you age? [PN: RANDOMIZE AND ACCEPT UP TO TWO RESPONSES. 'OTHER, PLEASE SPECIFY' AND 'I AM NOT CONCERNED ABOUT AGING' SHOULD ALWAYS APPEAR LAST]
| RANDOMIZE | A lot | Somewhat | Not very much | Not at all |
|---|---|---|---|---|
| Mental and physical well-being | ☐ | ☐ | ☐ | ☐ |
| Cognitive/brain health | ☐ | ☐ | ☐ | ☐ |
| Being socially connected | ☐ | ☐ | ☐ | ☐ |
| Being active and mobile | ☐ | ☐ | ☐ | ☐ |
| Being independent | ☐ | ☐ | ☐ | ☐ |
| Being a contributor to society | ☐ | ☐ | ☐ | ☐ |
| Being able to age at home | ☐ | ☐ | ☐ | ☐ |
| Continuing to learn | ☐ | ☐ | ☐ | ☐ |
| Being valued | ☐ | ☐ | ☐ | ☐ |
| Being able to do what one feels is important | ☐ | ☐ | ☐ | ☐ |
15. Is there anything else that you associate with 'healthy aging?' [OPEN-END]
ENABLERS AND BARRIERS TO HEALTHY AGING
Healthy aging is about developing and maintaining the physical and cognitive abilities that enable wellbeing as one ages. It is supported by environments that allow people to do what they value as they age.
16. Overall, would you describe the community in which you currently live as being … ?
| RANDOMIZE | Excellent | Good | Fair | Poor | Very Poor |
|---|---|---|---|---|---|
| Affordable housing | ☐ | ☐ | ☐ | ☐ | ☐ |
| Health care, mental health and dental care services | ☐ | ☐ | ☐ | ☐ | ☐ |
| In-home services that support independent living | ☐ | ☐ | ☐ | ☐ | ☐ |
| Well-maintained sidewalks | ☐ | ☐ | ☐ | ☐ | ☐ |
| Accessible and affordable public transit | ☐ | ☐ | ☐ | ☐ | ☐ |
| Safe, easy to access buildings and public spaces | ☐ | ☐ | ☐ | ☐ | ☐ |
| Employment and volunteer opportunities for older adults | ☐ | ☐ | ☐ | ☐ | ☐ |
| Community-based social and recreational activities and events | ☐ | ☐ | ☐ | ☐ | ☐ |
| Accessible and affordable high-speed Internet | ☐ | ☐ | ☐ | ☐ | ☐ |
| Exercise programs for older adults | ☐ | ☐ | ☐ | ☐ | ☐ |
| Opportunities for lifelong learning | ☐ | ☐ | ☐ | ☐ | ☐ |
18. Many factors contribute to healthy aging. In your view, which two of the following are the most important? [PN: RANDOMIZE. ACCEPT UP TO TWO RESPONSES. 'OTHER, PLEASE SPECIFY' SHOULD ALWAYS APPEAR LAST.]
COMMUNICATIONS AND TECHNOLOGICAL LITERACY/PROFICIENCY
Now we have a couple of questions about how you do or would access information on the topic of healthy aging.
19. Who do you trust the most when it comes to providing you with information related to healthy aging? Please select up to 2 responses. [PN: RANDOMIZE. ACCEPT UP TO TWO RESPONSES. 'OTHER, PLEASE SPECIFY LAST' SHOULD ALWAYS APPEAR LAST.]
20. Do you recall seeing anything from the Government of Canada or the Public Health Agency of Canada on the topic of healthy aging in the last 2 years?
| RANDOMIZE | Very interested | Somewhat interested | Not very interested | Not interested at all |
|---|---|---|---|---|
| Healthy aging | ☐ | ☐ | ☐ | ☐ |
| Falls and injuries | ☐ | ☐ | ☐ | ☐ |
| Healthy nutrition | ☐ | ☐ | ☐ | ☐ |
| Maintaining physical and cognitive health | ☐ | ☐ | ☐ | ☐ |
| Preventing elder abuse | ☐ | ☐ | ☐ | ☐ |
| Aging at home | ☐ | ☐ | ☐ | ☐ |
| Oral health | ☐ | ☐ | ☐ | ☐ |
| Immunization | ☐ | ☐ | ☐ | ☐ |
DEMOGRAPHICS
These last few questions will allow us to compare the survey results among different groups of respondents. Your answers will remain anonymous and confidential.
22. Do you have a family doctor/physician?
23. Are you responsible for the primary care of someone with a long-term health condition, physical or mental disability, or problems related to aging?
24. What is your sexual orientation? [PN: ACCEPT ONE RESPONSE ONLY]
25. Which of the following best describes your marital status? [PN: ACCEPT ONE RESPONSE ONLY.]
26. Do you live alone?
26a. [PN: IF 'NO' AT Q.26, ASK] Please indicate whether you are living with any of the following? Please select all that apply.
27. What is the highest level of formal education that you have completed?
28. Which of the following best describes your total household income last year, before taxes, from all sources for all household members?
29. Which of the following ethnicity(ies) do you identify as? Please select all that apply.
29a. [IF INDIGENOUS AT Q.29, ASK:]Are you …?
29b.[IF INDIGENOUS AT Q.29, ASK]Do you live on a reserve or First Nation community for at least 6 months of the year?
30. Were you born in Canada?
30a. [IF NO AT Q.30, ASK] How many years have you lived in Canada?
31. How would you describe the area in which you reside? Is it …
32. Which of the following best describes your current living situation? Do you …
33. What didn't we ask as part of this survey, that you would like us to know about healthy aging? [OPEN-END]
Santé Canada/ASPC - Étude de recherche sur le vieillissement en santé
ÉBAUCHE du questionnaire EN LIGNE (le 6 février 2023)
INTRODUCTION
Nous vous remercions d'accepter de participer à ce sondage. Il est réalisé par The Strategic Counsel au nom de L'agence de la santé publique du Canada afin de connaître votre opinion sur le vieillissement. Participer à ce sondage ne devrait pas prendre plus de 15 à 20 minutes. Toutes vos réponses resteront totalement confidentielles et anonymes, et votre participation est volontaire.
