2014-705 Joint Health Canada/Public Works and Government Services Canada audit of nursing services contracts in Northern Manitoba (Final report)

September 18, 2014
On this page
Executive summary
- Health Canada (HC) is responsible for the delivery of primary care nursing services in remote First Nations and Inuit Communities. In Manitoba, the care is delivered to approximately 45,000 First Nations reserve residents in 21 nursing stations and two federal hospitals. As most reserve communities are too small and remote to support a physician, the Health Canada (HC) primary care model relies heavily on registered nurses based in nursing stations. A key component of primary care is the provision of 24/7 urgent care. As such, contract relief nurses are often required to fill vacant positions and to replace nurses who are temporarily absent. Since 2003, Public Works and Government Services Canada (PWGSC) has been involved in the contracting for relief nursing services with HC. Between 2003 and 2012, Standing Offer Agreements (SOA) were used for nursing services. Since 2012, these services have been procured through Task Authorization Contracts (TAC) to allow for better protection of confidential business information.
- The objective of the audit was to assess the award and administration of contracts for nursing services in Northern Manitoba for compliance with Government of Canada contracting policies and regulations. The audit scope included nursing services contracts that were awarded in Northern Manitoba from November 1, 2012 to July 2014. The audit was conducted in accordance with the Internal Auditing Standards for the Government of Canada and the International Standards for the Professional Practice of Internal Audit. Sufficient and appropriate procedures were performed and evidence gathered to support the accuracy of the audit conclusion.
- Since 2012, HC and PWGSC have been partnering to produce a national nursing procurement strategy and national procurement vehicle, to ensure that skilled contract relief nurses are readily available to provide a range of nursing services in Northern remote and isolated communities, while providing the best value for money solution. The procurement strategy has been evolving and several areas have been strengthened since the transition from the SOAs to TACs. The national procurement vehicle is now being implemented and has been designed to better support the essential and ongoing nature of the business requirements, and to help ensure that the administration of the contracts is in compliance with the Government of Canada contracting policies and regulations.
- The audit examined Wave 1 TACs issued by PWGSC on behalf of HC from November 1, 2012 to October 31, 2013, Wave 2 TACs covering the period from November 1, 2013 to October 31, 2014, and Wave 3 TACs (national procurement vehicle) issued in June and July 2014. It also examined a sole source contract issued by HC under its own delegated authority for the period from April 2 to June 30, 2013. The amount expended between November 1, 2012 and July 17, 2014 for nursing services in Manitoba in Waves 1 and 2 and under the sole source contract was $18,901,228.
- The audit determined that there was no option to extend the Wave 1 contracts past their expiry on October 31, 2013. It also found that task authorizations (TA) issued under the Wave 1 TACs before October 31, 2013 expired with the Wave 1 TACs on October 31, 2013. Finally, it found that the Wave 2 contracts did not overlap with the Wave 1 contracts. Because program activities require that nurses be scheduled up to two months in advance, this resulted in HC issuing TAs outside of the Wave 1 contracts. The audit also found that TA monitoring weaknesses by HC during Wave 1 resulted in contract limits being exceeded on one of the TACs and on the sole source contract issued by HC. To allow for payment of the invoices, HC was required to issue confirming orders in the amount of $1,707,533 that covered a period of approximately three months beyond the expiry of the Wave 1 TACs (November 2013 to January 2014).
- A number of factors contributed to these errors. It began with misunderstanding and miscommunication by HC and PWGSC at the planning stage. It was compounded by weaknesses in oversight by both departments, as well as weaknesses in HC's information for oversight, contract administration and TA monitoring, within a context of an obligation to ensure continuity of essential health services. As a result, planning, oversight, information for reporting, contract administration and TA monitoring have all improved for the Wave 2 TACs that were issued, as well as for the Wave 3 multi-year national nursing TACs that were awarded effective June and July 2014.
- Audit testing found some compliance issues related to billing under the Wave 1 and Wave 2 TACs. They include TAs not being properly authorized by HC, as well as billing errors that were not caught in the HC verification process. There is, however, evidence that invoices continue to be challenged by HC and corrections made. Wave 3 will be centrally managed by HC at headquarters, and covers Manitoba, Ontario and Quebec. Wave 3 will include additional monitoring and control features.
- The audit makes three recommendations that will help strengthen the management of the TACs and ensure accurate billing on the part of suppliers. HC and PWGSC agree with the recommendations and have provided an action plan describing measures to be taken to strengthen the administration of contracts for nursing services in Northern Manitoba.
Introduction
Background
- Health Canada (HC) is responsible for the delivery of primary care nursing services in remote First Nations and Inuit communities. In Manitoba, the care is delivered to approximately 45,000 First Nations reserve residents in 21 nursing stations and two federal hospitals. As most reserve communities are too small and remote to support a physician, the HC primary care model relies heavily on registered nurses based in nursing stations. A key component of primary care is the provision of 24/7 urgent care. As such, contract relief nurses are often required to fill vacant positions and to replace nurses who are temporarily absent.
- Certain regions of the country rely more than others on HC nurses for the delivery of primary care nursing services. Due to difficulties in recruiting nurses for communities in remote and isolated areas that often have no road access, the region of Manitoba is highly dependent on agency nurses.
- Primary care nursing services are the first point of contact in the First Nations and Inuit health system delivered by HC. The nursing station model of service delivery is currently based on registered nurses (herein, referred to as nurses) offering an initial assessment or triage of clients' health needs. Nurses assess the health situation to determine if the need for care is urgent or non-urgent and identify the necessary actions to take. Critical, emergent and urgent care involves the immediate treatment where there is an immediate threat to life or function, acute trauma or illness. This is done in consultation with a physician and is supported by the First Nations and Inuit Health clinical practice guidelines. It may also require securing and coordinating medical transportation to provincial health services if the care requires a more advanced treatment team.
- HC has historically had difficulty recruiting and retaining nurses in Northern Manitoba, where nurses often have a sense of professional isolation, given the small size of the health care team in the community, and where community dynamics and tensions can also place a significant strain on nurses who remain in one community. While continued efforts are devoted by HC to recruitment activities to fill the 107 full-time nursing positions in Manitoba, as of 2013-14, there continues to be a significant ongoing vacancy rate of approximately 37 percent. Contract relief nurses are thereby required to fill vacant positions and to replace nurses who are temporarily absent.
