
Public Health Agency of Canada
www.publichealth.gc.ca
Common menu bar links
Institutional links
Diseases & Conditions
Health & Safety
Research & Statistics
Agency Information
Search Box
Canadian Perinatal Health Report - 2008 EDITION
Introduction
The Canadian Perinatal Health Report, 2008 Edition is the fifth national surveillance report from the Canadian Perinatal Surveillance System (CPSS), continuing an important information dissemination activity of the Maternal and Infant Health Section, Public Health Agency of Canada. In 1995, the Section and the CPSS Steering Committee developed the conceptual framework for the CPSS, identified appropriate perinatal health indicators and their data sources, and began analysis and interpretation of the data. Since then, the CPSS has produced numerous publications, including four national surveillance reports and over 50 peer-reviewed papers.* These publications, and other activities of the CPSS, have been favourably reviewed by external evaluators.1 This fifth CPSS report is the third Canadian Perinatal Health Report. It presents temporal trends and differences observed at the national and provincial/territorial levels for 29 perinatal health indicators.
CPSS Conceptual Framework
The CPSS considers a health surveillance system to be a network of people and activities that maintain the surveillance process.2 The surveillance itself is a continuous and systematic process of data collection, analysis and interpretation of information for monitoring health problems2 with the aim of contributing to improved health outcomes. Figure A depicts the cycle of surveillance.3
FIGURE A National Health Surveillance
Overlying this concept of health surveillance is the concept of the determinants of health—that health status is influenced by a range of factors including, but not limited to, health care.4 Therefore, it is important to monitor not only health outcomes but also factors—such as behaviours, physical and social environments, and health services—that may affect those outcomes. Information on trends in and patterns of various risk and protective factors helps to explain patterns of morbidity and mortality, and may point the way to effective interventions and appropriate allocation of health resources. Health surveillance is thus a core competency and strategic objective of the Public Health Agency of Canada, as “effective and timely surveillance is critical to the ability of the government and provinces/territories to accurately track, plan for and respond to diseases.”5
CPSS Structure
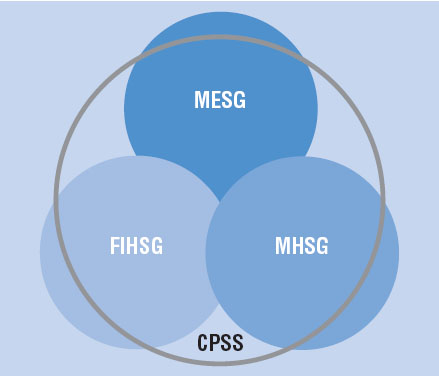
The mandate of the CPSS is to contribute to improved health for pregnant women, mothers and infants in Canada through ongoing monitoring and reporting on perinatal health determinants and outcomes. The CPSS collaborates with Statistics Canada, the Canadian Institute for Health Information (CIHI), provincial and territorial governments, health professional organizations, advocacy groups and university-based researchers. Representatives of these groups and several international experts serve on the CPSS Steering Committee and its study groups: the Fetal and Infant Health Study Group (FIHSG), Maternal Health Study Group (MHSG) and the Maternity Experiences Study Group (MESG). This intersectorial and intergovernmental structure effectively engages stakeholders as full partners in shaping and conducting national perinatal health surveillance, and has been recognized as an innovative and important strength of the CPSS.1 The principles and objectives of the CPSS are described in more detail elsewhere.6,7
FIGURE B Structure of the Canadian Perinatal Surveillance System
Study Groups of the Canadian Perinatal Surveillance System
Fetal and Infant Health Study Group
The mandate of the FIHSG is to conduct surveillance on fetal and infant mortality and morbidity.
Current study group activities include the Canadian Congenital Anomalies Surveillance Network
with the mandate to support the development and maintenance of a population-based congenital
anomalies surveillance system; and a Working Group on First Nations, Inuit and Métis Infant
Mortality Data with the mandate to identify and support strategies to improve the quality of the
data on infant mortality in these populations. In collaboration with Statistics Canada, members
of the FIHSG are also exploring linking the already combined infant birth-death records with
the person-oriented hospital birth and delivery records in order to create a more comprehensive
national database on perinatal events. The FIHSG primarily uses existing data sources for its
surveillance efforts.
Maternal Health Study Group
The mandate of the MHSG is to conduct surveillance on key behaviours, health services
and outcomes related to maternal health. Current study group projects include the surveillance
of cesarean delivery and planning toward a second report on maternal mortality and severe
morbidity in Canada, scheduled for publication in 2010. Members of the MHSG are also involved
in the Canadian component of a World Health Organization (WHO) survey on mode of delivery
and maternal and perinatal outcomes. The MHSG primarily uses existing data sources for its
surveillance efforts.
Maternity Experiences Study Group
The mandate of the MESG is to guide the development, implementation, expert analysis and
reporting of a national Maternity Experiences Survey. The first survey of its kind in Canada, its
primary objective is to provide information for an in-depth examination of Canadian women’s
knowledge, experiences and practices during pregnancy, birth and the early postpartum months,
and of their perceptions of perinatal care as an integral component of perinatal health surveillance.
