
Public Health Agency of Canada
www.publichealth.gc.ca
Common menu bar links
Institutional links
Diseases & Conditions
Health & Safety
Research & Statistics
Agency Information
Search Box
E-mail this page
Research Update
Alcohol Use and Pregnancy: An Important Canadian Public Health and Social Issue
[Previous] [Table of Contents] [Next]
4 Women's Alcohol Use Patterns During Pregnancy
What the Studies Say It appears from the published data on women's use of alcohol during pregnancy that the rate of alcohol use has generally declined in both Canada and the US from the mid to late 1990s. However, it is important to emphasize here the limitations of self-report data as well as the frequent exclusion of marginalized women from survey data. Nonetheless, approximately one seventh of Canadian women (less than 15%) use alcohol while pregnant, and a similar but lower percentage was found in the US. Canadian women who report using alcohol during pregnancy appear to use it infrequently, although the data are limited. For women of childbearing age (18–44), the reported rate of alcohol use is similar, albeit slightly lower compared with the percentage of women who use alcohol in the general population. A small proportion of women report heavy drinking during pregnancy, though again the data are limited. Comparing the definitions of heavy drinking, both of which are linked to increased risk of damage to the fetus, it appears that a greater percentage of women engage in drinking 12 or more drinks a week than drink 5 or more drinks on one occasion. Canadian studies on the use of alcohol by pregnant Aboriginal women conclude a high rate and level of use; however, there have been limited comparisons made with other populations and there is a lack of clear understanding for this (e.g. possibly more candid self-reporting by Aboriginal women, the influence of other mitigating factors such as poverty).
4.1 Drinking While Pregnant and Levels of Consumption
It is important to state at the outset that the lives of the women conveyed in the data should not be judged, as this would contribute to the detrimental stigma that surrounds women who use alcohol during pregnancy. Further, although the women are using a substance while pregnant, in nearly all cases, they had started before becoming pregnant.52 An evaluation report by Poole (2000) of the Sheway Project for high-risk and pregnant and parenting women reminds us in her review of the international literature that “women using substances during pregnancy have been described both as struggling with the many pressures put on them and demonstrating remarkable strength and resourcefulness.53 This cannot be forgotten.
… the lives of the women conveyed in the data should not be judged, as this would contribute to the detrimental stigma that surrounds women who use alcohol during pregnancy.
Insight: Who's at Risk?...Because Risks Change and Vary
Although women who drink during pregnancy are at risk of having a child with FASD, prevalence and incidence rates of the former cannot be equated with prevalence and incidence rates of the latter. Also, women who drink during pregnancy are not a homogeneous group, and include women who are alcohol dependent, women who abuse alcohol on an episodic basis, and women who drink infrequently or regularly at low amounts. Amount, timing and frequency of alcohol intake, alongside other factors such as mother's health and genetic susceptibility of the fetus, are critical factors in determining risk for FASD.
The collection of information on women's use of alcohol during pregnancy may be undertaken through the use of three methodologies:
- self-report questionnaires and interviews
- screening tools
- biomarkers
First, most of the information collected on alcohol use in pregnancy is based on self-report data gathered through interviews, self-administered questionnaires and intake histories administered for either clinical or research purposes.54 In addition to the limitations identified with survey questionnaires above, the use of self-report methodologies to collect information about alcohol use in pregnancy is further limited by the associated social stigma, feelings of guilt and shame and/or fear of repercussions (including fear of child welfare involvement and, in some jurisdictions in the US, incarceration).55-57 The validity of self-report data may be enhanced when it is gathered in the context of a respectful, nonjudgmental, ongoing and trusting relationship in which women are engaged with a health care or social service provider.58
Second, the use of screening tools to identify levels of alcohol use in pregnant women is a potentially good source for data, but at present there is no consistent application of screening tools. In addition, some health care professionals hesitate to use them (reasons include absence of training in use of the tools and no coverage for their use in medical plans).59 The screening methodology also relies on self-report and is therefore limited by the factors discussed above. Once again, the ability of women to be honest in their responses on screening tools is enhanced if the tools are administered within the context of a respectful, trusting and ongoing relationship with a service provider.
|
Multiple Risk Factors The Saskatoon Pregnancy and Health Study found that 36% of the women interviewed reported engaging in two risk behaviours during the first trimester of their pregnancy, the most common combinations being alcohol and caffeine use (24%). About 16% of respondents reported three risk behaviours, which were in almost all cases drinking, smoking and caffeine consumption.63 |
Third, biological markers are a means to collect information after a woman has delivered a baby. Biomarkers (hair and meconiumxiv) are biological data taken from the neonate in order to identify a mother who has used alcohol at risky levels in her pregnancy and to identify an infant who has been exposed. The use of biomarker data to identify women and children is not routinely used in Canada, and remains controversial. Further research has been recommended,60 with the stipulation that it must be conducted alongside an inclusive social and legal-ethical policy debate regarding the use of biomarkers to identify women and children. Keeping these limitations in mind, the data that are available are nonetheless important to help to begin to identify drinking patterns among pregnant women that in turn can be used to inform current discussions on what works best to respond to pregnant women's use of alcohol and related harms.
The use of alcohol by women during pregnancy is an important issue to examine on its own. However, it is necessary to preface this discussion with the recognition that alcohol use, and most specifically alcohol abuse, commonly occurs in combination with other substances. It is widely acknowledged that heavy substance-using women rarely use a single substance.61,62 It is also recognized that not all substances are equally harmful, and associated factors such as combinations of use, levels of exposure and related risk behaviours contribute to differing outcomes. The Maternal Health Practices and Child Development Study in the US (Pennsylvania) reported that 76% of adult women who smoked during the first trimester of pregnancy also used alcohol.64 Further, among pregnant US teenagers surveyed, 61% who smoked during the first trimester of their pregnancy also reported drinking alcohol.65 This has important implications for effective responses to pregnant women's use of alcohol and related harms in that alcohol use cannot be viewed in isolation from other potentially harmful behaviours or from the realities of women's lives (e.g. poverty, low social support) that lead to the behaviours.
Keep in mind that there are weaknesses with survey data.66 It is also evident in the presentation of the survey findings that many of the datasets are not comparable, and so what emerges are “pieces of a picture” that together provide as complete a picture as possible. As will be relayed in the recommendation section, there is much need for improvement in the data that are collected in Canada on women's drinking during pregnancy to provide an accurate portrayal. The intent of this overview is to provide a general statement based on often very disparate and incomplete survey findings.
The percentage of women reporting alcohol use during pregnancy has recently decreased in Canada.67 The most recent published data on the prevalence of women's use of alcohol during pregnancy is located in the 2005 overview, Report on Maternal and Child Health in Canada, which relayed that “roughly 14% [of mothers] reported drinking alcohol (any amount) during pregnancy.”68 Similarly, the 2000-01 CCHS indicates that 13.7% of all women who reported using alcohol in their lifetime also consumed alcohol during their last pregnancy. Similar findings were also reported in the 1998-99 National Longitudinal Survey of Children and Youth (NLSCY): 14.4% of women reported drinking at some point during their pregnancy, and 4.9% drank throughout.69 Comparing these ratesxv to the 1994-95 National Population Health Survey (NPHS) and the 1994-95 NLSCY, these surveys similarly reported that between 17% and 25% of women drank alcohol at some point during their pregnancy, and between 7% and 9% drank alcohol throughout their pregnancy.70,71 For the most part, women who reported drinking during their pregnancy in the 2000-01 CCHS did so infrequently: 75.4% drank less than once per month, 9.7% once per month, 6.5% two or three times per month, 5.3% once per week and 1.3% drank every day.72
Insight: Self-Reporting – Does It Reveal the Whole Picture?
