
Public Health Agency of Canada
www.publichealth.gc.ca
Common menu bar links
Institutional links
Diseases & Conditions
Health & Safety
Research & Statistics
Agency Information
Search Box
Canadian Perinatal Health Report - 2008 EDITION
An Overview of Perinatal Health in Canada - Part B
Behaviours and Practices in Pregnancy
One key determinant of maternal behaviours and practices in pregnancy is maternal education. This factor is closely associated with rates of breastfeeding, maternal smoking, exposure to second-hand smoke and periconceptional folic acid supplementation; higher maternal education is typically linked with healthy choices. For this reason, it is encouraging to observe increases in the proportion of Canadian mothers who completed college/university. As documented in this Report (page 58), this proportion increased from 56.9% (95% CI: 55.2–58.6) in 2000 to 69.6% (95% CI: 68.1–71.2) in 2005. Over the same period, rates of breastfeeding initiation increased from 81.6% (95% CI: 80.3–82.8) in 2000 to 87.0% (95% CI: 85.7–87.9) in 2005, while maternal smoking rates declined from 17.7% (95% CI: 16.6–18.8) to 13.4% (95% CI 12.4 to 14.4).
The proportion of live births to teenage mothers continued to decrease, with the proportion of live births to mothers aged 15 to 19 decreasing from 6.8% in 1995 to 4.8% in 2004 (page 63). Over the same period, the age-specific live birth rate among females aged 15 to 19 decreased from 25.4 to 15.4 per 1,000 females. The proportion of live births to women 35 years of age and over increased from 11.2% in 1995 to 15.4% in 2004, while the age-specific live birth rate among women aged 35 to 49 years increased from 11.8 in 1995 to 13.5 per 1,000 females in 2004 (pages 235 and 236). The increasing trend towards delayed childbearing is of enormous clinical and public health concern. Older maternal age is responsible for higher rates of preterm birth, fetal growth restriction, perinatal mortality and serious neonatal morbidity.52–54 Maternal mortality rates are also higher among older mothers.55 The excess (relative) risks that attend childbearing at older ages are a concern even though the absolute risks of adverse perinatal outcomes are typically low.
FIGURE 8 Age-specific live birth rates among females 20–44 years
Canada, 1962, 1982 and 2004
Live births per 1,000 females
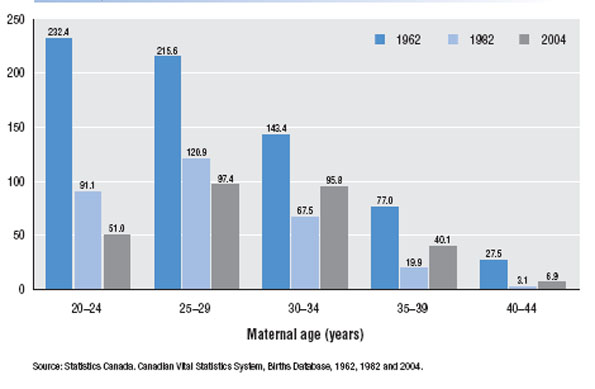
Nevertheless, it is important to recognize that this phenomenon has different impacts at the individual level, the population level and the social level. Although the individual-level risks associated with delayed childbearing are well recognized, the population health impact is less discussed. There have been steep fertility declines in the Canadian population over the last five decades and women over 30 years of age are the only subgroups showing any recovery in fertility patterns (Figure 8). Also, the population impact of older maternal age on outcomes such as preterm birth and SGA live births is substantially smaller than the increase in risk of these outcomes at the individual level. Whereas older maternal age increases the risk of preterm birth/SGA live birth by 50%–100%, the population rate of preterm birth/SGA would only decrease by about 10% if women 35 years of age and older stopped having babies. Finally, it should be recognized that more babies are born following assisted reproductive technology treatments to women under 35 years of age compared to those over 35.56 None of this mitigates the individual-level hazards associated with older maternal age, and women contemplating postponing childbirth should be aware of the risks associated with such a decision.57,58 Still, it bears emphasizing that delayed childbearing is now commonplace in industrialized countries and represents a social phenomenon with complex antecedents.
Pre-pregnancy weight
Excess pre-pregnancy weight is an increasingly common risk factor for various adverse outcomes that affect the mother, fetus and infant.59-61 Unfortunately, national-level databases in Canada do not contain information on this indicator and monitoring trends over time is therefore not possible. The recent Maternity Experiences Survey carried out by the CPSS should remedy this surveillance deficiency, especially if it is repeated on a periodic basis. Various provincial databases which contain good quality data on pre-pregnancy weight are another source of information on this issue and such information provides a reasonable picture of secular trends in Canada. Data from the Reproductive Care Program of Nova Scotia show that maternal pre-pregnancy weight ≥90 kg increased from 3.4% in 1988 to 13.1% in 2006 in that province. Similarly, data from the British Columbia Reproductive Care Program show that pre-pregnancy body mass index (BMI) ≥30 kg/m2 increased from 10.6% in 2001 to 11.4% in 2005.62 This disquieting trend in maternal size reflects similar well-recognized trends in body size in Canada and elsewhere that transcend gender and age.
