
Public Health Agency of Canada
www.publichealth.gc.ca
Common menu bar links
Institutional links
Diseases & Conditions
Health & Safety
Research & Statistics
Agency Information
Search Box
E-mail this page
Epi Update: Ciprofloxacin resistance to Neisseria gonorrhoeae in Canada, 2006
Background
Gonorrhea, a sexually transmitted infection (STI) caused by the bacterium Neisseria gonorrhoeae, is the second most commonly reported STI in Canada. Ciprofloxacin, an antibiotic belonging to the quinolone class of antibiotics, is commonly used to treat gonorrhea. In recent years, gonorrhea resistance to ciprofloxacin has developed, prompting enhanced monitoring and re-evaluation of current treatment recommendations.
Symptoms
Symptoms of gonorrhea usually appear 2-7 days after infection, however, the majority of infected females and some infected males will not show any symptoms. These asymptomatic carriers act as a "silent" reservoir for the spread of this infection. In males, symptoms include purulent discharge from the penis and pain on urination. Females may experience purulent genital discharge, abdominal or pelvic pain, burning on urination, and abnormal vaginal bleeding. Females are disproportionately affected by the complications of this infection. Untreated infection in females may lead to pelvic inflammatory disease, which in turn may cause tubal infertility, chronic pelvic pain and life-threatening ectopic pregnancy. In both males and females, rectal and pharyngeal infections can occur, and extension from the genital sites can lead to disseminated gonococcal infection.
Uncomplicated gonorrhea can be treated easily with single-dose antibiotics1 however a challenge arises when resistant strains are treated with antibiotics to which the bacteria have developed a resistance.
Epidemiology of Neisseria gonorrhoeae in Canada
There has been a gradual but steady increase in the number of reported gonococcal infections in Canada since 1997, increasing from approximately 4500 cases in 1997 to approximately 9,000 cases in 2005. This represents a rate increase of greater than 90% from 15 cases per100,000 to 28 cases per100,000 in 1997 and 2005, respectively. Gonorrhea predominantly affects males 20 to 29 years old and females 15 to 24 years old 2. The rise in reported rates has been evident in both sexes since 1997, although it has been greater among males (106%) than females (76%) ( Figure 1).
Figure 1: Reported Rates1 of Gonorrhea in Canada, 1980 - 20052
1 Rate per 100,000
population. Population estimates provided by Statistics
Canada.
2 2005 numbers are preliminary and changes are
anticipated;
Reporting delay may contribute to apparent decreases between 2004
and 2005.
Risk factors for Neisseria gonorrhoeae infection
It appears that a network of people engaging in high-transmission activities plays a key role in the high prevalence of gonorrhea currently seen in Canada 1.
Individuals at increased risk of gonorrhea infection include:
- Those who have had contact with a person with proven infection or a compatible syndrome 1;
- Travellers to an endemic country or those who have had unprotected sex with a partner originating from an area with high endemicity (there is also a higher risk of resistance in this population) 1;
- Commercial sex workers and their sexual partners 1;
- Sexually active youth younger than 25 years of age with multiple partners 1;
- Street-involved youth 1;
- Young women with lack of social power or skills to engage in safer sex 3;
- Individuals with frequent STI re-infections or multiple infections 4;
- Individuals with inconsistent condom use and a high rate of partner turnover 4.
Neisseria gonorrhoeae resistance to ciprofloxacin
When resistant strains of Neisseria gonorrhoeae are treated with antibiotics to which the bacteria have decreased susceptibility it may be difficult or impossible to cure and persistent infection may develop. A standard treatment regimen is expected to cure 95% or greater of all gonorrhea infections 5. Thus, an antibiotic should not be used in situations where resistance has developed in greater than 3% to 5% of strains 1.Quinolone-resistant Neisseria gonorrhoeae (QRNG) has emerged and spread relatively recently, primarily in areas experiencing a high burden of gonococcal disease in combination with antibiotic overuse or misuse. The emergence and spread of QRNG may have been accelerated by the introduction of the quinolones for the treatment of other diseases, in addition to the treatment of gonorrhea 5.
In Canada, the proportion of ciprofloxacin resistance has increased from less than 1% in the early 1990s, to 2.4% in 2003, 6.2% in 2004, reaching a high of 15.7% in 2005 6 (National Microbiology Lab (NML) unpublished data, 2006) (Figure 2).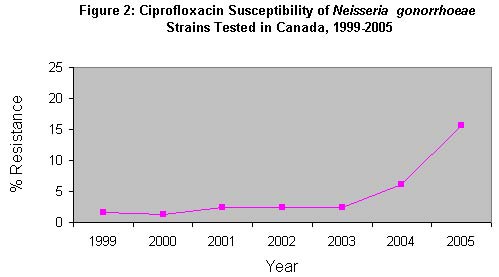
Percentages are calculated using the number
of specimens tested as the denominator.
