
Public Health Agency of Canada
www.publichealth.gc.ca
Common menu bar links
Institutional links
Diseases & Conditions
Health & Safety
Research & Statistics
Agency Information
Search Box
E-mail this page
A Guide to HIV/AIDS Epidemiological and Surveillance Terms
[Previous] [Table of Contents] [Next]
Frequently Asked Questions (FAQs)
in HIV/AIDS Monitoring and Epidemiological Research in Canada
Before you start ...
The table of contents lists Frequently Asked Questions (FAQs) answered in this guide.
The FAQs are organized around the issue they address.
If the answer to the listed FAQ includes frequently used terms contained within this guide, these terms appear in the answer in bold. These terms are only bolded the first time they appear in the answer.
If the listed FAQ is further explained in another FAQ, the number of the other FAQ is in parentheses following the entry of the listed FAQ or may be listed in the answer.
Table of Contents
Exposure Categories, Risk Behaviours
1. What are the exposure categories used for HIV and AIDS surveillance by the Centre for Infectious Disease Prevention and Control (CIDPC) at Health Canada and how are they determined? (See also FAQ 8)
2. Are the exposure categories used by the Centre for Infectious Disease Prevention and Control (CIDPC) different from those used by the provinces and territories? (See also FAQs 1, 8)
3. How are the exposure categories used in reporting HIV/AIDS surveillance data different from reported risk behaviours? (See also FAQ 1)
HIV Testing
4. What is the difference between non-nominal HIV testing and anonymous HIV testing?
Notification and Reporting of Positive HIV Test Results and AIDS Diagnoses
5. What does it mean when AIDS and HIV infection are described as notifiable diseases?
6. When a person receives an AIDS diagnosis, who will be notified?
7. If a person tests positive for HIV, who will be notified?
8. Do all provinces and territories submit the same information relating to AIDS diagnoses and positive HIV test reports?
9. Do all provinces and territories use a standardized HIV and AIDS reporting form? If not, how does this affect the accuracy of the data reported in the Epi Updates and Surveillance reports?
10. How long does it take before a positive HIV test result appears in national HIV statistics?
11. Will positive HIV test results be counted more than once at the national level if a person is tested both anonymously and using their name, or if a person tests positive in more than one province or territory?
12. In reporting HIV/AIDS data:
a) What is the definition of a pediatric case?
b) Why are children defined as less than 15 years of age and adults 15 years of age and older?
c) Why are AIDS surveillance data for adults divided into 5-year groups?
Limitations in HIV/AIDS Reporting
13. Are all positive HIV test results reported? If not, which do not get included in the Surveillance Report and Epi Updates?
14. What limitations affect the reporting of HIV and AIDS data?
15. What methods are used by the Centre for Infectious Disease Prevention and Control (CIDPC) to take account of data limitations? (See also FAQ 14)
16. The definition of AIDS has changed over time. How does the Centre for Infectious Disease Prevention and Control (CIDPC) account for these changes when reporting AIDS data?
17. Are comparisons of AIDS statistics between countries limited by different definitions of AIDS?
Positive HIV Test Reports, HIV Incidence and New HIV Diagnoses
18. a) Is there a difference between positive HIV test reports and HIV incidence?
b) Is there a difference between positive HIV test reports and new HIV diagnoses?
HIV Incidence and HIV Prevalence
19. What is the difference between HIV incidence and HIV prevalence?
20. How does the Centre for Infectious Disease Prevention and Control (CIDPC) estimate national HIV incidence and HIV prevalence? (See also FAQ 19)
21. How accurate are the national incidence and prevalence estimates of Canadians living with HIV infection?
22. How do you know that up to one-third of prevalent HIV infections may be undiagnosed? (See also FAQ 20)
Epidemiology and Surveillance
23. What is the difference between the terms epidemiology and surveillance?

Exposure Categories, Risk Behaviours
1. What are the exposure categories used for HIV and AIDS surveillance by the Centre for Infectious Disease Prevention and Control (CIDPC) at Health Canada and how are they determined? (See also FAQ 8)
CIDPC uses exposure categories in HIV/AIDS surveillance to keep track of the most likely route through which HIV was transmitted.
