
Public Health Agency of Canada
www.publichealth.gc.ca
Common menu bar links
Institutional links
Diseases & Conditions
Health & Safety
Research & Statistics
Agency Information
Search Box
Special Report of
the Canadian Tuberculosis Committee
Tuberculosis Among the Aboriginal
Peoples of Canada, 2000 to 2004
Tuberculosis Prevention and Control, Public Health Agency of Canada and First Nations and Inuit Health Branch, Health Canada
Background
The incidence rate of active tuberculosis (TB) in Canada is considered low, especially in the global context. Canada’s overall TB incidence rate in 2004 was 5.0 per 100,000 population. However, the incidence rate of TB in Canada is comprised of the combined rates of three originbased groups: ‘Canadian-born Aboriginal peoples’, ‘Canadian-born non-Aboriginal’, and ‘foreign-born’, each with its own unique risk-factor and epidemiologic profile. Examination of the epidemiology of TB in these groups reveals large differences in the incidence rate of TB, with the highest rates reported among Canadian-born Aboriginal peoples.
Various reports have described the epidemiology of TB in Canadian-born Aboriginal peoples1-3 highlighting prevention strategies, disproportionately high rates of disease, and a contrasted demographic and clinical picture when compared to the other origin-based groups. This report updates the epidemiology of TB among Aboriginal peoples of Canada and further examines selected demographic and clinical characteristics of persons with TB in this population.
Methods
Cases of new or relapsed TB disease reported to the Canadian Tuberculosis Reporting System (CTBRS) from 2000 to 2004 were examined. Cases of TB are reported to the CTBRS from each of the 10 provinces and 3 territories according to the national case definition. The CTBRS contains clinical and demographic characteristics on each case including origin. For this report, cases were divided into the following groups: Canadian-born Aboriginal peoples (Status and non-Status North American Indians*, Métis† and Inuit‡ peoples), Canadian-born non- Aboriginal and foreign-born. If origin or other data were reported as unknown, the case was excluded from the analysis.
* Indian people in Canada, both “status” and “non-status”. Status Indians are registered with the federal government as Indians, according to the terms of the Indian Act.
† People of mixed Aboriginal and European ancestry who identify themselves as Métis and are distinct from First Nations people, Inuit or non-Aboriginal people.
‡ An Aboriginal people in Northern Canada, who live primarily in Nunavut, Northwest Territories, northern Quebec and northern Labrador. The word means “people” in the Inuit language – Inuktitut.
Updated annual population estimates by geography, age and sex for the overall Canadian4, total Aboriginal, Inuit, and Métis5 groups were obtained from Statistics Canada. Foreign-born population estimates are based on the 2001 census in a Statistics Canada, Demography Division customized product. Population estimates specific to the Status (North American) Indian group were obtained from Indian and Northern Affairs Canada6 §. Coinciding updated population estimates for the non-Status North American Indian group were not available; therefore rates for this group are not included in this report. Updated population estimates are also not available for total Aboriginal, Inuit, Métis and foreign-born groups prior to 2001. For some graphs, historical rates using previously published population estimates and projections from different sources are displayed. Proportions are calculated using only cases with complete data in the denominator. Epidemiologic data are presented cumulatively for cases identified and reported from 2000 to 2004, unless otherwise specified.
§ The INAC population estimates are believed to be more accurate estimates of the true population counts for those identifying themselves with Status Indian origin.
Results
Incidence rate
From 2000 to 2004, 8,397 new and relapsed TB cases were reported to the CTBRS. Origin data were available for 8,229 (98%) of these cases. A total of 1,330 (16%) cases were reported as Canadian-born Aboriginal, 1,300 (16%) cases occurred in Canadian-born non-Aboriginals and 5,599 (68%) were among foreign-born individuals. Incidence rates reveal a disproportionate burden of disease among Aboriginal peoples. In 2004, the total Aboriginal rate was 4.8 times higher than the Canadian rate and 26.4 times higher than the rate of Canadian-born non- Aboriginals (see Table SR-1).
Table SR-1
| Origin Group | Number of Cases | Proportions of Cases | Rate |
|---|---|---|---|
| Canadian born – Aboriginal* | 268 | 16.6 | 23.8 |
| Status (registered) Indian | 202 | 12.5 | 27.5 |
| Inuit | 41 | 2.5 | 80.4 |
| Métis | 6 | 0.4 | 1.9 |
| Non-status Indian** | 19 | 1.2 | – |
| Canadian born non-Aboriginal | 214 | 13.3 | 0.9 |
| Foreign-born | 1,115 | 69.1 | 16.6 |
| Unknown | 16 | 1.0 | |
| Canada |
1,613 |
100.0 |
5.0 |
| * Canadian-born Aboriginal = Status (registered) Indian + Inuit + Métis + Non-status Indian ** Rate for non-status Indian not available as there are no accurate population estimates available |
|||
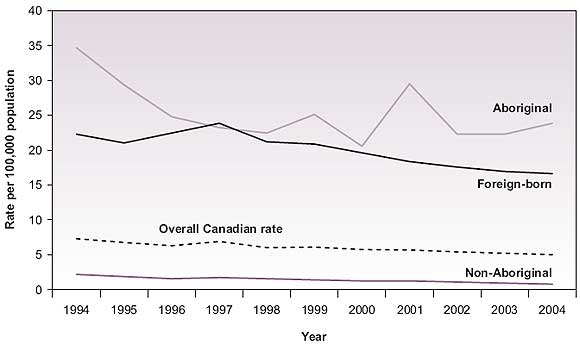
During the early 1990's the incidence rate of TB among Aboriginal peoples showed consistent decline. Though subject to fluctuations, the incidence of TB in this population since then appears to be stabilizing at a disproportionately high rate (see Figure SR-1).
Figure SR-1
TB incidence rate by origin – Canada: 1994**-2004
TB rates among individual Aboriginal groups showed varying patterns (see Figure SR-2). The incidence rate among Status Indians declined slowly during the 1990s. However it now appears to have stabilized. The incidence rate among the Métis has remained low at a median rate of 1.8 per 100,000††. The most striking finding is the rate of disease among the Inuit group. Large fluctuations in the incidence rate are evident, due to periodic outbreaks occurring in a relatively small population. In order to examine the trend in the incidence rate among the Inuit, the three-year moving averages of the incidence rate is presented in Table SR-2.
**Population denominators for the total Aboriginal population are not available prior to 1994
†† Separate population estimates are not available for the Métis group prior to 2001.
Figure SR-2
TB incidence rate by Aboriginal origin – Canada: 1994-2004
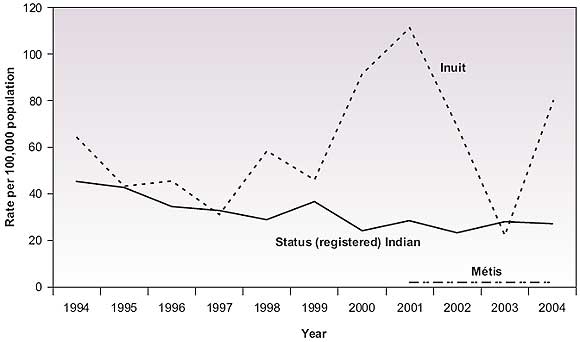
Table SR-2
| Year | Cases | Incidence rate | Three-year moving average rate |
|---|---|---|---|
| 1994 | 35 | 64.5 | |
| 1995 | 24 | 43.1 | 51.0 |
| 1996 | 26 | 45.5 | 39.8 |
| 1997 | 18 | 30.9 | 45.0 |
| 1998 | 35 | 58.7 | 45.2 |
| 1999 | 28 | 45.9 | 65.4 |
| 2000 | 56 | 91.5 | 82.9 |
| 2001 | 53 | 111.4 | 90.2 |
| 2002 | 33 | 67.8 | 67.1 |
| 2003 | 11 | 22.1 | 56.7 |
| 2004 | 41 | 80.4 |
Geographic distribution
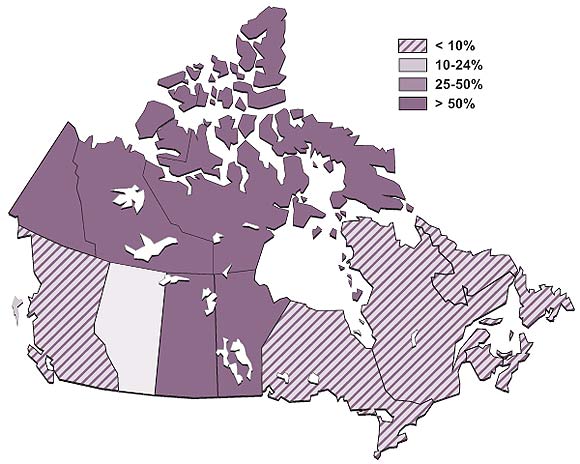
Figure SR-3 presents the proportion of cases with Aboriginal origin in the provinces and territories. Proportions were highest in the Prairie provinces and the North (includes Northwest Territories, Nunavut and Yukon).
Figure SR-3
Proportion of total TB cases in Aboriginal peoples by province/territory – Canada: 2004
Age and sex
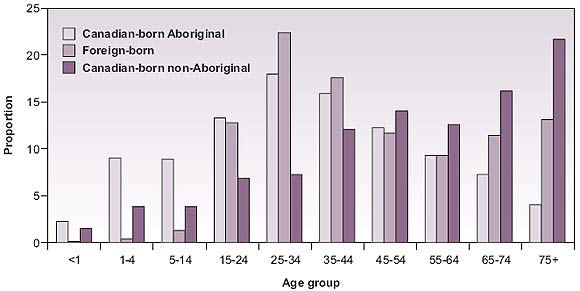
The age profile of TB cases differs greatly between the three origin-based groups. Thirty-five percent of cases among Aboriginal peoples were less than 25 years old at diagnosis compared with only 16% among Canadian-born non-Aboriginals and 14% among foreign-born cases. Persons aged 65 years and older accounted for only 12% of Aboriginal TB, whereas this demographic represented 38% of all TB reported in Canadian-born non-Aboriginals and 24% of foreign-born cases (Figure SR-4). Accordingly, cases among Aboriginal peoples were younger (median 34 years) than cases among Canadian-born non-Aboriginal people (median 55 years) and the foreign-born (median 42 years). Males accounted for a majority of reported cases in all ethnic origins (Aboriginal 54%, Canadian-born non-Aboriginal 65%, foreign-born 51%).
Figure SR-4
Proportion of TB cases by age group and origin – Canada: 2000-2004
Clinical presentation
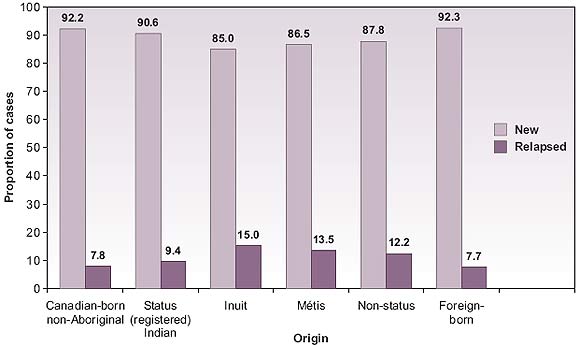
A history of previous TB disease (relapsed case) was reported for 657 (8%) of cases. More cases among Aboriginal peoples were reported as relapsed (11%) compared to cases among Canadianborn non-Aboriginal (8%) and the foreign-born (8%) (Figure SR-5).
Figure SR-5
Proportion of cases reported as new or relapsed by origin – Canada: 2000-2004
The proportion of cases among Aboriginal peoples presenting as primary TB (19%) was higher than those among Canadian-born non-Aboriginal (2.4%) and foreign-born (6.4%) (Figure SR-6).
Figure SR-6
Proportion of tuberculosis cases by main diagnostic site and origin – Canada: 2000-2004
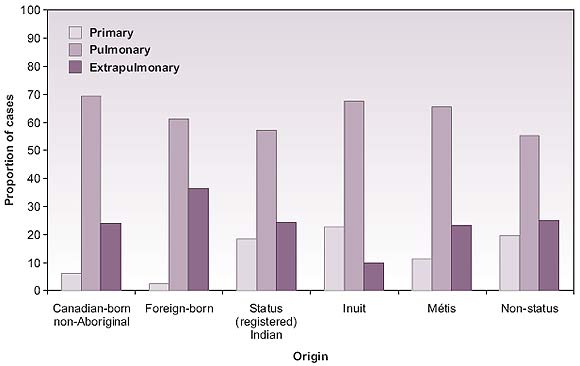
The proportion of cases among Aboriginal peoples that were pulmonary smear positive (34%) was similar to cases among Canadian-born non-Aboriginal (32%) but higher than cases among the foreign-born (21%).
For cases of pulmonary TB, the proportion of those with cavitary‡‡ disease was highest among Canadian-born Aboriginal peoples (11%) [Canadian-born non-Aboriginal cases (4%); foreignborn cases (3%)].
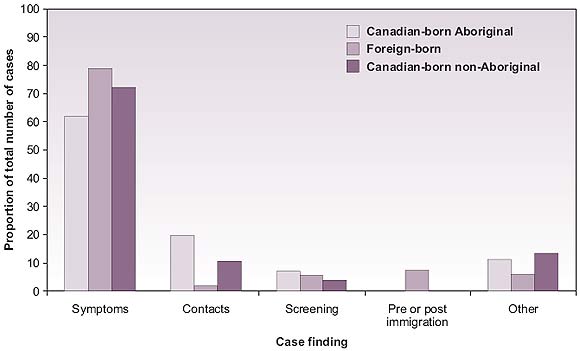
Cases among Aboriginal peoples were least likely to be detected through the identification of symptoms (62%) as compared with 72% of cases among the Canadian-born non-Aboriginal and 79% among the foreign born. (Figure SR-7).
‡‡ Derived as a percent of all pulmonary cases using the ICD-9 or ICD-10 codes for tuberculosis of lung with cavitation.
Figure SR-7
Case finding by origin – Canada: 2000-2004
Drug resistance
Table SR-3 presents the proportion of cases, by origin, with any drug resistance and with multidrug resistance.
Table SR-3
| Origin group | Resistance % (n) |
|
|---|---|---|
Any drug resistance |
MDR-TB |
|
| Canadian-born Aboriginal |
1.7 (23) | 0.2 (2) |
| Canadian-born non-Aboriginal |
5.3 (69) | 0.3 (4) |
| Foreign-born cases |
10.0 (562) | 1.2 (69) |
| Canada |
7.9 (654) |
0.9 (75) |
HIV co-infection
The HIV status of TB cases is largely underreported in Canada. HIV status was known in only 30% of the Canadian-born Aboriginal cases, 15% of the Canadian-born non-Aboriginal cases and 15% of the foreign-born cases. Using available data, the proportion of cases who were HIV seropositive was 16% in Canadian-born Aboriginal cases, 24% of the Canadian-born non- Aboriginal cases and 8% of the foreign-born cases. In the unlikely event that these were the only co-infected cases, the co-infection rates were 5% among Canadian-born Aboriginal TB cases, 4% among Canadian-born non-Aboriginal cases and 1% among the foreign-born cases.
Treatment and treatment outcomes
In cases for which treatment mode was reported, the proportion of Aboriginal TB cases that were treated using directly observed therapy (DOT) was higher 1,036 (90%) than both Canadian-born non-Aboriginal 228 (48%) and foreign-born 665 (36%) TB cases. Treatment mode was missing in 59% of all cases. Table SR-4 presents the treatment outcome for all cases by origin group.
Table SR-4
| Origin group | Outcome % (n) |
||
|---|---|---|---|
Cured or treatment completed |
Death |
Other |
|
| Canadian-born Aboriginal |
85 (216) | 8 (19) | 7 (18) |
| Canadian-born non-Aboriginal |
74 (96) | 10 (13) | 16 (20) |
| Foreign-born cases |
77 (726) | 3 (25) | 20 (188) |
| Canada |
79 (1,038) |
4 (57) |
17 (226) |
| * ‘Other’ includes ‘treatment failure’, ‘absconded’ and ‘treatment ongoing’. | |||
Discussion
This report provides a five-year profile of TB among Aboriginal peoples of Canada. The rate of TB disease among Canadian Aboriginal peoples has stabilized at a level substantially higher than Canadian-born non-Aboriginals and the foreign-born. The geographic distribution of TB rates remains constant, with higher disease burden among Aboriginal peoples in the North and lowest in the East. This is consistent with the prevailing theory of disease presentation related to time of first contact with European settlers2-8 . TB cases among Canadian Aboriginal peoples appear to be younger with higher proportions of relapsed cases and diagnoses of primary disease.
Higher rates of cavitary disease and primary TB suggest delayed detection of disease and ongoing transmission of infection in the community. These findings highlight challenges in access and delivery of health care in some Aboriginal communities and the need for greater vigilance or suspicion of TB symptoms by health care practitioners.
High cure and treatment completion rates are encouraging and TB drug-resistance has still not emerged as an issue of concern among Canadian Aboriginal peoples. This may be related to higher proportion of cases being treated using directly observed therapy (DOT). Nevertheless, vigilance must be maintained through active clinical follow-up of cases and contacts under treatment.
Given that the HIV status of TB cases is largely underreported in Canada, the proportions reported here are likely overestimates, biased towards testing in those with co-existing risk factors of HIV infection. The World Health Organization has estimated HIV prevalence in all adult incident TB cases in Canada for 2004 to be 8.7%9 . The lack of sufficient data on HIV coinfection in TB cases highlights the need for systematic HIV testing and reporting for all TB cases in Canada. This information is vital for monitoring the progress of the prevention and control of TB in Canada including in Aboriginal peoples.
The fact that the burden of TB disease in Canadian-born Aboriginals remains at over 25 times that of the Canadian-born non-Aboriginal peoples in 2004 is unacceptable. In fact, this rate disparity has increased from 20 times the non-Aboriginal rate in 19993 . With country of birth in common, attributable risk factors may include a large reservoir of illness in some Aboriginal communities and challenges in providing adequate primary and public health services to peoples in remote areas. Furthermore, many Aboriginal peoples in Canada face lower socioeconomic conditions leading to malnutrition and over-crowded living conditions. Further challenges to the prevention and control of TB include high prevalence of latent TB infection, higher rates of diabetes and end-stage renal disease, genetic factors, factors related to living in isolated communities, substance abuse, and HIV10,11,12 .
In the spirit of the Stop TB Global Plan goal of halving the prevalence of TB disease worldwide by 2015, the Canadian Tuberculosis Committee has established a goal of reaching a national incidence rate of 3.6/100,000 population by 201513 . In order to reach this goal, significant decreases in the rate of TB in Canadian-born Aboriginal peoples are required. These decreases are highly dependent on improvements in socio-economic conditions, early detection of cases, improved TB knowledge and vigilance in primary healthcare workers, appropriate and complete treatment, and the availability of adequate resources.
Reference List
- Enarson DA. Tuberculosis in Aboriginals in Canada. Int J Tuberc Lung Dis 2001; 2(9):S16-S22.
- Hoeppner V, Marciniuk D. Tuberculosis in aboriginal Canadians. Can Respir J 2000; 7(2):141-146.
- Public Health Agency of Canada. Tuberculosis in Canadian-born Aboriginal peoples. Public Health Agency of Canada; 2002. URL: http://www.phac-aspc.gc.ca/publicat/tbcbap-tbpac/special_report-eng.php
- Statistics Canada, Demography Division, Demographic, Estimates Section, Population estimates 0-90+ July Canada - Provinces 1971-2005. 2005. Ottawa, Statistics Canada. 11-22-0050.
- Statistics Canada. Projections of the Aboriginal populations, Canada, provinces and territories 2001 to 2017. 91-547-XIE. 2005. Ottawa, Statistics Canada.
- Registered Indian Population by Sex and Residence 2003. INAC [ 2003 Available from: URL: http://www.aincinac. gc.ca/pr/sts/rip/rip03_e.pdf
- Phypers, M. Special Report of the Canadian Tuberculosis Committee. Tuberculosis and HIV Co-Infection in Canada. CCDR, April 15 2007; 33 (8).
- Waldram JB, Herring DA, Young TK. Contact with Europeans and infectious diseases. In: Aboriginal health in Canada. Toronto: University of Toronto Press Incorporated, 1995;43-64
- World Health Organization. Global tuberculosis control: surveillance, planning, financing. WHO Report 2006. Geneva: World Health Organization, 2006 (WHO/HTM/TB/2006.362).
- MacMillan HL, MacMillan AB, Offord DR, Dingle JL. Aboriginal Health. Can Med Assoc J 1996, 155(11):1569-1578.
- Public Health Agency of Canada. Housing conditions that serve as risk factors for tuberculosis infection and disease. CCDR 2007;33(ACS-9):1-13.
- Tuberculosis Control in First Nations and Inuit Populations. In: Long R, Ellis E, editors. Canadian Tuberculosis Standards. 6th edition. Ottawa, ON: Public Health Agency of Canada. In press 2007: 298-307.
- Stop TB Partnership and World Health Organization. Global Plan to Stop TB 2006-2015. Geneva: World Health Organization, 2006 (WHO/HTM/STB/2006.35).
Acknowledgements
Alberta Health and Wellness Division of Tuberculosis Control Manitoba Tuberculosis Control Program Department of Health and Wellness Department of Health and Community Services Department of Health and Social Service Office of the Chief Medical Officer of Health Department of Health & Social Services Vaccine Preventable Diseases and TB Control Unit Department of Health and Social Services |
Direction de la Protection de la Santé Publique Tuberculosis Control Program Department of Health and Social Services, Yukon Association of Medical Microbiology and Infectious Disease Canada Canadian Lung Association Canadian Public Health Laboratory Network Canadian Thoracic Society Citizenship and Immigration Canada Correctional Service Canada First Nations and Inuit Health Branch National Microbiology Laboratory Tuberculosis Prevention and Control |