Introduction
From 2005 to 2020, the anticipated increase in deaths from cancer in the world is 104%, whereas the anticipated increase is 180% in the Arab region (Rastogi, Hildesheim & Sinha, 2004). In the Arab region, breast cancer (BC) is the first type of cancer in incidence and mortality rates (WHO, 2009). The region witnesses more than 60% of reported BC cases detected at a late stage, stage III or higher, “when cure is improbable even with the best treatments” (Ibid: 18).
BC represents the most frequent and growing cancer in females (and sometimes in males and females combined) in the four countries under study—Egypt, Jordan, Morocco, and Oman (e.g., MoH Egypt, 2010; MoH Jordan, 2008; MoH Morocco, 2009; MoH Oman, 2009). Each country has three types of agents for BC preventative and early detection measures: cancer agent (CA), government agent (GA) or ministry of health (MoH), and World Health Organization (WHO) office. In Egypt, although, the deposed first lady of Egypt, Suzanne Mubarak, was diagnosed with cancer in 2000, she began discussing national cancer control in September 2010 (IAEA, 2010). Additionally, despite the presence of the Breast Cancer Foundation of Egypt (BCFE), the Ministry of Health and Population (MoHP) Egypt, and the Eastern Mediterranean Region office (EMRO), Egypt lacks a national cancer control program (NCCP). Similarly, Oman lacks a NCCP despite the presence of the National Association for Cancer Awareness (NACA), the Ministry of Health (MoH) Oman, and the WHO Oman.
On the contrary, in Jordan, the Jordan Breast Cancer Program (JBCP) along with the MoH Jordan and local WHO office developed the national Breast Cancer Screening and Diagnosis Guidelines, and a NCCP is established (e.g., JBCP, n.d.; MoH Jordan, n.d.). Similarly, in Morocco, Association Lalla Salma against Cancer (ALSC) leads Morocco’s NCCP along with MoH Morocco’s Cancer Prevention and Control Program (e.g., ALSC, n.d.; ALSC, n.d.). ALSC focuses on BC through its Breast and Cervical Cancer Early Detection Program. Meanwhile, the WHO Morocco provides general technical support to national health endeavors (WHO Morocco, 2011).
The distinction between countries with and without a NCCP is found vital for this study because it highlights the importance of networks in raising awareness on BC’s preventative and early detection measures, as well as the significance of these networks for the needed control of BC’s rising incidence and mortality rates in Arab countries. This study explores and evaluates the agents’ strength in applying tensions to the constraining structure for BC’s preventative and early detection measures through the lens of the ‘asabiyya-driven structuration framework.
What is ‘Assabiya?
‘Asabiyya, which generates from the root “‘asab” or to bind, implies binding individuals into a group (Kayapinar, 2008). Ibn Khaldûn’s The Muqaddimah is characterized by linguistic novelty because he reveals the deeper layers within conventional terms (Lawrence, 2005). The term has progressed from describing blood ties, family, and tribal organizations to referring to larger institutional structures or alliances and civilizations (Ibid). Ibn Khaldûn lends ‘asabiyya depth, breadth, and functionality by presenting its flexibility across time and space with his ambiguous take on it (e.g., Laroussi, 2005; 2008). Many Western scholars were intrigued by the concept of ‘asabiyya so they modernized it and applied it to Western societies throughout the centuries (e.g., Alatas, 2006b; Darling, 2007; Dhaouadi, 2005; 2008; Fromherz, 2010; Laroussi, 2008). Although ‘asabiyya emerged in the Middle-Eastern context of the 14th century, it has been modernized and transformed into a hybrid concept that bridges Western and Middle-Eastern cultures.
One of the most prominent translations describes ‘asabiyya as “the cohesive force of the group, the conscience that it has of its own specifity and collective aspirations, and the tension that animates it” (Lawrence, 2005: xv). ‘Asabiyya is one of Ibn Khaldûn’s “most untranslatable terms” and cannot have an equal synonym or translation (Kayapinar, 2008: 379-400). Ade Kearns and Ray Forrest (2000) analyze the dimensions of social cohesion within advanced societies, which encompass the elements of ‘asabiyya discussed in The Muqaddimah. Kearns and Forrest (2000) list the interlinked elements that indicate the presence and strength of ‘asabiyya: social networks and social capital, as well as social order and territorial functioning and belonging, or what Niklas Luhmann refers to as autopoiesis.
The Breast Cancer Context
The environment under study is the multifaceted and complex Arab society. The Arab society encompasses the female population at risk (due to the absence of preventative and early detection knowledge, attitudes, and behaviours), the environment structure, and distinct institutional clusters or social systems (e.g., Fuchs, 2003; Galaskiewicz & Wasserman, 1994; Wasserman & Faust, 1994). The definition of structure is adopted from Anthony Giddens as the “rules and resources, organized as properties of social systems” (1984: 25). The scarce resources are understood as the resources needed or sought by agents within the structure.
The Constraining Structure
The structural properties are the constraining and enabling “institutionalized features of social systems, stretching across time and space” (e.g., Giddens, 1984: 195; Haines, 1988: 171). The social system under study embodies the hybrid cluster of the CAs, GAs, and WHO agents in the Arab region that network to combat rising incidence and mortality rates of BC. The cluster’s structural properties include structural principles, which are understood as the agreed-upon or different self-referential distinct principles of the preventative and early detection measures (Giddens, 1984). The WHO promotes BC control within the context of comprehensive NCCPs, which include preventative and early detection components (WHO, 2011).
