
Public Health Agency of Canada
www.publichealth.gc.ca
Common menu bar links
Institutional links
Diseases & Conditions
Health & Safety
Research & Statistics
Agency Information
Search Box
E-mail this page
Research Update
Alcohol Use and Pregnancy: An Important Canadian Public Health and Social Issue
[Previous] [Table of Contents] [Next]
5 Characteristics and Circumstances of Women Who Use Alcohol During Pregnancy
What the Studies Say The co-existing conditions experienced by pregnant women who use alcohol are generally related to other substance use (e.g. illicit drugs, tobacco), mental health (e.g. cognitive impairments, depression) and life circumstances (e.g. violence, low social support). Recent Canadian surveys and studies contribute a partial understanding of the characteristics and life circumstances of women who use alcohol while pregnant. Though the data are sporadic and some focus only on one province, it is still meaningful. Overall, women who have higher incomes and are older are more likely to report drinking alcohol during their pregnancy, younger and older women are more frequent drinkers, and younger women are much more likely to drink 5 or more drinks on one occasion as well as to have the lowest incomes. There is limited information available on regional variations, but what does exist shows the highest rates of alcohol use during pregnancy by women in Quebec and the lowest rates in Atlantic Canada. The need for further research is clear.
5.1 Issues Faced by Pregnant Women Who Use Alcohol
Current research indicates that, for many women, pregnancy is a reason to reduce or stop alcohol use.92-95 However, this is not the case for all women. Further, it is important to recognize that not all women discover their pregnancy immediately, and therefore continue to drink into their first trimester and for some even beyond. This may lend insight into the profile of women who drink during pregnancy. It is important to know not only the rates, frequency and levels at which women drink during pregnancy, but also their characteristics and circumstances, to help inform current discussions on what strategies and approaches are most effective. Similar to the review of data on women's use of alcohol, the surveys and research reported in this section do not provide a complete understanding. They do, however, provide a starting point for describing women who drink while pregnant and the breadth of interconnected factors that influence their lives. This is necessary to accurately and comprehensively identify risk factors for specific populations.96
A 2004 report on substance abuse treatment and care for women released by the United Nations, Office on Drugs and Crime, described women with substance use problems as generally
…having fewer resources (education, employment, income) than men, are more likely to be living with a partner with a substance use problem, have care of dependent children and have more severe problems at the beginning of treatment.… [They] also have higher rates than men of trauma related to physical and sexual abuse and concurrent psychiatric disorders, particularly post-traumatic stress disorder and other mood and anxiety disorders (1).
According to the Canadian literature on women's use of alcohol during pregnancy, there is a vast interplay of issues that pregnant females face alongside their substance use. One factor previously mentioned is use of other substances. Additional factors relate to social, legal and health issues97-101 (see Table 1). It is important to acknowledge that complete agreement on these factors does not exist among the various studies,102 but they do reflect a pattern that is also seen in the US literature.103-109 It is also important to recognize that among Aboriginal women in Canada these factors frequently reside in the context of colonial oppression and its aftermath, such as ongoing social and economic marginalization and the intergenerational link between residential schooling and FAS/FASD among Aboriginal peoples.110
|
Table 1: Summary of Co-existing
Conditions Experienced by Pregnant Women Who Use
Alcohol
|
|
| sole parenting | violence, abuse, sexual exploitation, trauma |
| child(ren) in custody/changes in custody | involvement in the criminal justice system |
| low income/social economic status/poverty | low social support |
| limited access to prenatal/postnatal care services | previous birth of a child with prenatal and exposure to alcohol and/or other substances |
| feeling/experiencing loss of control | low education and literacy levels |
| menial, low-paying employment problems | concurrent physical and mental health |
| cognitive impairments, possibly due to FASD | co-existing use of other substances |
| unplanned pregnancy/pregnancies low self-esteem | shame |
| historical and cultural factors pregnancy | depression and other mental health issue(s) |
| older in age | heavy consumption of alcohol prior to inadequate nutrition |
| mother's own prenatal exposure to alcohol, tobacco or other drugs | alcohol, tobacco or other drug exposure at young age |
| poor early childhood environment of the women (stress, abuse, neglect) | paternal/partner alcohol and drug use during the pregnancy |
| physical, mental, social and spiritual imbalance | unstable housing and living conditions |
Some insight into the co-existing conditions that pregnant alcohol-using women face can also be acquired from the study of birth mothers of children diagnosed with FAS. A leading research project in Washington State in the US by Astley et al. (2000) generated a profile of women who had given birth to a child diagnosed with FAS and identified factors that helped and/or hindered the mother's ability to achieve abstinence.xxiii, 111 Of 80 women enrolled in the study, 50 had achieved abstinence by the time of their interview and 25 did not. Similar to the characteristics reported above, overall the women were identified as high risk, many of them dealing with mental health issues as well as victimization from abuse. The authors reported on the life circumstances of women who had achieved abstinence as having, on average:
significantly higher I.Q.s, higher household incomes, larger more satisfactory social support networks and were more likely to report a religious affiliation. While they were equally likely to have mental health disorders, those who had achieved abstinence were more likely to have received treatment…. Those who had achieved abstinence reported higher levels of drinking just before the birth of the index child and were more likely to have parents who had problems with alcohol use (513).