Si vous souhaitez demander un autre format du sondage, veuillez communiquer avec:
Matt Proulx
Téléphone: 844-207-7527 ext. 4032
E-mail: Matthew.Proulx@logitgroup.com
Cliquez ici [AFFICHER DANS UNE NOUVELLE FENÊTRE DU NAVIGATEUR*] pour vérifier son authenticité.
Cette recherche est parrainée par L'agence de la santé publique du Canada. Veuillez noter que votre participation restera totalement confidentielle et qu'elle n'affectera en rien vos relations avec le gouvernement du Canada, y compris L'agence de la santé publique du Canada. Vous pouvez contacter Trista Heney, Associate, The Strategic Counsel à 416-975-4465 ext. 272 pour vérifier la légitimité de ce sondage. TEXTE À AFFICHER LORSQU'UN RÉPONDANT CLIQUE :
Cliquez ici [AFFICHER DANS UNE NOUVELLE FENÊTRE DU NAVIGATEUR *] pour plus d'information sur la façon dont sont traités les renseignements personnels recueillis dans le cadre de ce sondage.
Les renseignements personnels que vous fournissez à L'agence de la santé publique du Canada sont régis par la Loi sur la protection des renseignements personnels et sont recueillis en vertu de l'article 4 de la Loi sur le ministère de la Santé, conformément à la Directive du Conseil du Trésor sur les pratiques relatives à la protection de la vie privée. Nous ne recueillons que l'information dont nous avons besoin pour mener à bien le projet de recherche.
Objectif de la collecte : Nous avons besoin de vos renseignements personnels, comme les données démographiques, pour mieux comprendre le sujet de la recherche. Cependant, vos réponses sont toujours combinées à celles des autres répondants à des fins d''analyse et de rapport. Vous ne serez jamais identifié(e). Pour plus d'information : Cette collecte de renseignements personnels est décrite dans le fichier de renseignements personnels Communications publiques (POU 914) disponible en ligne ici. Vos droits en vertu de la Loi sur la protection des renseignements personnels : En plus de protéger vos renseignements personnels, la Loi sur la protection des renseignements personnels vous donne le droit de demander l'accès et la correction de vos renseignements personnels. Vous avez également le droit de déposer une plainte auprès du Commissaire à la protection de la vie privée du Canada si vous pensez que vos renseignements personnels ont été traités de façon inappropriée. TEXTE À AFFICHER LORSQU'UN RÉPONDANT CLIQUE :
Cliquez ici [AFFICHER DANS UNE NOUVELLE FENÊTRE DU NAVIGATEUR*] pour savoir ce qui se passera à la suite du sondage.
Le rapport final, préparé par le cabinet The Strategic Counsel, sera accessible au public sur le site Web de Bibliothèque et Archives Canada : http://www.bac-lac.gc.ca/ TEXTE À AFFICHER LORSQU'UN RÉPONDANT CLIQUE :
QUESTIONS DE SÉLECTION
1. In what language would you prefer to continue the survey?
Dans quelle langue préféreriez-vous poursuivre l'enquête?
2. En quelle année êtes-vous né(e)? [Note : GÉRER LES QUOTAS PAR AGE]
[Note : INSÉRER UNE LISTE DÉROULANTE DES ANNÉES]
En quel mois êtes-vous né(e)?
[Note : INSÉRER UNE LISTE DÉROULANTE DES MOIS]
SI AGÉ DE MOINS DE 50 ANS (NÉ APRÈS jan 1973), TERMINER.
3. Quel est votre genre? [Note : GÉRER LES QUOTAS PAR GENRE GLOBAL ET PAR GENRE SELON L'AGE ]
4. Veuillez fournir les 3 premiers caractères de votre code postal. [Note : RÉATTRIBUER AUX PROVINCES-TERRITOIRES ET GÉRER PAR RÉGION ]
__ __ __
RENSEIGNEMENTS GÉNÉRAUX SUR LA SANTÉ
5. Diriez-vous que votre santé en général est...?
6. Vous identifiez-vous à l'un des groupes suivants? Sélectionnez toutes les réponses qui correspondent.
QUALITÉ DE VIE ET ACTIVITÉS PRÉSENTES
Les quelques questions qui suivent portent sur votre vie, votre routine et les types d'activités auxquelles vous participez.
7. Dans l'ensemble, comment évalueriez-vous votre qualité de vie? Diriez-vous qu'elle est…?
| METTRE AU HASARD | Excellente | Bonne | Acceptable | Mauvaise | Très mauvaise |
|---|---|---|---|---|---|
| Votre bien-être mental | ☐ | ☐ | ☐ | ☐ | ☐ |
| Votre bien-être physique | ☐ | ☐ | ☐ | ☐ | ☐ |
| Vos relations avec les autres | ☐ | ☐ | ☐ | ☐ | ☐ |
| Votre participation à des activités sociales et communautaires | ☐ | ☐ | ☐ | ☐ | ☐ |
| Votre raison de vivre | ☐ | ☐ | ☐ | ☐ | ☐ |
| Votre bien-être financier | ☐ | ☐ | ☐ | ☐ | ☐ |
| PRÉSENTER LES OPTIONS ALÉATOIREMENT | Au moins une fois par jour | Au moins une fois par semaine | Au moins une fois par mois | Au moins une fois par année | Jamais |
|---|---|---|---|---|---|
| Activité physique (natation, marche, danse, jardinage) | ☐ | ☐ | ☐ | ☐ | ☐ |
| Passe-temps ou intérêts personnels (peinture, photographie, observation des oiseaux, musique, suivre un cours) | ☐ | ☐ | ☐ | ☐ | ☐ |
| Activités dans un centre communautaire local (en personne ou en virtuel) | ☐ | ☐ | ☐ | ☐ | ☐ |
| Communiquer avec la famille et les amis | ☐ | ☐ | ☐ | ☐ | ☐ |
| Faire du bénévolat | ☐ | ☐ | ☐ | ☐ | ☐ |
10. Quelle affirmation parmi les suivantes décrit le mieux votre situation d'emploi actuelle? Est-ce que vous…? [ACCEPTER UNE SEULE RÉPONSE.]
11. [SI « RETRAITÉ » OU « NE FAIT PAS PARTIE DE LA POPULATION ACTIVE », PASSER À Q.12. SI « AUTRE », DEMANDER] À quel âge pensez-vous prendre votre retraite?
