
Public Health Agency of Canada
www.publichealth.gc.ca
Common menu bar links
Institutional links
Diseases & Conditions
Health & Safety
Research & Statistics
Agency Information
Search Box
E-mail this page
Supplement
2004 Canadian Sexually Transmitted Infections Surveillance Report
Viral STIs and Enhanced Surveillance
To provide a more complete picture of the transmission, acquisition and burden of STIs in Canada, this chapter addresses some infections that fall outside the scope of nationally reportable bacterial STIs2. Co-infection with multiple viral or bacterial STIs is common, especially in high-risk populations. Therefore, risk factors and populations that cross infections need to be taken into consideration when developing public health interventions.
Human immunodeficiency virus (HIV), a nationally reportable viral infection, has multiple modes of transmission, one of which is sexual contact. While detailed national surveillance data are published in a separate report, sexual transmission trends are highlighted here. Human papillomavirus (HPV) and herpes simplex virus (HSV) are both considered highly prevalent infections in the Canadian population with significant morbidity and sequelae. Compared with hepatitis B, sexual transmission of hepatitis C is usually inefficient except under certain circumstances.
Two national enhanced surveillance initiatives provide important information on an STI relatively new to Canada and a population which would likely not be captured in routine surveillance data. Lymphogranuloma venereum (LGV) is an emerging bacterial STI under enhanced surveillance. While the number of reported cases is relatively small, surveillance data assist in determining the epidemiology of the infection in Canada and appropriately targeting prevention and promotion messages. The Enhanced Surveillance of Canadian Street Youth (E-SYS) measures the rates of STIs, blood-borne pathogens and risk determinants in this high-risk population, which often has limited access to basic health care services and may be difficult to reach through school, telephone or other residence-based approaches.
Viral STIs
HIV
The presence of an ulcerative bacterial STI (e.g. syphilis or anogenital herpes) or non-ulcerative STI (e.g. chlamydia or gonorrhea) increases the risk of acquiring and/or transmitting HIV. In turn, HIV infection increases the risk of acquiring or transmitting an STI(33). Increasing trends in bacterial STIs may be precursors to increases in HIV infection in certain populations due to the synergistic relationship between these infections. In addition, HIV trends and patterns of transmission are an important component to consider when interpreting STI trends in a given population.
National surveillance of HIV is carried out by the Surveillance and Risk Assessment Division, PHAC, in cooperation with provincial, territorial and local partners. Semi-annual surveillance reports, summaries on specific topics (Epi Updates) and reports summarizing the estimates of HIV prevalence and incidence in Canada are also available. Statistics described in this section are reported in the HIV and AIDS in Canada, Surveillance Report to December 31, 2004(77).
- A total of 57,674 positive HIV tests were reported to the PHAC between November 1985 (when reporting began) and December 31, 2004.
- Positive test reports had been decreasing between 1995 and 2000 but increased in 2001 and 2002. Since 2002, test reports have remained steady at approximately 2,500 per year (Figure 1).
- The majority of HIV case reports are in males, however, females accounted for slightly greater than 25% of HIV case reports in 2004.
- Before 1995 females accounted for less than 10% of positive test reports, but this has risen throughout the late 1990s and early 2000s.
- Individuals 30-39 years old accounted for the highest proportion of positive test reports in 2004, and this was true for both males and females.
- Sexual transmission accounts for a significant proportion of reported HIV cases.
- Approximately 45% of positive test reports in 2004 were in men who have sex with men (MSM), and this has been an increasing trend since 2001 (Figure 2).
- The heterosexual exposure category continues to account for a significant proportion of HIV-positive test reports (30% in 2004) and has surpassed intravenous drug use (IDU) as the second largest exposure category.
- 25% of heterosexual positive HIV test reports in 2004 were from an HIV-endemic country, a number that has been increasing since 1998.
- 40.5% of those in the heterosexual exposure category reported sexual contact with a person at risk.
- 34.5% of heterosexual positive HIV test reports had no identified risk.
- Almost one-fifth of HIV-positive test reports had IDU as their exposure category.
MSM continue to be at considerable risk for infection with HIV and other STIs. Risk factors include engaging in unprotected anal intercourse, both receptive and insertive, with casual or regular partners, and practising unsafe sex with a known HIV-positive partner(78). A recent survey of MSM showed that 31% of HIV-negative and 63% of HIV-positive participants reported one or more episodes of unprotected receptive anal intercourse; 49% of HIV-negative and 43% of HIV-positive individuals reported unprotected insertive anal intercourse(72).
