| |
|||||||||||||||||
|
|
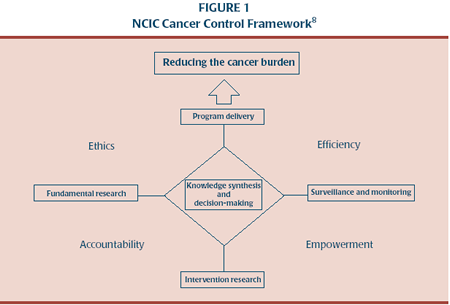
The role of knowledge translation for cancer control in CanadaEva Grunfeld, Louise Zitzelsberger, Charles Hayter, Neil Berman, Roy Cameron, William K Evans and Hartley Stern AbstractThe definition and scope of cancer control has been evolving since its inception. The most recent model of cancer control in Canada has acknowledged the importance of knowledge translation to ensure that research results are implemented in practice and will be used to inform policy. However, without effort, the process of translation does not happen on a consistent basis. Knowledge translation focusses on improving the adoption of an innovation, e.g., research results. A number of health organizations in Canada have identified knowledge translation as an important activity and have begun to develop departments or initiatives dedicated to its achievement. As the emphasis in cancer control is on the application of knowledge, knowledge translation has a role to play in attaining the objectives of cancer control in Canada. It is an ideal time for the Canadian Strategy for Cancer Control and other Canadian cancer control initiatives to determine where they will locate knowledge translation in relation to their objectives. Key words: cancer control; knowledge translation IntroductionCurrently accepted frameworks of cancer control emphasize the importance of applying research findings at the individual or population level towards the aim of reducing the cancer burden.1 The literature has shown, however, that without determined efforts to disseminate and encourage adoption of research - knowledge translation - research results are not consistently integrated into practice.2 To date, cancer control activities in Canada have been and continue to be mainly local and provincial in scope. However, since 1999, efforts have been underway to create a national strategy, the Canadian Strategy for Cancer Control (CSCC). One of the characteristics of the CSCC is a focus on research-to-policy-to-practice.3 Research in the field of knowledge translation can make an important contribution towards realizing the goals of cancer control by encouraging the active use of research. In this paper, we provide an introduction to cancer control in general, and its development in Canada in particular. Knowledge translation has received growing recognition as an important field in the research process. A number of Canadian initiatives, including those associated with cancer, have acknowledged knowledge translation as an important activity. The principal aim of this paper is to highlight the importance of knowledge translation to the achievement of cancer control objectives in Canada. Cancer controlCancer control, as defined by the National Cancer Institute of Canada (NCIC)4 and adopted by the CSCC,5 aims "... to prevent cancer, cure cancer, increase survival and quality of life for those who develop cancer, by converting knowledge gained through research, surveillance and outcome evaluation into strategies and actions." The basic goal of cancer control is the "useful application of results"6 of cancer research. Over time, cancer control has developed into a scientific field in its own right that bridges basic and applied research.7 It covers the spectrum of activities related to cancer within a population:3 fundamental research, interventional research, surveillance and monitoring, plus implementation (policies and program delivery) across the cancer continuum from health promotion/prevention, through screening/detection to treatment and care. Accordingly, it requires a multi-disciplinary approach including involvement of biomedical, behavioural, social and population researchers; health care providers; policy-makers; administrators; educators; volunteers; patients; advocates; fund raisers; and others involved in cancer control.6,8 The concept of cancer control is used in contradistinction to "cancer care", which is a health care system activity. Cancer control, on the other hand, is a population-based activity, which aims to ensure that developments in cancer control research translate into benefits for the population as a whole.7,9 Cancer control frameworksSeveral frameworks that capture the theoretical bases and broad spectrum of cancer control activities have been developed in the United States and Canada. The frameworks were developed to define and guide the cancer control activities1 of initiatives at the national level. In 1984, Greenwald and Cullen published a formative paper presenting a framework to guide the cancer control research of the US National Cancer Institute.7 Until then, the role of research in cancer control was not explicit. The focus had been on service delivery without any overt statement about the key role played by research in defining best practices for service delivery. The Greenwald and Cullen framework7 conceptualized cancer control activities as linear and sequential, from basic research at one end to delivery of cancer control programs to the public at the other end. While this framework did underscore the pivotal role of research in the process, it did not fully develop the complex steps from research to application. Nor did it consider the research-to-practice process as going beyond the demonstration project, and therefore, missed the important phase of knowledge translation. More recent frameworks have captured the iterative nature of cancer control activities, highlighted the need for a multidisciplinary effort, and acknowledged the importance of knowledge translation.1,8,10 In 1994, the Advisory Committee on Cancer Control (ACOCC) of the NCIC published a framework intended to capture all activities that contributed to the reduction of the cancer burden in Canada8 (see Figure 1). ACOCC's aim in developing the framework was to provide the breadth needed to encompass the NCIC's planning needs and aid in decision-making around funding priorities. Four main activities - fundamental research, interventional research, surveillance and monitoring, and program delivery - were linked to knowledge synthesis and decision - making. These activities were to operate within a set of operating principles of accountability, empowerment, ethics and efficiency.
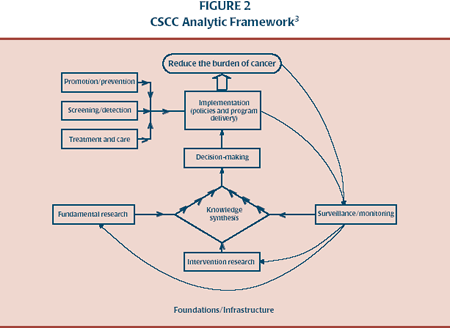
Most recently, the CSCC has expanded upon the framework originally developed by the NCIC (see Figure 2).3 The analytic framework identifies the direction of knowledge flow via the various cancer control activities to actualize the "research-to-policy-to-practice" process. Knowledge translation activities take place across the cancer continuum, from promotion/prevention to treatment/care. Foundations and infrastructure include anything that acts to support the activities in the framework (for example, resources, facilities, standards, and coalitions). This is the framework the CSCC has adopted to help guide its development and implementation. Knowledge translationIt is well recognized that the results of research are unevenly adopted in practice.2 Recognition of this gap has focussed attention on understanding factors affecting the transfer of knowledge. Knowledge translation, as defined by the Canadian Institutes of Health Research (CIHR), is "the exchange, synthesis and ethically-sound application of research findings within a complex system of relationships among researchers and knowledge users".11 As a relatively new discipline it lacks consistent terminology.12 Some related terms are as follows: knowledge utilization,13 knowledge translation,11 knowledge transfer,14,15 and research use.16 These terms are sometimes clearly defined and sometimes used interchangeably.17,18,19 There is a growing body of research on the topic of knowledge translation relevant to health care, and two overviews of systematic reviews20,21 have synthesized the key findings: no one intervention strategy works and no one theoretical model is fully explanatory or predictive; rather, successful translation requires multifaceted intervention strategies with different theoretical underpinnings depending on the characteristics of the environment, the innovation, and the potential adoptors.2,17,20,22,23 Knowledge translation modelsKnowledge translation was originally seen as a linear process - if research findings were made available, it was assumed that they would be read and used.21 However, recent literature suggests that the process is complex,24 interactive25 and reliant on the user's knowledge, beliefs and experiences.17 Several models or frameworks of knowledge translation have been presented.13,16-18,23 Most identify similar elements,17,26 and no one model has been generally accepted as superior.13,14,27
The following three models are examples of those developed in Canada. The Ottawa Model of Research Use (OMRU)16 and the CIHR model28 are models developed within the context of health research. Landry et al.'s model13 identifies stages outlining the process of research use in general. The OMRU16 is a theoretical, interdisciplinary model. Unlike less comprehensive models, it was created to encompass the key elements of the complete knowledge translation process, including its impact on health outcomes. Key elements are the characteristics of the practice environment, potential adopters, and the evidence-based innovation (e.g., evidence new to the adopter); strategies for transferring the innovation into practice, adoption and use of the innovation, and the impact of adoption - outcomes. The model is intended as a guide for policymakers concerned with the transfer of evidence-based research results into practice and for researchers studying the knowledge translation process. Landry et al.13 conceptualized the process of research use as a hierarchical scale called the "Ladder of Research Utilization". The higher level achieved on the "ladder", the more successful the degree of translation. The first stage of the process is transmission, indicating that the researcher has transmitted research results to the community concerned. The second stage is cognition - the research has been read and understood. The third stage sees the research being cited as a reference by others. Efforts by practitioners and professionals to adopt the research results comprise stage four. At stage five, the results have influenced the decisions of practitioners and professionals. In the final stage, research results have been applied and extended by those concerned. Landry et al.'s research focus is on understanding what factors are involved in researchers climbing up one stage of the ladder to the next, and why some succeed while others fail. CIHR situates knowledge translation in a different location than both the OMRU16 and Ladder of Research Utilization.13 Both outline activities to implement innovations (e.g., research findings) whereas CIHR initiates knowledge translation within the research cycle. Knowledge translation is seen as an integral part of the research cycle beginning with the definition of research questions and methodologies through to influencing future research according to the impact of knowledge use.28 Within the research cycle, CIHR identifies six opportunities where there is occasion for knowledge exchange that go beyond the basic approach of publication after research. These opportunities occur at the time of definition of research questions and methodologies; while conducting research (e.g., participatory research); through publishing findings in accessible formats; by contextualizing research findings; by decision-making and taking action based on findings, and finally through influencing future research. CIHR suggests that researchers need to be trained in the most effective approaches for knowledge exchange on the basis of how knowledge will be used. The uses to which knowledge can be applied, as identified by CIHR, include research policy-making, planning and administration, health care provision, maintenance and improvement of personal health, and commercialization. The three models presented here each describe knowledge translation from a somewhat different perspective. Eveland recommends that the knowledge translation process be iterative and evolutionary, and that any model should be selected for its utility for a particular purpose.14 Knowledge translation initiatives in CanadaRecognition of the importance of knowledge translation in the research process is evidenced by the number of organizations that have identified knowledge translation as an important activity. The CIHR website28 provides a list of resource materials that identifies university sites, local, provincial and national organizations, Canadian funding agencies, as well as US and international organizations as useful links on knowledge translation. A publication prepared in 2001 by the Canadian Population Health Initiative (CPHI) of the Canadian Institute for Health Information29 identified 17 organizations (16 Canadian, one US) involved in health or social research and/or policy with an identified focus on knowledge translation. CPHI performed an environmental scan examining the range of strategies used by these organizations for the transfer of research knowledge. The strategies used by these organizations were analyzed according to three criteria: target audience (who was engaged), timing (when during the research process did this engagement occur) and method (how was the target audience engaged). The scan highlighted a number of specific methods organizations can use to engage policy makers in the results of research. Taken together, the strategies used by organizations in the scan represent a valuable tool kit for CPHI and others in applying research knowledge to policies affecting the health and wellbeing of Canadians. Knowledge translation and cancer controlIn 1937, the US Congress defined cancer control as the "useful application of [research] results with a view to the widespread use of the most effective methods of prevention, diagnosis, and treatment".30 This phrase captures perfectly the relation between cancer control and knowledge translation.18 Research on the process and outcomes of knowledge translation has been recently identified as an essential part of the cancer control framework.6,7 From a historical perspective, the products of research have not always been well integrated with other aspects of cancer control in Canada. Early cancer control activities centred on patient care.31 When the Canadian Medical Association discussed the form of its national cancer control strategy in the 1930s, there was much debate about whether research or education should be the main priority.32 The Canadian Cancer Society, established in 1937, chose public and professional education as its mandate. The NCIC, which came into being approximately a decade later, decided to focus on research.33 Thus, research was fragmented from cancer control in the early efforts to establish a national strategy. More recently, both the NCIC framework for cancer control (see Figure 1)8 and the analytic framework adopted by the CSCC (see Figure 2)3 have recognized knowledge translation as an important component. The 1994 NCIC framework integrated the linear model proposed by Greenwald and Cullen into one of its main activities -interventional research. However, it took Greenwald and Cullen's work one step further. While the process described by the model began with basic research and ended with the delivery of health care programs, the NCIC framework added dissemination and adoption studies as a final step. The expanded NCIC framework adopted by the CSCC3 retains three of the four main activities of the framework on which it is based: interventional research, fundamental research and surveillance and monitoring. However, it differs in that decision making has been separated from knowledge synthesis and becomes an activity further along the research-to-policy-to-practice progression. Program delivery is changed to implementation and now incorporates not only program but policy delivery. Implementation is considered the final step in the cancer control process -implementing policies and programs where applicable in the cancer continuum to reduce the burden of cancer. A recent review of how cancer control has been conceptualized in the US and Canada (e.g., through the frameworks already described above) has emphasized the need to both accelerate the translation of research into practice and "plan for, study and resource the research to practice and policy cycle".1 Otherwise there is a danger that research efforts will continue to be poorly disseminated and adopted. Specifically with respect to cancer initiatives in Canada, a number of organizations have added knowledge translation as a new and important activity.1 Although it does not mention knowledge translation specifically, the CSCC has identified a research-to-policy-to-practice progression as the overall activity of its analytic framework. The Joint Advisory Committee on Cancer Control in conjunction with the Advisory Committee on Research (ACOR) of the NCIC have highlighted the translation of research to practice as one of the four top priorities for action.34 As well, the partnership between NCIC and the Canadian Cancer Society has led to the funding of initiatives such as the Canadian Tobacco Control Research Initiative, the Centre for Behavioural Research and Program Evaluation, and the Sociobehavioural Cancer Research Networks, all of which focus on the links between research and application.1 The CSCC model as a knowledge translation vehicle is not specific to cancer control. The concept and organizational structure is applicable to any disease site or health issue, however, the practical implementation is more easily achieved in the cancer control sector due to pre-existing dedicated government (e.g., cancer agencies), non-governmental (e.g., NCIC) and professional (e.g., Canadian Association of PsychoOncology) entities that all share a common goal. Such a vehicle is achievable in any area where the knowledge creators and synthesizers (researchers, academics) and knowledge implementers (service providers such as cancer agencies), can be brought together to address common goals. Relevance of knowledge translation to cancer control in CanadaA role for knowledge translation is implicit within the NCIC definition of cancer control - the conversion of knowledge gained into strategies and actions to reduce the cancer burden.4 Miller35 has identified a number of strategies implemented at the policy and practice levels that have begun to have an impact on trends in cancer incidence and mortality in Canada, e.g., tobacco control policies affecting lung cancer, and dietary modification affecting colorectal cancer. Prevention strategies are thought to be the biggest priority for the future. While fundamental and clinical research continues to add to the control of cancer, there is increased recognition of the impact of behavioural and social factors, and of the need for research in these areas.1,6 Coinciding with this recognition is a focus of recent research interest on knowledge translation of behavioural factors that influence the adoption of innovations.36-38 The CSCC, as a national level broad-based initiative, has an opportunity to act in Canada as a key agent10 responsible for knowledge translation with respect to cancer control. While the CSCC has identified six areas of priority for action (Standards; Guidelines; Primary Prevention; Rebalancing Focus; Human Resource Planning; and Strategic Research), identifying specific activities to be carried out within each of these priorities and ways in which they will be implemented and evaluated is at an early stage. It is an ideal time for the CSCC to determine where it will locate knowledge translation in relation to its objectives. Ho et al.39 stated that knowledge translation includes the application of research findings to practice on at least three levels: the practices of health professionals (and we would add, to the practices of the population), policy-making by health authorities and governments; and implementation of strategies to enable health professionals and policy makers to work together to put policies into practice. The challenge for the CSCC, and all cancer control and cancer research initiatives in Canada, is to consider how they will actualize knowledge translation on each of these levels. ConclusionDespite the knowledge gains made by research with respect to cancer control, there remains a gap between what is known and what is practised across the entire spectrum of cancer control activities.6 Translation of research knowledge has been identified as one of the key phases of cancer control.5,6 Knowledge translation is a new and evolving field, the importance of which is beginning to be recognized by cancer control initiatives in Canada. References
Author References Eva Grunfeld, Cancer Care Nova Scotia, Halifax, Nova Scotia,
Canada, and Dalhousie University, Halifax, Nova Scotia, Canada
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
[Previous] [Table of Contents] [Next]
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Last Updated: 2004-08-11 | |||