| |
|||||||||||||||||
|
|
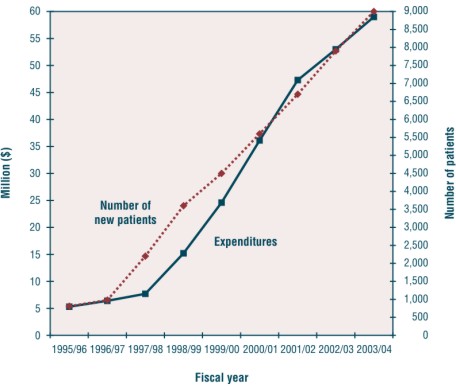
Cross-Canada Forum Cancer Care Ontario's New Drug Funding Program: Controlled introduction of expensive anticancer drugs William K Evans, Marilyn Nefsky, Joseph Pater, George Browman and Donald H Cowan Abstract In the mid 1990s, the high cost and increasing number of new anticancer and supportive care drugs began to result in an inequality of access to promising new treatment approaches in the Province of Ontario. Starting with a single drug, paclitaxel, in 1995, Cancer Care Ontario's New Drug Funding Program has evolved into a provincial program that enables cancer patients in Canada's most populous province to equitably access new and expensive, intravenously administered drugs. This article describes the development of the program, including the evolution of the administrative mechanisms necessary to manage the program and the decisions of the policy advisory committee that shape provincial funding policies. In fiscal year 2000/2001, the Program made 14 drugs available for 24 indications for a total provincial expenditure of approximately $37.7 million. These intravenous drugs can now be accessed through nine Regional Cancer Centres, the province's only cancer hospital (Princess Margaret Hospital) and 80 community hospitals and will directly benefit more than 8,700 patients. Key Words: equitable access; funding policy; New Drug Funding Program Background Cancer Care Ontario (CCO), a provincial agency funded by the Ontario Ministry of Health and Long Term Care (MOHLTC), is mandated to integrate and coordinate the cancer control services in the province of Ontario, Canada. CCO is the principal advisor to the MOHLTC on all cancer issues. It manages the province's nine Regional Cancer Centres, the Ontario Breast and Cervical Screening Programs, as well as the Ontario Cancer Registry. The Regional Cancer Centres are ambulatory treatment facilities associated with major hospitals in the larger cities of the province. They provide multidisciplinary consultation and care by medical, radiation and surgical oncologists. The Regional Cancer Centres also provide supportive care and operate outreach programs that link the tertiary treatment facilities to surrounding community hospitals and care providers. Through community clinics, CCO is able to deliver at least some chemotherapy in smaller communities close to home. In Canada, the method of funding medications for cancer patients varies somewhat between provinces. However, all drugs administered to patients in hospitals, or intravenous drugs given in the outpatient departments of hospitals or ambulatory cancer centres, are provided to patients as an insured service in Canada's publicly funded universal access health care system. Chemotherapy drugs are either paid for through the global budgets of the hospital providing the care or through dedicated cancer centres. The institutional global budgets are set by the provincial governments through their Ministries or Departments of Health. In Ontario, under the terms of the Canada Health Act1, it is not possible to bill patients or their third party insurance provider for the cost of intravenous drugs administered in a hospital or cancer centre. In some provinces, chemotherapy is administered through community hospitals by medical oncologists not affiliated with provincial cancer agencies. In Ontario, approximately 50% of the chemotherapy administered in the province is given through this informal cancer system. Until recently, when a new chemotherapy drug was approved for release in Canada by the federal government, its availability in a particular facility was dependent on whether the hospital or cancer centre could accommodate the additional cost of the drug in its operating budget. With the fiscal restraint exercised in Ontario's health care system over the past 10 years, it has been increasingly difficult for institutions to accommodate expensive new drugs in their budgets, leading to inequality of access to new drugs by patients. Initial steps in establishing a provincial systemic therapy funding program Between 1993 and 1994, the Ontario Ministry of Health undertook a series of consultations with patients, the public and care providers to determine how the cancer care system in Ontario could be improved. At that time, patients reported that care was of high quality, but fragmented. Strong arguments were made for an organization that could integrate the care and services of all cancer care providers. A Provincial Cancer Network was established, which in turn set up a number of working groups, including a Systemic Therapy Working Group. This group recommended that a managed systemic therapy program be established in Ontario and that all cancer-specific and relevant supportive care drugs be managed and funded through a single agency, rather than through the multiplicity of players that existed at the time.2 It was felt that such a program would help to ensure equitable access to anticancer drugs by all patients in the province. At approximately the same time, there was concern that breast and ovarian cancer patients were having difficulty accessing paclitaxel (Taxol™), one of the first of the new and expensive anticancer agents. Many Ontario physicians, who wanted to prescribe paclitaxel for their patients, were unable to do so because their hospital budget could not absorb the unplanned and large