|
Handbook on Sensitive Practice for Health Professionals: Lessons
from Women Survivors of Childhood Sexual Abuse
Our mission is to help the people of Canada maintain and improve
their health.
Health Canada
Handbook on Sensitive Practice for Health Professionals
–Lessons from Women Survivors of Childhood Sexual Abuse was
prepared by Candice Schachter, Carol Stalker and Eli Teram for
the Family Violence Prevention Unit, Health Canada.
Également en français sous le titre Manuel de
pratique sensible à l’intention des professionnels de
la santé – Leçons tirées de survivantes
d’abus sexuel dans leur enfance
The opinions expressed in this report are those of the authors
and do not necessarily reflect the views of Health Canada.
Contents may not be reproduced for commercial purposes, but any
other reproduction, with acknowledgements, is encouraged.
This publication may be provided in alternate formats upon request.
For further information on family violence issues, please contact:
The National Clearinghouse on Family Violence
Family Violence Prevention Unit Healthy Communities Division
Centre for Healthy Human Development Health Canada Address Locator:
1909D1 9th Floor, Jeanne Mance Bldg., Tunney’s Pasture Ottawa,
Ontario K1A 1B4 CANADA
Telephone: 1-800-267-1291 or (613) 957-2938
Fax: (613) 941-8930
Fax Link: 1-888-267-1233 or (613) 941-7285 TTY: 1-800-561-5643
or (613) 952-6396 Web Site: http://www.phac-aspc.gc.ca/nc-cn
© Her Majesty the Queen in Right of Canada, 2001 Cat. H72-21/179-2000E
ISBN 0-662-29522-6
| Table of Contents |
|
|
| Acknowledgements |
vii |
|
| |
|
|
|
| I. |
The Handbook as a Tool for Clinical Pratice |
1 |
|
| A. |
Who this handbook is for |
1 |
|
| B. |
How it pertains to my clinical practice |
1 |
|
| C. |
Its utility |
1 |
|
| D. |
The content |
1 |
|
| E. |
Terminology |
2 |
|
| F. |
How it was developed |
2 |
|
| G. |
Its limitations |
3 |
|
| H. |
What this handbook is NOT |
3 |
|
| I. |
How to use the handbook |
3 |
|
| |
|
|
|
| II. |
Background Information About Childhood Sexual
Abuse |
5 |
|
| A. |
What is childhood sexual abuse? |
5 |
|
| B. |
What is ritual abuse? |
5 |
|
| C. |
How prevalent is childhood sexual abuse? |
5 |
|
| D. |
What should health professionals know about the
dynamics of |
|
|
| |
childhood sexual abuse? |
6 |
|
| |
1. Sexual abuse is traumatic |
6 |
|
| |
2. Sexual abuse is a violation of body, boundaries,
and trust |
6 |
|
| E. |
What are the long-term effects of childhood sexual
abuse? |
7 |
|
| F. |
What survivors bring to treatment |
8 |
|
| |
1. Feeling safe is crucial |
8 |
|
| |
2. Transference and Counter-transference |
8 |
|
| |
3. Feelings, experiences and behaviours that
may interfere with |
|
|
| |
treatment |
9 |
|
| |
|
|
|
| III. |
Principles of Sensitive Practice |
13 |
|
| A. |
The fundamental importance of helping the client
to feel safe |
13 |
|
| |
1. Respect |
13 |
|
| |
2. Rapport |
13 |
|
| |
3. Sharing control |
14 |
|
| |
4. Sharing information |
14 |
|
| |
5. Respecting boundaries |
14 |
|
| |
6. Fostering a mutual learning process |
15 |
|
| |
7. Consideration of ebbs and flows |
15 |
|
| |
8. Demonstrating an awareness of the prevalence
and sequelae of |
|
|
| |
violence and childhood sexual abuse |
16 |
|
iii
| Table of Contents |
|
|
|
|
|
| |
|
|
|
|
|
| |
|
|
|
|
|
| IV. |
Guidelines for Sensitive Practice |
17 |
|
| |
A. |
Introduction |
17 |
|
| |
B. |
Preparation for the initial appointment |
18 |
|
| |
|
1. |
The right to choose a clinician and a facility |
18 |
|
| |
|
2. |
Helping prepare the client for treatment |
18 |
|
| |
C. |
Initial evaluation |
18 |
|
| |
D. |
Other treatment considerations |
19 |
|
| |
|
1. |
Consent |
20 |
|
| |
|
2. |
Language and communication |
20 |
|
| |
|
3. |
Clothing |
21 |
|
| |
|
4. |
Touch |
21 |
|
| |
|
5. |
Privacy |
22 |
|
| |
|
6. |
Other environmental considerations |
23 |
|
| |
|
7. |
Issues related to pain |
23 |
|
| |
|
8. |
Time factors |
24 |
|
| |
|
9. |
Control and adherence to treatment |
25 |
|
| |
|
10. |
Encouraging reconnection with the body |
26 |
|
| |
|
11. |
Encouraging and modelling self-care |
26 |
|
| |
|
12. |
Problem solving |
26 |
|
| |
|
13. |
Continuity of care |
27 |
|
| |
E. |
Dealing with the client who is upset |
27 |
|
| |
|
1. |
Identifying triggers |
27 |
|
| |
|
2. |
Recognizing body language that may indicate
discomfort, |
|
|
| |
|
|
triggering, dissociation |
27 |
|
| |
|
3. |
Managing triggers and dissociation |
28 |
|
| |
|
4. |
After the experience |
30 |
|
| |
|
5. |
Working with survivors who have Dissociative
Identity Disorder |
30 |
|
| |
F. |
Disclosure of childhood sexual abuse |
30 |
|
| |
|
1. |
Introduction |
30 |
|
| |
|
2. |
What is disclosure? |
30 |
|
| |
|
3. |
Clinician-initiated inquiries |
30 |
|
| |
|
4. |
Survivor-initiated disclosure of past abuse |
31 |
|
| |
|
5. |
What should I say when someone discloses? |
32 |
|
| |
|
6. |
What should I NOT say or do when someone discloses? |
32 |
|
| |
|
7. |
After a client has disclosed |
33 |
|
| |
G. |
Health care records |
34 |
|
| |
|
1. |
Confidentiality of records |
34 |
|
| |
|
2. |
Some issues in documentation |
34 |
|
| |
H. |
Discharge |
35 |
|
| |
I. |
Other suggestions to assist both client
and clinician |
36 |
|
| |
|
1. |
Community resources and counselling |
36 |
|
| |
|
2. |
Taking care of yourself |
37 |
|
| |
|
3. |
Consultation with other health professionals |
37 |
|
| |
J. |
The clinician’s contribution to
the survivor’s healing |
37 |
|
iv
| |
Table of Contents |
|
|
|
|
| |
|
|
|
| |
|
|
|
| V. Concluding Comments |
|
39 |
|
| |
|
|
|
| References |
|
41 |
|
| |
|
|
|
| Appendix A: Diagnostic Criteria for Post
Traumatic Stress Disorder |
|
45 |
|
| |
|
|
|
| Appendix B: Dissociation |
|
46 |
|
| |
|
|
|
| Appendix C: |
Suggestions for Clients at Out-patient Physical
Therapy Facilities |
47 |
|
| |
|
|
|
| Appendix D: Sample Consent Form |
|
49 |
|
| |
|
|
|
| Appendix E: Recommended Reading |
|
50 |
|
| |
|
|
|
| Index |
|
51 |
|
v
Acknowledgements
The authors wish to thank all of the survivors, physical therapists,
physical therapy students and counsellors who participated in the
three phases of this research project. These individuals gave generously
of their time and energy: without them, this handbook would not
have been possible.
We would also like to thank those who organized and assisted with
the focus groups in Phases Two and Three: Lesley Bainbridge, Susan
Bagley, Cheryl Blahut, Brenda Collacott, Tes Cournoyer, Peter Cox,
Chantale Dumoulin, Sharon Elliott, Barbara Gibson and the College
of Physiotherapists of Ontario, Maureen Graham, Shayna Hornstein,
Sheri McConnell, Kathy Mulder, Jodi Payant, Elizabeth Sled and Marilyn
Veikle. Sincere thanks are also extended to Anne Derrick, Diana
Majury, Karen Busby, Gwen Beaton, Heather Dzioba, Maureen Kennedy,
Judy Russell and Marusha Taylor.
The authors gratefully acknowledge the direction and expertise
of the Family Violence Prevention Unit, Health Canada.
The authors also thank the following for permission to reprint
previously published material.
•
|
Components of the section on disclosure
and some quotations from survivors have been reprinted from:
Teram, E., Schachter, C. L., & Stalker,
|
| |
C.
|
A. Opening the doors to disclosure: Childhood
sexual abuse survivors reflect on telling physical therapists
about their trauma. Physiotherapy (1999).85:88–97
with the permission of Physiotherapy.
|
•
|
Components of the background information
on childhood sexual abuse, principles and guidelines and survivors’
quotations have been reprinted or adapted and reprinted from:
Schachter, C. L., Stalker, C. A., & Teram,
|
| |
E.
|
Toward sensitive practice: issues for physical
therapists working with survivors of childhood sexual abuse.
Physical Therapy (1999).79:248–261 with
permission of the American Physical Therapy Association.
|
•
|
Some survivors’ quotations have
been taken from: Stalker, C. A., Schachter,
|
| |
C.
|
L., & Teram, E. Facilitating effective relationships
between survivors of childhood sexual abuse and health professionals:
lessons from survivors who have received physical therapy.
Affilia: Journal of Women and Social Work (1999).14:176–198
with the permission of the authors.
|
Lastly, the authors gratefully acknowledge the support received
from the following funders:
- Health Canada
- Physiotherapy Foundation of Canada
- University of Saskatchewan College of Medicine Scientific Teaching
and Research Fund
- University of Saskatchewan President’s SSHRC Grant Program
- University of Saskatchewan New Faculty Start-up Grant Program
- Wilfrid Laurier University Research Grants Program
vii
I. The Handbook as a Tool for Clinical Practice
A. Who is this handbook for?
This handbook has been written for health professionals and students
who are not trained as mental health professionals or psychotherapists
and who have limited experience working with survivors of childhood
sexual abuse. The handbook offers ideas and suggestions for ways
to practise that are sensitive to the needs of survivors of childhood
sexual abuse. We have termed these ideas and suggestions “sensitive
practice”.
- How can the information in this handbook benefit my clients?
The research on which this handbook is based has shown how important
it is for survivors to feel safe. The survivor who does not feel
safe may not be able to fully participate in or benefit from treatment.
In some instances, the survivor may even stop treatment because
he or she does not feel safe enough to continue. This handbook offers
suggestions that can help the clinician facilitate the feeling of
safety during treatment, thereby assisting the client to benefit
more fully from treatment.
- How does this handbook pertain to my clinical practice?
At least 1 in 5 women and 1 in 10 men are survivors of childhood
sexual abuse.1 The high prevalence rates and research
indicating that childhood trauma is associated with a greater risk
of a wide variety of health problems suggests that health professionals
work, often unknowingly, with survivors.
Sensitive practice is not just for survivors of childhood sexual
abuse. All clients need sensitive practitioners.2
Although this handbook focuses on female survivors of childhood
sexual abuse, it captures essential features of clinical practice
for all clients. Thus, the reader will find ideas in this
handbook that can be applied to (or already reflect) his or her
current practice. The handbook goes on to highlight specific practice
suggestions for the clinician working with clients who have histories
of abuse.
D. What is in the handbook?
This handbook is divided into three sections:
- Background Information About Childhood Sexual Abuse. This
section will assist the clinician to understand more fully why
sensitive practice is important for the client who is a survivor.
The dynamics, long-term effects and types of feelings, experiences
and behaviours that may interfere with treatment are described.
- Principles of Sensitive Practice. These principles underlie
all interactions between health professionals and their clients.
- Guidelines for Sensitive Practice.
These are practical suggestions that health professionals can
incorporate into clinical practice.
1
Handbook on Sensitive Practice for Health Professionals: Lessons
from Women Survivors of Childhood Sexual Abuse
E.
|
Terminology used in the handbook
• The
terms survivor and client are used interchangeably,
both because the clinician may not be aware of a client’s
history of childhood sexual abuse and because this information
is not required for a clinician to practise sensitively.
• The handbook uses the word survivor instead
of victim. In using the term survivor, we celebrate the
strength and resourcefulness of the person who developed ways
of coping with her abuse.3
• The terms
abuse and violence are used interchangeably throughout
this handbook. Abuse may not always involve physical injury;
however, it is a violation of the person and is usually experienced
as traumatic.4
• This handbook uses
the feminine pronoun because it is based on research with women
survivors. While there appear to be some differences in the
way that males and females respond to child sexual abuse, “outcome
studies have actually had difficulty demonstrating consistent
differences in symptomatology between abused boys and girls
or men and women. It would appear, based on current research,
that there are more similarities than differences in the impact
of abuse [on males and females].”1, p. 47 Although
we believe that the Principles for sensitive practice (Section
III) and Guidelines for sensitive practice (Section IV) may
be helpful in working with all survivors, further research about
the specific needs of men is required.
|
- How the handbook was developed
This handbook is the product of a multi-disciplinary research
study designed to explore ways that health professionals can best
address the health care needs of adult female survivors of childhood
sexual abuse. The project initially focused on physical therapy,
but as the reader will see, this handbook goes beyond the bounds
of physical therapy practice to describe sensitive practice in all
health professions.