The environmental constraints consist of external structural constraints, which constitute environmental trends and social attitudes, and material constraints. The environmental trends include late stage discovery, inequalities in health service utilization, exposure to carcinogenic substances, unhealthy diet, overweight or obesity, physical inactivity, and tobacco use (e.g., Magrath & Litvak, 1993; Rastogi, Hildesheim & Sinha, 2004; WHO, 2004). The overlapping social attitudes include lack of awareness, negligence, fear, fatalism, low self-efficacy, stigma, and misinformation (e.g., Barg & Grier, 2008; El Saghir, 2008; JBCP, 2010; ALSC, 2006; Lamyian et al., 2007; Omar et al., 2003).
Moreover, the material constraints include themes of weak infrastructure, cost or time constraints, centralization, lack of or weak information technology systems, and lack of training and expertise (e.g., Madanat & Merrill, 2002; Magrath & Litvak, 1993; Rastogi, Hildesheim & Sinha, 2004; Shorbaji, 2006; WHO, 2005). The weak infrastructure constitutes weak epidemiological research capabilities, lack of training for health-related information communication technologies, and a general lack of protocols and ethical rules for health-related technology (e.g., Rastogi, Hildesheim & Sinha, 2004; Shorbaji, 2006; WHO, 2005). Furthermore, women do not attend to the proper screening measures because of cost or time constraints, inadequate or overcrowded healthcare clinics, inadequate distribution of clinics, lack of effective physician-patient relationship, and uninformed physicians and nurses (e.g., Madanat & Merrill, 2002; Magrath & Litvak, 1993).
The agents also face internal structural constraints, which constitute the differences in position-practice relations resulting in agents not fulfilling their role and their positioning (Giddens, 1984). Moreover, difference in structural principles or lack of adherence to the cluster by agents or subsystems causes internal structural constraints (Ibid). Themes of bureaucracy, lack of coordination, lack of unified and strategic focus, misuse of resources, management issues, lack of community mobilization, inactivity in setting policies and plans, and lack of political support are investigated.
The Agency of Social Networks
At the heart of the cluster within the social system are the CAs’, the GAs’, and the WHO agents’ social practices or social networks and autopoiesis. The components of a network are agents, resources, and relational ties (e.g., Giddens, 1984; Tucker, 1998; Vega-Redondo, 2007). Networks are evaluated based on elements of civic culture, social order, and social solidarity (Kearns & Forrest, 2000).
Civic culture is established when the group exhibits unified structural principles, cooperation, social action, social position, and social role (e.g., Alatas, 2006a; Ibn Khaldûn, 2005; Kearns & Forrest, 2000). Social order refers to mutual dependencies and goals between a group and its members, where they all share the resources within a network of obligations and expectations that lack internal contradictions (e.g., Ibn Khaldûn, 2005; Kearns & Forrest, 2000). This element encompasses rules, social power, and leadership. Lastly, the social solidarity element requires a lack of internal constraints, reduction in wealth disparities, and network of solidarity. The network of solidarity is a network with a high degree of diverse resources and ties including strong ties, weak ties, and cross-linkages, as well as community involvement (e.g., Angelusz & Tardos, 2001; Carpiano, 2008; Cattell, 2001). Strong ties embody partnerships including alliances and memberships, projects including campaigns and events, training including activities, leadership, plans, sponsorship, and reports including research. Weak ties include political support, recognition including respect, and donation (Galaskiewicz & Wasserman, 1994). Cross-linkages are represented by activity participation, conferences attendance, conference participation, discussions including meetings, kiosks, lectures, and references (Ibid).
The Agency of Autopoiesis
Autopoiesis is the process of strategic use of communication to self-create or maintain a system from the internal and external complexity (Luhmann, 1995). Autopoiesis is evaluated by the following criteria: communicative events, historical and self-descriptive references, interactions, recursivity, internal codes and guidelines, and functional subsystems (e.g., Goodman et al., 1997; Luhmann, 1995; Seidl & Becker, 2006). The process of autopoiesis refers to optimal territorial functioning and belonging element of ‘asabiyya, which is when members feel that they belong to a cluster, thereby willing to participate in its social networks. A small-scale territorial functioning and belonging is indicated through the lack of access to resources and mobility of members, whereas a large-scale territorial functioning and belonging is indicated through the strained operations of members and chieftain of the group (Kearns & Forrest, 2000). Optimal territorial functioning and belonging leads to social capital, or an enabling environment.
The Social Capital Structure
Pierre Bourdieu defines social capital as a collective asset shared by members of a defined group, with clear boundaries, obligation of exchange, and mutual recognition with a focus on resources, group membership, and networks (e.g., Bhandari & Yasunobu, 2009; Fulkerson & Thompson, 2008; Lin, 2001). Social capital is dissected into external social capital or social reproduction, and internal social capital or system reproduction, as well as potential social capital. External social capital embodies the forms of social support, social leverage, and social order (Carpiano, 2008). Social support is represented by implemented screening measures, and social leverage is represented by increased reach and awareness. Meanwhile, downstaging, increased incidence, decreased incidence levels, mortality rates, weight reduction, and smoking reduction represent social order. Internal social capital includes social support through networking and cancer-fighting tools (plans, booklets, programs that represents tools for fighting cancer), social leverage through networking, decentralization, and cancer-fighting tools, social order through cancer-fighting tools, and organizational participation through networking, decentralization, and cancer-fighting tools. The potential social capital is split into potential internal social capital and potential external social capital as well. Potential external social capital tackles three forms of social capital: social support through potential community empowerment and mammography units’ expansion, social leverage through potential awareness and community empowerment, and social order through potential comprehensive BC coverage. Meanwhile, potential internal social capital tackles the following forms of social capital: social support through potential networking, social leverage through potential information, networking, and cancer-fighting tools, social order through cancer-fighting tools, and organizational participation through cancer-fighting and potential networking. Social capital is one of the three indicators of ‘asabiyya.
