
Public Health Agency of Canada
www.publichealth.gc.ca
Common menu bar links
Institutional links
Diseases & Conditions
Health & Safety
Research & Statistics
Agency Information
Search Box
Healthy settings for young people in Canada
Previous | Table of Contents | Next
Emotional Health in Context
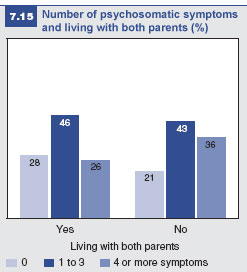
 As shown in Figure 7.15, young people
living with both parents are less likely to
have 4 or more psycho- somatic symptoms
(26%) than children with other living
arrangements (36%).
As shown in Figure 7.15, young people
living with both parents are less likely to
have 4 or more psycho- somatic symptoms
(26%) than children with other living
arrangements (36%).
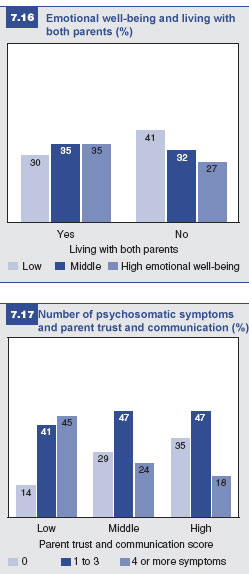
Young people in households with both parents (35%) have a higher emotional well-being score than those not living with both parents (27%) (Figure 7.16).
Ultimately, the effect of the parent-child
relationship on emotional health is much
more important than living with both
parents. While 45% of students with a low
score on the parent trust and communication
scale have 4 or more psychosomatic
symptoms, only 14% report having no
symptoms (Figure 7.17). In contrast, only
18% of young people with a high score on
the parent trust and communication scale
have 4 or more psychosomatic symptoms,
while 35% 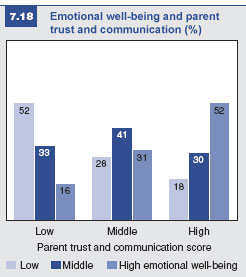 report no symptoms.
report no symptoms.
Figure 7.18 shows the relationship between two scales: parent trust and communication and emotional wellbeing. Fifty-two percent of students with a high score on the parent trust and communication scale have a high emotional well-being score, compared to only 16% of those with a low parent trust and communication score.
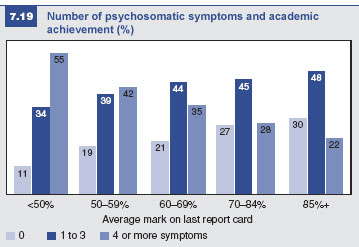
Figure 7.19 demonstrates that the number of psychosomatic symptoms decreases steadily as marks increase. Fifty-five percent of students with averages in the lowest academic achievement category have 4 or more psychosomatic symptoms; this number drops to 42%, 35%, 28%, and 22% in the higher school achievement categories.
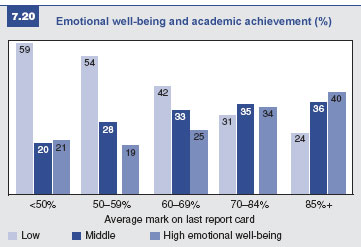
Good marks also influence emotional well-being (Figure 7.20). Fifty-nine percent of students with an average mark of less than 50% have a low emotional well-being score, while only 24% of students with an average mark of 85% or higher fall into this group.
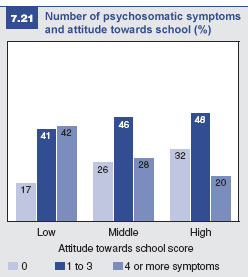

Students (at 42%) with low quality of school experience (i.e., a low score on the attitude towards school scale) are more likely to report 4 or more psycho- somatic symptoms than students with a middle score on the attitude towards school scale (at 28%) (Figure 7.21). In turn, even fewer students (at 20%) with a high attitude towards school score are likely to have 4 or more psychosomatic symptoms.