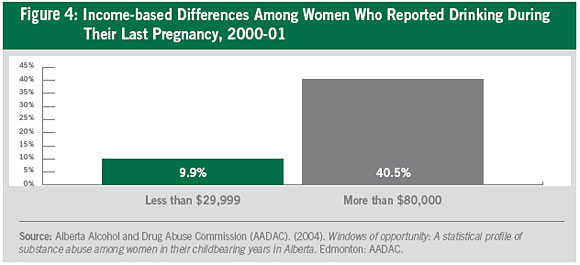
AADAC's analysis of 2000-01 CCHS data for Alberta revealed clear income-based differences among women who reported drinking alcohol during their last pregnancy. Women with higher incomes were more likely to report drinking: 40.5% of women with an income over $80,000 reported drinking, and this rate steadily declined to 9.9% of women with an income of $29,999 and under.112 This finding for Alberta is supported in analyses of Canadian data in the 1994-95 NPHS and the 1994-95 NLSCY. Both surveys reported that alcohol use during pregnancy was most common among women with higher incomes.113
|
Regional Variation in Alcohol Use There was little information located on regional variation in alcohol use by pregnant women; however, analysis of the 1998-99 NLSCY reported the highest rate of use in Quebec (25.1%) and the lowest in Atlantic Canada (7.7%).121 This was also found in the analysis of the 1994-95 and 1996-97 NLSCY.122,123 In addition, a 2000 survey of Canadian women found that women in Quebec were much less likely to state that they would stop using alcohol if they were to become pregnant.124 |
The 1994-95, 1996-97 and 1998-99 NLSCY data also indicate that women who are older are more likely to report alcohol consumption during pregnancy. The most recent 1998-99 NLSCY data reveal that 14.1% of children under 2 and whose mothers were under 25 at the time of the survey were exposed to some alcohol prenatally compared with 21.6% of children whose mothers were 35 years and older.114
AADAC also examined the frequency of alcohol intake by women in Alberta who were pregnant at the time of the survey. It was found that women of childbearing age in the youngest age group (18–20) were the least likely to drink less than once per month. Women in both the youngest and oldest groups (18–20 and 31–44) were more likely to be frequent drinkers (between one and six times a week) than women between 21 and 30.115 It is noted in the report that this finding fits with the US research showing more frequent drinking among women of college age and those who are older.116
Examining the amount of alcohol consumed per occasion by Alberta women of childbearing age (18–44), young women were most likely to report drinking 5 or more drinks on one occasion (14.1% of women 18–20 years of age drank this amount once or more per week versus 6.2% in the 21–25 age group). In the two oldest age groups (26–44), only 3% of women reported consuming 5 or more drinks on one occasion once or more per week. Once again, the report acknowledges that this finding is consistent with other research on drinking patterns, including US studies.117 To illustrate, the 2002 US Behavioral Risk Factor Surveillance Survey reported that binge drinking for women who are pregnant and women of childbearing age is highest among 18- to 24-year-olds (19.4%), followed by 25- to 34-year-olds (13.1%) and then those 35 to 44 years of age (8.6%).118 So, although higher income pregnant women in Alberta were more likely to be drinkers, when they did drink, lower income pregnant women were more likely to binge drink (i.e. drink 5 or more drinks on one occasion) once per month or more (22.4% of women with incomes between $10,000 and $19,000) and once per week or more (9.2% of women with incomes less than $10,000, 5.7% in the $10,000 to $19,999 income group, and 4% to 5% in income groups over $20,000).119 The Saskatoon Pregnancy and Health Study similarly determined that pregnant women with higher incomes were more likely to use alcohol.120
xxiii. Abstinence was defined as "consumed no alcohol or consumes minimal quantities only on special occasions" Astley, S., Bailey, D., Talbot, C., & Clarren, S. (2000). Fetal alcohol syndrome (FAS) primary prevention through FAS diagnosis: II. A comprehensive profile of 80 birth mothers of children with FAS. Alcohol & Alcoholism, 25(5), p. 513.
[Previous] [Table of Contents] [Next]