Data collection for the national survey was completed in January 2007 achieving a response
rate of 78%. Data editing and analysis activities are ongoing and results will be reported in the
CPSS’s sixth national report, scheduled for publication in 2008.
CPSS Indicators
A health indicator is a measurement that, when compared with either a standard or desired level of achievement, provides information regarding a health outcome or important health determinant.7 In order to identify perinatal health indicators that should be monitored by a national perinatal surveillance system, the CPSS considered the importance of the health outcome or determinant, the scientific properties of the indicator, such as its validity in measuring that outcome or determinant, and the feasibility of collecting the data required to construct it. Appendix C lists the 54 indicators that resulted from this process.
Outline of the Report
This report contains information on 29 perinatal health indicators for which we currently have national data. Two of these indicators, rate of periconceptional folic acid supplementation and rate of maternal exposure to second-hand smoke, are new to the report. Also, the indicator on breastfeeding rates has been enhanced to include rates of exclusive breastfeeding. Indicators are grouped as health determinants (behaviours and practices, and health services) and health outcomes (maternal, fetal and infant). As in the CPSS’s previous Perinatal Health Reports, for each indicator, surveillance results are presented, data limitations discussed and key references listed. Statistics for each indicator consist mainly of temporal trends at the national level and interprovincial/territorial comparisons for the most recent year for which data are available.
The principal data sources used for this Perinatal Health Report were vital statistics, hospitalization data and the Canadian Community Health Survey. Population estimates and induced abortion statistics from Statistics Canada were also used. In comparison to the data sources and methods used for previous reports, three differences are noteworthy. First, with the exception of two indicators on hospital readmission, all indicators using hospitalization data were calculated using CIHI’s Hospital Morbidity Database rather than its Discharge Abstract Database. Second, indicators using hospitalization data are reported by province/ territory of residence rather than province/territory of hospitalization. And, third, indicators previously based on the National Longitudinal Survey of Children and Youth are now based on data from the Canadian Community Health Survey. Because these data sources are limited in their ability to identify populations at risk, accurately measuring and reporting on disparities in perinatal health in Canada remains a challenge and the lack of this information is a limitation in CPSS reports. Additionally, as in previous CPSS publications, Ontario vital statistics data were excluded from most vital statistics-based indicators due to concerns about data quality. Ontario has begun to take steps to respond to this important problem and we hope to be able to include Ontario data in national statistics in future reports. Ontario vital statistics are reported separately in Appendix H.
A detailed description of each data source, including data quality and the methods for calculating each indicator based on the data source, is presented in the Data Sources and Methods section of the report. The ICD-9 and ICD-10 codes used for each indicator are also detailed in that section.
Summary
Perinatal health surveillance has an important and fundamental role in providing the necessary information to be used to improve the health status of pregnant women, mothers and infants in Canada. It comprises a dynamic, integrated system of ongoing data collection, linkage, validation, analysis and interpretation on vital perinatal health issues. The result is information that permits identification of “red flags,” tracking of temporal trends and geographic disparities, as well as consideration of the impact of changes in clinical practice and public health policy. Perinatal health surveillance provides both a measurement tool (where we have been in the past, where we are at present) and a stimulus to action (where we need to be in the future).
Reg Sauve, MD, MPH, FRCPC
Professor of Paediatrics and Community
Health Sciences
University of Calgary
Visiting Scientist to Public Health Agency
of Canada
Chairperson, CPSS Steering Committee
Susie Dzakpasu, MHSc
Senior Epidemiologist, Maternal and Infant
Health Section
Health Surveillance and Epidemiology Division
Public Health Agency of Canada
References
- Attenborough R, Kirby R, Paneth N. CPSS External Evaluators’ Report [Internet]. Ottawa: Public Health Agency of Canada; 2005 [cited 2007 Dec 7]. Available from: http://www.phac-aspc.gc.ca/rhs-ssg/extreport/index.html
- Buehler JW. Surveillance. In: Rothman KJ, Greenland S, editors. I. 2nd ed. Philadelphia: Lippincott-Raven; 1998. p. 435–57.
- McCarthy B. The risk approach revisited: a critical review of developing country experience and its use in health planning. In: Liljestrand J, Povey WG, editors. Maternal Health Care in an International Perspective. Proceedings of the XXII Berzelius Symposium; 1991 May 27–29, Stockholm, Sweden. Uppsala, Sweden: Uppsala University; 1992. p. 107–24.
- Federal, Provincial and Territorial Advisory Committee on Population Health. Strategies for population health: investing in the health of Canadians. Ottawa: Minister of Supply and Services Canada; 1994.
- Public Health Agency of Canada. The Public Health Agency of Canada strategic plan: 2007–2012, knowledge, information, action [Internet]. Ottawa: Her Majesty the Queen in Right of Canada, represented by the Minister of Health Canada; 2007 [cited 2007 Dec 7]. Available from: http://www.phac-aspc.gc.ca/publicat/2007/sp-ps/index-eng.html
- Health Canada. Canadian Perinatal Surveillance System progress report. Ottawa: Minister of Supply and Services Canada; 1995.
- Health Canada. Canadian Perinatal Surveillance System Progress Report 1997–1998. Ottawa: Minister of Public Works and Government Services Canada; 1998.
* A complete list of CPSS publications can be found in Appendix I.