
|
|
|
The Left Atrium
Contents
• Good people in bad systems [PDF] • Bitter pills [PDF] • Office visit [PDF] • A trip to the mall [PDF] • Bodysnatching in Canada [PDF] Good people in bad systems To err is human: building a safer health system Linda T. Kohn, Janet M. Corrigan and Molla S. Donaldson, editors Washington: National Academy Press; 2000 312 pp. US$34.95 (cloth) ISBN 0-309-06837-1
Early on, the book provides alarming statistics about the frequency of medical errors and emphasizes the disparity between the true incidence of those errors and the public's often optimistic perception of a health care delivery system that almost always operates flawlessly. Later, the authors cover the conventional "human factors" issues in discussions of why errors occur, how they should be reported and what can be done to help prevent them. (Strangely, little emphasis is placed on long work shifts and sleep deprivation, problems that almost all residents will attest to.) The authors also discuss how the "forces of legislation, regulation, and market activity" influence the quality of clinical care.
However, the authors go beyond a conventional treatment of the problem of human error by offering a national agenda for designing a safer health care infrastructure that will reduce mistakes and improve patient safety. Such an initiative, they argue, will improve patient safety through more effective health care leadership, better data collection and analysis and a higher level of safety awareness. The problem, they argue, "is not bad people in health care — it is that good people are working in bad systems that need to be made safer."
Not everyone is happy with the methodology and conclusions of this book, as indicated by extensive commentaries and critiques published in JAMA, the New England Journal of Medicine and elsewhere. Still, if raising consciousness of the problem of human error in medicine was their main objective, the authors have succeeded admirably.
Easy to read and relatively free of jargon, this book can be covered at a single sitting. It is the first in a series of publications from the Committee on Quality of Health Care in America, an initiative of the Institute of Medicine of the US National Academy of Sciences. Many books from the National Academy can be read free online; including To Err Is Human: Building a Safer Health System.
D. John Doyle Contents
• Good people in bad systems [PDF] • Bitter pills [PDF] • Office visit [PDF] • A trip to the mall [PDF] • Bodysnatching in Canada [PDF] Lifeworks Bitter pills
Colleen Wolstenholme wears a simple silver pendant around her neck. At first glance, it looks like a small amulet or good-luck charm. It is, however, a provocative comment on the use of drugs and the treatment of women in contemporary society.
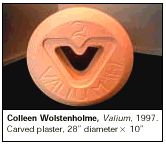
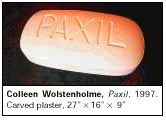
Wolstenholme, an artist now living in Hantsport, Nova Scotia, has created a line of jewellery — pendants, earrings, bracelets — that replicate the design of name-brand psychotropic medications such as Valium, Zoloft, Xanax, Dexedrine and Paxil. They make a fashion statement and a political one. Wearing the jewellery has become for some people, particularly women, a badge of honour. They no longer feel ashamed at taking antidepressants, says Wolstenholme. They no longer have to hide the fact from friends and coworkers. "For me," she adds, "it's about being honest. Society likes to sweep this under the rug."
The 37-year-old artist, who majored in sculpture at The Nova Scotia College of Design and received a Master of Fine Arts in goldsmithing from New York State University, began her exploration of women's issues as a reaction to images of rail-thin women in the media. She created a 12" × 8" wooden wardrobe that housed, instead of the dresses and shoes one might expect, fabric female genitals. From here, Wolstenholme created a seven-foot, five-sided padded cell reminiscent of a confessional. Locking women away within the confines of religion or in a mental institution was the old way of treating women, she explains. The new way is drugs.
From wardrobes and padded cells, Wolstenholme moved to oversize reproductions of pills weighing as much as 150 pounds, reflecting the weight they carry in our society. The giant plaster sculptures — blindingly white, evoking sterility and pallor — made their first public appearance at "grunt," a gallery of contemporary art in Vancouver, as part of a show called Desire, a travelling exhibition that recently had its last show in Halifax.
"I like people to be able to look at my work and 'get' it," Wolstenholme says. "I'm not into the ivory tower approach to art."
There doesn't seem to be any doubt that Wolstenholme is getting her message across. She has toured with Lilith Fair, the premiere rock festival for women musicians, selling her jewellery, and her exhibitions have been well received.
Empathy is at the core of her work, Wolstenholme says. Having received medical treatment for depression several years ago, she empathizes with women who need to discuss their mental health openly and without embarrassment. She understands their desire to feel valued in a world that, historically, has been dismissive of their needs.
Donalee Moulton Contents
• Good people in bad systems [PDF] • Bitter pills [PDF] • Office visit [PDF] • A trip to the mall [PDF] • Bodysnatching in Canada [PDF] Illness and metaphor Office visit
Dr. Helmcken's office was a tiny two-room cottage on the lower end of Fort Street near Wharf Street. It sat in a hummocky field; you walked along two planks and came to three steps and the door. The outer room had a big table in the centre filled with bottles of all sizes and shapes. All were empty and all dusty. Round the walls of the room were shelves with more bottles, all full, and lots of musty old books. The inner office had a stove and was very higgledy-piggledy. He would allow no one to go in and tidy it up.
The Doctor sat in a round-backed wooden chair before a table; there were three kitchen chairs against the wall for invalids. He took you over to a very dirty, uncurtained window, jerked up the blind and said, "Tongue!" Then he poked you round the middle so hard that things fell out of your pockets. He put a wooden trumpet bang down on your chest and stuck his ear to the other end. After listening and grunting he went into the bottle room, took a bottle, blew the dust off it, and emptied out the dead flies. Then he went to the shelves and filled it from several other bottles, corked it, gave it to Mother and sent you home to get well on it. He stood on the step and lit a new cigar after every patient as if he was burning up your symptoms to make room for the next sick person.
Emily Carr
From Emily Carr, "Doctor and Dentist," Contents
• Good people in bad systems [PDF] • Bitter pills [PDF] • Office visit [PDF] • A trip to the mall [PDF] • Bodysnatching in Canada [PDF] Room for a view A trip to the mall
My first stop was the pharmacy, to fill a prescription for the bowel prep for my upcoming (q 50 years) flexible sigmoidoscopy. A hedge against the long-term risk of colon cancer. As for the short term, I moved to my next station in the mall: the gas mask distribution centre.
Although the West may have forgotten Saddam Hussein, he is still a well-recognized threat in Israel. There is good evidence, despite the best efforts of the UN inspectors (who have been off the job for two years, anyway) that Hussein still has a clutch of missiles ready to drop nerve gas and other biological weapons on our heads. (No matter that only a kilometre away from our neighbourhood live thousands of Arabs who would also suffer from such a terrorist act.) With this danger in mind, the Home Front of the army asks us, both Jews and Arabs, to periodically update our gas-mask kits — which contain, among other things, an atropine syringe for use against nerve gas.
Given the upsurge of violence in Israel and the territories, it is hard to deny the possibility that the whole region might spiral downward into war, making the upgrading of the family gas masks all too relevant. Hence my trip to the mall.
A sound and light show has been played over our houses for 15 of the last 21 January evenings. Somewhere around 7:30, just in time to make the evening news at 8:00, the machine guns begin to shoot from Beit Jala, a suburb of Bethlehem, toward Gilo, a suburb of Jerusalem. When I am foolish enough to venture onto the front lawn, I can even observe the tracers. Just last night, one of the bullets found its mark in the neck of an Israeli woman standing at her window.
Shortly after our neighbours shoot at us, the Israeli army fires back, trying with mixed success to quell the gunfire. The sounds of this fighting are very close, echoing off the stony hills of Jerusalem.
It's amazing how one gets used to such things. At first, the noises and flashes were terrifying. After a few nights my terror was supplanted by a sickening feeling in the pit of the stomach, especially when I tried, unsuccessfully, to convince my small children that the bullets would not reach our house.
It is clear that both sides are suffering. From my side, I know that most Israelis yearn for peace, and that only a negotiated settlement will put an end to the fighting. In the meantime, I wait, hope and pray for talks to resume: as Winston Churchill once said, "To 'jaw jaw' is better than to 'war-war.'" And I contemplate the question that people ask me: Will the fighting drive me back to Canada? I have always loved my native land a mari usque ad mare, but the Jews have waited to return to their native homeland for 2000 years. I think I will stick around to do my part, hoping that the gas masks and atropine syringes will stay in their cartons and that two peoples will learn, one day, to share this small patch of land in peace. I'll undergo my colon cancer screening test, and I'll keep the gas masks handy. Just to keep all the possibilities covered.
A. Mark Clarfield Contents
• Good people in bad systems [PDF] • Bitter pills [PDF] • Office visit [PDF] • A trip to the mall [PDF] • Bodysnatching in Canada [PDF] Past progressive Bodysnatching in Canada This article should have included the following acknowledgement: "The author thanks Dr. Tom Ringrose (preceptor) and Ms. Arty Coppes-Zantinga for their helpful suggestions during the preparation of this article and Dr. William Whitelaw for the support provided through the Calgary History of Medicine Club." [CMAJ 2001;164(8):1129]
The nefarious practice of bodysnatching is probably as old as the study of anatomy, but on this continent it was roughly coeval with the founding in 1756 of the first American medical school, in Philadelphia. Canada's first medical school was established in Montreal considerably later, in 1822, but the days of "the resurrection men" were far from over. By 1850 there were 42 medical schools in the United States and Canada, and with them had arisen a need for anatomical specimens. But the lack of legally available cadavers drove professors and students to obtain their raw material by clandestine means.1
The robbers were usually medical students, who stole bodies for their own study or sold them to anatomy instructors. In doing so, they continued a longstanding tradition of their European counterparts; for example, in early 18th-century Edinburgh, students at the Royal College of Surgeons were required to sign an agreement not to engage in grave robbing.1 In Canada, bodysnatching was practised by both English- and French-speaking medical students, although with slightly different motivations. Francophone students tended to be poorer than their anglophone counterparts and needed the money to pay for their education.2,3 By contrast, English-speaking students tended to join bodysnatching expeditions more out of a spirit of daredevilry. They were frequently intoxicated and hence frequently caught.3
To evade detection by the authorities, school staff developed ways to spirit away their corpses at a moment's notice. In some places a pulley was used to hoist the cadaver up the chimney. Alternatively, a block and tackle might be rigged to raise the corpse through a trap door into a domed ceiling: "At the first sign of trouble, up went the corpse ... . The students then shut the trapdoor and removed the ladder ... a rapid scrub down — and the searchers would find absolutely nothing."4 To further confuse the authorities and make identification of the corpse difficult, the corpse's head would be skinned and scars excised.
To avert public outrage the robbers were selective. McGill graduate Dr. Griffith Evans reminisced in 1862 that "plenty of negroes were obtained cheap, packed in casks, and passed over the border as provisions, or flour."4 Robbers would also prowl potter's fields, churchyards, hospitals and poorhouses.4
Although penalties for bodysnatching were increased, such desecrations were rarely prosecuted, for the authorities sympathized with the plight of the medical schools.4 Consequently, the emphasis shifted from punitive legislation to the creation of laws that would make corpses available. An Act to Regulate and Facilitate the Study of Anatomy was passed in the Legislative Assembly of the Province of Canada in 1843 and later amended in 1883. As a result, the Canadian Medical and Surgical Journal was able to report in 1884 that the robbing of graves in Canada had ceased.2
Deepa Francis References
Copyright 2001 Canadian Medical Association or its licensors |
 Aimed at the nontechnical reader, To Err Is Human deals openly and frankly with medical errors and their consequences, focusing primarily on the situation in the United States. The authors argue that human error in US health care is a leading cause of patient morbidity and mortality, and they provide evidence that "at least 44 000 and perhaps as many as 98 000 American die in hospitals each year as a result of medical errors." This is more than the total number who die in the US every year as a result of traffic accidents, breast cancer and AIDS. No doubt, a similar problem exists in Canada.
Aimed at the nontechnical reader, To Err Is Human deals openly and frankly with medical errors and their consequences, focusing primarily on the situation in the United States. The authors argue that human error in US health care is a leading cause of patient morbidity and mortality, and they provide evidence that "at least 44 000 and perhaps as many as 98 000 American die in hospitals each year as a result of medical errors." This is more than the total number who die in the US every year as a result of traffic accidents, breast cancer and AIDS. No doubt, a similar problem exists in Canada.
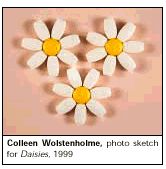 Wolstenholme is now expanding her pharmacologic theme in a new show slated to open at the SAW Gallery in Ottawa in April 2002. The centerpiece of this work is, again, giant pills, this time arranged to look like daisies. The centre of each daisy is a yellow amitriptyline; the petals are white Buspar.
Wolstenholme is now expanding her pharmacologic theme in a new show slated to open at the SAW Gallery in Ottawa in April 2002. The centerpiece of this work is, again, giant pills, this time arranged to look like daisies. The centre of each daisy is a yellow amitriptyline; the petals are white Buspar.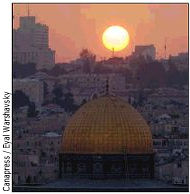 What a ridiculous figure I must have cut: a middle-aged, balding doctor, dressed for work in my sports jacket, tie and cuffed pants with the family's five gas-mask kits slung over my shoulder. I was on my way to our local shopping mall (the only one in Jerusalem, in fact) to look after my health. For the short and the long term.
What a ridiculous figure I must have cut: a middle-aged, balding doctor, dressed for work in my sports jacket, tie and cuffed pants with the family's five gas-mask kits slung over my shoulder. I was on my way to our local shopping mall (the only one in Jerusalem, in fact) to look after my health. For the short and the long term.