- Since 2013, Public Works and Government Services Canada (PWGSC), as the contracting authority, has been involved in the contracting for relief nursing services for HC, as the project authority, using competitive Standing Offer Agreements (SOA) to acquire these services. However in 2012, PWGSC informed HC that (Footnote *), Task Authorization Contracts (TAC) were better suited for this type of requirement and this industry. A contract with Task Authorizations (TA) is a method of supply for services under which all of the work or a portion of the work will be performed on an "as and when requested basis" through predetermined conditions, including an administrative process involving the issuance of TAs. Contracts with TAs are used in service contracting situations when there is a defined need by a client to rapidly have access to one or more categories of service(s) that are expected to be needed on a repetitive basis during the period of the contract.
- In September 2012, a national nursing services procurement working group was created to engage the regions in the development of a national procurement vehicle. It was initially anticipated that the national procurement vehicle would be in place by May 2013. This was later updated to May 2014. In the interim, PWGSC and First Nations and Inuit Health Branch (FNIHB), Manitoba Region, put in place two waves of TACs (Waves 1 and 2). During the period covered by Wave 1, the delay in award (Footnote *).
- (Footnote *).
- The total expenditures on nursing services under the Wave 1 and 2 contracts and the sole source contract were $18,901,228.
- Since then, a national procurement vehicle for nursing services in Manitoba, Ontario and Quebec has been put in place and is referred to as Wave 3 in this report. The TACs awarded under Wave 3 are three-year contracts with five option years that were effective July 24, 2014. The value of these contracts is $120,145,656.
- A mapping of the timing of contracts is included in Table 1. A summary of supplier, contract value and type and actual expenditures is included in Appendix C.
Table 1: Summary of the three waves of nursing services contracts
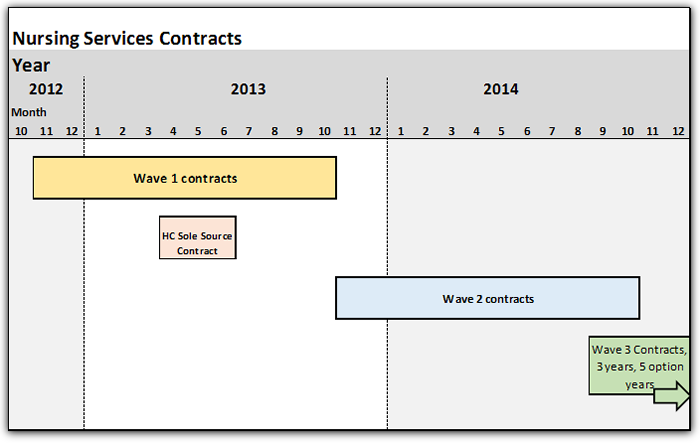
Image description
This image presents a graph that illustrates the timeframe of contracts awarded by PWGSC for the three waves (from 2012 to 2014) and the timeframe of the sole source contract awarded by Health Canada. This table presents a 3 year timeframe and presents the duration of Wave 1 contracts (from November 2012 to October 2013); the Health Canada Sole Source Contract (from April to June 2013); the Wave 2 contracts (from November 2013 to October 2014); and the Wave 3 contracts (3 year contracts with 5 option years) (starting on July 2014).
Audit objective
- The objective of the audit is to assess the award and administration of contracts for nursing services in Northern Manitoba for compliance with Government of Canada contracting policies and regulations. Details on the audit criteria can be found in Appendix A. Conclusions against each individual criterion can be found in Appendix B.
Audit scope
- The scope of the audit included all nursing services contracts in the Manitoba Region that were awarded from November 1, 2012 to present (i.e. July 2014); and covered governance, risk management and the controls related to the procurement process from tendering to award, and contract administration including TA monitoring and basis of payments. This includes the TACs issued by PWGSC on behalf of HC in November 1, 2012 (Wave 1); November 1, 2013 (Wave 2); July 24, 2104 (Wave 3); and the sole source contract issued by HC on April 2, 2013.
- As use of the Wave 3 contracts had not commenced at the time of the audit, the audit did not examine the following for Wave 3: information for reporting and decision making; contract management; TA monitoring; and basis of payments (referred to as criterion 1.4, 3.5, 3.6 and 3.7 respectively in Appendix A).
Audit approach
- The audit criteria outlined in Appendix A were developed using the Office of the Comptroller General of Canada's Audit Criteria Related to the Management Accountability Framework: a tool for Internal Auditors, the Government of Canada policies and regulations for contract award and administration, the Treasury Board (TB) framework for the management of risk, the PWGSC Integrated Risk Management Policy and the PWGSC acquisition program risk assessment framework.
- The audit examined the governance, risk management and controls related to the procurement process from tendering to award, as well as contract administration, including TA monitoring and basis of payments. The audit approach included a review of documentation, policies, standards, guidelines, frameworks, business processes and nursing service contracts, as well as interviews and observations, inquiry, testing and analysis. Interviews were conducted in the National Capital Region and in the Winnipeg region with employees of both HC and PWGSC.
Statement of conformance
- In the professional judgment of the Chief Audit Executives of HC and PWGSC, sufficient and appropriate procedures were performed and evidence gathered to support the accuracy of the audit conclusion. The audit findings and conclusion are based on a comparison of the conditions that existed as of the date of the audit, against established criteria that were agreed upon with management. Further, the evidence was gathered in accordance with the Internal Auditing Standards for the Government of Canada and the International Standards for the Professional Practice of Internal Auditing. The audit conforms to the Internal Auditing Standards for the Government of Canada, as supported by the results of the quality assurance and improvement programs of both HC and PWGSC.
Findings, recommendations and management responses
1. Governance
Audit criterion: Procurement and contracting needs/requirements are identified in a coordinated and timely manner.
- It is important that the project authority identify and plan procurement needs in a timely manner, and allow sufficient time for the procurement process. It is also important that the contracting authority work with the project authority to help ensure that the requirements can be met in a way that achieves best value for Canadians. Appropriate planning ensures that proper resources are available to deliver the program mandate as per the project authority's stated requirements.
- The nursing services required by Health Canada (HC) are ongoing and generally planned one to two months in advance and two or three months ahead of time during critical periods such as the summer months, Christmas and New Year's. These business planning requirements make it important to appropriately manage the transition from one contracting vehicle to the other, at the end of the contract.
- In March 2012, following Public Works and Government Services Canada's (PWGSC) advice that it was no longer appropriate to use Standing Offer Agreements (SOA) (Footnote *), HC submitted to PWGSC a requisition for the issuance of Task Authorization Contracts (TAC) to meet its nursing services requirements that were estimated at $18M annually. In finalizing the procurement strategy, it was determined that one-year TACs would be issued since there was not enough time to put in place TACs with option years, as this would bring the total value of the contracts over $20M (Footnote *). Further, it was anticipated that a national procurement vehicle would be in place by May 2013, replacing Manitoba-specific contracts. Both parties also agreed that one-year TACs would provide a test period that would allow for the identification of modifications/changes to be incorporated into the national procurement vehicle.