[Note : INSÉRER UNE LISTE DÉROULANTE - 50 ET PLUS]
À PROPOS DU VIEILLISSEMENT
Maintenant, nous avons quelques questions concernant votre opinion sur le vieillissement.
12. Que pensez-vous en général de [si âgé de 50 à 64 ans : la perspective de vieillir / si âgé de 65 ans et plus: l'expérience du vieillissement] ? Diriez-vous que votre sentiment général est :
13. Quelles sont les 2 choses qui vous préoccupent le plus en vieillissant? [Note : PRÉSENTER LES OPTIONS ALÉATOIREMENT SI POSSIBLE ET ACCEPTER JUSQU'À DEUX RÉPONSES. SI POSSIBLE, INCITER À FOURNIR « AUTRE, VEUILLEZ PRÉCISER » et « JE NE ME PRÉOCCUPE PAS DU VIEILLISSEMENT » EN DERNIER]
| PRÉSENTER LES OPTIONS ALÉATOIREMENT | Beaucoup | Un peu | Pas beaucoup | Pas du tout |
|---|---|---|---|---|
| Bien-être mental et physique | ☐ | ☐ | ☐ | ☐ |
| Santé cognitive ou du cerveau | ☐ | ☐ | ☐ | ☐ |
| Être en contact avec les autres | ☐ | ☐ | ☐ | ☐ |
| Être actif(ve) et mobile | ☐ | ☐ | ☐ | ☐ |
| Être indépendant(e) | ☐ | ☐ | ☐ | ☐ |
| Apporter une contribution à la société | ☐ | ☐ | ☐ | ☐ |
| Pouvoir vieillir à la maison | ☐ | ☐ | ☐ | ☐ |
| Continuer d'apprendre | ☐ | ☐ | ☐ | ☐ |
| Être apprécié(e) | ☐ | ☐ | ☐ | ☐ |
| Pouvoir faire ce que l'on juge important | ☐ | ☐ | ☐ | ☐ |
15. Y a-t-il autre chose que vous associez au « vieillissement en santé »? [QUESTION OUVERTE]]
FACTEURS HABILITANTS ET OBSTACLES AU VIELLISSEMENT EN SANTÉ
Le vieillissement en santé consiste à développer et maintenir les capacités physiques et cognitives qui favorisent le bien-être en vieillissant. Il est favorisé par des environnements qui permettent aux gens de faire ce qu'ils aiment en prenant de l'âge.
16. De façon générale, décririez-vous la collectivité dans laquelle vous vivez actuellement comme étant...?
| PRÉSENTER LES OPTIONS ALÉATOIREMENT | Excellente | Bonne | Acceptable | Mauvaise | Très mauvaise |
|---|---|---|---|---|---|
| Logement abordable | ☐ | ☐ | ☐ | ☐ | ☐ |
| Services de soins de santé, de soins dentaires et services en santé mentale | ☐ | ☐ | ☐ | ☐ | ☐ |
| Services à domicile qui favorisent une vie indépendante | ☐ | ☐ | ☐ | ☐ | ☐ |
| Trottoirs bien entretenus | ☐ | ☐ | ☐ | ☐ | ☐ |
| Transport en commun accessible et abordable | ☐ | ☐ | ☐ | ☐ | ☐ |
| Bâtiments et espaces publics sûrs et faciles d'accès | ☐ | ☐ | ☐ | ☐ | ☐ |
| Possibilités d'emploi et de bénévolat pour les adultes plus âgés | ☐ | ☐ | ☐ | ☐ | ☐ |
| Activités et événements sociaux et récréatifs communautaires | ☐ | ☐ | ☐ | ☐ | ☐ |
| Internet haute vitesse accessible et abordable | ☐ | ☐ | ☐ | ☐ | ☐ |
| Programmes d'exercices pour les adultes plus âgés | ☐ | ☐ | ☐ | ☐ | ☐ |
| Possibilités d'apprentissage tout au long de la vie | ☐ | ☐ | ☐ | ☐ | ☐ |
18. De nombreux facteurs contribuent à un vieillissement en santé. Selon vous, quels sont les deux facteurs suivants qui sont les plus importants? Est-ce…? [Note :PRÉSENTER LES OPTIONS ALÉATOIREMENT. ACCEPTER JUSQU'À DEUX RÉPONSES. INCITER À FOURNIR « TOUTE AUTRE RÉPONSE » EN DERNIER.]
LITÉRACIE/COMPÉTENCES EN MATIRE DE COMMUNICATIONS ET DE TECHNOLOGIE
Nous avons maintenant quelques questions sur la façon dont vous accédez ou souhaiteriez accéder à l'information sur le thème du vieillissement en santé.
19. À qui faites-vous le plus confiance lorsqu'il s'agit de vous fournir de l'information sur le vieillissement en santé? Veuillez sélectionner jusqu'à 2 réponses. [Note :PRÉSENTER LES OPTIONS ALÉATOIREMENT. ACCEPTER JUSQU'À DEUX RÉPONSES.INCITER À FOURNIR « TOUTE AUTRE RÉPONSE » EN DERNIER. ]
20. Vous souvenez-vous d'avoir vu quelque chose de la part du gouvernement du Canada ou de l'Agence de la santé publique du Canada sur le thème du vieillissement en santé au cours des 2 dernières années?
| PRÉSENTER LES OPTIONS ALÉATOIREMENT | Très intéressé(e) | Plutôt intéressé(e) | Pas très intéressé(e) | Pas du tout intéressé(e) |
|---|---|---|---|---|
| Vieillissement en santé | ☐ | ☐ | ☐ | ☐ |
| Chutes et blessures | ☐ | ☐ | ☐ | ☐ |
| Alimentation saine | ☐ | ☐ | ☐ | ☐ |
| Maintien de la santé physique et cognitive | ☐ | ☐ | ☐ | ☐ |
| Prévention de la maltraitance des personnes âgées | ☐ | ☐ | ☐ | ☐ |
| Vieillir à domicile | ☐ | ☐ | ☐ | ☐ |
| Santé buccodentaire | ☐ | ☐ | ☐ | ☐ |
| Immunisation | ☐ | ☐ | ☐ | ☐ |
COMPOSANTE DÉMOGRAPHIQUE
Ces quelques dernières questions nous permettront de comparer les résultats du sondage entre différents groupes de répondants. Vos réponses demeureront anonymes et confidentielles.