Defining ‘Asabiyya-Driven Structuration
‘Asabiyya is understood as a hybrid and “cohesive force of the group, the conscience that it has its own specifity and collective aspirations, and the tension that animates it” (Lawrence, 2005: xv). The elements of ‘asabiyya are social networks, autopoiesis, and social capital. Structuration is defined as the constraints, social capital, social networks, and autopoiesis driving the continuity or transmutation of structures, thereby driving the reproduction of the cluster within the Arab society. Moreover, system reproduction is defined as the stability and continuity of the cluster, which can constitute or lead to progressive change within the cluster that enables it to cause further social reproduction due to autopoiesis and internal social capital (Bakken & Hernes, 2003). Meanwhile, social reproduction is understood as the progressive change in the environment that helps control incidence and mortality rates through external social capital (Cohen, 1989). So ‘asabiyya-driven structuration is the structuration driven by social networks, autopoiesis, and social capital—‘asabiyya’s three elements—for system and social reproduction of the BC context in the region.
If weakening, ‘asabiyya leads to an increase in constraining structure, thereby leading to cluster dissolution. This weakening is apparent when social networks, autopoiesis, and social capital—its three elements—are weakening. Absence of autopoiesis and social capital are demonstrated through the lack of their elements. In regards to weak social networks, it is presented by lack of the following: civic culture, social order, and social solidarity. The absence of power balance, leadership, and rules coupled with the presence of inclusion and exclusion, where members experience unequal access to resources embodies the absence of social order, which results in internal contradiction and disruption within the group (Lacoste, 1984). But as long as the group retains its ‘asabiyya, authority that disappears in one branch will, of necessity, pass to another branch of the same group (Ibn Khaldûn, 2005).
The deficiency of civic culture is indicated when BC or cancer are not prioritized, agents are unaware of their needs or incapable, and practice-position roles are not fulfilled. Moreover, structural contradiction exists due to differences in structural principles and priorities (Giddens, 1984). On the other hand, absence of social solidarity is indicated by unequal access to resources, excessive expansion, overwhelming cross-linkages, and unacknowledged needs. Excessive expansion causes a strain in the central node’s energy and operations or over dependence, which decreases the overall performance of the network (Vega-Redondo, 2007). Similarly, this weakening stems from cross-linkages that overwhelm from reserving its autonomy and strength to its internal operations (e.g., Vega-Redondo, 2007; Wellman, 1988). This increase in constraining structure followed by cluster dissolution or the shift of power from one branch to another is a progressive move because a more highly productive cluster that learns from its predecessors develops (e.g., Arneil, 2006; Fuchs, 2003). Finally yet most importantly, the duality of structure notion, which argues that structure is the driver to and outcome from social networks, serves as the underlying principle of this study (e.g., Haines, 1988; Magrath & Litvak, 1993; Rose, 2006).
Methodology
This study encompasses four research questions that explore and evaluate the environment and social system layers, as well as the ‘asabiyya-driven structuration. Hence, after exploring the context, this research explores the constraints, then explores and evaluates the social networks, autopoiesis, and social capital. The following questions are answered from the perspective of the CAs, GAs, and WHO agents:
RQ1: What is the context of BC’s preventative and early detection measures in Egypt, Jordan, Morocco, and Oman?
RQ2: What are the constraints that the CAs, the GAs, and the WHO agents face in networking for BC’s preventative and early detection measures in Egypt, Jordan, Morocco, and Oman?
RQ3: How do the CAs, the GAs, and the WHO agents network for BC’s preventative and early detection measures in Egypt, Jordan, Morocco, and Oman?
RQ4: What social capital is noted from the cluster of CAs, GAs, and WHO agents in Egypt, Jordan, Morocco, and Oman?
While RQ1 explores the agents’ scope of responsibility, as well as the scarce and valued resources, RQ2 explores the precondition of ‘asabiyya, environment constraints (material constraints and external structural constraints), and internal structural constraints. RQ3 examines and evaluates social networks and autopoiesis along with their components. Lastly, RQ4 examines and evaluates the external, internal, and potential social capital. All the research questions are posed to understand whether ‘asabiyya is strengthening or weakening in the region, as well as the current or potential ‘asabiyya-driven structuration, including system and social reproduction, or cluster dissolution.
This study employs a qualitative research design following an inductive style. A relevant sample of four countries is chosen through purposive sampling method. The following criteria are employed after a list of all the countries in the Arab League is compiled: the WHO EMR countries, war-related civil unrest, and the availability of a WHO office, CA, and a website for both, as well as high expenditure on health per capita for every region. These sampling criteria enable the exploration of the topic in a rich pool of networks and resources from all sub-regions of the Arab region. The four countries under examination represent the four sub-regions in the Arab region: Central Countries, Bilad al Sham or Greater Syria, Gulf Corporation Council, and the Maghreb. A generalization is made in regards to the Arab region through inductive reasoning. By exploring these four countries, this paper seeks richness of the information rather than representativeness and generalization. Nevertheless, the four countries are referred to as the Arab region mainly because of their location. Therefore, the qualitative findings are contingent to the four countries only.