- These new TACs moved HC from a SOA model to a TAC model. A key difference between these two models is that the services being procured through a TA issued under a TAC must be completed on or before the expiry date of the TAC, while call-ups issued for services against the SOA before expiry remain valid after the expiry of the SOA.
- On November 1, 2012, PWGSC Manitoba Region issued two one-year TACs covering the period from November 1, 2012 to October 31, 2013 (Wave 1). A third contract, with a company owned by a former public servant, was awarded on June 5, 2013, (Footnote *). The delay in issuing the third contract required HC to issue its own contract to a fourth bidder for the period from April 2, 2013 to June 30, 2013.
- In February 2013, in anticipation of a delay in award of the national procurement vehicle to May 2014, it was determined that it would be prudent to put in place six-month TACs effective from November 1, 2013 to April 30, 2014, with a six-month option period to be invoked at the convenience of HC for the period from May 1, 2014 to October 31, 2014 (Wave 2). Three TACs were issued on November 1, 2013, the day after the Wave 1 contracts expired, and a fourth was issued on February 19, 2014 to a company owned by a former public servant, (Footnote *).
- The effectiveness of the planning for the transition from the Wave 1 contracts to the Wave 2 contracts was hampered by miscommunication and misunderstanding by both departments, particularly in relation to the management of TAs at contract expiry in the context of HC's business planning requirements. Because there was no option to extend the Wave 1 contracts, because TAs issued under the Wave 1 contract expired with the Wave 1 contract, and because the Wave 2 contracts did not overlap with the Wave 1 contracts, HC was unable to complete advance contracting for nursing relief services. To ensure continuity of service, HC issued TAs outside of the authority of the Wave 1 contracts.
- The audit found that Wave 3 contracts were well planned. Three contracts were issued between June 19 and July 24, 2014, well before the expiry of the Wave 2 contracts. In addition, the Wave 3 contracts are three-year contracts that include five one-year renewal options allowing for increased flexibility, in addition to a moving six-month transition period that can be invoked at any of the interim contract end-dates.
- In conclusion, the transition between Waves 1 and 2 might have gone more smoothly with better communication and understanding during the planning phase by both departments. The Wave 3 process was found to be well planned.
Audit criterion: Adequate oversight exists over the procurement process and contract administration.
- It is important that the project authority and contracting authority discharge their respective responsibilities to oversee contracts for the whole life-cycle, to ensure compliance with legislated requirements and proper support for delivery of the business requirements, in accordance with the terms and conditions of the contract.
- PWGSC provides oversight over the procurement process, as the contracting authority responsible for this process. It also provides departments and agencies with expert procurement advice related to contract administration. As the project authority, HC is primarily responsible for setting the procurement requirements and for ensuring oversight over the administration of the contract.
- PWGSC provided adequate oversight over the procurement process for all three waves of TACs. In its capacity as contracting authority and advisor on contract administration, PWGSC provided HC with the Guide to Preparing and Administering Task Authorizations. The guide provides procedural guidance and advice on preparing and administering TAs. As well, oversight responsibilities for both departments for contract administration were documented in a Record of Agreement (see section 1.3). The purpose of the Record of Agreement (the Agreement) is to formalize the responsibilities of PWGSC and HC regarding their respective roles and responsibilities when using TACs. The Agreement emphasizes that HC and PWGSC work closely together at all times during the period of the contracts.
- For Wave 1, HC oversight over contract administration was provided by the First Nations and Inuit Health Branch (FNIHB) in Winnipeg, which reviewed monthly variance financial reports. These reviews focused on commitments and expenditures recorded in the financial system. This level of oversight did not provide assurance that the contract limits would not be exceeded or that work allocation was effectively managed.
- PWGSC provided contract administration oversight in Wave 1 by maintaining an expenditure tracking spreadsheet, based on invoices sent directly to PWGSC from the supplier, as required by the contract. PWGSC informed us that this information was provided late, making it difficult to track actual expenditures in a timely manner and to effectively monitor contract dollar value limits. HC provided usage reports (that is, total cost of invoice processed), upon request by PWGSC.
- The information provided to and monitored by FNIHB and PWGSC was insufficient (see section 1.4) to allow either department to fulfill its oversight responsibilities, in accordance with the Agreement. As a consequence, those providing oversight were not able to monitor and ensure that contract authorities were not exceeded.
- For Wave 2, oversight over the administration of the TACs was enhanced. Both departments provided oversight based on the expectations in the Agreement. Sufficient information was being provided (see section 1.4) by HC's program delivery unit, such that HC and PWGSC could oversee each contract to ensure that cost and workload allocations were within contracting limits. Both departments also oversaw contract end-dates and contract usage percentages. Finally, both departments held teleconferences weekly to discuss and review all the information related to the above oversight activities. There were also monthly meetings between PWGSC and the suppliers.
- For Wave 3, oversight has been further strengthened by incorporating improved monitoring and control measures into the contract terms and conditions, to ensure that the total aggregate value submitted does not exceed the limitation of expenditures. This included a requirement from the contractor to provide a utilization report to the contracting authority on a quarterly basis. These expectations should further enhance the overall contract management.
- In conclusion, oversight over the procurement process by PWGSC was adequate for all three waves of TACs. Oversight in Wave 1 over the use of TACs and administration of TAs was not carried out in accordance with the Agreement by both departments because insufficient information was provided. Both oversight and sufficiency of information improved significantly in Wave 2 as a result of improved collaboration and monitoring. Wave 3 includes improved control measures that have been incorporated into the contract terms and conditions.
Audit criterion: Roles and responsibilities of the contracting authority and the project authority are clearly described.
- It is important to have roles and responsibilities that are clearly described and understood by the contracting authority and the project authority during all phases of the contract life-cycle, to properly support contract management activities.
- As noted, the Agreement between the two departments pertaining to the use of TAs for all three waves of contracts formalized the respective roles and responsibilities of each department. The document described the departments' respective roles and responsibilities relating to the management of the contract and the use of TAs, such as TA limit and approval authority, including verification of sufficient funds in the contract; the TA process, including expiry dates; the contract amendment process; contract administration; and reporting requirements.
- In conclusion, the roles and responsibilities of PWGSC as contracting authority and of HC as project authority were clearly described.