22. Avez-vous un médecin de famille?
23. Êtes-vous responsable des soins primaires d'une personne souffrant d'une maladie de longue durée, d'un handicap physique ou mental, ou de problèmes liés au vieillissement?
24. Quelle est votre orientation sexuelle? [Note : ACCEPTER UNE SEULE RÉPONSE.]
25. Laquelle des catégories suivantes décrit le mieux votre état matrimonial? [Note : ACCEPTER UNE SEULE RÉPONSE.]
26. Vivez-vous seul(e)?
26a. [Note : SI « NON » À LA Q.26, DEMANDER] Veuillez indiquer si vous vivez avec l'une des personnes suivantes? Sélectionnez toutes les réponses qui correspondent.
27. Quel est le plus haut niveau de scolarité que vous ayez atteint?
28. Laquelle des catégories suivantes décrit le mieux le revenu total de votre ménage avant impôts déclaré l'an dernier, provenant de toutes les sources pour tous les membres du ménage? [Note : ACCEPTER UNE SEULE RÉPONSE.]
29. À laquelle ou lesquelles des ethnies suivantes vous identifiez-vous? Sélectionnez toutes les réponses qui correspondent.
29a. [SI L'ON RÉPOND PAR « AUTOCHTONE » À LA Q.29, DEMANDER :] Faites-vous partie des…?
29b.[SI L'ON RÉPOND PAR « AUTOCHTONE » À LA Q.29, DEMANDER :]Vivez-vous dans une réserve ou collectivité des Premières Nations pendant au moins 6 mois au cours de l'année?
30. Êtes-vous né(e) au Canada?
30a. [SI L'ON RÉPOND « NON » À LA Q.30, DEMANDER :] Depuis combien d'années habitez-vous au Canada?
31. Comment décririez-vous la région dans laquelle vous vivez? Est-ce...?
32. Laquelle des affirmations suivantes décrit le mieux vos conditions de vie actuelles? Est-ce que vous...?
33. Qu'est-ce que nous n'avons pas demandé dans le cadre de ce sondage que vous aimeriez que nous sachions en parlant de vieillissement en santé? [QUESTION OUVERTE]
RECRUITMENT SPECIFICATIONS
| Group | Date | Time (EST) | Location | Composition |
|---|---|---|---|---|
| 1 | Mon., March 13th | 5:00-6:30 | Atlantic | Urban |
| 2 | Mon., March 13th | 5:00-6:30 | Atlantic | Rural |
| 3 | Mon., March 13th | 7:00-8:30 | Nationwide | Older men |
| 4 | Tues., March 14th | 5:00-6:30 | Ontario | Urban |
| 5 | Tues., March 14th | 7:00-8:30 | Ontario | Rural |
| 6 | Tues., March 14th | 8:00-9:30 | Nationwide | Older adults with high SES |
| 9 | Wed., March 15th | 6:30-8:00 | Nationwide | Older women |
| 10 | Thurs., March 16th | 7:30-9:00 | Prairies | Urban |
| 11 | Thurs., March 16th | 9:00-10:30 | Prairies | Rural |
| 12 | Mon., March 20th | 6:30-8:00 | Nationwide | Older adults identifying as racialized |
| 13 | Mon., March 20th | 7:30-9:00 | Nationwide | Older adults with low SES |
| 14 | Tues., March 21st | 7:30-9:00 | BC/North | Urban |
| 15 | Tues., March 21st | 8:00-9:30 | Nationwide | Indigenous older adults |
| 16 | Wed., March 22nd | 8:30-10:00 | BC/North | Rural |
| 17 | Wed., March 22nd | 8:00-9:30 | Nationwide | Older adults living with disabilities |
| 18 | Thurs., March 23rd | 7:00-8:30 | Nationwide | Older adults identifying as LGBTQ2S+ |
| 19 | Thurs., March 23rd | 7:30-9:00 | Nationwide | Older adult newcomers to Canada |
INTRODUCTION
Hello, my name is [RECRUITER NAME]. I'm calling from The Strategic Counsel, a national public opinion research firm, on behalf of the Government of Canada. / Bonjour, je m'appelle [NOM DU RECRUTEUR]. Je vous téléphone du Strategic Counsel, une entreprise nationale de recherche sur l'opinion publique, pour le compte du gouvernement du Canada.
Would you prefer to continue in English or French? / Préfériez-vous continuer en français ou en anglais? [CONTINUE IN LANGUAGE OF PREFERENCE]
RECORD LANGUAGE
English CONTINUE
French THANK AND END
On behalf of the Government of Canada, we're organizing a series of online video focus group discussions to explore your views on aging.
The format is a "round table" discussion, led by an experienced moderator. Participants will be given a cash honorarium in appreciation of their time.
Your participation is completely voluntary and all your answers will be kept confidential. We are only interested in hearing your opinions - no attempt will be made to sell or market you anything. The report that is produced from the series of discussion groups we are holding will not contain comments that are attributed to specific individuals.
But before we invite you to attend, we need to ask you a few questions to ensure that we get a good mix/variety of people in each of the groups. May I ask you a few questions?
SCREENING QUESTIONS
1. Have you, or has anyone in your household, worked for any of the following types of organizations in the last 5 years?
1a. Are you a retired Government of Canada employee?
| Under 18 years of age | IF POSSIBLE, ASK FOR SOMEONE OVER 18 AND REINTRODUCE. OTHERWISE THANK AND END. |
| 18-49 | THANK AND END |
| 50-54 | CONTINUE |
| 55-59 | CONTINUE |
| 60-64 | CONTINUE |
| 65-69 | CONTINUE |
| 70-74 | CONTINUE |
| 75+ | CONTINUE |
| VOLUNTEERED Prefer not to answer | THANK AND END |
ENSURE A GOOD MIX.
| LOCATION | CITIES | |
|---|---|---|
| Urban Atlantic |
Cities could include (but are not limited to):
ENSURE A GOOD MIX. NO MORE THAN TWO PER PROVINCE. |
CONTINUE -GROUP 1 |
| Rural Atlantic |
Towns could include (but are not limited to):
ENSURE A GOOD MIX. NO MORE THAN TWO PER PROVINCE. |
CONTINUE -GROUP 2 |
| Urban Ontario |
Cities could include (but are not limited to): Toronto, Ottawa, Hamilton, Kitchener, London, Oshawa, Windsor, Barrie, Guelph, Kingston, Thunder Bay, Sudbury, Peterborough, North Bay, Cornwall ENSURE A GOOD MIX OF CITIES ACROSS THE REGION. NO MORE THAN TWO PER CITY. |
CONTINUE -GROUP 4 |
| Rural Ontario |
Towns/villages could include: Alberton, Algonquin Highlands, Amaranth, Bancroft, Blue Mountains, Bracebridge, Brock, Callander, Central Huron, Champlain, Chatsworth, Cochrane, Deep River, Dryden, Elliot Lake, Enniskillen, Gravenhurst, Hanover, Hawkesbury, Huntsville, Kincardine, Laurentian Hills, Muskoka Lakes, Nipissing, Parry Sound, Petawawa, Red Lake, Temiskaming Shores, Tweed ENSURE A GOOD MIX. |
CONTINUE -GROUP 5 |
| Urban Prairies |
Cities include (but are not limited to):
ENSURE A GOOD MIX OF CITIES ACROSS THE REGION. NO MORE THAN TWO PER PROVINCE. |
CONTINUE -GROUP 10 |
| Rural Prairies |
Cities include (but are not limited to):
ENSURE A GOOD MIX OF CITIES ACROSS THE REGION. NO MORE THAN TWO PER PROVINCE. |
CONTINUE -GROUP 11 |
| Urban BC/North |
Cities include:
ENSURE A GOOD MIX OF CITIES ACROSS THE REGION. |
CONTINUE -GROUP 14 |
| Rural BC/Rural and Urban North |
Cities include:
ENSURE A GOOD MIX OF CITIES ACROSS THE REGION. SKEW TO THOSE RESIDING IN SMALLER COMMUNITIES. |
CONTINUE -GROUP 16 |
| Canada |
RECORD PROVINCE AND CITY/TOWN/VILLAGE ENSURE A GOOD MIX BETWEEN PROVINCES |
CONTINUE -GROUP 3, 6, 9, 12, 13, 15, 17, 18, 19 |
4. Were you born in Canada?
VOLUNTEEREDPrefer not to answerTHANK AND END
| Less than 5 years | CONTINUE |
| 5 to <10 years |
|
| 10 to <20 years |
|
| 20 to <30 years |
|
| 30 or more years |
|
| Don't know/Prefer not to answer | THANK AND END |
ENSURE A GOOD MIX BY TIME LIVED IN CANADA.
4b. ASK ONLY IF GROUP 19 Which country did you migrate from to come to Canada?
5. ASK ONLY IF GROUP 18What gender do you identify with? [INTERVIEWER TO READ ALL]
5a.ASK ONLY IF GROUP 18How do you describe your sexual orientation? [INTERVIEWER TO READ ALL]
IF RESPONDENT SELECTS EITHER 'MALE' OR 'FEMALE' AT Q.5 AND 'STRAIGHT/HETEROSEXUAL' AT Q.5A, THANK AND END. ENSURE A GOOD MIX. LIMIT THE NUMBER OF 'OTHER, PLEASE SPECIFY'
6. ASK ONLY IF GROUP 15Do you identify as Indigenous?
6a. ASK ONLY IF GROUP 15Do you identify as … ?
ENSURE A GOOD MIX ON AND OFF RESERVE.
7. ASK ONLY IF GROUP 17Do you identify as any of the following? Select all that apply.
A person with a disability? A person with a disability is a person who has a long-term or recurring impairment (such as vision, hearing, mobility, flexibility, dexterity, pain, learning, developmental, memory or mental-health related) which limits their daily activities inside or outside the home (such as school, work or in the community in general). CONTINUE
Someone with a medical condition that weakens your body's ability to fight off infections (such as heart disease, diabetes, HIV, asthma)?
7a. ASK ONLY IF GROUP 17What type of disabilities and/or health conditions do you live with? Select all that apply.
ENSURE A GOOD MIX.
8. ASK ONLY OF GROUP 12Do you self-identify as a visible minority as defined by the Employment Equity Act? IF REQUIRED, INTERVIEWER TO READ: The Act defines visible minorities as "persons, other than Aboriginal peoples, who are non-Caucasian in race or non-white in colour."
9. DO NOT ASK GROUP 15Which of the following racial or cultural groups best describes you? (multi-select)
ENSURE A GOOD MIX.
10. DO NOT ASKRecord gender.
| Under $20,000 | IF GROUP 6, THANK AND END |
| $20,000 to just under $40,000 | IF GROUP 6, THANK AND END |
| $40,000 to just under $60,000 | IF GROUP 6, THANK AND END |
| $60,000 to just under $80,000 | IF GROUP 6 OR 13, THANK AND END |
| $80,000 to just under $100,000 | IF GROUP 13, THANK AND END |
| $100,000 to just under $150,000 | IF GROUP 13, THANK AND END |
| $150,000 and above | IF GROUP 13, THANK AND END |
| VOLUNTEERED Prefer not to answer | THANK AND END |
ENSURE A GOOD MIX.
| Grade 8 or less | IF GROUP 6, THANK AND END |
| Some high school | IF GROUP 6, THANK AND END |
| High school diploma or equivalent | IF GROUP 6, THANK AND END |
| Registered Apprenticeship or other trades certificate or diploma | IF GROUP 13, THANK AND END |
| College, CEGEP or other non-university certificate or diploma | IF GROUP 13, THANK AND END |
| University certificate or diploma below bachelor's level | IF GROUP 13, THANK AND END |
| Bachelor's degree | IF GROUP 13, THANK AND END |
| Post graduate degree above bachelor's level | IF GROUP 13, THANK AND END |
| VOLUNTEERED Prefer not to answer | THANK AND END |
ENSURE A GOOD MIX.
13. Which of the following categories best describes your current employment status? Are you…
ENSURE A GOOD MIX. MAY SKEW RETIRED.
14. Would you be comfortable reading a document and participating in a group discussion in English?
[NOTE TO INTERVIEWER - IF RESPONDENT INDICATES AT ANY POINT THAT THEY WILL NEED THE ASSISTANCE OF A CAREGIVER OR PERSONAL SUPPORT WORKER IN ORDER TO PARTICIPATE, PLEASE ASSURE THAT WE WILL ACCOMMODATE]
15. Have you attended a focus group discussion, or participated in an interview or survey, which was arranged in advance and for which you received a sum of money?
16. How long ago was that?
17. As this group is being conducted online, in order to participate you will need to have high-speed Internet and a computer with a working webcam, microphone and speaker. RECRUITER TO CONFIRM THE FOLLOWING. TERMINATE IF NO TO ANY.
19. How skilled are you at using online meeting platforms on your own, using a scale of 1 to 5, where 1 means you are not at all skilled, and 5 means you are very skilled?
20. During the discussion, you could be asked to read or view materials on screen and/or participate in poll-type exercises online. You will also be asked to actively participate online using a webcam. Can you think of any reason why you may have difficulty reading the materials or participating by video?
IF RESPONDENT OFFERS ANY REASON SUCH AS SIGHT OR HEARING PROBLEM, A WRITTEN OR VERBAL LANGUAGE PROBLEM, A CONCERN WITH NOT BEING ABLE TO COMMUNICATE EFFECTIVELY, ANY CONCERNS WITH USING A WEBCAM OR IF YOU AS THE INTERVIEWER HAVE A CONCERN ABOUT THE PARTICIPANT'S ABILITY TO PARTICIPATE EFFECTIVELY, PLEASE ASSESS WHETHER ACCOMMODATIONS CAN BE MADE.
The next question is creative in nature - please have fun when answering!
21. If you could invite someone to dinner, past or present, who would you invite, and why?
NOTE: RESPONDENTS THAT ARE INVITED TO PARTICIPATE MUST BE ARTICULATE AND ABLE TO EXPRESS THEMSELVES WITH EASE. ALL PARTICIPANTS MUST EXHIBIT REASONABLE ABILITY TO ARTICULATE COHERENT THOUGHTS, IN COMPLETE SENTENCES, AND RESPOND FAIRLY PROMPTLY. PLEASE ENSURE:
If there is any doubt, PLEASE DON'T RECRUIT!
22. The focus group discussion will be recorded for research purposes only. Do you consent to being recorded?
23. The report that will be prepared based on the discussions may contain anonymous quotations from participants. These quotations will not identify you, but may include comments that you made during the discussion. Do you consent to being quoted anonymously in the report that will be prepared following the groups?
INVITATION TO FOCUS GROUP:
I would like to invite you to a focus group discussion. You will receive a $100 honorarium in appreciation for your time. The discussion will last about 90 minutes and will be held:
INSERT DATE AND TIME OF GROUP BASED ON CHART ON PAGE 1.
We will be calling to verify the information given and will confirm this appointment the day before. May I please have your full name, a telephone number that is best to reach you at, and your e-mail address to send you the details for the group?
You will receive an e-mail from [insert recruiter] with the instructions to login to the online group. Should you have any issues logging into the system specifically, you can contact our technical support team at support@thestrategiccounsel.com .
We ask that you are online at least 15 minutes prior to the beginning of the session in order to ensure you are set up and to allow our support team to assist you in case you run into any technical issues.
You may be required to view some material during the course of the discussion. If you require glasses to do so, please be sure to have them handy at the time of the group. Also, you will need pen and paper in order to take some notes throughout the group.
This is a firm commitment. If you anticipate anything preventing you from attending (either home- or work-related), please let me know now and we will keep your name for a future study.
If for any reason you are unable to attend, please let us know as soon as possible at [1-800-xxx-xxxx]so we can find a replacement.
Thank you very much for your time.
RECRUITED BY: ____________________
DATE RECRUITED: __________________
CONSIGNES DE RECRUTEMENT
| GROUPE | DATE | HEURE (DE L'EST) |
LIEU | COMPOSITION DU GROUPE |
|---|---|---|---|---|
| 7 | 15 mars | 17 h 00-18 h 30 | Québec | Urbain |
| 8 | 15 mars | 19 h 00-20 h 30 | Québec | Rural |
INTRODUCTION
Bonjour, je m'appelle [NOM DU RECRUTEUR].Je vous téléphone du Strategic Counsel, une entreprise nationale de recherche sur l'opinion publique, pour le compte du gouvernement du Canada. / Hello, my name is [RECRUITER NAME]. I'm calling from The Strategic Counsel, a national public opinion research firm, on behalf of the Government of Canada.
Préfériez-vous continuer en français ou en anglais? / Would you prefer to continue in English or French? [CONTINUER DANS LA LANGUE PRÉFÉRÉE]
NOTER LA LANGUE ET CONTINUER
Nous organisons, pour le compte du gouvernement du Canada, une série de groupes de discussion vidéo en ligne afin d'explorer votre point de vue sur le vieillissement.
La rencontre prendra la forme d'une table ronde animée par un modérateur expérimenté. Les participants recevront un montant d'argent en remerciement de leur temps.
Votre participation est entièrement volontaire et toutes vos réponses seront confidentielles. Nous aimerions simplement connaître vos opinions : personne n'essaiera de vous vendre quoi que ce soit ou de promouvoir des produits. Notre rapport sur cette série de groupes de discussion n'attribuera aucun commentaire à une personne en particulier.
Avant de vous inviter à participer, je dois vous poser quelques questions qui nous permettront de former des groupes suffisamment diversifiés. Puis-je vous poser quelques questions?