In order to provide insight on the present and future of the CAs, the GAs, and the WHO agents, qualitative content analysis and in-depth interviews are carried out with NVivo as a tool for analysis. Eight informants are interviewed: one expert from the CA and the WHO NCD focal point in the GA. An ethical clearance from the Research Ethics Board at the University of Ottawa was obtained to conduct these interviews.
Findings and Discussion
The Progressive and Hierarchal Constraining Structure
The findings of the content analysis and in-depth interviews demonstrate a great deal on the dynamics of the ‘asabiyya-driven structuration of BC prevention and early detection in the Arab region. In this study, the social system under study embodies the hybrid cluster of CAs, GAs, and WHO agents. The scopes of responsibility for the fight against BC in the Arab region present common themes of structural principles (Giddens, 1984). While agents in countries with a NCCP realize that prevention and early detection are more cost-effective, agents in countries without a NCCP focus mainly on treatment (Magrath & Litvak, 1993). Another structural principle is relating BC to family planning, which increases venues to reach women and sponsors thereby expanding networks in Arab countries. However, this principle constricts countries without a NCCP; for example, at the MoH Oman the Family and Community Health Department’s and the EMRO’s screening pilot program does not involve the NCD Department at the MoH Oman. Most agents carry a country-specific scope of responsibility only except for the EMRO, the ALSC, and the BCFE. Additionally, the CAs carry most of the weight of BC responsibility, regardless of the GAs’ support. Nevertheless, political support is the most valued and scarce resource driving major constraints, especially in countries without a NCCP.
Information and research is generally lacking in regards to environmental constraints, which present the pre-condition to ‘asabiyya. However, prominent internal constraints transform the environmental constraints into barriers rather than drivers, which is the case in countries without a NCCP (Giddens, 1984). Nevertheless, the precondition of ‘asabiyya is met in countries with a NCCP because of the strong presence of environmental constraints and almost absent internal constraints (Ibid). The main internal constraint in the region is the lack of political support, bureaucracy, and unfulfilled position-practice relations. Since the countries with a NCCP witness political support through its nearly optimal social networks, most internal issues—similar to ones of countries without a NCCP—disappeared.
The Optimal and Weak Social Networks
The main ingredients in the journey to optimal networks are civic culture, social order, and social solidarity (Kearns & Forrest, 2000). In regards to the civic culture, countries without a NCCP lack cooperation, while ones with a NCCP witness unity of principles but differ on platform inclusion, where many health sector agents are not included in national BC efforts in Morocco (being addressed by MoH Morocco). Meanwhile, countries without a NCCP lack cooperation platforms so agents seek platforms abroad. Social action is present when CAs and WHO agents maximize their community and regional potential, as well as GAs that maximize their potential in spearheading the unity of making a difference to a pre-existing state of affairs, which is optimal in Jordan (Giddens, 1984). Countries without a NCCP witness social action from CAs, which maximize their social positioning, only. However, these countries lack local political positioning. By taking on regional and international roles thereby spreading their resources too thinly, countries without a NCCP fall behind on unified principles, cooperation, social action, social position, and social role, while countries with a NCCP nearly fulfill civic culture.
Like the civic culture element, the social order element is not fulfilled completely. However, balance of social power is present in Jordan and Morocco through a cyclic resource transmission where group members share the resources within the network of obligations and expectations of mutual dependencies, but the hierarchal resource transmission in the other Egypt and Oman calls for power balance (e.g., Ibn Khaldûn, 2005; Kearns & Forrest, 2000). On a regional level, the most central agents are the EMRO followed by the ALSC because they serve as the ultimate connector for the EMR Alliance against Cancer. On the country level, a consistent local chieftain that combats cancer actively and proactively is present in Jordan only, other countries present issues of inconsistency, absence, or ineffective chieftains that leads to lack of optimal rule creation. Although a general commonality of rules exists, Jordan is the only country witnessing full participation and unity for its scientifically driven and flexible rules.
Although social order is present, Jordan lacks community mobilization. On the other hand, community mobilization exists in Morocco despite the limited participation of health sector agents. Nevertheless, agents in countries with a NCCP are aware of these shortages, while most agents in ones without a NCCP are unaware of the dire shortages, which result in the absence of diversity and solidarity in their network. Agents in countries without a NCCP seek regional partnerships in the absence of country-specific networking and unity thereby spreading their limited resources too thinly. Similarly, agents in Morocco seek regional alliances when not completely fulfilling its network of solidarity. Overall, none of the countries under study fulfills social solidarity, social order, and civic culture for an optimal social network yet but countries with a NCCP are way ahead of ones without a NCCP.
The Strong and Vulnerable Shields of Autopoiesis
Similar trends are demonstrated when evaluating autopoiesis, or the strategic use of communication to self-create or maintain a system from internal and external complexity on the country level (Giddens, 1995). On the regional level, autopoiesis potential lies in the four countries distinct coded communication systems on the country level that have the potential to adhere and complement a regional system (e.g., Luhmann, 1995; Seidl & Becker, 2006). On the local level, GAs lack in autopoiesis the most, whereas WHO agents present WHO-specific autopoiesis. Currently the process of autopoiesis in the Arab region represents cases of small-scale and large-scale territorial functioning and belonging. Small-scale territorial functioning and belonging result from CAs that carry out agent-specific autopoiesis, which leads to a lack of access to resources and mobility of members. Moreover, large-scale territorial functioning and belonging exist in Morocco and Egypt where agents seek regional and international positioning before fulfilling internal position leading to strained operations of members and chieftain of the group (Kearns & Forrest, 2000). Ultimately, optimal social networks and its shield of autopoiesis require dire developments and changes to create an enabling structure.
The Presence and Absence of Social Capital Momentum
At the regional level, the potential social capital is present. However, on the country level, countries with a NCCP present more internal social capital and external social capital than countries without a NCCP. More specifically, the WHO agents in the four countries note the most internal social capital given their highly optimal and autopoietic network. Nevertheless, the CAs carry most of the potential social capital in countries with a NCCP, while WHO agents note the most potential in countries without a NCCP. Overall, countries with a NCCP, as well as WHO system, witness more capital on all levels: social support, social leverage, social order, and organizational participation. Countries with a NCCP present more potential for advancement due to their external and internal social capital than countries without a NCCP. Most importantly, external and internal social capital builds more potential social capital.
The momentum in social capital accumulation along with nearly optimal and autopoietic social networks—‘asabiyya’s element—drive social and system reproduction or structuration for countries with a NCCP as Figure 1 shows.
Figure 1: The Countries with a National Cancer Control Program Model
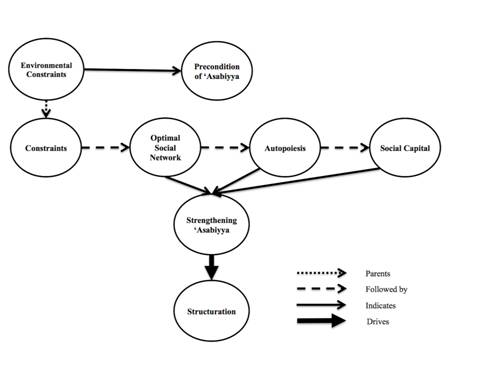
The model presents how countries with a NCCP are driving local BC structuration by their strengthening ‘asabiyya, which will enable them to fulfill autopoietic and optimal social networks. To overcome the shortages presented in these countries and accelerate their local BC structuration, some changes and development need to take place.
Countries without a NCCP present a different story as Figure 2 shows. Agents are leading a downhill battle facing BC and lack political support with weak social networks, vulnerable autopoiesis, and non-existent social capital.
Figure 2: The Countries without a National Cancer Control Program Model
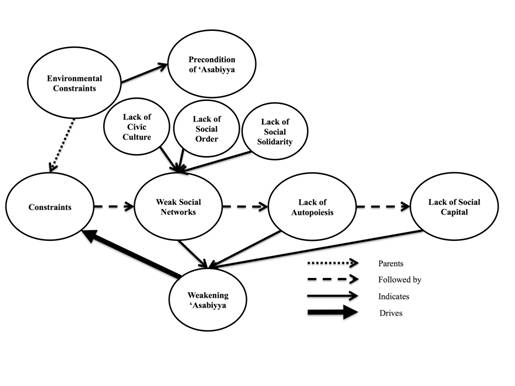
They present lack of mutual dependencies, leadership, and optimal rule creation in regards to inclusion and exclusion, which presents lack of social control (Lacoste, 1984). Moreover, most agents in countries without a NCCP lack capability, fulfillment of practice-position roles, and awareness of the magnitude of BC thereby BC is not a prioritized, topped with an absence of freedom of action. This situation presents lack of civic culture leading to structural contradictions (e.g., Cohen, 1989; Giddens, 1984). Furthermore, the countries without a NCCP witness excessive expansion straining the central node’s energy and overall performance of the network, and overwhelming cross-linkages (GAs excepted) leading to weakening autonomy for internal operations, as well as unacknowledged needs and unequal access to resources and benefits. Thus social solidarity is absent in countries without a NCCP (e.g., Vega-Redondo, 2007; Wellman, 1988). Overall, countries without a NCCP witness a weak social networks coupled with a lack of autopoiesis (e.g., Bakken & Hernes, 2003; Bhandari & Yasunobu, 2009; Lin, 2001). Additionally, autopoiesis is agent-specific, non-recursive, and lacks local, inclusive, scientific, and modifiable internal guidelines. Countries without a NCCP witness small-scale territorial functioning and belonging or large-scale territorial functioning and belonging. Lastly, the absence of an optimal and autopoietic social network leads to a lack of momentum in social support, social leverage, social order, and organizational participation, hence social capital is absent.
The Networking Struggle for Breast Cancer Structuration
Countries without a NCCP are limited because of their focus on treatment, and lack of coordination where the CAs carry all the weight. Nevertheless, the precondition of ‘asabiyya is met because of the presence of common environmental constraints on the country and regional level as the driving force. However, the internal constraints of countries without a NCCP present the absence of the most valued and scarce resource in the region—political support—that hinders the driving force of social networks. “Governments must show political commitment to progressively step up the implementation of high-quality screening and early detection programmes, which are an investment rather than a cost”, says Dr. Bernard W. Stewart, co-editor of World Cancer Report 2014 (WHO IARC, 2014).
Social networks remain at the country level with an absence of some important local ties. Nevertheless, seeds of regional networks have been planted. These seeds will not blossom until the countries under study reach an optimal local social network. The countries with a NCCP witness nearly optimal social networks, while countries without a NCCP are far behind. The vulnerable autopoietic shield results in small-scale and large-scale territorial functioning and belonging because CAs reach for alternatives due to GAs’ weak leadership of maintaining the system in the face of environmental complexity. On the other hand, the nearly autopoietic and optimal social network in countries with a NCCP lead to social capital.
The autopoietic and optimal social networks in countries with a NCCP lead to substantial internal and external social capital resulting in a progressive momentum of potential social capital. This momentum fosters an enabling structure for countries with a NCCP to keep moving forward for further social and system reproduction. Meanwhile, local social and system reproduction is absent in countries without a NCCP. Therefore, a regional network remains unattainable unless extensive changes and developments take place in each country to accelerate ’asabiyya-driven structuration locally.
This discussion indicates that countries without a NCCP witness a weakening ‘asabiyya facing the increasing BC constraints in the region. In countries without a NCCP, the increasing constraining structure followed by cluster dissolution is progressive because a new aware and productive cluster learns from its predecessors and the harsher environment.
Conclusion and Recommendations
Although both models demonstrate different outcomes, the ultimate outcome is similar. Struggle and agency leads inevitably to BC structuration in the region. By exploring and evaluating agents’ strength in applying tensions on the constraining BC structure, this study provides insight on the current and future networking struggle for BC structuration in the Arab region. After structuration is reached on the country level, a regional ‘asabiyya-driven structuration can be sought.
The overall goal of the strategic recommendations is to foster regional strengthening ‘asabiyya to combat BC successfully in the Arab region. This paper proposes that agents embrace two phases of change locally and regionally. On the country level, the first phase establishes optimal social networks for countries with and without a NCCP. In the first phase, it is proposed that Jordan mobilizes the community by involving the non-health sector, while Morocco develops a partnership with other health sector agents with ALSC as the main leadership. Generally, it is advised that agents in countries with and without a NCCP maximize scarce resource by adopting scientific thinking, collaborating with academic bodies, and developing scientific committees. More specifically, it is suggested that CAs in countries without a NCCP approach a local political figure seeking political recognition (preferably someone with family-based or personal experience with cancer) to adopt cancer or BC. It is proposed that this political figure leads the unity and maintain mutual dependencies through its institution by involvingthe GAs, NGOs, private sector, and WHO agents for the cause. Additionally, it is proposed that CAs and WHO agents employ their capability for community work and expertise. After social roles are fulfilled, it is recommended that agents in countries without a NCCP develop a local cluster by maximizing local positioning. This paper suggests that Egypt forms weak ties first, and then Egypt and Oman strengthen their ties through local projects and alliances. It is advised that agents in countries without a NCCP employ international and regional ties as cross-linkages only to remain focused locally. These recommendations for optimal social networks set the stage for autopoietic work.
The second phase aims at autopoiesis or optimal territorial functioning and belonging on the country level. It is advised that agents seek interactions on a need-basis. This paper recommends that agents in countries without a NCCP undergo communicative events by processing information internally from interactions and utterance into understanding. It is proposed that agents develop their own modifiable internal guidelines based on local scientific data or internally processed external recommendations. This paper advises that all local health-related agents under the umbrella of the chieftain follow local routine scientific research to create these guidelines. It is recommended that GAs in countries with and without a NCCP present routine BC work more often. Meanwhile, it is advised that CAs present country-specific recursivity more often. Moreover, this paper suggests that CAs in Egypt, Jordan, and Oman propose an annual and local cancer-specific event to the political figure for approval. Overall, the optimal and autopoietic social networks recommendations for countries with and without a NCCP are proposed to build strategies for ‘asabiyya-driven structuration on the country level.
After local structuration is reached in Arab countries (as well as countries in the regional alliance), it is suggested that the first regional phase harnesses and expands upon the potential and current networks for regional goals of combatting BC. Since the EMR Alliance against Cancer includes almost all CAs in Arab countries with a focus on combating cancer in the region, this alliance can be harnessed. It is proposed that the network include strong ties, weak ties, and cross-linkages with the necessary political support specific to regional health and cancer domain. This paper suggests that this alliance creates a regional committee and an international advisory committee. It is advised that these committees begin by compiling and processing research from each country and develop a regional cancer registry as the first step to utilizing social positioning and establishing social roles. It is necessary that this alliance include local leadership, or politically powerful agents from each country. This paper advises that all chieftains participate in creating regional plans and guidelines based on scientific data under the umbrella of the EMRO and ALSC, the main chieftains of this alliance. It is suggested that the main chieftains ensure the power is balanced and all agents are involved in the creation of a common framework of definitions, rules, priorities, and laws. This paper advises that the leadership ensures no reduction in wealth disparities, as well as recognition of members’ need if country-specific needs arise. Additionally, it is recommended that agents ensure open access to resources for the ultimate goal of networking to eradicate BC on the regional level. Overall, the first phase recommendations propose that the EMR Alliance against Cancer fulfills an optimal social network, which requires autopoiesis to be maintained.
In phase two, it is proposed that the optimal territorial functioning on the regional level fulfill communicative events, historical and self-descriptive references, recursivity, and internal guidelines similar to that of the WHO agents, when establishing roots in Arab countries. Overall, the recommendations for reaching optimal and autopoietic social networks on the country level are proposed to provide the platform for the ultimate goal of optimal and autopoietic social networks on the regional level. These recommendations seek to achieve the overall goal, which is to foster regional strengthening ‘asabiyya to combat BC successfully in the Arab region.