Audit criterion: Procurement and contracting information used for reporting and decision-making is accurate and complete.
- Appropriate information should be available to support contract management through the life-cycle of the contract. To support procurement award, the contracting authority should provide decision-makers within PWGSC and HC with complete, accurate and timely information to ensure timely contract award that complies with TB contracting regulations. To support contract administration, the project authority should provide decision-makers within HC and PWGSC with complete, accurate and timely actual and forecasted expenditures under the contracts, compared to the contract limits and each vendor's allocated percentage of total spending. This information is needed to properly manage the offering of future nursing assignments within the terms, conditions and limits of the contracts.
- The information provided by PWGSC to decision-makers to support contract award was sufficient. There are formal reporting procedures in place in PWGSC, where information is provided to decision-makers prior to contract award. For Waves 1 and 2, this included regular meetings and a workload management system that ensured accurate and timely information related to the award processes. For Wave 3, the procurement process was integrated within the departmental and branch governance reporting, review and approval structure. Also, before any approval process, the client department is consulted about the content of the approval documents and the implication of final decisions.
- In addition, the audit found, in the procurement phases of all three waves of contracts, evidence of emails and telephone conversations with PWGSC management as well as between PWGSC and Health Canada. In both Waves 1 and 2, it was also noted that there was increased communication once one of the successful bidders was identified as a former public servant in receipt of a pension (Footnote *).
- As discussed in section 1.2, information provided by HC during Wave 1 to those providing oversight in HC and PWGSC was insufficient to allow for effective oversight over contract administration.
- For Wave 2, the FNIHB Manitoba Region Nursing Directorate maintained a TA tracking spreadsheet and provided it on a weekly basis to HC and PWGSC management responsible for providing oversight. The TA spreadsheet provided the following details, by supplier, for each TA: basic qualitative information (such as start and end-dates, nursing station, TA number, etc.); and actual and forecast expenditures. The spreadsheet also provided summary information, by supplier, namely: contract value, estimated usage ($ and %) and accepted and refused assignments offered to each supplier. The forecast expenditures comprised an average cost estimate based on the history of actual costs. The FNIHB Manitoba Region Nursing Directorate also provided a copy of approved and signed TAs to PWGSC. The audit team was informed by HC and PWGSC that other key information was discussed at the weekly teleconference such as issues with suppliers, staffing trends, etc.
- The audit team was also informed that HC's financial management system (Software Application Program (SAP)) is being configured to provide a better and more comprehensive approach of monitoring actual and forecasted expenditures.
- In conclusion, contracting information provided by HC in support of decision-making improved from Wave 1 to Wave 2. Additional system enhancements are planned to track all individual TAs to be issued under Wave 3. However, the audit could not examine contracting information for Wave 3, as use of these contracts had not commenced at the time of the audit.
2. Risk management
Audit criterion: A procurement risk assessment is performed in accordance with relevant policies and procedures.
- Contract risk management covers the risk assessment conducted by the contracting authority during the contract tendering and award phase.
- The PWGSC Procurement Risk Assessment Tool, related to contract tendering and award, is designed to support the proper procurement, in accordance with contracting policies and regulations.
- PWGSC performed a procurement risk assessment for Waves 1, 2 and 3. Copies of the assessments are on file and supported the development of the procurement strategy.
- As indicated earlier in the report, HC had to issue its own contract to a qualified bidder under Wave 1 (see section 1.1). The sole source method of supply was considered the proper interim arrangement to meet HC's requirements for the provision of health services to First Nations and Inuit communities.
3. Internal control
Audit criterion: The contract tendering process complies with contracting policies and regulations.
- In contract tendering, the contracting authority takes the business requirements established by the project authority, selects the proper contracting vehicles, designs the Request for Proposal and issues the request for services. For Waves 1 and 2, contract tendering was managed by PWGSC in Winnipeg. For Wave 3, it was managed by PWGSC Headquarters, given the national nature of the procurement strategy. HC assumed the role of contracting authority for the sole source contract.
- In February 2012, (Footnote *), PWGSC determined that the appropriate contracting vehicle for nursing services was TACs. The Wave 1 Request for Proposal was designed accordingly. Both PWGSC and HC participated in the development of the Request for Proposal. The contract tendering process provided adequate timelines for industry to respond, as well as appropriate communications such as a bidder's conference with all answers shared with industry. The documentation is on file.
- A similar process was followed by PWGSC for Wave 2 TACs. It also met the required standards and policy requirements for contract tendering.
- For Wave 3, the process followed by PWGSC involved an industry engagement session followed by ten individual meetings with interested suppliers. This was followed with two Requests for Information prior to the release of the Request for Proposal.
- HC issued the sole source contract under its own special delegated contracting authority for the provision of health services to First Nations and Inuit communities. There was justification on file for the sole source method of supply.
- Overall, PWGSC conducted the contract tendering process in accordance with contracting policies and regulations for the three waves of TACs, and HC issued the sole source contract in accordance with its own delegated authority.
Audit criterion: The method of bidder selection is consistent with the method outlined in the solicitation.
- Contracts should be fairly and accurately awarded by the contracting authority in a timely fashion, based on the results of the tendering process.
- The contract award process followed by PWGSC for the TACs awarded under Waves 1, 2 and 3 was consistent with the method outlined in the solicitation documents. Files included the signed bid evaluation documents and executed contracts awarded in accordance with the Request for Proposal and proposals received. Successful bidders met all the requirements set out in the Request for Proposal for Waves 1, 2 and 3. In each of Waves 1 and 2, one of the successful bidders was owned by a former public servant in receipt of a pension. (Footnote *).
- The sole source contract awarded by HC was issued in a timely manner to a qualified bidder under Wave 1. The contract awarded by HC did not incorporate the rates that were provided by the supplier in its Wave 1 proposal and HC was not successful in its attempt to have the supplier honour those rates, which resulted in fewer hours of service received from this supplier
- In conclusion, PWGSC followed the method of bidder selection outlined in the solicitation documents (Footnote *). HC awarded a sole source contract in accordance with its own delegated authority.
Audit criterion: The required certifications are provided by the supplier to the contracting authority to prepare the contract (for example, code of conduct, employment equity, Procurement Strategy for Aboriginal Business (PSAB), Canadian content and the availability of resources and their education and experience), by the project authority to the contracting authority (Footnote *).
- As part of preparing the contract (Footnote *), the suppliers and project authority must provide the contracting authority with required certifications. Certifications were required regarding the code of conduct, employment equity, Procurement Strategy for Aboriginal Business (PSAB), Canadian content, the availability of resources and nursing education and experience requirements. The project authority also needed to provide certifications regarding the available budget, and the contracting authority had to provide certification regarding gender impacts and strategic environmental assessment.