QUESTIONS DE SÉLECTION
| Une société d'études de marché | REMERCIER ET CONCLURE |
| Une agence de commercialisation, de marque ou de publicité | REMERCIER ET CONCLURE |
| Un magazine ou un journal | REMERCIER ET CONCLURE |
| Un ministère ou un organisme gouvernemental fédéral, provincial ou territorial | REMERCIER ET CONCLURE |
| Un parti politique | REMERCIER ET CONCLURE |
| Dans les relations publiques ou les relations avec les médias | REMERCIER ET CONCLURE |
| Dans le milieu de la radio ou de la télévision | REMERCIER ET CONCLURE |
| Non, aucune de ces réponses | CONTINUER |
1a. Êtes-vous un ou une employé(e) retraité(e) du gouvernement du Canada?
| Moins de 18 ans | SI POSSIBLE, DEMANDER À PARLER À UNE PERSONNE DE 18 ANS OU PLUS ET REFAIRE L'INTRODUCTION. SINON, REMERCIER ET CONCLURE |
| 18 à 49 ans | REMERCIER ET CONCLURE |
| 50 à 54 ans | CONTINUER |
| 55 à 59 ans | CONTINUER |
| 60 à 64 ans | CONTINUER |
| 65 à 69 ans | CONTINUER |
| 70 à 74 ans | CONTINUER |
| 75 ans ou plus | CONTINUER |
RÉPONSE SPONTANÉE |
REMERCIER ET CONCLURE |
ASSURER UN BON MÉLANGE.
| LIEU | VILLES | |
|---|---|---|
| Québec urbain |
Ces villes peuvent notamment comprendre : Montréal, Québec, Gatineau, Laval, Sherbrooke, Trois-Rivières, Saguenay, Saint-Jean-sur-Richelieu, Châteauguay, Drummondville, Granby, Beloeil, Saint-Hyacinthe, Victoriaville, Salaberry-de-Valleyfield, Rimouski. ASSURER UN BON MÉLANGE. |
CONTINUER -GROUPE 7 |
| Québec rural |
Les villes peuvent inclure (mais ne sont pas limitées à) : Val-David, Sainte-Madeleine, Laurier Station, Pointe-Lebel, Chute-aux-Outardes, La Guadeloupe, Price, Fort-Coulonge, Pointe-aux-Outardes, Grenville, Roxton Falls, Hébertville-Station, Saint-Jeanne-d'Arc, Ayer's Cliff, Stukley Sud. ASSURER UN BON MÉLANGE. |
CONTINUER -GROUPE 8 |
4. Êtes-vous né(e) au Canada?
RÉPONSE SPONTANÉEPréfère ne pas répondreREMERCIER ET CONCLURE
| Moins de 5 ans | CONTINUER |
| 5 ans à moins de 10 ans | |
| 10 ans à moins de 20 ans | |
| 20 ans à moins de 30 ans | |
| 30 ans ou plus | |
| Je ne sais pas/je préfère ne pas répondre | REMERCIER ET CONCLURE |
BIEN REPRÉSENTER LES PARTICIPANTS EN FONCTION DU NOMBRE D'ANNÉES VÉCUES AU CANADA.
5. Lequel ou lesquels des groupes raciaux ou culturels suivants vous décrivent le mieux? (plusieurs réponses possibles)
VISER UNE COMPOSITION DIVERSIFIÉE SUR LE PLAN DE L'APPARTENANCE AUX GROUPES RACIAUX/CULTURELS
6. NE PAS POSER LA QUESTION Noter le sexe.
| Moins de 20 000 $ | |
| 20 000 $ à moins de 40 000 $ | |
| 40 000 $ à moins de 60 000 $ | |
| 60 000 $ à moins de 80 000 $ | |
| 80 000 $ à moins de 100 000 $ | |
| 100 000 $ à moins de 150 000 $ | |
| 150 000 $ ou plus | |
| RÉPONSE SPONTANÉE : Préfère ne pas répondre | REMERCIER ET CONCLURE |
ASSURER UN BON MÉLANGE.
| École primaire | |
| Études secondaires partielles | |
| Diplôme d'études secondaires ou l'équivalent | |
| Certificat ou diplôme d'apprenti inscrit ou d'une école de métiers | |
| Certificat ou diplôme d'un collège, cégep ou autre établissement non universitaire | |
| Certificat ou diplôme universitaire inférieur au baccalauréat | |
| Baccalauréat | |
| Diplôme d'études supérieur au baccalauréat | |
| RÉPONSE SPONTANÉE : Préfère ne pas répondre | REMERCIER ET CONCLURE |
ASSURER UN BON MÉLANGE.
9. Laquelle de ces descriptions correspond le mieux à votre situation d'emploi actuelle? Est-ce que…
ASSURER UN BON MÉLANGE. PEUT BIAISER LES RETRAITÉS.
10. Seriez-vous à l'aise de lire un document et de participer à une discussion de groupe en français?
[NOTE POUR L'INTERVIEWEUR - SI LA PERSONNE INTERROGÉE INDIQUE À UN MOMENT DONNÉ QU'ELLE AURA BESOIN DE L'AIDE D'UN SOIGNANT OU D'UN ASSISTANT PERSONNEL POUR PARTICIPER, ASSUREZ-VOUS QUE NOUS ALLONS NOUS ADAPTER].
11. Avez-vous déjà participé à un groupe de discussion, à une entrevue ou à un sondage organisé à l'avance en contrepartie d'une somme d'argent?
12. C'était il y a combien de temps?
13. Étant donné que ce groupe se réunira en ligne, vous aurez besoin, pour participer, d'un accès Internet haut débit et d'un ordinateur muni d'une caméra Web, d'un microphone et d'un haut-parleur en bon état de marche. CONFIRMER LES POINTS CI-DESSOUS. METTRE FIN À L'APPEL SI NON À L'UN DES DEUX.
14. Avez-vous utilisé des logiciels de réunion en ligne tels que Zoom, Webex, Microsoft Teams, Google Hangouts/Meet, etc., au cours des deux dernières années?
15. Sur une échelle de 1 à 5 où 1 signifie que vous n'êtes pas du tout habile et 5 que vous êtes très habile, comment évaluez-vous votre capacité à utiliser seul(e) les plateformes de réunion en ligne?
16. Au cours de la discussion, vous pourriez devoir lire ou visionner du matériel affiché à l'écran, ou faire des exercices en ligne comme ceux qu'on trouve dans les sondages. On vous demandera aussi de participer activement à la discussion en ligne à l'aide d'une caméra Web . Pensez-vous avoir de la difficulté, pour une raison ou une autre, à lire les documents ou à participer à la discussion par vidéo?