Pre-pregnancy weight highlights one particular challenge in perinatal surveillance since national-level data on this indicator are not readily available. Adapting data in regional databases for the purpose of national surveillance in this situation represents a wise use of resources and strengthening provincial-level databases is clearly in the best interests of perinatal health surveillance and perinatal health in Canada. In this context, it is important to note that for reasons not readily apparent, there has been an unfortunate increase in missing information on pre-pregnancy weight in both the Nova Scotia and the British Columbia databases.62,63 Whereas the Reproductive Care Programs in both these provinces do a commendable job of maintaining their highly detailed databases, more support and focus on strengthening data quality is essential to ensure greater utility.
Health Services
Rates of labour induction in Canada, which had increased from 20.7% in 1995 to a peak high of 23.7% in 2001, dropped to 21.8% in 2004 (page 74). Cesarean delivery rates, on the other hand, continued their monotonic increase, with total cesarean rates increasing from 17.6% in 1995, to 21.1% in 2000 and 25.6% in 2004 (page 78). These figures provide an interesting contrast with those from the United States, both in terms of the similarities and the differences. In the United States, labour induction rates increased steadily from 16.0% in 1995 to 21.2% in 2004, while total cesarean rates increased from 20.8% in 1995 to 29.1% in 2004.64 Large differences were evident in the rate of vaginal birth after cesarean (VBAC); VBAC rates were 19.9% in Canada and 9.2% in the United States in 2004.
Episiotomy rates continued to decline in Canada—20.4% of women delivering vaginally had an episiotomy in 2004 compared with 31.1% in 1995. The rates of the more severe, third- and fourth-degree perineal lacerations showed contrasting trends, with third-degree lacerations increasing slightly from 3.0% in 1995 to 3.3% in 2004 and fourth-degree lacerations declining from 0.7% in 1995 to 0.6% in 2004. Overall, however, third- and fourth-degree lacerations (combined) did not show an increase or decrease and the possibility of changes in labelling (third- versus fourth-degree laceration) cannot be excluded.65
Trends in length of hospital stay following birth and in readmission rates after hospital discharge showed encouraging patterns, especially for newborns. In 1995, 20.1% of normal birth weight newborns were discharged within two days after birth and this rate increased to 27.3% in 2004. A similar trend was observed among low birth weight infants. Rates of neonatal admission did not increase over the same period; 3.7 per 100 infants discharged after the birth admission were readmitted within the neonatal period in 1995 compared with 3.4 per 100 infants in 2004. Maternal length of stay also decreased between 1995 and 2004, while rates of readmission increased marginally over the same period (1.5 to 1.7 per 100 vaginal deliveries, and 2.8 to 3.0 per 100 cesarean deliveries). These trends imply substantial gains in the efficient use of hospital resources over the last decade without any apparent compromise of patient safety. The confidence one can place in these estimates and the resulting inferences is unfortunately somewhat reduced because of methodologic issues, however. The exact time of birth is not currently available in either CIHI’s Discharge Abstract Database or the Hospital Morbidity Database, and hence estimates of the length of stay for newborns and postpartum length of stay for mothers represent approximations.
Maternal Health
The maternal mortality ratio (MMR) for Canada was 5.5 (95% CI: 4.2–7.2) per 100,000 live births in 2002–2004. This rate was not statistically different from the same rate in 1999–2001 (4.2, 95% CI: 3.2–5.7). Even though the point estimate of the MMR in 2002–2004 was higher than in previous years, this is unlikely to be of significance especially since there were no striking increases in any of the specific causes of maternal death (page 103). A similar non-significant increase in the MMR was observed in the United Kingdom as well (11.4 per 100,000 maternities in 1997–1999 and 13.1 per 100,000 maternities in 2000–200255 ).
Among the direct causes of maternal death, death due to postpartum hemorrhage (PPH) has been of particular interest in Canada in recent years. This is because the Canadian Perinatal Health Report, 2003 reported a two-fold increase in the rate of hysterectomy for PPH between 1991 and 1999.66 The increase remained unexplained at that time and hypotheses proposed included changes in obstetric practice, increases in older maternal age and increases in adherent placenta due to a higher prevalence of women with a previous cesarean delivery. The Maternal Health Study Group of the CPSS has since carried out a detailed investigation of this issue.67 The principal underlying phenomenon appears to be a temporal increase in atonic PPH (page 105). Whereas the cause of the increase in atonic PPH remains unclear, it is worth noting that a similar unexplained increase in PPH has been documented in Australia,68,69 and maternal deaths due to PPH have increased in the United Kingdom in recent years.55 The editorial comment that accompanied the Canadian publication stated: “The rise in atonic postpartum haemorrhage, which many of us have observed . . . remains unexplained . . . If any of our readers have any suggestions for [this] puzzling [increase], please share them with us.”70
The frequency of induced abortions in Canada, which the CPSS has tracked in each of its Perinatal Health Reports, appears to have reached a plateau in recent years. However, it is unclear if the data provide an accurate picture of the situation in Canada. Some of the causes for the problems with data quality arise because of newer technologies that are more difficult to track (such as very early abortions carried out in physicians’ offices and those carried out using pharmacologic agents). Other causes and issues, detailed in the section on Induced Abortions (page 109), should however be addressed in the interests of national surveillance.
Fetal and Infant Health
Large-for-gestational-age (LGA) live births have increased in frequency since 1995, although this trend has stabilized in the last three years. Regional variations were large, with Quebec having the lowest frequency (10.2%) and the Northwest Territories having the highest (20.4%). Small-for-gestational-age live births in Canada show the opposite temporal trend (page 130), and the Northwest Territories had the lowest rate of such babies (5.1% in 2004). These regional variations in fetal growth may reflect differences in population ethnicity. The broader question of whether fetal growth standards (i.e., the standard cut-offs used for determining whether an infant is SGA or LGA) should be customized for ethnicity and other factors is part of an emerging debate in the international perinatal literature.71,72 The final consensus on this issue will have an important bearing on clinical practice and perinatal health in Canada.
Of the three specific anomalies highlighted in the Congenital Anomalies section (page 158), the birth prevalence of Down syndrome and cleft palate appear unchanged, while the frequency of neural tube defects has been reduced by more than half between 1995 and 2004. The decline in the birth prevalence of neural tube defects has occurred secondary to prenatal diagnosis and also, from 1998 onwards, due to food fortification with folic acid. Several studies have documented the effects of folic acid food fortification in Canada.73–76 The most recent seven-province study showed a 46% decline in neural tube defects, with the magnitude of the decrease proportional to the baseline pre-fortification rate.76
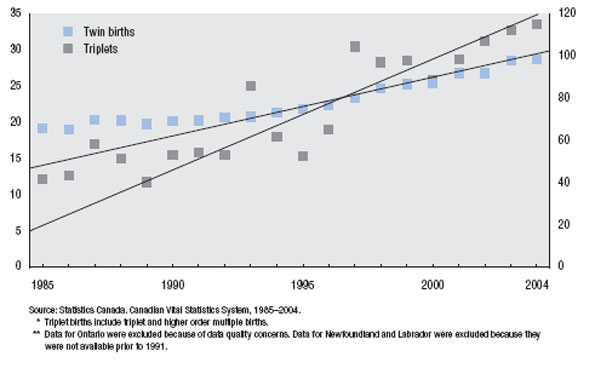
The rate of multiple births increased from 2.2% in 1995 to 3.0% in 2004. The relative increase in triplet and higher order multiple births was larger than the increase among twins (Figure 9), and neither trend appeared to show any signs of a plateau. Much of this increase was due to increases in the use of assisted reproductive technologies (ART). The increase in multiple births is not surprising—both because the number of ART cycles performed in Canada has increased from 7,884 in 2001 to 11,068 in 2004, and because the percentage of (in vitro fertilization/intra-cytoplasmic sperm injection) cycles with two or more embryos has increased from 49% in 2001 to 66% in 2004.56
Two indicators of severe neonatal morbidity, namely, the rate of neonatal sepsis and the rate of endotracheal intubation have shown encouraging trends between 1995 and 2004. The rates of each morbidity and the changes observed over the last decade varied by birth weight category (page 150). The increases in intubation particularly among infants with a birth weight <1,000 g are promising, especially in the light of recent research findings showing that among such newborns intensive neonatal care technologies have moved beyond the stage of reducing death at the expense of increases in both disability-free survival and disability-associated survival.77 We appear to be at a stage where rates of death and disability-associated survival are both being reduced among infants with a birth weight between 500 and 999 g.78
FIGURE 9 Temporal trends in the rates of twin and triplet births*
Canada (excluding Ontario, and Newfoundland and Labrador),** 1985–2004
Twin births per 1,000 total births (primary Y-axis)
Triplet births per 100,000 total births (secondary Y-axis)
Conclusion
The Canadian Perinatal Health Report, 2008 Edition documents a variety of surveillance phenomena that range from simple trends describing improvements in determinants of health (e.g., declining rates of maternal smoking, rising rates of breastfeeding) to more complex patterns in health outcomes (e.g., rising rates of preterm birth and declining rates of SGA). In addition, several enigmatic phenomena require further study and elucidation, including the mystery surrounding missing birth registrations in Ontario and the increases in atonic PPH in Canada (which mirror similar unexplained increases in Australia and the United Kingdom). Finally, there are several areas identified where surveillance information could benefit from improvements in data quality, including indicators such as the induced abortion rate. It is also clear that better quality information on First Nations, Inuit and Métis and other vulnerable subpopulations is necessary in order to identify and target disparities in perinatal health. Nevertheless, the general tone of the Report is upbeat, with clear documentation of many small and large improvements in perinatal health. The information, especially the regional comparisons, can be used to create benchmarks for improvement in the future. It is hoped that this Report will be widely used to inform clinical, public health and health policy decision making and to spur efforts aimed at improving perinatal health surveillance.
K.S. Joseph MD, PhD
Professor, Perinatal Epidemiology Research Unit
Departments of Obstetrics & Gynaecology, and Pediatrics
Dalhousie University and the IWK Health Centre
Member, Steering Committee, Canadian Perinatal Surveillance System