expense. In an effort to address this inequity, Cancer Care Ontario made the decision to fund paclitaxel from its reserve funds for those breast and ovarian cancer patients treated in CCO Regional Cancer Centres until such time as the MOHLTC agreed to fund it. CCO's Practice Guideline Initiative Cancer Care Ontario's Practice Guidelines Initiative was established about the same time that CCO was confronting the issue of paclitaxel funding for breast and ovarian cancer. This initiative, which is now based at McMaster University and funded through the MOHLTC, coordinates the development of clinical practice guidelines in Ontario using systematic literature reviews to identify the current best evidence to guide practice.3,4 Twelve multidisciplinary Disease Site Groups, comprising health care providers, community representatives and researchers, use a consistent literature search strategy, specific data analysis methodology and a standardized format to report a detailed summary of the best available evidence on a clinical topic. The program is intended to provide practitioners with evidence-based recommendations on current best practice for specific clinical situations in the treatment of cancer patients. Reports are published in peer-reviewed journals and are available on the CCO Practice Guideline Web site at <www.cancercare.on.ca/ccopgi>. In 1995, the CCO Practice Guideline Initiative developed guidelines for the use of paclitaxel for patients with metastatic breast cancer and Stage III and IV ovarian cancer. These guidelines defined the criteria by which patients would be eligible to receive paclitaxel. The Paclitaxel Funding Program Cancer Care Ontario proposed to the provincial government that paclitaxel be funded according to the guidelines and that CCO take on the role of reimbursing institutions for their usage of the drug and for the monitoring of its use and effectiveness. The government accepted this proposal in April 1995. Only those hospitals with appropriate facilities and medical personnel to supervise chemotherapy administration were permitted to participate in the paclitaxel funding program. The guidelines for the use of paclitaxel were provided to the participating hospitals, as well as eligibility and follow-up forms to be completed for each patient. This information allowed CCO to track the number of patients treated, the indication for treatment, the number of cycles administered to patients and the drug expenditure by treatment facility. Institutional billing forms for monthly submissions for reimbursement were also developed. Hospitals were reimbursed by CCO quarterly for the drug if it was administered to eligible patients according to guidelines. Funding was not provided for the chemotherapy administration costs, such as the cost of personnel to prepare and deliver the drugs. The development of the new Drug Funding Program Subsequent to the establishment of the paclitaxel funding program, Ontario's Ministry of Health asked CCO to develop a proposal for a managed systemic therapy program. A program design committee recommended that the Program be phased in over several years and that the first phase be the funding for the new and expensive intravenous drugs. The committee addressed issues such as facility and professional standards, information systems, financial management and contract purchasing. It also recommended that a policy advisory committee be formed to guide the development of the Managed Systemic Therapy Program. Based on the initial success of managing the provincial paclitaxel funding program, the MOHLTC approved the establishment of the provincial New Drug Funding Program (NDFP) in May 1997. The Policy Advisory Committee and the approval process for new drugs The Policy Advisory Committee (PAC) for the New Drug Funding Program includes cancer centre oncologists, community oncologists, a nurse, a pharmacist, an epidemiologist, community representatives, a representative of the Ontario Hospital Association, an ethicist, representatives of the Practice Guideline Initiative, and a representative of the MOHLTC. It reviews the evidence in practice guidelines received from the Disease Site Groups of the Practice Guideline Initiative and recommends to CCO whether the new drug should be funded through the NDFP and under which circumstances. The PAC judges the evidence presented to it through the Guideline initiative according to a hierarchy of evidence in which multiple randomized trials or meta-analyses are most valued, followed by single randomized trials of reasonable size, small randomized trials and data from Phase II trials.5 Over the several years of its deliberations, the PAC has established a hierarchy of benefits that places the greatest value on cure, followed in order of importance by prolongation of survival, relief or prevention of symptoms or complications of disease, improved quality of life, reduction in symptomatic toxicity compared with standard therapy, prolongation of disease-free survival and tumour shrinkage.5 When there is evidence that a new drug alone or in combination with other agents increases the survival of a particular group of cancer patients, a decision to recommend funding is invariably made without difficulty. The values of the members of the PAC play an important role when the evidence is limited to improvement in response rates, reduction in the toxicity of treatment or enhanced quality of