SI LE RÉPONDANT SIGNALE UN PROBLÈME DE VISION OU D'AUDITION, UN PROBLÈME DE LANGUE PARLÉE OU ÉCRITE, S'IL CRAINT DE NE POUVOIR COMMUNIQUER EFFICACEMENT, SI L'UTILISATION D'UNE CAMÉRA WEB LUI POSE PROBLÈME, OU SI VOUS, EN TANT QU'INTERVIEWEUR, AVEZ DES DOUTES QUANT À SA CAPACITÉ DE PARTICIPER EFFICACEMENT AUX DISCUSSIONS, VEUILLEZ ÉVALUER SI DES ADAPTATIONS PEUVENT ÊTRE FAITES.
La prochaine question est de nature créative - amusez-vous en formulant votre réponse!
17. Si vous pouviez inviter une personne du présent ou du passé à dîner, qui serait-ce et pourquoi?
NOTE : LES RÉPONDANTS INVITÉS À PARTICIPER DOIVENT S'EXPRIMER CLAIREMENT ET AVEC AISANCE. ILS DOIVENT POUVOIR FORMULER DES PENSÉES COHÉRENTES, EN FAISANT DES PHRASES COMPLÈTES, ET RÉPONDRE ASSEZ RAPIDEMENT. VEILLER NOTAMMENT À CE QUI SUIT :
En cas de doute, SVP NE PAS RECRUTER!
18. La discussion sera enregistrée, strictement aux fins de la recherche. Est-ce que vous consentez à ce qu'on vous enregistre?
19. Le rapport qui sera préparé à partir des discussions pourrait contenir des citations anonymes provenant des participants. Ces citations ne vous nommeront pas, mais elles pourraient contenir des commentaires que vous avez faits durant la discussion. Est-ce que vous consentez à être cité(e) de façon anonyme dans le rapport qui sera préparé à la suite des discussions?
INVITATION À UN GROUPE DE DISCUSSION :
J'aimerais vous inviter à un groupe de discussion. En remerciement de votre temps, vous recevrez un montant de 100 $. La discussion durera environ 90 minutes et aura lieu :
DONNER LA DATE ET L'HEURE EN FONCTION DU NO DE GROUPE INDIQUÉ DANS LE TABLEAU DE LA PAGE 1.
Nous vous rappellerons la veille pour confirmer le rendez-vous et les renseignements. Puis-je avoir votre nom complet, le numéro de téléphone où vous êtes le plus facile à joindre et votre adresse électronique, pour vous envoyer tous les détails concernant le groupe de discussion?
Nom :
Numéro de téléphone :
Adresse courriel :
Vous recevrez un courrier électronique du [insérer le nom du recruteur] expliquant comment rejoindre le groupe en ligne. Si la connexion au système vous pose des difficultés, veuillez en aviser notre équipe de soutien technique à : support@thestrategiccounsel.com .
Nous vous prions de vous mettre en ligne au moins 15 minutes avant l'heure prévue, afin d'avoir le temps de vous installer et d'obtenir l'aide de notre équipe de soutien en cas de problèmes techniques. Veuillez également redémarrer votre ordinateur avant de vous joindre au groupe.
Vous pourriez devoir lire des documents au cours de la discussion. Si vous utilisez des lunettes, assurez-vous de les avoir à portée de main durant la rencontre. Vous aurez également besoin d'un stylo et de papier pour prendre des notes.
Ce rendez-vous est un engagement ferme. Si vous pensez ne pas pouvoir participer pour des raisons personnelles ou professionnelles, veuillez m'en aviser dès maintenant et nous conserverons votre nom pour une étude ultérieure. Enfin, si jamais vous n'êtes pas en mesure de participer, veuillez nous prévenir le plus rapidement possible au [1-800-xxx-xxxx] pour que nous puissions trouver quelqu'un pour vous remplacer.
Merci de votre temps.
RECRUTEMENT FAIT PAR : ____________________
DATE DU RECRUTEMENT : __________________
INTRODUCTION (5 MINUTES)
PERSPECTIVES AND OUTLOOK ON AGING (20 MINUTES)
VIEWS ON HEALTHY AGING (45 MINUTES)
Before we continue, let me share some information with you about healthy aging. [NOTE TO MODERATOR: SHARE DEFINITION OF HEALTHY AGING ON SCREEN]
The World Health Organization (WHO) defines healthy aging as "the process of developing and maintaining the functional ability that enables wellbeing in older age." Functional ability is about having the capabilities that enable all people to be and do what they have reason to value. This includes a person's ability to:
COMMUNICATIONS AND OUTREACH (15 MINUTES)
WRAP-UP (5 MINUTES)
POLLING EXERCISE #1:What factors or features are most important to making a community age-friendly? From the list shown, select the top 5. You can select up to 5, but no more than 5. You can also select 'other' if there is another factor or feature not shown on the list.
POLLING EXERCISE #2: What is the best way to refer to you? ONE RESPONSE ONLY.
INTRODUCTION (5 MINUTES)
PERSPECTIVES SUR LE VIEILLISSEMENT (20 MINUTES)
POINTS DE VUE SUR LE VIEILLISSEMENT EN SANTÉ (45 MINUTES)
L'Organisation mondiale de la Santé (OMS) définit le vieillissement en santé comme étant le « processus de développement et de maintien des aptitudes fonctionnelles qui favorise le bien-être pendant la vieillesse ». Les aptitudes fonctionnelles sont les capacités qui permettent à chacun de se réaliser et d'accomplir ce qui lui tient à cœur. Cela comprend sa capacité :
COMMUNICATIONS ET SENSIBILISATION (15 MINUTES)
CONCLUSION (5 MINUTES)
SONDAGE N O 1 :Quels facteurs ou caractéristiques sont les plus importants pour créer une collectivité favorable aux personnes âgées? Choisissez les cinq principaux facteurs dans la liste suivante. Vous pouvez en sélectionner jusqu'à cinq, mais pas plus . Vous pouvez aussi choisir la réponse « Autre facteur » si vous pensez à un facteur ou une caractéristique qui n'est pas sur la liste.
SONDAGE NO2 : Quel est le terme qui convient le mieux pour parler de vous? UNE SEULE RÉPONSE.
[1] Healthy ageing and functional ability, World Health Organization, Oct. 26, 2020 (https://www.who.int/news-room/questions-and-answers/item/healthy-ageing-and-functional-ability).