Attitude towards school has a protective influence on emotional well-being (Figure 7.22) which is similar to its protective influence on psychosomatic symptoms (see Figure 7.21). Twenty-three percent of students with a low attitude towards school score have a high emotional well-being score, while 45% of students with a high attitude towards school score have a high emotional well-being score.
There is a connection between the communication with friends and emotional well-being scales. Twenty-seven percent of students with a low communication score have high emotional well-being, in contrast to 38% of students with high communication levels (Figure 7.23).
Psychosomatic symptoms and communication with friends The HBSC data show that different scores on the communication with friends scale have minimal influence on reports of psychosomatic symptoms, with variations as small as 0 to 3% (not shown). |
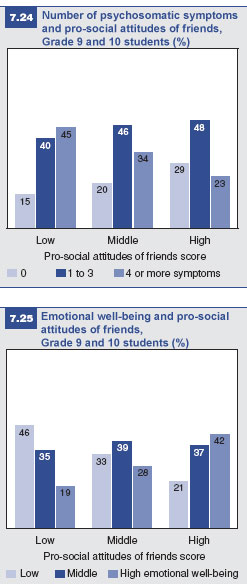
Pro-social attitudes of friends are strongly
related to psychosomatic symptoms. Fortyfive
percent of students with a low score
on the pro-social attitudes of friends scale
have four or more psychosomatic symptoms,
compared to only 23% of students
with a high pro-social attitudes score.
Conversely, 29% of students with a high
pro-social attitudes score have no symptoms,
compared to just 15% of those with
a low score (Figure 7.24).
Pro-social attitudes are also related to emotional well-being. As seen in Figure 7.25, 46% of students in the group with low levels of pro-social attitudes among their friends also have low emotional well-being (and only 19% have high emotional wellbeing); 42% of students in the group that have a high pro-social attitudes score also have high emotional well-being (and only 21% have a low emotional well-being score).
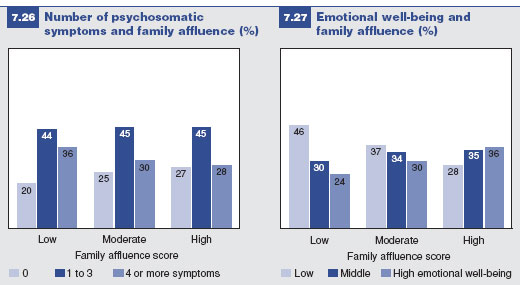
Students from highly affluent families tend to have fewer psychosomatic symptoms (Figure 7.26) and higher emotional well-being (Figure 7.27) than students from families low in affluence. Students from families with moderate affluence occupy a middle position between the other two groups with respect to emotional well-being (Figure 7.27), but are quite similar to the students from highly affluent families in terms of psychosomatic symptoms (Figure 7.26).
 Summary
Summary
While emotional health tends to be similar for both boys and girls in Grade 6, by Grade 10, girls clearly are experiencing poorer emotional health than boys. The critical period for girls appears to be between Grades 6 and 7, when their emotional health becomes markedly poorer. This gender gap seems to be increasing from previous years of the survey.
All four contexts – home, school, peers, and socio-economic status – show a relationship to emotional health. With respect to the home setting and socioeconomic conditions, parent trust and communication is much more critical to understanding emotional health than living with both parents or family affluence. Similarly, quality of school experience (attitude towards school) is more important than academic achievement. Finally, pro-social attitudes of friends are more important than communication with friends for emotional health and well-being.
In each of these contexts, the issues with the greatest impact on emotional health are also the issues most amenable to intervention efforts. By understanding the contributing contextual factors, educators and health care professionals should be better able to develop targeted intervention programs.
References
1 Pedersen, J., and T. Aarkrog (2001). A 10-year follow-up study of an adolescent psychiatric clientele and early predictors of readmission. Nordic Journal of Psychiatry, 55:11-16.
2 BC Partners for Mental Health and Addictions (2006). Personal costs of mental disorders and addictions. Retrieved May 3, 2007 from http://www.heretohelp.bc.ca/publications/factsheets/personalcosts.shtml