life. In these cases, there is much discussion as to the value to society of making expensive treatments available for these indications. Decisions are made by consensus and are generally unanimous, although occasionally there are dissenting views. The need for a guideline to support the provincial funding policy on a new drug is usually recognized by the members of one of the 12 Disease Site Groups (DSGs) of the Practice Guideline Initiative. The DSG then develops the guideline using the practice guideline development cycle previously described by Browman et al.3 On occasion, the impetus for a provincial policy may come from CCO's Systemic Therapy Program leader, the Director of Treatment Services, the MOHLTC, patient advocacy groups or industry. In these cases, the Systemic Therapy Program leader makes a request to the Director of the Program in Evidence-based Care to direct the development of a guideline through the appropriate provincial Disease Site Group. Recommendations to fund new intravenous anticancer drugs are taken forward by CCO to the MOHLTC, with an economic impact analysis based on an estimate of the total population of patients who might be expected to benefit. These estimates are crude, given the lack of tumour stage specific information, detailed information on practice patterns and knowledge of the rate of uptake of new treatment approaches. The MOHLTC has invariably supported the recommendations coming from the PAC and has provided the funds necessary to meet the patient care needs. Current scope of the New Drug Funding Program The scope of the New Drug Funding Program has continued to broaden, and in fiscal year 2000/2001 included 14 drugs for 24 indications. These 14 drugs represent all of the new intravenous drugs that have come on the market with evidence in support of their use since the inception of the NDFP. New drugs and new indications for previously approved drugs are constantly under review. The chemotherapy agents and their indications for funding are listed in Table 1. In addition, the Table shows the CCO guideline number where full details of the guideline recommendations can be found on the website at <http://www.cancercare. on.ca/ccopgi>. The rapid growth in the number of drugs funded and the number of patients treated is shown graphically in Figure 1. It is estimated that the 2001/2002 drug budget will be approximately $50 million and benefit over 9,000 patients. This represents an average growth in expenditures of approximately $10.7 million per annum. The average chemotherapy drug cost per treated case reimbursed through the NDFP was $5,528 in 1999/2000. To date, the NDFP is only responsible for making recommendations on the new intravenous anticancer and supportive care drugs. Oral and subcutaneously administered drugs are reviewed and approved through a separate process by the Ontario Drug Benefit Program (ODB). Agents approved by ODB are placed on the provincial drug formulary and are provided free to patients 65 years and over and to those on social assistance. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
The total chemotherapy drug cost for the province of Ontario is difficult to estimate because accurate information is difficult to obtain from the non-CCO centres delivering intravenous chemotherapy. The amount expended on oral drugs through the Ontario Drug Benefit Plan can be obtained more readily but the direct expenditures by patients not covered by the plan can only be estimated. When evaluated in 1993, oral agents made up 58% of the total chemotherapy drug expenditures and CCO centres represented 24.5% of expenditures on intravenous drugs.6 Assuming that these ratios applied in 2000/2001, the total provincial chemotherapy drug budget would have been approximately $200 million, of which 18.9% would have been attributable to the New Drug Funding Program. The number of health care facilities participating in the NDFP grew from 49 in 1995 to 92 in 2000. The amount of funding reimbursed to some hospitals for the new expensive drugs has grown to approximately 50% of their entire oncology drug budget. CCO reimburses facilities only for those patients who meet the agreed-upon eligibility criteria. Costs for patients who do not meet the criteria must be absorbed by the hospital or cancer centre's budget. The costs of administering these drugs must also be addressed through an institution's operating budget. Within CCO regional cancer centres, complexity-adjusted workload – staffing ratios for nurses and pharmacy staff – guide the development of the institutional operating plans. In non-CCO institutions, the absence of accepted planning standards for systemic therapy staff is a source of difficulty, but the development of such standards is being addressed through a collaborative initiative with the MOHLTC. As the number of drugs and indications funded by the Program has grown, the number of patients and the information being transmitted to CCO on paper forms has increased enormously. To ease the burden of collecting and processing this vast amount of data, a software program was specifically developed for the Program. ChemoTrac™, developed by DKK Health Systems Inc. (www.dkk.net) in consultation with CCO and pharmacists from community hospitals, allows users to identify the disease, the drugs and the treatment regimen, including all of the treatment dates. The primary purpose of the program is to provide