- HC provided certification that the contracts were within the available budget. The employer-employee relationship was not at risk, as HC has established measures to ensure that no employer-employee relationship is established under the new contracts.
- (Footnote *).
- Suppliers provided information about nurses (education and experience) and the following certifications: code of conduct, employment equity, PSAB and Canadian content. By signing the front page of the Request for Proposal, bidders certified that they are in compliance with the provisions of the code of conduct and that they are not named on the Federal Contractor's Program (FCP) for employment equity "FCP Limited Eligibility to Bid" list. Moreover, Canadian content certification was required prior to contract award and PSAB certification was required with their proposal.
- In conclusion, the suppliers, the project authority and contracting authority provided all the required certifications.
Audit criterion: Proper consideration is given to matters such as intellectual property, procurement set-aside, land claims agreements, security requirements and contractor liability.
- The preparation of the procurement vehicle should include proper consideration by the contracting authority and project authority of various other aspects, in order to properly address several other requirements of the Crown.
- For Wave 1, two of three suppliers were joint ventures and for Wave 2, three of four suppliers were joint ventures. All suppliers in both waves were eligible for the procurement set-aside under the Federal PSAB. The nursing services contracts used the set-aside under PSAB. In Wave 3, priority was given in the Request for Proposal to aboriginal businesses. Two of the three successful bidders for Wave 3 qualified under the PSAB.
- It was also determined that intellectual property and comprehensive land claims agreements were not applicable for this requirement. The contracts were considered low-risk under the TB Policy on Decision Making in Limiting Contractor Liability in Crown Procurement Contracts. As such, the standard liability clause was used.
- Security clearances for nursing personnel and the suppliers themselves are key requirements of this procurement. The audit observed that nurses and suppliers providing services under these contracts have been granted the necessary security clearances. PWGSC also maintains a roster of qualified nurses and ensures that the security clearances for the nurses as well as other required certifications and training requirements have been met.
- In conclusion, proper consideration was given by HC and PWGSC to other procurement aspects for the nursing service contracts.
Audit criterion: Contract administration discipline is implemented to ensure sound administration of the contracts.
- A solid contract management framework helps the project authority to ensure that the use of contracts complies with their terms and conditions and properly supports business requirements.
- The FNIHB Manitoba Region Nursing Directorate was primarily responsible for managing Wave 1 and 2 contracts, determining the business requirements, issuing TAs, paying invoices and ensuring proper control and reporting of expenditures. Wave 3 contracts will be centrally managed by the Nurse Relief Coordination Unit (NRCU) in FNIHB in Ottawa, in collaboration with the FNIHB Manitoba Region.
- For Wave 1 and 2 contracts, the nurse placement coordinator, in consultation with the nurse managers, provided the suppliers with a description of their relief nursing requirements. The suppliers identified proposed resources and submitted their TAs to HC. TAs included information required in the TACs. For Wave 1, the nurse managers subsequently approved the TAs once they verified that the proposed resources were listed in the nursing roster. The roster certifies the validity of nurses' credentials. PWGSC maintains the roster, based on suppliers' submissions, and forwards it to HC on a weekly basis. The approval process of TAs was strengthened in Wave 2 with the sign-off by the FNIHB Regional Director, HC. The TA form now includes a deadline for the submission of invoices. Moreover, PWGSC approval on individual TAs is required once the contract reaches 70% of the contract value.
- For Wave 1 and 2 contracts, the nurse placement coordinator also kept a log of TAs issued in a scheduling system. The audit noted the following: (i) some of the TAs issued by HC in Wave 1 were signed after the work had begun; (ii) some TAs were issued before expiry of the Wave 1 contracts for services to be provided after the expiry date of the contracts; (iii) TAs were issued for one of the Wave 1 contracts and the sole source contract in excess of the contract limit. At the time of the audit, HC was preparing the necessary confirming orders in the amount of $1,707,533 to facilitate payment to the suppliers for the work outside of the terms and conditions of the TACs and the sole source contract.
- As indicated earlier in the report, in Wave 1, PWGSC maintained an expenditure tracking spreadsheet that was based on invoices received from suppliers, and HC maintained records of expenses for monthly variance reporting and forecasting. In Wave 2, the FNIHB Manitoba Region Nursing Directorate and PWGSC maintained and reconciled their expenditure tracking spreadsheets from approved TAs and invoices to ensure that cost and allocation of work were within the contracting limits, monitored contract end-dates and contract usage percentages. PWGSC and FNIHB management discussed the reconciled tracking spreadsheet that was updated weekly for decision-making and oversight purposes. HC also provided a copy of the approved TAs and invoices to PWGSC. Furthermore, PWGSC met monthly with each supplier to discuss invoicing and other issues.
- Controls related to purchase authorization and payments in accordance with contract terms and conditions are addressed in section 3.7.
- In conclusion, contract administration issues by HC were identified for Wave 1 and with the sole source contract. HC's contract administration discipline increased during Wave 2 and helped ensure sound administration of the contracts.
Audit criterion: Task authorizations are monitored in order to track expenditures and percentage of allocation.
- Issuance and monitoring of TAs are key components of the control framework applicable to these contracts. Suppliers are not to send nurses or incur non-refundable costs until they have received a TA signed by the project authority. Monitoring by the project authority is required to ensure that it does not sign TAs when it is estimated that services or total expenditures for a given supplier would exceed the contract dollar value limit or expiry date.
- The audit did not find evidence that HC tracked expenditures and percentage of supplier allocation for the TAs issued under Wave 1 TACs. Further, as a result of insufficient monitoring, contract expenditure limits were exceeded (see section 3.5).
- As a result of the issues identified in Wave 1, TAs were tracked and monitored in Wave 2 by HC program staff using a TA tracking tool. Because of this tracking and monitoring, contract minimums were met and maximums were not exceeded.
- The audit concluded that TAs were not well-monitored in Wave 1 by HC. For Wave 2, the TAs were better monitored to help ensure that expenditure limits and percentages of allocation were respected.
Audit criterion: Payments are made only for services received, in accordance with contract terms and conditions and in the appropriate period. All purchases are appropriately authorized.
- The project authority needs a full set of functioning processes and controls to ensure that payments are made for appropriately authorized services received and are in accordance with the terms and conditions of the contract. The audit conducted detailed testing on a sample of 50 invoices paid or payable under TACs, to ensure that controls were in place and functioning effectively. The sample was selected judgmentally, considering the number of invoices and dollar value of the invoices for each supplier and contract. The testing included:
- pre-authorization and approval;
- compliance with contract condition;
- nurse certification; and
- mathematical accuracy.