Figure 1. Positive HIV test reports by year of test, 1995-2004
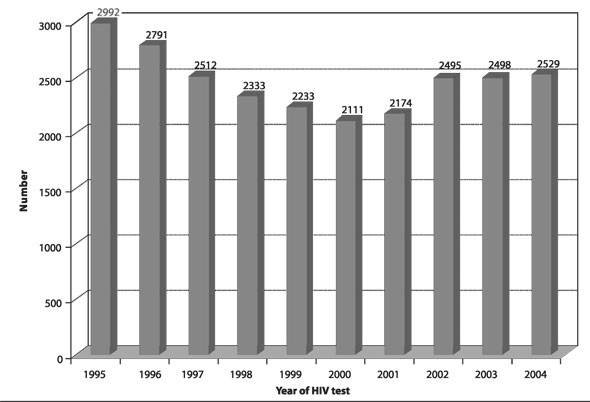
Source: Surveillance and Risk Assessment Division, Centre for Infectious Disease Prevention and Control, Public Health Agency of Canada, 2006.
Figure 2. Adult positive HIV test reports by exposure category, 1995-2004
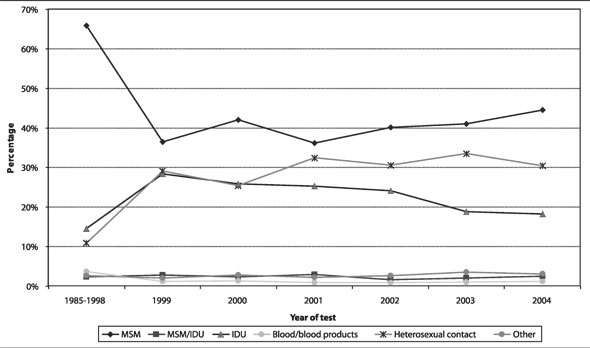
Source: Surveillance and Risk Assessment Division, Centre for Infectious Disease Prevention and Control, Public Health Agency of Canada, 2006.
Human papillomavirus (HPV) and anogenital warts
- Based on published studies in Canada and the US, HPV is likely one of the most common STIs in North America(79-82).
- Over 100 different types of HPV exist, of which 35 or more infect the anogenital epithelium.
- High-risk HPV may cause abnormal Pap smear results in women and could lead to cancers of the cervix, vulva, vagina, and anus. In men, cancer of the anus or penis may develop.
- Low-risk HPV also may cause abnormal Pap results or anogenital warts(42).
- The most common high-risk (oncogenic) types include types 16 and 18, which account for approximately 70% of cervical cancers(83).
- Low-risk types 6 and 11 account for approximately 90% of anogenital warts(83).
- Testing for HPV in Canada is not routine, however, screening programs are in place to detect cervical abnormalities, pre-cancerous lesions and cervical cancer due to HPV infection in women.
- There are limited Canadian data on the incidence and prevalence of HPV infection and no published studies on the epidemiology of anogenital warts in Canada. Most studies focus primarily on HPV infection in women and its sequelae.
- The burden of infection in females affects those under the age of 30 years(79,84,85).
- Studies have found point prevalence rates of high-risk HPV among females overall ranging from 10.8% to 25.8% (population studied and testing methods vary)(79-81,84,85).
- The prevalence of high-risk HPV among females 13 to 20 years of age in Nunavut has been found to be as high as 42%(84).
- The incidence of high-risk HPV among females 15 to 19 years of age was found to be 25% over a 14-month period(79).
- A vaccine against HPV types 6, 11, 16 and 18 for women has recently been licensed for use in Canada.
- Further HPV prevalence studies are currently under way in Canada. The design of a sentinel surveillance system for HPV is in progress to establish baseline measures of HPV prior to the introduction of the vaccine and to monitor future trends.
Anogenital herpes simplex virus (HSV)
- Anogenital HSV is of major public health importance. Not only is infection associated with significant morbidity, but herpetic lesions may also facilitate the transmission of HIV(86,87).
- Anogenital HSV infection caused by either HSV-1 or HSV-2 can cause vesicular lesions and painful ulcers that may recur at intervals(86).
- Many HSV infections are asymptomatic, and asymptomatic shedding of the virus results in transmission. Suppressive therapy may help to reduce silent shedding and transmission, but there is no known cure for HSV infection.
- Complications due to anogenital herpes infection include aseptic meningitis and other neurological complications, extra-genital lesions and disseminated infection(42).
- Perinatal transmission of HSV from a mother to her child may occur in utero, during or after birth, and may have devastating (86,87) consequences.
- The prevalence of anogenital HSV increased markedly throughout the world during the 1980s and 1990s(42); however, Canadian data on HSV seroprevalence are quite limited.