information to CCO so that CCO can reimburse the hospitals for the use of the approved systemic therapy drugs. The program is currently used by 43 hospitals. As soon as a suitable encryption process is developed, the data will be transmitted by e-mail. Drug utilization is monitored by CCO to ensure that patients being funded meet the criteria and that CCO is not paying for more than the recommended dose or number of treatment cycles. The program provides a unique opportunity for the review of data that has been collected on a province-wide basis. Data from ChemoTrac™ is imported into a CCO database, which also interfaces with CCO's Oncology Patient Information System (OPIS). Using these databases, outcome studies for specific new drugs (taxanes in breast cancer; rituximab in lymphoma) have been undertaken and provide a population-based experience with these agents in contrast to the results of treatment in highly selected patient populations in clinical trials. The large and growing amount of data available in the New Drug Funding Program's database and the potential to import the data from ChemoTrac™ into either the Ontario Cancer Registry or Canadian Institute for Health Information databases will make it possible to undertake health services research to address questions about equality of access, compliance with guidelines, and the outcomes achievable in the general population with these new agents. An ongoing audit is determining the consistency of practice in relation to the PAC approved indications for drug use. Benefits to patients, hospitals and the MOHLTC The New Drug Funding Program has been of benefit to patients, hospitals and to the MOHLTC. The Program has been successful in expediting the introduction of new and expensive drugs in a standard manner on a provincial basis. Access to expensive drugs is not limited by a patient's ability to pay, place of residence or the capacity of the health care facility's drug budget to absorb the cost of a new drug. Eligible patients can gain access to new drugs from a great many locations in the province, as funding follows the patient rather than being sequestered in the budgets of individual institutions. Health care institutions need not be concerned about finding funds within constrained budgets to cover the cost of new drugs. CCO is the advocate for funding for each new drug on a provincial basis, so hospitals do not have to negotiate a budget increase each time a new drug becomes available. The MOHLTC benefits because CCO, as the sole purchaser of a number of the new anticancer drugs in the Province, has been able to negotiate lower prices than individual health care institutions, thereby reducing the cost to the health care system. CCO recommends to the Ministry which new drugs should be funded based on the best available evidence. The process of rigorous guideline development and policy review provides the MOHLTC with reassurance that new anticancer drugs are only introduced after a careful review of the evidence and that the recommended therapeutic indications will be of value to Ontarians. The Program has been able to provide equal access to effective new intravenous agents for eligible patients throughout the province. A weakness of the current program is that its scope does not include all anti-neoplastic and relevant supportive care drugs, unlike the situation in British Columbia, where the British Columbia Cancer Agency has responsibility for the approval of all agents. The great strength of Ontario's program is that it is built on a very strong evidence base through the work of disease site groups within CCO's Program in Evidence-based Care. The Policy Advisory Committee completes the final step in translating research evidence to clinical practice by establishing policy based on the value of the clinical benefits described in the CCO guidelines. This valuation is undertaken in the context of other new agents being considered for use in cancer, not within the larger context of all cancer control activities. The importance to patients and families of receiving state-of-the-art treatment results in treatment being given a high priority in any discussion of cancer control resource allocation. Within the chemotherapy treatment domain, CCO's New Drug Funding Program assures that policy decisions on the use of new and expensive drugs are evidence based, prioritized on the basis of a hierarchy of benefits and values and implemented in a manner assuring equitable access. References 1. Canada Health Act, 1984. 2. Life to Gain: A Cancer Strategy for Ontario. Queen's Printer for Ontario, 1994 Cat #2226232. 3. Browman GP, Levine MN, Mohide EA, et al. The Practice Guidelines Development Cycle: A conceptual tool for practice guidelines development and implementation. J Clin Oncol 1995;13:502–512. 4. Evans WK, Newman T, Graham I, et al: Lung cancer practice guidelines: Lessons learned and issues addressed by the Ontario Lung Cancer Disease Site Group. J Clin Oncol 15:3049–3059, 1997. 5. Pater JL, Browman GP, Brouwers MC, et al. Funding new drugs in Ontario: Closing the loop in the practice guidelines development cycle. J Clin Oncol 2001;19:3392–3396. 6. Evans WK, Walker H. Expenditures on anticancer systemic therapy agents in Ontario in 1993. Ann Cancer Control Research 1997; 7:481–491. [Previous] [Table of Contents] [Next] |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Last Updated: 2003-01-06 | |||