In discussing an HIV test with a health care provider, a person may report one or several behaviours known to carry a risk of HIV infection (risk factors). Even though all risk factors associated with a positive HIV test result are included in the positive HIV test report and entered into the national HIV/AIDS database, only one exposure category is assigned to a positive HIV test report for national reporting. That exposure category will correspond to the activity or situation (risk factor) that is considered to have the highest risk of HIV transmission of all those that the person has reported to a health care professional during HIV testing.
The exposure categories are listed in an exposure category hierarchy. The categories are listed from the one considered to carry the highest risk of HIV infection to the one considered to carry the lowest risk.
The exposure categories currently in use in Canadian HIV/AIDS surveillance and reporting are described in the TERMS section under the term "EXPOSURE CATEGORY".
2. Are the exposure categories used by the Centre for Infectious Disease Prevention and Control (CIDPC) different from those used by the provinces and territories? (See also FAQ 1 and FAQ 8)
In Canada, collection of AIDS surveillance data is the responsibility of each provincial or territorial health authority. The same applies to the collection of HIV surveillance data in provinces or territories where HIV infection is notifiable. As a result, exposure categories used for data collection may vary slightly among provinces and territories and from those reported in a national summary by CIDPC.
It is important to recognize that provincial and territorial surveillance co-ordinators and CIDPC representatives meet regularly to ensure agreement on the definitions and assignment of exposure categories used at the national level.
3. How are the exposure categories used in reporting HIV/AIDS surveillance data different from reported risk behaviours? (See also FAQ 1)
In discussing an HIV test with a health care provider, a person may report one or several behaviours known to carry a risk of HIV infection (risk factors). However, the risk factors will be used to assign only one exposure category to a positive HIV test report for national reporting.
It is important to note that this assigned exposure category is the most likely way that the individual became infected with HIV according to the exposure category hierarchy. It is possible for someone who has engaged in more than one HIV-related risk behaviour to have contracted HIV through one of the other HIV transmission routes listed as risk factors.
HIV Testing
4. What is the difference between non-nominal HIV testing and anonymous HIV testing?
In both non-nominal HIV testing and anonymous HIV testing the name of the person being tested is not used. However, there are some differences between these two types of testing for HIV infection.
Although it varies by province and territory, in general, the differences are that in anonymous HIV testing, the person ordering the test usually does not know and does not want to know the identity of the person being tested. The person ordering the test and the laboratory carrying out the testing on the blood sample use only a code, and they do not know to whom the code belongs. If the person being tested wants an anonymous HIV test, he or she would need to go to a specialized clinic, where the identity of the person being tested is unknown to those who order the test and no personal information is recorded. In contrast, in non-nominal HIV testing, although the test may be ordered using a code or the initials of the person being tested, the person ordering the test knows the identity of the person being tested. For example, if the person being tested goes to their health care provider to request an HIV test but does not want the test ordered using his or her name, the test would be considered non-nominal. The test would not be anonymous however, as the health care provider who ordered it knows the identity of the person being tested and could contact that person if required.
A second difference between these two types of HIV testing lies
in how the information relating to a positive HIV test result is
recorded in the health care record of the person being tested. If
the test is ordered anonymously, test results are not
recorded. It is only the person being tested who may decide to
include the test result in the health care record. In contrast, in
non-nominal HIV testing, the information relating to a positive HIV
test is entered into the health care record of the person
being tested.
The other major difference between these two types of testing is the availability of anonymous HIV testing. Whereas non-nominal HIV testing is available in all provinces and territories, anonymous HIV testing is available in only eight provinces (British Columbia, Alberta, Saskatchewan, Ontario, Quebec, New Brunswick, Nova Scotia and Newfoundland and Labrador). This information was collected in a 1998 survey of all provinces and territories. Usually, anonymous HIV testing is only available in specialized clinics, organized and supported by local public health departments. In British Columbia, anonymous HIV testing is available in any physician's office.
|
Availability of anonymous,
non-nominal/non-identifying, |
|||
|
Province/territory |
Anonymous HIV testing |
Non-nominal/ |
Nominal/ |
|
British Columbia |
|
|
|
|
Yukon Territories |
|
|
|
|
Alberta |
|
|
|
|
Northwest Territories |
|
|
|
|
Nunavut |
|
|
|
|
Saskatchewan |
|
|
|
|
Manitoba |
|
|
|
|
Ontario |
|
|
|
|
Quebec |
|
|
|
|
New Brunswick |
|
|
|
|
Nova Scotia |
|
|
|
|
Prince Edward Island |
|
|
|
|
Newfoundland and Labrador |
|
|
|
|
1 Based on a survey conducted in 1998. |
|||


More information on anonymous and non-nominal/non-identifying as well as nominal/name-based HIV testing is available in the TERMS section under the term "HIV TESTING OPTIONS".