- A population-based study of women in British Columbia in 1999 found an age-adjusted seroprevalence of 58.9% for HSV-1 and 17.3% for HSV-2(86).
- In a low-risk population in Ontario between 2000 and 2001, age-standardized seroprevalence rates (males and females combined) of 51.1% and 9.1% were found for HSV-1 and HSV-2 respectively(88).
- Among STD clinic attendees in Alberta between 1994 and 1995, HSV-1 seroprevalence was found to be 56% and HSV-2 seroprevalence was found to be 19%(89).
- A 3-year enhanced surveillance study was conducted to determine the incidence, determinants, and morbidity and mortality rates of neonatal herpes simplex virus (NNHSV) in Canada(87).
- About 20 cases were detected a year (5.9 cases per 100,000 live births).
- Of cases with known HSV-type, 62.5% were HSV-1.
- 40% of mothers were unaware of their HSV infection prior to delivery and obvious genital lesions were rarely present.
- These results have clear implications for prenatal prevention of neonatal HSV infection.
Sexually transmitted hepatitis C virus (HCV)
The role of sexual transmission in the spread of HCV has been a matter of debate and dissention for many years. Although it appears that sexual transmission under most circumstances is inefficient, some studies have highlighted increased HCV incidence among MSM and in particular those who are HIV-positive.
- Studies have suggested that HIV infection and/or certain sexual behaviours are major risk factors for sexual transmission of HCV(90-92):
- Unprotected receptive anal intercourse
- Fisting
- Having a sexual partner with a history of IDU
- Anogenital herpes
- HIV infection
- > 20 sexual partners in the previous year
- > 100 lifetime sexual partners.
- In one study, two-thirds of all HCV seroconversions occurred in non-IDU engaging in high-risk behaviours, suggesting that certain sexual practices may have a role in the transmission of HCV(93).
- Biological evidence shows that HCV can be detected in semen using molecular techniques and adds further weight to the argument that sexual transmission may play a role in the spread of the virus(91).
- The Enhanced Hepatitis Strain Surveillance System (EHSSS), a population-based system that was initiated in October 1998 in Canada, collects detailed information on risk factors, including sexual transmission, for newly acquired cases of HCV.
- EHSSS data to 2004 suggest that a small proportion (6%) of newly acquired HCV infections in Canada may be related to sexual transmission(94).
Hepatitis B virus (HBV)
Although HBV is the most common cause of sexually transmitted hepatitis, it is also a vaccine preventable disease. For information on the epidemiology of HBV and on the HBV vaccine please consult the Canadian Immunization Guide(95), available online at http://www. phac-aspc.gc.ca/publicat/cig-gci/index-eng.php.
Enhanced surveillance
Lymphogranuloma venereum (LGV)
- Until recently, LGV was rare in industrialized countries and was usually acquired in endemic countries.
- LGV is endemic to parts of Africa, Asia, South America and the Caribbean.
- In 2003, cases were reported in MSM in the Netherlands and more recently elsewhere in Europe and North America.
- LGV is not a nationally reportable infection in Canada. In light of the increase in cases seen in North America and Europe, however, the PHAC, in partnership with the provinces and territories, established an enhanced national surveillance system for LGV in February 2005.
- LGV is a sexually transmitted infection caused by Chlamydia trachomatis serotypes L1, L2 and L3. Unlike chlamydia serovars A-K, which cause the more common genital infection and conjunctivitis, LGV serovars are invasive, preferentially affecting the lymph tissue.
- LGV can be transmitted through vaginal, anal or oral sexual contact.
- LGV is commonly divided into primary, secondary and tertiary (chronic, untreated) stages.
- The incubation period for primary LGV is 3 to 30 days; it is characterized by small, painless papule(s) at the site of inoculation that may ulcerate, are self-limiting and may go unnoticed.
- Secondary LGV usually begins within 2 to 6 weeks of the primary lesion, usually presenting as proctitis with inguinal and/or femoral lymphadenopathy; it may involve bloody, purulent or mucous anal discharge and systemic symptoms such as fever and malaise.
- Tertiary LGV leads to chronic inflammatory lesions that cause scarring, lymphatic obstruction and rectal strictures and can cause extensive destruction of the genitalia.
- Between February 2005 and August 2006, 79 cases of LGV were reported to PHAC; 42 were confirmed cases and 37 were probable cases.
- Of the reported cases, date of onset ranged from November 2001 to June 2006 (where information was available) (Figure 3).
- All reported cases have been male. The majority have been in Caucasian MSM between the ages of 21 and 62 (Table 1).