The research was conducted in three phases. In the first phase,
27 adult female survivors of childhood sexual abuse in Saskatchewan
and Ontario were interviewed. Following the conventions of qualitative
research methods, recruitment of new participants was stopped when
the researchers sensed a saturation of the data (that is, when themes
continued to be repeated and no new themes emerged).
The survivors, who were predominantly Canadian-born Caucasian,
ranged in age from 19 to 62 and had a broad range of educational
backgrounds, professions and socio-economic status. All women had
begun their journeys of healing from childhood sexual abuse. They
had been referred to both in-patient and out-patient physical therapy
for orthopaedic and cardiorespiratory problems. The women described
their experiences in physical therapy, and how practitioners could
be more sensitive to their needs. For a summary and analysis of
the findings of the interviews, the reader is referred to Schachter,
Stalker & Teram,5 Teram, Schachter & Stalker6
and Stalker, Schachter & Teram.7
2
The Handbook as a Tool for Clinical Pratice
The researchers chose to interview women initially because statistics
suggest the prevalence of childhood sexual abuse is significantly
higher in females than males.1,8–11 This is not
to suggest that the experience of male survivors is in any way less
important than that of females. We subsequently sought to recruit
male survivors but were unsuccessful. We hope that our work will
lead to research investigation of sensitive practice specifically
with male survivors.
In the second phase of the project, groups of physical therapists
and survivors worked together to develop recommendations for the
Guidelines for Sensitive Practice. Group members who were physical
therapists applied the ideas in their clinical practices and offered
feedback to the groups. The groups then used this feedback to refine
their recommendations.
In the final phase of the project, the information from the interviews
and working groups was used to draft the handbook. The words of
survivors who were interviewed for the study are included throughout
the handbook to provide powerful illustrations of their feelings
and thoughts. In successive drafts, physical therapists, physical
therapy students, survivors and counsellors across Canada offered
their feedback. This broad consultative process was designed to
ensure clinical applicability of the handbook.
G. Limitations of the handbook
It is important to point out that race, culture, class, sexual
identity, stage of recovery from childhood trauma and other factors
will affect a survivor’s response to a health professional.
Thus, this document does not capture every individual response nor
does it inclusively describe every aspect of clinical practice that
is sensitive to survivors. While acknowledging these limitations,
we feel that the handbook offers health professionals both a useful
framework and many broadly applicable suggestions for all types
of practice.
H. What this handbook is NOT
The ideas described in this handbook are not intended to encourage
health professionals to step outside their scope of practice and
develop skills in the realm of psychotherapy. In addition, this
handbook is not meant to be used as a tool to intentionally facilitate
emotional release. Lastly, the handbook is not meant to help
the clinician detect whether the client is a survivor of abuse.
I. How to use the handbook
We encourage the clinician and student to approach the handbook
in the following ways.
- Reflect on the links among the background information about
childhood sexual abuse, the principles of sensitive practice and
the guidelines for sensitive practice.
3
Handbook on Sensitive Practice for Health Professionals: Lessons
from Women Survivors of Childhood Sexual Abuse
•
|
Discuss with others the ideas expressed
here.
|
•
|
Consider:
|
| |
–
|
how the ideas and suggestions apply to you;
|
| |
–
|
how you would actively implement the suggestions
in your practice; and
|
| |
–
|
what your responses would be in various situations
described in the handbook.
|
You may initially feel that certain suggestions in the handbook
do not apply to your practice. Before dismissing the suggestion,
consider two questions:
1.
|
Why does this suggestion not apply?
|
2.
|
Is there another way to incorporate part of this
suggestion or the essence of the suggestion into my practice?
|
4
II. Background Information About Childhood Sexual Abuse
- What is childhood sexual abuse?
The sexual abuse of a child is a criminal act. “Child sexual
abuse occurs when a child is used for the sexual gratification of
an adult or adolescent. It involves the exposure of a child to sexual
contact, activity or behaviour, and may include invitation to sexual
touching, intercourse, or other forms of exploitation, such as juvenile
prostitution or pornography.”4, p.1 The child’s
consent to such activity is a moot issue because “authority
and power enable the perpetrator, implicitly or directly, to coerce
the child into sexual compliance.”12, p.9 Children
who are sexually abused are often also abused physically and emotionally.
3) psychopathological ritualism where mentally disturbed individuals
abuse children while using idiosyncratic rituals. Ritual abuse is
sometimes used synonymously with the term “satanic abuse,”
but this would be correct only when child abuse is combined with
rites and practices by people who worship Satan.
Reports by children and adults of horrific abuse, torture and
brainwashing have been repeatedly received from many parts of the
world, and many of the reports are virtually identical in detail,
even though the informants are unknown to each other. While police
have been able to find physical evidence for some allegations, for
many they have been unsuccessful. Consequently, there is controversy
regarding the prevalence of this form of abuse. Since ritual abuse
often involves sadistic acts and degradation of the victim, it can
have very serious long-term effects.13
B. What is ritual abuse?
Ritual or ritualistic abuse refers to abuse at the “extreme
end of the spectrum of child sexual abuse.”13, p. 163
Individuals who have experienced ritual abuse often identify
both as survivors of childhood sexual abuse and ritual abuse. Ritual
abuse usually involves a combination of physical, sexual and emotional
abuse, and frequently refers to abuse suffered by individuals as
part of a group, and in the context of a powerful belief system.
Finkelhor, Williams and Burns14 describe three subtypes:
1) true cult-based in which sexual abuse is only one element of
the child’s involvement in cult rituals and beliefs, 2) pseudo-ritualistic,
in which sexual abuse is the principal activity and cult rituals
are secondly, and
- How prevalent is childhood sexual abuse?
The 1984 Royal Commission on Sexual Offences Against Children
and Youth reported that 22% of women and 10% of men had experienced
childhood sexual abuse before the age of 18 years in Canada.8
While there is some variation in prevalence rates reported
by different studies in the literature, most reviewers have concluded
that at least 20% of women and from 5% to 10% of men in North
America have experienced sexual abuse during childhood. The
percentage
5
Handbook on Sensitive Practice for Health Professionals: Lessons
from Women Survivors of Childhood Sexual Abuse
of adults reporting histories of childhood sexual abuse may vary
in part because of the use of different ages to define the end of
childhood, and whether experiences such as abuse by peers, witnessing
exhibitionism, exposure to pornography, or receiving unwanted invitations
to engage in sexual activities are included within the definition.
- What should health professionals know about the dynamics
of childhood sexual abuse?
Difficulties which survivors may experience when seeing health
professionals can result from past abuse. While the clinician cannot
change a survivor’s history, an appreciation of the dynamics
and long-term effects can provide a better understanding of the
client’s reactions during treatment. The following summary
has been derived from mental health research, clinical literature
and interviews with survivors.
1. Sexual abuse is traumatic
Many of the reactions of childhood sexual abuse survivors are
similar to those experienced by survivors of other kinds of overwhelming
life events such as military combat, sexual assault in adulthood,
and natural disasters, and are included in the criteria for Post
Traumatic Stress Disorder4,15 (see Appendix A). While
some adults who were sexually abused as children do not report long-term
negative effects, most mental health professionals and researchers
agree that a history of childhood sexual abuse is associated with
a range of significant difficulties in adulthood.
Our society tends to place violent acts on a continuum: certain
acts are judged to be “not as violent” as others. We then
proceed to place trauma that results from violence and the victim’s
reactions to the violent acts on a similar continuum. Such judgements
are harmful to those who have experienced violence. It is not the
role of health professionals to make judgements about the relative
severity of the violence, the resulting trauma or an individual’s
reactions to the experiences.
- Sexual abuse is a violation of body, boundaries and trust3
The violations of body, boundaries and trust can affect the survivor’s
relationships with herself, her body and others. When a child is
abused, she feels out of control and powerless. She is invalidated:
her sense of reality is challenged and what she wants does not count.
As a result, the child learns that her body does not belong to her
and that she has no right to have any say over what happens to her
body. She learns to disown and not care about her body. To live
through the abusive episodes, she may have learned to disregard
or ignore signals of pain, injury, alarm, danger or other sensations
that her body generates, or to disconnect from her body. Thus, the
survivor’s relationship or connection with her body can be
damaged.3,4
Childhood sexual abuse is, by definition, a violation of boundaries.
Most children learn about boundaries early in life through day-to-day
interactions. They internalize ideas about what is personal or private,
and about what physical and emotional closeness and distance mean.
When a child sees and experiences that others respect her boundaries
and her
6
Background Information About Childhood Sexual Abuse
wishes for privacy and separateness, it reinforces the idea that
she is a valuable person. She learns that she is separate from others,
that she is a self, and that she has an identity of her own. But
the child who is sexually abused learns that her body belongs to
someone else. Her body is used to meet someone else’s needs,
and her feelings, wishes and needs are not important. Thus, her
relationship or connection to her sense of self, and her sense of
who she is, are damaged.3,4
Most sexual abuse is perpetrated by people known to the child
– family members, baby sitters, friends of the family, teachers,
coaches, clergy, etc. –people given responsibility for protecting
and nurturing the child. The consequences of this experience can
be profoundly devastating. When such people take advantage of her,
the child is betrayed. The world becomes an unsafe place as she
learns that people who say that they care, or are in care taking
roles, cannot be trusted. Thus, her relationship with others (including
health professionals) can be damaged.3,4
- What are the long-term effects of childhood sexual abuse?
Numerous studies have documented that childhood sexual abuse is
associated with mental, interpersonal and physical health problems
in adulthood.16 Long-term sequelae can affect many aspects
of function, including cognitive, emotional, behavioural, interpersonal
and physical. The following describes some types of difficulties
that have been documented by researchers and health professionals.
Cognitive – Studies indicate that child abuse is often
associated with distorted beliefs and perceptions about one’s
self, one’s behaviour, and the intentions of others. These
distortions can lead to guilt, self-blame and low self-esteem.10
Perceptions of helplessness, chronic danger and consequent
hypervigilence (extreme sensitivity and watchfulness for possible
danger) are common.10 Belief that one is powerless may
present as passivity or, conversely, as behaviour that others experience
as controlling.10
Emotional – Long-term correlates include depression,
anxiety, anger, fear, dissociation (defined on page 10) and numbing
of feelings.10,17
Behavioural – Studies reveal a number of actions used
by survivors to cope with or avoid distress or emotional pain. These
include substance abuse and addiction, self-harm, suicide attempts,
eating disorders and health risk behaviours such as earlier onset
of smoking, earlier sexual intercourse and multiple sexual partners.18
Interpersonal – Difficulties include reluctance to
trust others, avoidance of intimacy and close relationships, sexual
problems and fear of being alone.10 Because survivors
have had basic boundaries violated and have experienced a lack of
sensitivity to their feelings and needs, some may have difficulty
learning usual social behaviours that require sensitivity to the
feelings and boundaries of others.
Physical – Studies repeatedly show that traumatic
childhood experiences, including childhood sexual abuse, are
7
Handbook on Sensitive Practice for Health Professionals: Lessons
from Women Survivors of Childhood Sexual Abuse
associated with higher rates of lower back pain,19 chronic
pelvic pain,20–22 gastrointestinal disorders,23
chronic headache24,25 and general medical problems.18,26
Some painful conditions may be a direct result of past abuse which
has left permanent structural damage and becomes more problematic
as the individual ages.
The stress of traumatic incidences can have long-term adverse
effects on normal physiological functioning.15 “The
growing fields of psychosomatic medicine, psychoendocrinology, and
psycho-immunology are increasingly providing information about the
relationship between external events, brain biochemistry, the body,
and the way the mind interprets all these events.”27,
p.21
Research on traumatic memory supports the concept of “somatic”
or “body memory.” Traumatic memories may be encoded as
part of the non-verbal “non-declarative” memory, independent
of normal language-based memory. Such traumatic memories can be
triggered by stress in the present that reminds the person of past
trauma, and can be experienced as “somatic” or “body
memory.”28
- What survivors bring to treatment
1. Feeling safe is crucial
A feeling or perception of safety is a crucial need for the survivor
because of the violations she has experienced in the past. This
need to feel safe is compelling in all aspects of the survivor’s
life, including her interactions with health professionals.
- Transference and Counter-transference
Transference: When Past Experiences Interfere with Present
Situations
The factors discussed in this section are related to the psychological
phenomenon of transference. This term refers to the displacement
of feelings and perceptions about past situations to experiences
in the present.
A number of psychological theories propose that we all experience
transference in our lives. While transference can be positive or
neutral, it can also be negative and may interfere with healthy
and adaptive functioning. For example, as a child, the survivor
may have been frequently criticized by a parent or the person who
abused her. She may then expect that the clinician (another authority
figure) will also criticize her, and perceive a critical attitude
where none is intended. Understanding the concept of transference
may help the clinician to avoid taking these responses personally.