Notification and Reporting of Positive HIV Test Results and AIDS Diagnoses
5. What does it mean when AIDS and HIV infection are described as notifiable diseases?
A notifiable disease is a disease that, by law, must be reported to the public health authority in the area in which the diagnosis is made. Please refer to the TERMS section under the term "NOTIFIABLE DISEASE" to obtain additional information for this question.
6. When a person receives an AIDS diagnosis, who will be notified?
AIDS is a notifiable disease. This means that, by law, a new AIDS diagnosis must be reported to the public health authority in the area in which the diagnosis was made. Information must be sent first to the local health department then to the provincial or territorial health authority. The province or territory then sends selected information to the Centre for Infectious Disease Prevention and Control (CIDPC). The stages in notifying an AIDS diagnosis are best explained by use of the figure below:
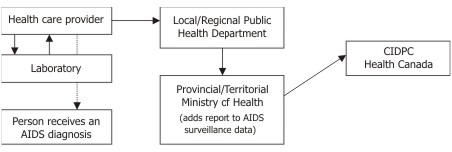
The information reported to CIDPC does not include names nor is it identifying. However, the information reported may include
1. demographic data, such as
- the person's age;
- the person's gender;
- his or her city of residence;
- the name of the diagnosing health care provider;
- the country of birth; and
- ethnicity.
2. risks associated with the transmission of HIV, listing possible ways the person may have become infected with HIV; and
3. laboratory data, which may include information on the date of the person's first positive HIV test result and the disease that defined the AIDS diagnosis.
7. If a person tests positive for HIV, who will be notified?
The law requires that information relating to a positive HIV test result be sent to the local health department and the provincial or territorial health authority in all provinces and territories except British Columbia (HIV infection became notifiable in Quebec on April 18, 2002). However, HIV infection is not legally notifiable at the national level by any Canadian province or territory.
Although notification of positive HIV test results to the Centre for Infectious Disease Prevention and Control (CIDPC) by provincial or territorial health authorities is not legislated by law, notification is voluntarily undertaken by all provinces and territories where HIV infection is notifiable. In addition, CIDPC receives information relating to positive HIV test reports from the provincial laboratory in British Columbia and Quebec. All positive HIV test reports are provided non-nominally to CIDPC. The information on what may be included in the report is available in FAQ 6.
8. Do all provinces and territories submit the same information relating to AIDS diagnoses and positive HIV test reports?
In Canada, collection of HIV/AIDS surveillance data is not carried out by the Centre for Infectious Disease Prevention and Control (CIDPC). Collection of AIDS surveillance data is the responsibility of each provincial or territorial health authority. The same applies to the collection of HIV surveillance data in provinces or territories where HIV infection is notifiable. As a result, each provincial or territorial health authority will not necessarily collect the same data. Thus, CIDPC does not receive the same surveillance data from each province and territory.
It is important to note, however, that most provinces and territories use a standardized form to report AIDS diagnoses. More information on the forms used to report to CIDPC is available in FAQ 9.
Some provinces and territories provide more information than others when notifying CIDPC of an AIDS diagnosis and a positive HIV test report. This particularly applies to information on ethnicity, age, and exposure category.
Ethnicity
Among some provinces and territories, the ethnic category is either not provided, is incomplete, or is generalized. For example, some provinces and territories report general ethnic categories such as Aboriginal person, while other provinces and territories report more specific ethnic information such as Inuit. Information on ethnicity associated with reported AIDS diagnoses (AIDS case reports) has improved since reporting of AIDS began. Since the beginning of reporting to the end of the year 2001, approximately 85% of AIDS case reports contained ethnic origin.
Age
When reporting the age of the person with a positive HIV test
result, some provinces and territories will report an age group as
opposed to a specific age. For example, some may report the age as
24 years, while other provinces and territories may report 20-29
years.