Table summary
This table presents statistics on the contract waves 1 and 2 and sole source contract in terms of the number and values of invoices from the sample and the percentage of contract tested.
Table 2: Contract invoices population and audit sample Contract wave Number of invoices Value of invoices Population Sample % Tested Population Sample % Tested Wave 1731 25 3.4% $11,322,660 $292,636 2.6% Wave 1 CO124 8 6.5% $1,603,824 $115,803 7.2% Sole Source35 3 8.6% $452,176 $29,634 6.6% Wave 2Footnote **307 14 4.6% $3,508,590 $155,705 4.4% Total1,197 50 4.2% $16,887,250 $593,778 3.5% - Invoices are received from suppliers in electronic format, together with supporting timesheets, travel invoices and the TA form. HC program staff review the invoice and supporting documentation. They communicate with the supplier and challenge the services and rates being invoiced. If issues are identified with the invoice, it is rejected and the supplier is requested to issue a new one. Once this challenge is complete, the electronic file is appended with evidence of the review and it is submitted for payment (via P2P, HC's payment system) and a copy of the invoice and supporting documentation is emailed to PWGSC. The HC Winnipeg office is using P2P and the associated SAP business processes for certification under Sections 34 and 33 of the Financial Administration Act.
- For the majority of invoices verified, proper procedures were followed and there was supporting documentation such as time sheets, on-call sheets and call-backs authorized by the HC nurse in charge and submitted with the invoice. Also, for most invoices sampled, the rates billed for services were in accordance with the supplier's contract. There were no advance payments. Travel charges were billed appropriately in Wave 1. For Wave 2, a simpler flat rate of $150 for travel in each direction was introduced and applied. The audit testing found errors in calculating hours in the contract payments and some signatures on TAs were dated after the task authorization started.
- Both Wave 1 and 2 contracts allow payment for stand-by at a rate of one hour paid for eight hours of stand-by. The nurses are also paid for a minimum of three hours if they are called back to work after their regular shift. The Wave 1 and 2 contracts all explicitly state that stand-by and call-back are not to be billed for the same time period. Contracts also state that on call time is to be billed at regular rates. Of the 50 invoices sampled, 10 contained errors related to billing for these two items, representing an error rate of 20%.
- During our testing we found that in Waves 1 and 2, seven of the seven invoices tested for one supplier billed for both stand-by and call-back for the same time period, resulting in double billing to the Crown. The dollar value of the amount double-billed was roughly $3,900 on the seven invoices tested. The total dollar value of these seven invoices was approximately $100,000, representing an error rate of 3.9%. The time sheets were signed by the nurse in charge. The error, which was in the billing, was not caught during the HC invoice verification process.
- During our testing, we also found that in Wave 2, three of the three invoices tested for one supplier included billing for stand-by at the overtime rate when the contract states that it will be paid at the regular rate of pay. The dollar value of the amount overbilled was approximately $1,300 for the three invoices tested. The total dollar value of these three invoices was approximately $35,000, representing an error rate of 3.7%.
- We further observed compliance errors in Wave 1 where the TAs were not signed before the work began and in one case the TA was never signed. Such errors were not observed in TACs issued under Wave 2.
- It was also noted that a copy of the time sheet is not sent directly from the nurse in charge at the nursing station to HC Winnipeg for comparison purposes. This exposes the Crown to the risk of a time sheet being altered after it has been signed. The draft process for the TACs issued under Wave 3 includes having the nurse in charge submit time sheets directly to headquarters to allow for a comparison to the hours billed by the supplier.
- For TACs issued under Wave 3, greater use of P2P by HC, an end-to-end solution for the electronic approvals of procurement transactions and invoices, is planned and as such, will contribute to reducing invoicing errors.
- In conclusion, most purchases were appropriately authorized by HC; however, some of the payments authorized were not in accordance with contract terms and conditions, which proved to be difficult to administer.
Recommendation 1
It is recommended that the Assistant Deputy Minister, Acquisition Branch of Public Works and Government Services Canada, in collaboration with the Assistant Deputy Minister, Regional Operations, First Nations and Inuit Health Branch of Health Canada, amend the Wave 3 contracts and supporting invoicing templates to reduce the risk of miscalculation of the hours billed.
Management response - Recommendation 1
Management has been proactive in mitigating risks identified from previous waves into the Wave 3 contracts. PWGSC and HC management agree with the recommendation to collaborate in the development and implementation of measures to reduce the risk of miscalculation of hours billed through the following actions:
- 1.1 Develop an invoicing template for use by all companies.
- 1.2 Amend contracts with all suppliers to append the new invoicing template.
Recommendation 2
It is recommended that the Assistant Deputy Minister, Regional Operations, First Nations and Inuit Health Branch of Health Canada, in collaboration with Assistant Deputy Minister, Acquisition Branch of Public Works and Government Services Canada, explore opportunities for more efficient management of task authorizations, to reflect appropriate roles and responsibilities.
Management response - Recommendation 2
Management has been proactive in exploring opportunities for efficient and effective contract management in the Wave 3 contracts. HC and PWGSC management agree with the recommendation to further clarify/define respective roles and responsibilities to help ensure the efficient management of TAs through the following actions:
- 2.1 Use a common TA tracking/monitoring tool.
- 2.2 Implement a Process Guide that outlines the roles and responsibilities of HC and PWGSC as they relate to preparing, tracking and sharing TAs.
- 2.3 In preparation for Wave 3, HC has established processes and procedures to deal with unforeseen requirements for nursing services or the extension of a TA, thereby reducing to the full extent possible the risk of occurrences where nurses are working in the absence of an authorized TA.
Recommendation 3
It is recommended that the Assistant Deputy Minister, Regional Operations, First Nations and Inuit Health Branch of Health Canada, in collaboration with the Chief Financial Officer of Health Canada, review all invoices for the suppliers who consistently overbilled the Crown and collect overpayments made.
Management response - Recommendation 3
Management identified and remedied the potential risk of overbilling associated with the overlap of stand-by and call-back services under the Wave 3 TACs. HC management agrees with the recommendation to review all prior invoices and will address this recommendation through the following actions:
- 3.1 The invoices for Waves 1 and 2 will be systematically reviewed and recalculated to determine the overpayments. A report will be produced outlining overpayments.
- 3.2 Overpayments will be recorded as accounts receivable and will be collected in accordance with the overpayment recovery plan.