Counter-transference
Counter-transference occurs when a health professional
transfers feelings and perceptions from past situations to the relationship
with the client, or allows the client’s transference response
to evoke a non-therapeutic response. “Counter-transference
may manifest as: needing to be liked or admired by one’s clients;
expecting to have one’s opinions on any and all topics endorsed.”
29, p.5
Both transference and counter-transference responses are normal,
but must be resolved ethically, so the client does not develop resistance
to healing, and the care that the clinician provides is
8
Background Information About Childhood Sexual Abuse
not compromised through emotional over-involvement or exploitation
of the therapeutic relationship.29
- Feelings, experiences and behaviours that may interfere
with treatment
Feelings and experiences commonly associated with childhood sexual
abuse can impede the therapeutic process by compromising the survivor’s
sense of safety. It is not possible to present a complete list because
feelings, experiences and behaviours can vary widely among individuals.
This section outlines some of the common feelings, experiences and
behaviours that survivors may bring to their relationships with
health professionals. Clinicians who broaden their understanding
of childhood sexual abuse will be better prepared to respond well
to unusual reactions to treatment that may be related to past abuse.
The reader is cautioned, however, that these reactions and feelings
are not limited to survivors. One cannot draw conclusions about
a client’s past solely on the basis of these feelings and behaviours.
The Principles and Guidelines for Sensitive Practice that follow
provide ideas for client-centred care that address the difficulties
that are briefly outlined in this section.
a. Fear and distrust
…[sitting in the clinic waiting room, I felt] nervous,
apprehensive, not exactly knowing what was going to happen…Just
as far as clothing was concerned or...touch, just not knowing…
Many survivors experience tremendous anxiety and fear of being
hurt during treatment. The survivor may distrust the health care
professional and therefore be hesitant to adhere to treatment.
b. Physical pain
For many, the experience of physical pain is cognitively associated
with past abuse. This may be seen in various ways: some survivors
have learned to numb their pain or dissociate from it; others may
feel the full force of both current pain and the pain of the abuse.
I think sometimes when survivors are in pain, and coming for
physiotherapy, it hooks us back into…our childhood where we
were in pain and…no one responded. And if you did indicate
you were in pain...the pain was trivialized or you were threatened
[not to tell] anyone.
c. The need to feel “in control”
The need to feel “in control” often arises from past
violations in which the child had no control over what was done
to her. As a result, a perceived lack of control will diminish the
survivor’s feeling of safety during treatment and may affect
treatment adherence.
I’m learning that if I don’t have a sense of control…I
will walk away from [the situation].
d. Discomfort with men
Perpetrators of childhood sexual abuse may be men or women; however,
statistics suggest that the majority of perpetrators are men.1
As a consequence, the female survivor may feel unsafe and
uncomfortable in the presence of the male health professional.
9
Handbook on Sensitive Practice for Health Professionals: Lessons
from Women Survivors of Childhood Sexual Abuse
[A male physical therapist and assistant were] in the room
with me, and I had my pants off, and this guy’s putting [ultrasound]
gel on my leg. And I felt really uncomfortable…Even though...
probably nothing could have happened, but I just didn’t like
the fact that I was in a room by myself with my pants off, with
two men. That was really eerie.
Some survivors may also feel uncomfortable around male clients.
In one instance, I was beside a couple of men [who were also
patients], and…I was lying down with my ankles on a cushion
and I felt very vulnerable and I remember not being able to concentrate
on what I wanted to do because I was worried about the two men beside
me. And in fact, it probably was very detrimental to the physiotherapy
I was trying to do. The men were harmless, but there’s a certain
vulnerability of lying down and not being able to flee…
e. Ambivalence about the body
Many survivors feel hate or shame about their bodies, and/or feel
disconnected from their bodies. The conflict between a survivor’s
need to seek treatment for a physical problem and her difficulty
in caring for her body may affect treatment. She may, for example,
ignore symptoms that could offer valuable insight into diagnosis
or response to treatment.
And [the amount of attention that I give to my body] ebbs and
flows too, depending on where I’m at and how well I’m
choosing to take care of my body. Which is a very difficult thing
for me physically to do, because when you don’t live there,
it’s just sort of a vehicle to get around.
f. Conditioning to be passive
Abuse often teaches children to avoid speaking up or questioning
authority figures. As adults, survivors may have difficulty expressing
their needs to the health care practitioner who is now the authority
figure.
[The therapist did something and] I really freaked but…I
didn’t show her I was freaking, because our history is that
you don’t let on if things are a problem for you. You just
deal with it however you can…by dissociating or what have you.
g. Triggers
A flashback is an experience of reliving something experienced
in the past. Some survivors have a susceptibility to flashbacks
and being overwhelmed by feelings related to the past. Examination
and/or treatment may “trigger” or precipitate flashbacks
or overwhelming emotions such as fear, anxiety, terror, grief or
anger. This may occur momentarily or for a longer period. Such experiences
are thought to involve a dissociative process.
And the goop that they put on me for the ultrasound gave me
flashbacks, nightmares, insomnia, I just couldn’t deal with
it.
h. Dissociation
Dissociation has been described as “a disruption in the usually
integrated functions of consciousness, memory, identity, or perception
of the environment.”30, p. 477 It may be sudden
or gradual, transient or chronic. Dissociation “should not
be considered inherently pathological and often does not lead to
significant distress, impairment or help-seeking
10
Background Information About Childhood Sexual Abuse
behavior.”30,p. 477 One common experience of dissociation
is highway hypnosis where an individual who has been driving a car
suddenly realizes that he or she does not remember what happened
during all or part of the trip.31
Dissociation can be viewed as a skill which the survivor used
to alter her attention for adaptive purposes – as a child,
she used this skill to cope with the abuse. When the survivor continues
to use this coping strategy in adulthood, it can interfere with
adaptive functioning.28 Many survivors report that they
are not able to have consistent control over this ability to “escape”
from the current (usually stressful) situation and some report having
been unaware of their tendency to dissociate for many years.
Some survivors describe experiencing themselves as being outside
their bodies, watching the present situation from a distance, an
experience which is thought to be the result of a dissociative process.
Some find it painful and difficult to come back to the present.
[In a physical therapy session] I would just get that same
dread feeling inside, and I would do the same coping that I would
have done when I was abused...Just trying to not feel my arms and
not really be there.
Researchers continue to study dissociation, a phenomenon which
has been said to be “devilishly complicated.”28,
p. 287 Considerable empirical research supports the hypothesis
that dissociation is a common response to a traumatic situation
and a response which is not exclusive to survivors of childhood
abuse.32 For a further explanation of dissociation, see
Appendix B.
i. Self-harm
Self-harm (such as scratching, cutting or burning the skin) is
a method of coping for some survivors. Health professionals may
see evidence of self-harm in the form of injuries or scars on the
arms, legs or abdomen.
There are many reasons why survivors harm themselves. It may serve
to distract or numb the survivor from her emotional pain; it may
shift her feeling of pain to one concrete area; it may serve to
end episodes of feeling numb. Others may seek to punish themselves
because of a sense of self-blame for past abuse.
11
III. Principles of Sensitive Practice
The fundamental importance of helping the client to feel safe
…I now am beginning to understand that my physical wellness
is really very connected to my emotional state, and if I’m
not comfortable, if I’m feeling unsafe, then I’m not going
to progress as quickly as a physiotherapist would want me to.
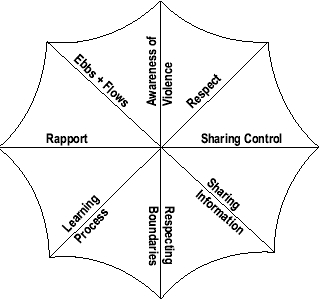
One of the primary goals of treatment must be the development
of feelings of safety for the client. Safety can be seen as a protective
umbrella: when it is open, the survivor can participate in the treatment
at hand. The spokes that keep the umbrella of safety open are the
principles of sensitive practice.
1. Respect
Respect can be defined as realizing the individuality of the other
person.33 The survivor may be very sensitive to any hint
of disrespect as a result of past abuse during which she was not
respected in a fundamental way.
I find [physical therapists and other health professionals]…
don’t even consider the fact that maybe you might feel uncomfort-able…A
lot of them…say, “Oh, we just see you as a patient…we
don’t see you as a person”…part of me says, “No
I don’t think so! You’re human, and I’m human, and
[therapy] is a personal thing….You’re looking at my
body, you’re touching my body
and you’re asking me about my life.”
That’s personal.
2. Rapport
While establishment of rapport is important in every therapeutic
relationship, it is an all-important component of facilitating feelings
of safety for the survivor. Development of rapport must begin at
the first moment of clinician-client interaction and must be given
ongoing attention.
The balance of professionalism and friendliness that contributes
to positive rapport is partly a function of individual style. But
the clinician who is distant and cold in his or her professionalism
is not likely to facilitate a positive connection with the client.
Conversely, an overly familiar style can feel invasive and disrespectful.
Developing a balance is
13
Handbook on Sensitive Practice for Health Professionals: Lessons
from Women Survivors of Childhood Sexual Abuse
crucial, keeping in mind that effective professionals convey genuine
caring while maintaining appropriate boundaries.
…
|
I was just another name on a
|
[
|
referral]… She had no warmth…I didn’t
|
experience being safe with her because I didn’t think
that this was somebody I could talk to at all, about anything! She
just was NOT interested…
3. Sharing control
As a child, the survivor was not allowed control over her own
body. Consequently, in adulthood, the sense of having control is
of paramount importance in the establishment and maintenance of
safety. By sharing control, the client can become a respected, active
participant rather than a bystander during treatment. The clinician
can act as a coach or facilitator, working with, rather than
on the client.
…[the physical therapist] brings definite knowledge and
expertise [into treat-ment]…So together with what I know and
what I can tell her, I would hope that she would be able to…assess
the situation and offer alternatives... So instead of her being
the expert and me being the patient, us being co-communicators about
my body. That’s what I’d like to see…
4. Sharing information
Sharing information with the client about the initial examination
and about every component of treatment also helps the client to
develop a sense of safety. Information sharing must be extended
to
the ways in which the client can best retain information about
her body and her treatment when she leaves her appointment.
Information must flow both from clinician to client and from client
to clinician. The onus for this two-way flow of information rests
with the clinician: she or he should explain the examination and
treatment and seek ongoing feedback about reactions to treatment
as well as about the client’s perceived progress.
5. Respecting boundaries
Respect of boundaries is a crucial safety issue.
As a survivor, I need to know that that person is not going
to invade my space. Or do harm to me. Not necessarily physically,
but emotionally.
The word “boundaries” refers to the outer limit of the
space we consider personal, in both physical and psychological terms.
Boundaries define or delineate the areas of the body and the limits
of information that we feel are appropriately under our control.
Touching a person without consent breaches a physical boundary;
asking very personal questions breaches a psychological or privacy
boundary. When a breach occurs, the individual feels violated.
The concepts of power and responsibility in the therapeutic relationship
factor prominently in any discussion of boundaries. “…[Boundaries]
recognize the inherent power inequity of the [therapeutic] relationship
and set limits
14
Principles of Sensitive Practice
for the therapist’s expression of power.”34, p.
50 In the position of power, health professionals are responsible
for ensuring that, first and foremost, the therapeutic relationship
serves the client’s needs. In failing to set or respect
boundaries, the clinician allows his or her needs to come before
the needs and best interests of the client. For example, a boundary
is violated if a practitioner, rushed for time, decides that she
or he does not have time to ask for consent before beginning a procedure.
In doing so, the clinician is addressing his or her need rather
than the client’s needs.
Boundaries can be confusing at times for both the client and clinician.
Boundary violations are often inadvertent. It is up to the clinician
to remain focused on maintaining appropriate boundaries for both
the client and herself or himself. While less common, the clinician
may also experience boundary violations. The survivor may sexualize
authority figures because as a child she learned to relate to the
abuser primarily in a sexual way. It is the clinician’s responsibility
to be alert to boundary violations and potential violations and
to address both, should they arise. The onus is always on the clinician
to clarify the situation and guard against violation of boundaries.
Some survivors who, by definition, experienced boundary violations
as children, may have only just begun to appreciate the importance
of boundaries. By demonstrating respect for and sensitivity to boundaries,
the clinician may serve as a model for the survivor who is learning
to establish healthy boundaries in her life.
- Fostering a mutual learning process
The principles outlined above underpin ways of interacting that
the survivor may not have experienced as a child and is only now
learning as an adult. She may need encouragement in her journey
to become a full, active participant in her health care. Concurrently,
the clinician must discuss shared responsibility for the survivor’s
health with the client in a way that invites participation without
creating unrealistic expectations of treatment outcomes.
…That assertiveness of [saying] “no” takes a
long time to get...it was somebody else giving me permission that
allowed me to say “no” until I could learn to give myself
permission [to do so]…
At the same time, the clinician is learning about working with
survivors. The survivors who participated in this research reminded
us that mistakes and uncomfortable situations are inevitable, but
that two remedies are invaluable. First, the clinician needs to
recognize his or her mistake and offer an apology. Second, the clinician
should discuss the situation with the client to resolve the problem
that has arisen.