The above findings are comparable to results from a 2000 survey of Canadian women's views on whether they would drink should they become pregnant; 85% said they would not.73 However, in a 2002 poll of Canadians' perceptions and opinions about women's use of alcohol during pregnancy, 22% felt that more than one third of pregnant women consumed alcohol.xvi, 74 Although the comparability of this Canadian poll data to pregnant women's self-reported use of alcohol is limited, it is interesting to note that this finding is considerably higher in comparison to the self-report data discussed.
In comparison, the 2002 US Behavioral Risk Factor Surveillance System survey established that approximately 10% of women reported alcohol use while pregnant.75 Using data from the same survey, the US Centers for Disease Control and Prevention found that the rate of any alcohol use during pregnancy declined from an average of 14.6% between 1988 and 1995 to 12.8% in 1999.xvii, 76 The drinking rate and decline match the Canadian findings.
Insight: Did You Know?
The 1996-97 NPHS found that 51% of sexually active 15- to 19-year-old females in Canada had sex without a condom without the explicit intention of becoming pregnant in the year prior to the survey.77
In the absence of available data on the prevalence of women's use of alcohol during pregnancy, drinking by women of childbearing age (typically defined as 11–44, 15–44 or 18–44 years) is often examined for insight. These data are also valuable because approximately 40% of pregnancies are reported to be unplanned, with higher rates among teenage and older women.78 A 2004 Alberta Alcohol and Drug Abuse Commission (AADAC) report analyzed the 2000-01 CCHS, comparing women 18 to 44 years of age who were or were not pregnant at the time of the survey. It is important to mention that most of the CCHS questions asked about the previous 12 months, so responses from women who were pregnant at the time of the study may reflect alcohol use prior to their pregnancy. Overall, 72.8% of women of childbearing age in Canada who were pregnant at the time of the survey, and 82.3% of those who were not, reported drinking alcohol in the past 12 months. Although not an equivalent study population, the 2002 US Behavioral Risk Factor Surveillance Survey found that more than half of female respondents who were of childbearing age (18–44), and were not using birth control, reported using alcohol.79
In AADAC's analysis of CCHS data for Alberta, women who were pregnant at the time of the survey were much less likely to drink on a regular basis (defined as at least once per week) than women who were not pregnant: 41.6% of pregnant women and 32.1% of nonpregnant women reported drinking less than once per month; 19.3% versus 16.2% drank once per month; 22.3% versus 20.2% drank 2 to 3 times per month; 11.1% versus 17.6% drank once per week, 5.8% versus 9.7% drank 2 to 3 times per week, and 2.1% of nonpregnant women drank 4 to 6 times per week and 2.0% drank every day.80 These numbers are encouraging in that they are lower in comparison to the CCHS data on the frequency of alcohol use by all Canadian women, keeping in mind that the ages and populations of the women are different.
|
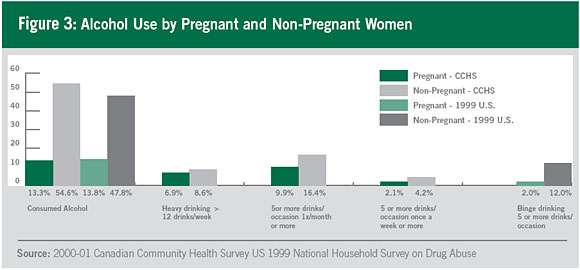
Heavy Drinking Rates The 2000-01 CCHS also measured heavy drinking as regularly drinking more than 12 drinks per week, and 6.9% of pregnant women at the time of the surveyxx and 8.6% of non-pregnant women reported heavy drinking. In examining heavy drinking in the week prior to the survey, 0.5% of pregnant and 3.6% of nonpregnant women reported drinking more than 12 drinks. Of those surveyed, 12.5% of pregnant and 47.7% of nonpregnant women reported consuming between 1 and 9 drinks in the week prior to the survey.84 In the US, the Centers for Disease Control and Prevention found that in 1999 more women reported heavy drinking while pregnant compared with pooled estimates of such drinking from 1998 to 1995. Specifically, 2.1% of women in 1999 reported having 7 or more drinks a week and 3.3% reported having 5 or more drinks on one occasion.85 The literature indicates that heavy drinking has a higher association with adverse pregnancy outcomes.86 |