Note: NML has not received any strain numbers from Nova Scotia for
2004.
Source : Public Health Agency of Canada, National
Microbiology Laboratory, 2006
Regional variation in ciprofloxacin resistance ranges from 0% to approximately 60%, with Quebec, Ontario, Alberta and British Columbia falling above the 3% threshold for quinolone resistance in 2005, according to testing undertaken by the NML (NML unpublished data, 2006).
Since 2004, less than half of the reported cases of gonorrhea were tested for gonococcal resistance by the NML (Table 1). The ability to test for resistance using phenotypic antimicrobial methods, which can only be performed on cultures, has decreased because of the increased usage of nucleic acid amplification testing (NAAT) 2.
|
Year
|
Reported Cases 1
|
Strains Tested Nationally
2
|
Percentage
|
|---|---|---|---|
| 1999 | 5,381 | 4,025 | 75% |
| 2000 | 6,189 | 4,458 | 72% |
| 2001 | 6,756 | 4,501 | 67% |
| 2002 | 7,365 | 4,465 | 61% |
| 2003 | 8,242 | 4,235 | 51% |
| 2004 | 9,270 | 4,018 | 43% |
| 2005 | 8,956 | 3,620 | 40% |
Note: NML has not received any
strains numbers from Nova Scotia.
1 2005 numbers are preliminary and changes are
anticipated.
2 Source: Public Health Agency of
Canada, National Microbiology Laboratory 2006 .
Treatment of ciprofloxacin resistantNeisseria gonorrhoea
Given the dramatic increase in ciprofloxacin resistance observed from 2003 to 2004, the Canadian Guidelines on Sexually Transmitted Infections, 2006 edition have qualified the use of the antibiotic ciprofloxacin as a first line treatment. It is currently recommended that when the case or contact are from, or epidemiologically linked to, a region or area with rates of quinolone resistance to N. gonorrhoeae greater than 3% to 5% then a set of alternative treatment recommendations should be followed 1.
Control of ciprofloxacin resistance in Neisseria gonorrhoeae
Continued monitoring for antimicrobial resistance is important for controlling transmission and ensuring high cure rates for this treatable infection. Measures to control antimicrobial resistant gonorrhea include early and accurate diagnosis to ensure the correct treatment, optimized patient adherence, judicious and appropriate use of existing treatments, the development of new treatments, case finding and partner notification, and appropriate follow-up 1.
Ongoing, timely, and representative surveillance of antimicrobial resistance will ensure that treatment recommendations remain accurate. Linking laboratory data to epidemiological data and identifying cases of resistance acquired both locally or abroad would permit a more complete picture of resistance by identifying further or more precisely groups at higher risk and thus allow health care practitioners to optimize the treatment of gonococcal infection.
References
- Public Health Agency of Canada. Canadian Guidelines on Sexually Transmitted Infections (STI) 2006 Edition. Ottawa; 2006.
- Public Health Agency of Canada. 2004 Canadian Sexually Transmitted Infections Surveillance Report. In press.
- Public Health Agency of Canada. Sub-regional variations in the epidemiology of Neisseria gonorrhoeae in a large urban region in Alberta, Canada: Results from spatial analyses using routinely collected surveillance data. Canada Communicable Disease Report, February 2006;32(4). http://www.phac-aspc.gc.ca/publicat/ccdr-rmtc/06vol32/dr3204a-eng.php
- De P, Singh AE, Wong T, Kaida A. Predictors of gonorrhea
reinfection in a cohort of sexually transmitted disease patients in
Alberta, Canada, 1991-2003. Sexually Transmitted Diseases, January
2007;34(1):30-36.
http://www.stdjournal.com/pt/re/std/abstract.00007435-200701000-00006.htm;jsessionid=
F3qBhktpbNJ9CLgTptTzQM0GBXQgccBvf3ylSyGnlGbJgj5vzNL5!267491070!-949856145!8091!-1
- World Health Organisation, John Tapsall. Antimicrobial
resistance in Neisseria gonorrhoeae. World Health
Organisation/Drug Resistance.2001 http://www.who.int/drugresistance/Antimicrobial_resistance_in_Neisseria_gonorrhoeae.pdf

- Mann J, Kropp R, Wong T, et al. Gonorrhea treatment guidelines
in Canada: 2004 update. CMAJ 2004; 171(11): 1345-1346
http://www.cmaj.ca/cgi/content/full/171/11/1345?etoc