Figure 3. Epidemiologic curve for LGV cases in Canada where symptom onset date known, reported up to August 2006
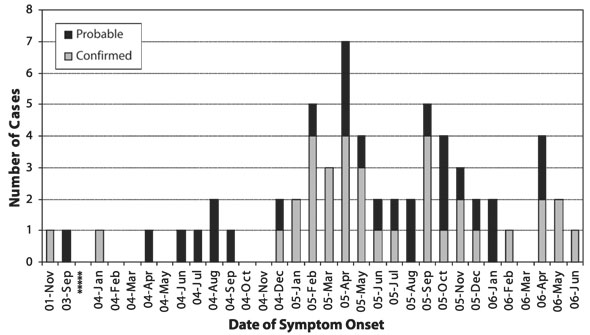
Table 1. Summary of demographic data for 79 reported cases of LGV in Canada
Feature |
No. of cases (%) |
Male |
79/79 (100) |
Ethnicity |
|
|
Caucasian |
30/36 (83.3) |
|
Asian |
1/36 (2.7) |
|
Caribbean |
1/36 (2.7) |
|
South American |
4/36 (11.1) |
Age range, years |
21-62 |
Mean age, years |
38.6 |
- Frequently reported sexual behaviour and risk factors are as follows:
- Over 90% have reported recent receptive or insertive anal or oral contact, often unprotected.
- The majority of cases reported sexual activity in a bathhouse or private residence; Internet partnering was frequently reported.
- Fisting and rectal use of crystal methamphetamine has been reported by a small number of cases (< 10%).
- Recent travel within Canada was reported by five cases; an additional five cases reported travel to endemic regions or areas reporting outbreaks outside Canada, including France, Mexico, Cuba and Jamaica.
- Co-infection with HIV (78%), HSV (26%) and HCV (14%) was also reported.
For further updated information, please refer to the PHAC LGV Epi Updates: http://www.phac-aspc.gc.ca/publicat/epiu-aepi/std-mts/lgv-eng.php.
STI in street youth: Enhanced Surveillance of Canadian Street Youth (E-SYS)
- E-SYS is a multi-centre sentinel surveillance system that monitors rates of STIs, blood-borne pathogens, behaviours and risk determinants in the Canadian street youth population(96).
- Compared with youth in the general Canadian population, higher rates of STIs and blood-borne pathogens have been reported in street youth (Table 2)(96).
- Bacterial STI rates among street youth are on the rise, which is consistent with the national trends in the general population (Table 1).
- HSV-2 prevalence among street youth increased from 14.2% to 18.8% between 2001 and 2003.
- Higher rates of HSV-2 were found among females than males.
- Street youth 20 to 24 years of age had higher rates of HSV-2 than those aged 15 to 19 years.
- As with HSV-2, HSV-1 prevalence among street youth increased from 2001 to 2003 (56.0% to 60.8%), and rates were higher among females and older street youth overall.
- High rates of hepatitis C were found in street youth (approximately 4.0%), although the rates did not change significantly between 1999 and 2003.
- The prevalence of HIV among street youth was approximately 1%.
- The burden of infection falls on older street youth (20 to 24 years), and there were no variations by sex. However, the case counts were small, and the results must be interpreted with caution.
- Testing was performed for human T cell lymphotropic virus (HTLV) in 2001 and 2003. In each year there was one laboratory-confirmed case of HTLV-1.
For further information and publications on E-SYS, please refer to the PHAC Sexually Transmitted Infections Web site: www.publichealth.gc.ca/sti.
Table 2. Rates1 of genital chlamydia, gonorrhea and infectious syphilis among street youth and in the general youth population in 1999, 2001 and 2003
Age |
1999 (%) |
2001 (%) |
2003 (%) |
|---|---|---|---|
Genital Chlamydia |
|||
15-19 years |
8.98% (0.65%) |
11.51% (0.74%) |
10.88% (0.82%) |
20-24 years |
7.87% (0.75%) |
11.38% (0.88%) |
11.04% (0.99%) |
Gonorrhea |
|||
15-19 years |
1.56% (0.06%) |
1.04% (0.07%) |
2.19% (0.08%) |
20-24 years |
0.90% (0.07%) |
2.12% (0.09%) |
4.38% (0.10%) |
Infectious Syphilis |
|||
15-19 years |
— |
0%(< 0.01%) |
0.25% (< 0.01%) |
20-24 years |
— |
0%(< 0.01%) |
1.31% (< 0.01%) |
1Rates in street youth are prevalence rates; the rates they are compared with in the general youth population (in brackets) are derived from reported cases.
2From a practical perspective, not all infections can be under national surveillance. There are significant costs associated with surveillance, both in terms of human resources and the implementation of surveillance systems. Various research studies complement national surveillance by examining non-nationally reportable STIs and their public health implications.