Conclusion
- The audit concludes that the award of the contracts by PWGSC was in compliance with government contracting policies and regulations. Some non-compliance was identified in the administration of the contracts by HC in Wave 1, the sole sourced contract and the transition from Wave 1 to Wave 2. Weaknesses in governance by both departments, specifically planning and oversight, contributed to contracting authorities being exceeded for all Wave 1 contracts and the sole source contract. Wave 3 (a national procurement vehicle) has been designed to support more effectively the essential and ongoing nature of the business requirements, and to help ensure that the administration of the contracts is in compliance with the Government of Canada contracting policies and regulations.
- Since 2012, HC and PWGSC have been partnering to produce a national nursing procurement strategy and national procurement vehicle to ensure that skilled contract relief nurses are readily available to provide a range of nursing services in Northern remote and isolated communities while providing the best value for money solution.
- As the national procurement strategy and vehicle were being developed, nursing services were supported by two waves of Task Authorization Contracts (TAC). Wave 1 covered the period from November 1, 2012 to October 31, 2013 and Wave 2 covered the period from November 1, 2013 to October 31, 2014. Wave 3 (national procurement vehicle) is now being implemented. Prior to the issuance of these three waves of TACs, nursing services were provided through Standing Offer Agreements (SOA).
- The tendering and awarding of TACs by PWGSC was done in compliance with contracting policies and regulations; procurement risk assessments were completed; the necessary certifications were provided by suppliers and HC; and there was proper consideration of procurement set-aside, security requirements and contractor liability.
- The transition from SOAs to TACs created unanticipated challenges for PWGSC and HC, which were resolved over the three waves of TACs awarded over the period from November 1, 2012 to July 2014.
- While PWGSC recognized at the onset that HC's requirement for nursing services, estimated at $18M annually, would typically include an option to extend the contract on expiry, there was insufficient time to implement a new procurement tool with option years since that would bring the total value of the requirement over $20M, (Footnote *). Further, it was anticipated that the national procurement vehicle would be in place by May 2013. In addition, the Wave 1 contracts expired October 31, 2013 and the Wave 2 contracts were issued by PWGSC on November 1, 2013, meaning there was no overlap between the contracts. Finally, TAs issued by HC before expiry of the TAC, expired on the same date as the contract.
- Because of delays in implementing the national procurement vehicle, no option to extend the Wave 1 contracts, no overlap between the Wave 1 and 2 contracts and the fact that TAs expired with the expiry of the TAC, HC prepared confirming orders in the amount of $1,707,533 for the TAs issued in September and October 2013 for services required from November 2013 to January 2014.
- As one of the successful bidders on the Wave 1 contracts was owned by a former public servant, (Footnote *). This contract was awarded by PWGSC on June 5, 2013, and prorated to account for the time expired. This required HC to issue its own contract to one of the qualified suppliers under the Wave 1 process. HC issued a sole source contract on the basis of the immediate requirement to provide necessary nursing services to First Nations communities.
- Contract administration also proved to be an important challenge during Wave 1 of TACs as there was a lack of understanding by HC of how to effectively and efficiently administer and control TAs, which resulted in contract limits being exceeded and in a lack of effective control over amounts that were being invoiced. Insufficient information was provided to HC and PWGSC to allow them to fully discharge their responsibilities for oversight over contract administration. For Wave 2 the audit observed much improved controls over TAs, a strong commitment on the part of both departments to work collaboratively, and a desire to perfect the tools that are used to manage and control TAs and related TACs. For Wave 2, we also noted that HC continued to experience challenges in verifying the accuracy of the amounts being invoiced.
- The audit makes three recommendations that will help strengthen the management of the TACs and ensure accurate billing on the part of suppliers. HC and PWGSC management agree with the recommendations and have provided an action plan describing the measures that they will be taking to strengthen the administration of contracts for nursing services in Northern Manitoba.
Appendix A – Specific lines of enquiry and criteria
Table summary
This appendix presents the lines of enquiry and audit criteria.
| Criteria title | Audit criteria |
|---|---|
Line of enquiry 1: Governance |
|
|
Procurement and contracting needs/requirements are identified in a coordinated and timely manner. |
|
Adequate oversight exists over the procurement process and contract administration. |
|
Roles and responsibilities of the contracting authority and the project authority are clearly described. |
|
Procurement and contracting information used for reporting and decision making is accurate and complete. |
Line of enquiry 2: Risk management |
|
|
A procurement risk assessment is performed in accordance with relevant policies and procedures. |
Line of enquiry 3: Internal control |
|
|
The contract tendering process complies with contracting policies and regulations. |
|
The method of bidder selection is consistent with the method outlined in the solicitation. |
|
The required certifications are provided by the supplier to the contract authority to prepare the contract (for example, code of conduct, employment equity, Procurement Strategy for Aboriginal Business (PSAB), Canadian content and the availability of resources, and their education and experience) by the project authority to the contracting authority (Footnote *) |
|
Proper consideration is given to matters such as intellectual property, procurement set-aside, land claims agreements, security requirements and contractor liability. |
|
Contract administration discipline is implemented to ensure sound administration of the contracts. |
|
TAs are monitored in order to track expenditures and percentage of allocation. |
|
Payments are made only for services received and in accordance with contract terms and conditions and in the appropriate period. All purchases are appropriately authorized. |
Appendix B – Scorecard
Table summary
This appendix presents the conclusion for each of the criterion.