This research merely investigates the tip of the iceberg. This research is unique in its nature, as it is the first research that aims to tackle BC from a non-medical, regional, and preventative and early detection perspective, hence, each theme explored can be investigated further. Many hurdles are present to study this topic including but not limited to: lack of information and disinterested informants. Furthermore, the instability caused by the Arab uprisings during 2011 made it challenging to get ahold of the informants and convince them to participate in the interview. Additionally, the lack of digital informational databases made it challenging to collect publications for content analysis. These challenges provide insight on many constraints and research opportunities in the region. This thesis overcame these challenges and rich data was collected and analyzed. This research presents the situation in four Arab countries only, thus, it represents an introduction to a comprehensive research project on all Arab countries. This study serves as a foundation for other studies that can cover one of the themes or concepts further in this region or other regions with similar conditions. |
References
Alatas, Syed F. (2006a). A Khaldûnian exemplar of a historical sociology for the south. Current Sociology, 54(3), 397-411.
Alatas, Syed F. (2006b). Ibn Khaldûn and contemporary sociology. International Sociology, 21(6), 782-795.
Angelusz, Róbert & Tardos, Róbert. (2001). Change and stability in social network resources: The case of Hungary under transformation. In Nan Lin, Karen S. Cook and Ronald S. Burt (Eds.), Social capital: Theory and research (pp. 297-320). New York: Aldine de Gruyter.
Arneil, Barbara. (2006). Diverse communities: The problem with social capital. Cambridge, UK: Cambridge University Press.
Association Lalla Salma against Cancer (ALSC). (2006, March 7). Connaissances, perceptions and attitudes a l’egard du cancer, [Press release]. Rabat, Morocco: Association Lalla Salma against Cancer.
Association Lalla Salma against Cancer (ALSC). (n.d.). Plan cancer 2010-2019. Retrieved September 22, 2011, from http://www.contrelecancer.ma/fr/plan-cancer?set_language=fr.
Bakken, Tore & Hernes, Tor. (Eds.). (2003). Autopoietic organization theory: Drawing on Niklas Luhmann’s social systems perspective. Herndon, VA: Copenhagen Business School Press.
Barg, Frances K. & Grier, Sonya A. (2008). Enhancing breast cancer communications: A cultural models approach. International Journal of Research in Marketing, 25(4), 335-342.
Bhandari, Humnath & Yasunobu, Kumi. (2009). What is social capital?: A comprehensive review of the concept. Asian Journal of Social Science, 37(3), 480-510.
Burt, Ronald S. (2008). Positions in networks. In Linton C. Freeman (Ed.), Social network analysis (pp. 145-177). London: Sage Publications.
Carpiano, Richard M. (2008). Actual or potential neighborhood resources for health: What can Bourdieu offer for understanding mechanisms linking social capital to health? In Ichiro Kawachi, S. V. Subramanian and Daniel Kim (Eds.), Social capital and health (pp. 83-94). New York: Springer New York.
Cattell, Vicky. (2001). Poor people, poor places, and poor health: The mediating role of social networks and social capital. Social Science & Medicine, 52(10), 1501-1516.
Cohen, Ira J. (1989). Structuration theory: Anthony Giddens and the constitution of social life. Basingstoke, UK: Macmillan.
Darling, Linda T. (2007). Social cohesion, ‘asabiyya, and justice in the late medieval middle east. Comparative Studies in Society and History, 49(2), 329-357.
Dhaouadi, Mahmoud. (2005). The ibar: Lessons of Ibn Khaldûn’s umran mind. Contemporary Sociology, 34(6), 585-591.
El Saghir, N. S. (2008). Responding to the challenges of breast cancer in Egypt and other Arab countries. National Cancer Institute, 20(4), 309-312.
Fromherz, Allen J. (2010). Ibn Khaldûn: Life and times. Edinburgh, UK: Edinburgh University Press.
Fuchs, Christian. (2003). Some implications of Pierre Bourdieu’s works for a theory of social self-organization. European Journal of Social Theory, 6(4), 387-408.
Fulkerson, Gregory M. & Thompson, Gretchen H. (2008). The evolution of a contested concept: A meta-analysis of social capital definitions and trends 1988-2006. Sociological Inquiry, 78(4), 536-557.
Galaskiewicz, Joseph & Wasserman, Stanley. (Eds.). (1994). Advances in social network analysis: Research in the social and behavioral sciences. Thousand Oaks, CA: Sage Publications.
Giddens, Anthony. (1984). The constitution of society: Outline of the theory of structuration. Cambridge, UK: Polity Press.
Goodman, Robert M., Steckler, Allan & Alciati, Marianne H. (1997). A process evaluation of the National Cancer Institute’s Data-based Intervention Research program: A study of organizational capacity building. Health Education Research, 12(2), 181-197.
Haines, Valerie A. (1988). Social network analysis, structuration theory and the holism-individualism debate. Social Networks, 10(2), 157-182.
Ibn Khaldûn, ‘Abd-ar-Rahman M. (2005). The Muqaddimah: An introduction to history. (Franz Rosenthal, Trans.). Princeton, NJ: Princeton University Press. (Original work published 1377).
International Atomic Energy Agency (IAEA). (2010). Suzanne Mubarak, Egypt's first lady, talks about fighting cancer in Africa. Retrieved September 9, 2011, from http://www.iaea.org/newscenter/news/2010/mubarak.html.
Jones, Mathew R. & Karsten, Helena. (2008). Giddens’s structuration theory and information systems research. MIS Quarterly, 32(1), 127-157.