- Consideration of ebbs and flows
Parts of my body at different times might be untouchable. It’s
gonna change, depending on what I’m dealing with. So, you’re
not going to be able to make a list and count on that every time
kinda thing: it’s gonna be a check-in every session.
15
Handbook on Sensitive Practice for Health Professionals: Lessons
from Women Survivors of Childhood Sexual Abuse
Neither coping with the effects nor healing from childhood sexual
abuse are linear processes. As a result, the survivor may vary in
the degree to which she is able to tolerate and participate in treatment
at various times. Such variations in the survivor’s tolerance
may occur rapidly (day-to-day) or may develop over longer periods
of time. To address the possibility for such change, the clinician
must repeatedly “check-in” with the client and be willing
to adjust the treatment approach accordingly.
- Demonstrating an awareness of the prevalence and sequelae
of violence and childhood sexual abuse
Many survivors look for indicators of a clinician’s awareness
of issues of violence and abuse. Demonstrating this awareness can
take a variety of forms. External indicators such as displaying
posters and
pamphlets from the local sexual assault centre offers a cue that
health professionals have such an awareness of the prevalence of
violence and abuse. Incorporating the Principles and Guidelines
of Sensitive Practice into daily practice is a strong indicator
of awareness of issues of violence and abuse.
…I’m way more interested in...how much awareness
[the therapist has] around trauma. So, that holds a lot of weight
with me.
16
IV. Guidelines for Sensitive Practice
A. Introduction
All survivors are not the same. Some survivors experience few
negative effects of past abuse. Some have learned to manage the
long-term effects in ways that do not interfere with their daily
functioning. Other survivors experience these effects in all aspects
of their lives.
Concurrently, survivors are also at different points on the continuum
of healing from past abuse. Some do not remember the abuse; others
are aware of the abuse but have avoided thinking about it or seeing
it as significant; still others have just begun or are well along
in their journeys of healing from childhood sexual abuse.
Not all survivors will share the same perspective on the relationship
between their physical and psychological health and past abuse.
Some survivors feel that their physical health and reactions to
treatment are intimately connected with their psychological state.
Others have not made such connections. All of the women who participated
in this research had begun their journeys of healing. They spoke
about the strong links between their physical health and past abuse.
Many described their interactions with health professionals at various
times in their lives: before they had begun to remember past abuse,
before they had begun to see connections between their health and
past abuse, and during or after the development of this awareness.
Thus, the clinician may be working with survivors whose responses
to their past abuse vary greatly.
[Survivors] may not link their health with the abuse or they’re
not at that sort of point in their life. I went a lot of years not
knowing how the abuse affected my body, my life, my emotions, everything,
and now looking back I think maybe if doctors or somebody would
have known that, it would have made a difference.
The Guidelines in all sections other than
Dealing with the client who is upset and Disclosure
of childhood sexual abuse represent a respectful way to work
with survivors and non-survivors alike. The guidelines in these
sections refer specifically to survivors of childhood sexual abuse.
Not every suggestion in the guidelines will apply to every
health profession, to every clinical setting or to every survivor.
Readers are encouraged to develop ways to apply the guidelines
in their own clinical practices.
Readers are also cautioned that the guidelines section of this
handbook is not a “stand-alone” document but, rather,
builds on the dynamics and long-term effects of childhood sexual
abuse and on the Principles of sensitive practice.
17
Handbook on Sensitive Practice for Health Professionals: Lessons
from Women Survivors of Childhood Sexual Abuse
B.
|
Preparation for the initial appointment
1. The right to choose a clinician
and a facility
|
The client has a right to make an informed choice about health
professionals with whom she will work. She also has the right to
request a referral to another clinician or facility if she is not
comfortable with her current situation.
Such options may not be easy or even possible in every situation;
nonetheless, health professionals are encouraged to seek ways to
support this principle.
As noted in the section on long-term effects of childhood sexual
abuse, many survivors are uncomfortable working with men. It is
important for male health professionals to recognize that the survivor’s
discomfort can stem from her past experiences. Frequently, the male
clinician and client are able to build a good therapeutic relationship.
But at times the survivor’s discomfort is too great and cannot
be overcome. How should the clinician proceed? We suggest that every
clinician practise sensitively and be willing to refer to another
practitioner if the client wishes.
- Helping prepare the client for treatment
A written introduction to treatment may help the client to understand
more about the therapeutic process to come. The
Suggestions for Clients at Out-Patient Physical Therapy Facilities
(Appendix C) is such an example. They provide a template which
can be modified for use by health professionals in diverse clinical
settings. In order to consider the literacy level of clients, these
suggestions were drafted using a readability formula.35
This information can be sent to the client before her first appointment,
given to her while she waits for her first appointment, and displayed
in waiting rooms or treatment areas. The information can help to
reduce anxiety at the outset and assist the clinician in beginning
to address some of the survivor’s needs from the first moment
of interaction.
C. Initial evaluation
The following suggestions can be used during the initial clinical
history taking and examination.
•
|
Draft the initial written Informed
Consent in “client-friendly” terms. Avoid technical
terms and use language that assures the survivor that she/he
is viewed as a whole individual (see Appendix D, Sample Consent
Form).
|
•
|
Make sure clients know they can have
someone with them at all times during treatment.
|
| |
–
|
Post this option on signs in the waiting room
and on appointment cards.
|
| |
–
|
Reinforce this option verbally.
|
•
|
Provide the client with the option
of a private room for the initial examination if possible.
|
•
|
Let the client know what the subjective
and objective evaluations involve before you proceed.
|
| • |
Seek verbal consent for each segment
of the evaluation |
| |
18
Guidelines for Sensitive Practice
•
|
Complete the initial medical history
before you ask the client to remove any clothing required
for the physical examination.
|
•
|
Allow enough time for answers during
clinical history taking. Many survivors have learned to ignore
their bodies and may require extra time to articulate a description
of their symptoms.
|
•
|
Seek a balance between offering descriptors
of symptoms (“Would you describe the pain as sharp or dull,
throbbing or aching?”), and encouraging the survivor to
identify and therefore “own” her symptoms.
|
•
|
If the client appears uncomfortable
or is having difficulty responding to one aspect of the subjective
assessment, it may be helpful to move on to another part of
the assessment and return to your previous questions later.
|
•
|
Ensure privacy for undressing and
changing and confirm that the client is ready – knock,
ask if the client is ready, and wait for permission –before
entering.
|
•
|
Before shifting the physical examination
from one area of the body to another, let the client know that
you would like to examine a different area of her/his body and
explain why.
|
•
|
Ensure that the client clearly understands
that she/he can ask you to pause, slow down or stop during the
physical exam.
|
•
|
Ask the client if she/he is comfortable
or ready to continue:
|
| |
–
|
intermittently during the exam;
|
| |
–
|
when shifting the exam from one part of the body
to another; and
|
| |
–
|
if her/his body language indicates discomfort.
|
•
|
Emphasize that you are willing to
be flexible during the evaluation and subsequent treatment to
lessen her discomfort or anxiety.
|
•
|
Offer explanations about the body
and its many connections, especially when examining areas other
than the site of symptoms. Reassure the client that locations
of pain and other symptoms distant from the site of her concern
are quite common.
|
•
|
Ask the client about her best time
of day for appointments before booking additional appointments.
A survivor who has trouble sleeping may wish to choose a time
of day that will maximize her ability to participate in treatment.
|
•
|
See the client, at least briefly,
in a fully dressed state after each session. This reinforces
that the clinician sees the client as a whole person.
|
•
|
Explain the clinician’s and
client’s roles in treatment after examination but before
treatment begins.
|
These suggestions may mean that an initial evaluation will take
longer than anticipated. Taking this extra time may help establish
rapport, trust and safety more quickly and thereby save time in
the long run.
D. Other treatment considerations
The following discussion expands upon some of the suggestions
for initial evaluation and presents additional ideas and suggestions
for clinical practice.
19
Handbook on Sensitive Practice for Health Professionals: Lessons
from Women Survivors of Childhood Sexual Abuse
1. Consent
Consent is a crucial issue for safety. Clinicians are advised
to review the guidelines for consent established by their professional
licensing bodies.
And [the physical therapist] would… tell me, “This
is what I’m going to do,” and she would … show on
herself a little bit, and then she’d ask, “[Are you] comfortable
with this?” And I’d say yes. And so she’d normally
put an ice pack or a heat pack on me and then come back in 15 minutes.
When she came back, right before she was going to [proceed with
further treatment], she’d ask me again, “Are you comfortable
with this? Is everything alright? And do you understand what I’m
doing?” And that was so much easier, because one minute you
can feel comfortable, and the next minute, you could feel uncomfortable...so
she gave me an opportunity that, if I were to change my mind and
feel uncomfortable, all of a sudden, for whatever reason, she would
know, and I’d be able to say something. So I felt like I was
in control, and I did have the say of what was going on.
Consent must be an ongoing, interactive process. Do not assume
that consent given today applies to all successive days: ask for
consent in each successive day of treatment.
- Always ask and receive verbal permission before proceeding with
each component of an examination or treatment each time you see
the client.
- Seek the client’s consent to allow students to observe
or participate in treatment. This should be done as far ahead
of time as possible and without the student present. Explain the
role(s) of the student and whether the student
will be present to observe, treat or both. Remind the client that
she may withdraw her consent to the student’s presence at any
time.
•
|
When using an electrophysical agent (such as
ultrasound and TENS), describe the physiological effects and
what it will feel like. Mention any gels, electrodes, etc.,
that will be used. Ensure that you have obtained verbal consent
for use of the modality after giving the explanation.
2. Language
and communication
|
Language can be used to amplify or minimize the power imbalance
in the therapeutic relationship.
- Avoid overuse of medical terminology: seek with the client a
common language that facilitates both a sense of safety for her
and a sense of professionalism for you.
- Seek a balance in the amount of information offered at one time
– offering too much information to the client may be just
as counterproductive as not offering enough.
- Monitor the client’s body language during treatment and
address with her any apparent discrepancies between verbal and
non-verbal responses.
…we send out signals…to people that we have been
abused…I was sending signals out, and I don’t think the
people were listening really and picking up on them…[I would
]cringe and move and I often said “what are you doing?”
20
Guidelines for Sensitive Practice
•
|
Monitor your own body language. Does your body
language convey the same message that your words deliver? Clients
are very perceptive of your non-verbal cues.
|
•
|
Show your client that you are listening to her.
Active listening is one effective technique to clarify what
the client is trying to say. Through the use of restatement,
reflection and clarification, you are “paraphrasing the
speaker’s words rather than reacting to them in order to
clarify if you have caught the intended meaning.”36,
p. 106
|
•
|
Consider offering a brief written summary of
the treatment session. While this can be time consuming, the
survivor may feel more involved in treatment as a result. Use
of photocopiers or carbon paper can reduce the time required.
3. Clothing
|
Having to undress to undergo treatment may leave the client feeling
vulnerable. Explain the rationale for your preference in clothing
and ask the client about her preference. Agreement on alternative
clothing or providing gowns that do not gape open may increase the
survivor’s feeling of safety and comfort during treatment.
Provide a variety of sizes of gowns and shorts for all body sizes
and ask if your client is comfortable with the options.
Remember, too, that what you wear may also have effects –
although a white lab coat generates a sense of professionalism,
it may increase the perception of the power imbalance and intimidate
some clients.
4. Touch
Touch may be associated with painful memories for survivors. As
a result, many survivors may have difficulty tolerating touch by
health professionals. For some survivors, this may change as trust
develops; for others the discomfort does not decrease.
…[having to go to a physical therapist] kinda bothered
me, because I don’t like to go to a place where people are
going to be touching me...Whether it’s my head or my toe, I
don’t like that…[If I tell them about my discomfort] I
don’t want them looking at me like,“What are you, bonkers?
I’m just touching your head or your foot! Like, no big deal!”….[At]
the thought of going to see somebody that’s going to be touching
me, then I start thinking about my past. And then I really start
stressing out.
Your approach to touch must emphasize the principles of sharing
control and sharing information.
•
|
Describe the touch that is required
during treatment.
|
•
|
It is critical that you ask for consent
to touch throughout a treatment session.
|
| |
–
|
Some clients may want a step-by-step description.
|
| |
–
|
Other clients may be comfortable giving consent
after a description of the whole procedure.
|
But when somebody tells me what they’re doing, and why
they’re doing it, as they’re doing it, then I feel more
comfortable. I’m still feeling a bit uncomfortable because
someone’s touching me.
21
Handbook on Sensitive Practice for Health Professionals: Lessons
from Women Survivors of Childhood Sexual Abuse
•
|
Check with the client if her body language suggests
a negative response to touch.
|
•
|
Always be aware of the physical distance between
the client and yourself during treatment. Avoid being in very
close proximity except when treatment requires it.
|
•
|
Avoid unnecessary physical contact. If treatment
involves bracing part of the client’s body against your
own body, explain this, and seek consent before proceeding.
5. Privacy
|
Addressing privacy needs of the client is another important step
in building and maintaining feelings of safety. The balance between
safety and privacy is not the same for all survivors. Some clients
will be more comfortable in a private room where no one can overhear
them. Some may prefer a private room as long as they can have someone
of their choice present during examination or treatment. Others
will forego privacy because they feel safer in a larger, common
space.
Not all clinical facilities can accommodate the client’s
need for a private room, and this issue should be addressed with
her at the outset of treatment. If an agreeable solution cannot
be found, the survivor’s needs may be better served by referral
to another clinician or facility.
…I felt...uncomfortable [in a curtained cubicle] ’cause
I thought anybody could just open up those curtains at any time…I
found when people would walk by…[and bump…the cubicle,
the curtains would… move, and I didn’t feel as safe or
as if this was my space. I felt like at any time it could be invaded…I
was really vulnerable…You hear everything around…It doesn’t
feel very personal, it doesn’t feel private, it doesn’t
feel safe.
- Post a notice in the reception area offering a private room
to clients if they prefer one.
- Ask the client about her need for privacy. Discuss alternatives
to meet her need for privacy.
- Ask the client to let you know if her need for privacy changes
and check her need for privacy as treatment progresses.
Although options for privacy are more limited in acute care settings,
clinicians are urged to address this issue with the client.
…for [personal parts of treatment]…I was in a real
room with walls and stuff. And that…made me feel more comfortable…It
felt like [the therapist] was acknowledging, “[This] shouldn’t
be shared with every-body…You should have privacy”…That
was really nice.
22
Guidelines for Sensitive Practice
- Other environmental considerations
Control over the environment is important for many survivors.
- Take the time to familiarize the client with the treatment area.
- Many survivors are most comfortable when they can see or be
near the door.
- Knock or announce yourself – and await permission –
before entering a client’s space.
- Offer secure storage of clothing if disrobing is required and
treatment is carried out at a distance from where the client has
undressed.
- Some clients may feel more comfortable if they bring along a
small familiar object that symbolizes safety and security. Avoid
being judgemental about such a coping technique.
- Identify separate men’s and women’s washrooms, wherever
possible.
Some survivors are strongly affected by lighting, floors and ceilings.
•
|
Ask the client about her comfort
level:
|
| |
–
|
with the lighting available in your facility.
|
| |
–
|
when she must assume a position facing the floor
or ceiling.
|
•
|
If problematic, explore alternatives
with her.
|
If your facility does not offer the environment your client needs
to feel safe, explain and give her the option of a referral to a
clinician in another facility.
7. Issues related to pain
Pain is a complex issue that is often difficult for both the survivor
and health professionals to sort out. Acute and/or chronic pain
may be complicated by past abuse. While “psychological distress
can find somatic expression,”37, p. 143 researchers
are also learning more about the long-term impact of trauma on the
physiological responses to stress that can also contribute to the
survivor’s pain.
Remember that:
- Some survivors may respond to pain by ignoring it, not taking
it seriously or dissociating when they experience pain.
- Some survivors may not feel pain.
- The survivor may experience pain associated with body (somatic)
memories as part of, or in addition to, other problems for which
she seeks your clinical expertise.
- The survivor may have had negative experiences with health professionals
who discredited her pain because it did not seem to match test
results or examination findings. Regardless of whether pain matches
examination findings, the client’s experience of pain is
real.
It is the clinician’s responsibility to address the client’s
pain, other symptoms and problems, in a systematic, non-judgemental
and thorough manner. The clinician needs to set realistic goals
with the client and work systematically toward these goals.
23
Handbook on Sensitive Practice for Health Professionals: Lessons
from Women Survivors of Childhood Sexual Abuse
Despite thorough exploration of all the treatment options within
a clinician’s scope of practice, there will be clients whose
pain the clinician is unable to resolve. If pain is not resolved
satisfactorily, it is the clinician’s responsibility to explain
that treatment options have been exhausted and to discuss other
options outside the clinician’s scope of practice.
- Document what you and the client said during such a discussion.
This record may be helpful if you see the client again at a later
time.
- Leave options for further consultation open.
- Consider joining or creating a health care team that will work
with the client to address the problem.
Consider referrals to clinicians or clinics that specialize in
the management of chronic pain and to other professionals who may
specialize in positioning, energy conservation, fitness, massage,
etc. Under some circumstances, the clinician may suspect that the
client’s problem is related in part to psychosocial issues
that are outside that clinician’s scope of practice. The clinician
can discuss this with the client and refer her for counselling.
Rehabilitation often follows a functional model rather than a
symptomatic model of treatment. In rehab, the client is asked to
disregard “reasonable symptoms in the absence of objective
signs of harm” in order to develop the functional tolerances
required to return to pre-injury employment and/or lifestyle. Survivors
participating in rehabilitation may require additional education
regard-
ing the phases of tissue healing and assistance in interpreting
the symptoms associated with “hurt” vs. “harm.”
8. Time factors
There are many time pressures on health professionals in today’s
health care system. While it is challenging for the clinician to
find the balance between time constraints and good care, it is important
to recognize the potentially grave consequences for the survivor
when the clinician is rushed. Treatment may feel very depersonalized,
robbing the survivor of her sense of safety. Without this sense
of safety, treatment is much less likely to be successful.
…[having enough time for the client]… doesn’t
happen very often with medical people. They gotta get on to the
next appointment all the time.You’re scheduled for your half-hour
and that’s it. And so maybe it means that the very first appointment
[should be]…a longer appointment, so that someone can relate
a bit before this person’s touching your body…
- Discuss time pressures with the client in order to plan how
best to meet her needs.
- Because of ambivalence about her body, it may take longer for
the survivor to develop the confidence to carry out an ongoing
independent program of self-management. A number of follow-up
appointments (scheduled, for example, at monthly intervals) may
be helpful.
24
Guidelines for Sensitive Practice
- Control and adherence to treatment
There [were] some of the exercises…that they wanted me
to do [after a total hip replacement]…And one of them that
I still today cannot do…You lie on your side... it’s a
scissor…[Even when the physical therapist] had the sling…around
my ankle and it had a handle and I could pull it and my leg would
go up, I couldn’t even do that. I’d get it so far, but
I wouldn’t go any further because I had to keep [my legs] so
tight…[and the physical therapist] got frustrated, she really
did.…she thought I wasn’t trying, and that wasn’t
true at all because I was doing the other [exercises] very well…
Difficulties with treatment adherence may be linked with past
abuse. Some survivors may be out of touch with their bodies and
have difficulty identifying signs of over-exertion or other body
signals. Others may perform too many exercises, perhaps in an attempt
to gain control over their bodies, to please the clinician or as
a form of self-harm. Some may have difficulties with certain actions
or body positions because of associations with past abuse. The following
suggestions may help the client achieve a desired level of adherence.
- Include a daily check-in before each treatment.
- Respond to the feedback before you proceed with treatment: come
up with alternatives together to avoid parts of treatment that
she finds difficult to tolerate.
- Explain the rationale for treatment.
- Discuss adherence difficulties with the client. Do not use blame
and guilt as tools to achieve adherence. Avoid using words such
as must and should. Rephrase objectives using comments
such as “do the best you can do.”
- Problems with adherence are often very pressing in acute care
settings. After surgery, for example, early mobilization can be
critical to recovery, but pain may overshadow such goals. The
clinician may be tempted to achieve adherence by using the language
of “must” and “should.” However, encouraging
the client to refocus on her initial goals of treatment may be
more effective in facilitating adherence.
- In out-patient or home care settings, the clinician may encourage
adherence by working with the client to structure the treatment
differently so that it fits the client’s life and lifestyle
better.
When incorporating exercise and activity into treatment:
- Offer clear and direct guidelines for exercise programs.
- Offer written and oral instructions that include what each exercise
should feel like.
- Give upper and lower limits for the number of repetitions and
sets to be done.
- Develop and progress through an exercise program slowly to allow
the client to build the neuromuscular skill required.
25
Handbook on Sensitive Practice for Health Professionals: Lessons
from Women Survivors of Childhood Sexual Abuse
•
|
Describe signs and symptoms of overuse to the
client and monitor the exercise prescription for signs of overuse.
|
•
|
Encourage the client to keep an exercise or treatment
log.
|
•
|
Encourage the client to view the home treatment
program as a tool she can use to care for herself.
10.
Encouraging reconnection with the body
|
[One part of treatment is] how healthy it has been for me to
start to get in touch with my body...I think that a physiotherapist
can really affect that [by giving] that supportive invitation to…come
back into their own body…I think it would make a big difference…
Herman4 suggests that part of a survivor’s healing
is reconnecting with her body. Health professionals may have a role
in this process.
- Some survivors have difficulty recognizing or interpreting physical
sensations and reactions to treatment. She may need to learn to
recognize and interpret sensations such as muscle fatigue, stretching
within reasonable limits, tension, relaxation, the reaction of
a joint to over-exertion, etc.
- Incorporate visualization of the exercise and sensations expected
during exercise. This may help the survivor develop the kinesthetic
sense needed before she begins to actually perform the exercise.
•
|
Use breathing exercises, yoga and relaxation
techniques.
|
•
|
If you know that you are working with a survivor
who is seeing a counsellor, you may want to offer to work jointly
with the client and her counsellor.
11. Encouraging
and modelling self-care
|
Taking care of one’s self – eating well, getting enough
rest, performing regular physical activity, taking time to relax,
etc. – can be challenging for many of us. Health professionals
can model self-care and encourage the survivor to develop strategies
for her own self-care. If the client has difficulty maintaining
self-care behaviours, she may appreciate knowing that she is not
alone!
12. Problem solving
When a client has difficulty with a treatment you suggest, explore
different strategies to attain the therapeutic goals. Be respectful
and non-judgemental when discussing alternatives to address the
problem for which she sought your expertise.
If you feel that your authority has been challenged, engage in
a dialogue instead of becoming defensive. Offer treatment options.
These may include treatments that you recommend, and treatments
for which you feel the goals will take longer to achieve or which
are not as effective but might be more acceptable to the client.
26
Guidelines for Sensitive Practice
13. Continuity of care
Switching clinicians without prior discussions with the client
can result in a feeling of a violation of established trust and/or
of the treatment contract.
•
|
If you know that you are going to be away from
work, give the client as much notice of your anticipated absence
as possible.
|
•
|
Discuss alternatives with the client; recommend
a colleague who is informed about, and sensitive to, survivor
issues.
|
•
|
Introducing the client to the clinician who is
covering your caseload would also be helpful.
|
•
|
If you practise alone, discuss the practical
aspects of your absence with the client.
|
•
|
Whenever possible, for unexpected absences, the
survivor should be notified and given a choice of whether to
attend an appointment with an alternate clinician.
E.
Dealing with the client who is upset
|
[On] the second visit, again, I had to lie on the table …[the
therapist] didn’t warn me and all of a sudden…I heard
the whirring and he raised the table and [I found myself] coming
toward the ceiling. I just felt attacked. But I kept it inside and
didn’t tell him what was happening. But I didn’t go back.
That was just too much.
Treatment may “trigger” the client to relive past abuse
(flashback) or to experience an overwhelming emotional response.
Such reactions may occur regardless of whether or not the survivor
has disclosed past abuse to you or even remembers past abuse.
Thus, this section applies both to those survivors who have disclosed
past abuse and to those who have not disclosed but appear very uncomfortable
or upset during treatment.
1. Identifying triggers
There is no complete, predictable list of triggers for
all survivors. Touch is frequently described as a trigger. Traction
and electrophysical agents such as TENS, ultrasound and interferential
current may also act as triggers.
Some survivors may be able to identify their triggers while others
may be unaware of their triggers.
[During] my first experience [in physical therapy], they didn’t
have any Kleenex, and the minute [the therapist started] touching
me I just started sobbing, without having any idea of… why…
- Recognizing body language that may indicate discomfort,
triggering, dissociation
Some survivors describe body language that communicates a high
level of discomfort:
27
Handbook on Sensitive Practice for Health Professionals: Lessons
from Women Survivors of Childhood Sexual Abuse
- pulling away
- shaking
- startling
- muscle tension and inability to relax
- sudden strong emotional reactions (such as tears).
Survivors have described many different physical reactions to
being triggered. Some of these may be understood as physiological
reactions to stress:
- shallow, rapid breathing, breath holding or a change in breathing
pattern
- rapid heart rate
- decreased concentration level.
A client who has been triggered may dissociate. If your client
is in a dissociative state, she may seem:
- distant
- unable to focus
- uninvolved in the present.
Once present after she has dissociated, the client may ask questions,
such as: “Where was I? What did I just say? What just happened?”
- Managing triggers and dissociation
…now, [clinicians] don’t have to handle the [whole]
crisis, but they do need to know how to recognize [it]. And how
to make a referral in a nice way…[by saying, for example] “Do
you see your counsellor tomorrow?” or “Is there someone
you can talk to?” They would definitely have their scope and
they wouldn’t need to go beyond that. But if they can recognize
what can happen when a woman is going through a flashback…How
to ground a person. It’s not hard...You know, just basic humanity
and reassurance. You know, “you’re okay, it’s safe
here.” Or [validating] the energy and the courage that it takes
to go through physio…And “yes, [physical therapy] can
trigger memories, and it can be really disturbing and distressful,
and what you’re feeling is normal.”
The goals of this section are 1) to provide information that will
help the clinician be a supportive ally and 2) provide the clinician
with ways to ensure that the client does not leave the session feeling
disoriented or embarrassed about her reactions to treatment. The
information in this section is not intended as instruction in counselling
techniques.
Regardless of whether you know that your client is a survivor
or not, if she demonstrates body language that indicates great discomfort,
stop immediately and inquire.
•
|
If a client has been triggered, stop
treatment immediately and try to help ground her in the present.
|
| |
–
|
Let her know where she is.
|
28
Guidelines for Sensitive Practice
| |
–
|
Reassure her that she is in a safe place now.
|
| |
–
|
Encourage her to take slow, deep breaths.
|
| |
–
|
Encourage her to sit up and put her feet on the
floor.
|
| |
–
|
Ask her to look at you and keep you in focus.
|
| |
–
|
Ask how she is feeling.
|
•
|
Avoid touch.
|
•
|
Continue to talk to her and reassure
her, using a calm voice, but do not bombard her with questions.
|
•
|
If the client has disclosed past
abuse, let her know that treatment can sometimes trigger flashbacks
or emotional responses and that this is not uncommon.
|
•
|
If your client has experienced a
strong emotional reaction, reassure her that it is okay to be
angry, sad or afraid (or whatever she is feeling).
|
•
|
If the client has dissociated:
|
| |
–
|
Ask her to keep her eyes open and to look at
you and around the room.
|
| |
–
|
Pose questions calmly and slowly: For example:
Are you here? Are you with me? Are you following me? Do you
have any techniques for staying present?
|
Once your client appears less upset or more present, speak to
her about what has just occurred:
- Give her the necessary time and space to recover from her experience.
A quiet room may be helpful.
- Do not ask for details of her abuse that contributed to her
being triggered.
- Acknowledge that people sometimes react to circumstances in
the present that remind them of past experiences.
- Ask her what she needs right now: Does she want company, or
to be left alone?
- Ask her whether she feels able to continue the treatment session.
Being triggered can be a frightening or bewildering experience.
Your client may benefit from talking to someone within her circle
of support about the experience.
- Remind her that her reaction is not uncommon and that it is
understandable and okay.
- Ask whether she has someone with whom she feels comfortable
talking about the experience after her appointment with you. This
may be a friend, family member or counsellor.
- If she would like to explore what has happened further but has
no one to talk with, refer her to a counsellor or other resources
in your community (such as the sexual assault centre).
- You may want to remind her that you can be a good listener,
but that you are not trained to be a counsellor.
If time constraints mean that you are unable to help an upset
client as fully as you would like, explain this and ask if someone
else can help. (This might be another staff member or a friend whom
you could call for her.)
29
Handbook on Sensitive Practice for Health Professionals: Lessons
from Women Survivors of Childhood Sexual Abuse
4. After the experience
The client may feel very vulnerable after being triggered. It
is important to discuss the experience with the client the next
time you see her to ensure that she is alright and reassure her
that you are not judging her actions or responses.
- Work with your client to identify what you can avoid or modify
in the future to avoid triggers. Focus your inquiries on treatment
rather than on the flashback or emotions during the experience.
- Ask the client if she has any techniques for staying present
and work with her to outline a strategy for the future.
Remember that while there will be instances in which your client
is able to identify the trigger, there may also be times when she
is unable to identify the cause of her reaction.
If you find that you are upset because of what has happened, reassure
the client that she has done nothing wrong. At a later time, you
may benefit from discussing your reactions to the events with someone
within your support system. This can be done without breaching confidentiality
(see Taking Care of Yourself, page 37).
- Working with survivors who have Dissociative Identity
Disorder
We recommend working with a multidis-ciplinary health care team
to assist the client who has disclosed Dissociative Identity Disorder.
If the client agrees, consult those practitioners with whom she
is already working, to determine how you can work collaboratively.
- Disclosure of childhood sexual abuse
1. Introduction
This discussion is based primarily on the experiences of survivors
working with physical therapists who often see clients for relatively
short periods of time and for specific problems. The components
of this discussion of disclosure also apply to a broad range of
health professionals who may see clients over longer periods of
time.
2. What is disclosure?
In its broad sense, disclosure refers to the survivor’s telling
the clinician that she was sexually abused as a child. The identification
of sensitivities and discomfort specific to treatment represents
a more limited form of disclosure that we call “task-centred
disclosure.”
3.
|
Clinician-initiated inquiries
a. Task-centred inquiries
|
The clinician should begin to inquire about the client’s
task-centred sensitivities and discomforts during the initial examination.
The information that the survivor reveals (such as problems tolerating
touch, certain body positions, etc.) is highly relevant to treatment.
This information should be applied during subsequent examinations
and treatment to facilitate feelings of safety. Such task-centred
disclosure focuses on the client’s sharing of specific information
that is immediately pertinent to the treatment without revealing
other personal information she is not prepared to share at that
time.
30
Guidelines for Sensitive Practice
Inquiries can take the form of a combination of close-ended and
open-ended questions. An example of a close-ended question before
beginning an examination of the lower limbs is, “I would like
to examine your legs now. Do you have any sensitivity to having
your legs touched?” Including an open-ended question at the
end of the initial appointment such as, “Is there anything
else you feel I should know before we begin?”, may allow the
client to share anything she considers relevant to the therapeutic
relationship but has not been specifically asked about.
Inquiries about sensitivities and discomforts can also be made
using questionnaires. Some survivors may be more comfortable with
this written approach. If a questionnaire is used, the client can
be given a choice about completing the questionnaire independently
or with the clinician.
While the clinician should initiate such inquiries during the
initial examination, she or he must be aware that the survivor may
choose to reveal sensitivities and discomforts only as treatment
progresses. The survivor may choose to disclose only after getting
to know the clinician and making her own assessment about whether
the clinician is a trustworthy person. Therefore, the clinician
cannot assume that the client has made all task-centred disclosures
early in treatment and must continue to inquire about difficulties
and follow up on non-verbal indicators of discomfort throughout
treatment.
b. Inquiries about past abuse
In some types of clinical practice, health professionals believe
that knowing that the client has a history of abuse will enable
them to better facilitate the
client’s safety and comfort and maximize treatment effects.
If asked about past abuse, the survivor may choose to disclose or
may take time to decide whether the clinician is trustworthy and
whether she feels safe enough to disclose.
- Survivor-initiated disclosure of past abuse
Some survivors feel that disclosing past abuse to the clinician
is important because of the impact of the abuse on their health
or their reactions to treatment. They may look for ways or times
to disclose to the clinician. One of the things that may hold the
survivor back is uncertainty about the clinician’s response
to a disclosure of childhood sexual abuse.
I didn’t know how they were going to react or if they
would shy away from it, or if that’s something they wanted
to hear. So I would tell them all the other stresses... that’s
one thing I got really frustrated about because I wanted to say
something, but I wasn’t sure on how or if that’s what
they wanted to hear.
Previous experiences with disclosure may also play a major role
in the assessment of whether the situation feels safe enough to
disclose.
I wasn’t feeling safe enough or I wasn’t sure, because
I’ve had experiences before where I have mentioned it, and
someone has just freaked out or else they’ve looked at me like
I’m from a different planet, like what am I doing even sharing
this with them? So I’m really hesitant on mentioning it to
people, especially in the health professions. I don’t want
to start talking about it or mention it, and get that rejection.
Cause that’s the worst.
31
Handbook on Sensitive Practice for Health Professionals: Lessons
from Women Survivors of Childhood Sexual Abuse
Thus, the clinician’s response to disclosure is very important
to the survivor.
- What should I say when someone discloses?
Well, for one thing, it’s really important [that the clinician
tell the survivor]… that you believe them, because this might
be the first person they’ve told. And also, it’s really
important to accept them as a person. You can say whatever your
real feelings are…“I’m really sad to hear that.”
It is important to offer appropriate verbal and non-verbal responses
to disclosure. The basic elements of appropriate responses are as
follows.
•
|
Acceptance of the information
(that is, letting the survivor know that you heard her words)
|
| |
–
|
Offer an expression of understanding
and support. For example:
|
| |
•
|
“I’m sorry that happened to you.”
|
| |
•
|
“Tell me how I can help you during your
time with me.”
|
•
|
Acknowledgement of the prevalence
of abuse Acknowledging your awareness of the prevalence
of abuse has the effect of reducing shame. You might say:
|
| |
–
|
“We know that at least 1 in
3 to 5 women (or 1 in 7 to 10 men) are survivors of childhood
sexual abuse. It is a terrible thing that so many children have
suffered in this way.”
|
•
|
Validation of your belief in the
survivor’s words and the consequences of the abuse for
her
|
| |
–
|
Validate the courage that it took to disclose.
|
| |
–
|
If your client is visibly distressed, acknowledge
it. “I see that this is painful (distressing, disturbing)
for you right now. What can I do to help?”
|
| |
–
|
Let her know that you do not think she was responsible
for the abuse.
|
Allow the survivor control over the timing and extent of her disclosure.
If you are under time constraints, find a way to inform the client
of this so that she will not feel dismissed or think she has done
something wrong by disclosing.
Canadian law in most provinces requires that suspected abuse of
children (under the age of 16) be reported to child welfare officials.
There is no legal obligation for you to report disclosure of past
abuse by an adult survivor to child welfare officials unless the
client also reveals current abuse of a child.
- What should I NOT say or do when someone discloses?
[Sometimes] someone [will start] to disclose [and professionals
will say] “you don’t have to tell me this if you don’t
want to.”…People who are really nervous about hearing
[a disclosure] keep saying that, and it gives the message “I
don’t want to hear this.”
32
Guidelines for Sensitive Practice
If a client discloses:
- do not remain silent, as you may be perceived as ignoring the
client’s words; and
- avoid an overwhelming response, loaded with a list of directive
statements (“shoulds”).
I told the physical therapist about my history of abuse. She
didn’t acknowledge [it]… She just kept right on going
with what she was doing… Oh boy! If somebody says it, then
you’ve got to acknowledge it. Because then what that says to
me, is that it’s not valid, it’s not important, it doesn’t
have anything to do with us.
In addition, DO NOT:
- offer pity (e.g., “Oh, you poor thing”)
- offer insincere concern
- tell the client to “Look on the bright side”
- dwell on the negative
- smile (While you may think your smile conveys compassion, a
neutral or concerned expression is more appropriate.)
- touch the person without permission even if you intend it as
a soothing gesture
- interrupt (Let the client finish speaking.)
- try to say something that will “fix it”
- say anything that invalidates her decision to disclose or her
experiences of abuse (e.g. “Don’t tell anyone about
it.” “But don’t you think your parents did the
best they could?”)
- tell the person to forget about it (e.g. “Put it behind
you.” “Get over it!” or “Don’t dwell
on the past.”)
- minimize the potential impact of past abuse (e.g. “I know
a woman that this happened to and she became an Olympic gold medalist.”
“Let’s just concentrate on your back pain.” “What’s
that got to do with your sprained ankle?”)
- ask intrusive questions that are not pertinent to treatment
- talk about yourself, your experiences, or someone else’s
experiences
- disclose your own history of abuse
- give the impression that you know everything there is to know
on the subject.
…don’t push the person and be really aware not to
use the “shoulds”, like “you should call the crisis
line”…or “are you seeing a therapist?”
7. After a client has disclosed
The survivor may feel more vulnerable and exposed after disclosure.
Reassure her that:
- disclosing was not wrong,
- you respect her,
33
Handbook on Sensitive Practice for Health Professionals: Lessons
from Women Survivors of Childhood Sexual Abuse
- you respect her decision to disclose as well as the information
that she revealed, and
- you will respect her confidentiality.
The client may still feel more vulnerable the next time you see
her. It may help to repeat these points again briefly at her next
appointment.
It is also important to talk with the client about how she feels
her past abuse may affect her response to treatment. Explore practical
issues within treatment. For example, “Is there anything about
treatment that we should change to make you more comfortable?”
and “As we proceed with treatment, please tell me if I am doing
anything that doesn’t feel right to you.” You may have
to balance the importance of taking time to discuss disclosure with
the client versus either beginning or continuing treatment. Discussing
the implications of disclosure on treatment will take additional
time but is likely to increase a survivor’s feeling of safety
in future treatment.
After disclosure, it is important to clarify what the survivor’s
expectations of the clinician are. Some survivors hope for, or expect,
a response that is beyond the clinician’s ability or scope
of practice. It is therefore important to delineate clearly what
your scope of practice is, and identify your clinical abilities
and limitations. If you feel the survivor requires help beyond your
scope of practice, suggest additional resources (see page 36). Focusing
on what treatment involves and can achieve and on how to best work
with the survivor’s sensitivities provides both the clinician
and client a solid basis from which to proceed with treatment after
disclosure.
G.
|
Health care records
1. Confidentiality
of records
|
While health professionals consider client charts confidential,
it is important to recognize the meaning and limitations of confidentiality
in each clinical setting. A client should be made aware of the level
of confidentiality that applies to her health care record. She should
be told:
- who has access to her chart within the health care setting both
in the present and future;
- that her record(s) can be released to other individuals only
with her consent; and
- that her records will be released when required by law.
When charting, the clinician should be mindful of the limits
of the confidentiality of the health care record.
2. Some issues in documentation
If the client has an unexpected reaction to treatment or to the
clinician, the clinician is advised to chart the events in as much
detail and as objectively as possible, as soon after the incident
as possible. Include the words and actions of the client, the clinician
and any other staff involved. The same advice is appropriate when
the client expresses discomfort with anything professionals do or
do not do.
Task-centred disclosures can be documented in a way that allows
for the identification of specific sensitivities or discomforts
without revealing the abuse history. Charting in this manner allows
34
Guidelines for Sensitive Practice
for communication of relevant information to other clinicians
without revealing more than the survivor is comfortable with. In
determining what and how much information to include in a client’s
record, the clinician should be guided by his or her assessment
of what notes are needed in order to provide the best service to
the client.
Documentation of abuse may have legal implications for the client
who is (or may in the future be) involved in a court case. This
may occur, for example, if the client chooses to proceed with criminal
charges or a civil action against an abuser or in relation to civil
litigation after a motor vehicle accident. These are a few of many
possible instances when health records may be subpoenaed. In some
instances, the records will be sought to support the client’s
case; in other instances, the records will be sought to try to challenge
the client’s credibility or the client’s account of events.
An in-depth discussion of the legal implications of health records
is beyond the scope of this handbook. The clinician is advised to
seek legal advice in any situation in which a client’s health
records are requested by a third party in the absence of the client’s
consent. A clinician should not release confidential records at
the request of the police or a lawyer without the client’s
consent. If records are subpoenaed, the clinician should seek the
advice of a lawyer. Subpoenaed records should not be released until
a court orders their release, usually following a hearing on this
issue.
Health professionals are advised to familiarize themselves
with current policies on maintenance of health care records issued
by their professional licensing bodies and by organizations with
whom they are affiliated.
H. Discharge
Many survivors have experienced feelings of abandonment, rejection
and subsequent shame in childhood that are carried forward into
adulthood. Under some circumstances, being discharged from treatment
may leave a survivor feeling as though the clinician is rejecting
her or minimizing her problem. The clinician can do several things
to help the client with closure.
•
|
Discuss discharge during the first
appointment, as part of the introduction to treatment. As treatment
progresses, raise the issue of discharge again to ensure that
the client’s needs are addressed.
|
•
|
Plan the timing and other details
of discharge with the survivor as far in advance as possible.
|
•
|
Review initial goals with the client
and ask about other goals that the client now has as the end
of treatment draws nearer.
|
•
|
Consider a follow-up appointment,
telephone call or email exchange 6 to
|
| |
8
|
weeks after regular treatment has stopped.
|
•
|
Leave the door open for the client
to return in the future if her condition worsens.
|
35
Handbook on Sensitive Practice for Health Professionals: Lessons
from Women Survivors of Childhood Sexual Abuse
I.
|
Other suggestions to assist both client and
clinician
1. Community resources
and counselling
|
It is important to reinforce that clinicians need not be all
things to all people. In treating the whole person, the clinician
should offer to assist the client to locate and access additional
community resources.
•
|
Get to know your community resources.
You can start by contacting:
|
| |
–
|
your local Sexual Assault Centre
|
| |
–
|
women’s centres
|
| |
–
|
family service agencies
|
| |
–
|
community mental health centres.
|
•
|
There may be other useful agencies
in your community. Ask your sexual assault centre or women’s
centre about other agencies that work with survivors.
|
•
|
When you call such agencies or organizations
to inquire about survivor services, ask:
|
| |
–
|
What types of services does the agency offer
to survivors (e.g. crisis intervention, individual counselling,
group therapy, support groups)?
|
| |
–
|
What do the services cost? Are services free
or on a fee-per-service basis? Does the agency have a sliding
fee scale in place?
|
| |
–
|
Does the agency usually have a waiting list?
If so, how long is the usual delay?
|
•
|
Prominently display posters and brochures
on abuse, with help-line numbers, such as:
|
| |
–
|
sexual assault centres often staff a 24-hours-a-day
crisis line
|
| |
–
|
battered women’s shelters, and
|
| |
–
|
mobile crisis units.
|
•
|
Locate and display good reference
materials.
|
| |
–
|
The local sexual assault centre may have a good
bibliography of resource materials that you can make available
to clients.
|
| |
–
|
The National Clearinghouse on Family Violence
has many resources.
|
Telephone: 1 800 267-1291 (613) 957-2938
Fax:
(613) 941-8930
http://www.phac-aspc.gc.ca/nc-cn
- Ask the staff of your local sexual assault centre if they maintain
a current list of counsellors, doctors and other health professionals
who deal sensitively with adult survivors of childhood sexual
abuse. If they do, you will be able to suggest that your client
contact the centre for such recommendations.
- Be careful not to give too much information about resources
at one time.
- Inquiring about whether your client is seeing a counsellor is
sometimes difficult. Your client may interpret this as silencing
or as a message that you think she is “not okay.” It
may be easier and less offensive to ask whether the client has
a support system that she can draw upon. This may also allow you
to raise the issue of counselling with greater ease.
36
Guidelines for Sensitive Practice
I think [physical therapists] have to know who the good [counsellors]
are that are gonna believe [survivors]. I think that…medical
people have to be very, very responsible in who they refer people
to…[someone] who understands the role that violence plays in
the lives of women and children. I think that’s critical…
•
|
Under some circumstances, the clinician may believe
that it would be helpful to the client to work on psychosocial
issues at the same time that she pursues treatment focused on
the body. This can be raised in such a way that the client begins
to consider that the physical condition may be compounded or
exacerbated by past experiences.
2. Taking
care of yourself
|
The understanding and compassion we have for our clients must
be extended to ourselves. One cannot always be prepared for what
happens during clinical practice! Every clinician needs to develop
strategies to address difficult events that occur with clients.
It is also crucial to remember that our comfort level for managing
difficult situations is never constant, even for the experienced
clinician.
You may benefit from the support of a colleague or counsellor
to process your reactions to a disclosure or a client’s emotional
reaction in treatment. This can and must be done without breaching
confidentiality. You can discuss your reactions to the event
without disclosing details about the survivor. Ignoring your discomfort
is not recommended. You may end up wanting to avoid the client,
and this may leave her feeling that she has done something wrong.
You are not expected to be the survivor’s primary source
of support. Many sexual assault centres can offer in-person training
or support if you need assistance in clarifying your roles and responsibilities.
- Consultation with other health professionals
Your client may be willing to have you speak with a physician
or counsellor with whom she is working. Such consultation can help
you feel more comfortable in your work with the client and may be
more effective than treating the client in isolation.
I think that we’re talking about really long-term partnerships
with a number of medical people...maybe a physiotherapist, a psychotherapist,
a family doctor.We need these nuclei of support, and they need to
be in touch with each other, and I have that, so I feel like I have
a network of support.
- The clinician’s contribution to the survivor’s
healing
The violations of childhood sexual abuse can result in disempowerment
for the survivor and disconnection from others.4 Recovery,
concludes Judith Herman (a psychiatrist and researcher), is based
upon the survivor’s empowerment and reconnection with herself
and others.4
While you are not a psychotherapist, you can make a significant
contribution to a survivor’s healing as an ally to her.
37
Handbook on Sensitive Practice for Health Professionals: Lessons
from Women Survivors of Childhood Sexual Abuse
Health professionals can:
- help to establish a connection between the survivor and themselves
through the creation of a safe, trusting therapeutic relationship;
- facilitate a reconnection between the survivor and her body;
and
- facilitate her empowerment by encouraging the survivor to become
an active participant in her health care.
So, what we have is a relationship of… mutual give and
take… [the clinician] gives me a lot of responsibility, I give
her a lot of information, we negotiate how best to work [together]
to help me to fulfil my needs and to let me have power over my own
life.
38
V. Concluding Comments
This handbook does not include all possible ways in which
health professionals can be sensitive to survivors, nor does it
include all of the ways that childhood sexual abuse may affect
a client’s experiences in treatment. We each bring different
styles, personalities and life experiences to our work. There is
no recipe for handling every set of circumstances. It is hoped that
this handbook will provide health professionals with knowledge of
childhood sexual abuse and ideas about how health professionals
can work with survivors that are both sensitive and within the professional’s
scope of practice.
39
References
1 Finkelhor, D. (1994). Current information on the scope
and nature of child sexual abuse. Future of Children, 4,
31–53.
2 Rothstein, J. M. (1999). The sensitive practitioner. Physical
Therapy, 79, 246–247.
3 Blume, E. S. (1990). Secret Survivors. New York:
Ballantine Books.
4 Herman, J. (1992). Trauma and recovery. New York:
Basic Books.
5 Schachter, C. L., Stalker, C. A., & Teram, E. (1999).
Toward sensitive practice: Issues for physical therapists working
with survivors of childhood sexual abuse. Physical Therapy,
79, 248–261.
6 Teram, E., Schachter, C. L., & Stalker, C. A. (1999).
Opening the doors to disclosure: Childhood sexual abuse survivors
reflect on telling physical therapists about their trauma.
Physiotherapy, 85, 88–97.
7 Stalker, C. A., Schachter, C. L., & Teram, E. (1999).
Facilitating effective relationships between survivors of childhood
sexual abuse and health professionals: Lessons from survivors who
have received physical therapy.
Affilia: Journal of Women and Social Work, 14, 176–198.
8 Badgley, R. (1984). Report of the federal committee
on sexual offenses against children and youth. Ottawa: Canadian
Government Publishing Centre.
9 Bagley, C. & Ramsay, R. (1985). Sexual abuse in childhood:
Psychosocial outcomes and implications for social work practice.
Journal of Social Work and Human Sexuality, 4, 33–47.
10 Briere, J. N. (1992). Child abuse trauma: Theory and
treatment of the lasting effects. Newbury Park: Sage.
11 Finkelhor, D., Hotaling, G., Lewis, I. A.,
& Smith, C. (1990). Sexual abuse in a national survey of adult
men and women: Prevalence, characteristics, and risk factors. Child
Abuse and Neglect, 14, 19–28.
12 Sgroi, S., Blick, L. C., & Poter, F. S. (1982). A
conceptual framework for child sexual abuse. In S. Sgroi (Ed.),
Handbook of Clinical Intervention on Child Sexual Abuse (pp.
9–37). Massachusetts: Lexington Books.
13 Jones, D. P. H. (1991). Ritualism and child sexual abuse.
Child Abuse and Neglect, 15, 163–170.
14 Finkelhor, D., Williams, L., & Burns, N. (1988). Nursery
Crimes: Sexual abuse in daycare. London: Sage.
15 van der Kolk, B. A. (1996). The body keeps the score: Approaches
to the psychobiology of posttraumatic stress disorder. In B. A.
van der Kolk, A. C.
McFarlane, & L. Weisaith (Eds.),
Traumatic Stress. The Effects of Overwhelming Experiences on
Mind, Body, and Society (pp. 214–241). New York: The Guilford
Press.
41
References
16 Finkelhor, D. (1990). Early and long-term effects of child
sexual abuse: An update. Professionals Psychology: Research and
Practice, 21, 5, 325–330.
17 Braun, B. G. (1988). The BASK model of dissociation. Dissociation,
1, 4–23.
18 Springs, F. E. & Friedrich, W. N. (1992). Health risk
behaviors and medical sequelae of childhood sexual abuse.
Mayo Clinic Proceedings, 67, 527–532.
19 Schofferman, J., Anderson, D., Hines, R., Smith, G., &
Keane, G. (1993). Childhood psychological trauma and chronic refractory
low-back pain.
Clinical Journal of Pain, 9, 260–265.
20 Harrop-Griffiths, J., Katon, W., Walker, E., Holm, L.,
Russo, J., & Hickok, L. (1988). The association between chronic
pelvic pain, psychiatric diagnoses, and childhood sexual abuse.
Obstetrics and Gynecology, 71, 589–594.
21 Reiter, R. C. & Gambone, J. C. (1990). Demographic
and historic variables in women with idiopathic chronic pelvic pain.
Obstetrics and Gynecology, 75, 428–432.
22 Walker, E., Katon, W., Harrop, G. J., Holm, L., Russo,
J., & Hickok, L. R. (1988). Relationship of chronic pelvic pain
to psychiatric diagnoses and childhood sexual abuse. American
Journal of Psychiatry, 145, 75–80.
23 Scarinci, I. C., McDonald, H. J., Bradley, L. A., &
Richter, J. E. (1994). Altered pain perception and psychosocial
features among women
with gastrointestinal disorders and history of abuse: A preliminary
model.
American Journal of Medicine, 97, 108–118.
24 Domino, J. V. & Haber, J. D. (1987). Prior physical
and sexual abuse in women with chronic headache: Clinical correlates.
Headache, 27, 310–314.
25 Felitti, V. J. (1991). Long-term medical consequences
of incest, rape, and molestation. Southern Medical Journal,
84, 328–331.
26 Golding, J. M. (1996). Sexual assault history and limitations
in physical functioning in two general population samples. Research
in Nursing and Health, 19, 33–44.
27 Bloom, S. L. (1997). Creating Sanctuary: Toward the
Evolution of Sane Societies. New York: Routledge.
28 Allen, J. G. (1993). Dissociative processes: Theoretical
underpinnings of a working model for clinician and patient. Bulletin
of the Menninger Clinic, 57, 287–308.
29 College of Chiropractors of Ontario, College of Massage
Therapists of Ontario, and College of Physiotherapists of Ontario.
(1998).
Where’s my line.
30 American Psychiatric Association (1994). Diagnostic
and Statistical Manual of Mental Disorders. (4th ed.)
Washington, D.C.: Psychiatric Association.
American
42
References
31 Putnam, F. (1995). Dissociation as a response to extreme
trauma. In R. Kluft (Ed.), Childhood Antecedents of Multiple
Personality (pp. 66–97). Washington: American Psychiatric
Press.
32 van der Kolk, B., van der Hart, O., & Marmar, C. R. (1996).
Dissociation and information processing in Posttraumatic Stress
Disorder. In B. A. van der Kolk, A. C. McFarlane, & L.
Weisaith (Eds.), Traumatic Stress. The Effects of Overwhelming
Experience on Mind, Body, and Society (pp. 303–327). New
York: The Guildford Press.
33 Fromm, E. (1962). The Art of Loving. New York:
Harper & Row.
34 Lott, D. A. (1999). Drawing boundaries.
Psychology Today, 32, 48–52.
35 National Institutes of Health. The SMOG Readability
Formula. 1982. NIH Publication.
36 Davis, C. M. (1998). Patient Practitioner Interaction:
An Experimental Manual for Developing the Art of Health Care.
(3rd ed.) Thorofare, NJ: SLACK Incorporated.
37 Roy, R. (1998). Childhood Abuse and Chronic Pain: A
Curious Relationship?
Toronto: University of Toronto Press.
38 Frankel, F. H. (1990). Hypnotizability and dissociation.
American Journal of Psychiatry, 147, 823–829.
39 Seltzer, A. (1994). Multiple personality: A psychiatric
misadventure. Canadian Journal of Psychiatry, 39, 442–445.
43
Appendix A: Diagnostic Criteria for Post Traumatic Stress Disorder
Source: Diagnostic and Statistical Manual of Mental
Disorders (4th ed.),2 pages 424–429.
According to the Diagnostic and Statistical Manual for Mental
Disorders
(4th ed.),2 a person is experiencing Post Traumatic
Stress Disorder when criteria in six categories are met. The first
category involves exposure to an event in which the person experienced
serious injury, threats of death or serious injury, witnessed actual
or threats of death or serious injury to others, or experienced
a threat to the “physical integrity of self or others.”30p427
In addition, the person responded to the traumatic event with
intense fear, helplessness or horror.
The second category of criteria requires that the person have
at least one of a number of possible indications that the trauma
is persistently re-experienced. Examples include: 1) repeated and
disturbing memories of the event that intrude into the person’s
awareness, including images, thoughts or perceptions; 2) repeated
distressing dreams of the event; 3) behaving or feeling as if the
event is happening again as in dissociative flashback episodes or
hallucinations; 4) acute distress in response to exposure to things
that remind the person of the traumatic event; and 5) physiological
reactivity to things that remind the person of the traumatic event.
The third category requires several examples of attempts to avoid
stimuli associated with the trauma and numbing of general responsiveness
which was not present before the traumatic event. Examples are:
attempts to avoid thoughts, feelings or talk associated with the
trauma; attempts to avoid activities, places or people that remind
the person of the trauma; difficulty remembering aspects of the
trauma; significantly reduced interest or participation in important
activities; feelings of detachment; reduced range of affect; or
feeling that one will not have a normal future.
The fourth category of criteria involves at least two symptoms
of increased arousal, such as difficulty sleeping, irritability
or outbursts of anger, difficulty concentrating, hypervigilance
or an exaggerated startle response.
In addition, the disturbing symptoms are required to have lasted
more than one month (fifth criteria), and are resulting in significant
difficulties in social, occupational or other important functioning
(sixth criteria).
For more detailed information, please consult the Diagnostic
and Statistical Manual of Mental Disorders (4th ed.).30
45
Appendix B: Dissociation
The literature lacks clarity regarding the concept of dissociation.17
The DSM-IV states that “the essential feature of the
Dissociative Disorders is a disruption in the usually integrated
functions of consciousness, memory, identity, or perception of the
environment”. 2, p.477 The DSM-IV also points out
that dissociation should not be considered inherently pathological,
and that a cross-cultural perspective is important “because
dissociative states are a common and accepted expression of cultural
activities or religious experiences in many societies”. 2,
p. 477
Different forms of dissociation have been postulated to exist
on a continuum7, one end of which includes such relatively
common experiences as “highway hypnosis”, where a person
who has been driving a car suddenly realizes that she does not remember
what happened during all or part of the trip. The other end of such
a continuum may include extreme forms of dissociation such as Dissociative
Identity Disorder (that used to be termed Multiple Personality Disorder).
Some authors argue that there is reason to question the idea of
a continuum of dissociation. They state that some forms of experience
termed dissociative are qualitatively different from others which
therefore speaks against the idea of a continuum. They argue for
caution in response to claims that do not acknowledge the limits
of our knowledge of this phenomenon.17
Dissociative Identity Disorder (DID) is the diagnosis assigned
to a relatively small proportion of survivors of childhood abuse.
As adults, among other diagnostic criteria, they have distinct “identities”
or “personality states” which recurrently take control
of behavior, and these individuals demonstrate “an inability
to recall important personal information that is too extensive to
be explained by ordinary forgetfulness”.2, p. 487 Researchers
have concluded that DID is almost always associated with a history
of severe child abuse.26 Controversy also exists regarding
the diagnosis of DID. Some psychiatrists argue that sociocultural
influences and iatrogenicity have contributed to the frequency of
the diagnosis of DID in recent years.33
46
Appendix C: Suggestions for Clients at Out-patient Physical
Therapy Facilities
Welcome to physical therapy! We are glad to work with you.
Physical therapy will include an assessment and treatment by the
physical therapist. Direct and open communication between the client
and the therapist is important. Below is a list of suggestions that
may help you at physical therapy.
You have the right to choose a male or female physical therapist.
- If you know this is important for you, please tell us when you
book your first appointment.
- If you decide later in treatment that you would rather work
with a therapist of a different gender, you may tell us then too.
- If we are unable to book you with your choice of a male or female
therapist, we may refer you to a facility that can.
You can choose to have someone accompany you during your physical
therapy appointments.
This person can be:
- a family member or friend, or
- a staff member from the clinic.
Physical therapy works best when you and your therapist work
as a team.
For example, your physical therapist will explain your treatment
to you. Please tell your physical therapist if:
- you are not comfortable with the treatment,
- you do not understand the treatment or language your therapist
is using, or
- you do not agree with the treatment.
Also, physical therapy works best when you talk to your physical
therapist about how the treatment is working (or not working!) for
you. The more you are able to tell your physical therapist, the
better he or she will be able to help you.
We will do our best to ensure your privacy.
- Your physical therapist may need you to wear a gown for some
treatments. If you would prefer to bring loose fitting clothing
from home, please tell your physical therapist.
- In some cases, it is necessary to change your clothing for your
treatment: you will have privacy to change your clothing.
- Please tell us if you would like the curtains drawn around your
treatment table during any part of treatment.
47
Physical therapy involves touch and movement of your body.
Tell your physical therapist if:
- certain parts of your body are sensitive to touch or movement,
- you are nervous about touch, or
- there is something your physical therapist can do to make you
more comfortable.
You have the right to stop treatment at any time, during or
after a session.
Reasons for which people might stop treatment:
• discomfort during treatment, or
- deciding to try a different type of medical care.
If you decide to try a different type of care, your physical
therapist may be able to give you the name of someone she or he
thinks can help you.
Above all, we want you to notice an improvement in your health.
Readers are encouraged to copy this sheet or amend it for use
in their practices.
48
Appendix D: Sample of Consent Form
I am about to be examined and treated by a physical therapist
and her or his assistants.
In order for me to be properly examined or treated, I will need
to wear shorts and a T-shirt. The physical therapist will need to
observe my body while it is still and while it is moving. It will
be necessary for the therapist to touch and move my body in assessment
and treatment. Should I feel uncomfortable about the assessment
and treatment process at any time, I can inform the physical therapist
and request that assessment and/or treatment be stopped. I can have
someone else in the room with me – either a friend or relative,
or someone else from the clinic, if available. In the latter case,
I can choose the gender of this person.
I will need to tell the physical therapist about my health problems,
both past and present. The therapist will ask my permission to contact
my doctor if he or she finds any new problems. I am aware that all
information I disclose and all information that will be charted
is confidential.
Physical therapy treatment may involve:
__________________
(plain language, be specific). Soreness after treatment is common
because joints and muscles are stretched. If I have any other symptoms,
I will tell my physical therapist.
My signature below indicates that I understand all of the above
information.
Client Signature Date
Witness Signature Date
49
Appendix E: Recommended Reading
Bloom, S. L. (1997). Creating Sanctuary: Toward the Evolution
of Sane Societies. New York: Routledge.
Blume, E. S. (1990). Secret Survivors. New York: Ballantine
Books.
College of Chiropractors of Ontario, College of Massage Therapists
of Ontario, and College of Physiotherapists of Ontario. Where’s
My Line. College of Physiotherapists of Ontario is located at: 230
Richmond Street West, 10th Floor, Toronto, ON M5V 1V6. Tel: (416)
591-3828.
Fax: (416)
591-3834. E-mail:
collegpt@worldchat.com. Http:// www.worldchat.com/public/collegpt
Davis, C. M. (1998). Patient Practitioner Interaction: An Experimental
Manual for Developing the Art of Health Care
(3rd ed.). Thorofare, NJ: SLACK Incorporated.
Herman, J. (1992). Trauma and Recovery.
New York: Basic Books.
Oksana, C. (1994). Safe Passage to Healing: Guide for Survivors
of Ritual Abuse. New York: Harper Perennial.
Peterson, M. R. (1992). At Personal Risk: Boundary Violations
in Professional–Client Relationships.
New York: W.W. Norton & Company.
Radomsky, N. A. (1995). Lost Voices: Women, Chronic Pain and
Abuse.
New York: Harrington Park Press.
Rush, F. (1980). The Best Kept Secret: Sexual Abuse of Children.
New York: McGraw Hill.
Smith, M. (1993). Ritual Abuse. What It Is, Why It Happens,
How to Help. San Francisco: Harper.
van der Kolk, B. A. (1996). The body keeps the score: Approaches
to the psychobiology of posttraumatic stress disorder. In B.A. van
der Kolk, A. C. McFarlane, & L. Weisaith (Eds.),
Traumatic Stress. The Effects of Overwhelming Experiences on
Mind, Body, and Society (pp. 214–241). New York: The Guilford
Press.
50
Index
Body memory, 8, 23 Boundaries, 3, 14
Childhood sexual abuse. definition, 5; dynamics, 6; long-term
effects, 7; prevalence, 5; ritual abuse, 5 Clothing, 21 Confidentiality
of records, 34 Consent, 20; consent form, 49 Consultation with other
health professionals, 37 Continuity of care, 27 Control, 9, 25;
and adherence with treatment, 25; sharing control, 14 Dealing with
the client who is upset, 27–30 Demonstrating an awareness of
the prevalence and sequelae of violence and abuse, 16 Discharge,
35 Disclosure of childhood sexual abuse, 30–34 Dissociation,
10, 27, 46 Dissociative Identity Disorder, 30 Ebbs and flows, 15
Encouraging and modelling self-care, 26 Encouraging reconnection
with the body, 26 Environmental considerations, 23 Feelings, experiences
and behaviours that may interfere with treatment; ambivalence about
the body, 10; conditioning to be passive, 10; discomfort with men,
9; dissociation, 10; fear and distrust, 9; need to feel “in
control”, 9; physical pain, 9; self-harm, 11; triggers, 10,
29-30
Flashback, 10, 27
Guidelines for sensitive practice, 2, 17–38 Health care records,
34 Helping prepare the client for treatment, 18 Initial evaluation,
18 Language and communication, 20 Learning process, 15 Pain, 6,
9, 23 Post Traumatic Stress Disorder , 45 Principles of Sensitive
Practice, 13–16 Privacy, 22 Problem solving, 26 Rapport, 13
Resources and counselling, 36 Respect, 13 Right to choose a clinician
and a facility, 18 Ritual abuse, 5 Safety, 1, 8, 13 Sharing information,
14 Taking care of yourself , 37 Terminology, 2 Time factors, 24
Touch, 21 Transference and Counter-transference, 8 Triggers, 10,
27
51
|

