
Public Health Agency of Canada
www.publichealth.gc.ca
Common menu bar links
Institutional links
Diseases & Conditions
Health & Safety
Research & Statistics
Agency Information
Search Box
E-mail this page
Report 3 - Exploring the Link Between Work-Life Conflict and Demands on Canada's Health Care System
Chapter 5 - How Does Work-Life Conflict Affect the Use of Canada's Health Care System?
The following research questions are addressed in this chapter of the report:
- To what extent are Canadian employees making use of the various facets of Canada's health care system?
- What is the impact of gender, job type, sector of employment and dependent care status on the use of Canada's health care system?
- How does work-life conflict (operationalized to include role overload, work to family interference, family to work interference and caregiver strain) affect the use of Canada's health care system?
The data discussed in this chapter of the report can be found in the appendices at the end of the report. They are also shown graphically in Figure 4.
This chapter is divided into eight parts. Data on Canadian employees' use of the health care system are addressed and discussed in Section 5.1 to Section 5.6. These six sections are grouped as follows: the first three sections (5.1 to 5.3) deal with visits to health care professionals (visits to the physician are discussed in Section 5.1 followed by visits to other types of health care professionals (5.2) and visits to mental health professionals (5.3). The next three sections (5.4 to 5.6) deal with the use of different types of facilities (inpatient care in hospital [5.4], visits to the emergency department [5.5], and outpatient care in clinics or hospitals [5.6]). Included in each of these sections is a discussion of how gender, job type, dependent care status and sector of employment are associated with each dimension of health care system use. The link between the use of the health care system and work-life conflict is made in Section 5.7 and a summary of the key findings with regard to use of the health care system is given in Section 5.8.
Figure 4
Percentage of Respondents Using Different Facets of the Health Care
System
(a) Visits to Physician, Use of Emergency Department, Medical Tests
on Outpatient Basis
5.1 Visits to the Physician
The delivery of health care, even when broadly defined, is primarily the responsibility of the family physician (Statistics Canada, 1999). While many models of primary health care exist, physician-centred solo and small group practice is the norm in Canada, and most Canadians turn to their family doctor for both routine, ongoing care and immediate care for minor health problems (CIHI, 2003).
Almost every Canadian interfaces with our health care system. In 2001, more than 23 million Canadians aged 15 or older (i.e. 94% of the population) accessed at least one type of first-contact health services. The primary reasons for seeking care included routine or ongoing care, immediate care for a minor health problem and/or health information or advice (CIHI, 2003). Where Canadians turn first for care depends very much on when they need help. Family doctors' offices are the leading place for care during regular office hours while hospital emergency departments are the point of first entry when problems arise at night (CIHI, 2003).
Recent estimates (CIHI, 2002) show that in 2000-01, 78% of Canadians aged 12 or older indicated that they had consulted a family doctor at least once in the past year. Data in the Medical Care Database and the National Physician Database (based on claims submitted by the fee-for-service physicians to provincial medical programs) indicate that the number of physician visits per insured Canadian have increased over time: from 4.5 per year in 1978-79 to 6.0 in 1993-94 (CIHI, 2003). Statistics Canada (1999) reports that in 1998 women between the ages of 18 and 54 were two to three times more likely than their male cohorts to have visited a physician.
Figure 4
Percentage of Respondents Using Different Facets of the Health Care
System
(b) Inpatient Hospital Stays, Visits to Mental Health
Professionals
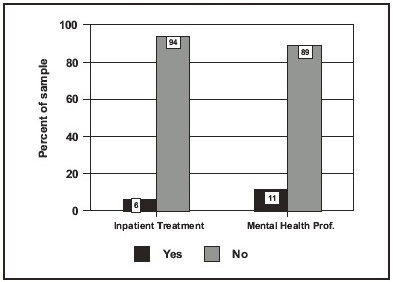
Figure 4
Percentage of Respondents Using Different Facets of the Health Care
System
(c) Visits to Other Health Care Professionals
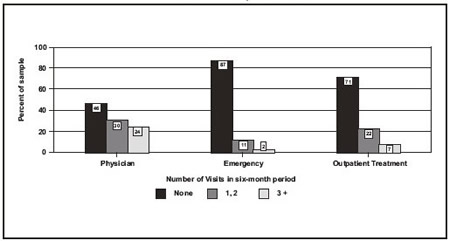
Half of the employees in this sample saw their physician in the past six months23
Just over half (54%) of the respondents sought care from their physician in the six months prior to the survey being conducted. One in four of these individuals visited his or her physician three or more times during this time period. In the following discussion, these individuals are considered to be "heavy" users of physician services.