Exposure category (See also FAQ 2)
There is variation among provinces and territories in terms of assigning an exposure category. For both AIDS and HIV,
- reports may be received at CIDPC with an exposure category already assigned by the province or territory;
- reports may be received at CIDPC with only a list of risk factors, used to assign only one exposure category for national reporting;
- reports may be received at CIDPC with no information at all on the possible way or ways by which the person became infected with HIV.
If risk factor information is available, CIDPC assigns the exposure category associated with the greatest risk of HIV transmission. Reports with no risk factors recorded are assigned to the "NIR" (no identified risk) exposure category. The assigned exposure category is then compared with the exposure category assigned by the province or territory, if one is available. If the national and provincial/territorial exposure category assignments do not match, the report will be followed up with the province or territory to determine the most accurate of the two exposure category assignments. Provinces and territories may have information available to them that was not forwarded to CIDPC.
9. Do all provinces and territories use a standardized HIV and AIDS reporting form? If not, how does this affect the accuracy of the data reported in the Epi Updates and Surveillance reports?
When AIDS surveillance first began, the Centre for Infectious Disease Prevention and Control (CIDPC) developed an AIDS Case Report Form in consultation with the provinces and territories to encourage standardized AIDS data reporting. In 1996-97 the name of the form was changed to the HIV/AIDS Case Report Form as the need for HIV surveillance at the national level was recognized.
Some provinces and territories use this form to record information, some use their own form. Regardless of the reporting form used, CIDPC receives selected information from each province and territory as described in FAQ 6.
The accuracy of the data reported in surveillance-related documents is limited by the differences in HIV/AIDS reporting among provinces and territories. As described in FAQ 8, these differences are not specifically related to the form itself but to differences in reporting completeness, and recording and interpretation of information.
10. How long does it take before a positive HIV test result appears in national HIV statistics?
Depending on the time of the year the HIV test took place, the Centre for Infectious Disease Prevention and Control (CIDPC) usually receives the positive HIV test report in the same year.
There may be a time lag between the time of testing and the time at which the positive HIV test report is entered into the national HIV/AIDS surveillance database. A positive HIV test report travels through several steps from the health care provider to the local health department and then to the provincial or territorial health authority before it is received by CIDPC. The positive HIV test report can be held up at any or each of these steps for a variety of reasons, including technological limitations as well as time and staffing constraints. This results in a delay between the time of testing and the time at which the positive HIV test report is entered into the national HIV/AIDS surveillance database. This time lag is frequently referred to as a reporting delay.
Consequently, because of reporting delays, the most recent positive HIV test reports may not be included in the current year's surveillance reports. However, as CIDPC continues to receive positive HIV test reports from previous years, national HIV/AIDS surveillance data are updated to reflect the year in which the HIV test was conducted. For example, if a person tested positive for HIV in 1990, but the positive HIV test report was not received at CIDPC until 1991, the positive HIV test report would be recorded for the year 1990 and not 1991.
11. Will positive HIV test results be counted more than once at the national level if a person is tested both anonymously and using their name, or if a person tests positive in more than one province or territory?
A person who undergoes testing for HIV more than once is referred to as a "repeat tester". If this person is tested for HIV both anonymously and using their name and the result is positive, it is possible that more than one positive HIV test report is contained in the national HIV/AIDS surveillance database for this person.
Similarly, if a person tests positive for HIV each time with a different health care provider either in the same province or territory or in different provinces or territories, it is possible that more than one positive HIV test report is contained in the national HIV/AIDS surveillance database for this person.
In both cases, these are called "duplicate tests". The inclusion of duplicate positive HIV test reports affects the accuracy of the information contained in the national HIV/AIDS surveillance database. For example, the number of positive HIV test reports will be higher, and some demographic groupings may be under- or over-represented.
Within provinces and territories, provincial and territorial surveillance co-ordinators attempt to identify and remove duplicate positive HIV test reports before the data are submitted to the Centre for Infectious Disease Prevention and Control (CIDPC). However, identifying and subsequently removing duplicate positive HIV test reports is difficult because of the non-nominal (without a name) or non-identifying nature of HIV infection reporting in some provinces and territories.