Jordan Breast Cancer Program (JBCP). (2010). Annual newsletter. Amman, Jordan: Jordan Breast Cancer Program.
Kayapinar, Akif M. (2008). Ibn Khaldûn’s concept of assabiyya: An alternative tool for understanding long-term politics?. Asian Journal of Social Science, 36(3), 375-407.
Kearns, Ade & Forrest, Ray. (2000). Social cohesion and multilevel urban governance. Urban Studies, 37(5-6), 995-1017.
Lacoste, Yves. (1984). Ibn Khaldûn: The birth of history and the past of the third world. London: Verso.
Lamyian, May, Hydarnia, Al-Irda, Ahmadi, Fadhl, Faghihzadeh, Soghrate & Aguilar-Vafaie, Maria E. (2007). Barriers to and factors facilitating breast cancer screening among Iranian women: A qualitative study. Eastern Mediterranean Health Journal, 13(5), 1160-1169.
Laroussi, Amri. (2008). The concept of ‘umran: The heuristic knot in Ibn Khaldûn. The Journal of North African Studies, 13(3), 351-361.
Lawrence, Bruce B. (2005). Introduction to the 2005 edition. In ‘Abd-ar-Rahman M. Ibn Khaldûn, The Muqaddimah: An introduction to history (pp.vii-xxv). Princeton, NJ: Princeton University Press.
Lin, Nan. (2001). Building a network theory of social capital. In Nan Lin, Karen Cook and Ronald S. Burt (Eds.), Social capital: Theory and research (pp. 3-30). New York: Aldine de Gruyter.
Luhmann, Niklas. (1995). Social systems. (John Bednarz & Dirk Baecker, Trans.). Stanford, California: Stanford University Press.
Madanat, Hala & Merrill, Ray M. (2002). Breast cancer risk-factor and screening awareness among women nurses and teachers in Amman, Jordan. Cancer Nursing, 25(4), 276-282.
Magrath, Ian & Litvak, Jorge. (1993). Cancer in developing countries: Opportunity and challenge. Journal of the National Cancer Institute, 85(11), 862-874.
Ministry of Health Egypt (MoH Egypt). (2010). Egypt national cancer registry: Aswan profile 2008. Cairo, Egypt: Ministry of Health Publications.
Ministry of Health Jordan (MoH Jordan). (2008). Jordan cancer registry: Cancer Incidence in Jordan. Amman, Jordan: Ministry of Health Publications.
Ministry of Health Morocco (MoH Morocco). (2009). Cancer incidence in Rabat 2005. Rabat, Morocco: Ministry of Health Publications.
Ministry of Health Oman (MoH Oman). (2009). Cancer incidence in Oman report of 2009. Muscat, Oman: Ministry of Health Publications.
Omar, S., Khaled, H., Gaafar, R., Zekry, A. R., Eissa, S. & El-Khatib, O. (2003). Breast cancer in Egypt: A review of disease presentation and detection strategies. Eastern Mediterranean Health Journal, 9(3), 448-483.
Rastogi, Tanuja, Hildesheim, Allan & Sinha, Rashmi. (2004). Opportunities for cancer epidemiology in developing countries. Nature Reviews Cancer, 4(11), 909-917.
Rose, Randall A. (2006). A proposal for integrating structuration theory with coordinated management of meaning theory. Communication Studies, 57(2), 173-196.
Seidl, David & Becker, Kai Helge. (2006). Organizations as distinction generating and processing systems: Niklas Luhmann’s contribution to organization studies. Organization, 13(1), 9-35.
Shorbaji, Nagib. (2006). E-Health in the Eastern Mediterranean Region. Cairo, Egypt: WHO Publications.
Tucker, Kenneth H. (1998). Anthony Giddens and modern social theory. London: Sage Publications.
Vega-Redondo, Fernando. (2007). Complex social networks. New York: Cambridge University Press.
Wasserman, Stanley & Faust, Katherine. (1994). Social network analysis: Methods and applications. Cambridge, UK: Cambridge University Press.
Wellman, Barry. (1988). Structural analysis: From method and metaphor to theory and substance. In Barry Wellman and Stephen D. Berkowitz (Eds.), Social structures: A network approach (pp. 19-62). New York: Cambridge University Press.
World Health Organization (WHO). (2004). Global strategy on diet, physical activity and health. Geneva, Switzerland: WHO publications.
World Health Organization (WHO). (2005). Noncommunicable diseases: Challenges and strategic directions. (EM/RC52/R.7). Geneva, Switzerland: WHO Publications.
World Health Organization (WHO). (2009). Towards a strategy for cancer control in the Eastern Mediterranean region. (WHO-EM/NCD/060/E). Cairo, Egypt: WHO Publications.
World Health Organization (WHO). (2011). Breast cancer: Prevention and control. Retrieved March 15, 2011, from http://www.who.int/cancer/detection/breastcancer/
en/index3.html.
World Health Organization Morocco (WHO Morocco). (2011). OMS-Maroc. Retrieved September 22, 2011, from http://www.emro.who.int/morocco/oms-rabat.
World Health Organization, International Agency for Research on Cancer (WHO IARC). (2014, February 3). Global battle against cancer won’t be won with treatment alone: Effective prevention measures urgently needed to prevent cancer crisis, [Press Release]. London: WHO IARC. Retrieved February 10, 2014, from http://www.iarc.fr/en/media-centre/pr/2014/pdfs/pr224_E.pdf. |