Examining the use of alcohol in the week prior to the 2000-01 CCHS, 13.3% of pregnant women in Canada and 54.6% of nonpregnant women reported drinking. There were similar findings in the US 1999 National Household Survey on Drug Abuse, in which it was estimated that 13.8% of women 15 to 44 years of age and pregnant, and 47.8% of women who were not pregnant and of childbearing age consumed alcohol.81
Drawing on the 1994-95 NPHS and the 1994-95 NLSCY to examine levels of alcohol use among women who reported drinking alcohol at some point during their pregnancy, 94% consumed fewer than 2 drinks on the days they drank, 3% had between 3 and 4 drinks, and less than 3% drank 5 or more drinks.82 The 2000-01 CCHS measured heavy drinkingxviii among women who reported drinking in the past year, and found that 9.9% of pregnant women at the time of the surveyxix and 16.4% of non-pregnant women reported having 5 or more drinks on one occasion once a month or more, and 2.1% of pregnant women and 4.2% of non-pregnant women reported consuming 5 or more drinks on one occasion once a week or more. Comparably, the 2002 US Behavioral Risk Factor Surveillance Survey found that 2% of pregnant women and 12% of women of childbearing years (18–44) engaged in binge drinking (5 or more drinks on one occasion).83
|
Disproportionate Focus on Aboriginal Women Canadian studies on women's use of alcohol during pregnancy, in particular in relation to FAS and FASD, disproportionately focus on Aboriginal women and the geographic areas in which they live.89 Further, Canadian studies of FAS/FAE prevalence rates have focused on Aboriginal communities where alcohol abuse and dependency are known to be high. This raises the concern that the high prevalence rates of FAS/FAE found in these communities will be used to describe rates of FAS/FAE in the general Aboriginal population.90 |
There are also provincial and local Canadian studies that report on the rate of women's drinking while pregnant and their levels of consumption. The studies often differ in methodologies and populations, and therefore are not easily comparable. Nonetheless, they add valuable insight into the subject area. A large majority focus on what they variously define as high-risk women. For example, the Saskatoon Pregnancy and Health Study accessed pregnant women for interviews through a prenatal program (not high-risk) and an outreach program (high-risk). Approximately 46% of the women interviewed reported drinking alcohol during the first three months of their pregnancy, with 75% consuming fewer than 2 drinks a week on average.87 A study of pregnant women in Toronto who were seeking counselling found that 3.1% of clinic patients and 0.8% of telephone clients reported having 5 or more standard drinks per occasion at some point during their pregnancy.88
The focus on Aboriginal communities with high rates of alcohol abuse and regions with large concentrations of Aboriginal peoples has meant that Canada lacks epidemiological data regarding other populations, making it difficult to determine whether or not Aboriginal women are at greater risk than other groups. Further attention also needs to be paid to the methodology surrounding studies with Aboriginal populations (e.g. possibly more accurate account of alcohol use by Aboriginal women because of the acknowledgement that alcohol use/abuse is a health and social problem among their people91 and greater attention on the influence of mitigating factors, such as poverty).
xiv. Meconium is the first stool of a newborn child.
xv. The CCHS analyses are for females 12 and older; however, the question is specific to the respondent's last pregnancy, making the data comparable to the NPHS and NLSCY.
xvi. Consumed alcohol more than once a week.
xvii. From the late 1980s to the mid 1990s, there was a reported increase in women's alcohol use during pregnancy by the US Centers for Disease Control and Prevention.
xviii. Also termed binge drinking.
xix. Recall the caveat in the collection of the data discussed above.
xx. Again, recall the caveat in the collection of the data discussed above.
[Previous] [Table of Contents] [Next]