The mean number of visits per employee was 1.5 in a six-month period or approximately 3 visits per year. The mean number of visits made in a six-month period by those who sought care was 2.9.
Women are more likely than men to have visited the physician
Women were substantially more likely than men to have sought care from a physician in the six months prior to the study being done. They also made more visits in a six-month period. This finding is particularly worthy of note in that it could be observed regardless of job type, dependent care responsibilities or sector of employment. Since there were no gender differences in perceived health and women were asked not to include maternity-related visits or check-ups in their total, it is hard to determine exactly what this finding reflects. Three explanations are plausible:
- Women are more likely than men to seek care when they are not well (e.g. women are making appropriate use of physician services and men are not seeking treatment for illness),
- Women are more likely to see their physician for non-physical concerns (e.g. counselling), or
- Women are more likely to seek treatment for "female" health issues, such as menopause care, menstrual issues and breast screening.
This gender difference in physician visits is almost identical to that reported by Statistics Canada.
Women in "other" positions in the organization are more likely to visit the doctor
Women in clerical and administrative positions within the organization make the greatest use of physician services (58% of the respondents in this group had visited a physician in the six months prior to the study being done compared to 56% of females in managerial/professional positions, 51% of men in "other" positions, and 50% of male managers and professionals).
The trends observed with respect to mean (X) number of visits to the physician are almost identical to those reported with respect to likelihood of use. Females in "other" positions made significantly more visits on average in a six-month period (X of 1.74) than women in managerial and professional positions (X = 1.57), male managers and professionals (X = 1.33 visits) and men in "other" positions (X = 1.39).
It is interesting to note that, while job type is associated with physician visits for the women in the sample (females in "other" positions are more likely to visit the physician than female managers and professionals), no such difference was noticed for the men in the sample. There are several plausible explanations for this finding (see Appendix B). First, it may be that managerial and professional jobs offer a health advantage to women. Alternatively, it may be that clerical and administrative jobs (i.e. pink collar jobs) have a more deleterious impact on the health of women than blue collar jobs do on the health of men. Finally, it is also possible that women in clerical and administrative positions who make the most visits to the physician have long-standing health issues which reduce their ability to advance in the organization.
Visits to the doctor not associated with dependent care status
Surprisingly, when gender is taken into account, dependent care status is not associated with the use of physician services. This runs counter to the popular belief that employees with children have a greater exposure to illness (e.g. children are a source of contagion in the family) and suffer poorer health as a consequence.
While women with dependent care were more likely than any other group to visit the physician (57% visited the physician in the six months prior to the study being conducted; X of 1.7 visits in six-month period), their use is not substantially higher than that observed for women without dependent care (56% visited the physician in the six months prior to the study being conducted; X of 1.6 visits in a six-month period). Similar findings were observed with respect to the men in the sample (49% of the men without dependent care and 50% of the men with dependent care visited the physician in the six months prior to the study; both groups of men made an average of 1.3 visits during this time period).
Public sector employees are more likely to have seen a physician
When gender is taken into account, it can be seen that public sector employees are more likely to have visited a physician than their counterparts in the private and NFP sectors. They also made more visits within a six-month period than employees in the other sectors. This finding is consistent with the fact that this group of employees was more likely to rate their health as fair/poor. The differences cannot, however, be attributed to age differences within the sector as public sector respondents reported the same age profile as those in the NFP sector. Rather, it may be working conditions within the sector (e.g. lower control, fewer rewards) that are negatively impacting health. Alternatively, it may be that it is easier for public sector employees to take time off work for medical appointments.
Men in the private sector are less likely to visit a physician
Men in the private sector sample were less likely to go to a doctor than any other group in the sample. Only 43% of the men in the private sector sample saw a doctor in the six months prior to the study being done (vs. 52% of men in the public sector sample and 50% of men in the NFP sample). Employees in this group made an average of one visit to a doctor in a six-month period.
5.2 Visits to Other Health Care Professionals
Over the past few years, the use of alternative health care has apparently become much more accepted by the public (Statistics Canada, 1999). More Canadians are turning to homeopathy, chiropractory, herbal products and other healing practices in addition to or instead of orthodox medical treatment (CIHI, 2002). In 2000-01, 60% of Canadians aged 12 or older consulted a dentist/orthodontist, 38% saw an eye specialist, 28% consulted other medical doctors and 19% visited a chiropractor or other type of complementary/alternative health professional. Who is most likely to consult other health care professionals? The data suggest the following groups are more likely: individuals with higher incomes, more highly educated middle-aged women and individuals with chronic conditions (CIHI, 2002).
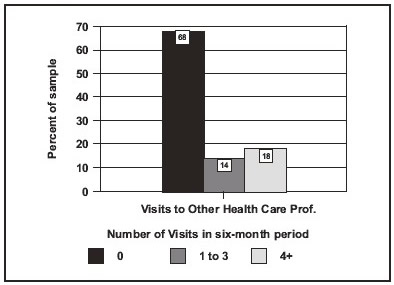
One in three respondents sought help from a health care professional other than a physician
One in three respondents sought medical care from a medical/health professional other than a physician. Just under one in five respondents could, in fact, be considered a heavy user of such care; these respondents made four or more visits in a six-month period. The average number of visits reported by people who sought care from other health care professionals is 5.0 in a six-month period; the average number of visits for the total sample is 1.5 in a six-month period. In other words, for this sample visits to other health care professionals were as frequent as physician visits. From the employer and the government's points of view, however, the use of these types of services has quite different consequences. Since the Canada Health Act does not specifically require the provinces and territories to insure non-physical medical services, such services are often not fully insured or are offered as restricted expenditures in private health plans. In other words, much of the cost of alternative health care services is paid for by employee benefit plans, whereas the costs associated with seeing a physician are borne by the government.
Women are more likely to seek care from other health care professionals
The tendency to seek care from other health care professionals is strongly associated with gender and sector of employment in the following manner:
- men in the private sector sample made less use of other health care professionals (less likely to seek care, fewer visits in a six-month time period) than other respondents, and
- women made more use of other health care professionals (more likely to seek care, more visits to other health care professionals in a six-month time period).
The gender differences are particular worthy of note in that they could be observed regardless of job type or dependent care status. These findings are identical to those noted with respect to visits to a physician and likely have the same underlying etiology.
5.3 Visits to Mental Health Professionals
In almost every Canadian community, family physicians play an important role in handling the mental health problems of their patients. The family physician is usually the first and may be the only contact with the medical system for people with mental health problems (CPA, 2000). The prevalence of mental health disorders in primary care settings is high and approximately one in three family practice patients has mental health problems (CPA, 2000).
It was difficult to get accurate Canadian data on the number of people seeking care from mental health professionals other than physicians. This difficulty can be attributed to the high number of potential sources of such care (e.g. counsellors, psychologists, employment assistance programs), the fact that this service is often not government-funded (e.g. insurance companies, employee benefits plans and individuals often pay for this service) and the fact that there is little cooperation between physicians and other health care professionals with respect to the collection of such data (CPA, 2000; Kates, 2002). Kates (2002) does, however, provide a useful reference point from a recent study done in Ontario which suggests that 35% of people with mental disorders are treated only by their family physicians, 40% are treated by mental health professionals and 25% receive care from both family physicians and mental health workers.
Data from this study relating to this topic are summarized below. It should be noted that we do not know what percent of the visits to a physician reported earlier were to seek care for mental health problems. We can, however, use our data on visits to a mental health professional to give us a conservative estimate24 of the extent to which mental health issues are of concern to Canadian employees.
One in ten employees sought care from a mental health professional
Just over one in ten (10.6%) of the respondents in this sample sought help from a mental health professional in the six months prior to the study being conducted. These individuals made an average of 4.1 visits in a six-month period, suggesting that they required some form of ongoing care. For the total sample, an average of 0.45 visits were made to a mental health professional in a six-month period.
Women are more likely to seek care from a mental health professional
Visits to a mental health professional are strongly associated with gender, with women making more use of this facet of the health care system than men. This finding is particular worthy of note in that it could be observed regardless of job type, dependent care responsibilities or sector of employment and is true with respect to both likelihood of use and number of visits. These findings are identical to those noted with respect to visits to a physician and visits to other health care professionals and likely have the same underlying etiology.
Job type not associated with mental health visits
When gender is taken into account, job type is not associated with visits to mental health professionals-an important finding because studies such as that done by the Whitehall group (e.g. Hemingway et al., 1997; Marmot and Davey, 1997) or Karasek and Theorell (1997) have talked about the stresses associated with working in clerical and administrative positions (i.e. high-demand/low-control jobs). The data from Report Two in this series (Duxbury & Higgins, 2003) would suggest that the disappearance in job type differences in these data can be attributed to the fact that the stresses and demands associated with being a manager/professional have increased over time while the amount of control such individuals wield has declined. There is no evidence that the stresses associated with pink and blue collar work have declined (i.e. that organizations have addressed the concerns of this group of employees).
Employed parents and elder caregivers more likely use services of mental health professionals
When gender is taken into account, employees with dependent care responsibilities were significantly more likely than their counterparts without such responsibilities to seek care from a mental health professional. In the six months prior to the study being conducted:
- 13% of mothers/female elder caregivers sought care compared to 11% of women without children/elder care responsiblities,
- 9% of fathers/male elder caregivers sought care compared to 7% of men without children/elder care responsibilites,
- mothers/female elder caregivers made an average of 0.5 visits to a mental health professional compared to 0.4 visits by women without children/elder care responsibilities,
- fathers/male elder caregivers made an average of 0.4 visits to a mental health professional compared to 0.3 visits by men without children/elder care responsibilities.
These data are very interesting as they indicate that combining work and caregiving responsibilities has a negative impact on the mental (rather than the physical) health of employees. This interpretation of the data is consistent with the fact that the employees in this sample with dependent care responsibilities reported higher levels of stress, burnout and depressed mood than their counterparts without dependent care responsibilities (see Duxbury & Higgins, 2003). It is also consistent with the fact that employees with dependent care responsibilities do not make significantly more use of any other dimension of health care looked at in this study, although they are more likely to rate their health as fair/poor. When these results are looked at through the lens of two of the most common workplace health models (Karesek and Theorell's [1990] Job Strain Model and Siegrist's [1996] High Effort/Low Reward Model), it seems appropriate to label the job of employed parent/elder caregiver as either high demand/low control and/or high effort/low reward. This classification would allow researchers to apply the vast research literature in these areas to the field of work-life conflict.
Women in the public sector make most visits to mental health professionals
The relationship between gender, sector of employment and use of mental health care services is quite complex but consistent with the patterns observed with respect to use of physician services and visits to other health care professionals: men working in the private sector make less use of such services than any other group while women working in the public sector make more use. These findings are likely due to a complex of factors, including age, perceived control, socio-economic status, perceived rewards, etc. Exploring these relationships is beyond the scope of this study.
5.4 Visits to Hospital: Inpatient Care
Inpatient hospital care refers to care requiring admission to a hospital, including general and allied specialty hospitals (Statistics Canada, 1999). Diseases of the circulation system accounted for the most hospital days (18%). Mental disorders accounted for the next highest number-largely because employees with these sorts of problems had very extended hospital stays (31.7 days on average). Women account for more hospital stays than men. Much of this difference can be attributed to women in the childbearing years (Statistics Canada, 1999).
Six percent of the employees in this sample were hospitalized in the past six months
In the six months prior to this study being conducted, 6 percent of the respondents in the sample required inpatient hospital care. This group of individuals spent an average of 2.3 nights in the hospital during this time period. The likelihood of requiring inpatient hospital care is not associated with gender, job type, dependent care status or sector of employment.
5.5 Visits to Hospital: Emergency Department
Emergency health services are generally described as medical services that are provided for health problems that require immediate care. This area of health services includes hospital emergency departments, urgent care centres and paramedical services (Statistics Canada, 1999). Wait time in hospital emergency rooms is often used as an indicator of health service delivery problems. Measuring wait times is a complex task (CIHI, 2003).25
In 1996-97, one in four Canadians (5.3 million) 12 years of age or older reported having used emergency health services at least once during the previous year (Statistics Canada, 1999). Overall, women were slightly more likely than men to use emergency health services (Statistics Canada, 1999).
Just over one in ten respondents sought care at a hospital emergency department
Just over one in ten of the employees in the sample (13%) sought medical care at a hospital emergency department for a personal health problem in the six months prior to this study being done (2% went to the emergency department 3 or more times). Respondents who sought care in an emergency department made an average of 1.6 visits in a six-month period. When the total sample is considered, employees made an average of 0.2 visits to emergency in a six-month period.
Visits to an emergency department were not associated with gender, dependent care or sector
Neither the likelihood of seeking care in an emergency department nor the number of visits made are substantively associated with gender, dependent care status or sector of employment.
Employees in "other" positions were more likely to visit an emergency department
Respondents in managerial and professional positions were substantively less likely to have sought care in an emergency department than their counterparts in "other" positions in the organization (15% of females and 14% of males in "other" positions visited the emergency department in the six months prior to the study being done vs. 11% of men and women in managerial and professional positions). There are several possible explanations as to why employees in "other" positions are more likely to use this form of health care. First, it may be that employees in this group are less likely to have a family practitioner and more likely to rely on emergency room physicians for medical problems and emergencies. This explanation of the data appears to apply to men in "other" positions in particular (i.e. they are more likely than their male counterparts in managerial and professional positions to say their health is fair/poor but no more likely to have visited a physician). Second, it may be that employees in "other" positions find it more difficult to get time off work to seek care from a physician. As noted above, employees who seek care outside of physician office hours typically go to the emergency department at the hospital. Finally, the fact that women in "other" positions are more likely than any other group of employees in this sample to say their health is fair/poor, to have visited a physician, and to have visited other health care professionals suggests that their higher number of visits to the emergency department also reflects the fact that this group of women is in poorer health.
5.6 Visits to Hospital/Clinic on an Out-patient Basis for Tests/Procedures
Hospital care is changing in Canada. Fewer people are being hospitalized overnight, but day surgery on an outpatient basis has increased (CIHI, 2002, 2003). Consider the following:
- The number of nights that Canadians spent in acute care hospitals fell by about 10% between 1995-96 and 2000-01. After taking population growth and the aging of the Canadian population into account, hospitalization rates fell by 16.5%.
- Canadians spent almost 21 million days as inpatients in acute care hospitals in 1999-2000-a decrease of 15.6% from 1994-95. During the same time period, the number who underwent day surgery increased by 18% in Ontario (CIHI, 2002).
Just under one in three employees sought care on an outpatient basis
Consistent with the national data reported above, substantively more of the employees in this sample received care on an outpatient basis (29.3% of the sample visited a hospital or clinic on an outpatient or day-use basis in the six months prior to the study being conducted) than stayed in hospital overnight (6%) or visited an emergency department (13%).
Women are more likely to receive treatment on an outpatient basis than men
The likelihood of receiving treatment on an outpatient basis is strongly associated with gender, with women being more likely to receive this type of care than men. This finding is particularly worthy of note in that it could be observed regardless of job type, dependent care responsibilities or sector of employment and is true with respect to both likelihood of use and number of visits. These findings are identical to those noted with respect to visits to a physician, use of other health care professionals and visits to mental health professionals and are likely to have the same underlying etiology.
Outpatient care is not associated with job type or dependent care status
Neither the likelihood of seeking care on an outpatient basis nor the number of outpatient visits made to a hospital or clinic are substantively associated with job type or dependent care status.
Female public sector employees are most likely to have received outpatient treatment; male private sector employees least likely
The relationship between gender, sector of employment and treatment on an outpatient basis is identical to the pattern observed for use of physician services, seeking care from another health care professional and visiting a mental health professional: men working in the private sector make less use of such services than any other group while women working in the public sector make more use than any other group.
5.7 Impact of Work-Life Conflict on Use of the Health Care System
As noted earlier in this report (Section 2.1), health care in Canada is a large, resource-intensive industry whose costs have been increasing dramatically over time. In 2002, Canada spent an estimated $122 billion (an average of $3,572 per person) on health care. Between 1997 and 2002, total health spending in Canada grew by almost $34 billion (an unprecedented rate of increase) and is at an all-time high, even after taking inflation and population growth into account (CIHI, 2003).
In Duxbury and Higgins (2003), we noted that between 1991 and 2001 (an overlapping time period) the proportion of employed Canadians experiencing high levels of work-life conflict has also increased.26 This section of the report attempts to draw a link between these two sets of data by addressing the following question: Is work-life conflict associated with greater use of Canada's health care system?
This section is broken down into four parts, each associated with a different form of work-life conflict. Role overload is examined first (5.7.1) followed by work to family interference (5.7.2), family to work interference (5.7.3) and caregiver strain (5.7.4).
5.7.1 Impact of role overload on the use of Canada's health care system
Data linking role overload to use of the health care system are provided in Appendix C and shown graphically in Figure 5. Relative risk data are provided in Appendix D.
Figure 5
Impact of High Role Overload on Use of Canada's Health Care
System 
Overloaded employees make greater use of Canada's health care system-especially services linked to mental health care
Almost 60% of the employees in this sample have high levels of role overload. What implications does this have on health and the burdens placed on Canada's health care system? The findings from these data are unequivocal: employees with high levels of role overload made greater use of Canada's health care system than those with low levels of role overload. Consider the following. In the six months prior to the study being done, compared to their counterparts with low levels of role overload, employees with high levels of role overload were:
- 2.6 times more likely to have sought care from a mental health professional,
- 2.4 times more likely to have received care on an outpatient basis 3 or more times,
- 1.8 times more likely to have seen a physician 3 or more times,
- 1.6 times more likely to have sought care from another health care professional 4 or more times,
- 1.5 times more likely to have had to spend at least one night in the hospital, and
- 1.4 times more likely to have visited a hospital emergency room.
Employees with lower levels of role overload were 1.3 times more likely not to have visited their physician in the past six months and made the lowest use of all of the dimensions of health care examined in this report (see Appendix C).
Taken together, these data would suggest that the health of Canadians (especially their mental health) would improve and use of Canada's health care system could be reduced if the number of employees experiencing high levels of role overload could be reduced. This would require both organizations and governments to address the issue of workloads and the use of office technology and to support employees with child care and elder care demands.
5.7.2 Impact of work to family interference on the use of Canada's health care system
Data linking work to family interference to the use of the health care system are provided in Appendix C and shown graphically in Figure 6. Relative risk data are provided in Appendix D.
Figure
6
Impact of High Work to Family Interference on Use of Canada's
Health Care
Employees with work to family interference make greater use of Canada's health care system
Approximately one in three of the employees in this sample has high levels of work to family interference. These individuals make more use of Canada's health care system than their counterparts who do not experience such interference. The magnitude of the relationship between work to family interference and use of Canada's health care system can be determined by examining the following relative risk data. In the six months prior to the study being done, compared to their counterparts with low levels of work to family interference, employees with high levels of work to family interference were:
- 1.7 times more likely to have sought care from a mental health professional,
- 1.7 times more likely to have received care on an outpatient basis 3 or more times,
- 1.6 times more likely to have seen a physician 3 or more times,
- 1.5 times more likely to have visited a hospital emergency room,
- 1.4 times more likely to have had to spend at least one night in the hospital, and
- 1.3 times more likely to have sought care from another health care professional 4 or more times.
5.7.3 Impact of family to work interference on the use of Canada's health care system
Data linking family to work interference to the use of the health care system are provided in Appendix C and shown graphically in Figure 7. Relative risk data are provided in Appendix D.
Figure 7
Impact of High Family
to Work Interference on Use of Canada's Health Care
System
Percent of respondents
with high and low levels of family to work interference who, in the
last six months, made the following use of these facets of the
health care system.
Family to work interference can be linked to poorer mental health
One in ten of the employees in this sample has high levels of family to work interference. While these individuals make more use of Canada's health care system than their counterparts who do not experience such interference, the magnitude of the relationship between this form of work-life conflict and the use of Canada's health care system is (with one exception) lower than observed for the other three forms of work-life conflict. Compared to their counterparts with low levels of family to work interference, employees with high levels of family to work interference were, in the six months prior to the study being done:
- 1.9 times more likely to have sought care from a mental health professional,
- 1.6 times more likely to have received care on an outpatient basis 3 or more times,
- 1.4 times more likely to have seen a physician 3 or more times,
- 1.3 times more likely to have visited a hospital emergency room, and
- 1.3 times more likely to have had to spend at least one night in the hospital.
One aspect of these data is worthy of note-the high association between family to work interference and the use of mental health care services (those with high levels of this form of interference are almost twice as likely to seek such care as those with low levels). What causes this association is hard to determine from these data as the direction of causality is not clear. We can speculate that putting family first in a society that materially and socially recognizes the opposite behaviour (i.e. putting work first) is associated with higher levels of stress and depression and lower self-esteem. This explanation assumes that family to work interference contributes to poorer mental health. Alternatively, it may be that family is more likely to rise in priority compared to work when there are problems at home, when demands associated with health care increase or when an individual is stressed or depressed (i.e. in poorer mental health). In this case, poorer mental health is assumed to lead to higher levels of family to work interference rather than the reverse. Future research should seek to determine the direction of causality of this relationship as it affects how the issue could best be addressed.
5.7.4 Impact of caregiver strain on the use of Canada's health care system
Data linking caregiver strain to the use of Canada's health care system are provided in Appendix C and shown graphically in Figure 8. Relative risk data are provided in Appendix D.
Figure 8
Impact of High Caregiver Strain on Use of Canada's Health Care
System
Percent of
respondents with high and low levels of caregiver strain who, in
the last six months, made the following use of these facets of the
health care system.
Caregiver strain can be linked to poorer physical health
Approximately one in four of the respondents to our survey has high levels of caregiver strain. This form of strain appears to be more closely linked to physical health problems and less strongly associated with mental health concerns than the other three forms of work-life conflict. In the six months prior to the study, compared to their counterparts with low levels of caregiver strain, employees with high levels of caregiver strain were:
- 1.8 times more likely to have received care on an outpatient basis 3 or more times,
- 1.5 times more likely to have visited a hospital emergency room,
- 1.5 times more likely to have had to spend at least one night in the hospital,
- 1.5 times more likely to have sought care from a mental health professional, and
- 1.4 times more likely to have seen a physician 3 or more times.
The data in Appendix C support the idea that employees with higher levels of caregiver strain are in poorer physical health. Respondents in this sample with high caregiver strain make the greatest use of physician services, and are the most likely to have spent time in hospital on both an inpatient and an outpatient basis. They also make the greatest use of the emergency room. It would appear from health care system could be reduced by providing more supports for employed Canadians who have to deal with elder care issues.
5.8 Summary: Use of the Health Care System
The data reviewed in this chapter indicate that employees with higher levels of work-life conflict make greater use of Canada's health care system.
High role overload, in particular, appears to be a substantive risk factor with respect to the incidence of physical and mental health problems that require employed Canadians to seek medical care. In the previous six-month period, compared to their counterparts with low levels of role overload, employees with high levels of role overload were 2.6 times more likely to have sought care from a mental health professional, 2.4 times more likely to have received care on an outpatient basis 3 or more times, 1.8 times more likely to have seen a physician 3 or more times, 1.6 times more likely to have sought care from another health care professional 4 or more times, 1.5 times more likely to have had to spend at least one night in the hospital and 1.4 times more likely to have visited a hospital emergency room.
These data suggest that the health of Canadians (especially their mental health) would improve and use of Canada's health care system could be reduced if the number of employees with high levels of role overload could be reduced. This would require both organizations and governments to address the issues of workload and increased use of office technology. It would also require that supports for the demands associated with both child and elder care be put into place in communities and organizations.
Similarly, employees who meet work demands at the expense of time for their family (about one in three of Canadian employees) are substantially more likely than those without this form of work-life conflict to have sought care from a mental health professional (relative risk of 1.7) and seen their physician 3 or more times in a six-month period (relative risk of 1.6). Also worthy of note is the fact that employees with high levels of work to family interference are 1.7 times more likely to have received care on an outpatient basis 3 or more times in a six-month period and 1.5 times more likely to have visited a hospital emergency room.
These data imply that demands on the health care system could be reduced if employers implemented policies which have been found to make it easier for employed Canadians to combine work and non-work roles. Suggestions here include greater use of flexible work arrangements such as flextime and compressed work weeks, and more judicious use of job-related travel.
The high levels of caregiver strain experienced by one in four of the respondents to this study appear to be closely linked to physical rather than mental health problems. In the previous six-month period, compared to their counterparts with low levels of caregiver strain, employees with high levels of caregiver strain were 1.8 times more likely to have received care on an outpatient basis, 1.5 times more likely to have visited a hospital emergency room and 1.5 times more likely to have had to spend at least one night in the hospital. It would appear from these data that demands on Canada's health care system can be reduced by providing more supports for employed Canadians who have to deal with elder care issues.
Finally, it is important to note that while individuals with higher levels of family to work interference make more use of Canada's health care system than their counterparts who do not experience such interference, the magnitude of the relationship between this form of work-life conflict and the use of Canada's health care system is (with one exception) lower than can be observed with the other three forms of work-life conflict. The exception to this trend is visits to mental health professionals. Employees with high levels of family to work interference are almost two times as likely to have sought care from a mental health professional than their counterparts with lower family to work interference. Future research in this area is needed to determine the direction of causality of this relationship.
The over-riding conclusion one reaches from the data presented in this chapter is that Canada can no longer afford to leave it to employers and employees to deal with issues around work-life conflict. The tendency to do so for the past decade has resulted in higher levels of work-life conflict (role overload and caregiver strain in particular). The data reviewed in this chapter link higher work-life conflict with greater use of the health care system and the concomitant increase in health care costs. While employers may be saving money by "doing more with less," downsizing and rightsizing, Canadian taxpayers are paying a premium for this strategy as it is their tax dollars that are funding the health care system. Employers are also paying "hidden" costs as the high use of other health care professionals is likely paid for by employer benefit plans.
The data in this chapter also support the idea that greater attention to workplace health issues (of which work-life conflict is one) may yield higher returns with respect to efficiencies within the health care system than other strategies that focus strictly on health care delivery systems.
[Previous] [Table of Contents] [Next]