Provincial and territorial files are also reviewed for duplicates at the national level. This is done by determining whether the age and gender of one report match those of a previously entered report. Where there is a match, other information relating to the person will be looked at to see whether or not the new report is really a duplicate.
If a duplicate is suspected, the provinces and territories involved are notified, and the decision as to where the report will be attributed is made between the provinces and territories involved. Generally, positive HIV test reports and AIDS diagnoses are assigned to the province or territory in which the person was living at the time of the positive HIV test or at the time at which the AIDS diagnosis was made.
12. In reporting HIV and AIDS data :
a) What is the definition of a pediatric case?
An AIDS case report or a positive HIV test report is described as pediatric if the person received a diagnosis of AIDS or tested positive for HIV before his or her 15th birthday.
Pediatric cases are included in both the HIV and AIDS section of the surveillance report. For AIDS, information is reported on children of all ages and from all provinces and territories. However, this is not the case for HIV.
Surveillance of HIV infection in children is more challenging than surveillance of AIDS, because children under two years of age (infants) can test positive (seropositive) at the time of their first HIV test but may test negative (seronegative) in subsequent HIV tests. This is a result of the circulating maternal antibodies in the blood. As a result, HIV surveillance information on infants needs to be monitored very carefully.
Monitoring these changes in serostatus is difficult because,
for most provinces and territories, HIV information on children
under two years of age cannot be separated out from the data
received by the Centre for Infectious Disease Prevention and
Control (CIDPC). Data are received as one group of all children
under 15 years of age. Therefore, CIDPC does not have the ability
to follow children under two years of age. CIDPC can only remove
children under two years of age from the data received from British
Columbia, Quebec and, since 2000, Ontario. Thus, in the HIV section
of the surveillance report, pediatric cases include data on
children under two years of age except for the data specific to
these three provinces.
In order to carefully monitor changes in the serostatus of children under two years of age, a separate initiative was started with the purpose of collecting HIV surveillance data only on infants. Information on infants known to be exposed perinatally to HIV infection is obtained through a national non-nominal, confidential survey of infants known to pediatricians in tertiary care centres and HIV specialists in HIV clinics across Canada. These data are collected from all provinces and territories by the Canadian Perinatal HIV Surveillance Program, coordinated by the Canadian Pediatric AIDS Research Group (CPARG). Support for the program is provided by the Canadian HIV Trials Network and CIDPC. The data from this source are reported in a separate section in the surveillance reports produced by CIDPC.
b) Why are children defined as less than 15 years of age and adults 15 years of age or older?
This definition is used because the Centre for Infectious Disease Prevention and Control (CIDPC) sometimes receives only age group data for positive HIV test reports (i.e., not individual ages) from provinces and territories. Often, these age group data are not well defined for people aged 0 to 14 years.
This definition of "children" is also applied to AIDS case reports to allow them to be compared and contrasted with HIV data.
More information on grouped data is available in FAQ 8.
c) Why are AIDS surveillance data for adults divided into 5-year groups?
Five-year age groupings for AIDS surveillance data are consistent with the surveillance guidelines developed by the World Health Organization/Joint United Nations Programme on HIV/AIDS (WHO/UNAIDS).
Limitations in HIV/AIDS Reporting
13. Are all positive HIV test results reported? If not, which do not get included in the Surveillance Report and Epi Updates?
The information relating to positive HIV test results contained in the national HIV/AIDS database and reported in the Epi Updates and Surveillance Reports is limited to those positive HIV tests reported to the Centre for Infectious Disease Prevention and Control (CIDPC).
The positive HIV test results that are reported to CIDPC are from only those
- who test positive for HIV through nominal, non-nominal or anonymous testing in British Columbia and Quebec and whose results are reported to CIDPC by their provincial testing laboratories;
- who test positive for HIV through nominal, non-nominal or anonymous testing in all other provinces and territories and whose results are reported to their local health department and subsequently to CIDPC by the provincial or territorial health authority.
The positive HIV test results that are not included in the Surveillance Report and Epi Updates are those that are not reported to CIDPC. The reasons why some positive HIV test reports are not reported are further explained in FAQ 14.
14. What limitations affect the reporting of HIV and AIDS data?
A data limitation is something that may affect the accuracy of data.
It is important to keep data limitations in mind when reading reports describing surveillance data. Some limitations that affect the reporting of HIV and AIDS data in Canada include the following.
Ethnicity Data
Not all provinces or territories routinely collect or report data on ethnic origin. Many of the data reported on ethnic origin at the national level vary in completeness and may result in underrepresentation among certain communities. Such data may also vary in accuracy, as ethnicity reporting is restricted to predefined ethnic categories and thereby limits the choice of ethnic designation. In addition, many individuals may not wish to self-identify to a specific group.
Underreporting
The number of reported AIDS cases and positive HIV test reports at any point in time is not a true reflection of the total number of people living with AIDS or HIV infection. This is because
- some individuals do not come forward after HIV testing but may be positive for HIV;
- some AIDS diagnoses and positive HIV test reports never get reported to provincial or territorial health authorities or to the Centre for Infectious Disease Prevention and Control (CIDPC).
Reporting Delay
There is often a substantial delay between the time at which a person tests positive for HIV or receives a diagnosis of AIDS and the time at which the report of that diagnosis is received by the Centre for Infectious Disease Prevention and Control (CIDPC). For additional information on reporting delay, please refer to FAQ 10.
Death Reports
Legislation requires registration of all deaths, regardless of cause, with the provincial and territorial registrars of the Offices of Vital Statistics. As a result, underreporting of deaths for which the underlying cause of death is HIV infection is minimal. The information collected is available annually by Statistics Canada.
The number of deaths among reported AIDS cases published in surveillance documents produced by CIDPC is a significant underestimate. There are a couple of reasons for this.
First, death is not a mandatory variable to be reported in the HIV/AIDS surveillance system in any Canadian province or territory or to CIDPC. As a result, the death of a person may not be reported at all (underreporting), or there may be a delay in the death report reaching CIDPC (reporting delay). Even though a health care provider may list AIDS as a cause of death in the medical record or on the death certificate, this information may never be reported to CIDPC as an "update". It is these updates that are reported in surveillance documents as deaths due to AIDS.
Second, deaths due to causes other than AIDS are less likely to be reported to CIDPC than deaths due to AIDS. For example, if a person living with AIDS died in a car collision, CIDPC may be less likely to receive an update than if the person died directly as a result of AIDS.
CIDPC is able to report information on deaths of AIDS cases only when they are linked to a previous AIDS case report. Without active follow-up, the health care provider completing the AIDS case report may not know whether a person has died, moved or just changed health care providers.
Duplicate Reports
The removal of duplicate positive HIV test reports is difficult because of the non-identifying nature of some positive HIV test results. However, all provinces and territories rule out duplicate reports as much as possible. If duplicate reports are missed, surveillance data may overestimate the number of positive HIV test reports.
For additional information on duplicate reports, please refer to FAQ 11.
HIV Reporting among Children under Two Years of Age (Infants)
Infants who are seropositive at the time of their first HIV test may, in fact, be seronegative on subsequent HIV tests. As any positive HIV test report for an infant has historically been included in the data for children, this may have resulted in an overestimate of HIV infection among children. However, CIDPC monitors any reported changes in the serostatus of infants, and the surveillance data for children are updated to reflect this change.
See FAQ 12 for further information on HIV
infection reporting among children under two years of
age.
15. What methods are used by the Centre for Infectious Disease Prevention and Control (CIDPC) to take account of data limitations? (See also FAQ 14)
There are some common statistical methods used by CIDPC to take account of data limitations and improve the accuracy of reported data.
For example, statistical methods are used to estimate and adjust for underreporting and to estimate and adjust for reporting delays. These adjusted numbers take into account regional variations in reporting delay.
As HIV and AIDS surveillance data do not provide the entire picture of people living with HIV infection, CIDPC also produces estimates of prevalence and incidence. For additional information on the methods used to estimate HIV prevalence and incidence, please refer to FAQ 20.
16. The definition of AIDS has changed over time. How does the Centre for Infectious Disease Prevention and Control (CIDPC) account for these changes when reporting AIDS data?
The definition of AIDS has changed only slightly since AIDS surveillance began. However, the national AIDS surveillance database has not been adjusted to take account of these changes. All reports of AIDS fall under the definition of AIDS that was current at the time of the AIDS diagnosis. Once in the database, the AIDS case report remains in the database. Information recorded on the reporting form also does not change.
The definition of the Canadian AIDS diagnosis has changed over time as more information has been gathered on the disease. In general, the definition has expanded to include additional diseases indicative of AIDS. This means that some cases that now fit the criteria for an AIDS diagnosis may not have fit the narrower criteria used in the past. For example, before 1993, AIDS would not have been diagnosed in an HIV positive individual who also had tuberculosis disease. Yet, this same person would now be considered to have AIDS, as the current definition for AIDS includes a diagnosis of tuberculosis disease in an HIV positive individual.
CIDPC considers this a limitation to the AIDS database. However, as the definition of AIDS has changed only slightly since surveillance began, the effects are considered to be minimal. For more information on data limitations, please see FAQ 14.
17. Are comparisons of AIDS statistics between countries limited by different definitions of AIDS?
Comparisons of AIDS statistics between countries are difficult because of the differences in the definition of AIDS and the different surveillance methods used between countries.
The definition of AIDS used in Canada is based on guidelines set by the Centers for Disease Control and Prevention in the United States. However, it is important to note that in contrast to the U.S. AIDS case definition, the list of specific disease indicators required for a Canadian AIDS diagnosis does not include a CD4 T-lymphocyte count less than 200 cells per cubic millimetre of blood (< 200/µL).
The definitions of AIDS used in other countries are based on different guidelines. Although global differences between guidelines and therefore the definition of AIDS exist, these differences are small.
The methods used to collect, analyze and report HIV/AIDS surveillance data may also vary from country to country.
Positive HIV Test Reports, HIV Incidence and New HIV Diagnoses
18. a) Is there a difference between positive HIV test reports and HIV incidence?
Yes. HIV incidence refers to the number of people who recently contracted HIV and is reported for a specific period of time - that is, the number of new HIV infections in that time period. Positive HIV test reports, on the other hand, are a reflection of the number of positive HIV tests that have been reported to public health authorities. They also apply to a specific period of time - that is, in documents produced by the Centre for Infectious Disease Prevention and Control (CIDPC), positive HIV test reports include only those people who have been tested (positive) and, of those, only the people for whom a report was received at CIDPC. It is also important to note that positive HIV test reports refer to the time of diagnosis of HIV infection, not to the time of infection with HIV, which may have been much earlier.
It is important not to confuse these two terms. HIV incidence refers to the number of new HIV infections per year. However, positive HIV test reports refer to the number of new diagnoses of HIV infection that are reported per year.
For example, in 1999, there were an estimated 4,190 Canadians newly infected with HIV (HIV incidence). There were 2,239 new diagnoses of HIV infection reported in Canada (positive HIV test reports) in 1999.
b) Is there a difference between positive HIV test reports and new HIV diagnoses?
As not all new HIV diagnoses will be reported to public health authorities, the number of positive HIV test reports will be an underestimate of the actual number of new diagnoses of HIV infection.
HIV Incidence and HIV Prevalence
19. What is the difference between HIV incidence and HIV prevalence?
HIV incidence is the number of new HIV infections occurring during a specified period of time while HIV prevalence is the total number of cases of HIV infection at a particular point in time. HIV prevalence can also be described as the total number of people living with HIV infection (including those living with AIDS) at a particular point in time.
In the area of HIV/AIDS research, prevalence gives us an idea of how many people are currently living with HIV infection, and incidence gives us a sense of how many people are newly infected, that is, how fast the HIV epidemic is growing.
20. How does the Centre for Infectious Disease Prevention and Control (CIDPC) estimate national HIV incidence and HIV prevalence? (See also FAQ 19)
Surveillance data relate only to HIV positive individuals who seek testing or medical care and whose positive HIV test was reported to public health authorities. Therefore, these data do not represent the total number of people who become infected with HIV each year (incidence) or the total number of people living with HIV infection (prevalence).
To take account of this, national HIV incidence and prevalence are estimated using direct and indirect methods. These methods use data from a wide variety of sources, such as provincial HIV testing databases, population-based surveys, targeted epidemiological studies, and census data.
The direct method estimates incidence and prevalence using epidemiological studies among specific population groups. These estimates are then multiplied by the estimated population at risk. Sizes for estimated populations at risk are obtained through a variety of methods, including projected population estimates, population-based surveys, and census data.
Two indirect methods are used together to estimate HIV prevalence. They are both based on the number of positive HIV diagnoses obtained from provincial HIV testing databases, and on information relating to HIV testing behaviour obtained from population surveys.
HIV incidence is also estimated using another indirect method. This method estimates HIV incidence by taking the difference between the two most recent prevalence estimates and adding the number of AIDS deaths that occurred between the two prevalence estimates. The result is an estimate of the number of new infections.
For further information on the national estimates for HIV prevalence and incidence, please refer to the reference listed for the Bureau of HIV/AIDS, STD and TB, Centre for Infectious Disease Prevention and Control, Health Canada, 2001a, at the back of the guide.
21. How accurate are the national incidence and prevalence estimates of Canadians living with HIV infection?
The methods used to estimate HIV prevalence and incidence among Canadians make maximum use of a wide variety of data sources, including AIDS case reports, provincial HIV testing databases, population-based surveys, epidemiological studies, and census data. The estimates are inevitably imprecise, but using several methods of estimation in a combined approach improves their accuracy. The advantages of the approach are its flexibility, and its ability to incorporate new data and to highlight gaps in existing knowledge.
The fact that the methods used to estimate national
trends in HIV
infection are largely determined by data collected from large
cities is a limitation. These estimates may not therefore
necessarily reflect local trends of HIV incidence and prevalence in
Canada.
22. How do you know that up to one-third of prevalent HIV infections may be undiagnosed? (See also FAQ 20)
The Centre for Infectious Disease Prevention and Control (CIDPC) has estimated the number of people who may be infected with HIV but are unaware of their infection - that is, the number of people who are living with HIV infection but whose infection has not been diagnosed.
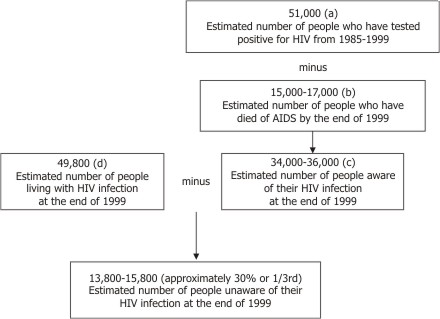
Several steps are involved in estimating the number of HIV infections that may be undiagnosed. The steps follow and are also represented in an example given in the diagram below.
1. The total number of Canadians (a) who tested positive for HIV and (b) who died from AIDS are first estimated. This is done by adjusting the numbers reported to CIDPC to take account of underreporting and delayed reporting. (Underreporting and delayed reporting are explained in FAQ 14.)
2. The estimated number of people who have died from AIDS (b) is subtracted from the number of people who have tested positive for HIV (a). The result is the total number of people who are aware of their HIV infection and are living (c). That is, their HIV infection has been diagnosed.
3. The total number of people living with HIV infection, either aware/diagnosed or unaware/undiagnosed (d) is then estimated. This is done by using a combination of different sources and methods. These are described in FAQ 20.
4. The total number of people who are aware of their HIV infection and are living (c) is then subtracted from the estimated total number of people living with HIV infection (d) - that is, both those aware/diagnosed and unaware/undiagnosed.
This results in an estimated number of undiagnosed HIV infections (those living with HIV infection but who have not yet been tested).
Epidemiology and Surveillance
23. What is the difference between the terms epidemiology and surveillance?
Epidemiology refers to the study of the occurrence, distribution and determining factors associated with the health and disease of a population - that is, the study of how often diseases or health events occur in different groups and why.
Surveillance is a key component of epidemiology. It can be defined as the ongoing collection, analysis, interpretation and dissemination of health related data such as data about HIV infection. In simpler terms, surveillance is "counting" the who and where of disease and "looking" at the patterns of disease. Surveillance is one of a number of methods used by epidemiologists to gather information on a disease such as HIV infection.
For example, an epidemiological study might examine behaviours that place people at risk of HIV infection (risk factors) or might investigate the people who display these risk behaviours. If researchers first wanted to determine the group of people that accounts for the greatest number of positive HIV test reports, they would look to surveillance data.
[Previous] [Table of Contents] [Next]