| Criterion | Waves | Conclusion | Rec # | |||
|---|---|---|---|---|---|---|
| 1 | SS | 2 | 3 | |||
Governance |
||||||
|
Needs Moderate Improvement | Satisfactory | Needs Minor Improvement | Satisfactory | The transition between Wave 1 and Wave 2 did not receive sufficient consideration by both departments during the procurement planning phase. However, the Wave 3 process was found to be well planned. The delay in issuing the third Wave 1 contract required HC to issue a sole source contract under its own delegated contracting authority. The contract was issued in a timely manner to a qualified bidder under Wave 1. | - |
|
Needs Moderate Improvement | Needs Moderate Improvement | Satisfactory | Satisfactory | Oversight over the use of TACs by both departments was deficient during Wave 1 and with the sole source contract due to insufficient information. It was strengthened in Wave 2 through better collaboration and information sharing. It will be further strengthened in Wave 3 by incorporating improved monitoring and control measures into the contract terms and conditions. | - |
|
Satisfactory | Satisfactory | Satisfactory | Satisfactory | Roles and responsibilities of the contracting authority (PWGSC) and project authority (HC) were clearly described. | - |
|
Needs Improvement | Needs Improvement | Satisfactory | Unknown; Cannot Be Measured | Contracting information maintained by the project authority (HC) for decision making was insufficient in Wave 1 and with the sole source contract, but it improved significantly in Wave 2. | - |
Risk management |
||||||
|
Satisfactory | Satisfactory | Satisfactory | Satisfactory | The procurement risk assessment was completed by PWGSC for all three waves of TACs. The sole source method of supply was considered the proper interim arrangement to meet HC's nursing services requirements. | - |
Internal control |
||||||
|
Satisfactory | Satisfactory | Satisfactory | Satisfactory | Contract tendering by PWGSC was done for the three waves of TACs, in accordance with contracting policies and regulations. The sole source contract that HC issued was in accordance with HC's delegated authority. | - |
|
Satisfactory | Needs Minor Improvement | Satisfactory | Satisfactory | PWGSC followed the method of bidder selection as outlined in the solicitation documents. HC awarded a sole source contract in accordance with its delegated authority. | - |
|
Satisfactory | Satisfactory | Satisfactory | Satisfactory | The suppliers, the project authority (HC) and contracting authority (PWGSC) provided all of the required certifications. | - |
|
Satisfactory | Satisfactory | Satisfactory | Satisfactory | The project authority (HC) and contracting authority (PWGSC) properly considered all relevant procurement aspects for the nursing service contracts. | - |
|
Needs Improvement | Needs Improvement | Satisfactory | Unknown; Cannot Be Measured | HC contract administration issues were identified in Wave 1 and with the sole source contract. However, HC's contract administration discipline increased in Wave 2 to ensure sound administration of the contracts. | - |
|
Needs Improvement | Needs Improvement | Satisfactory | Unknown; Cannot Be Measured | The audit concluded that TAs were not well-monitored by HC in Wave 1 and with the sole source contract. For Wave 2, the TAs were better monitored, providing sufficient and timely information that helped to ensure proper oversight over the monitoring of expendi- tures and percentage of allocation. |
- |
|
Needs Moderate Improvement | Needs Moderate Improvement | Needs Moderate Improvement | Unknown; Cannot Be Measured | While most purchases were appropriately authorized by HC, the payments were not always in accordance with the terms and conditions of TACs, which were difficult to administer. | 1, 2, 3 |
SS = HC sole source contract
Appendix C – Summary of nursing services contracts
Table summary
This appendix presents detailed information on each contract of the three waves and the sole source contract (list of vendors; date, number and contract amount; expenditures to July 17, 2014; and contract type).
| Detailed list of contracts for each wave | Contract amount | Expenditures (to July 17, 2014) | Contract type | Contract award | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| From | To | Vendor | Contract number | Originally planned | Actual | Task authori- zations |
Confirming orders | |||
Wave 1 |
1/Nov/12 | 31/Oct/13 | Pedabun 35 Nursing Inc. | H3551-112960/001/WPG | $12,600,000 | $12,600,000 | $9,379,253 | Task Authori- zation |
Competitive (Ranked #1) | |
| $525,027 | Confirming Order | |||||||||
| 5/Jun/13 | 31/Oct/13 | First North Health Group | H3551-112960/002/WPG | $3,600,000 | $1,252,500 | $783,516 | Task Authori- zation |
Competitive (Ranked #2) | ||
| $1,020,427 | Confirming Order | |||||||||
| 1/Nov/12 | 31/Oct/13 | Venture Health Care/AHSA | H3551-112960/003/WPG | $1,800,000 | $1,800,000 | $1,159,892 | Task Authori- zation |
Competitive (Ranked #3) | ||
| $73,815 | Confirming Order | |||||||||
HC Sole Source |
2/Apr/13 | 30/Jun/13 | Indigenous Health Group | 4500297377 | $400,000 | $400,000 | $400,235 | Long Form Contract | Sole Source | |
| $88,264 | Confirming Order | |||||||||
Wave 2 |
19/Feb/14 | 31/Oct/14 | First North Health Group | H3551-123194/001/WPG | $11,700,000 | $11,700,000 | $2,514,508 | $- | Task Authori- zation |
Competitive (ranked #1) |
| 1/Nov/13 | 31/Oct/14 | Pedabun 35 Nursing Inc. | H3551-123194/002/WPG | $3,900,000 | $3,900,000 | $1,542,158 | - | Task Authori- zation |
Competitive (ranked #2) | |
| 1/Nov/13 | 31/Oct/14 | Venture Health Care/AHSA | H3551-123194/003/WPG | $1,950,000 | $1,950,000 | $455,250 | - | Task Authori- zation |
Competitive (ranked #3) | |
| 1/Nov/13 | 31/Oct/14 | Indigenous Health Group | H3551-123194/004/WPG | $1,950,000 | $1,950,000 | $958,883 | - | Task Authori- zation |
Competitive (ranked #4) | |
Wave 3 |
24/Jul/14 | 23/Jul/17 | Venture Health Care/AHSA | HT360-123541/001/XF | $60,072,828 | $60,072,828 | $- | $- | Task Authori- zation |
Competitive (ranked #1) |
| 19/Jun/14 | 18/Jun/17 | Pedabun 35 Nursing Inc. | HT360-123541/002/XF | $36,043,697 | $36,043,697 | - | - | Task Authori- zation |
Competitive (ranked #2) | |
| 19/Jun/14 | 18/Jun/17 | Bayshore HealthCare Ltd. | HT360-123541/003/XF | $24,029,131 | $24,029,131 | - | - | Task Authori- zation |
Competitive (ranked #3) | |
Table summary
Summary of contracts for each wave - This appendix presents detailed information on each contract of the three waves and the sole source contract (list of vendors; date, number and contract amount; expenditures to July 17, 2014; and contract type).
| Summary of contracts for each wave | Contract amount | Expenditures (to July 17, 2014) | |||
|---|---|---|---|---|---|
| Contracts | Originally planned | Actual | Task authorizations | Confirming orders | Total |
Wave 1 - one year |
$18,000,000 | $15,652,500 | $11,322,661 | $1,619,269 | $12,941,930 |
HC Sole Source - three months |
$400,000 | $400,000 | $400,235 | $88,264 | $488,499 |
Wave 2 - six months with a six month option period exercised |
$19,500,000 | $19,500,000 | $5,470,799 | - | $5,470,799 |
Wave 3 - three years with five one-year renewal options |
$120,145,656 | $120,145,656 | - | - | $- |
Grand total |
$158,045,656 | $155,698,156 | $17,193,695 | $1,707,533 | $18,901,228 |
- Date modified: