
![]()
![]()

![]()
![]()
![]()
![]()
Raves: a review of the culture, the drugs and the prevention of harm
Erica Weir
CMAJ 2000;162(13):1843-8
See also:
- Dancing through time [Letter]
- Some light from the heat: implications of rave parties for clinicians [Commentary]
Contents
Abstract
Raves are all-night dance parties attended by large numbers of youth, sometimes in excess of 20 000. The rave scene, which is international in scope, is distinguished by clandestine venues, hypnotic electronic music and the liberal use of drugs such as ecstasy (3,4-methylenedioxymethamphetamine), GHB (gamma-hydroxybutyrate) and ketamine. Several rave-related deaths in Canada in 1999 alerted health authorities, parents and police to the health risks of rave attendance. Family physicians, emergency physicians and pediatricians should have some understanding of raves, the drugs and the health risks so they can effectively counsel and treat patients. The rave culture in Canada and the drugs commonly used at raves are reviewed, and strategies and initiatives for harm reduction are discussed.
[Contents]
In January 2000, Ontario's Deputy Chief Coroner, Dr. Bonita Porter, announced an inquest into the death of Allan Ho, a 21-year-old man who collapsed at a rave party and later died at Humber River Regional Hospital Emergency Department on Oct. 10, 1999.1 Several other rave-related deaths in Ontario and Nova Scotia in the fall of 1999,2 raised the possibility of raves as public health hazards; although alarmed parents and politicians called for a crackdown on raves and threatened prohibition, the rave community protested the media exaggeration and requested a balanced perspective and response. Family physicians, pediatricians and emergency physicians should have some and understanding of the rave culture, the drugs often used at raves and the associated health risks so they can communicate knowledgeably with patients, recognize potential drug use and provide advice about harm reduction.
Raves are all night dance parties sometimes attended by as many as 20 000 youths who dance vigorously and continuously to repetitive electronic music played by celebrated disc jockeys (DJs). Raves first appeared in Britain and the United States in the mid-1980s and have since spread to other countries including Australia, India, Belgium, Egypt and Canada. "Ravers" have been described as a shadowy subculture of youth who, in reaction to the materialism of the "me" generation,3 have embraced a party etiquette of peace, love, unity and respect, which is captured in the rave logo "PLUR."4 Embodying a musical blend of psychedelic hippiedom and pneumatic punk, raves centre around mobile sound systems, hypnotic rhythms, clandestine venues and the liberal use of drugs such as 3,4-methylenedioxymethamphetamine (MDMA; "ecstasy") and gamma-hydroxybutyrate (GHB). Ravers seek sensory amplification and euphoric transcendence through a combination of marathon trance dancing, drug use and music.
There is not much published in the medical literature on the subject of raves. A PubMed search using "rave" or "raves" as keywords produced only 17 English articles on rave dances since 1995; these included 6 descriptive epidemiology studies mostly from the United Kingdom, Canada and Australia,5–10 7 case reports on the medical complications of rave-related drug use,11–17 2 educational articles on the pharmacology of ecstasy18,19 and 1 review of raves with a focus on ecstasy.20 There were no articles on "raves" and "harm reduction." In contrast, a PubMed search combining the keywords "ecstasy" and "drug use" produced 247 articles published in the last 5 years. Whereas there is an abundance of articles on the pharmacology of ecstasy and the complications associated with its use, there is a paucity of literature on the public and preventive health aspects of rave attendance.
Drawing from the fields of sociology4 and pop culture,3 information from drug-prevention workers,21,22 Web sites pertaining to drug use and raves,23–27 as well as on recent medical literature, an overview of the rave culture, the illicit drugs available at raves and harm reduction issues and initiatives is presented. Information on the acute management of specific poisonings is mentioned only briefly; more comprehensive protocols are available in a recent review article28 and from poison control centres. Contact information for Canadian poison control centres is listed in the lilac section of the most recent edition of the Compendium of Pharmaceuticals and Specialties.29
[Contents]
The rave culture
The rave scene, which has been active in Canada since the late 1980s, has spawned a flourishing industry of promoters, performing DJs, fashion designers and graphic artists; 4 key components distinguish the rave scene: the music, the venue, the people and the drugs.
The underground or noncommercial music featured at raves is distinct from the music played at conventional nightclubs. Most of the genres of rave music are produced by computers and include little or no vocals. Artists and independent record companies press small quantities of "white labels" (i.e., 12-inch singles with no packaging) and distribute them directly to DJs. Radio and multinational record companies are bypassed. Types of rave music include "house," "acid house," "hardcore," "ambient," "faster moving hardcore" or "happy hardcore," "jungle" or "drum&bass," and "techno" or "trance". As an example, the "techno" sound has been described as "repetitive, remorselessly loud and fast, surging past the listener in mind-numbing waves."3 The DJs, often regarded as performing artists in much the same way as those who create the music, can be the main draw for raver attendance.
Because alcohol is often not available at raves there is usually no age restriction on admission. Raves typically last all night and are held at different venues each time. Originally, raves were held at clandestine locations such as farmers' fields, with news of the location released just hours before the event in an attempt to deter police surveillance. More often now raves are held in legal spaces such as concert halls, underground parking lots and warehouses. Given the high and unpredictable number of attendees, concerns have arisen about sanitary conditions at these events — in some instances, portable toilets have been brought in. The heat and humidity generated at large raves has led to the insistence that running water be available at the parties as well.
It is estimated that most rave attendees are between 15 and 25 years of age4 and are from middle-class backgrounds. Raving is an expensive leisure activity; the cost of admission ranges from $10 to $50, and the cost of the drugs ranges from $10 to $40 per night. The requisite clothing (Fig. 1) could include baseball hats, T-shirts emblazoned with logos, baggy pants, running shoes, knapsacks, barrettes, infant toys, plastic chains and infant soothers. As the clothing suggests ravers pride themselves on their lack of pretension and their open acceptance of themselves and their community. From their viewpoint the androgynous dress diminishes distinctions based on physical attractiveness and sexual orientation. Many ravers perceive the events to be safe havens for outcasts, "nerds" and "computer geeks,"4 who are attracted by the use of computers to produce the music and the Internet to promote the scene.27,30
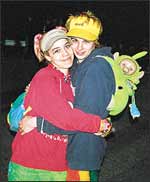 | Fig. 1: Baseball caps, knapsacks, beads and infant toys are typical rave paraphernalia. (Photo courtesy of Andrew McCracken) |
[Contents]
The drugs
Not all ravers use drugs; however, many illicit drugs are available at raves and are used liberally to enhance the "vibe" (Table 1). Conspicuously absent from the list is alcohol; undoubtedly, a minority of rave attendees consume alcohol at raves, but most ravers agree that alcohol does not belong in the rave scene32 because it is believed to incite aggression and violence. Although ecstasy is the most notorious rave drug, cannabis appears to be the most popular drug among ravers.4 Most physicians are probably already familiar with the pharmacological profiles and medical management of cannabis, cocaine, d-lysergic acid diethylamide (LSD), phencyclidine (PCP) and crystal methamphetamine (speed) ingestion, which are well documented in standard texts.31,33 The popularity of crystal methamphetamine has risen recently,34,35 as has the use of gamma-hydroxybutyrate and ketamine, relative newcomers to the illicit drug rave scene, has also increased.
Gamma-hydroxybutyrate is a naturally occurring metabolite of the inhibitory neurotransmitter gamma-aminobutyric acid and is thought to function as a neurotransmitter or neuromodulator itself.36 It produces a biphasic dopamine response and triggers the release of an opiate-like substance. Within the central nervous system gamma-hydroxybutyrate mediates sleep cycles, temperature regulation, cerebral glucose metabolism and blood flow, memory and emotional control; it is normally present in human serum and readily crosses the blood–brain barrier. Gamma-hydroxybutyrate is used clinically in some countries in resuscitations, anesthesia and in the treatment of addictions and narcolepsy.36,37 It is rapidly absorbed after ingestion (elimination half-life is 27 minutes), and the primary route of elimination is expired breath.
The illicit use of gamma-hydroxybutyrate, or "liquid ecstasy," has grown in North America where it is distributed to ravers and to body builders for purported euphoric and "fat-burning" metabolic effects.36 Colourless and odourless, gamma-hydroxybutyrate has also been cited as one of the several "date rape" drugs. Adverse effects have have been reported after it has been surreptitiously slipped into drinks at nightclubs and after it has been used intentionally for the euphoric effects.37 Ingestion of gamma-hydroxybutyrate causes behavioural changes, such as increased aggression and impaired judgement, as well as a spectrum of neurological effects ranging from mild (e.g., nystagmus, ataxia) to severe (e.g., frank apnea interspersed with periods of violent combativeness). Within the past 5 years poison control centres in North America have reported increased numbers of gamma-hydroxybutyrate overdose cases, mostly resulting in coma and respiratory depression, which may be potentiated by the concomitant ingestion of alcohol.28,37 There is no antidote for gamma-hydroxybutyrate overdose; treatment is restricted to nonspecific supportive care including ventilatory support if necessary and atropine for persistent bradycardia.36,37
Ketamine is a rapid-acting intravenous or intramuscular anesthetic that delivers a unique combination of hypnotic, analgesic and amnesic effects with minimal respiratory depression.38 It produces a "dissociative" state32 characterized by profound analgesia and amnesia without necessarily producing loss of consciousness. First introduced clinically more than 30 years ago, its role soon diminished because of significant psychomimetic side effects during recovery, experienced more often by adults than children.32 It is still used clinically for certain indications such as the intramuscular sedation of children for short procedures. Clinical interest has been rekindled with new insights into its isomers, mechanism of action and profound analgesic properties.38 Ketamine's neuropharmacology is complex. Although ketamine interacts with multiple binding sites including N-methly-d-aspartate (NMDA) and non-NMDA glutamate receptors, nicotinic and muscarinic cholinergic receptors, and monoaminergic and opioid receptors38 most of the analgesic, amnesic and psychomotor effects are associated with NMDA receptor antagonism.
Usually obtained through diversion from legitimate sources such as veterinary clinics, ketamine first entered the rave scene in the early 1990s.39 Its use has been growing both the United Kingdom and North America, but reports of ketamine-associated deaths are rare.40 Literature on the acute management of ketamine overdose is sparse. The recognized adverse events associated with ketamine ingestion (i.e., oxygen desaturation, apnea, stridor, laryngospasm, emesis and aspiration) suggest that protecting the airway should be the first priority in an emergency.41 Accidents appear to pose a greater risk than toxicity for ketamine users because of the intensity of the dissociative state and loss of physical control. In addition, according to reports of recent police seizures of "designer" drugs, ketamine is being deliberately packaged in tablet form with logos that make it look like 'ecstasy." Thus, users run the risk of unwittingly ingesting ketamine thinking it is ecstasy.42
Ecstasy (3,4-methylenedioxymethamphetamine [MDMA]) was patented in 1914 as an appetite suppressant but was never produced commercially.18 It resurfaced as an adjunct to psychotherapy in the late 1970s and since the mid-1980s has become popular at raves. MDMA shares properties with both amphetamine and hallucinogenic drugs;20 its effects on mood are mediated primarily by activity on dopaminergic and serotonergic pathways.43 MDMA targets the serotonin transporter, stimulating serotonin (5-hydroxytrytamine [5-HT]) efflux and inhibiting 5-HT uptake.44,45 In rodents MDMA administration results in a neurodegeneration of 5-HT terminals and a long-term neurotoxic decrease in 5-HT in several brain regions,18 raising the possibility that the use of ecstasy may cause long-term neurotoxicity in humans.
Users report enhanced sensations and feelings of empathy and well being. Common short-term adverse effects include sweating, tachycardia, fatigue and muscle spasms including jaw clenching.43 By 1997 there were 53 reports in the UK of ecstasy producing severe acute toxicity resulting in death20. The most common mechanism appears to be fatal hyperthermia, complicated by disseminated intravascular coagulation (DIC), rhabdomyolysis, renal failure, cardiac arrhythmias and seizures.18,20,43 High environmental and core-body temperatures and muscular exertion from marathon dancing may lower the threshold for serious MDMA-associated adverse effects. Management of toxic ingestion of MDMA is largely supportive (Box 1).46 Treatments that may decrease mortality include active cooling measures (e.g., cool intravenous fluids)28 and possibly the use of the muscle relaxant dantrolene and anticonvulsant and sedative medications, particularly benzodiazepines.18 The extent to which dantrolene is of value is questioned, however; it too has dose-dependent adverse effects such as hepatitis.28 The use of neuroleptics requires care because of the theoretical risk of producing the neuroleptic malignant syndrome.18
Complications following ecstasy ingestion are unpredictable and do not appear to be dose dependent.43 Most people who use ecstasy experience no complications; however, uncertainty about the purity of the substance, possible contaminants and concomitant ingestion make it difficult to determine toxicity and predict medical consequences. The epidemiology is complicated by the fact that it is not compulsory to report overdoses or to test for the ingestion of illicit substances. In addition, self-reports are often not reliable because of the number of adulterates available; many of the pills sold at raves have logos on them for identification purposes, but tablets with the same logo stamp may not contain the same ingredients. An examination of tablets sold as ecstasy in Europe between 1995–1997 revealed that of 69 tablets with an identifying logo, 30 contained MDMA, with doses ranging from 2 mg to 149 mg; another 8 contained a mixture of substances including amphetamines, ephedrine, caffeine and aspirin. Overall, approximately 10% of drugs sold as ecstasy contain no active ingredient.43 A more recent study conducted in the UK reported that concentrations of MDMA varied 70-fold between tablets.47 The ingestion of ecstasy, as with most illicit drugs, essentially reduces to a game of Russian roulette because the contents of the tablets are unknown and unregulated and the dealers and suppliers are concealed and unaccountable.
In a bid to reduce harm the rave community has established organizations to educate ravers about pills and introduced ecstasy-testing kits and laboratory pill analysis programs.26 The plethora of anecdotal information on the Internet, however, no matter how well intentioned, can prompt the naïve user toward "irrational" rational drug use based on partial information and misinformation. Examples include the practice of "preloading;"26 concomitant ingestion of ecstasy with fluoxetine HCl (Prozac), 5-hydroxytryptophan, vitamin C or l-tyrosine in a bid to reduce neurotoxicity; and the concomitant ingestion of ecstasy and sildenafil citrate (Viagra) for enhanced "sextasy" effects.28
[Contents]
Harm reduction versus prohibition
Great Britain responded to the health risks posed by raves by attempting to prohibit them. Rave organizers faced fines of up to 20 000 pounds and 6 months in prison, and police were allowed to remove vehicles and sound equipment from any rave event. These measures seemed to fail because the parties simply moved into legitimate clubs, and this increased the risks involved with mixing drugs and alcohol. A recent UK survey of 16- to 29-year-olds showed that 9% of respondents had used ecstasy; this rose to 91% among members of the dance-club scene.43
Fig. 2: Volunteers with the Ottawa Association |  |
An alternative is to encourage harm reduction by ensuring that buildings meet safety and health standards, adequate security is provided to accommodate the large number of attendees and education about health effects (Box 2) is available from trained volunteers (Fig. 2) and from pamphlets and information cards (see Fig. 3). Such initiatives have been adopted by the rave community21,26 and municipal27 and public health authorities22 and are being considered by some provincial regulatory authorities.1 The inquest into Mr Ho's tragic death is investigating the circumstances surrounding his death as well as some of the broader issues and concerns associated with rave parties. Issues the inquest may explore include the promotion of raves, licensing requirements, security measures, emergency resources and sanitation.1 It is not clear if the more controversial and challenging issues such as the vetting of reliable drug information on the Internet or the provision of on-site drug testing will be addressed.
A recent study suggests the average raver's "shelf life" is only about 2 years4 — the time it might take to earn a graduated driving license or to realize, perhaps, that ecstasy is not empathy. For most youths rave attendance may simply be the collective rite of passage of a generation spurning individualism and materialism in pursuit of empathy and euphoria. During this passage physicians may need to offer the support and advice necessary to reduce the potential of harm. In the end we may not be able to deter Icarus from flying to the sun but might convince him to take frequent rests and replenish his fluids during the flight.
Competing interests: None declared.
 |
Send a letter to the editor Envoyez une lettre à la rédaction |
[Contents]
Dr. Weir is the Editorial Fellow of CMAJ and is a dual resident in Community Medicine and Family Medicine at McMaster University, Hamilton, Ont.
This article has been peer reviewed.
References
-
Inquest in the death of Allan Ho announced [press release]. Toronto: Ontario Ministry of the Solicitor General; 2000 Jan 27.
Prittie J. Canada's rave scene under microscope as inquest starts into participant's death. National Post [Toronto] 2000 May 9. Available: www.nationalpost.com (accessed 2000 May 24).
Smith AJ. "The third generation." The New Statesman and Society. 1992;Sept 11 (5):31-2.
Weber T. Raving in Toronto: peace, love, unity and respect in transition. J Youth Stud 1999;2(3):317-36.
Brown ER, Jarvie DR, Simpson D. Use of drugs at raves. Scott Med J 1995;40(6):168-71. [MEDLINE]
Buxton J, Craig C, Daly P, Bigham M, Bell A, Fyfe M. An outbreak of mumps among young adults in Vancouver, British Columbia associated with rave parties. Can J Public Health 1999;90(3):160-3. [MEDLINE]
Lenton S, Boys A, Norcross K. Raves, drugs and experience: drug use by a sample of people who attend raves in Western Australia. Addiction 1997;92(10):365-6.
Forsyth AJ, Barnard M, McKegancy NP. Musical preference as an indicator of adolescent drug use. Addiction 1997;92(10):1317-25. [MEDLINE]
Adlaf EM, Smart RG. Party subculture or dens of doom? An epidemiological study of rave attendance and drug use patterns among adolescent students. J Psychoactive Drugs 1997;29(2):193-8. [MEDLINE]
Forsyth AJ. Places and patterns of drug use in the Scottish dance scene. Addiction 1996;91(4):511-21. [MEDLINE]
Seymour HR, Gilman D, Quin JD. Severe ketoacidosis complicated by ecstasy ingestion and prolonged exercise. Diabet Med 1996;13(10):908-9. [MEDLINE]
Coore JR. A fatal trip with ecstasy: a case of 3,4-methylenedioxymethamphetamine/3,4-methylenedioxyamphetamine toxicity. J R Soc Med 1996;89(1):51P-2P.
Wollina U, Kammler HJ, Hesselbarth N, Mock B, Bosseckert H. Ecstasy pimples — a new facial dermatosis. Dermatology 1998;197(2):171-3. [MEDLINE]
Box SA, Prescott LF, Freestone S. Hyponatremia at a rave. Postgrad Med J 1997;73(855):53-4. [MEDLINE]
Sultana SR, Byrne DJ. Ravers hematuria. J R Coll Surg Edinb 1996;41(6):419-20. [MEDLINE]
Fidler H, Dhillon A, Gertner D, Burroughs A. Chronic ecstasy (3,4,methylenedioxymethamphetamine) abuse: a recurrent and unpredictable cause of severe hepatitis. J Hepatol 1996;25(4):563-6. [MEDLINE]
MacConnachie AM. Ecstasy poisoning. Intensive Crit Care Nurs 1997;13(6):365-6. [MEDLINE]
Green AR, Cross AJ, Goodwin GM. Review of the pharmacology and clinical pharmacology of 3,4 methylenedioxymethamphetamine (MDMA or "Ecstasy"). Psychopharmacology (Berl) 1995;119(3):247-60. [MEDLINE]
Hegadornen KM, Baker GB, Bourin M. 3,4-Methylenedioxy analogues of amphetamine: defining the risks to humans. Neurosci Biobehav Rev 1999;23(4):539-53. [MEDLINE]
Schwartz R, Norman M. MDMA and the rave: a review. Pediatrics 1997;100(4):705-8. [MEDLINE]
Toronto Raver Info Project. Contact: trip@ctchc.com.
City of Toronto Public Health Drug Prevention Centre. Available: www.city.toronto.on.ca/drugcentre (accessed 2000 May 22).
National Institute on Drug Abuse resource page on club drugs. Available: www.nida.nih.gov/NIDAHome1.html (accessed 2000 May 22).
Prevline. Prevention online. National Clearinghouse for Alcohol and Drug Information Web site. Available: www.health.org (accessed 2000 May 22).
The Lycaeum — an anectotal collection of drug information. Available: www.lycaeum.org/drugs (accessed 2000 May 22).
DanceSafe. A nonprofit organization established to promote health and safety within the rave and nightclub community. Available: www.dancesafe.org (accessed 2000 May 22).
A rave promoter Web site. Available: www.hullabaloo-raves.com (accessed 2000 May 22).
Jones A, Volans G. Management of self poisoning. BMJ 1999;319:1414-7. Available: www.bmj.com/cgi/content/full/319/7222/1414.htm (accessed 2000 May 1).
Canadian Pharmacists Association. Compendium of pharmaceuticals and specialties. 35th ed. Ottawa: The Association; 2000.
A rave promoter Web site. Available: www.skyjack.org (accessed 2000 May 22).
Tintinelli J, Kelen G, Stapczynski J. Emergency medicine — a comprehensive study guide. 5th ed. New York: McGraw-Hill Professions Division; 2000.
Salt P. Rave review. Nurs Times 1993;89(50):36-8. [MEDLINE]
Gilman AG, Rall TW, Nies A, Taylor P, editors. Goodman and Gilman's the pharmacological basis of therapeutics. 8th ed. Toronto: Pergamon Press; 1990.
Increasing morbidity and mortality associated with abuse of methamphetamine — United States, 1991–1994. MMWR 1995;44(47):882-6.
White M. Ya ba dabba doom. The Face 1999;35:110-4.
Li J, Stokes SA, Woeckener A. A tale of novel intoxication: a review of the effects of gamma-hydroxybutyric acid with recommendations for management. Ann Emerg Med 1998;31(6):729-33. [MEDLINE]
Gamma hydroxy butyrate use — New York and Texas, 1995–1996. MMWR 1997;46(13):281-3.
Kohrs R, Durieux M. Ketamine: teaching an old drug new tricks. Anesth Analg 1998;87:1186-93. [MEDLINE]
Dalgarnos PJ, Shewan D. Illicit use of ketamine in Scotland. J Psychoactive Drugs 1996;28(2):191-9. [MEDLINE]
Moore KA, Kilbane EM, Jones R, Kunsman GW, Levine B, Smith M. Tissue distribution of ketamine in mixed drug fatality. J Forensic Sci 1997;42(6):1183-5. [MEDLINE]
Pena BM, Krauss B. Adverse events of procedural sedation and analgesia in a pediatric emergency department. Ann Emerg Med 1999;34(4 pt 1):483-91. [MEDLINE]
Anonymous...such as ketamine [letter]. BMJ 1996;313:424. Available: www.bmj.com/cgi/content/full/313/7054/424.htm (accessed 2000 May 1).
Milroy CM. Ten years of 'ecstasy'. J R Soc Med 1999;92:68-72. [MEDLINE]
Rudnick G, Wall SC. The molecular mechanism of ecstasy (3,4-methylenedioxymethamphetamine (MDMA)): serotonin transporters are targets for MDMA-induced serotonin release. Proc Natl Acad Sci U S A 1992;89(5):1817-21. [MEDLINE]
Crespi D, Mennini T, Gobbi M. Carrier-dependent and Ca(2+)-dependent 5-HT and dopamine release by (+)-amphetamine, 3,4-methylenedioxymethamphetamine, p-chloroamphetamine and (+)-fenfluramine. Br J Pharmacol 1997;121(8):1735-43. [MEDLINE]
Rochester JA, Kirchner JT. Ecstasy (3,4-methylenedioxymethammphetamine): history, neurochemistry and toxicology. J Am Board Fam Pract 1999;12(20):137-42. [MEDLINE]
Sherlock K, Wolff K, Hay AW, Conner M. Analysis of illicit ecstasy tablets: implications for clinical management in the accident and emergency department. J Accid Emerg Med 1999;16:194-7. [MEDLINE]
© 2000 Canadian Medical Association or its licensors
![]()